-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
1/12
Journa l of Consul t ing and C l in ica l Psychology2001, Vol.
69, No. 4, 643-654 In the pub l i c domainDOI :
10.I037//0022-006X.69.4.643
Shaping Cocaine Abstinence by Successive ApproximationKenzie L.
Preston, Annie Umbricht , Conrad J. W o n g , and David H.
EpsteinNat ional Ins t i tu te on Drug Abuse
Cocaine-us ing methadone-maintenance pa t ients were randomized
to s tandard contingency management(abs t inence group, n = 49) or
to a contingency des igned to increase contact with re inforcers
(shapinggroup, n = 46). For 8 weeks , both groups earned esca la t
ing-va lue vouchers based on thrice-weeklyurina lyses : The abs t
inence group earned vouchers for coca ine-negative urines only; the
shaping groupearned vouchers for each urine specimen with a 25% or
more decrease in coca ine metabol i te (first 3weeks) and then fo r
negative u rines only ( las t 5 weeks). Cocaine use was lower in
the s ha p ing g roup , b u tonly in the last 5 weeks , when the
response requirem ent was identica l . Thus , the shaping conting
encyappeared to better prepare pa t ients fo r abs t inence. A 2nd
phase of the s tudy showed tha t abs t inenceinduced by esca la t
ing-va lue vouchers can be ma in ta ined by a nonesca la t ing
schedule , sugges t ing tha tc on t ing e nc y managem ent can be
pract ica l as a maintenan ce trea tment.
In the subs tant ia l effort expended to find effective
therapies fo rcocaine abuse, contingency management has been among
the mostsuccessful t reatments to date. Contingency management was
de-veloped using operant principles whose effectiveness had
beendemonstrated preclinically (Bigelow & Si lve rman, 1999).
Cont in-gent re inforcement of target behaviors, such as drug
abstinenceand par t ic ipat ion in t reatment activit ies, can be a
powerfu l tool inestablishing pos i t ive behavioral changes in
drug abusers (Higgins,Sti tzer, Bigelow, & Liebson, 1986;
Kidorf & Stitzer, 1996; M c-Ca u l , Stitzer, Bigelow, &
Liebson, 1984; Stitzer, Iguchi, & Felch,1992). One of the most
effective applications of the procedure hasused a monetary-based
escalating-reinforcement schedule in whichthe value of the
incentive increases with each consecutive drug-nega t ive urine
specimen, whereas lapses (posit ive urine speci-mens) and missed
specimen collections result in loss of the incen-tive and a return
of the next earned incentive to the original value(Higgins e t al.,
1991, 1993, 1994). This procedu re has been usedsuccessfully in a
number of c l in ics , inc lud ing our own (Kirby,Marlowe,
Festinger, Lamb, & Plat t , 1998; Silverman et al.,
1996,1998).Most studies using contingency management have made
thede l ive ry of incent ives cont ingent on d rug-negat ive ur ine
speci-mens (i.e., reinforcement of abstinence). Although this
technique
Kenzie L. Pres ton, Ann ie Umb richt , Conrad J . Wong, an d
David H.Eps te in, Intramura l Research Program, Nationa l Ins t i
tu te on Drug Abuse,Bal t imore , Maryland.Conrad J . Wong is now a
t the Department of Psych ia try and Behaviora lBiology, Johns
Hopkins Univers i ty School of Medicine.This s tudy was supported
by the Intram ura l Research Program of theNational Ins t i tute on
Drug Abuse. We are grateful to the Archway trea t-m e nt staff and
technicians ; to Kenneth Silverman an d Charles R. Schus terwho
helped des ign the cl inica l t ria l ; to Robert Broo ner who
monitored themethadone-maintenance trea tment; and to A nna DeJe s
us w ho assisted inth e c o n d u c t of this s tudy.Correspondence
concerning this a r t ic le should be addressed to KenzieL.
Preston, In t ramura l Research Program, Nationa l Ins t i tute on
DrugAbuse, 5500 Nath an Shock Drive, Bal t imore , Maryland 21224.
Electronicmail may be sent to kpr e s t o n @ i n t r a .n i d a .n
i h .go v .
has been effective for many patients, experience in our clinic
hasshown that some part icipan ts who reduce their cocaine use will
notimmediately produce negative urine specimens. Cocaine ur i
nescreens are typically considered posit ive above a cutoff of
300ng /ml in benzoylecgonine equivalents (BZE); benzoylecgonine,the
major metaboli te of cocaine, has a urinary excretion half-lifeof 6
to 8 hr (Ambre, 1985) and can usual ly be detected for 48 hr(Saxon,
Calsyn , Haver, & Delaney, 1988). In some cases, patientsmay
cease or reduce their cocaine use, yet go unreinforce d becausenot
enough t ime ha s elapsed before sample collection, esp ecially
ifinitial BZE levels were high. For example, in patients who
hadappeared unrespons ive to a voucher cont ingency in one of
ourearlier studies (Silverman et al., 1996), quanti tat ive
urinalysesshowed significant decreases in BZE levels (from a mean
ofapproximate ly 60,000 ng/ml during baseline to approxi-mately
30,000 ng /ml d u r i ng th e voucher cont ingency) . Thesepat
ients had presumably reduced their cocaine use, yet they re-ceived
few or no vouchers because their BZE concentrationsremained above
the standard cutoff . Upon not receiving a voucher,such patients
may have become discouraged and relapsed to druguse before
achieving abstinence of adequate duration to have anegative urine
screen.
In th i s s tudy we tested a var ia t ion of cont ingency
managementin which incentives were ini t ially given fo r decreases
in BZEconcentrations and subsequently were given only for
samplestest ing negative for BZE at the standard cutoff .
Reinforcement ofsuccessive approximations of a desired behavior (
in this case,cocaine abstinence) is known in the operant condit
ioning li teratureas shaping (Catania, 1973). Shaping has an
extensive history fo rt raining desirable behaviors in nonhumans
and has been usedsuccessful ly to modify behavior in c l inical
popula t ions as well(e.g., se e Catania, 1973; Meyer &
Chesser, 1970). W e hypothe-sized that patients would be more
likely to reach th e ul t imate goalof cocaine abs t inence if
incremental decreases in BZE concent ra-t ions were reinforced
early in t reatment. This shaping of absti-nence was compared with
a more typical contingency procedure inwh i ch incentives were
given only fo r samples test ing negative fo rBZE at the s tandard
cutoff .
643
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
2/12
644 PRESTON, U M B R I C H T , W ON G , A N D EPSTEI NA
secondary goal of the study was to evaluate the use of amaintenance
cont ingency as a fol low-up to the escala t ing-re inforcement
procedure. Patients who completed the main inter-
vent ion phase of the present study were switched to a
nonescalat-ing reinforcement schedule (with fixed-amount vouchers
an d take-home doses given as incent ives fo r negative urine
specimens). Thisw as tested against a control procedure in w hi c h
th e samef ixed-amoun t vouchers an d take-home doses were
givennoncon t ingen t ly .
MethodParticipants
Par t ic ipan ts were selected from 28 5 patients consecutively
admitted fo rm e th adone maintenance a t Arch way Cl inic , the
trea tment research programof th e Nat ional Ins t i tu te on Drug
Abuse Intramura l Research Program inBalt imore, M D . Appl icants
were first screened by te lephone and then intw o on-s i te visits
tha t included medica l , psychia tr ic , and drug-use his tor ies
,a phys i ca l exa mina t ion , u r ine and blood screens, and a
battery of assess-m e nt ins t ruments : Addict ion Severi ty Index
(McLel lan e t a l . , 1985); Na -t iona l I ns t i tu te on Menta
l Heal th D iagnos t ic In terview Schedule (Helzer,C roug h an , R
obins , & Ratcliff, 1981); Beck Depress ion Inventory (B DI
;Beck & Steer , 1987); Symptom Check Lis t90Revised
(SCL-90-R;Derogat is , 1977); and the Shipley Ins t i tute of
Living Scale (Zachary,1986). Persons were eligible for the s tud y
if they were between 18 and 65years of age, if they qual i f ied fo
r methadone maintenance accord ing toFood an d Drug A d mini s t r
a t ion gu id e line s , and if they reported histories
ofintravenous opiate use. Two studies were conducted concurrently,
thiss tudy focusing on coca ine use and the other focus ing on
opiate us e(Preston, Umbricht , & Epste in, 2000). Patients
were eligible for the opiateor coca ine s tudy if at least 3 of 15
ur ine specimens col lected during a5-week basel ine trea tment
phase tes ted pos i t ive fo r morphine (heroinmetaboli te ) or
BZE, respectively. Patients who met the criteria for cocainebu t
not for opiates were assigned to the present cocaine st udy .
