Embed Size (px)
Citation preview
16 November 2012Respiratory Physiology
Lab this week: EKGs and Blood Pressure. Bring calculator and textbook to lab.
Wear clothes and shoes you can run in comfortably.
Work on Hemorrhage Diagram!
Nice, concise review of CV Physiologywith excellent figures
1QQ 28 for 8:30
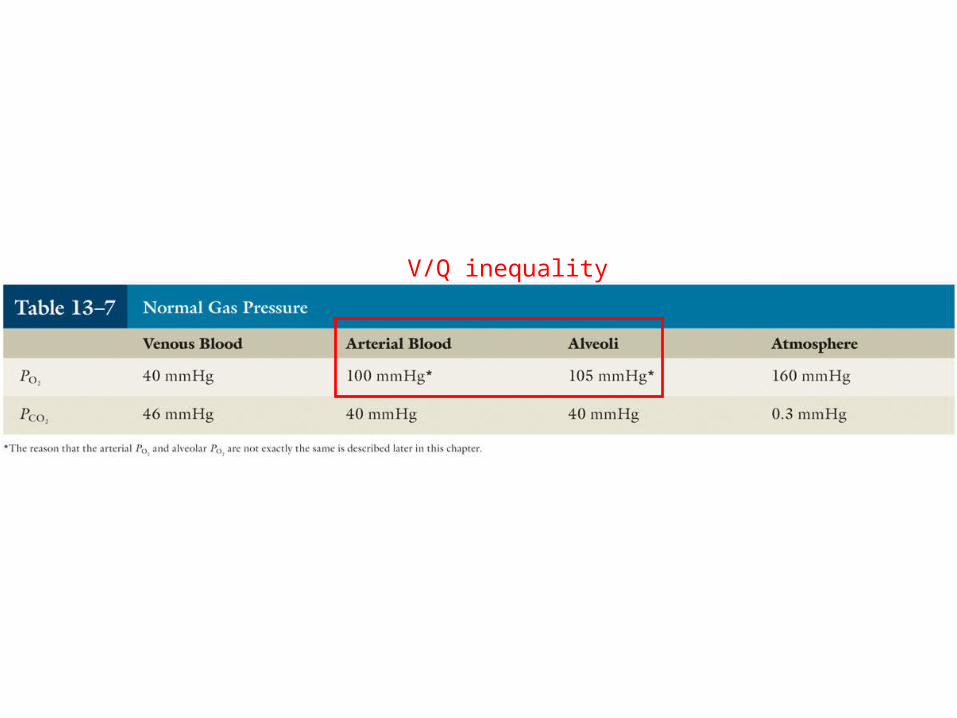
1. What is the partial pressure of oxygen in atmospheric air at sea level? What about in the alveolus? What are these values not identical?
2. Which has the highest partial pressure of oxgyen and why: pulmonary arterial blood, pulmonary venous blood, system arterial blood?
3. How are bronchioles and arterioles similar?
1QQ 28 for 9:30
1. Inspiration is an “active” event whereas a normal expiration is a “passive” event. What does this mean in terms of muscle activity, and what is responsible for expiration if muscles aren’t contracting?
