Embed Size (px)
Citation preview

CL 0.3521
UCL
0.6053
LCL
0.0988
0.000
0.100
0.200
0.300
0.400
0.500
0.600
0.700
Pre
va
len
ce
of
Bro
ad
-Sp
ec
tru
m A
nti
bio
tic
Pre
sc
rip
tio
ns
Period
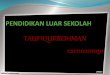
Broad-Spectrum antibiotic prescriptions forUncomplicated AOM
AOM CP Implementation
Background
Daniele Dona1,2, Maura Baraldi3, Giulia Brigadoi3, Silvia Zingarella3, Rebecca Lundin4, Rana F. Hamdy1, Theoklis Zaoutis1, Liviana Da Dalt3 & Carlo Giaquinto2,4
(1)Department of Pediatrics, Division of Infectious Diseases, The Children's Hospital of Philadelphia, Philadelphia, PA,
(2)Division of Pediatric Infectious Diseases, Department for Woman and Child Health, University of Padua, Padua, Italy,
(3)Pediatric Emergency Department, Department for Woman and Child Health, University of Padua, Padua, Italy,
(4)PENTA Foundation, Padua, Italy
• Italian pediatric antimicrobial prescription rates are among the highest in Europe. Identifying effective
stewardship activities is essential [1].
• Where resources are limited for establishment of a robust Antimicrobial Stewardship Program (ASP),
clinical pathways (CPs) represent a reasonable and feasible first step for implementation [2]
• Objective: To evaluate the impact of CPs on antibiotic prescriptions, including drug (narrow vs broad
spectrum) and duration of therapy for acute otitis media (AOM), pharyngitis and community-acquired
pneumonia (CAP)
Effect of clinical pathways on antibiotic prescriptions in an emergency department:
Italian pediatric antimicrobial stewardship starts here
Methods• Intervention: On 1 October 2015 CPs for the management of AOM, Pharyngitis and CAP were
implemented at the Pediatric Emergency Department of the University Hospital of Padua. Three
educational lectures were presented and CPs were distributed as a laminated pocket card.
• Quasi experimental study: Baseline period (10/15/2014 – 04/15/2015) and post intervention period
(10/15/2015 – 04/15/2016)
• Outcomes: Proportion provided prescriptions following “wait and see” approach (AOM only), proportion
provided prescriptions by drug, days of therapy (DOT) and Length of Therapy (LOT) for combination
therapy.
• Data Analysis: process control p-charts were created using QI macros p-chart software. Chi-square,
Fisher’s exact test and Wilcoxon rank sum test were used to evaluate differences from baseline to post-
intervention.
• Definitions:
• Broad-spectrum antibiotics: Amoxicillin-clavulanate, cephalosporins and macrolides were
considered broad-spectrum antibiotics
• Treatment failure: 1)change in antibiotic regimen for persistence of symptoms; 2 ) change in
antibiotic regimen for adverse drug events; 3) relapse of symptoms within 30 days from discharge
date with new antibiotic prescription; 4) new antibiotic prescription in case “wait and see” was the
first line therapeutic choice (only for AOM).
Conclusions
1899
Results
• Evidence-based CPs supported by adequate provider education can
effectively influence prescribing practices for AOM, pharyngitis and
CAP reducing overall and broad spectrum antibiotic prescription
without compromising clinical outcomes.
• CPs represent a promising, resource efficient antimicrobial stewardship
tool especially in an ED setting.
AOM
Pharyngitis
Figure 1. Process control p-charts of broad-spectrum antibiotic
prescriptions for AOM at the ED. An immediate and stable decrease in
broad-spectrum antibiotic use is indicated after CP implementation,
especially for uncomplicated AOM (AOM without otorrea).
CAP
Figure 4. Process Control P-charts of Broad-spectrum antibiotic prescriptions
for CAP at the ED. A stable decrease in broad-spectrum antibiotic use for CAP
is indicated after CP implementation.
Figure 7. Process Control P-charts of Broad-spectrum antibiotic prescriptions for GAS
Pharyngitis at the ED. A dramatic decrease in broad-spectrum antibiotic use is
indicated after pharyngitis CP implementation.
Pre-intervention period Post-intervention period P value
295 278
Treatment N % N %
Wait and see 64 21.7 92 33.1 <0.01
Antibiotic therapy 231 78.3 186 66.9 <0.01
Amoxicillin 74 25.1 96 34.5 <0.05
Broad spectrum (amoxi-
clavulanate
+cephalosporins+
