Embed Size (px)
Citation preview
OutcomesNephrology and Hypertension
2006


Outcomes | 2006
Quality counts when referring patients to hospitals
and physicians, so Cleveland Clinic has created a series
of outcomes books similar to this one for its institutes
and departments. Designed for a health care provider
audience, the outcomes books contain a summary of
our surgical and medical trends and approaches; data
on patient volume and outcomes; and a review of new
technologies and innovations. We hope you find these
data valuable. To view all our outcomes books, visit
Cleveland Clinic’s Quality Web site at
clevelandclinic.org/quality/outcomes.

2 | Nephrology and Hypertension 2006

Nephrology and Hypertension | �
Chairman’s Letter 4
Department Overview 6
Quality & Outcome Measures 9
Patient Experience 25
Innovations 26
New Knowledge �8
Staff Listing 42
Department Contacts | How to Refer Patients 44
Locations 45
Cleveland Clinic Overview 46
Online Services 47
Contact Numbers 48
Table of Contents |

4 | Nephrology and Hypertension 2006
Innovative health management plays a critical role in achieving exceptional patient outcomes. Healthcare professionals realize achieving successful results is directly correlated to assembling the very best team and focusing on impact questions that affect the outcomes in the individual patient. During 2006 the department expanded the numbers of scientists, clinical faculty and physician extenders, i.e. nurse practitioners and physician assistants who actively confront difficult research issues and clinical problems across a broad spectrum of renal and hypertensive diseases.
Over the past several decades, the Department of Nephrology and Hypertension at Cleveland Clinic has made a number of contributions aimed at improving overall patient outcomes in the areas of chronic kidney disease, transplantation, hypertension and dialysis. Organizing healthcare teams around specific themes within the Nephrology and Hypertension Department, i.e. CKD, dialysis, transplant, hypertension and renal diseases, represents the first step to creating innovative approaches to managing health in our patients. Horizontal integration of specific research platforms will spearhead the translation of discoveries in the lab, or from clinical research initiatives, to the bedside.
Critical initiatives in 2007 include the expansion of the Chronic Kidney Disease Clinic, the continuing mining of Cleveland Clinic Acute Kidney Injury Database, ongoing analysis of quality results in our chronic dialysis facilities, optimization of both patient and allograph survival following transplantation, and evaluation of new approaches to the treatment of polycystic kidney disease, glomerulonephritis, and stone disease. Moreover, redefining the levels of optimal
Chairman’s Letter |

Nephrology and Hypertension | 5
blood pressure and recognizing the importance of the pre-hypertension patient further emphasizes the critical role innovative health care models can have in preventing complications that result from both inadequate recognition, as well as treatment. Moving forward, a number of key education programs for the public and patients with kidney disease and hypertension will provide an essential component to ensuring increased patient awareness and successful treatment goals into the future.
We invite comments and suggestions regarding the data and information contained in the current Outcomes book and we look forward to participating in managing the health of patients with renal disease and hypertension. Measuring outcomes provides us insight into how well we are doing in attaining our goal of being the best in the field. The entire Department of Nephrology and Hypertension remains dedicated to ensuring the most innovative approaches to managing health and tracking outcomes in our patients with renal disease and/or hypertension now and in the future.
Martin J. Schreiber Jr., M.D. Chairman, Department of Nephrology and Hypertension

6 | Nephrology and Hypertension 2006
Department Overview |
Cleveland Clinic was honored to be ranked No. � for kidney disease in the country by U.S.News & World Report. We understand this recognition is a function of our clinical and scholarly activities; however, we also wish to recognize the scholarly contribution of our department in terms of basic and clinical research, as well as our participation in the new medical school. Many of our faculty have actively participated in the renal curriculum of the medical school and some have been facilitators for problem-based learning exercises throughout the year. We continue to strive to deliver optimal patient care, cutting edge research and medical education.
The Department focuses on five major disease areas: chronic kidney disease (CKD), dialysis, renal transplantation, hypertension and general nephrology (stones, glomerulonephritis, etc.). The outcomes presented in this report are formatted under these specific themes.
From the outset, our department recognizes the benefits and challenges involved in reporting outcomes data from our subspecialty. For example, our outpatient dialysis activities are monitored mostly by an independent quality assessment program because they entail operations of the Ohio Renal Care Group/Fresenius Medical System (ORCG/FMS), which is a shared initiative among MetroHealth Medical Center, ORCG/FMS and Cleveland Clinic. The product of this monitoring program is a detailed quarterly report that compares a range of patient outcomes to absolute standards, as well as those achieved by other dialysis units regionally and nationally. This quality report provides a model for our other outpatient activities. Medical care in our dialysis units lends itself extremely well to quality monitoring because of six features: 1) it is largely procedural; 2) it involves a readily identifiable population; �) the population is numerically stable over time; 4) the population shares a common disease state; 5) the population has regularly measured, standardized indicators; and 6) the indicators are recorded electronically for ready retrieval.

