Embed Size (px)
Citation preview

©2005 McGraw-Hill Ryerson Ltd.
Chapter 4
Prenatal Development and Birth

©2005 McGraw-Hill Ryerson Ltd.
Prenatal Development
and Birth
Prenatal
DevelopmentBirth
The Postpartum
Period

©2005 McGraw-Hill Ryerson Ltd.
Prenatal Development

©2005 McGraw-Hill Ryerson Ltd.
The Course of Prenatal Development
• The Germinal Period• The Embryonic
Period• The Fetal Period

©2005 McGraw-Hill Ryerson Ltd.
The Germinal Period
• It is the period that occurs the first 2 weeks after conception.
• By about 1 week after conception, the zygote is composed of 100 to 150 cells.
• This period includes the creation of the zygote, continued cell division, an attachment of the zygote to the uterine wall.
• Implantation, or attachment to the uterine wall, occurs about 10 days after conception.

©2005 McGraw-Hill Ryerson Ltd.
The Differentiation of Cells
• The Blastocyst – the inner layer of cells that develops during the germinal period and later becomes the embryo
• The Trophoblast – the outer layer of the cells that develops during the germinal period and later provides nutrition and support for the embryo

©2005 McGraw-Hill Ryerson Ltd.
The Embryonic Period
• The period that occurs from 2 to 8 weeks after conception
• The rate of cell differentiation intensifies, support systems for the cells form, and organs appear
• The name of the mass of cells now changes from zygote to embryo

©2005 McGraw-Hill Ryerson Ltd.
Cell Layers of the Embryo
• Endoderm – inner layer; develops into the digestive and respiratory systems
• Ectoderm – outermost layer; becomes the nervous system, sensory receptors (ears, nose, eyes), and skin parts (hair and nails)
• Mesoderm – middle layer; becomes the circulatory system, bones, muscles, excretory system, and reproductive system

©2005 McGraw-Hill Ryerson Ltd.
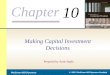
Prenatal Life-Support Systems
• The Placenta – consists of a disk-shaped group of tissues in which small blood vessels from the mother of the offspring intertwine but do not join– Very small molecules (oxygen, water, salt, food from
mother’s blood, carbon dioxide) pass back and for the between mother and infant
• The Umbilical Cord – contains two arteries and one vein and connects the baby to the placenta
• The Amnion – a bag or envelope that contains a clear fluid in which the developing embryo floats

©2005 McGraw-Hill Ryerson Ltd.

©2005 McGraw-Hill Ryerson Ltd.
Important Embryonic Developments
• Third Week – neural tube develops• 21 days – eyes begin to appear• 24 days – heart cells begin to differentiate• Fourth Week – first appearance of the urogenital
system, arm and leg buds appear, chambers of the heart take shape, blood vessels surface
• Fifth to Eight Week – arms and legs differentiate further, face starts to form, intestinal track develops, facial structures fuse
• 8 Weeks – organisms weighs 1/30 ounce and is 1 inch long

©2005 McGraw-Hill Ryerson Ltd.
Definition of Organogenesis• The process of organ formation that takes
place during the first 2 months of prenatal development

©2005 McGraw-Hill Ryerson Ltd.
The Fetal Period
• The period begins 2 months after conception and lasts, on average, 7 months
• Significant time period:– Three months after conception– The end of the fourth month– The end of the fifth month– The end of the sixth month– The end of the seventh month– The eighth and ninth months

©2005 McGraw-Hill Ryerson Ltd.
The End of the Fourth Month
• The fetus is 6 in. long and weighs 4–7 oz.
• A growth spurt occurs in the body’s lower parts
• Prenatal reflexes are stronger
• Arm and leg movements can be felt by the mother for the first time

©2005 McGraw-Hill Ryerson Ltd.
The End of the Fifth Month
• The fetus is 12 in. long and weighs close to 1 lb.
• Structures of the skin have formed (such as toe and fingernails)
• The fetus is more active and shows a preference for a particular position in the womb