macrolides)
157 53.2 90 32.4 <0.001
Amoxicillin-clavulanate 106 35.9 70 25.2 <0.01
Cephalosporins 47 15.9 16 5.8 <0.001
Macrolides 4 1.4 4 1.4 0.79
Pre intervention Period
298
Post intervention Period
366p-value
Patients not treated with abx 147 49.3 200 54.6 0.17
Pharyngitis treated with abx (Strept
group A (GAS) Pharyngitis)
151 50.7 166 45.4 0.17
Antibiotic option for Pharyngitis
Amoxicillin 81 54 155 93 <0.001
Broad-spectrum
(amoxi-clav + cephalosporins +
macrolides)
70 46 11 7 <0.001
Amoxicillin-clavulanate 60 40 5 3 <0.001
Cephalosporin 10 7 6 4 0.28
Table 1 Treatment options and treatment failure analysis for AOM
Pre-intervention
period
Post-intervention
period
p valueNumber of outpatients 56 41
Total DOT 620 342
N % of DOT N % of DOT
Amoxicillin 338 54.5 243 71.1 <0.0001
Cephalosporins 60 9.7 29 8.5 0.5
Macrolides 132 21.3 22 6.4 <0.0001
Amoxicillin-clavulanate 90 14.5 48 14.0 0.8
References
1 - European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe 2013. Annual report of the European Antimicrobial
Resistance Surveillance Network (EARS-Net). Stockholm: The Centre; 2014.
2 - Samore MH, Bateman K, Alder SC, et al. Clinical decision support and appropriateness of antimicrobial prescribing: a randomized trial. JAMA. 2005 Nov
9;294(18):2305–2314.
Table 3 Treatment options and treatment failure analysis for PharyngitisTable 2 Treatment options for CAP
Figure 5. Days of therapy pre and post-implementation
Figure 6. Length of therapy pre and post implementation
Figure 2. Duration of therapy in median days of therapy (DOT)
each month in pre- and post-intervention by age and diagnosis.
Among children >2 years old with uncomplicated AOM, duration
of therapy changed from exceeding guidelines pre-intervention to
meeting guidelines afterwards.
Therapy Duration for Children < 2 YO with
AOM
Fig.1
Fig.7
Fig.8
Fig.4 Broad-spectrum antibiotic prescriptions for CAP
DOT pre and post implementation
LOT pre and post implementation
Figure 8. Duration of therapy in median days of therapy
(DOT) each month in pre- and post-intervention
Broad-spectrum antibiotic prescriptions for Pharyngitis
Treatment Duration for Children with Pharyngitis
Treatment Failure Pre-intervention Period Post-intervention Period p-value
Children available for follow-up 214 (72.5% of total AOM) 206 (74.1% of total AOM)
Treatment failures 26 12.1 23 11.2 0.75
Changed abx for
persistence of symptoms12 5.6 5 2.4 0.10
Changed abx for side
effects 3 1.4 4 1.9 0.96
Ab prescription after
“wait and see”7 3.3 13 6.3 0.14
Ab prescriptions for new
episode within 30 days4 1.9 1 0.5 0.39
Treatment failures Pre-intervention period Post-intervention period P value
Patients available for follow up98 (64.9% of tretaed
pharyngitis)
118 (71.1% of treated
pharyngitis)
Treatment failure 6 6 8 7 0.93
Changed abx for persistence of
symptoms2 2 3 3 0.83
Changed abx for side effects 2 2 2 2 0.75
Ab prescriptions for new
episode within 30 days2 2 3 2.5 0.83
Treatment failures Pre-intervention period Post-intervention period
p valueNumber of outpatients
available for follow-up44 34
N % N %
Changed abx for
persistence of
symptoms
1 2.3 4 11.8 0.3
Changed abx for
side effects 0 0 0 0
Ab prescriptions for
new episode within
30 days
0 0 0 0
AOM CP ImplementationAOM CP Implementation AOM CP ImplementationAOM CP Implementation
Therapy Duration for Children > 2 YO with
uncomplicated AOM
Therapy Duration for Children > 2 YO with
complicated AOM
AOM CP ImplementationAOM CP Implementation
Fig.2



















![Yakima herald (Yakima, Wash.) 1899-09-14 [p ] · tion of Local](https://img.pdfslide.net/doc/110x75/5faf3302d3b87b0fed298d16/yakima-herald-yakima-wash-1899-09-14-p-tion-of-local-.jpg)


![La democracia. (Ponce, P.R.) 1899-02-06 [p ]](https://img.pdfslide.net/doc/110x75/62ceb4e02e96af262e5f86db/la-democracia-ponce-pr-1899-02-06-p-.jpg)


![La democracia. (Ponce, P.R.) 1899-05-22 [p ]](https://img.pdfslide.net/doc/110x75/62e273af36725e5f5f3d925f/la-democracia-ponce-pr-1899-05-22-p-.jpg)


![Washington Weekly Post. (Washington, DC) 1899-10-31 [p 2]](https://img.pdfslide.net/doc/110x75/62a0b29355accc0cf5065db3/washington-weekly-post-washington-dc-1899-10-31-p-2.jpg)