2. How would you calculate the partial pressure of oxygen in the atmosphere at the summit of Mt. Everest?
3. How are arterioles and bronchioles similar?
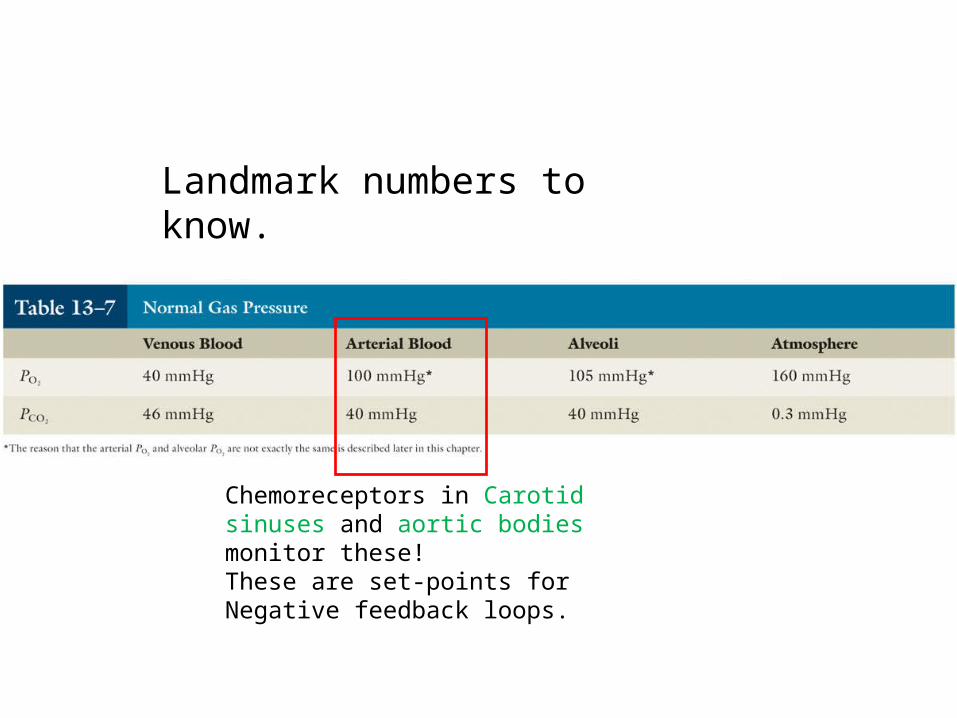
Landmark numbers to know.
Chemoreceptors in Carotid sinuses and aortic bodies monitor these!These are set-points for Negative feedback loops.
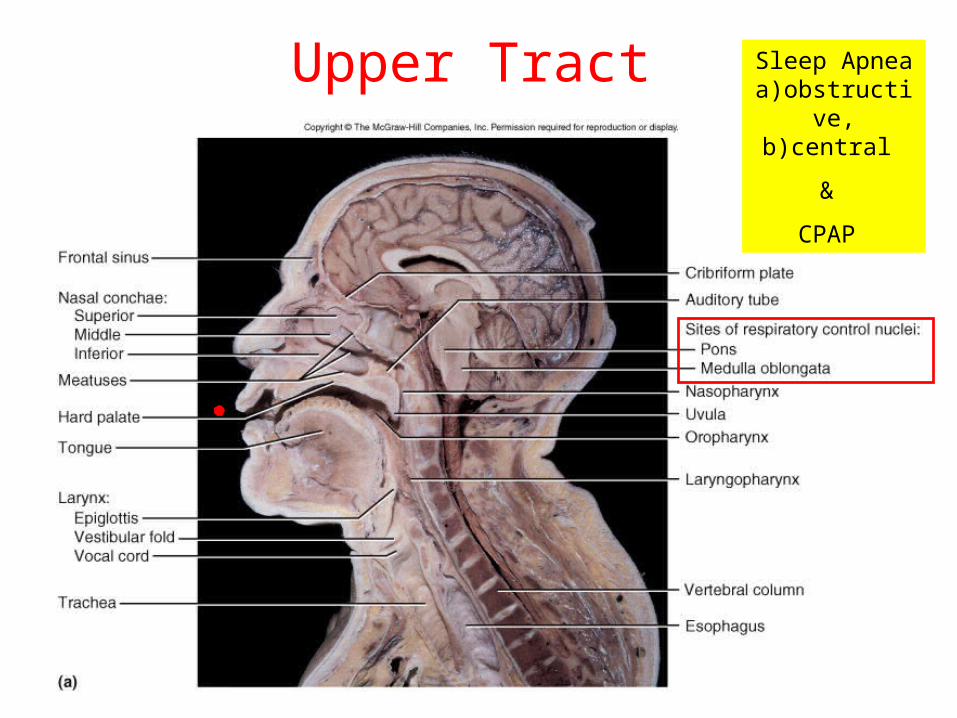