Nephrology and Hypertension | 7
Clinical activities in our non-dialysis inpatient and outpatient care areas are not as amenable to quality management because, in their current configuration, they lack most of these six features. Accordingly, we propose a strategy of restructuring our clinical and scholarly activities within each theme area so we may better respond to patient needs and appropriately monitor quality and outcomes of all our activities.
The outcomes we have selected for each theme area in this report forecast some of the important clinical and scholarly activities we believe are crucial to our mission. We are excited to incorporate recent advances in Cleveland Clinic’s electronic medical record (EMR) to monitor the quality of our processes of care and outcome data within individual disease theme areas. In utilizing the EMR, we recognize that diagnostic categories need to be accurate (i.e., diagnosis established) and precise (i.e., adjusted to its context) to report meaningful outcomes. We are eager to take on these challenges. Our initial goal is to arrive, in the shortest possible time, at an accurate and exacting baseline within each theme area. That way, we can launch meaningful monitoring of our clinical care, document the benefits of our services to patients and referring physicians and continually improve performance and patient care.
A snapshot of our department’s clinical activities can be viewed in Tables 1 and 2. Outpatient visits, hospital admissions, length of stay, and number of chronic outpatient hemodialysis patients remain strong. The Renal Function Lab is a busy clinical enterprise and intensely involved in clinical research protocols. With respect to volume trends, the number of inpatient and ICU dialysis treatments increased over the past four years. By intent and design, the number of outpatient hemodialysis sessions performed in the in-hospital M82 unit has curtailed to permit growth of our in-hospital and ICU programs.

8 | Nephrology and Hypertension 2006
Table 1: Selected Department Statistics
Total patient visits 18,�80
Total new patients 496
Admissions 688
Patient days 4,�59
Average length of stay (days) 6.�4
Glomerular filtration rate (GFR) 582
Total inpatient hospital consultations 1,4�8
Table 2: 2006 Inpatient Dialysis Treatments by Treatment Type
Service
Inpatient hemodialysis 4,69�
Intensive care hemodialysis 1,628
Continuous AV hemofiltration 2,72�
Slow continuous hemofiltration 1�1
Ultrafiltration 47
Continuous cycling peritoneal dialysis (CCPD) 501
Continuous ambulatory peritoneal dialysis (CAPD) 14

Nephrology and Hypertension | 9
Quality & Outcome Measures |
Chronic Kidney Disease (CKD)
Physicians within the CKD theme area are responsible for the establishment of a formal CKD Clinic. The CKD Clinic will accept patients referred from Cleveland Clinic and outside physicians for evaluation and management of their CKD. Enrollment of patients in the CKD Clinic and use of the Electronic Medical Record (EMR) will permit the establishment of a CKD database of the demographics, clinical parameters and outcomes of these patients. In addition to providing significant outcomes, the CKD database will be fertile ground for identifying and enrolling patients in clinical research projects.
Two important outcomes projects within the CKD theme areas are:
• Anemia Management Project • Validation of Predictive Equations for Glomerular Filtration Rate (GFR)
A clinical program was developed for the evaluation and management of the anemia of CKD using erythropoietin (EPO) preparations, intravenous iron supplementation and continuous nurse monitoring of treatment results. Appropriately managing anemia is critical to avoid left ventricular hypertrophy, risk for congestive heart failure, etc.
As shown in Figure 1A, the number of patients treated with EPO increased dramatically from 2002 to 2006. The number of patients treated in the Anemia Management Project more than quadrupled over this time – evidence of marked program growth.
Figure 1B depicts the project’s success, showing the percentage of patients reaching target hemoglobin greater than 11 gm. Prior to the initiation of this project, less than half the CKD patients treated with EPO reached target hemoglobin. Development of a structured program, using a suitable clinical algorithm, achieved success due to the hard work of both our dedicated nursing staff and Saul Nurko, M.D. who play an integral part in the CKD Anemia Management Project.

