Embed Size (px)
Citation preview

Folate,&Grains
HealthFolate, grains and health have
been making headlines in the
past decade. Not only does folic
acid play a signifi cant role in
the prevention of birth defects, but
fortifying grains with folic
acid has shown preliminary
benefi ts for reducing risk of
cancer, stroke and heart disease
and improving cognitive function.
I N T R O D U C T I O N

2 Wheat Foods Council
TABLE OF CONTENTSIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cover
Folate Basics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Defi ning Folic Acid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Functions of Folate. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Sources of Folate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Adequate Folate Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Folic Acid Needs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Bioavailability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Defi ciency. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Current Intake Levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4-5
Toxicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Folate and Grains . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Grains and Needs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Fortifying Grains with Folic Acid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Grains & Folate on Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Impact of Grains and Folate on Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Folate and NTDs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Impact of Folic Acid Fortifi cation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6-7
Heart Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Emerging Health Connections. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8-9
Nervous System. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Kidney . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10-11
About the Author . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Back Cover

3Wheat Foods Council
Defi ning Folic AcidThe need for folic acid, one of the B vitamins, was discovered in the 1930s when anemia during pregnancy was cured with a yeast extract. Further research in the 1940s isolated the cure for anemia from spinach, and it was named folate after the Latin word folium, meaning leaf.1
The words folate, folacin and folic acid often are used interchangeably, but there are differences in the forms. Folate is the collective term, but also describes the nutrient found naturally in foods. Folate and folacin are generic descriptions for compounds with nutritional properties and chemical structures similar to those found in folic acid, the synthetic form, often used in fortifi ed foods and in vitamin supplements.1
Functions of FolateFolate functions in the production of new DNA (genetic material) and
also in the metabolism of nucleic acids for genetic coding, and amino acids for protein building. Necessary for red blood cell production in bone marrow, folate also is key for cell division when DNA replicates. Folate is vital to body tissues in the intestine, skin, bone marrow, and to the fetus, where cells undergo rapid division. Folate also prevents accumulation of metabolites, such as homocysteine, which may be linked to greater risk of cardiovascular disease and stroke.
Sources of FolateSources of folate include leafy green vegetables (spinach, broccoli, asparagus), legumes (lentils, black beans), yeast, liver and enriched grain foods such as ready-to-eat cereals, breads, and pasta, in addition to certain nuts.2 About half of naturally occurring folate is absorbed, compared to 80 percent of fortifi ed folic acid and all of supplemented folic acid.1 Although many foods provide folate, it is diffi cult for most people to consume enough from these foods, often making supplementation necessary.1 (See Table 1.)
FOLATE BASICS
*Based on USDA National Nutrient Database2, **DFE = Dietary Folate Equivalents1
Table 1. Selected food sources of folate and folic acid
FOOD AMOUNT FOLATE (mcg)* % Daily Value (DV)
GrainsCheerios® 1 cup 330 80Wheat germ ¼ cup 80 20Oatmeal, instant, cooked ½ cup 80 20Pasta, plain, cooked 2 ounce 60 15Bread, white, enriched 1 slice 40 10Crackers, saltines 4 20 6Bread, whole wheat 1 slice 15 4Vegetables & FruitsAsparagus, cooked ½ cup 130 30Spinach, cooked ½ cup 130 30Broccoli, cooked ½ cup 90 25Avocado ½ medium 80 20Beets, cooked ½ cup 65 15Orange juice 6 ounces 35 10Legumes & NutsLentils ½ cup 180 45Black beans ½ cup 130 30Kidney beans, red ½ cup 115 30Garbanzo beans ½ cup 80 20Soy nuts, roasted 1 ounce 60 15Peanuts, dry roasted 1 ounce 40 10MeatBeef liver, cooked 3 ounces 185 45
DFE** (Based On 400 mcg)

4 Wheat Foods Council
Folic Acid Needs The current recommendation for folate is 400 micrograms (mcgs) per day of dietary folate equivalents (DFEs) for adult men and women (19+ years) and teens (14 to 18 years).1 (See Figure 1.) Children require less, and pregnant (600 mcgs/day) and lactating women require more folate (500 mcgs/day).1 Folate can come from fortifi ed foods and supplements, in addition to that coming from natural food sources in a varied diet. (See Table 2.)