Upper Tract Sleep Apneaa)obstructive,
b)central
&
CPAP
Continuous Positive Airway Pressure
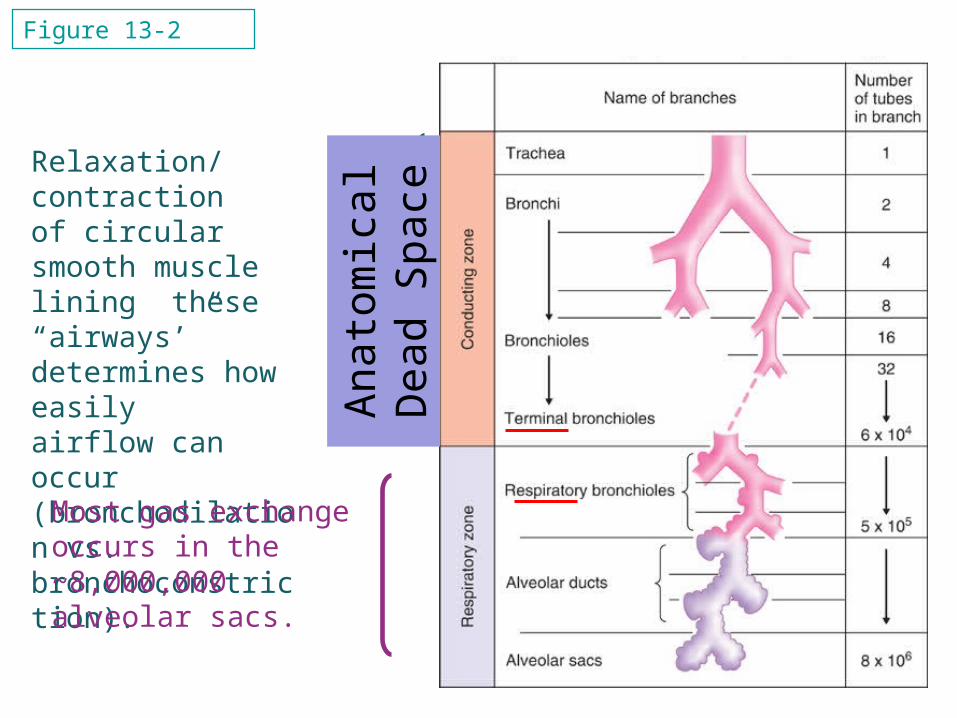
Relaxation/contractionof circular smooth musclelining these “airways’” determines how easily airflow can occur(bronchodilation vs.bronchoconstriction).
Most gas exchange occurs in the~8,000,000 alveolar sacs.
Figure 13-2
Anat
omic
alD
ead
Spac
e