©2005 McGraw-Hill Ryerson Ltd.
The End of the Sixth Month
• The fetus is approximately 14 in. long and weighs about 2 lbs.
• The eyes and eyelids are completely formed
• A fine layer of hair covers the head
• A grasping reflex is present
• Irregular breathing movements occur

©2005 McGraw-Hill Ryerson Ltd.
The End of the Seventh Month
• The fetus is 16 in. long and weighs 3 lbs.
• The fetus is adding body fat
• The fetus is very active
• Basic breathing begins

©2005 McGraw-Hill Ryerson Ltd.
The Eighth and Ninth Months
• The fetus grows longer and gains substantial weight, about another 4 lbs.
• Fatty tissues develop, and the functioning of organ systems, such as heart and kidneys, increases
• At birth, the average North American baby is about 20 in. long and weighs 7 lbs.

©2005 McGraw-Hill Ryerson Ltd.
Cultural Beliefs about Pregnancy
• Specific actions in pregnancy are often determined by cultural beliefs.
• Two fundamental views of pregnancy:– Pregnancy is a medical condition.– Pregnancy is a natural occurrence.
• It is important for health-care providers to become aware of health practices of various cultural groups, along with their health beliefs about pregnancy and prenatal development.

©2005 McGraw-Hill Ryerson Ltd.
Exploring Teratology
• Teratology – the field of study that investigates the causes of birth defects.
• Teratogen – any agent that causes a birth defect.• Numerous teratogens exist, thus almost every fetus is
exposed to at least some.• Specific teratogens do not usually cause a specific birth
defect.• It may take a long time for the effects of a teratogen to
show up.• Only about half of all potential effects appear at birth.

©2005 McGraw-Hill Ryerson Ltd.
Prenatal Sensitivity to Teratogens
• Sensitivity during Organogenesis
• Sensitivity during the Fetal Period

©2005 McGraw-Hill Ryerson Ltd.
Sensitivity during Organogenesis
• The probability of a structural defect is greatest during organogenesis.
• 15–25 days after conception, the brain is most vulnerable.
• 24–40 days after conception, the eyes are most vulnerable.
• 20–40 days after conception, the heart is most vulnerable.
• 24–36 days after conception, the legs are most vulnerable.

©2005 McGraw-Hill Ryerson Ltd.
Sensitivity during the Fetal Period
• Exposure is less likely to cause anatomical defects.
• Exposure is more likely to stunt growth.
• Exposure to more likely to create problems in organ functioning.

©2005 McGraw-Hill Ryerson Ltd.
Prescription and Nonprescription Drugs
• Both can have possible effects on the fetus.• A tragic example is with the tranquilizer
thalidomide, prescribed in the early 1960s.– Clearly demonstrated the varying periods of sensitivity
to teratogens through differing outcomes based on when mothers used the drug.
• Mothers do not have to be chronic drug users for the fetus to be harmed.
• Taking the wrong drug at the wrong time is enough to physically handicap offspring for life.

©2005 McGraw-Hill Ryerson Ltd.
Prescription Drugs that Can Function as Teratogens
• Antibiotics (streptomycin, tetracycline)
• Some depressants• Certain hormones
(progestin, synthetic estrogen)
• Accutane

©2005 McGraw-Hill Ryerson Ltd.
Nonprescription Drugs that Can Function as Teratogens
• Diet Pills• Aspirin• Caffeine
– A small increase in the risks for spontaneous abortion and low birthweight occurs for pregnant women consuming >150 mg caffeine per day.
– No effects were found for pregnant women who drank decaffeinated coffee.
– FDA recommends either no caffeine or very little.