Patients w homet the cri ter ia fo r both drugs were randomly ass
igned to one of thestudies. Persons with current major psychiatric
il lness or uns table ser iousmedical i l lness were excluded. The
local ins t i tu t ional review board fo rh u m a n research
approved this s tudy, and al l part ic ipants gave informedwri t
ten cons en t p r io r to part ic ipa t ion.Standard Treatment
Al l part ic ipants received, without charge, s tandard
methadone mainte-nanc e tha t consisted of da ily methadone an d
weekly individual counselingt h r o u gho u t the 25-week s tudy.
Methadone HO (Mall inckrodt , St. Louis,MO ) w as adminis tered ora
l ly in a cons ta n t vo l ume (35 ml) of a cherry-f lavored so lu
t ion . Metha d one dose w as stabil ized at 50 mg within th e f
irstweek of t r e a tment an d held cons tant through th e 25-week
s tudy. Counsel -in g sess ions were problem focused and included
both support ive andmotiva t ional techniq ues . Counselors
completed a semis tructured psycho-socia l assessment and master t
rea tment plan fo r each participant thatguided the focus of a l l
counsel ing sess ions . Reduc tion of subs tance use wasth e pr
imary goal. Counselors helped participants develop a funct
ionalanalys is of their subs tance use , identify an d avoid high-r
isk subs tance us es i tua t ions , a void f r iends an d
acquaintances w ho used drugs, cope withurges to use drugs , an d
examine acute an d long-term consequences of druguse .Urine and
Breath Toxicology
Each Monday, Wednesday, and Friday urine specimens were
collectedunde r th e observa tion of trained laboratory
technicians. W e conductedqua l i t a t ive testing with a n enzyme
mult ipl ied im m unoassay technique
(Syva, Palo Alto, CA) system that gave qualitative results for
cocaine(BZE), opia tes (morphine) , benzodiazepines (oxazepam),
phencycl id ine ,barb i turates, and marijuana . Cutoff
concentrations fo r pos i t ive specimenswere 300 ng /m l for
cocaine, opiates, and benzodiazepines; 25 ng /m l fo rPCP; and 50
ng/ml for marijuana . BZE concentra t ions were measured
byfluorescence polar iza t ion immunoassay (FPIA) us ing TD x
Cocaine M e-tabolite Assay reagents (TDx; Abbott Laboratories,
Abbott Park, IL) on aTD x instrument. Cross-reactivity wa s 100%
for BZE and less than 1% fo rcocaine, ecgonine methyl ester, an d
ecgonine. Th e assay provides accuratequant i ta t ion for
concentra t ions between 30 and 5,000 ng/ml ; specimenswith
concentra t ions higher than 5,000 ng/ml were diluted to concentra
t ionswithin the 30 to 5,000 ng/ml range an d reanalyzed. Breath
alcohol levelswere determined with an Alco-Sensor III
(Intoximeters, St. Louis, MO).
Self-Report QuestionnairesWe collected participants '
self-reports of drug use immediately after
each urine collection. Participants were asked whether they had
used, theam oun t and nu mb er of times used, and the dollars spent
on alcohol, opiates,coca ine , benzodiazepines , phencycl id ine ,
or marijuana on each day s incetheir last cl inic visit. On
Wednesdays, participants completed a cravin gques t ionnaire and
the Lifes tyle Changes Ques t ionnaire (Silverman et al.,1998). On
the craving qu es t ionnaire , part ic ipants ra ted how m uch they
hadwanted coca ine an d heroin during th e past week on a scale
from 0 (not atall) to 4 (extremely). On the Lifestyle Changes
Questionn aire, p articipantsindica ted whether they ha d engaged
in any of nine act ivi t ies to stop,reduce, or avoid coca
ine/heroin use during th e past week (analyzed as totalnum b e r o
f items endorsed) an d whether they ha d engaged in any c r imina
lactivity.
Study Timeline and GroupsThe s tudy was conducted in three con
secutive phases : a 5-week basel ine
trea tment phase, an 8-week intervention, and a 12-week
maintenancephase. Baseline began on s tudy enrol lment and
continued unt i l th e partic-ipant had provided 15 urine
specimens, typically at the end of 5 weeks. Atthe end of baseline,
participants were randomized to one of two interven-tion groups ,
an experimenta l group re inforced fo r decreases in drug use anda
control group re inforced for coca ine-negative urine specimens
only. Atthe end of the intervention, part ic ipants remaining in
trea tment wereoffered 12 weeks of addit iona l methadone main
tenance; ha l f of the part ic-ipants in each group were random ly
ass igned to con t inue on a ma in tena ncecontingency or to switch
to a noncontingent condit ion. (This "rerandom-iza t ion" aspect of
the study design is similar to that used in the Pittsburghstudy of
maintenance trea tments fo r depression; Kupfer e t al., 1992.)Trea
tment an d data collection otherwise remained th e same throughout
th es tudy.
Intervention
During the intervention, all participants could earn vouchers on
the basisof urine specimens collected every Monday, Wednesday, and
Friday. Theabs t inence group (n = 49) earned vouchers for each
urine specimen thattested cocaine negative on the qualitative urine
screen at the 300 ng/mlBZE cutoff. This criterion for earning
vouchers was in place throughoutthe 8 weeks of intervention.
Patients in this group received th e fol lowinginstruction at the
beginning of the intervention: "For the next 8 weeks, youca n earn
vouchers fo r provid ing urine samples which indica te tha t yo u
haveno t used cocaine." The shaping group (n = 46 ) earned vouchers
for eachurine specimen whose BZE concentration was 25% or less than
that of thespecimen collected 48 hr to 72 hr earl ier during the
previous clinic visit orless than 300 ng/ml . This shaping
contingency was in effect for 3 weeks ,fol lowed by 5 weeks of an
abs t inence contingency ( identica l to the one
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
3/12
SH A PI N G COCA I N E A B STI N EN CE 645used for the abs t
inence group). Pa t ients in this group received the fol lowingins
truct ions :
For the next 8 weeks , you can earn vouchers for provid ing
urinesamples which indica te tha t you have decreased your use or
not usedcocaine. During the f irs t 3 weeks we wil l measure the
amo unt ofcoca ine in your u r ine . If the a m o u n t of coca ine
in your u r ine isdecreased by at least one quarter (25%) compared
to your previousurine sample , you wil l earn a vouc her. You wil l
also receive a voucherif your urine sample is coca ine-free during
Weeks 1 to 3. DuringWeeks 5 to 8, you wil l earn vouchers only if
your ur ine sample iscocaine- free .
The 25% cri ter ion was chosen to reflect what we thought would
bec l in ical ly s ignif icant decreases in use and was based on
earl ier work in ourc l in ic showin g tha t a 50% decrease in BZE
conc entra t ion genera l ly ind i-ca tes abs t inenc e (Preston,
Silverma n, Schus ter , & Cone, 1997).
The voucher in centive program was based on tha t developed by
Higginsan d colleagues (Higgins et al . , 1991, 1993, 1994). The
values of thevouchers were the same for both groups . Values began
a t $2.50 an dincreased in value by $1.50 fo r each consecutive
voucher earned. Inaddition, for every three consecutive vouchers
earned, participants receivedan addit iona l voucher worth $10. A
part ic ipant who met the cr i ter ia forearning a voucher for 8
consecutive weeks could earn a tota l of $554(average $9.89 per
day). If the participant did not meet the criteria forearning a v
oucher, the part ic ipant d id not receive a voucher, and the va
lueof the next earned vo ucher w as reset to $2.50. Earned vouchers
were givento part ic ipants the day after ur ine col lect ions
(Tuesday, Thursday, andSaturday). The vouchers were exchangeable
for goods and services (e .g . ,passes to the movies , exercise
equipment, dr iver ' s l icense , or gift cert if i-ca te) tha t
would support a drug-free l i fes tyle . When th e part ic ipant
accu-mula ted enough vouchers to purchase a desired item, a staff
memberreviewed the reques t to determine w hether the des ired i
tem was cons is tentwith tha t part ic ipant ' s t rea tment goa ls
. I tems were purchased by staffmemb ers and given to part ic
ipants in the cl inic; no m oney was givendirec t ly to part ic
ipants .
