Embed Size (px)
Citation preview

11Clinical Lung Cancer July 2004
meeting highlights
40th Annual Meeting of the American Society of Clinical Oncology
New Orleans, LouisianaJune 2004
2004Highlights From:
Intertrial ComparisonSuggests PharmacogenomicsMay Affect Outcome
The results of clinical trials performedin one region of the world may not trans-late directly to another region. A varietyof factors could account for these discrep-ancies, one of which may be that geneticdifferences between ethnic populations af-fect pharmacodynamics. For example, itis established that individuals with differ-ent allelotypes of cytochrome P450 en-zymes metabolize drugs differently andthis certainly affects outcome.1
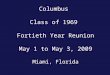
The Southwest Oncology Group(SWOG) and the Japan Multi-CenterTrial Organization (JMTO) conductedan analysis of the efficacy and toxicity inpatients with advanced non–small-celllung cancer (NSCLC) treated on the pa-clitaxel/carboplatin arm of the SWOG0003 trial conducted in the United Statesand the four-arm cooperative study(FACS) sponsored by JMTO and con-ducted in Japan (Figure 1). The trials hadidentical eligibility, treatment regimens,
response, and toxicity criteria so thatpharmacogenomic and demographic dif-ferences could be directly compared. The
comparative analysis of the same regimenfrom both trials was presented by Gan-dara and colleagues at the 40th Annual
Prepared by: Nancy Price, PhD, G. Kesava Reddy, PhDReviewed by: Chandra P. Belani, MD
Electronic forwarding or copying is a violation of US and International Copyright Laws.Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted by Cancer Information Group, ISSN #1525-7304, provided the appropriate fee is paid directly to Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923 USA 978-750-8400.
Figure 1. Comparison of JMTO FACS and SWOG 0003 Trials
Cisplatin 80 mg/m2 on day 1Gemcitabine 1 g/m2 days 1 and 8
every 3 weeks
Cisplatin 80 mg/m2 on day 1Irinotecan 60 mg/m2
weekly for 3 weeks every 4 weeks
Cisplatin 80 mg/m2 on day 1Vinorelbine 25 mg/m2
on days 1 and 8 every 3 weeks
Carboplatin AUC of 6 on day 1 Paclitaxel 200 mg/m2 on day 1
every 3 weeks
Abbreviation: AUC = area under the curve; JMTO FACS = Japan Multi-Center Trial Organizationfour-arm cooperative study; NSCLC = non–small-cell lung cancer; PS = performance status; SWOG = Southwest Oncology Group
Carboplatin AUC of 6 on day 1 Paclitaxel 225 mg/m2 on day 1
every 3 weeks
Carboplatin AUC of 6 on day 1 Paclitaxel 225 mg/m2
every 3 weeks Tirapazamine I.V. over 2 hours
Histologically and/or cytologically documented clinical stage IIIB/IV NSCLC, PS of 0/1, measurable disease, adequate organ function, no prior chemotherapy, no other type of malignancy
R A N D O M IZ E
JAPAN TRIAL
US TRIAL

12 Clinical Lung Cancer July 2004
Meeting of the American Society of Clin-ical Oncology (ASCO) in June 2004.2
Six hundred two patients were accruedto the FACS trial between October 2000and June 2002. The SWOG trial was ac-tivated in November of 2000 and closedin November of 2002. In both trials, pa-tients had stage IIIB/IV NSCLC, a per-formance status of 0/1, measurable dis-ease, and adequate organ function. In theJMTO FACS trial, carboplatin was givenat an area under the curve of 6 with pa-clitaxel 200 mg/m2 on day 1 every 3weeks, wherease in the SWOG trial, car-boplatin was administered at the samedose but the paclitaxel dose was higher, at225 mg/m2. One hundred eighty-six pa-tients were enrolled in the paclitaxel/car-boplatin arm of the SWOG trial, and 145were enrolled in the paclitaxel/carbo-platin arm of the JMTO trial. The pa-
tient characteristics in both trials werecomparable, and the median age was 63years. In the JMTO and SWOG trials, re-spectively, 32% and 37% of patients werewomen, 81% and 87% had stage IV dis-ease, and 79% and 82% had squamoushistology.