©2005 McGraw-Hill Ryerson Ltd.
Psychoactive Drugs
• Alcohol• Nicotine• Illegal Drugs

©2005 McGraw-Hill Ryerson Ltd.
Alcohol
• Heavy drinking• Moderate drinking

©2005 McGraw-Hill Ryerson Ltd.
Heavy Drinking during Pregnancy
• Fetal Alcohol Spectrum Disorder (FASD) – the term used to refer to a broad category of disabilities and diagnoses related to prenatal exposure to alcohol.– Includes fetal alcohol syndrome (FAS); partial FAS (pFAS), also
known as fetal alcohol effects (FAE); alcohol-related neuro-developmental disorder (ARND); and alcohol-related birth defects (ARBD).
– FAS is characterized by three criteria:• Prenatal and/or postnatal growth delay• Characteristic cranio-facial anomalies• Central nervous system impairments
– If two of the criteria is present, the child is said to have pFAS or FAE.
– Adults with FAS found to have a high incidence of mental disorders, such as depression and anxiety.

©2005 McGraw-Hill Ryerson Ltd.
Moderate Drinking during Pregnancy
• “Moderate” is defined as 1 to 2 drinks a day.
• Infants were less attentive an alert, with effects still present at 4 years of age.
• One recent study showed that prenatal alcohol exposure was a better predictor of adolescent alcohol use and its negative consequences than was family history of alcohol problems.

©2005 McGraw-Hill Ryerson Ltd.
Nicotine
• Fetal and neonatal deaths are higher among smoking mothers.
• There exists a higher incidence of preterm births and lower birthweights.
• Intervention programs designed to get pregnant women to stop smoking can reduce some of smoking’s negative effects, especially in raising birthweights.

©2005 McGraw-Hill Ryerson Ltd.
The Research on Smoking during Pregnancy
• Studies have shown urine samples of newborns with smoking mothers had substantial amounts of one of the strongest carcinogens in tobacco smoke (NNK).
• Another study showed prenatal exposure to nicotine was related to poorer language and cognitive skills at 4 years of age.
• Respiratory problems and SIDS are more common among the offspring of mothers who smoked during pregnancy.

©2005 McGraw-Hill Ryerson Ltd.
Illegal Drugs
• Cocaine• Marijuana• Heroin

©2005 McGraw-Hill Ryerson Ltd.
Cocaine Use during Pregnancy
• The most consistent finding is that cocaine exposure during prenatal development is associated with reduced birthweight, length, and head circumference.
• A recent study associated cocaine exposure with impaired motor development at 2 years of age.
• Fetal cocaine exposure is also linked with impaired information processing (poor attentional skills through 5 years of age; impaired processing of auditory information after birth).

©2005 McGraw-Hill Ryerson Ltd.
Other Related Influences
• Research findings must be interpreted with caution due to the presence of other factors in the lives of pregnant women who use cocaine:– Poverty– Malnutrition– Other substance abuse: marijuana, alcohol,
amphetamines

©2005 McGraw-Hill Ryerson Ltd.
Marijuana Use during Pregnancy
• Associated with increased tremors and startles among newborns
• Associated with poorer verbal and memory development at 4 years of age

©2005 McGraw-Hill Ryerson Ltd.
Heroin Use during Pregnancy
• Young infants are addicted and show withdrawal symptoms characteristic of opiate abstinence:– Tremors– Irritability– Abnormal crying– Disturbed sleep– Impaired motor control
• Behavioural problems are still present at the first birthday.
• Attention deficits may appear later in development.

©2005 McGraw-Hill Ryerson Ltd.

©2005 McGraw-Hill Ryerson Ltd.
Environmental Hazards
• Radiation: nuclear environments, X-rays, computer monitors
• Chemicals: carbon monoxide, mercury, lead, pesticides, PCBs
• Heat: saunas, hot tubs

©2005 McGraw-Hill Ryerson Ltd.
Findings on Radiation Exposure
• Can cause gene mutation
• Can cause chromosomal abnormalities
• X-rays can effect the developing embryo most during the first several weeks after conception

©2005 McGraw-Hill Ryerson Ltd.
Findings on Hazardous Chemicals
• Early exposure to lead affects children’s mental development
• Women who ate PCB-polluted fish were more likely to have smaller, preterm infants who reacted slowly to stimuli
• Prenatal exposure to PCBs has also been associated with problems in visual discrimination an short-term memory in 4-year-old children

©2005 McGraw-Hill Ryerson Ltd.
Effects of Exposure to High Temperatures
• Prolonged exposure to heat in saunas or hot tubs that raise the mother’s body temperature creates a fever that endangers the fetus.
• The high temperature may interfere with cell division and may cause birth defects or even fetal death.