Bronchopulmonary segments and Surgical resection
Bronchopulmonary segments and Surgical resection
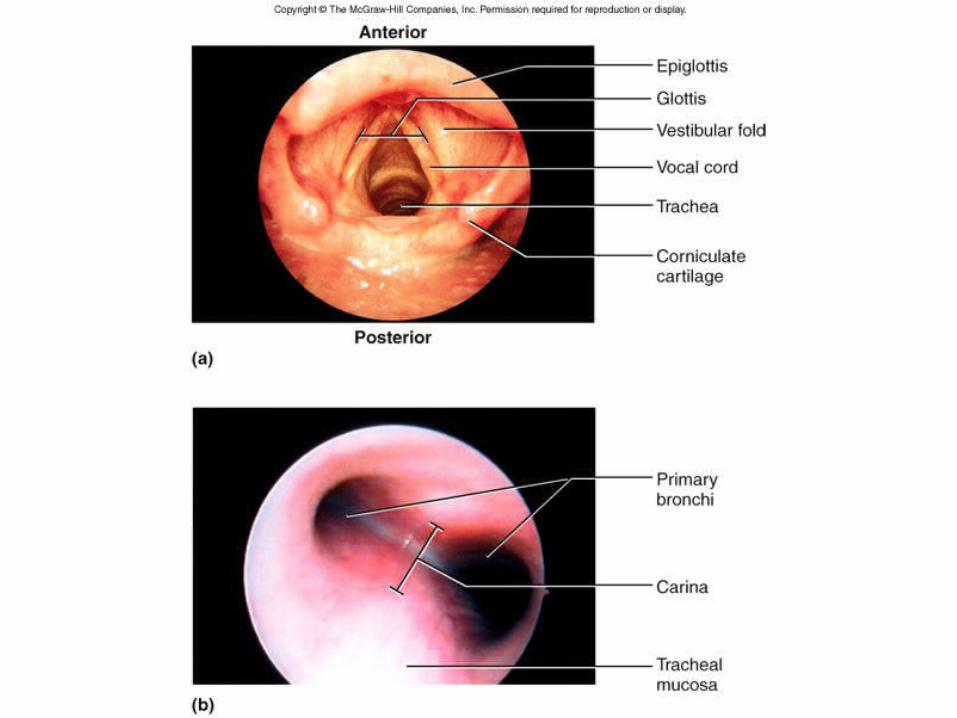
Figure 22.5
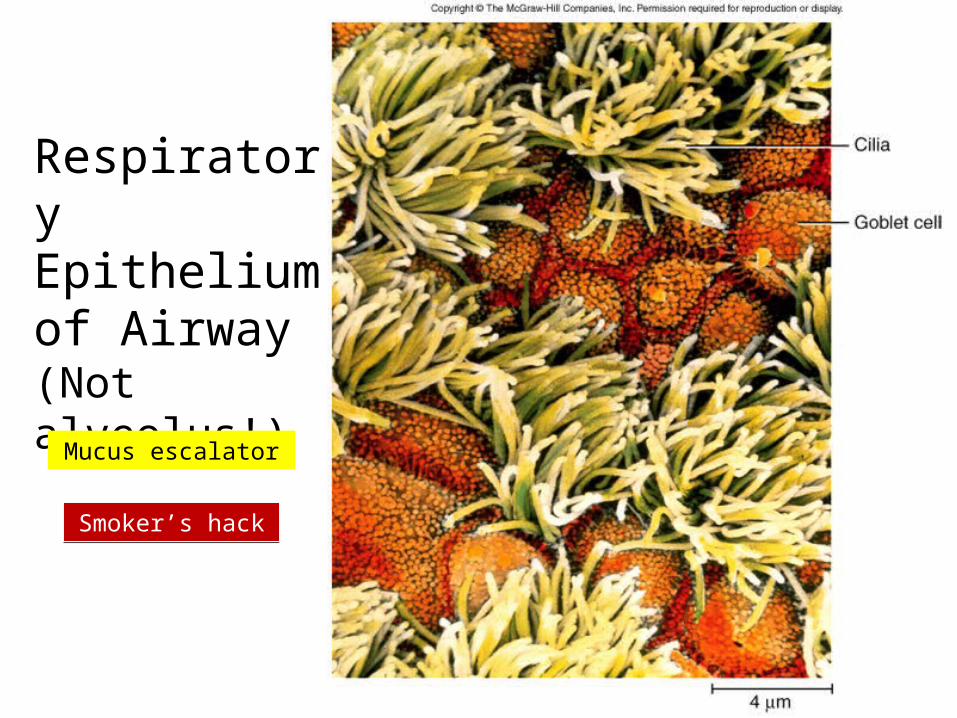
RespiratoryEpitheliumof Airway(Not alveolus!)
Mucus escalator
Smoker’s hackSmoker’s hack
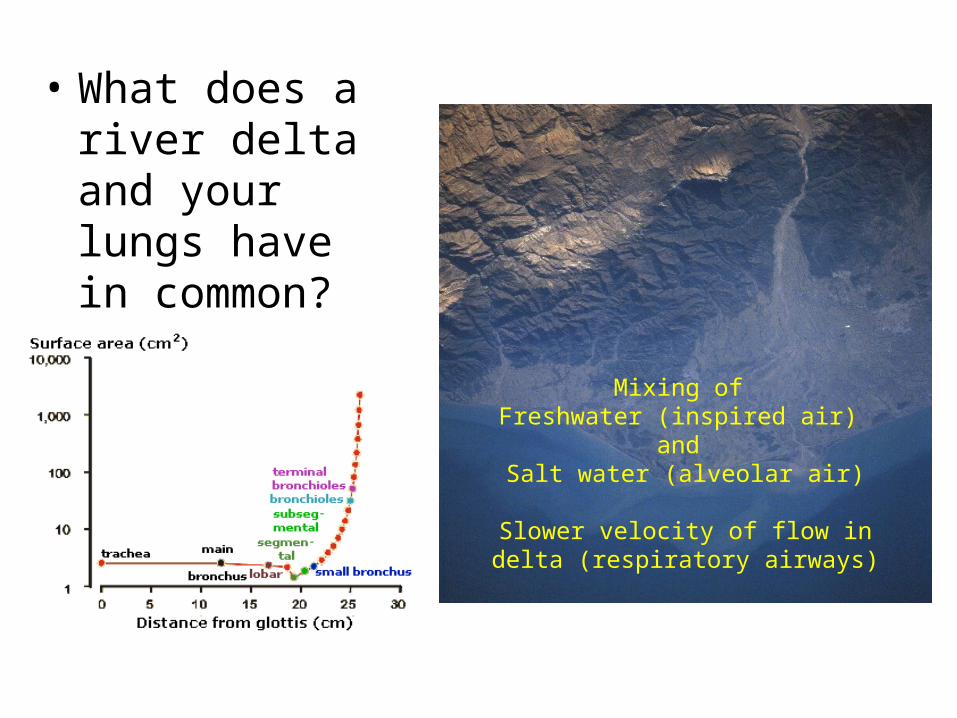
• What does a river delta and your lungs have in common?
