Embed Size (px)
Citation preview
2nd Workshop of CKD-MBD(Insufficienza Renale Cronica - Alterazioni
Metabolismo Minerale)ERA-EDTA Working Group
Milan, 5th December 2014 - Room WASHINGTON A
Programme
• 9.00 - 9.10 INTRODUCTION. M. Cozzolino (Italy)
• 9.10 - 9.40 OPENING LECTURE: CKD-MBD in 2014: WHAT IS NEW?. M. Cozzolino
• 9.40 - 10.20 UPTODATE 2014: HOT TOPICS. Chairs: Z. Massy (France) - D. Goldsmith (UK)• 9.40 P. URENA-TORRES (France) Bone disease in CKD. • 10.00 P. EVENEPOEL (Belgium) CKD-MBD in kidney transplant• 10.20 A. COVIC (Romania) The hidden phosphate
• 10.20 - 10.40 COFFEE BREAK
• 10.40 - 12.40 ORAL PRESENTATIONS. Chairs: J. Bover (Spain) - V. Brandenburg (Germany) - S. Mazzaferro (Italy)
• 12.30 - 13.10 LECTURE: PROGRESSION OF RENAL DISEASE AND CKD-MBD: WHICH LINK? M. Vervloet (The Netherlands)
• 13.10 - 14.00 LUNCH
• 14.00 - 15.30 MEET THE EXPERTS: HOW TO TREAT CKD-MBD PATIENTS• 14.00 M. VERVLOET- B. BRANDENBURG Phosphate binders: calcium based vs. calcium free• 14.30 D. GOLDSMITH - S. MAZZAFERRO Vitamin D?• 15.00 Z. MASSY - J. BOVER Calcimimetic• 15.30 P. URENA-TORRES - P. EVENEPOEL New biomarkers
• 15.30 - 16.20 WHAT DID WE LEARN? Chairs: M. Cozzolino - M. Vervloet
• 16.20 - 16.30 CLOSING REMARKS AND NEXT STEPS. M. Cozzolino
P. EVENEPOEL (Belgium)CKD-MBD in kidney transplant
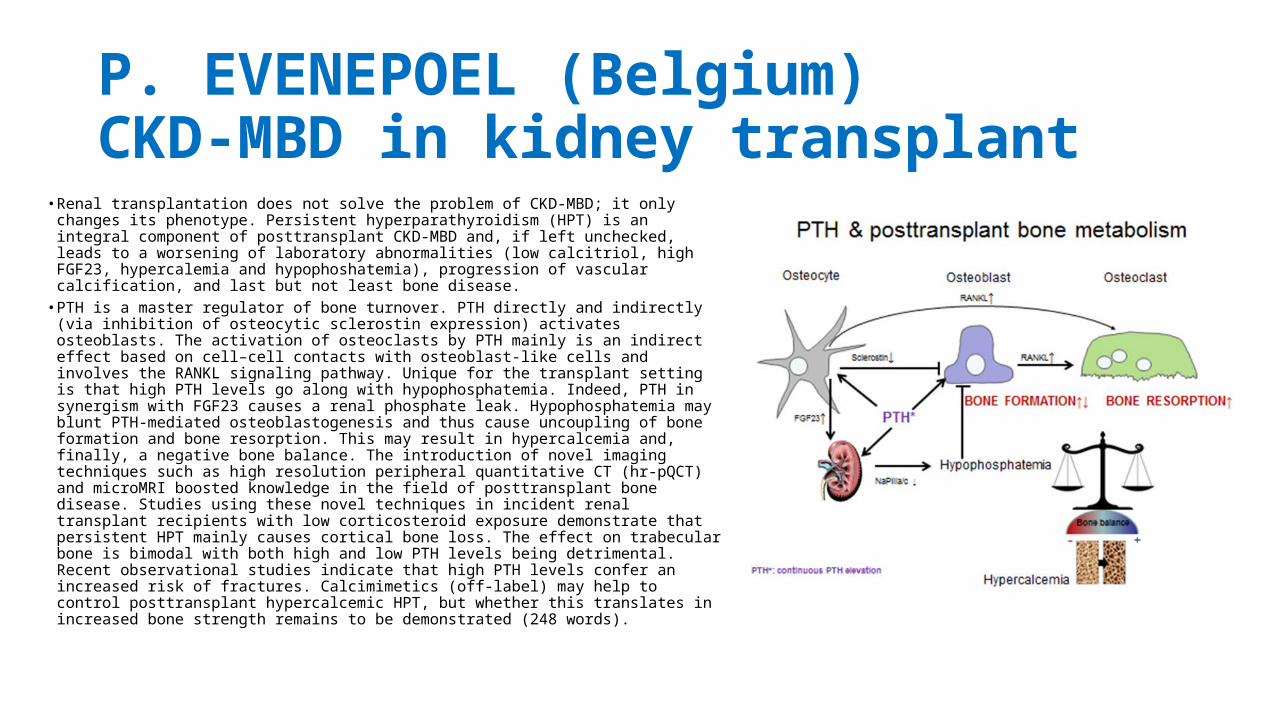
• Renal transplantation does not solve the problem of CKD-MBD; it only changes its phenotype. Persistent hyperparathyroidism (HPT) is an integral component of posttransplant CKD-MBD and, if left unchecked, leads to a worsening of laboratory abnormalities (low calcitriol, high FGF23, hypercalemia and hypophoshatemia), progression of vascular calcification, and last but not least bone disease.