Maintenance ContingencyA t the end of the intervention phase ,
part ic ipants were rerandomized to
one of two ma in tena nce cond i t ions : con t ingen t or
noncontingent. Part ic i-pants in the contingent group received a
$10 voucher for each coca ine-negative specimen submitted for the
thr ice-weekly u rine tests . In addit ion,if part ic ipants had
two out of three coca ine-negative u rine specimensdur ing the
week, they received a dose of methadone on Sa turday to take a th
om e on Sunday. Part ic ipants ass igned to the noncont ingen t g
roup re -ceived vouchers and take-home doses indepen dent of their
ur ine resul ts .Each non contin gent group part ic ip ant was rand
om ly yoked to a part ic ipan tin th e contingent group,
independent of in te rven tion g roup a s s ignment . Fo reach cl
inic visit numbered from 1 to 36 (3 per week fo r 12 weeks) tha t
th ec on t ing e n t part ic ipan t earned a vo ucher or take-home
dose for tes t ingcoca ine-negative , th e non con tinge nt part ic
ipant received an identica lvoucher or take home dose fo r provid
ing urine . If the n o n c o n t i n g e n tpart ic ipant d id not
provide a ur ine specimen or d id not a t tend cl inic , theincent
ive was forfe i ted; part ic ipants were not told when this
occurred .Rules fo r us ing vo uche r s r ema ined as in the
intervention phase; unusedvouche r money a ccum ul a ted across the
entire s tudy and could be used forup to 1 year after study part ic
ipa t ion ended.Data Analysis
Because part ic ipants were rerandomized into new groups between
theintervention and main tenanc e phases , da ta from the two
phases wereanalyzed separately (b ut similar ly). The analyses
described here apply toboth phases , with exceptions as noted .
To ensure comparabil i ty between groups , w e analyzed intake
measuresby analys is of variance (ANOVA; for continuous variables)
, Pearson ch isquare (for categorical variables), or Fisher's exact
test (for categoricalvariables with expected cell sizes less than
5) . Retention rates werecompared between groups with surviva l ana
lys is , by us ing a log-rank tes tof time until the provision of
the final urine sample; participants who leftbefore the final week
of the experimental phase ( intervention or mainte-nance) were
coded as dropouts . Part ic ipants with three or more sporadi-ca l
ly miss ing u rine tes ts (i.e., not because of dropout) du ring
the experi-mental phase were coded as poor a t tenders ; this was
compared betweengroups with Fisher's exact tes t . Voucher earnings
were compared byA N O V A ; percentages of part ic ipants never
earning a voucher were com-pared by Pearson chi-square tes t .The t
ime course of coca ine u se during interv entio n was ana lyzed
withgeneralized l inear mixed models fi t with the SAS macro GLIM
MIX (Lit te l ,Mill iken, Stroup, & Wolfinger , 1996). GLIMMIX
analyzes d ichotomousrepeated m easures with miss ing da tapoints
by invoking the SAS procedu reMI XED w i th a logit l ink (SAS,
1997) and gives adjusted proportions. Afirs t-order autoregress ive
error s tructure was used. Continuous measurestaken a t repea ted t
imepoints during intervention (such as BZE levels ,craving, se l f-
reported u se , and l i fes tyle changes) were ana lyzed with
mixedregressions (SAS MIXED procedure) . Each model con ta ined one
within-subjec t factor (Time) an d four between-subjects factors :
contingency,basel ine percentage nega tive (or mean), poor a t
tendance, and dropout(Hedeker & Gibbons , 1997). Analyses of
maintenance-phase da ta con-trolled for pr ior contingenc y as an
addit iona l be tween-subjects factor; somemaintenance-phase
analyses a l so control led fo r intervention percentagenegative
.
In the interventio n phase , e ight intake measures d iffered
between groupsat p s.10; in the maintenance phase , five intake
measures d ifferedbetween groups a t p & .10. To control for po
tentia l con foun ding , wecons idered each intake measure fo r
inclus ion in the G L I MMI X and mixed-regression models if it had
a ma in effect on the outcome mea s ure at ps.05 and if tha t
effect remain ed s ign i f ican t w hen it was entered into a
modelwith th e factors l isted in the previous paragraph. In no
case di d tha t occur.
Because the BZE da ta were heav ily r ight-skewed, a l l nonzero
va lueswere log- transformed (D elucchi, Jones , & Batki ,
1997) to reduce thein f luence of extremely high values before th e
data were entered into amixed-regress ion model .
Longes t du ra t ion of coca ine abs t inenc e was ca lcula ted
for each p art ic-ipant as the longes t run of consecutive coca
ine-negative urine specimensduring intervention and main tenanc e
phases ; groups were compared by anA N O V A .
Al l analyses were two-ta i led; a was set at .05, with trends
noted at .10.
Resul tsParticipant Characteristics
Of the 285 part icipants who enrolled in the study, 253
com-pleted th e 5-week baseline. O f these 253, 22 participants met
thecriteria for cocaine use o nly, 29 met the criteria for opiate
use only,an d 190 participants met the cri teria for both opiate
and cocaineuse. Twelve patients did not meet cri teria for e i ther
drug; theyreceived standard treatment for the durat ion of the s
tudy. A tota lof 95 participants were randomized to one of two
groups in thepresent s tudy; the two groups did not differ in terms
of drugcri teria met, x*(l, N = 95) = 0.38, p = .54. Their
demographicinformation is shown in Table 1. A mong the 43
demographicvariables compared, e ight differed across in te rvent
ion groups a tp < .10: The shaping group ha d more i l legal
income, more yearsof sedative use, more recent days of cocaine use,
more recent daysof heroin use, higher BD I scores, and more psychia
t r ic symptom-
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
4/12
646 PRESTON, UMBRICHT, WONG, AN D EPSTEINTable 1Demographic
Characteristics of Patients
Intervention phase
VariableAge (in years; M SD )Male (% )African American (%
)Marital status (%)MarriedDivorced/widowedNever
marriedSeparatedEmployment (%)
F u l l t imePart timeUnemployedIncome past 30 days(U.S. $; M
SD)LegalIl legalEducation (in years;M SD)Self-reported l i f e
years ofdrug us e (M
SD)HeroinCocaineAlcoholSedatives/tranquilizersMarijuanaDrug use in
past 30 days
(M
SD)HeroinCocaineAlcoholSedatives/tranquilizersMarijuanaCurrent
DSM-III-Rdiagnosis(% of Ss; from DIS)PhobiaPTSDAntisocial
personalityNicot ine dependenceHeroin dependenceCocaine
dependenceAlcohol dependenceSedative dependenceBD I (M SD)SCL-90-R
GlobalSeverity Index(M SD fShipley Ins t i tute of LivingScale (M
SD)
VocabularyAbstract thinkingPrior cont ingenc yAbst inence (%
)Shaping (% )
Abstinence( = 49)38.2 6.15152
14184127271657
642 47870 7611.5 1.8
15.2 7.66.0 7.53.6 6.20.02 0.13.6 6.222.3 1 1 . 49.9 10.04.1
7.30.2 0.60.8 1.9
621853965310417.5 10.560.4 8.8
39.7 9.947.9 9.0
Shaping(n = 46)
37.9 5.3595922204613281557
71 5 526868 1,91911.6 1.9
12.3 8.36.6 6.04.4 8.00 .7 2 . 14.0 6.7
25.9 8.315.8 10.53.7 7.00.9 3.01.0 2.8
13275298597421.6 10.367.7 10.4
39.9 10.848.4 9.7
Analysis"F ( l , 9 3 ) = 0.06^(1) = 0.56^(D = 0.47^(3) =
3.04
X*(2) = 0.05
F(l, 93) = 0.52F(l, 93) = 8.39F ( l , 93 ) = 0.18F ( l , 9 3 ) =
3.18F(l, 93) = 0.18F ( l , 93 ) = 0.28F(l , 93) = 4.43F ( l , 9 3 )
= 0.11F(l, 93 ) = 3.13F(l, 93) = 7.84F(l, 93) = 0.11F(l, 93) =
2.46F(l, 93) = 0.22
^(1) = 3.02^(1) = 0.01^(1) = 0.31
F(l, 93) = 3.62F ( l , 9 2 ) = 13.53
F(l, 93) = 0.01F(l, 93) = 0.06
P.81.45.49.39
.98
.47
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
5/12
SHAPING COCAINE ABSTINENCE 647atology on the SCL-90-R but had
fewer years of heroin use and alower prevalence of Antisocial
Personality Disorder.
After completing the intervention, 80 participants were
reran-domized to one of the maintenance groups. The
demographiccharacteristics of the rerandomized maintenance groups
are alsoshown in Table 1. The groups did not differ in terms of
prior groupduring intervention. Five demographic variables differed
acrossgroups at p < .10: The contingent group had less legal
income,more years of alcohol and marijuana use, more recent days
ofcocaine use, more recent days of marijuana use, and lower
prev-alence of nicotine dependence.Intervention Phase (Shaping vs .