Mixing of Freshwater (inspired air)
and Salt water (alveolar air)
Slower velocity of flow in delta (respiratory airways)
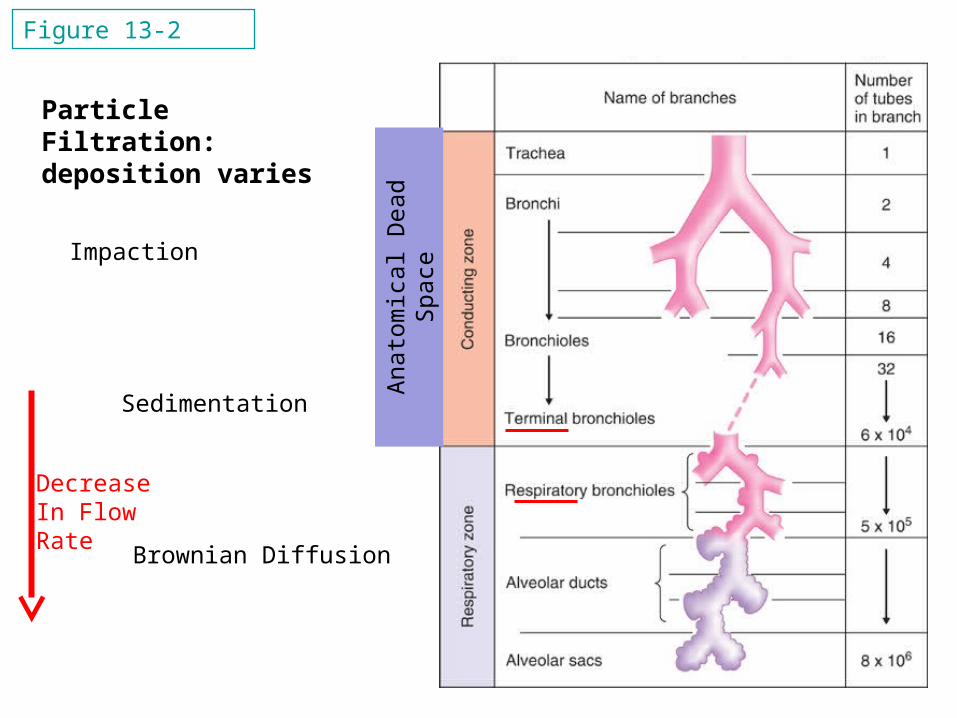
Figure 13-2
Anat
omic
al D
ead
Spac
e
Impaction
Sedimentation
Brownian Diffusion
Particle Filtration: deposition varies
DecreaseIn FlowRate
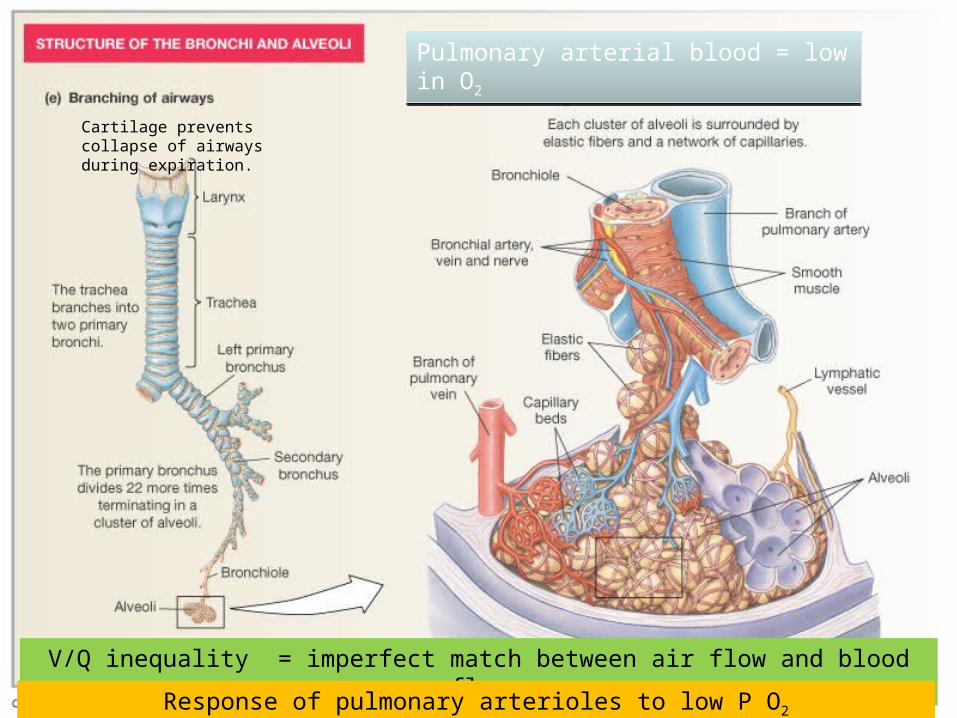
Pulmonary arterial blood = low in O2Pulmonary arterial blood = low in O2