10 | Nephrology and Hypertension 2006
In 2006, the Anemia Management Project served as an example of the capabilities of active Continuous Quality Initiative (CQI) review process. It was observed that a lower percentage of patients were reaching target hemoglobin. The CQI review process determined lengthening the treatment frequency intervals and missed treatments were primary causes of failure to meet target. Appropriate interventions were put into place and the problem was corrected. Congratulations to the CQI team!
Anemia Management
400
300
200
100
02002 2003 2004
Average Monthly Census2005 2006
#
Volume
Patients Reaching Target100
75
50
25
02002 2003 2004 2005 2006
%
Figure 1A
Figure 1B

Nephrology and Hypertension | 11
With the inception of the Kidney Disease Outcomes Quality Initiative (K/DOQI) project under the direction of the National Kidney Foundation (NKF), CKD is defined and staged based upon estimates of glomerular filtration rate (GFR). K/DOQI recommended clinicians use predictive equations such as the MDRD formula1 or Cockcroft-Gault equation2 to estimate GFR. Our department has been instrumental in the development and validation of such strategies using the estimated GFR (eGFR). Dr. Joseph Nally actively participated with the NKF in ongoing discussions and work groups on this important topic. For nearly two decades, the Renal Function Laboratory, directed by Dr. Phillip M. Hall, was the NIH core facility for formally measuring iothalamate GFR. More than 15,000 GFR measurements were performed over the last decade. With the more recent advent of the eGFR, Drs. Emilio Poggio and Phillip Hall, along with their research team (Hank Rolin and Sue Saunders), have been instrumental in validating the accuracy and limitations of the eGFR concept.
Data from recent publications of Dr. Poggio, et al. demonstrate:
• Use of the eGFR from the MDRD equation is valid in a stable, outpatient CKD population with GFR from 15 to 60 ml/min/1.7� m2.
• The eGFR in the CKD population is applicable to both diabetic and non-diabetic CKD patients.
• The eGFR in CKD patients with a kidney transplant is a reasonable estimate of kidney function.
1. Peterson JD, Adler S, Burkart JM, Greene T, Hebert LA, Hunsicker G, et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease Study. Ann Intern Med 1995;12�:754-762.
2. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976;16:�1-41.

12 | Nephrology and Hypertension 2006
Limitations to the current eGFR predictive equations include:
eGFR with the MDRD equation is NOT appropriate for use in the hospitalized patient because the predictive equation tends to overestimate true iothalamate-measured GFR. eGFR does NOT provide an appropriate estimate of GFR in patients with normal kidney function such as a potential kidney donor with a GFR greater than 70 mL/min/1.7� m2.
Dr. Poggio is collaborating with other investigators throughout the nation to study the potential role of incorporating measurements of cystatin C (a newer technique to measure renal function) into predictive equations to provide more precise estimates of GFR across all levels of kidney function. This is further discussed in the Innovations section.
•
•
GFR in Stable outpatient CKD or Normal Kidney Function
GFR in Patient with Kidney Transplant
Poggio ED, et al. J Am Soc Nephrol 2005;16:459-466.
Poggio ED, et al. Am J Transplant 2006;6:100-108.
0
30
60
90
120
150
180
iGFR
(mL/
min/
1.73
m2 )
0 30 60 90 120 150 180eGFRMDRD (mL/min/1.73m2)
-30
0
30
60
90
120
150
180
eGFRMDRD (ml/min/1.73m2)
-30 0 30 60 90 120 150 180
Iotha
lamate
GFR
(ml/m
in/1.
73m2 )

Nephrology and Hypertension | 1�
Dialysis
Outpatient Dialysis
Medical care in our dialysis unit lends itself extremely well to quality monitoring and outcomes determination because of the six features noted in the Department Overview. The most important outcome related to our outpatient dialysis practice at ORCG/FMS is that of patient mortality. Comparing survivals of patients in our program with other programs throughout the United States ensures our patients continue to receive the best care, which can result in a survival advantage. There is a patient survival advantage for ESRD patients undergoing hemodialysis at an ORCG/FMS facility with a Cleveland Clinic nephrologist as a medical director. As opposed to the average one-year national mortality rate of 21.8%, our five outpatient dialysis facilities had a composite mortality rate of only 14.9%, which represents a survival advantage exceeding 25% for our patients.
Patient Mortality25
20
15
10
5
0Unit A Unit B Unit C
Outpatient Dialysis Facilities
Unit D Unit E CCComposite
%Mortality
USRDS Benchmark
n=231 n=82 n=119 n=54 n=45 n=531

14 | Nephrology and Hypertension 2006
Intensive Care Unit (ICU) Nephrology and Acute Renal Failure
Our most frequent consultations in the ICU relate to acute renal failure. Cleveland Clinic’s ICU nephrology team provides consultative care and treatment to some of the most complex medical cases in the United States, a result of the expertise of our surgeons and the reputation of Cleveland Clinic. Recently, in collaboration with the Department of Cardiothoracic Anesthesia, we analyzed our experience with acute renal failure after open-heart surgery (OHS).
Acute renal failure (ARF) can be defined as either a 50% reduction in GFR or the need for acute dialysis therapy, an obviously more severe degree of renal compromise. The records of ��,217 patients who had open-heart surgery at Cleveland Clinic between 199� and 2002 were analyzed. Overall frequency of renal events by gender and race are shown in the table. Notably, we learned the risk of renal failure is higher in women and in patients who undergo combined valve and coronary artery bypass graft (CABG) surgery.