AbstinenceContingencies)
Retention, missing urine specimens, and voucher
earnings.Overall, 80 (84%) of 95 participants completed all 8 weeks
ofintervention. Survival analysis showed no significant
between-groups difference in retention rates. Groups also did not
differ inn u m b e r s of missed urine specimens (Table 2).
Total voucher earnings did not differ between groups, but then u
m b e r of vouchers earned in the first 3 weeks was
significantlyhigher in the shaping group (Table 2). Participants in
the absti-nence group were significantly more likely to fail to
contact thereinforcer (i.e., to earn at least one voucher), even
during the
final 5 weeks of intervention, when the response requirement
forthe two groups was identical (Table 2).
Cocaine useurine screens. Overall, approximately 15% ofa ll
urine specimens were cocaine negative during the 5-weekbaseline,
with participants in the shaping group having aslightly, though not
significantly, higher proportion of negativeurines (Table 3; Figure
1). The trend during baseline was for therate of negative urine
specimens to decreasethat is, for use toincrease. This trend was
reversed in both groups with the onsetof th e contingent-voucher
invention, resulting in a significanteffect of phase (baseline vs.
intervention, see Table 3). Duringthe first 3 weeks of
intervention, the percentage of cocaine-negative urine specimens
increased similarly in both groups(Figure 1). At the end of the
third intervention week, when thes h a p i n g group was switched
to the more stringent requirementof earning vouchers for
cocaine-negative urine specimens, thepercentage of cocaine-negative
urine specimens in that groupincreased fu r the r . No
corresponding increase occurred in theabstinence group. Data from
the intervention phase were en-tered into a generalized linear
mixed model, controlling fordropout, poor attendance, and each
participant's percentage ofcocaine-negative urine specimens during
baseline. There wasno main effect of group, b u t there was a s i g
n i f i c a n t Group XD ay interaction, F(23, 1842) = 2.13, p <
.002), reflecting the
Table 2Retention, Missing Urine Specimens, and Voucher Earnings
During Intervention and Maintenance
Variable Abstinence Shaping Analysis
Reached Week 8 of intervention, nCompleted Week 8 of
intervention, nTotal weeks in treatment, including baseline
(M SD )Sporadically missing urines d uring interventionM SD%
poor attendersaVoucher earnings (U.S. $; M SD)Number of vouchers
earned in first 3 weeks(M SD)Number of vouchers earned in final 5
weeks(M SD)Participants earning no vouchersFirst 3 weeks, nFinal 5
weeks, nThroughout intervention phase, n
Number enrolledReached Week 12 of maintenance, nCompleted Week
12 of maintena nce, nTotal weeks in treatment, including b
aseline(M SD )Sporadically missing urines during maintenanceM SD%
Poor attenders"Voucher earnings (U.S.$; M SD)Number of take-home
doses of methadone(M SD)
Intervention43 (88%)43 (88%)
12.34 1.931.12 1.9416$101 1852.69 3.313.71 5.76
23 (47%)27 (55%)19 (39%)Maintenance
4136 (88%)34 (83%)24.5 1.71.2 1.59.8$135 1324.4 7.7
phase40 (87%)37 (80%)
12.23 2.040.87 1.059$115 1705.09 2.525.17 5.51
2(4%)14 (30%)2 (4%)phase
3935 (90%)34 (87%)24.7 1.11.6 1.728.2$119 1263.7 4.6
Log-rank /(I) = 0.83F(l, 93) = 0.06F(\, 93) = 0.61^(1) = 1.25F (
l , 9 3 ) = 0.15F(l , 93) = 15.60F(l , 93) = 1.60^(1) = 22.20^(D =
5.88/(I) = 16.33
Log-rank ^(1) = 0.25F(l, 78) = 0.23F ( l , 78) = 1.91/(I) =
4.47F ( l , 78) = 0.30F(l, 78) = 0.46
.36
.80
.44.26.70
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
6/12
648 PR ESTON , UMB R I CH T, W O N G , A N D EPSTEINTable 3Urine
Test Results During Intervention: Mean Percentage of
Drug-NegativeSpecimens an d Standard Deviation
G rou p A N O VAAbstinence
VariableCoca ine -nega t ivebBase l ineInte rvent ionOpia te
negative15Basel ineIn terven t ionBenzodiazepine negative15Basel
ineIn te rvent ionC annab i s negat ive6Base l ineInte rvent
ionAlcohol -nega tive0Base l ine
Inte rvent ion
M
12275858938984869894
SD
1837293816242927
521
Shaping Phase Phase X GroupM
17336157959290879899
SD F "131.432034 0.1223
30 5.481417 0.612427 1.6154
P F- p< .001 2.01 .16
.73 0.39 .54
< .02 0.05 .82
.44 0.73 .40
.21 3.80 < .06
Note. A N O V A = analysis o f var iance.8 d fs = 1 , 9 3 . b
Urine spec imens. c Breath specimens.
s up e r i o r pe r f o r m a n ce of the sh a p in g g r o u p
du r in g th e la t te r pa r tof the i n t e r v e n t i o n
.Other measures of coca ine use also appeared to favor th e shap-in
g in tervent ion , t h o u gh not to a statistically signif icant
degree.Mean BZE levels were 48,389 (SEM = 8,644) ng/ml in theshap
ing gr o u p and 56,340 (SEM = 8,626) in the abst inence
group,mixed regression, F(l, 90) = 1.70, p = .20. The longest dura
t ionof abst inence , in fer red from consecut ive nega t ive
specimens, av-eraged 5.5 (SEM = 1.1) in the shaping group and 5.1
(SEM = 1.2)in the a bs t in e n ce g r o u p , A N O V A , F(l, 93)
= 0.04, p = .83; thedifference remained nons ign i f i can t in an
ana lysis of covariancecont ro l l ing fo r each p ar t ic ipant '
s base l ine percentage nega t ive .
Use of other drugs. There were only minor changes in otherdrug
use f rom baseline to intervention, with rates of use similaracross
the two in te rvent ion groups (Table 3) . There was a signif-i can
t effect of phase (baseline vs . in te rvent ion) on percentage
ofbenzodiazepine-negat ive urine specimens, with both groups hav-in
g sl ight ly fewer nega t ive specimens dur ing th e in te rvent
ion . Th enear-s ignificant (p = .054) Phase X Group in terac t ion
fo r alcoholreflects th e s l igh t ly greater tenden cy for the
abst inence group totest posi t ive fo r a lcohol dur ing th e in
te rvent ion . In both cases,however , the rates of positives fo r
benzodiazepines an d alcoholwere relatively low and of doubt fu l
cl in ica l s ign if icance .
Self-reported cocaine use, heroin use, cocaine craving,
positivelifestyle changes, an d criminal activity. Self-reported
frequencyof coca ine use tended to be higher dur ing baseline in
the shapinggroup than in the abst inence group; thus , when in
tervent ion da tawere ana lyzed in a mixed regression controlling
fo r baseline, therewas a trend toward a m a in effect of group,
favoring th e shapingintervent ion (Table 4) . There were no signif
icant group differencesin other self-reported indices of coca ine
or heroin use, drug crav-ing, lifestyle changes, or criminal
activities (Table 4) . However ,s ignificant improvem ents occur
red from base l ine to intervention
(in both groups) in f requency, amount , and cost of heroin use,
incraving for cocaine and heroin, and in c r iminal activities
(repeated-measures ANOVAs on whole-phase means; data not
shown).Maintenance Phase (Abstinence Contingency vs .Noncontingent
Vouchers)
Retention, missing urine specimens, an d voucher earnings.Eighty
participants com pleted the intervention and were rerandom-ized,
with approximately half of each intervention group assignedto each
of the contingent and noncontingent maintenance groups.Sixty-eight
(85%) of the 80 participants com pleted all 12 weeks ofmaintenance.
Survival analysis showed no signif icant between-groups difference
in retention rates during either phase. Groupsalso did not differ
in n u m be r s of missed urine specimens, in totalvoucher
earnings, or in number of take-home doses of methadone(Table 2) .
However, there were signif icantly more poor attenders(participants
missing three or more ur ine specimens) in the non-cont ingent
group; this w as controlled for in mixed models.
