-
8/8/2019 18864419-Thoracentesis
1/25
Th o ra ce n t e s is
Sacro, Joy Marian Victoria M.
-
8/8/2019 18864419-Thoracentesis
2/25
Thoracentesis
is an invasive procedure to remove fluid or air from the pleural
space fordiagnostic or therapeutic purposes.
It is done with a needle (and sometimes
a plastic catheter) inserted through thechest wall, generally
afteradministration of local anesthesia .
The recommended location varies
depending upon the source. Somesources recommend the midaxillary
line, in the sixth, seventh, or eighthintercostal space .
http://en.wikipedia.org/wiki/Pleural_effusionhttp://en.wikipedia.org/wiki/Pneumothoraxhttp://en.wikipedia.org/wiki/Pleural_cavityhttp://www.webmd.com/hw-popup/placement-of-a-thoracentesis-needlehttp://en.wikipedia.org/wiki/Local_anesthesiahttp://en.wikipedia.org/wiki/Midaxillary_linehttp://en.wikipedia.org/wiki/Intercostal_spacehttp://en.wikipedia.org/wiki/Intercostal_spacehttp://en.wikipedia.org/wiki/Midaxillary_linehttp://en.wikipedia.org/wiki/Local_anesthesiahttp://www.webmd.com/hw-popup/placement-of-a-thoracentesis-needlehttp://en.wikipedia.org/wiki/Pleural_cavityhttp://en.wikipedia.org/wiki/Pneumothoraxhttp://en.wikipedia.org/wiki/Pleural_effusion
-
8/8/2019 18864419-Thoracentesis
3/25
Why is it done? Removal of fluid and air from the
pleural cavity Diagnostic aspiration of pleural fluid Pleural
biopsy Instillation of medication into the
pleural space
Relieve shortness of breath and paincaused by a pleural
effusion.
-
8/8/2019 18864419-Thoracentesis
4/25
Overview Thoracentesis is done to find the cause of a
pleural
effusion. It also may be done to help the patient
breatheeasier.
During the procedure, the doctor will insert a thinneedle or
plastic tube into the pleural space and drawsout the excess fluid.
Usually, doctors take only theamount of fluid needed to find the
cause of the pleuraleffusion. However, if there's a lot of fluid,
they may takemore. This helps the lungs expand and take in more
air,which allows breathing easier.
After the fluid is removed from the chest, it's sentfor testing.
Once the cause of the pleural effusion isknown, the doctor will
plan treatment. For example, if an infection is causing the excess
fluid, the patient maybe given antibiotics to fight the infection.
If the cause isheart failure, the patient will be treated for
thatcondition.
Thoracentesis usually takes 10 to 15 minutes. Itmay take longer
if there's a lot of fluid in the pleural
-
8/8/2019 18864419-Thoracentesis
5/25
-
8/8/2019 18864419-Thoracentesis
6/25
What To Expect BeforeThoracentesis
You will be asked to sign a consent formbefore a
thoracentesis.
Before thoracentesis, your doctor will talk toyou about the
procedure and how to prepare
for it. Tell your doctor what medicines you'retaking, about any
previous bleeding problems,and about allergies to medicines or
latex.
Also, certain conditions may increase thedifficulty of
thoracentesis. Let your doctorknow if you have:
- Had lung surgery. The scarring from thefirst procedure may
make it difficult to do thisprocedure.
- A long-term (chronic), irreversible lungdisease, such as
emphysema .
http://www.webmd.com/hw-popup/emphysema-8115http://www.webmd.com/hw-popup/emphysema-8115
-
8/8/2019 18864419-Thoracentesis
7/25
Pro ce d u re
-
8/8/2019 18864419-Thoracentesis
8/25
-
8/8/2019 18864419-Thoracentesis
9/25
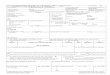
Find the anatomical landmarksbefore you perform the
thoracentesis.
-
8/8/2019 18864419-Thoracentesis
10/25
Clean the area with iodine
-
8/8/2019 18864419-Thoracentesis
11/25
Open the kit and make surethat you know which tube and
needle are used for
-
8/8/2019 18864419-Thoracentesis
12/25
Practice sliding the flexiblecatheter.
-
8/8/2019 18864419-Thoracentesis
13/25
Prepare for local anesthesia.