ADEQUATE FOLATE STATUS
Bioavailability When folate or folic acid is consumed, enzymes in the small intestine convert it to a smaller form for absorption in the colon and for transport to target tissues by the bloodstream. Within the blood, folate is present in an inactive form 5-methyltetrahydrofolate (5-methyl THFA). Vitamin B
12 (cobalamin) is needed to transform
inactive 5-methyl THFA to active tetrahydrofolic acid. Without B12,
folate is not accessible to the body and defi ciency occurs.3
Symptoms of folate defi ciency are megaloblastic anemia, with large immature red blood cells and damaged DNA components. A defi ciency in either folate or vitamin B
12 leads to an identical
megaloblastic anemia—such that one defi ciency easily masks the other—making it diffi cult to determine the cause of the anemia and the treatment to correct it.3 (See Figure 2.)
Defi ciencyA defi ciency of folate can occur when the folate consumed is not accessible to the body, as described above. Also, defi ciency can arise when the need for folate by the body is increased (as in pregnancy or lactation), when dietary intake of folate is inadequate, and when the body excretes more folate than usual. Malabsorption syndromes,
Age Males & Females Pregnancy Lactation (Years) (mcg folate/day) (mcg folate/day) (mcg folate/day)
1-3 150 – – 4-8 200 – – 9-13 300 – – 14-18 400 600 500 19+ 400 600 500
Table 2: Folate needs for adults and children¹
What are Dietary Folate Equivalents (DFEs)?DFE is a new measure developed to help account for thedifference in the absorption of food folate and syntheticfolic acid from dietary supplements or food fortifi ed withfolic acid¹
1 DFE = 1 mcg folate naturally occurring in food1 DFE = 0.6 mcg folic acid from fortifi ed food or supplements
Figure 1. Dietary Folate Equivalents (DFEs)
alcoholism, and drug abuse can cause defi ciency as can certain drug treatments or the use of non-steroidal anti-infl ammatory medications and aspirin.1
Signs of folic acid defi ciency often are subtle and include diarrhea, loss of appetite, pale skin, nausea, and weight loss with poor absorption of other nutrients, as well as anemia in adults and slow growth rate in children.
Women with inadequate folic acid intake are more likely to give birth to low birth weight (less than 5 ½ pounds) and premature infants4 as well as to infants with neural tube defects (NTDs) which may involve the brain, spinal cord, meninges (membranes) and skull. Defi ciency of this vitamin also has been linked to cardiovascular disease,5,6 stroke,5,7 osteoporosis,8 cancer,9 dementia and cognitive defi cit.10
Figure 2. Megaloblastic anemia involves largeimmature red blood cells, large mature red blood cells and damaged DNA.
Current Intake Levels
Folate intake levels within the American population vary widely and may or may not meet recommended levels.11 About 50-100 mcg folate per day must be absorbed to replenish daily amounts of folate that are metabolized and excreted. If not enough folate is consumed, signs of defi ciency may appear in four to fi ve months.3

5Wheat Foods Council
A recent study evaluating folate intake among college-educated women (mean age 32 years) showed that 36 percent of those who were pregnant and 32 percent of those lactating were not able to meet daily folate requirements (600 mcgs and 500 mcgs, respectively) from diet alone—even when consuming folate-fortifi ed foods.12 In another study, adult women consuming foods fortifi ed with folic acid or supplements had actual folate intakes that well-exceeded recommended intake levels per day.11
ToxicityAll enriched fl our and grain foods in the U.S. are required by law to be fortifi ed with folic acid. Though benefi ting some of the population, there is risk of exposing others to folate intakes that are higher than recommended. Scientifi c evidence shows that consuming high levels of folate can mask vitamin B
12
defi ciency, leading to neurological damage. Other fi ndings suggest that high folate intake may create less stability among people with epilepsy being treated with anti-convulsive medications. The Tolerable Upper Intake Level (UL) of folic acid is 1,000 mcg per day for adults, 800 mcg for teens, 14 to 18 years, and even less for children.1 Yet some experts believe the current intake of folic acid (with food fortifi cation) is safe enough to recommend even higher levels of fortifi cation as benefi cial. Clearly, further study of these recommendations is warranted.
FOLATE AND GRAINSGrains and NeedsThe 2005 Dietary Guidelines for Americans and MyPyramid.gov, the food guidance system, recommend eating plenty of grains, fruits and vegetables in addition to low-fat dairy foods—foods that often fall short on American tables.13,14 Grains provide an important energy source—carbohydrate—that makes up the foundation of a healthy diet. Also, grains supply a variety of nutrients such as fi ber, B vitamins (such as thiamin, ribofl avin, niacin and folic acid), in addition to magnesium, and iron that are important for good health.
Assuming an average calorie intake of 2,000 calories per day, about six 1-ounce serving equivalents of grains are recommended daily, with at least half (three) of the servings being whole grain—containing the germ, endosperm and bran layers of the grain.13,14 A half serving of whole grain contains 8 grams; 16 grams of whole grain makes a full serving.15 (See Figure 3.)