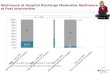
Cocaine use urine screens. For the contingent group,
thepercentage of cocaine-negative ur ine specimens f luctuated
around40%; for the noncontingent group, i t f luctuated around 20%
(Fig-ure 2). There was substantial day-to-day variabili ty in each
group,bu t no clear upward or downward trend in either . Before
testingbetween-groups differences, we noted that the contingent
groupoverrepresented participants who had already achieved high
de-grees of abstinence during intervention. Therefore, each
partici-pant 's percentage of cocaine-negative ur ine specimens
during in-tervention was included as a covariate in a generalized
linearmixed model; th e other covariates were dropout, poor
attendance,pr ior contingency, and maintenance group (contingent
vs. noncon-t ingent). The main effect of maintenance group w as
signif icant,F(l, 73) = 6.58, p < .02. Adjusted percentages of
cocaine-
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
7/12
SHAPING COCAINE ABSTINENCE 649601
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60 63 66
69 72 75Baseline Intervention MaintenanceNumber of consecutive
urine specimens
Figure 1 . Percen tage of par t ic ipan ts cocaine a bs t i n en
t on 75 success ive u r ine tes t days in the basel ine phase(1 5
specimens), in terven t ion phase (2 4 specimens), an d m a i n t
en a n ce pha s e (3 6 specimens) in the two t r e a t m en
tgroups: abs t inenc e group (vouchers fo r coca ine-negat ive u r
ine specimens on ly ), shaping group (vouchers fo rdecreased
cocaine metabolite concen t ra t ion for 3 weeks fo l lowed
vouchers for coca ine-negat ive u r ine specimenson ly). Data shown
here are raw percen tage va lues ; miss ing specimens ( including
those due to dropout) aret r ea ted as posi t ive . For the abs t
inence group, n = 49 in the basel ine and in terven t ion phases
and 43 in them a i n t en a n ce phase; for the s ha p i n g g r o
u p , n = 45 in the basel ine an d in terven t ion phase and 37 in
them a i n t en a n ce phase. Note tha t the shaded area represen
ts the on ly por t ion o f the s tudy dur ing which the twogroups
were t rea ted d i f feren t ly (see in terpre ta t ion in Discuss
ion). Dur ing the main tenance phase, par t ic ipan tswithin each
grou p were rerand omized to new c on t ingencies (see Figu re 2);
da ta in this figure a re co l lapsed acrossthose con t ingencies
.
negat ive ur ine spec imens were 7% in the nonc ont ingen t
group and22% in the cont ingent group. (These pe rcentages appear
lo wbecause they ar e adjusted for all effects in the model , inc
lud ingeach pa r t ic ipant ' s ear l ie r pe rcentage of negat ive
ur ine spec imens .We present them here for in te rgroup compar i
sons ra the r than asabsolute indicators of pe rformance . ) Th e
effect of pr ior cont in-gency is discussed below.The longest
duration of abstinence, inferred from consecut ivenegat ive spec
imens , showed a t rend toward be ing s igni f icant lygreater in
the co nt ingent group (M = 8.2, SEM = 1.7) than in then o n co n t
i n g e n t g roup (M = 4.3, SEM =1.0), F(l, 78) = 3.92, p
=.051.
Use of other drugs. There were no signif icant be
tween-groupdifferences in use of o t he r d rug s d u r i ng m a i
n t e nanc e as determinedin ur i ne or breath screens (Table 5)
.Self-reported cocaine use, heroin use, cocaine craving,
positive
lifestyle changes, an d criminal activity. There were fe w
differ-ences be tween the maintenan ce groups on se l f- repor ted
measures(Table 6). Trends (p < . 10) toward s igni f icant Group
X W eekinteractions occurred only in mean dollars spent on cocaine
perday and m e a n a m o u n t o f heroin used per day.
E f f e c t of prior contingency. One of the mixed models
(de-scribed above in the section Cocaine use urine screens)
enabledus to evaluate th e effect of pr ior cont ingency (shaping
vs. absti-nence) whi le cont rol l ing for current cont ingency and
othe r var i -ables. The effect of pr ior cont ingency was not s
igni f icant , F(l,73) = 1.21,/ j = .27, but par t ic ipants
formerly in the shaping groupdi d tend to maintain higher rates of
cocaine-negative urine than didparticipants formerly in the
abstinence group, regardless of reran-domiza tion (Figure 1).
Adjusted percentages of cocaine-nega tiveurine specimens were 26%
(former shaping) versus 19% (formerabstinence) in the abs t inence
groups and 10% (former shaping)versus 4% (former abs t inence) in
the noncont ingent groups . Asbefore, we present these adjusted
percentages for intergroup com-par i sons rather than as absolute
ind icators of pe rformance .
DiscussionT he r e s u l t s s how t ha t c on t i ng e nc y
manag e me n t fo r c oc a i neab us e c an b e more e f fe c t i
ve w he n i n t rod uc e d i n a s t e p w i s efash ion . R e i n
fo rc e me n t o f decreases in ur ine BZE concent ra-t i ons p r i
o r t o i n i t i a t i on o f ab s t i ne nc e r e i n fo r c e me
n t ( s hap i ng
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
8/12
650 PRESTON, UMBRIC HT, WONG , AND EPSTEINTable 4Self-Reported
Cocaine an d Heroin Use, Craving, Lifestyle Changes,an d Criminal
Activity Intervention
Grou p Mixed regressionAbst inence Shaping Group Week
VariableSelf-reported cocaine use 8Mean frequency per
dayBaselineInterventionIntervention (adj)bMean amoun t per day
(mg)Basel ineInterventionIntervention (adj)bMean dollars spent per
dayBasel ineInterventionIntervention (adj)bSelf-reported heroin
usea
Mean f requency per dayBasel ineIn te rvent ionIntervention
(adj)bMean amount per day (mg)Basel ineInterventionIntervention
(adj)bMean dol lars sp ent per dayBasel ineInterventionIntervention
(adj)bWeekly self-report questionnaireC oc a i ne cravingcBasel
ineInterventionIntervention (adj)bHeroin craving 0Basel
ineInterventionIntervention (adj)bLifestyle changes '1BaselineIn te
rvent ionIntervention (adj)bCriminal activities'1Basel
ineInterventionIntervention (adj)b
M
0.320.310.5430.429.881.6
2.181.943.53
0.150.110.150.190.120.251.210.781.16
1.561.511.571.431.160.973.744.023.880.070.020.001
SD M SD F p F p
0.26 0.46 0.410.35 0.30 0.320.49 0.47 0.47 2.98 < .09 1.20
.2330.3 44.2 49.740.7 55.4 206.1186.2 84.4 181.8 0.09 .77 0.90
.60
3.05 2.69 3.033.15 2.02 3.104.83 3.08 4.75 0.49 .49 1.04 .41
0.15 0.18 0.160.18 0.11 0.120.21 0.13 0.20 0.55 .46 1.23 .210.18
0.29 0.590.19 0.22 0.730.49 0.23 0.47 0.12 .73 1.00 .471.48 1.39
1.831.41 0.64 1.031.89 0.90 1.83 1.23 .27 0.96 .52
0.77 .52 0.840.94 .27 0.961.12 .35 1.09 2.52 .12 1.73 .101.03
.39 1.061.21 .20 1.081.47 1.03 1.36 0.13 .72 1.13 .342.21 4.22
1.732.64 4.05 2.132.87 3.53 2.78 0.90 .35 1.21 .290.19 0.17
0.530.14 0.05 0.160.03 0.04 0.03 1.76 .19 1.07 .38
Group X WeekF P
0.76 .79
0.75 .80
0.85 .67
0.45 .99
1.01 .44
0.98 .50
0.58 .77
0.38 .91
0.88 .53
1.35 .22Note. Adj = adjusted.a Data w ere available for 95
participants. Degrees of freedom are (1, 90) for grou p and (23,
1927) for t ime andGroup X Time. b Adjusted means control for
baseline, dropout, and poor attendance; they are presented hereas
in tergroup compar isons ra ther than as absolute indicators of
performance. c Data were available for 93participants. Degrees of
freedom are (1, 88) for group and (7, 534) fo r time an d Group X
Time. Craving wa srated on a scale of 0-4. d Data were available
for 93 par t ic ipants . Degrees of freedom are (1, 88) for gr oup
and(7, 534) for t ime and Group X Time. Lifestyle changes are
reported as the mean sum of the i tems reported perweek. Criminal
activit ies are the mean of the total reported per week.
group) resu l ted in lower coca ine use (as indica ted by
morecoca ine-nega t ive ur ine specimens) than did a co n t in ge n
cy th a tre inforced o nly coca ine-nega t ive ur ine specimens
(abstinencegroup). Although both groups had similar rates of coca
ine-nega t ive ur ine specimens dur ing the fi rs t 3 weeks of the
inter-ve n t i on , th e shaping group showed an increase in nega t
ive
specimens on escalation of the cont ingency requirement .