• PTH is a master regulator of bone turnover. PTH directly and indirectly (via inhibition of osteocytic sclerostin expression) activates osteoblasts. The activation of osteoclasts by PTH mainly is an indirect effect based on cell–cell contacts with osteoblast-like cells and involves the RANKL signaling pathway. Unique for the transplant setting is that high PTH levels go along with hypophosphatemia. Indeed, PTH in synergism with FGF23 causes a renal phosphate leak. Hypophosphatemia may blunt PTH-mediated osteoblastogenesis and thus cause uncoupling of bone formation and bone resorption. This may result in hypercalcemia and, finally, a negative bone balance. The introduction of novel imaging techniques such as high resolution peripheral quantitative CT (hr-pQCT) and microMRI boosted knowledge in the field of posttransplant bone disease. Studies using these novel techniques in incident renal transplant recipients with low corticosteroid exposure demonstrate that persistent HPT mainly causes cortical bone loss. The effect on trabecular bone is bimodal with both high and low PTH levels being detrimental. Recent observational studies indicate that high PTH levels confer an increased risk of fractures. Calcimimetics (off-label) may help to control posttransplant hypercalcemic HPT, but whether this translates in increased bone strength remains to be demonstrated (248 words).
M. Cozzolino (Italy)CKD-MBD in 2014: WHAT IS NEW? • Since the beginning stages of CKD, although patients are completely
asymptomatic, important mineral homeostasis disorders happen. These disorders, involving serum level calcium, phosphorus, parathyroid hormone, and vitamin D, have a striking impact on patients prognosis as they affect cardiovascular system. The new term of “ Chronic Kidney Disease-Mineral Bone Disease” (CKD-MBD) was birth to label bone disease during CKD as a systemic disorder tightly linked to cardiovascular calcifications and disabilities.

BONE/KIDNEY/CARDIOVASCULAR LINK:THE CENTRAL ROLE OF CKD-MBD
CKDMBD
Mortality
P. URENA-TORRES (France). Bone disease in CKD• Progressive chronic kidney disease (CKD) ineluctably leads to mineral and bone disorders (MBD). The
numerous biochemical alterations observed in CKD, namely the reduced natural and active vitamin D metabolites, hypocalcemia, hyperphosphatemia, high parathyroid hormone (PTH), high fibroblast growth factor 23 (FGF23), high sclerostin, and low klotho, independently or in concert affect bone metabolism and ultimately bone quality and quantity. However, alone or combined, these circulating biomarkers are poor predictor of the type of bone disease in CKD.
• To establish a firm diagnosis of the type of bone disease in CKD the qualitative and quantitative histomorphometric evaluation of a bone biopsy still remains the gold standard.
• The bone histomorphometric nomenclature system describes essentially five types of bone disease in CKD: osteitis fibrosa or high bone turnover, adynamic bone disease, osteomalacia, mixed lesions associating high bone turnover and osteomalacia, and osteopathies due to trace metal overload. This classification of CKD bone diseases is mainly based on three parameters: bone formation rate after tetracyclin double labeling, bone volume, and the amount of unmineralized osteoid surface or in other words the presence or not of mineralization trouble.