Ways To Eat More Whole Grains ❖ Choose whole grain hot or cold breakfast cereal
❖ Check labels for “whole” ingredients: “whole grain oats”, “whole wheat”
❖ Experiment with whole grain barley in soups, stews or side dishes
❖ Eat brown rice instead of white
❖ Try bulgar, kasha, or couscous as a new world side dish
❖ Dine on whole wheat or buckwheat pasta for a change
❖ Use whole wheat pita bread and whole wheat pretzels as dippers
❖ Seek out low-fat popcorn and graham crackers for snacks
❖ Blend unique grains like quinoa or amaranth into pilafs or sides
Fortifying Grains with Folic AcidThe evidence in support of the vital role of folic acid in preventing neural tube defects (NTDs) lead the U.S. Food and Drug Administration to create a mandatory folic acid fortifi cation program in January 1998. This program specifi es that all white breads and other enriched grain products, such as fl our, rice, pasta, cornmeal, farina, breakfast cereal, and noodles be fortifi ed with 140 mcg folic acid per 100 grams (3.5 ounces) of food.16 Enriched grain products were selected to deliver folic acid for several reasons:
❖ Thiamin, ribofl avin, niacin, and iron were already being added to enrichgrain products of nutrients lost during processing.
❖ Grain foods are widely consumed and likely to have a great impact.
The goal of the fortifi cation effort was to increase consumption of folate by women of childbearing age to reduce risk of pregnancies affected by NTDs. The fortifi cation level was chosen to balance the benefi ts of increased folic acid to prevent birth defects, with any potential adverse effects such as masking vitamin B
12 defi ciency in the elderly.16 In addition to
fortifi cation, an extra 300 mcg folic acid daily is needed—either through intake of fortifi ed foods or from a dietary supplement—to meet current folate recommendations for women of childbearing age.
Whole grain foods and organic foods are not, by defi nition or law, required to be enriched and therefore, are not fortifi ed with folic acid under the 1998 folic-acid fortifi cation program.16 Some argue that because these foods make up an increasing part of grain intake, perhaps they ought to be fortifi ed as well. Though optional, some food manufacturers choose to fortify whole grains with folic acid and other nutrients as indicated on nutrition labels and ingredient lists.
Figure 3. Ways to eat more whole grains
6 Wheat Foods Council
GRAINS & FOLATE ON HEALTHImpact of Grains and Folate on HealthFolate, grains and the healthful benefi ts they provide have been in the forefront of nutrition and health news in the past decade. The 1998 folic acid grain fortifi cation plan was implemented to reduce the incidence of NTDs among newborns in the U.S. A number of studies demonstrated a signifi cant 20-30 percent decline in risk of heart disease when three or more servings of whole grain foods were consumed daily.17,18 Other studies have asserted that diets high in whole grains,17,18 fruits, vegetables and legumes may offer protection against coronary heart disease, vascular disease and stroke,5-7,17-19 as well as cancer.20,21
Epidemiological studies have suggested that a defi ciency of folate may be linked to an increased risk for certain types of cancer including colorectal, pancreatic, cervical, and breast cancers.9,20 Emerging data have purported links between folate intake and bone health,22 kidney health23 and cognition.24 Indeed,diets rich in folate and containing adequate whole grain appear to offer some health benefi ts.