©2005 McGraw-Hill Ryerson Ltd.
Other Maternal Factors
• Infectious Diseases
• Nutrition
• Emotional States and Stress
• Maternal Diabetes
• Maternal Age

©2005 McGraw-Hill Ryerson Ltd.
Infectious Diseases
• Rubella• Syphilis• Genital Herpes• AIDS

©2005 McGraw-Hill Ryerson Ltd.
Rubella
• Also known as German Measles, the greatest damage occurs when mothers contract it in the 3rd and 4th weeks of pregnancy, although infection during the 2nd month is also damaging.
• A rubella outbreak in the mid 1960s resulted in 30,000 prenatal and neonatal deaths.
• It also caused more than 20,000 infants to be affected, displaying mental retardation, blindness, deafness, and heart problems.

©2005 McGraw-Hill Ryerson Ltd.
Syphilis
• Syphilis is a sexually transmitted disease.• It is more damaging in later prenatal
development, 4 months or more after conception.
• It damages organs after they are formed, including– Eye lesions (which can cause blindness)– Skin lesions
• If it is present at birth it can cause problems with the central nervous system and gastrointestinal tract.

©2005 McGraw-Hill Ryerson Ltd.
Genital Herpes
• Newborns contract the virus when they are delivered through the birth canal of a mother with genital herpes.
• One-third of babies delivered through an infected birth canal die.
• One-fourth of babies delivered through an infected birth canal become brain damaged.
• If an active case of genital herpes is detected close to a woman’s due date, a cesarean section can be performed to keep the newborn safe.

©2005 McGraw-Hill Ryerson Ltd.
AIDS
• AIDS is a sexually transmitted disease which destroys the body’s immune system.
• A mother can infect her offspring in three ways:– During gestation across the placenta.– During delivery through contact with maternal body fluids.– Postpartum through breast feeding.
• Babies born to infected mothers can be– Infected and symptomatic.– Infected but asymptomatic (with the possibility of developing
symptoms up until 15 months of age).– Not infected at all.

©2005 McGraw-Hill Ryerson Ltd.
Nutrition
• A developing fetus depends completely on its mother for nutrition, which comes from her blood.
• Important factors of nutritional status are– Total number of calories– Levels of protein, vitamins, and minerals– Folic acid
• A folic acid deficiency is linked with neural tube defects, such as spina bifida.

©2005 McGraw-Hill Ryerson Ltd.
Emotional States and Stress
• Effects on Pregnancy• Effects on Labour and Delivery

©2005 McGraw-Hill Ryerson Ltd.
Effects of Stress on Pregnancy
• A mother’s stress can be transmitted to the fetus.
• When a pregnant woman experiences intense fears, anxieties, and other emotions, physiological changes occur:– Respiration– Glandular secretions, such as adrenaline
• These affect the fetus by, for example, restricting the blood flow to the uterine are depriving the fetus of adequate oxygen.

©2005 McGraw-Hill Ryerson Ltd.
Effects of Stress on Labour and Delivery
• A mother’s emotional state during pregnancy can influence the birth process.
• An emotionally distraught mother may have irregular contractions and a more difficult labour.
• This can lead to irregularities in the baby’s oxygen supply or irregularities after birth.
• Research had found that pregnant women who are optimists have less adverse birth outcomes.

©2005 McGraw-Hill Ryerson Ltd.
Maternal Diabetes
• Diabetes is a disorder of the metabolism, which most often is caused by the inability of the body to properly absorb sugar and starch from the blood.
• Gestational diabetes may occur during pregnancy, usually during the 24th week.
• To ensure a smooth pregnancy and a healthy baby, women with diabetes must take several precautions:– Follow an appropriate meal plan that helps to maintain normal blood
glucose levels.– Monitor glucose levels frequently.– Control and treating hypoglycemia.– Add or maintain an appropriate level of physical activity.