Despite the lower dose of paclitaxel(200 mg/m2 vs. 225 mg/m2), more grade3/4 hematologic toxicities were seen inJapanese patients than in American pa-tients (Table 1). Grade 3/4 neutropeniaoccurred in 70% of Japanese patientscompared with 26% of American pa-tients, and febrile neutropenia occurredin 18% of Japanese patients comparedwith 3% of American patients. MoreJapanese patients than American patientsmissed treatment cycles and had dose re-ductions (Table 2). Conversely, there wasa lower incidence of neuropathy in Japan-ese patients.
Although the response rates to paclitax-el/carboplatin were similar in bothgroups, the median survival (12 monthsvs. 9 months) and 1-year survival rates(51% vs. 37%, P = 0.009; Table 3) weresignificantly greater in the Japanese group.
Clinical RelevanceThe analysis of patients from the 2 tri-als implies that differences in ethnicityand pharmacogenomics are signifi-cant factors in the efficacy and toxicityof chemotherapy regimens. The differ-ent outcomes between the Japaneseand American patients underscore theimportance of increased internationalcollaboration in trial design.
Erlotinib Fails to ImproveOutcomes When Combinedwith Carboplatin/Paclitaxel or Gemcitabine/Cisplatin inNon–Small-Cell Lung Cancer
Although the Iressa® NSCLC Trial As-sessing Clinical Treatment (INTACT) 1 and2 trials showed no survival advantage whengefitinib is added to standard platinum-based chemotherapy versus chemotherapyalone in patients with NSCLC, a subsetanalysis (INTACT 2) of patients with ade-nocarcinoma who received therapy for > 90days demonstrated statistically significantprolonged survival, suggesting a gefitinib ef-fect.3,4 Moreover, subsequent analysis ofsubsets indicated that the patients with acti-vating mutations in the EGFR are highlysensitive to gefitinib therapy.5,6
Erlotinib (Tarceva™, OSI 774) is struc-turally related to gefitinib and has a similarspectrum of clinical efficacy, toxicity, andsafety profiles, with skin rash and diarrheaas dose-limiting toxicities in advancedNSCLC.7 To evaluate the addition of er-lotinib to carboplatin/paclitaxel and gemci-tabine/cisplatin chemotherapy regimens, 2prospective randomized phase III trials(TRIBUTE and TALENT) were per-formed in patients with previously untreat-ed advanced NSCLC (stage IIIB/IV).8,9
Unlike the INTACT 1 and INTACT 2trials, in which gefitinib was terminated
Table 1: Paclitaxel/Carboplatin Toxicity Comparison Between SWOG 0003 and JMTO FACS
Grade3/4
AdverseEvent
Neutropenia
Febrile Neutropenia
Neuropathy
Anemia
48 (26%)
6 (3%)
30 (16%)
12 (6.5%)
SWOG0003
(N = 186)
JMTO FACS
(N = 145)P Value
102 (70%)
26 (18%)
5 (3%)
22 (15%)
< 0.0001
< 0.0001
0.001
0.010
Abbreviations: JMTO FACS = Japan Multi-Center Trial Organization four-arm cooperative study;SWOG = Southwest Oncology Group
Table 2: Paclitaxel/Carboplatin Delivery Comparison Between SWOG 0003 and JMTO FACS
Dose Reductions
6 Cycles Received
> 3 Cycles Received
Median Number of Delivered Cycles
26%
68 (36.5%)
100 (54%)
4
SWOG0003
(N = 186)
JMTOFACS
(N = 145)P Value
Pending
16 (11%)
35 (24%)
3
–
< 0.0001
< 0.0001
–
Abbreviations: JMTO FACS= Japan Multi-Center Trial Organization four-arm cooperative study; SWOG = Southwest Oncology Group
Table 3: Efficacy Comparison Between SWOG 0003 and JMTO FACS
ResponseRate
CompleteResponse
PartialResponse
Progression-Free Survival
1-YearSurvival
62 (34%)
3 (1.6%)
59 (32.4%)
4 Months
37%
SWOG0003
(N = 182)
JMTOFACS
(N = 145)P Value
47 (32%)
1 (0.7%)
46 (31.7%)
4.5 Months
51%
0.75
0.27
0.89
–
0.009
Abbreviations: JMTO FACS= Japan Multi-Center Trial Organization four-arm cooperative study;SWOG = Southwest Oncology Group