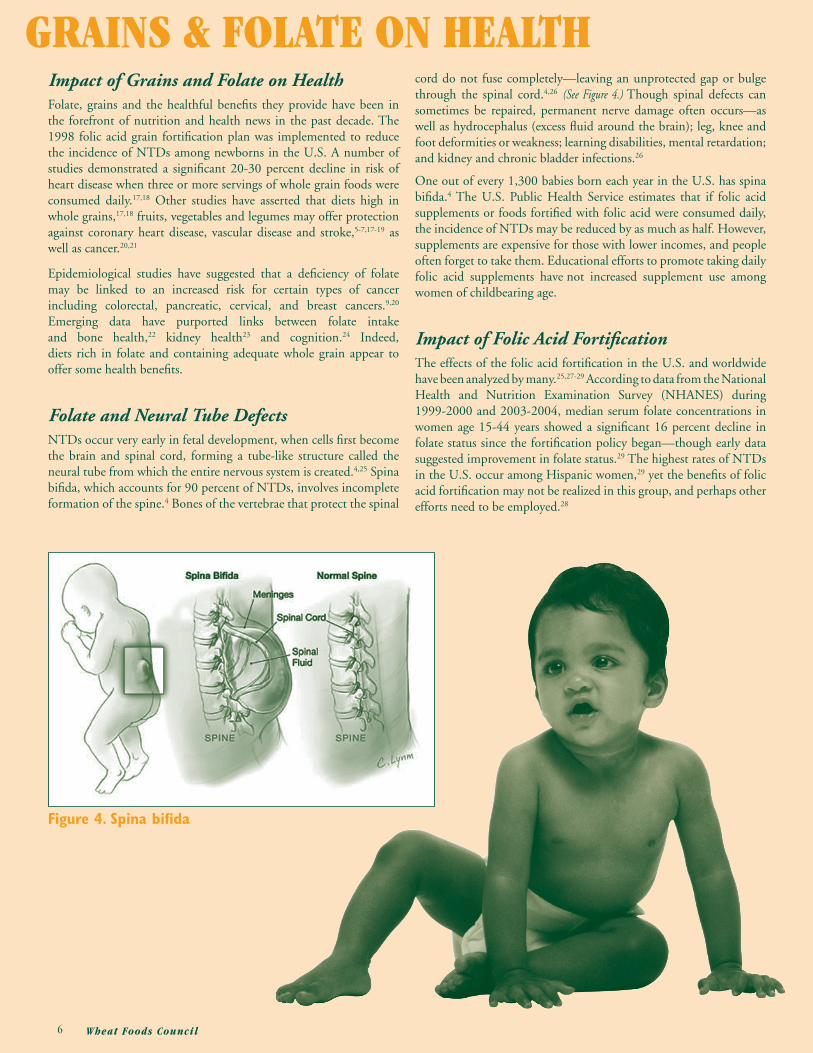
Folate and Neural Tube Defects NTDs occur very early in fetal development, when cells fi rst become the brain and spinal cord, forming a tube-like structure called the neural tube from which the entire nervous system is created.4,25 Spina bifi da, which accounts for 90 percent of NTDs, involves incomplete formation of the spine.4 Bones of the vertebrae that protect the spinal
cord do not fuse completely—leaving an unprotected gap or bulge through the spinal cord.4,26 (See Figure 4.) Though spinal defects can sometimes be repaired, permanent nerve damage often occurs—as well as hydrocephalus (excess fl uid around the brain); leg, knee and foot deformities or weakness; learning disabilities, mental retardation; and kidney and chronic bladder infections.26
One out of every 1,300 babies born each year in the U.S. has spina bifi da.4 The U.S. Public Health Service estimates that if folic acid supplements or foods fortifi ed with folic acid were consumed daily, the incidence of NTDs may be reduced by as much as half. However, supplements are expensive for those with lower incomes, and people often forget to take them. Educational efforts to promote taking daily folic acid supplements have not increased supplement use among women of childbearing age.
Impact of Folic Acid Fortifi cationThe effects of the folic acid fortifi cation in the U.S. and worldwide have been analyzed by many.25,27-29 According to data from the National Health and Nutrition Examination Survey (NHANES) during 1999-2000 and 2003-2004, median serum folate concentrations in women age 15-44 years showed a signifi cant 16 percent decline in folate status since the fortifi cation policy began—though early data suggested improvement in folate status.29 The highest rates of NTDs in the U.S. occur among Hispanic women,29 yet the benefi ts of folic acid fortifi cation may not be realized in this group, and perhaps other efforts need to be employed.28
Figure 4. Spina bifi da

7Wheat Foods Council
Better results are apparent elsewhere. In Canada, a 39 percent increase in serum folate concentrations with minimal changes in vitamin B
12
status were noted in women before and after folate fortifi cation.30 In Chile, folic acid fortifi cation of wheat fl our has lead to a signifi cant 74 percent increase in mean serum folate concentrations among healthy women of reproductive age.31 To date, more than 40 countries now fortify grain foods with folic acid.
Despite an initial rise soon after folic acid grain fortifi cation, serum folate levels have actually declined in the U.S. since 1999-2000.29 Perhaps this decline in folate status is due, in part, to the popularity of low-carbohydrate diets and increased consumption of whole grain products that may contain less folic acid than enriched ones. Metabolic changes evident in an ever-increasing obese population may contribute as well. However, the reasons for this folate status decline are yet to be determined.