Cartilage prevents collapse of airways during expiration.
V/Q inequality = imperfect match between air flow and blood flow
Response of pulmonary arterioles to low P O2
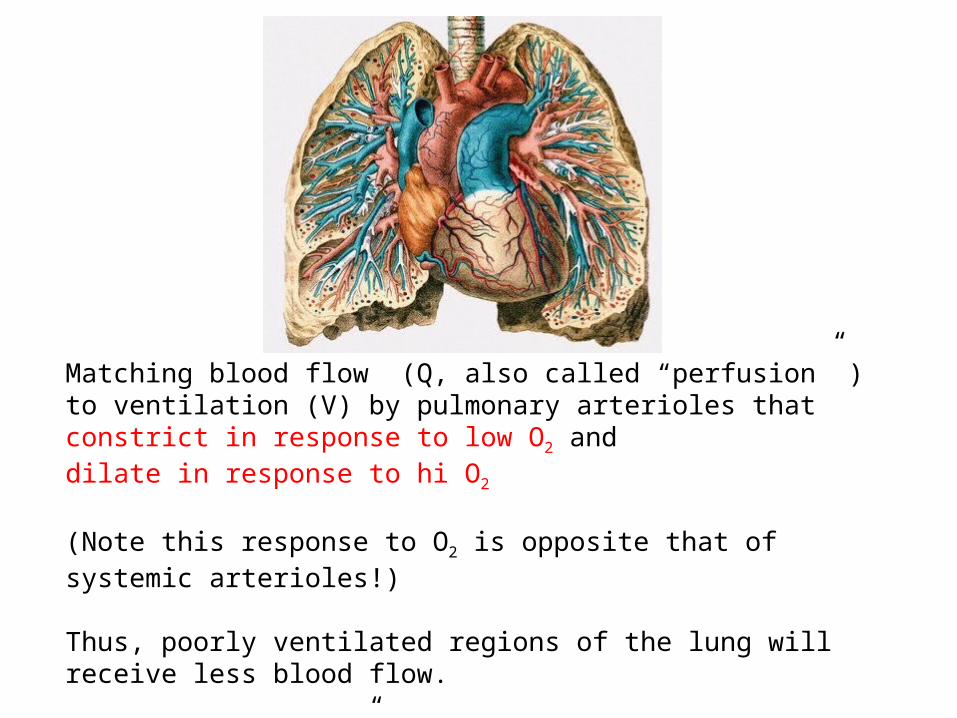
Matching blood flow (Q, also called “perfusion” ) to ventilation (V) by pulmonary arterioles that constrict in response to low O2 anddilate in response to hi O2
(Note this response to O2 is opposite that of systemic arterioles!)