Thisadded t r ea tment e f fec t was evident dur ing th e la tter 5
weeks ofth e in te rvent ion and tended to be mainta ined across a
12-weekmaintenance t r ea tment . As we had hypothesized, pa r t ic
ipants inthe shaping group contac ted th e re inforcer more f
requent ly thandid those in the abst inence group.
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
9/12
SH A PI N G COCA I N E A B STI N EN CE 651601
50"
40-
30
20
10 contingentnoncontingent
42 45 48 51 54 57 60 63 66 69 72 75Number of consecutive urine
specimens
Figure 2. Percentage of part ic ipants coca ine abs t inen t on
36 success iveur ine tes t days in the maintenance phase in the two
trea tment groups :con t ingen t g roup (vouche r s a nd t a ke
-home me tha d one doses for coca ine-negative urine specimens; n =
41), noncon tingen t group (vouchers andtake-home methadone doses
independent of urine tes t resul ts ; n = 39).A p p rox im a te ly
half of the patients ha d part ic ipa ted in the abs t inence
groupan d half ha d participated in the s ha p ing g roup jus t p r
io r to the ma in tena ncephase. Data shown here a re raw
percentage va lues ; m i s s i n g s pec imens( inc luding those
due to dropout) a re t rea ted as pos i t ive .
The present findings extend the body of work on
shaping(reinforcement of successive approximations of a final
target be-havior ) as a method of substance-abuse treatment.
Shaping hasbeen used to increase substance-abuse patients '
completion oftreatment-plan tasks (Iguchi, Belding, Morral, L amb ,
& H us b and ,1997). Patients received contingent vouchers for
counselor-assigned behaviors directed at meeting treatment goals,
such asgaining employment. I f the patient did not complete an
assignedtask, a less diff icul t task was s ubsti tuted; if the
task was completed,a more diff icul t task was assigned.
Contingencies were thustailored to each patient 's needs. The
shaping procedure was ap-parent ly successful, as patients had
significant increases in drug-free urine specimens compared with
patients receiving voucherreinforcement of drug-negat ive ur ine
spec imens an d with patientsin a standard-care group.
Prior studies have also involved reinforcement of decreases
inbiological indicators o f drug use; this ha s been attempted
mostfrequent ly with tobacco, using exhaled carbon monoxide (CO)
asthe indicator of use. Early studies did not involve shaping in
thestrictest sense because th e response requirements never
changed;mone tary rewards were given each t ime part icipants
reached afixed target of 50% of baseline CO (Sti tzer &
Bigelow, 1982;Schmitz, Rhoades, & Grabowski, 1995) or a fixed
target of 16 or 8ppm (Sti tzer & Bigelow, 1985). In the lat ter
study, i t was notedthat the use of a diff icul t t a rge t (8 p p
m) led to fa i lures to contac tthe reinforcer, leading the authors
to suggest that such a targetshould not be int roduced abrupt ly.
The deve lopment of a s l id ing-scale procedure , in which the
magni tude of each reward wasinversely related to the amo unt of CO
detected (Sti tzer & Bigelow,1984), led to a study similar to
the current one, in which asliding-scale phase was followed by an
abstinence-contingencyphase (Sti tzer, Rand, Bigelow, & Mead,
1986). In that study,
Table 5Urine Test Results: Percentage of Drug-Negative Specimens
in Maintenance
VariableCocaine nega tive0
M (SEM)Ad j fo r basel ine urineAd j fo r in te rven t ion ur
ineOpia te negative 0M (SEM)Ad j fo r basel ine urine
Benzodiazepine negat ive 0M (SEM)Ca nna b i s nega tive 0M
(SEM)Alcohol negative*1M (SEM)
C on t ing e n t
3 7 ( 6 )372261(5)669 3 ( 2 )75(6)9 7 ( 1 )
A N O V A a GLIMMIX "G roup G roup G roup Da y
N onc on t ing e n t F p F p F p
21 (4.5) 5.06 .0273 4.71 < .04 1.76 < .017 6.58 < .02
1.63 < .02
58(5 ) 0.31 .57860 . 0.47 .50 1.19 .2187(4) 1.81 .18286(4) 2.66
.10798 (1) 0.33 .566
Group X DayF P
1.29 .121.11 .30
0.97 .52
Note . Genera l ized l inear mixed model (GLIM MIX) is an SAS
macro tha t ana lyzes d ichotom ous repea ted m easures with miss
ing da tapoints by invokingth e SAS procedure MIXED with a logit l
ink. A N O VA = a na l ys i s o f var iance , adj = adjus ted .* A
N O V A degrees of freedom are 1 and 78; mis s ing ur ine samples
were considered pos i t ive fo r coca ine an d opia tes for A N OVA
s . b GLIMMIX degreesof freedom for group are 1 and 73 and for day
and Group x Day, 35 and 2,410. Adjus ted (Adj) percentages a re
from GLIMMIX models; they appear lowbecause they c ontrol for
intervention -phase contingenc y, dropout, poor a t tendance, and e
i ther basel ine urin e sample tes ts or intervention urine tes ts
; theyare presented here for intergroup comparisons ra ther than as
absolute ind ica tors of performance. GLIMMIX models were not
fitted for benzodiazepines ,cannabis, or alcohol because low rates
of use led to underd ispe rs ion ( lack of varia t ion) in the da
ta . c Urine specimens . d Breath specimens .
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
10/12
652 PRESTON, UMBRICHT, WONG, AND EPSTEINTable 6Self-Reported
Cocaine an d Heroine Use, Craving, Lifestyle Changes,an d Criminal
Activity Maintenance
Mixed regressionGroup Group Week Group X Week
Variable Contingent Noncontingent F p F pSelf-reported cocaine
use"Mean frequency per day:M (SEM)Ad j M (SEM)Mean amount per day
(mg)
M (SEM)Ad j M (SEM)Mean dollars spent per dayM (SEM)Ad j M
(SEM)Self-reported heroin us e3Mean frequency per dayM (SEM)Ad j M
(SEM)
Mean amoun t per day (mg)M (SEM)Ad j M (SEM)Mean dollars spent
per dayM (SEM)Ad j M (SEM)Weekly self-report questionnaireCocaine
cravingbM (SEM)Ad j M (SEM)Heroin craving5M (SEM)Ad j M
(SEM)Lifestyle changes 0M (SEM)Ad j M (SEM)Criminal activities'M
(SEM)Ad j M (SEM)
0.27(0.06) 0.41(0.07)0.42(0.09) 0.54(0.09) 1.66 .20 0.92 .61
1.06
0.08(0.02) 0.12(0.03)0.11(0.03) 0.15(0.03) 1.29 .26 0.88 .67
0.950.11(0.03) 0.13(0.04)0.16(0.04) 0.19(0.03) 1.05 .31 1.04 .41
1.400.52(0.14) 0.76(0.26)0.75(0.26) 1.07(0.24) 1.66 .20 0.75 .86
1.251.21(0.15) 1.22(0.15)1.43(0.18) 1.39(0.17) 0.05 .82 1.21 .27
0.691.25(0.18) 1.13(0.15)1.57(0.20) 1.38(0.20) 0.85 .36 0.90 .54
1.314.14(0.42) 4.23(0.43)3.90 (0.46) 3.62(0.43) 0.36 .55 0.90 .54
0.350.03 (0.02) 0.02 (0.02)0.05(0.02) 0.04(0.02) 0.11 .74 0.80 .64
1.06
.3828.5(7.3) 41.9(14.7)42.0(14.4) 35.7(13.9) 0.20 .66 0.97 .52
0.92 .611.86(0.60) 1.59(0.30)4.82(1.80) 3.91(1.71) 0.22 .64 1.09
.33 1.32 < .10
.55
.06
.15
.75
.22
.97
.39Note. Adjusted (Adj) means control for baseline,
intervention-phase contingency, dropout, an d poor atten-dance.a
Data were available for 80 participants. Degrees of freedom are 1
and 73 for group and 35 and 2,410 for timean d Group X Time. b Data
were available for 78 participants. Degrees of freedom are 1 and 71
for groupan d 1 1 and 684 for t ime and Group X Time. Craving wa s
rated on a scale of 0-4. c Data were available for 78participants.