NTD incidence, the main thrust behind fortifi cation, however, has dropped by an estimated 26 percent in the U.S., and perhaps to an even greater degree in Canada.25,29 Yet reports fail to demonstrate a substantial decline in hospitalizations of newborns with folate-sensitive birth defects beyond those anticipated from a reduction in NTDs.27 Cost-benefi t evaluations suggest that folic acid fortifi cation in the U.S. is associated with annual economic benefi ts in the range of $312 to $425 million dollars—well-exceeding the projected $88 to $145 million in savings.32
Heart Health Much epidemiological data have connected low dietary intake of folate and elevated blood levels of homocysteine (a metabolite of amino acids)33,34 with increased risk of coronary heart disease, heart attack and stroke.35,36 Consuming higher levels either by eating more food folate sources, including enriched grains, or by folic acid supplementation, therefore, would reduce homocysteine levels33,34,37, potentially reducing risk of heart disease and stroke.7 For that reason, researchers recommend folic acid fortifi cation in countries where it is not yet implemented.38
Recent clinical research results, however, have weakened the evidence linking folate intake (and blood folate levels) to heart health.37,39,40 One study of patients with vascular disease or diabetes showed 20 percent declines in homocysteine with greater folate intake, but no reduced risk of death from cardiovascular causes.39 Another study of patients with heart attacks showed that though homocysteine levels were reduced by 27 percent, there was no effect on endpoints (either a second heart attack, stroke, or death) attributed to heart disease.40 These studies demonstrate that folate can reduce homocysteine levels in the blood, but does not appear to reduce cardiovascular disease risk. Researchers suggest that homocysteine may be a marker, but perhaps not a cause, of heart disease.39,40
When making overall dietary recommendations to reduce heart disease risk, many studies5-7,19 suggest that diets high in whole grains,17,18 fruits, vegetables and legumes may be somewhat protective against coronary heart disease and stroke (reducing risk by up to 20 to 30 percent).17 The exact mechanism is not clear but studies correlate a reduced level of homocysteine with higher consumption of whole grains.17,18 Researchers speculate that perhaps other components of whole grains, such as vitamin B
6, folate, magnesium, fi ber and
vitamin E may play important, yet unknown, roles.36

8 Wheat Foods Council
Cancer Epidemiological studies have suggested that folate defi ciency is linked to an increased risk for certain types of cancer.9,21,38,41-44 In an analysis of cancer and folate status associations in 20 different studies, Kim showed that high folate intake could reduce risk of colon cancer by as much as 40 percent when compared with low folate intake.9 Furthermore, researchers reported a 75 percent reduction in colon cancer risk for women with at least 15 years of high folic acid intake (400 mcg/day or more).42 This is particularly signifi cant because colon cancer is the second-most prevalent cancer in the U.S., with approximately 139,500 new cases reported each year.45 Newer epidemiological data suggest that increased consumption of plant foods such as whole grains, vegetables and fruits (sources of folate) and reduced intake of red meats correlate with decreased risk of colorectal cancer.21 A continuous and long history of adequate folate intake from food sources and supplementation may provide the best protection against colorectal cancers.
Adequate folic acid and folate intake has been shown to be effective in protecting against pancreatic cancer in men who smoke41 and against breast cancer in women who drink even moderate amounts of alcohol9. Other researchers have found a clear correlation between folic acid intake and the reduction of breast cancer risk.43 A recent
study of women with breast cancer (and age-matched controls), showed that greater consumption of whole grains, and vegetables had a reduced association with breast cancer.20 Researchers noted that greater intakes of folate were inversely associated with breast cancer as well.20,46
Fortifi cation improves folate intake but still may not be enough to achieve recommended levels as noted in a group of female smokers of reproductive age with cervical dysplasia—at high risk for developing cervical cancer.44 The mechanism behind the protective effect of folic acid against cancer has not yet been ascertained. Meanwhile, those who already have cancer should be cautioned not to increase folate intake based on evidence that supplementation may enhance existing tumor development.41
Emerging Health Connections
BoneFinding ways to reduce bone fractures related to osteoporosis and improve bone health become of even greater importance with an aging population. Elevated levels of homocysteine have been associated with reduced bone mineral density,22,35 increased risk for

9Wheat Foods Council
hip fracture47 and increased risk of osteoporosis in populations of women.8 Newer research suggests there may be a connection between homocysteine levels, folate, vitamin B
6 and vitamin B
12 status 48 and
bone metabolism but the mechanism for this association needs to be established.22
Nervous System Because folic acid is critical for proper functioning of the nervous system, it can affect cognition particularly in older individuals.10 In otherwise healthy subjects, low folate levels and high homocysteine levels are linked to patterns of cognitive impairment also found in aging.10,24,49 Folate defi ciency is associated with depression10,24,35 and dementia10 in geriatric patients and contributes to aging brain processes and increased risk of cognitive defi cit.35,49 Overall, supplementation with folic acid has been shown to improve the mental health of patients.10,24,35
KidneyAdequate folic acid intake may help reduce incidence of cardiovascular disease in renal patients.50 Some studies show that elevated levels of homocysteine are not associated with worsening renal function or a higher prevalence of cardiovascular disease.51 Renal insuffi ciency and reduced levels of vitamin B
12 with adequate folate may contribute
to increased risk of elevated homocysteine levels 50 among patients with end-stage renal disease. Clearly, improving folate status may be benefi cial in reducing high levels of homocysteine in patient populations with kidney disease.23
OtherEmerging research nods to a decreased risk of prostate cancer in men consuming diets high in folate but data is still inconclusive.52 A possible role for folate in eye health is preliminary but data may suggest a connection.