Thus, poorly ventilated regions of the lung will receive less blood flow.
So…. Q is “matched” to V, but not perfectly.
And low perfusion in a region leads to bronchoconstriction.
V/Q inequality
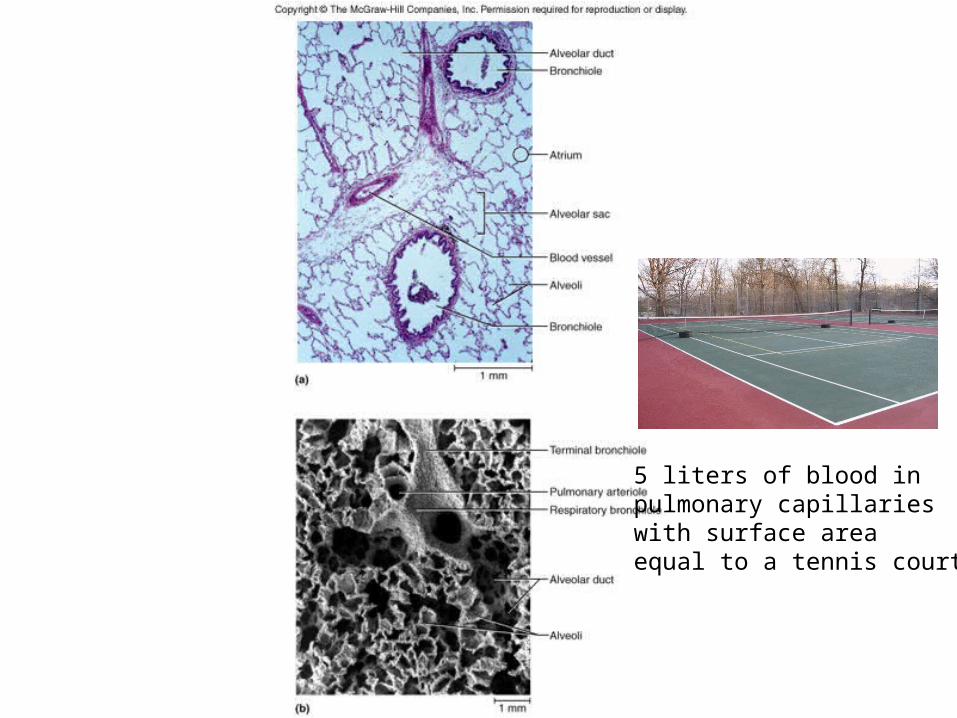
Figure 22.10
5 liters of blood inpulmonary capillarieswith surface areaequal to a tennis court
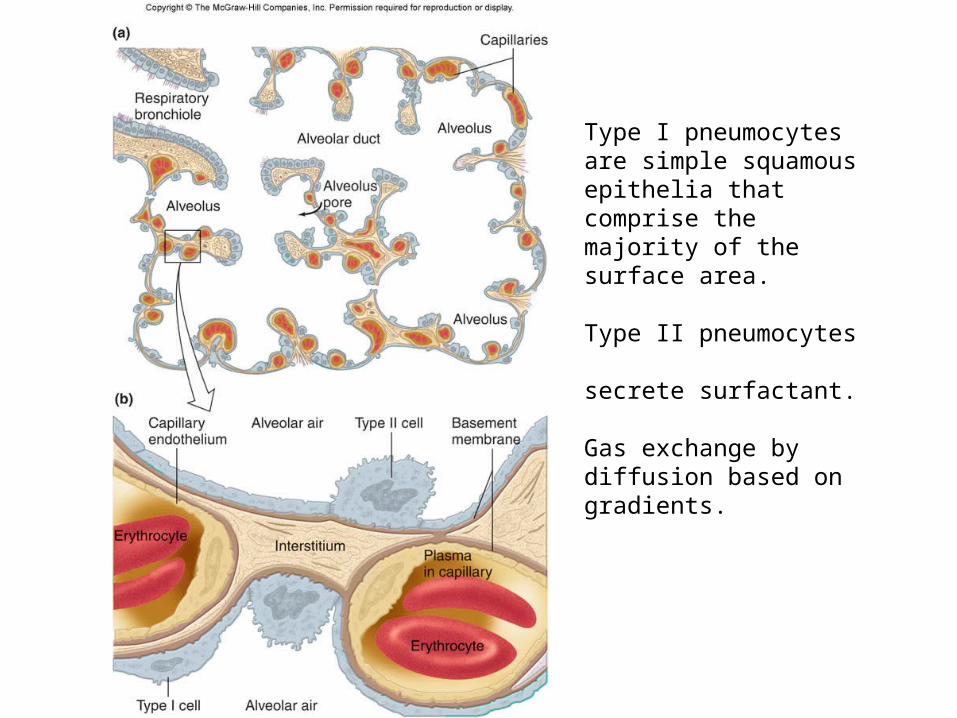
Type I pneumocytes are simple squamous epithelia that comprise the majority of the surface area.