Figure 2: TRIBUTE/TALENT Study Design
ErlotinibArm*
(150 mg daily)
PlaceboArm†
HER1/EGFR–positive or negative, stage IIIB/IV NSCLC
*The TRIBUTE trial evaluated carboplatin/paclitaxel chemotherapy with concurrent and continued erlotinib and the TALENT trial evaluated cisplatin/gemcitabine chemotherapy with concurrent and continued erlotinib.†In the TRIBUTE trial, the placebo arm was treated with placebo plus 6 cycles of carboplatin/paclitaxel chemotherapy and continued placebo, and in the TALENT trial, the placebo arm was treated with placebo plus 6 cycles of cisplatin/gemcitabine chemotherapy and continued placebo.Abbreviations: EGFR = epidermal growth factor receptor; NSCLC = non–small-cell lung cancer
RANDOMIZE

13Clinical Lung Cancer July 2004
after chemotherapy, in the TRIBUTE andTALENT studies, erlotinib was startedconcurrently with chemotherapy and con-tinued after completion of chemotherapy.The findings of these studies were pre-sented at the Annual Meeting of ASCO in2004. The results of these studies are dis-cussed herein.
In the TRIBUTE study, patients withpreviously untreated stage IIIB/IVNSCLC were randomized to 6 cycles ofcarboplatin/paclitaxel chemotherapy with(1) erlotinib (150 mg orally per day) fol-lowed by maintenance erlotinib or (2)placebo (Figure 2).8 The primary end-point of the study was overall survival.The secondary endpoints of the studywere time to progression, objective re-sponse rate, duration of response, time tosymptomatic progression, and safety.
A total of 1079 patients with stageIII/IV NSCLC were enrolled. The armswere well balanced for age, sex, diseasestage, and histology (Table 4).
The addition of erlotinib to paclitax-el/carboplatin chemotherapy did not im-prove the overall survival. Erlotinib com-bined with paclitaxel/carboplatin had no
effect on objective response rate (21.5%for the patients receiving erlotinib com-pared with 19.3% for patients receivingplacebo). No significant difference wasseen in the median duration of response(5.5 months for the erlotinib arm and 5.0months for the placebo arm; P = 0.32).Time to progression remained unchangedwith the addition of erlotinib to paclitax-el and carboplatin chemotherapy (5.1months for the erlotinib arm and 4.9months for the placebo arm; P = 0.36).The median survival in erlotinib-treatedpatients was 10.6 months, comparedwith 10.5 months for patients in theplacebo group, with a hazard ratio (HR)of 0.995, (P = 0.95; Table 5). Adverseevents attributed to erlotinib includedrash and diarrhea.
However, a retrospective subset analysisshowed that erlotinib prolonged survival inpatients who were in the category of never-smokers (median survival of 23 monthsfor never-smokers vs. 10 months for smok-ers; HR, 0.49; 95% CI, 0.28-0.85).10
The TALENT trial studied the benefitof adding erlotinib to gemcitabine/cispla-tin in patients with advanced NSCLC.9 A
total of 1172 patients were enrolled from164 sites worldwide. In the erlotinib arm,533 patients had evaluable disease, as did536 patients in the placebo arm. The de-mographic and disease characteristicswere well balanced between the 2 treat-ment groups (Table 4).
Erlotinib did not improve the objectiveresponse rate when added to gemcita-bine/cisplatin (complete response, 1.5% vs.1.7%; partial response, 30% vs. 28.2%).Overall survival (9.9 months in the er-lotinib arm vs. 10.1 months in the placeboarm), 1-year survival rate (41% in the er-lotinib arm vs. 42% in the placebo arm),and median time to progression (5.4months in the erlotinib arm vs. 5.6 monthsin the placebo arm) were not improved bythe addition of erlotinib to gemcitabine/cisplatin chemotherapy (Table 5).
