Embed Size (px)
Citation preview

2 cases of hypertension
Year 1 Michaelmas term 2006

Case 1
• 37 year old, type 1 diabetic schoolteacher
• Recently moved to area and presents for routine check-up
• Blood pressure 220/120

What should “normal” blood pressure be?

Blood pressure
• Systolic between 90 and 135 mmHg (90–135 Torr, 12–18 kPa)
• Diastolic between 50 and 90 mmHg (50–90 Torr, 7–12 kPa)

What are the risks of high blood pressure?

Risks of high blood pressure
• Heart failure
• Heart attack
• Stroke
• Kidney failure
• In diabetes increases risk of microvascular complications: retinopathy, nephropathy etc.

You find out his BS control is poor (HbA1C 12%)
How can poor control lead to high blood pressure?

Hypertension and DM
• Poor diabetic control damages the kidneys (glomerosclerosis).
• Eventually this results in diabetic nephropathy and diabetic renal failure
• Diabetes is the most common disease responsible for renal dialysis and transplantation in the UK

How would you find out if his kidneys were damaged?

Signs of diabetic nephropathy• Proteinuria <20mg in 24h- normal
• 20-200mg microalbuminuria
• >200mg diabetic nephropathy
• N.b. if blood glucose control improved and blood pressure control achieved can slow or even stop progression

Anything wrong in the eyes?

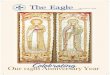
The fundus in hypertension:• Grade I – mild narrowing or sclerosis of retinal
arteries and they are more tortuous. This is called copper wiring or sometimes silver wiring.
• Grade II – thickening of the small arteries pushes on the veins so that the veins appear nipped as they cross the arteries. This is also called A-V nipping
• Grade III – in addition to A-V nipping there are haemorrhages or cotton wool spots. The latter are exudates
• Grade IV – is papilloedema which is swelling of the optic nerve head. It is rarely seen these days and may be associated with the severe headache of hypertensive encephalopathy

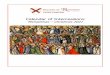
Anything wrong on his ECG?

Left ventricular hypertrophy• R wave V5 plus S wave V1 >35mm
• Non-specific and insensitive test
• Can clarify with echocardiogram
• LVH associated with cardiovascular risk and death rate

Treatment?

ACE inhibitors or angiotensin II receptor blockers drugs of
choice• Evidence that blocking the renin-
angiotensin system is treatment of choice in diabetic nephropathy- get more renal protection for same fall in b.p. compared to other drugs.

Any side effects from ACE inhibitors?

Side effects of ACE inhibitors
• 10% get a dry cough, worse at night
• Check renal function before and after (in case have a renal stenosis)

What blood pressure would you aim for?

Aim for…
140/80 or less. In patients with known renal involvement aim for 130/70

What other drugs might you add to achieve the target, and what
are the problems?

Other drugs:
• May need 3-4 types of drug as a combination
• Diuretics potentiate action of ACE or A2 receptor blockers- used as “second-line”
• “third-line” beta-blocker or calcium channel blocker

Potential problems:• Diuretics cause…. Diuresis• Thiazides may cause hyperglycaemia, precipitate
gout and increase LDL cholesterol• Beta-blockers block warning signs of
hypoglycaemia and may make peripheral vascular disease worse. They also have an adverse effect on lipid profile and can potentiate bronchospasm in asthmatics. Can cause ankle oedema 10-20%

Any other changes in treatment?

Further treatment:• Support from diabetic specialist nurse
• Stronger diabetic control
• Aim for HbA1C <7.5%
• Make sure cholesterol is <5.0
• Give statin to lower cholesterol

And Case 2:
• 26 year old solicitor
• Needed a check up as wanted to take up SCUBA diving
• Found to have b.p. of 210/140


On examination…• Pulse normal at the wrist but femoral pulses
felt weak and delayed compared to wrist or carotid
• Apex beat displaced to left
• Continuous machine-like murmer across precordium and back
• Palpable thrill over patients back
• Fundi:

A-V nipping

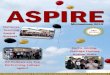
A Chest X ray was arranged…..


Any idea of the diagnosis?


Coarctation of the aorta
• Means “narrowing”- distal to ductus arteriosus• Occurs around 1:10,000 people• More common in Turner’s syndrome; male:
female 4:1• Presents with high blood pressure in arms and low
pressure in legs• CXR shows rib-notching from collateral vessels• May be treated with surgery or balloon
angioplasty

Blood pressure determined by Cardiac output X peripheral
resistance

Other causes of hypertension?

Other causes of hypertension?
• Primary “Essential” most common. Cause unknown Positive family history. May be associated with age, obesity and alcohol
• Secondary:
• Renal disease
• Renal artery stenosis
• Conn’s syndrome (aldosterone secreting tumour)

And….
• Phaeochromocytoma (adrenaline/noradrenaline secreting tumour)
• Drugs e.g corticosteroids
• And pregnancy: Pre-eclampsia