Summary
Grain foods fortifi ed with folic acid plus foods naturally containing the vitamin should be consumed on a daily basis. Research suggests that many people could also benefi t from taking a folic acid supplement to ensure adequate intake. Diets abundant in fortifi ed grains, folic acid and folate may provide numerous health benefi ts affecting the U.S. population and those of other nations as well.

10 Wheat Foods Council
REFERENCES1. Institute of Medicine. Food and Nutrition Board. Dietary Reference
Intakes: thiamin, ribofl avin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, choline. National Academy Press. Washington, DC, 1998.
2. United States Department of Agriculture. National Nutrient Database. 2007. http://www.nal.usda.gov/fnic/foodcomp/search/ accessed on 1/24/07.
3. Gentili A. Folic Acid Defi ciency. 2006. http://www.emedicine. com/med/topic802.htm accessed on 1/16/07.
4. March of Dimes. Quick reference and fact sheet: folic acid. 2007. http://www.marchofdimes.com/printableArticles/14332_1151.asp accessed 1/12/07.
5. Flight I, Clifton P. Cereal grains and legumes in the prevention of coronary heart disease and stroke: a review of the literature. Eur J Clin Nutr. 2006;60:1145-1159.
6. Hu FB, Willett WC. Optimal diets for prevention of coronary heart disease. JAMA. 2002;288:2569-2578.
7. Yang Q, Botto LD, Erickson JD, Berry RJ, Sambell C, Johansen H, Friedman JM. Improvement in stroke mortality in Canada and the United States, 1990 to 2002. Circulation. 2006;113:1335-1343.
8. Cagnacci A, Baldassari F, Rivolta G, Arangino S, Volpe A. Relation of homocysteine, folate, and vitamin B12 to bone mineral density of postmenopausal women. Bone. 2003; 33:956-959.
9. Kim Y-I. Folate and cancer prevention: a new medical application of folate beyond hyperhomocysteinemia and neural tube defects. Nutr Rev. 1999;57:314-321.
10. Reynolds EH. Folic acid, aging, depression and dementia. Br Med J. 2002;324:1512-1515.
11. Firth Y, Murtaugh MA, Tangney CC. Estimation of individual intakes of folate in women of childbearing age with and without simulation of folic acid fortifi cation. J Am Diet Assoc. 1998;98:985-988.
12. Sherwood KL, Houghton LA, Tarasuk V, O’Connor DL. One-third of pregnant and lactating women may not be meeting their folate requirements from diet alone based on mandated levels of folic acid fortifi cation. J Nutr. 2006;136:2820-2826.
13. United States Department of Agriculture. Nutrition and Your Health: Dietary Guidelines for Americans, 2005. http://www. health.gov/dietaryguidelines/dga2005/document/html/chapter5.htm accessed on 1/15/07.
14. United States Department of Agriculture. MyPyramid.gov. http:// www.mypyramid.gov/ accessed on 1/16/07.
15. Whole Grains Council. Identifying legitimate whole grain products. http://www.wholegrainscouncil.org/WholeGrainStamp.html accessed on 1/22/07.
16. US Food and Drug Administration. Fed Register. 1996;61:8761- 8797.
17. Liu S, Stampfer MJ, Hu FB, Giovannucci E, Rimm E, Manson JE, Hennekens CH, Willett WC. Whole-grain consumption and risk of coronary heart disease: results from the Nurses’ Health Study. Am J Clin Nutr. 1999;70:412-419.
18. Lutsey PL, Steffen LM, Feldman HA, Hoelscher DH, Webber LS, Luepker RV, Lytle LA, Zive M, Osganian SK. Serum homocysteine is related to food intake in adolescents: The Child and Adolescent Trial for Cardiovascular Health. Am J Clin Nutr. 2006;83:1380- 1386.
19. Song WO, Chung C-E, Chun OK, Cho S, Serum homocysteine concentration of US adults associated with fortifi ed cereal consump- tion. J Am Coll Nutr. 2005;24:503-509.
20. Adzersen K-H, Jess P, Freivogel KW, Gerhard I, Bastert G. Raw and cooked vegetables, fruits, selected micronutrients, and breast cancer risk: a case-control study in Germany. Nutr Cancer. 2003;46:131-137.