Clinical RelevanceThe TALENT and TRIBUTE trials failedto show a benefit when erlotinib wasadded to chemotherapy in patientswith NSCLC. Interestingly, in thesmall subset of patients who hadnever smoked, the addition of er-lotinib did confer a survival advan-tage. Presence of the EGFR mutationhas been found to be a key predictorof response to gefitinib. Analysis ofEGFR mutations may identify a subsetof patients who may derive a survivaladvantage with erlotinib when addedto chemotherapy. Subgroup analysesare currently ongoing to identify pre-dictive markers of response and clin-ical benefit. It will also be of interestto analyze the available blocks forpresence of EGFR mutations.
Activity of Cetuximab in Patientswith Recurrent Non–Small-CellLung Cancer
Inhibition of EGFR by small-moleculetyrosine kinase inhibitors like gefitinib anderlotinib has resulted in tumor shrinkageand response rates of 10%-19% in patientswith relapsed/refractory NSCLC.11-13
Cetuximab is a chimeric monoclonalantibody that binds to the extracellulardomain of EGFR and blocks ligandbinding, producing cell cycle arrest and
Table 4: Characteristics of Patients in TRIBUTE and TALENT Trials8,9
Dose
TALENT StudyTRIBUTE Study
Median Age
Stage IV Disease
Tumor Histology
Adenocarcinoma
Squamous cell
Prior Radiation Therapy
Prior Surgery
Erlotinib Arm(n = 539)
Placebo Arm(n = 540)
Erlotinib Arm (n = 533)
Placebo Arm(n = 536)
62.7 Years
84%
60%
18%
22%
36%
62.6 Years
82%
61%
16%
22%
37%
60.0 Years
65%
38%
41%
13%
22%
59.1 Years
67%
38%
41%
11%
24%
Table 5: Patient Survival in Response to Erlotinib Treatment in the TRIBUTE and TALENT Trials
Response
TALENT StudyTRIBUTE Study
Overall Survival
Time to Progression
One-Year Survival Rate
Objective Response Rate
Erlotinib Arm(n = 539)
Placebo Arm(n = 540)
Erlotinib Arm (n = 533)
Placebo Arm(n = 536)
10.6 Months
5.1 Months
46.9%
21.5%
10.5 Months
4.9 Months
43.8%
19.3%
9.9 Months
5.4 Months
41%
31.5%
10.1 Months
5.6 Months
42%
29.9%

14 Clinical Lung Cancer July 2004
inhibition of tumor cell growth.14,15
Phase I trials have established the opti-mal biologic dose of cetuximab to be200-400 mg/m2. Within this range, ce-tuximab downregulates EGFR and in-hibits downstream signaling. The pri-mary toxicity with cetuximab treatmentis acneiform rash and allergic reactions.16
A current phase II study by Lynch andcolleagues evaluates single-agent activityof cetuximab in patients with NSCLCthat fails to respond to platinum-basedtherapy.17 Interim results of the studywere presented at the Annual Meeting ofASCO in 2004.
Patients with EGFR-positive or EGFR-negative stage IIIB/IV NSCLC who haverecurrent or metastatic disease after ≥ 1chemotherapy regimen including plat-
inum-based therapy are eligible for thestudy. Eligible patients are required tohave a performance status of 0/1. Patientsreceived an initial cetuximab dose of 400mg/m2 on day 1 of cycle 1 (4-week cycle),followed by weekly cetuximab doses of250 mg/m2. Weekly treatment with ce-tuximab was continued until disease pro-gression or unacceptable toxicity.
The primary endpoint of the study wasresponse rate to cetuximab therapy. A re-sponse rate was determined for pagtientswith EGFR-positive disease, those withEGFR-negative disease, and the totalstudy population. The secondary end-points of the study were time to progres-sion, overall survival, and safety.
At the time of interim analysis, a totalof 49 patients (EGFR positive, n = 43;EGFR negative, n = 6) had recurrent stageIII/IV NSCLC. The baseline characteris-tics of the patients are shown in Table 6.