©2005 McGraw-Hill Ryerson Ltd.
Maternal Age
• Adolescence
• The Thirties and Beyond

©2005 McGraw-Hill Ryerson Ltd.
Adolescence
• Infants born to adolescents are often premature. • The mortality rate of infants born to adolescent
mothers is double that of infants born to mothers in their twenties.
• May be due to– Immature reproductive systems– Poor nutrition– Lack of prenatal care– Low socio-economic status

©2005 McGraw-Hill Ryerson Ltd.
The Thirties and Beyond
• The risk of Down Syndrome increases after the mother reaches age 30.
• Women have more difficulty getting pregnant after age 30.
• As women remain active, exercise regularly, and are careful about their nutrition, their reproductive systems may remain healthier at older ages.

©2005 McGraw-Hill Ryerson Ltd.
Paternal Factors
• Men’s exposure to lead, radiation, certain pesticides, pretochemical may cause abnormalities in sperm that lead to miscarriage or disease.
• When fathers have a diet low in vitamin C, their offspring have a higher risk of birth defects and cancer.
• Early findings point to a connection between cocaine use in fathers an birth defects.
• Father’s smoking during pregnancy may lead to lower birth weight and potential for their offspring developing cancer.
• Older fathers may place their offspring at risk for certain birth defects, such as Down syndrome and dwarfism.

©2005 McGraw-Hill Ryerson Ltd.
Prenatal Care
• Usually involves a package of medical care services in a defined schedule of visits
• Often includes educational, social, and nutritional services
• Includes screening for conditions that can affect the baby or mother
• Is extremely valuable, especially for first-time mothers• It is very important for women in poverty because it links
them with other social services• Can motivate women to have positive attitudes toward
pregnancy• Not all women have access to or seek out adequate
prenatal care

©2005 McGraw-Hill Ryerson Ltd.
Positive Prenatal Development
• In most pregnancies, prenatal development does not go awry and development occurs along with a positive path.
• Prospective parents should be careful to avoid the vulnerabilities to fetal development.

©2005 McGraw-Hill Ryerson Ltd.
Birth
The Birth
Process
Special
Neonatal
Considerations
Measures
of Neonatal
Health and
Responsiveness

©2005 McGraw-Hill Ryerson Ltd.
Exploring the Birth Process
• Stages of Birth
• The Fetus/Newborn Transition
• Childbirth Strategies

©2005 McGraw-Hill Ryerson Ltd.
The First Stage of Birth
• This is the longest of the three stages, lasting an average of 12–24 hours.
• Uterine contractions are 15–20 minutes apart and last up to 1 minute.
• Contractions cause the cervix to stretch and open.
• Contractions get closer together as the stage progresses.
• By the end of this stage the cervix is dilated to about 4 inches.

©2005 McGraw-Hill Ryerson Ltd.
The Second Stage of Birth
• This stage begins when the baby’s head starts to move through the cervix and birth canal.
• It terminates when the baby completely emerges from the mother’s body.
• This stage lasts about one and a half hours, and involves the mother bearing down to push the baby out.
• Contractions come about every minute and last about a minute.

©2005 McGraw-Hill Ryerson Ltd.
The Third Stage of Birth
• This stage is called “afterbirth” and lasts only minutes.
• It involves the detachment and expulsion of the placenta, umbilical cord, and other membranes.

©2005 McGraw-Hill Ryerson Ltd.
The Fetus/Newborn Transition
• Being born involves considerable stress for the baby.• Anoxia (the condition in which the fetus/newborn has an
insufficient supply of oxygen) can cause brain damage, and is concern if delivery takes too long.
• Large quantities of adrenaline and noradrendaline are secreted to protect the fetus in the event of oxygen deficiency.
• After the umbilical cord is cut, 25 million air sacs in the lungs must fill with air.
• The newborn’s bloodstream is redirected through the lungs and to all parts of the body.
• The baby is born with a protective covering of skin grease, called vernix caseosa, which is cleaned off.