21. Campos FG, Logullo Waitzberg AG, Kiss DR, Waitzberg DL, Habr-Gama A, Gama-Rodrigues J. Diet and colorectal cancer: current evidence for etiology and prevention. Nutr Hosp. 2005;20:18-25.
22. Herrmann M, Widmann T, Herrmann W. Homocysteine—a newly recognized risk factor for osteoporosis. Clin Chem Lab Med. 2005;43:1111-1117.
23. Menon V, Wang X, Greene T, Beck GJ, Kusek JW, Selhub J, Levey AS, Sarnak MJ. Homocysteine in chronic kidney disease: effect of low protein diet and repletion with B vitamins. Kidney Int. 2005;67:1539-1546.
24. Quadri P, Fragiacomo C, Pezzati R, Zanda E, Forloni G, Tetta manti M, Lucca U. Homocysteine, folate and vitamin B12 in mild cognitive impairment, Alzheimer disease and vascular dementia. Am J Clin Nutr. 2004;80:114-122.
25. Mills JL, Signore C. Neural tube defect rates before and after food fortifi cation with folic acid. Birth Defects Res A Clin Mol Teratol. 2004;70:844-845.
26. Centers for Disease Control and Prevention. Folic Acid Now. 2005. cdc-nceh99-0463. http://www.cdc. gov/ncbddd/folicacid accessed 1/16/07.
27. Robbins JM, Tilford JM, Bird TM, Cleves MA, Reading JA, Hobbs CA. Hospitalizations of newborns with folate-sensitive birth defects before and after fortifi cation of foods with folic acid. Pediatrics. 2006;118:906-915.
28. Rader JI, Schneeman BO. Prevalence of neural tube defects, folate status, and folate fortifi cation of enriched cereal-grain products in the United States. Pediatrics. 2006;117:1394-1399.

11Wheat Foods Council
29. Centers for Disease Control and Prevention. Morbidity and Mortal- ity Weekly Report. 2007;55:1377-1380.
30. Ray JG. Folic acid food fortifi cation in Canada. Nutr Rev. 2004; 62:S35-S39.
31. Hertrampf E, Cortes F, Erickson JD, Cayazzo M, Freire W, Bailey LB, Howson C, Kauwell GPA, Pfeiffer C. Consumption of folic acid-fortifi ed bread improves folate status in women of reproductive age in Chile. J Nutr. 2003;133:3166-3169.
32. Grosse SD, Waitzman NJ, Romano PS, Mulinare J. Reevaluating the benefi ts of folic acid fortifi cation in the United States: economic analysis, regulation, and public health. Am J Pub Health. 2005;95:1917-1922.
33. Ganji V, Kafai MR. Population reference values for plasma total homocysteine concentrations in US adults after the fortifi cation of cereals with folic acid. Am J Clin Nutr. 2006;84:989-994.
34. Malinow MR, Duell BP, Hess DL, Anderson PH, Kruger WD, Phillipson BE, Gluckman RA, Block PC, Upson BM. Reduction of plasma homcyst(e)ine levels by breakfast cereal fortifi ed with folic acid in patients with coronary heart disease. N Engl J Med. 1998;338:1009-1015.
35. Refsum H, Nurk E, Smith AD, Ueland PM, Gjesdal CG, Bjelland I, Tverdal A, Tell GS, Nygard O, Vollset SE. The Hordland Homo- cysteine Study: a community-based study of homocysteine, its deter- minants, and as sociations with disease. J Nutr. 2006;136:1731S- 1740S.
36. Kelly PJ, Shih VE, Kistler JP, Barron M, Lee H, Mandell R, Furie KL. Low vitamins B6 but not homocysteine is associated with increased risk of stroke and transient ischemic attack in the era of folic acid grain fortifi cation. Stroke. 2003;34:e51-54.
37. Brilakis ES, McConnell JP, Ballman KV, Klee GG, Berger PB. Lack of association between plasma homocysteine and angiographic coronary artery disease in the era of fortifi cation of cereal grain fl our with folic acid. Atherosclerosis. 2002;165:375-381.
38. Konings EJ, Goldbohm RA, Brants HA, Saris WH, van denBrandt PA. Intake of dietary folate vitamers and risk of colorectal carci- noma: results from The Netherlands Cohort Study. Cancer. 2002;95:1421-1433.
39. Lonn E, Yusuf S, Arnold MJ, Sheridan P, Pogue J, Micks M et al. Homocysteine lowering with folic acid and B vitamins in vascular disease (HOPE 2). N Eng J Med. 2006;354:1567-1577.