A total of 33 patients were evaluable fortreatment response. Of the 33 evaluablepatients, 2 patients (6%) had partial re-sponse, 7 patients (21%) had stable dis-ease (Table 7), and 24 patients had pro-gressive disease (73%). There was no evi-dence of EGFR mutations in the 2 re-sponding patients. Of the 2 other patientsin whom EGFR mutations were detected,1 had stable disease and the other had dis-ease progression on cetuximab.
The primary toxicity seen with cetux-imab therapy is an acneiform rash (grade3, 4.1%), similar to that seen with thesmall-molecule EGFR tyrosine kinase in-hibitors erlotinib and gefinitib. Othergrade 3 toxicities are asthenia/malaise(12.2%) and diarrhea (2%). Grade 4 nau-sea/vomiting occurred in 1 patient (2%).
Clinical RelevanceEpidermal growth factor receptor inhibi-tion by cetuximab results in a responserate of 6% in patients with recurrentNSCLC. Cetuximab has single-agentactivity in advanced and recurrentNSCLC. Preliminary analysis suggeststhat, in contrast to erlotinib andgefinitib, tumor mutations in the EGFRdo not appear to be a factor in cetux-imab response. It is conceivable that dif-ferent subsets of patients with lung can-cer may benefit from small-moleculeEGFR tyrosine kinase inhibitors versusEGFR-targeted monoclonal antibodies.
Panitumumab (ABX-EGF), aFully Human Anti-EGFR Antibody,Combined with Paclitaxel/Carboplatin for AdvancedNon–Small-Cell Lung Cancer
Members of the EGFR family are fre-quently overexpressed in NSCLC and othermalignancies.18 Overexpression of EGFR islinked to poor clinical outcome in NSCLC.Hypothetically, this could be attributable toEGFR signaling, which promotes cell sur-vival, angiogenesis, and proliferation.19
Recognition of the tumor-promotingproperties of EGFR has encouraged de-velopment of new targeted therapies de-signed to disrupt EGFR function. Mono-clonal antibodies such as cetuximab andpanitumumab (ABX-EGF) and thesmall-molecule tyrosine kinase inhibitorsgefitinib and erlotinib are examples ofEGFR-targeted agents. Monoclonal anti-bodies target the extracellular domain ofthe EGFR to block ligand interaction,whereas small-molecule tyrosine kinaseinhibitors work intracellularly.
Gefitinib and erlotinib have single-agent activity in recurrent NSCLC20,21
and gefitinib sometimes produces remark-able responses in patients with EGFR mu-tations.22,23 However, these agents havefailed to improve overall efficacy whenadded to chemotherapy combinations inrandomized phase III trials.3,4,8,9
In contrast, cetuximab has demonstrat-ed synergistic activity when combinedwith irinotecan for advanced colorectalcancer and was recently approved by theUS Food and Drug Administration forthe treatment of irinotecan-resistant col-orectal carcinoma.24 Cetuximab also ap-peared to improve response rates in a ran-domized phase II study when combinedwith vinorelbine/cisplatin chemotherapyfor the first-line treatment of advancedand metastatic NSCLC.25
Panitumumab is a fully human anti-body against the EGFR produced in thegenetically engineered XenoMouse sys-tem.26 Panitumumab is specific for, andhas high affinity with, the EGFR. In vitrostudies show that panitumumab blocksligand binding, prevents EGFR-mediatedtyrosine kinase activity, and causes recep-
Table 6: Characteristics of Patients with Recurrent NSCLC
Dose
Total Number of Patients
Median Age
Disease Stage
III
IV
Tumor Histology
Adenocarcinoma
Squamous cell
Prior Chemotherapy Regimens
1
2
3
> 3
EGFR-PositiveDisease
EGFR-NegativeDisease
43
64 Years
7 (16.3%)
36 (83.7%)
21 (48.8%)
7 (16.3%)
17 (39.5%)
20 (46.5%)
6 (14.0%)
0
6
62 Years
2 (33.3%)
4 (66.7%)
4 (66.7%)
1 (16.7%)
3 (50%)
1 (16.7%)
1 (16.7%)
1 (16.7%)
Abbreviations: EGFR = epidermal growth factor receptor; NSCLC = non–small-cell lung cancer
Table 7: Response to Cetuximab in Patients with Recurrent NSCLC
Dose
Complete Response
Partial Response
Stable Disease
Overall Response
Evaluable Patients(n = 33)
0
2 (6%)
7 (21%)
2 (6%)
Abbreviation: NSCLC = non–small-cell lung cancer

15Clinical Lung Cancer July 2004
tor internalization.27 Antitumor activityof panitumumab was demonstrated inanimal xenograft models. At the 2004Annual Meeting of ASCO, Crawford andcolleagues reported the results from part1 of a phase II study of panitumumabcombined with carboplatin/paclitaxel inpatients with advanced NSCLC.28
The trial is an open-label, 2-part studyfor patients with stage IIIB/IV NSCLCand demonstrable EGFR expression.During the dose-escalation phase, panitu-mumab was administered at varying dosesof 1, 2, or 2.5 mg/kg per week in combi-nation with paclitaxel 200 mg/m2 andcarboplatin at an area under the curve of6, given every 3 weeks. Part 2 of the trialwas designed to compare time to diseaseprogression and regimen efficacy, as wellas safety and quality of life. Part 1 of thetrial is summarized herein.