• As an example, patients with an increased amound of unmineralized osteoid sufaces, low number of osteoblast and osteoclast cells, and a decreased bone formation rate are classified as having osteomalacia. Tetracycline double labeling shows the absence or a light diffusion of tetracycline labeling and a marked increase in osteoid surfaces. In secondary hyperparathyroidism with severe osteitis fibrosa, the chronic and marked excess of PTH leads to marrow fibrosis, expansion of osteoid surfaces, woven osteoid, increased number and activity of osteoblasts, numerous osteoclasts and resorptive surfaces. Tetracycline labels cover the majority of the bone mineralization surfaces and a larger space between the double-labeled staining indicating accelerated bone formation. No mineralization defect is observed. In adynamic bone disease there is no tetracycline labeling along the bone surface. There a very low number of osteoblast and osteoclast cells. Low bone turnover is represented by the absence of differentiation of the double-tetracycline labeling.
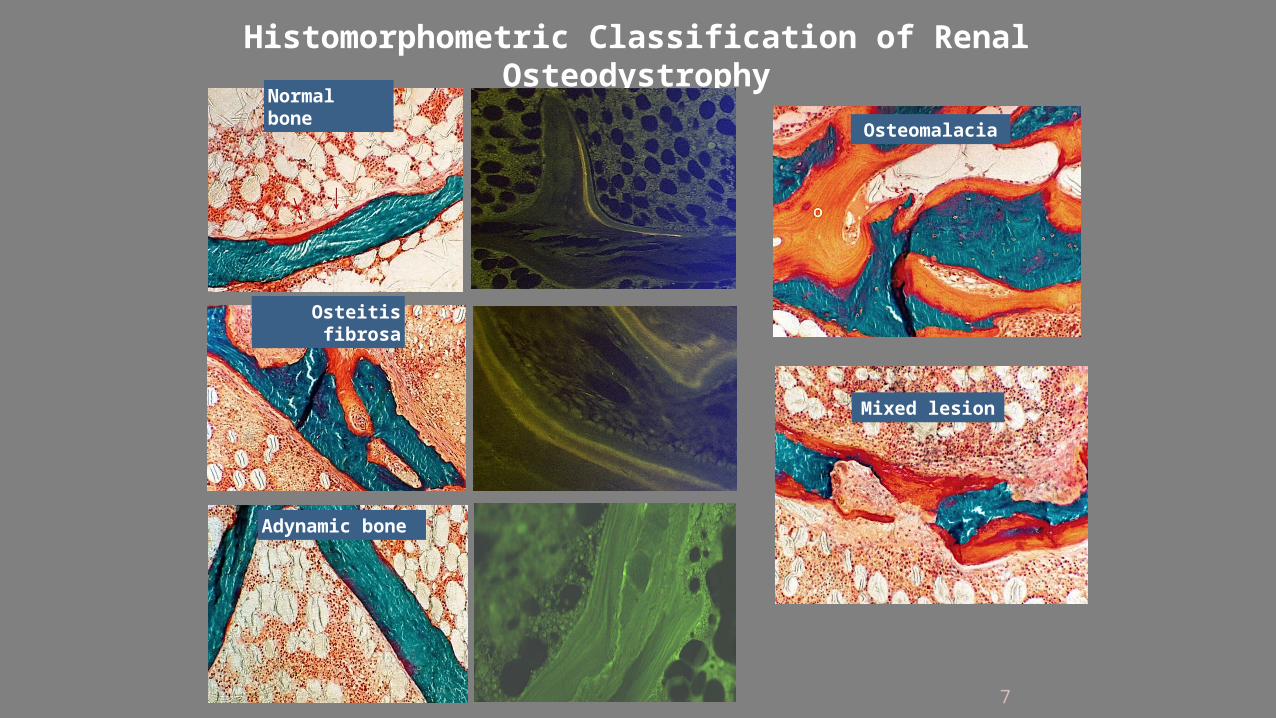
Osteomalacia
Mixed lesion
Histomorphometric Classification of Renal Osteodystrophy
Normal bone
Adynamic bone
Osteitis fibrosa
7
ORAL PRESENTATIONS
• Young researchers from Europe presented original researches as Poster or Oral presentation (see the Abstracts at …..).• The WG Board also selected the three best contributions and the
winners were:• Melissa Verkaik (the Netherland)• Maarten de Jong (the Netherland)• Paola Ciceri (Italy)