40. Bonaa KH, Njolstad I, Ueland PM, Schirmer H, Tverdal A, Steigen T, Wang H, Nordrehaug JE, Arnesen E, Rasmussen K. Homocysteine lowering and cardiovascular events after acute my- cardial infarction. N Eng J Med. 2006;354:1578-1588.
41. Stolzenberg-Solomon RZ. Dietary and other methyl-group avail ability factors and pancreatic cancer risk in a cohort of male smok- ers. Am J Epidemiol. 2001;153:680-687.
42. Giovannucci E, Stampfer MJ, Colditz GA, Hunter DJ, Fuchs C, Rosner BA, Speizer FE, Willett WC. Multivitamin use, folate and colon cancer in women in the Nurses’ Health Study. Annals Intern Med. 1998;129:517-524.
43. Shrubsole MJ, Jin F, Dai Q, Shu Z-O, Potter JD, Hebert JR, Gao Y-T, Zheng W. Dietary folate and breast cancer risk: results from the Shanghai Breast Cancer Study. Cancer Res. 2001;61:7136-7141.
44. Shikany JM, Heimburger DC, Piyathilake CJ, Desmond RA, Greene PG. Effect of folic acid fortifi cation of foods on folate intake in female smokers with cervical dysplasia. Nutrition. 2004;20:409-414.
45. Centers for Disease Control and Prevention. http://www.cdc.gov/ cancer/colorectal/statistics/ accessed 1/22/07.
46. Zhang SM, Willett WC, Selhub J et al. A prospective study of plasma total cysteine and the risk of breast cancer. Cancer Epide- miol Biomarkers Prev. 2003;12:1188-1193.
47. McLean RR, Jacques PF, Selhub J, Tucker KL, Salelson EJ, Broe KE, Hannan MT, Cupples LA, Kiel DP. Homocysteine as a predic- tive factor for hip fracture in older persons. N Engl J Med. 2004;50:2042-2049.
48. Morris MS, Jacques PF, Selhub J. Relation between homocysteine and B-vitamin status indicators and bone mineral density in older Americans. Bone. 2005;37:234-242.
49. Elias MF, Sullivan LM, D’Agostino RB, Elias PK, Jacques PF, Selhub J, Seshadri S, Au R, Beiser A, Wolf PA. Homocysteine and cognitive performance in the Framingham Offspring Study: age is important. Am J Epidmiol. 2005;162:644-653.
50. Robinson K, Gupta A, Dennis V, Arheart K, Chaudhary D, Green R,Vigo P, Mayer EL, Selhub J, Kutner M, Jacobsen DW. Hyperho- mocysteinemia confers an independent increased risk of atherosclero- sis in end-stage renal disease and is closely linked to plasma folate and pyridoxine concentrations. Circulation. 1996;94:2743-2748.
51. Menon V, Sarnak MJ, Greene T, Wang X, Pereira AA, Beck GJ, Kusek JW, Selhub J, Collins AJ, Levey AS, Shlipak MG. Relation- ship between homocysteine and mortality in chronic kidney disease. Circulation. 2006;113:1572-1577.
52. Stevens VL, Rodriguez C, Pavluck AL, McCullough ML, Thun MJ, Calle EE. Folate nutrition and prostate cancer incidence in a large cohort of US men. Am J Epidemiol. 2006;63:989-996.

ABOUT THE AUTHOR
10841 South Crossroads Drive, Suite 105Parker, Colorado 80134Telephone: 303/840.8787Fax: 303/840.6877Web Site: www.wheatfoods.orgE-Mail: [email protected]
Elyse A. Cohen, MS, LN
Health and Nutrition Communications
Elyse A. Cohen, MS, LN, is an independent consultant specializing in health and nutrition communications for consumer and technical applications.
Elyse managed health communications and claim compliance, and pioneered health strategy at General Mills, Hebrew National Foods and Kraft-General Foods. She was Managing Editor of Contemporary Nutrition, the fi rst-ever newsletter for health professionals. As Nutrition Editor of Betty Crocker’s cookbooks and magazines, Elyse contributed to hundreds of publications. Elyse is co-author of Betty Crocker’s Living with Cancer Cookbook. Her writing is published in Food Technology, and other journals, in books such as Whole Grains in Health and Disease, and Nutrition in Exercise and Sport and web-based works.
Elyse holds a Master of Science in Nutritional Sciences from the University of Wisconsin-Madison and a Bachelor of Science in Food Chemistry and Nutrition from Douglass College, Rutgers University, NJ. Elyse is also a licensed nutritionist.





