Eligible patients had histologically con-firmed stage IIIB NSCLC with pericardialor pleural effusion or stage IV NSCLC,EGFR-staining intensities of 2+ to 3+ onimmunohistochemistry (IHC) in ≥ 10%of tumor cells, and bidimensionally meas-urable disease. Patients with controlledand asymptomatic brain metastases whohad not received steroid therapy for ≥ 1week were permitted in the trial.
In the first part of the trial, a total of19 patients were enrolled in the 3 co-horts to determine the dose, safety, and
pharmacokinetics of the combinationregimen. One hundred seventy-five pa-tients have been enrolled in the secondpart of the trial, and these results will beavailable at a later date.
Six patients received panitumumab 1mg/kg, 7 received 2 mg/kg, and 6 received2.5 mg/kg. The treatment was well toler-ated, and the addition of panitumumab topaclitaxel/carboplatin chemotherapy didnot appear to worsen tolerability.
Grade 4 toxicities were limited to 1 pa-tient with neutropenia. Grade 3 toxicitiesincluded 1 patient each with neutropeniaand fatigue and 2 with grade 3 parony-chia. As is common with anti-EGFR ther-apies, panitumumab treatment was associ-ated with a skin rash in a majority of pa-tients. Skin rashes were mostly mild tomoderate, with 3 patients developing agrade 3 rash (Table 8). Because panitu-mumab is a fully human antibody, infu-sion-related hypersensitivity reactionswere not seen except for 1 patient who de-veloped urticaria. Human anti-human an-tibodies were not noted in any of thetreated patients.
The pharmacokinetics of panitumum-ab are dose-dependent and saturationlevels of serum panitumumab were ob-served at the highest dose level studied.Panitumumab did not interact with oraffect the pharmacokinetics or serum lev-els of paclitaxel.
Efficacy data in this cohort of 19 patientsare still immature. At 6 weeks, all but 2 pa-tients at each dose level had stable disease.Four of 11 patients who responded at anypoint in time had 3+ EGFR staining inten-sities on IHC and 1 patient had IHC 2+staining. All 5 patients with a response atany time had a skin rash. The median sur-vival is 17 months.
Clinical RelavancePanitumumab can be safely combinedwith paclitaxel/carboplatin at dosesup to 2.5 mg/kg in patients withNSCLC. Pharmacokinetic interactionsbetween paclitaxel and panitumumabwere not observed. The median sur-vival results are provocative. The sec-ond part of the study has completedenrollment (n = 175) and will providea better sense of the efficacy of pani-tumumab 2.5 mg/kg weekly com-bined with paclitaxel/carboplatincompared with paclitaxel/carboplatinalone (Figure 3).