©2005 McGraw-Hill Ryerson Ltd.
Childbirth Strategies
• Childbirth Settings and Attendants
• Methods of Delivery• http://vad.mhhe.com/
provided_module.cfm?ModuleID=216 (Birth and the Newborn: “Childbirth Education Alternatives”)

©2005 McGraw-Hill Ryerson Ltd.
Childbirth Settings and Attendants
• 99% of all births in Canada take place in hospitals, and over 90% are attended by physicians.
• Relatively new birthing rooms approximate a home setting, yet allow for medical intervention if necessary or desired.
• Approximately 1% of Canadian women are attended by a midwife, most of whom are nurses who have been specially trained in delivering babies.
• In many other countries, babies are more likely to be born at home, and women are much more likely to choose a midwife than a physician.
• A doula is a caregiver who provides continuous physical, emotional, and educational support before, during, and after birth.

©2005 McGraw-Hill Ryerson Ltd.
Methods of Delivery
• Medicated• Natural• Prepared• Cesarean

©2005 McGraw-Hill Ryerson Ltd.
Medicated Childbirth
• Health practitioners recommend the least possible medication during delivery.
• Three basic kinds of drugs used for labour:– Analgesia: used to relieve pain (tranquilizers,
barbiturates, narcotics)– Anesthesia: block sensation in an area of the body, or
blocks consciousness (epidural)– Oxytocics: synthetic hormones that stimulate
contractions (Pitocin)
• Individuals differ as to how drugs affect them.

©2005 McGraw-Hill Ryerson Ltd.
Natural Childbirth
• Developed by an English obstetrician to reduce the mother’s pain by decreasing her fear through education about childbirth and by teaching her to use breathing methods and relaxation techniques during delivery.
• It considers the doctor’s relationship with the mother as an important aspect of reducing her perception of pain, and he or she should be present during active labour to provide reassurance.

©2005 McGraw-Hill Ryerson Ltd.
Prepared Childbirth
• Developed by French obstetrician Ferdinand Lamaze and is similar to natural childbirth with the addition of a special breathing technique to control pushing in the final stages of labour.
• It also included a more detailed anatomy and physiology course.
• Other prepared childbirth techniques have been developed, combining aspects from both of these methods and emphasizing fathers as labour coaches.

©2005 McGraw-Hill Ryerson Ltd.
Cesarean Delivery
• The baby is removed from the mother’s uterus through an incision made in her abdomen.
• Usually performed if the baby is in a breech position, causing the baby’s buttocks to emerge from the vagina first.
• Also used if:– The baby is lying crosswise in the uterus– The baby’s head is too large to fit through the pelvis– The baby develops complications– The mother is bleeding vaginally

©2005 McGraw-Hill Ryerson Ltd.
Special Neonatal Considerations

©2005 McGraw-Hill Ryerson Ltd.
Preterm Infants and Age-Weight Considerations
• Preterm and Low-Birthweight Infants
• Long-Term Outcomes for Low-Birthweight Infants

©2005 McGraw-Hill Ryerson Ltd.
Preterm and Low-Birthweight Infants
• A preterm infant is one who is born prior to 38 weeks after conception
• A low-birthweight infant is born after a regular gestation period of 38–42 weeks but weighs less than 5 ½ lbs.
• Both are considered high-risk infants. • A short gestation period does not necessarily
harm an infant, and neurological development continues after birth on the same timetable.
• Premature infants with a precariously low birthweight are considered high risk.

©2005 McGraw-Hill Ryerson Ltd.
Long-Term Outcomes for Low-Birthweight Infants
• Most low-birthweight infants are normal and healthy; as a group they have more health and developmental problems.
• The number and severity of problems increase as birthweight decreases.
• With the improved survival rate of such infants come increases in severe brain damage.
• Lower brain weight is associated with greater likelihood of brain injury.

©2005 McGraw-Hill Ryerson Ltd.
Long-Term Outcomes for Low-Birthweight Infants (cont’d)
• Low-birthweight infants are also more likely to have lung or liver diseases.
• School age children who were low-birthweight babies are more likely to have learning disabilities, attention deficit disorder, or breathing problems like asthma.
• Children born very low in birthweight have more learning problems and lower levels of achievement in reading and math than moderately low-birthweight children.