Type II pneumocytes secrete surfactant.
Gas exchange by diffusion based on gradients.
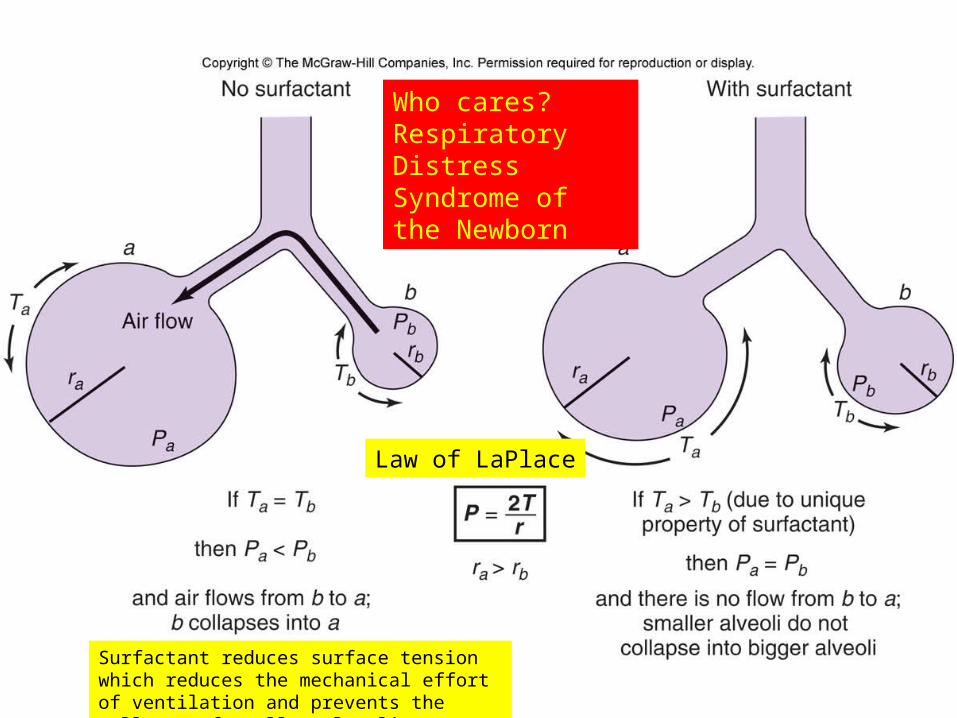
Figure 13.17Who cares? Respiratory Distress Syndrome of the Newborn
Law of LaPlace
Surfactant reduces surface tension which reduces the mechanical effort of ventilation and prevents the collapse of smaller alveoli.



![Flashcards Clothes colours - ESL kids Lab Microsoft PowerPoint - Flashcards Clothes colours [Compatibility Mode] Author Kissy Created Date 2/23/2009 6:57:48 PM](https://img.pdfslide.net/doc/110x75/5ad037ac7f8b9aca598d6637/flashcards-clothes-colours-esl-kids-microsoft-powerpoint-flashcards-clothes.jpg)









![Corpuls3 Software 2 - Rotes Kreuz … Neuer Softkey [Einst.] in der Vorschau des R-EKGs Über den Softkey [Einst.] in der Vorschau des R-EKGs ist es nun möglich, direkt in den Konfigurationsdialog](https://img.pdfslide.net/doc/110x75/5b8696557f8b9a162d8d42f1/corpuls3-software-2-rotes-kreuz-neuer-softkey-einst-in-der-vorschau-des-r-ekgs.jpg)