Table 8: Toxicities of Panitumumab Combined with Paclitaxel/Carboplatin
PanitumumabDose
Fatigue Neutropenia Paronychia RashDyspepsia
1.0 mg/kg(n = 6)
2.0 mg/kg(n = 7)
2.5 mg/kg(n = 6)
0
1
0
0
0
0
0
2
0
0
0
0
0
0
0
1
2
0
Grade3
Grade4
Grade3
Grade4
Grade3
Grade4
Grade3
Grade4
Grade3
Grade4
0
1
0
0
0
0
0
0
1
0
0
1
Figure 3: Part 2 of the Randomized Phase II Trial of Panitumumab with Paclitaxel/Carboplatin in Advanced NSCLC
Abbreviations: AUC = area under the curve; NSCLC = non–small-cell lung cancer
Paclitaxel 200 mg/m2 I.V.
over 3 hoursCarboplatin
AUC of 6 every 3 weeks
Panitumumab2.5 mg/kg I.V.
every week
Paclitaxel 200 mg/m2 I.V.
over 3 hoursCarboplatin
AUC of 6 every 3 weeks
RANDOMIZE
Stage IIIB/IV NSCLC(N = 175)
References1. Kaiser R, Sezer O, Papies A, et al. Patient-tailored
antiemetic treatment with 5-hydroxytryptamine type3 receptor antagonists according to cytochrome P-450 2D6 genotypes. J Clin Oncol 2002; 20:2805-2811.
2. Gandara DR, Ohe Y, Kubota K, et al. Japan-SWOGcommon arm analysis of paclitaxel/carboplatin in ad-
vanced stage non-small cell lung cancer (NSCLC): amodel for prospective comparison of cooperativegroup trials. Proc Am Soc Clin Oncol 2004; 23:616(Abstract #7007).
3. Giaccone G, Herbst RS, Manegold C, et al. Gefitinibin combination with gemcitabine and cisplatin in ad-vanced non-small-cell lung cancer: a phase III trial--
INTACT 1. J Clin Oncol 2004; 22:777-784.4. Herbst RS, Giaccone G, Schiller JH, et al. Gefitinib
in combination with paclitaxel and carboplatin inadvanced non-small-cell lung cancer: a phase IIItrial--INTACT 2. J Clin Oncol 2004; 22:785-794.
5. Lynch TJ, Bell DW, Sordella R, et al. Activating mu-tations in the epidermal growth factor receptor un-

16 Clinical Lung Cancer July 2004
derlying responsiveness of non-small-cell lung cancerto gefitinib. N Engl J Med 2004; 350:2129-2139.
6. Paez JG, Janne PA, Lee JC, et al. EGFR mutations inlung cancer: correlation with clinical response togefitinib therapy. Science 2004; 304:1497-1500.
7. Perez-Soler R. The role of erlotinib (Tarceva, OSI774) in the treatment of non-small cell lung cancer.Clin Cancer Res 2004; 10:4238s-4240s.
8. Herbst RS, Prager D, Hermann R, et al. TRIBUTE- A phase III trial of erlotinib HCl (OSI-774) com-bined with carboplatin and paclitaxel (CP) chemo-therapy in advanced non-small cell lung cancer(NSCLC). Proc Am Soc Clin Oncol 2004; 23:617(Abstract #7011).
9. Gatzemeier U, Pluzanska A, Szczesna A, et al. Resultsof a phase III trial of erlotinib (OSI-774) combinedwith cisplatin and gemcitabine (GC) chemotherapy inadvanced non-small cell lung cancer (NSCLC). ProcAm Soc Clin Oncol 2004; 23:617 (Abstract #7010).
10. Miller VA, Herbst R, Prager D, et al. Long survivalof never smoking non-small cell lung cancer(NSCLC) patients (pts) treated with erlotinib HCl(OSI-774) and chemotherapy: Sub-group analysis ofTRIBUTE. Proc Am Soc Clin Oncol 2003; 24: 628(Abstract #7061).
11. Fukuoka M, Yano S, Giaccone G, et al. Multi-insti-tutional randomized phase II trial of gefitinib forpreviously treated patients with advanced non-small-cell lung cancer. J Clin Oncol 2003; 21:2237-2246.
12. Kris MG, Natale RB, Herbst RS, et al. Efficacy ofgefitinib, an inhibitor of the epidermal growth factorreceptor tyrosine kinase, in symptomatic patientswith non-small cell lung cancer: a randomized trial.JAMA 2003; 290:2149-2158.