Degrees of freedom are 1 and 71 for group and 11 and 684 for time
and Group X Time. Lifestyle changesare reported as the mean sum of
the i tems reported per week. Criminal activities are the mean of
the total.
participants' reductions in smoking during the sliding-scale
phasepredicted their subsequent ability to abstain. However, all
partic-i pan t s in that study were exposed to the sliding scale;
there was noabs t inence-only group fo r comparison.We know of only
two published studies (prior to this one)i nvo lv ing reinforcement
of decreases in biological indicators ofcocaine use. In one of
them, the reinforcement was used only as am e a n s to induce
abstinence so that withdrawal symptoms could bes tudied; thus,
there was no baseline condition and no control group(Evans , Levin,
Fischman, & Foltin, 1998). Nonetheless, there wassome
suggestion of eff icacy. Nine non-treatment-seeking cocainesmokers
earned vouchers for each urine specimen that had adecreased
concentration of BZE (compared with the previouslycollected
specimen). Of 81 specimens collected, 68% had concen-t ra t ions
lower than the previous specimen, 56% had decreases of50% or
greater (suggesting no new use since the prior specimen
collection), and 23% of all specimens were negative for
BZE.Another study used a sliding scale (monetary reinforcers of $10
or$12 for each successive decrease in the level of BZE and $12
or$15 for each cocaine-negative specimen) in 12
cocaine-dependentmethadone-maintenance patients (Elk et al., 1995).
The procedurewas effective; BZE levels significantly decreased and
cocaine-negative specimens increased compared with a period of
baselinetreatment. Again, there was no abstinence-contingency
controlgroup, nor was there a subsequent attempt to introduce
anabstinence-only requirement.In our study, those two elementsan
abstinence-contingencycontrol group and an elevation of the
response requirementenabled the most striking of our findings: The
shaping group's rateof cocaine use differed f rom that of the
abstinence group onlywhen the response requirement ceased to
differ. During the first 3weeks of intervention (the only time when
the shaping contingency
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
11/12
SH A PI N G COCA I N E A B STI N EN CE 653was in effect), part
icipants in both groups sharply reduced theirrates of use relative
to baseline (Figure 1). On the basis of everyavailable drug-use
measure, the two groups were behaving almostidentically. The
difference lay in the consequences: For part ici-pants in the
shaping group, reductions in cocaine use were rein-forced more
frequently (Table 2). In the subsequent 5 weeks ofintervention,
when the response requirement for both groups wasabstinence, the
former shaping part icipants maintained a higherrate of abstinence
than did those for whom the response require-m e n t had been
abstinence all along. Even in the ensuing mainte-nance phase, this
trend continued (though not to a degree thatreached stat ist ical
significance) within each of the new reinforce-ment schedules to
which part icipants were rerandomized.
These results are reminiscent of findings from the applied
be-havior analysis l i terature on compliance, where i t has been
shownthat re inforcement of a high-probabili ty behavior ( i .e . ,
a behaviorthat part icipants will readily engage in ) increases
subsequent com-pliance with a requirement to perform a
low-probabili ty behavior(i.e., a behavior that part icipants will
not readily engage in ; Mace,Mauro, Boyaj ian, & Eckert, 1997).
This "high-p procedure" de-scribes our shaping intervention, which
reinforced a behavior( reduc tion of d rug-use f requency) that
occurs in nearly all part ic-ipants at the start of a voucher
intervention, even if vouchers aregiven noncontingently (Preston et
al., 2000).The effectiveness of the high-/? procedure has been
interpretedas an example of behavioral momentum, defined by Nevin
as theproduc t of response rate an d resistance to change (Nevin,
1992;Ne v i n , Mandell, & Atak, 1983). According to this
theory, greaterdensity of reinforcement of a behavior leads to
greater resistancefo r the behavior to change, even when the
reinforcement schedulechanges (P laud & Gaither, 1996; Plaud ,
Gaither, & Lawrence,1997). The aptness of the "momentum"
metaphor ha s been ques-t ioned (Houl ihan & Brandon, 1996),
but our results at least add tothe body of data to which i t seems
applicable.
The maintenance-phase re sul t s ar e encouraging . Cont
ingencymanag e me n t is intended for use in real-world clinical
set t ings, an done of i ts most effective variants is the
escalating-reinforcementprocedure used in the intervention phase
(and in many of our others tud ies)but thi s var iant has the
inherent l imi ta t ion of e scala t ingcost. O ur
maintenance-phase results show that even in patientswho have been
exposed to escalating reinforcement, abstinencecan be at least part
ly sustained by a more modest schedule ofnonescalating
reinforcement ( i .e . , fixed-amount vouchers and take-home
doses). Comparable findings have been reported by Higginset al.
(1994), who successfully followed an escalating schedulewith one in
which each negative urine specimen was reinforcedwith a state
lottery t icket. Nonescalating schedules could havepractical
applications fo r patients w ho return to frequent cocaineuse w h e
n an escala ting cont ingency is d iscont inued .The present study
had a number of l imitat ions. First , there wasno nonvoucher or
noncont ingent -voucher cont rol group wi thwh i ch to compare th e
shaping and abstinence groups. Neverthe-less, patients in both
groups clearly improved with the onset ofcont ingency management ,
an d (wi th du e acknowledgement of thel imitat ions of historical
controls) their improvements appearedgreater than those of
noncontingent-voucher groups in our otherstudies (Silverman et al.,
1996, 1998). Second, patients weremainta ined on re la t ive ly low
m ethadone doses; th e rates of heroinand cocaine use might have
been lower had methadone doses beenhigher or indiv idua lized.
Finally, the overall level of improvemen t
may have been reduced by the delayed delivery of re inforcers
andby the short duration of the intervention. Vouchers were given
1da y after urine specimens were collected because of our use of
anoutside laboratory to obtain qua nti tat ive urine test results.
Delay ofdelivery can weaken the strength of a re inforcer.Overall ,
shaping (by means of re inforcement of decreases inurine-cocaine
metaboli te concentrations) led to more part icipantscontac t ing
th e reinforcer and a greater density of reinforcer deliv-er y per
participant. When a more stringent response requirementwas
introduced, cocaine abstinence was enhanced for part icipantswho
had previously been reinforced on the shaping schedule. W econclude
that this procedure prepared part icipants for
abstinence.Improvements were sustained in a maintenance treatment
provid-ing nonescalating reinforcers that were contingent on
abstinence.
ReferencesAmbre, J . (1985) The urinary excre t ion of coca ine
and metabol i tes in
h um ans : A kinetic analysis of publ ished da ta . Journal of
AnalyticalToxicology, 9, 241-245.
Beck, A. T., & Steer, R. A. (1987) Beck Depression Inventory
manual.New York: The Psychologica l Corpora t ion Harcourt Brace
Jovanovich.Bigelow, G. E., & Silverman, K. (1999). Theoretical
and empirical foun-dations of contingency m anagement t rea tm ents
for drug abuse. In S. T.
Higgins & K. Silverman (Eds.), Motivating behavior change
amongillicit-drug abusers: Contemporary research on
contingency-managementinterventions (pp. 15-31). Sa n Diego, CA :
Academic Press.
Catania, A. C. (1973). The nature of learning. In J. A. Nevin
& G. S.Reynolds (Eds.), Th e study of behavior, learning,
motivation, emotion,an d instinct, (pp. 31-68). G l enview , IL :
Scot, Foresman.Delucchi, K. L., Jones, R. T., & Batki , S. L.
(1997) Measuremen t proper-ties of qua nt i t a t ive u r ine
benzoyl ecgonine in cl inica l t r ia l s research.Addiction, 92,
297-302.
Derogatis , L. R. (1977). SCL-90-R administration, scoring &
proce-dures manual - II for the revised version. Tow s on, MD :
Clinica l Psy-chometr ic Research.Elk, R. , Schmitz, J., Spiga, R.,
Rhoades, H., Andres, R., & Grabowski, J.(1995) Behaviora l t
rea tment of coca ine-dependent pregnant wom en andTB-exposed
patients. Addictive Behaviors, 20, 533-542.
Evans , S. M., L ev in , F. R., Fischman, M. W., & Fol t in,
R. W. (1998).Smoked coca ine se lf-administ rat ion in females and
voucher incentivesfo r abst inence . Journal of Substance Abuse,
10, 143-162.
Hedeker, D. , & Gibbon s , R. D. (1997). Appl ica t io n of
random-effectspat te rn-mixture models fo r miss ing da ta in
longitudina l s tud ies . Psycho-logical Methods, 2, 64-78.Helzer,
J., Croughan, J., Robins, L., & Ratcliff, K. (1981). National
In stitute ofMental Health Diagnostic Interview Schedule: Its
history, characteristics,an d validity. Archives of General
Psychiatry, 38 , 381-389.
Higgins , S. T., Budney, A. J., Bickel, W. K., Foerg, F. E.,
Donham, R., &Badger, G. J. (1994). Incen tives improve outco me
in outpa t ient behav-ioral t rea tment of coca ine dependence.