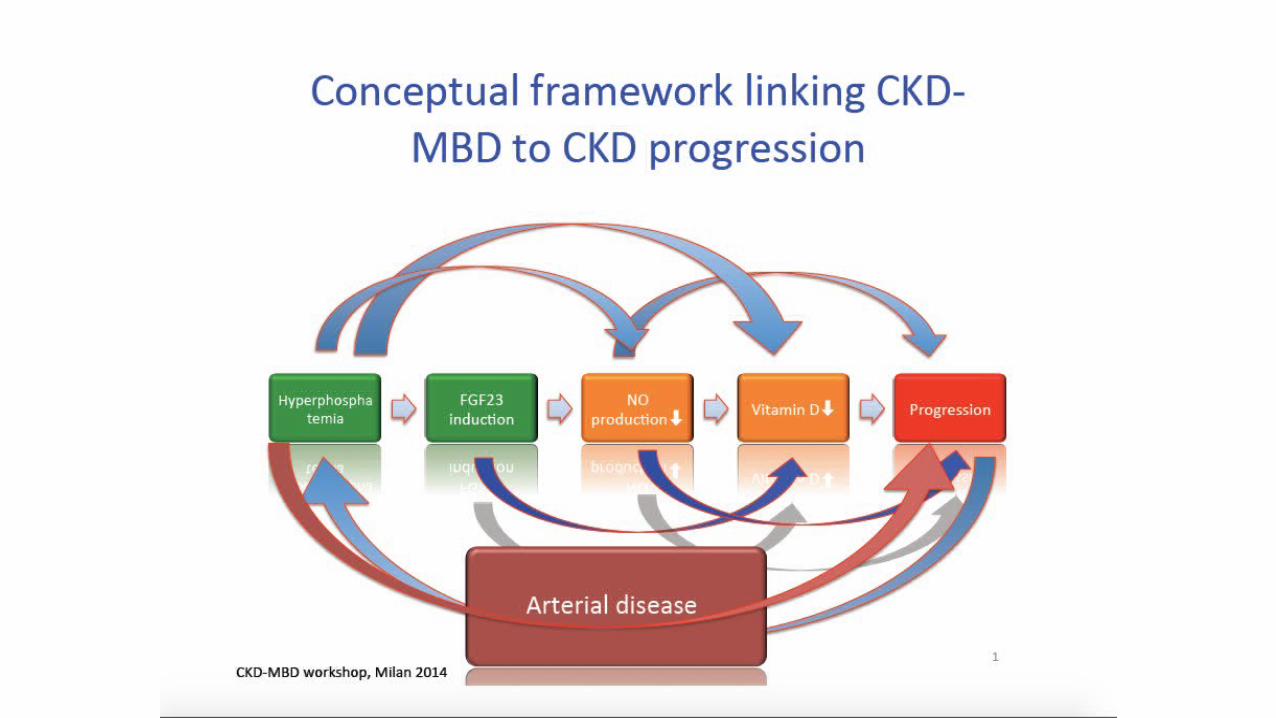
M. Vervloet (The Netherlands)PROGRESSION OF RENAL DISEASE AND CKD-MBD: WHICH LINK?
• Several components of CKD-MBD are implicated to aggravate CKD progression. Especially for low levels of active vitamin D, hyperphosphatemia, increased levels of FGF23 and low kidney tissue levels either epidemiological or pathophysiological arguments advocate a role in CKD progression. To a large extent the presumed mechanisms are renal tissue fibrosis. In addition CKD-MBD induced arterial disease can affect renal perfusion. A final important notion is that several vicious circles may be at hand amplifying renal risk.
MEET THE EXPERTS’ SESSION on“HOW TO TREAT CKD-MBD PATIENTS”
In these meetings two chairmen and some 20 people openly discussed, is separate meeting rooms, some specific arguments mainly pointing to practical implications. Groups were as follows:1. M. VERVLOET - B. BRANDENBURG Phosphate binders: calcium
based vs. calcium free2. D. GOLDSMITH - S. MAZZAFERRO Vitamin D?3. Z. MASSY - J. BOVER Calcimimetic4. P. URENA-TORRES - P. EVENEPOEL New biomarkerThese meetings lasted roughly one hour and half and were followed by a final report and discussion in the plenary room










![mom] mod mbo mbo mbb mbm mbd mbd mbb mbmJ mbd cnb« … · mom] mod mbo mbo mbb mbm mbd mbd mbb mbmJ mbd cnb« mmo mmb mmm mmd mmd mmb ma-ml mmd mdo mdo m db mdm mdd mdd m db mdGY)J](https://img.pdfslide.net/doc/110x75/5f01ee397e708231d401bcfa/mom-mod-mbo-mbo-mbb-mbm-mbd-mbd-mbb-mbmj-mbd-cnb-mom-mod-mbo-mbo-mbb-mbm-mbd.jpg)


