13. Perez-Soler R, Chachoua A, Huberman M, et al. A
phase II trial of the epidermal growth factor receptor(EGFR) tyrosine kinase inhibitor OSI-774, follow-ing platinum-based chemotherapy, in patients (pts)with advanced, EGFR-expressing, non-small celllung cancer (NSCLC). Proc Am Soc Clin Oncol2001; 20:310a (Abstract #1235).
14. Kies MS, Harari PM. Cetuximab (Imclone/Merck/Bristol-Myers Squibb). Curr Opin Investig Drugs2002; 3:1092-1100.
15. Herbst RS, Langer CJ. Epidermal growth factor re-ceptors as a target for cancer treatment: the emergingrole of IMC-C225 in the treatment of lung and headand neck cancers. Semin Oncol 2002; 29:27-36.
16. Baselga J, Pfister D, Cooper MR, et al. Phase I stud-ies of anti-epidermal growth factor receptor chimericantibody C225 alone and in combination with cis-platin. J Clin Oncol 2000; 18:904-914.
17. Lynch TJ, Lilenbaum R, Bonomi P, et al. A phase IItrial of cetuximab as therapy for recurrent non-smallcell lung cancer (NSCLC). Proc Am Soc Clin Oncol2004; 23:634 (Absract #7084).
18. Bunn PA Jr, Franklin W. Epidermal growth factor re-ceptor expression, signal pathway, and inhibitors innon-small cell lung cancer. Semin Oncol 2002;29:38-44.
19. Arteaga CL. Overview of epidermal growth factor re-ceptor biology and its role as a therapeutic target inhuman neoplasia. Semin Oncol 2002; 29:3-9.
20. Nakagawa K, Tamura T, Negoro S, et al. Phase Ipharmacokinetic trial of the selective oral epidermalgrowth factor receptor tyrosine kinase inhibitor gefi-tinib (“Iressa”, ZD1839) in Japanese patients withsolid malignant tumors. Ann Oncol 2003; 14:922-930.
21. Kris MG, Natale RB, Herbst RS, et al. Efficacy of
gefitinib, an inhibitor of the epidermal growth factorreceptor tyrosine kinase, in symptomatic patientswith non-small cell lung cancer: a randomized trial.JAMA 2003; 290:2149-2158.
22. Lynch TJ, Bell DW, Sordella R, et al. Activating mu-tations in the epidermal growth factor receptor un-derlying responsiveness of non-small-cell lung cancerto gefitinib. N Engl J Med 2004; 350:2129-2139.
23. Paez JG, Janne PA, Lee JC, et al. EGFR mutations inlung cancer: correlation with clinical response togefitinib therapy. Science 2004; 304:1497-1500.
24. Saltz LB, Meropol NJ, Loehrer PJ Sr., et al. Phase IItrial of cetuximab in patients with refractory colorec-tal cancer that expresses the epidermal growth factorreceptor. J Clin Oncol 2004; 22:1201-1208.
25. Rosell R, Daniel C, Ramlau R, et al. Randomizedphase II study of cetuximab in combination with cis-platin (C) and vinorelbine (V) vs. CV alone in thefirst-line treatment of patients (pts) with epidermalgrowth factor receptor (EGFR)-expressing advancednon-small-cell lung cancer (NSCLC). Proc Am SocClin Oncol 2004; 23: 618 (Abstract #7012).
26. Yang XD, Jia XC, Corvalan JR, et al. Developmentof ABX-EGF, a fully human anti-EGF receptor mon-oclonal antibody, for cancer therapy. Crit Rev OncolHematol 2001; 38:17-23.
27. Lynch DH, Yang XD. Therapeutic potential of ABX-EGF: a fully human anti-epidermal growth factor re-ceptor monoclonal antibody for cancer treatment.Semin Oncol 2002; 29:47-50.
28. Crawford J, Sandler AB, Hammond LA, et al. ABX-EGF in combination with paclitaxel and carboplatinfor advanced non-small cell lung cancer (NSCLC).Proc Am Soc Clin Oncol 2004; 23:634 (Abstract#7083).
References (continued)