Archives of General Psychiatry,51, 568-576.Higgins , S. T., Budn
ey, A. J ., Bickel , W. K. , Hughes, J. R., Foerg, F., &Badger,
G . (1993). Achieving coca ine abs t inence with a
behavioralapproach. American Journal of Psychiatry, 150,
763-769.
Higgins , S. T., Delaney, D . D ., B u d n e y , A . J. ,
Bickel, W . K., Hughes, J. R.,Foerg, F., & Fenwick, J. W.
(1991). A behavioral approach to achievinginitial coca ine abs t
inence. American Journal of Psychiatry, 148, 1218-1224.Higgins , S.
T., Stitzer, M. L., Bigelow, G. E., & Liebson, I. A.
(1986).Contingent methadone del ivery: Effects on i l l ic i t-opia
te use. Drug an dAlcohol Dependence, 1 7, 311-322.Houlihan, D.,
& Brandon, P. K. (1996). Compl iant in a moment: A commen-tary
on Nevin. Journal of Applied Behavior Analysis, 2 9, 549-555.
-
7/30/2019 2001, Preston e.t. Shaping Cocaine Abstinence by
Successive Approximations
12/12
654 PRESTON, UMBRICHT, WONG, AND EPSTEINIguchi, M. Y., fielding,
M. A. , Morral, A . R. , Lamb, R. J., & Husband,S. D. (1997).
Reinforcing operants other than abstinence in drug abusetreatment:
An effective alternative fo r reduc ing drug use. Journal of
Consulting an d Clinical Psychology, 6 5, 421-428.Kidorf, M.,
& Stitzer, M. L. (1996). Contingent use of take-homes
andsplit-dosing to reduce i ll icit drug use of methadone patients.
Behavior
Therapy, 2 7, 41-51.Kirby, K. C, Marlowe, D. B., Festinger, D.
S., Lamb, R. J. , & Platt, J. J.(1998). Schedule of voucher
delivery influences initiation of cocaine absti-nence. Journal of
Consulting and Clinical Psychology, 66, 761-767.Kupfer , D . J. ,
Frank, E., Perel, J. M. , Comes, C., Mallinger, A. G., Thase,M. E.,
McEachran, A. B. , & Grochocinski, V. J. (1992). Five-year
outcome for maintenance therapies in recurrent depression.
Archives ofGeneral Psychiatry, 49, 769-773.
Littel , R. C., Millik en, G. A., Stroup, W. W., & W
olfinger, R. D. (1996).SA S system for mixed mo dels. Gary, NC: SAS
Publicat ions.Mace, F. C ., Maur o , B., Boyajian, A. E. , &
Eckert , T. L. (1997). Effects ofre inforce r qual i ty on
behavioral momen tum: Coordinated appl ied an dbasic research.
Journal of Applied Behavior Analysis, 30 , 1-20.McCa ul , M. E.,
Stitzer, M. L. , Bigelow, G. E. , & Liebson, I. A. (1984).Cont
ingency management in tervent ions: Effects on t reatment
outcomedur ing met hadone de toxif icat ion. Journal of Applied
Behavior Analysis,17, 35-43.McLel lan, A. T., Luborsky, L. ,
Cacciola, J. , Griffith, J. , Evans, F., Barr,H. L., & O'Brien,
C. P. (1985). New data from the Addiction SeverityIndex: Reliab i l
i ty an d validity in three centers. Journal of Nervous andMental
Disease, 173,412-423.
Meyer, V. , & Chesser, E. S. (1970). Behavior therapy in
clinical psychi-atry. New York: Science House.
Nevin, J. A. (1992). An in tegrat ive model for the study of
behavioralm o m e n t u m . Journal of Experimental Analysis of
Behavior, 57, 301-316.N e v in , J. A., Mandell, C ., & Atak,
J. R. (1983). The analysis of behavioralm om e n tum . Journal of
the Experimental Analysis of Behavior, 39 ,49-59.
Plaud, J. J. , & Gai ther , G. A. (1996). Human behavioral
momentum:Impl ica t ions for applied behavior analysis an d
therapy. Journal of Be-havior Therapy an d Experimental Psychiatry,
2 7, 139-48.
Plaud, J. J. , Gaither, G. A., & Lawrence, J. B. (1997).
Operant schedulet ransformat ions an d h u m a n behavioral
momentum. Journal of BehaviorTherapy an d Experimental Psychiatry,
2 8, 169-79.Preston, K. L. , Silverman, K. , Schuster, C . R. ,
& Cone, E. J. (1997).Assessment of cocaine us e with quant i ta
t ive ur inalysi s an d estimation ofne w uses. Addiction, 92,
Ill-Ill.
Preston, K. L., Umbricht, A., & Epstein, D. H. (2000).
Methadone doseincrease an d abstinence reinforcement fo r treatment
of continued heroinuse in methadone maintenance patients. Archives
of General Psychiatry,57, 395-404.SAS Insti tute. (1997). The MIXED
procedure. In SAS/STAT Software:
Changes an d enhancements through release 6 . 1 2 . (pp.
571-701). Cary,N C : Author .Saxon, A. J. , Calsyn, D. A., Haver,
V. M. , & Delaney, C. J. (1988). Clinicalevaluation of urine
screening fo r drug abuse. Western Journal of Med-icine, 149,
296-303.Schmitz, J. M., Rhoades, H., & Grabowski, J. (1995).
Contingent rein-forcement for reduced carbon monoxide levels in
methadone mainte-nance patients. Addictive Behaviors, 2 0,
171-179.Silverman, K., Higgins, S. T., Brooner, R. K., Montoya, I.
D., Cone, E. J. ,Schuster, C . R. , & Preston, K. L. (1996).
Sustained cocaine abstinence
in methadon e maintenance patients through voucher-based
reinforce-ment therapy. Archives of General Psychiatry, 53 ,
409-415.Silverman, K. , Wong, C . J., Umbricht-Schneiter, A.,
Montoya, I. D .,Schuster, C. R., & Preston, K. L. (1998). Broad
beneficial effects ofcocaine abstinence reinforcement among
methadone patients. Journal ofConsulting an d Clinical Psychology,
6 6 , 811-824.Stitzer, M. L., & Bigelow, G. E. (1982).
Contingent reinforcement forreduced carbon monoxide levels in
cigarette smokers. Addictive Behav-iors, 7, 403-412.
Stitzer, M. L., & Bigelow, G. E. (1984). Contingent
reinforcement forreduced carbon monoxide reduction: Within-subject
effects of payamount . Journal of Applied Behavior Analysis, 1 7,
477-483.Stitzer, M. L., & Bigelow, G. E. (1985). Contingent
reinforcement forreduced breath carbon monoxide levels:
Target-specific effects on cig-arette smoking. Addictive Behaviors,
1 0, 345-349.Stitzer, M. L., Iguchi, M. Y. , & Felch, L. J.
(1992). Contingent take-homeincentive: Effects on drug use of
methadone maintenance patients.Journal of Consulting an d Clinical
Psychology, 6 0, 927-934.Stitzer, M. L. , Rand , C . S. , Bigelow,
G. E., & Mead, A. M. (1986).Cont ingent payment procedures for
smoking reduction and cessation.Journal of Applied Behavior
Analysis, 1 9, 197-202.Zachary, R. A. (1986). Shipley Institute of
Living Scale. Revised Manual.Lo s Angeles: Western Psychological
Services.
Received Ma y 1, 2000Revision received September 26, 2000
Accepted October 8, 2000
ORDER FORMStart my2001 subscription toJournal of Consultingand
Clinical Psychology! ISSN: 0022-006X
$92.00, APA Member/Affiliate$183.00, Individual
Non-Member$408.00, InstitutionIn DC add 5.75% sales laxT O T A L A
M O U N T E N C L O S E D $
Subscription orders mu st be prepaid. (Subscriptions are ona
calendar basis on ly.) Allow 4-6 weeks for delivery of thefirst
issue. Call fo r international subscription
rates.SENDTHISORDERFORMTO:American Psychological
AssociationSubscriptions750 First Street, NEWashington, DC
20002-4242Or call (800) 374-2721, fax (202) 336-5568.TDD/TTY
(202)336-6123. Email: [email protected]
Send me a Free Sample Issue QQCheck Enclosed (make payable to
APA)Chargemy: QVISA QMastaCand QAmericanExpressCardholder NameCard
No. Exp. date
Signature (Required for Charge)Credit CardBilling AddressCity
State Zip _Daytime PhoneSHIP TO:NameAddressCity . State. .Zip.APA
Customer #
GADO lPLEASE DO NOTREMOVE - A PHOTOCOPY MAYBEUSED