©2005 McGraw-Hill Ryerson Ltd.
Gender Ambiguity
• Gender Ambiguity (intersexuality or hermaphroditism) – occurs when a child is born with both male and female features.
• Surgical procedures and treatment are available to provide specific male or female genitatia.

©2005 McGraw-Hill Ryerson Ltd.
Measures of Neonatal Health and Responsiveness
• The Apgar Scale
• The Brazelton Neonatal Behavioural Assessment Scale

©2005 McGraw-Hill Ryerson Ltd.
The Apgar Scale
• A method widely used to asses the health of newborns at 1 and 5 minutes after birth
• It evaluate infants’– Heart rate– Respiratory effort– Muscle tone– Body colour– Reflex irritability
• Obstetrician or nurse assess the newborn and gives a scale of 0, 1, or 2 on each item.
• A score of 7–10 is good, 5 indicates possible development of difficulties, 3 or below signals an emergency.

©2005 McGraw-Hill Ryerson Ltd.
The Brazelton Neonatal Behavioural Assessment Scale
• Performed within 24–36 hours after birth to evaluate neurological development, reflexes, and reactions to people.
• The newborn is rated on each of 27 items, contributing to four categories: physiological, motoric, state, and interaction.
• Babies are also given global classification such as “worrisome,” “normal,” “superior.”
• Parents are shown the importance of social interaction with their infant and how to positively respond to their baby.

©2005 McGraw-Hill Ryerson Ltd.
The Postpartum
Period
What Is the
Postpartum
Period?
Physical
Adjustments
Emotional and
PsychologicalAdjustments
Bonding

©2005 McGraw-Hill Ryerson Ltd.
What is the Postpartum Period?
• The period after childbirth or delivery• Woman’s body adjusts, physically and
psychologically, to the process of childbearing.
• Last about 6 weeks; body returns to near prepregnant state.
• Influenced by what precedes it – method and circumstances of delivery affect speed of readjustment

©2005 McGraw-Hill Ryerson Ltd.
What is Postpartum Period? (cont’d)
• Adjustment and adaptation include:– Learning to care for baby– Recovering from childbirth– Caring for baby– Learning to feel good as a mother– Father caring for mother– Father learning to care for baby

©2005 McGraw-Hill Ryerson Ltd.
Physical Adjustments
• Involution is the process by which the uterus returns to its prepregnant size, 5–6 weeks after birth.
• Nursing the baby helps contract the uterus rapidly.• Menstruation begins 4–8 weeks after delivery if mother is
not breast feeding.• Breast feeding causes delay in menstruation for several
months, but ovulation can still occur.• Physicians usually recommend refraining from sexual
intercourse for approximately 6 weeks following birth.• Exercise is recommended for the postpartum period, as
are relaxation techniques to relax and refresh the mother.

©2005 McGraw-Hill Ryerson Ltd.
Emotional and Psychological Adjustments
• Emotional fluctuations are common for the mother in the postpartum period and can be caused by – Hormonal change– Fatigue– Inexperience/lack of confidence with the baby– The extensive time and demands of caregiving
• Mothers may benefit from professional help in dealing with their problems if difficulties persist.
• Fathers undergo postpartum adjustment as well, in caregiving and with concerns that the baby comes first and gets all the mother’s attention.

©2005 McGraw-Hill Ryerson Ltd.
Bonding
• Bonding is the occurrence of close contact, especially physical, between parents and newborn in the period shortly after birth.
• This is a critical time when an important emotional attachment is formed that provides a foundation for optimal development in years to come.
• Research supports the importance of bonding, but challenges the significance of the first few days of life as a critical period.

©2005 McGraw-Hill Ryerson Ltd.
Bonding (cont’d)
• Close contact does bring tremendous pleasure, and can set in motion a climate for improved interaction after the mother and infant leave the hospital.
• Many hospitals offer a “rooming in” arrangement, in which the baby remains in the mother’s room for most of its hospital stay.