-
8/8/2019 18864419-Thoracentesis
14/25
Prepare the area.
-
8/8/2019 18864419-Thoracentesis
15/25
Perform the procedure (undersupervision, if you are not
certified).
Anesthetize the skin and pleura, try toreach the effusion
fluid.
-
8/8/2019 18864419-Thoracentesis
16/25
Prepare the flexible catheter.
-
8/8/2019 18864419-Thoracentesis
17/25
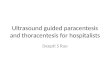
Pass the flexible catheter over thetap needle into the pleural
space andbegin aspirating the fluid in thevacuum tubes.
-
8/8/2019 18864419-Thoracentesis
18/25
-
8/8/2019 18864419-Thoracentesis
19/25
-
8/8/2019 18864419-Thoracentesis
20/25
What To Expect AfterThoracentesis
After thoracentesis, you may need achest x ray to check for any
lungproblems. Your blood pressure and
breathing will be checked for up to afew hours to make sure you
don't havecomplications.
Your doctor will let you know when youcan return to your normal
activities,such as driving, physical activity, andworking.
Once at home, call your doctor right
-
8/8/2019 18864419-Thoracentesis
21/25
Nursing activities
-An explanation helps to orient the patient to the procedure,
assists the patient to mobilize resources, and
provides an opportunity to ask
3. Inform the patient about the procedure: a. The nature of the
procedure
b. The importance of remainingimmobile
c. Pressure sensations to be experiencedd. That no discomfort is
anticipated after
the procedure.
2. Assess the patient for allergyanesthetic agent to be used.
Givesedation if prescribed.
- posteroanterior and lateral chest x-rayfilms are used to
localize fluid and air in the pleural cavity and to aid
indetermining puncture site.
1. Ascertain in advance whether chest x-ray films have been
prescribed andcompleted and the consent form has
been signed.
RATIONALE
-
8/8/2019 18864419-Thoracentesis
22/25
-If air is in the pleural cavity, the thoracentesissite is
usually in the second or thirdintercostals space in the
midclavicular line
because air rises in the thorax.
6. Expose the entire chest. The site for aspiration is
determined from chest x-ray filmsand by percussion.
-Sudden and unexpected movement by the patient can cause trauma
to the visceral pleuraand lung.
5. Support and reassure the patient during the procedure.a.
Prepare the patient for cold sensation of skin germicide solution
and of pressuresensation from infiltration of local
anestheticagent.
b. Encourage the patient to refrain fromcoughing.
-The upright position facilitates the removal of fluid that
usually localizes at the base of thechest. A position of comfort
helps the patientto relax.
4. Make the patient comfortable with adequatesupports. If
possible, place the patient uprightand is one of the following
positions:
a.Sitting on the edge of the bed with feet
supported and arms and head on a padded over-the-bed table.
b.Straddling a chair with arms and headresting on the back of the
chair.c.Lying on the unaffected side with thewith the bed elevated
30 to 45 degrees if unable to assume a sitting position.
-
8/8/2019 18864419-Thoracentesis
23/25
9. After the needle is withdrawn, pressure isapplied over the
puncture site and a small,sterile dressing is fixed in place.
-when a large quantity of fluid is withdrawn, athree-way adapter
serves to keep air fromentering the pleural cavity.-The hemostat
steadies the needle on the chestwall. Sudden pleurific chest pain
or shoulder
pain may indicate that the visceral or diaphragmatic pleura is
being irritated by theneedle point.
8. The physician advances the thoracentesisneedle with the
syringe attached. When the
pleural space is reached, suction maybe appliedwith the
syringe.a. A 20-ml syringe with a three-way adapter (stopcock) is
attached to the needle and theother to the tubing leading to a
receptable thatreceives the fluid being aspirated)
b. If a considerable quantity of fluid isremoved, the needle is
held in place on the
chest wall with a small hemostat
-An intradermal wheat is raised slowly, rapidinjection causes
pain. The parietal pleura isvery sensitive and should be well
infiltrated
with anesthetic before the thoracentesis needleis passed through
it.
7. The procedure is performed under asepticconditions. After the
skin is cleansed, a localanesthetic is injected slowly with a
small-
caliber needle into the intercostals space bythe physician.
-
8/8/2019 18864419-Thoracentesis
24/25
-
8/8/2019 18864419-Thoracentesis
25/25