Nephrology and Hypertension | 15
Effect of Type of Surgery on ARF
Thacker et al., et al. Am J Kidney Dis April 200�.
12
10
8
6
4
2
0
%
n=231
AFR requiring dialysis50% or greater decline in GFR not requiring dialysis
CABG Only(n=12,840)
Valve Only(n=5,344)
CABG & Valve(n=3,282)
Other(n=1,123)
2.6%
1.2%
2.8%
1.7%
4.6%
3.3%
6%
5.3%
Frequency of Events after OHS: Univariate Analysis
> 50% decline in GFR ARF -D not requiring dialysis
Overall �.1 % 1.8 %
Males 2.5 % 1.6 %
Females 4.6 % 2.4 %
Non-African-Americans �.1 % 1.7 %
African-Americans 4.5 % 2.9 %

16 | Nephrology and Hypertension 2006
Risk Factor PointFemale Gender 1IABP (Intraaortic Balloon Pump) 2CHF (Congestive Heart Failure) 1LVEF (Left Ventricular Ejection Fraction) <�5 % 1Valve Surgery Only (reference to CABG) 1CABG + Valve (reference to CABG 2Other Cardiac Surgeries (reference to CABG) 2COPD (Chronic Obstructive Pulmonary Disease) 1IDDM (Insulin Dependent Diabetes) 1Prior Cardiac Surgery 1Emergency Surgery 2Pre-op Creatinine (mg/dl): 1.2 to <2.1 2Pre-op Creatinine (mg/dl): >2 5
Frequency of ARF-Dialysis According to Risk Categories
Thakar et al, Am J Kidney Dis; April 200�.
30
20
10
0
%ARF-Dialysis
Validation data95% CI
Test data
0-28,4168,519
Risk CategoryTest NValidation N
3-56,0975,978
6-81,1811,173
9-13144169
Information derived from the OHS database enabled us to develop a predictive model for ARF, subsequently validated in a separate cohort of patients. Based on this information and experience, patients are now categorized into one of four risk levels for ARF, based on a point system that weighs preoperative risk factors. Frequency of ARF-dialysis according to risk categories is also demonstrated. Laminated copies of this predictive model are available by contacting Roseanne McCormick at 216.444.5788 or at [email protected].
Nephrology and Hypertension | 17
Mortality Overall Males Females
Total Cohort 2.2% 1.8% �.1%*
ARF Dialysis 61.2% 56.5% 68.6%**
> 50% Drop in GFR 14.1% 1�.�% 14.6%^ or Dialysis
(* P< 0.001; ** P = 0.01; ^ P = 0.6�)
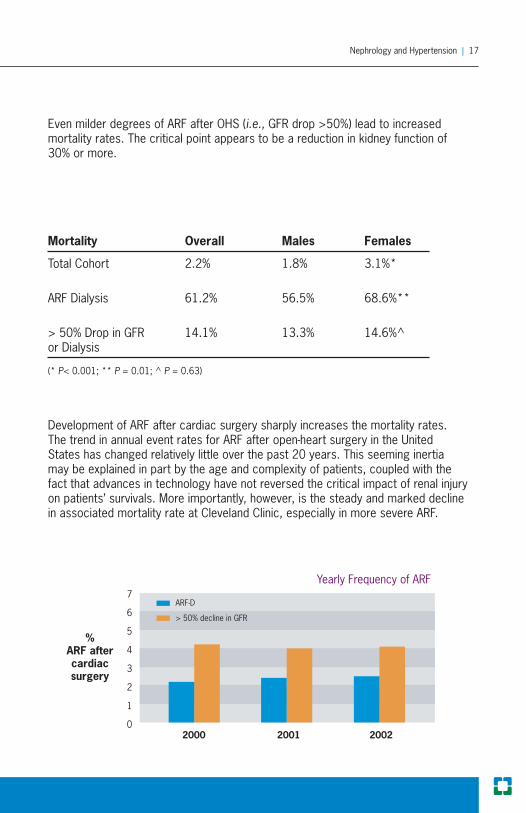
Development of ARF after cardiac surgery sharply increases the mortality rates. The trend in annual event rates for ARF after open-heart surgery in the United States has changed relatively little over the past 20 years. This seeming inertia may be explained in part by the age and complexity of patients, coupled with the fact that advances in technology have not reversed the critical impact of renal injury on patients’ survivals. More importantly, however, is the steady and marked decline in associated mortality rate at Cleveland Clinic, especially in more severe ARF.
Yearly Frequency of ARF7
6
5
4
3
2
1
02000 2001 2002
ARF-D
> 50% decline in GFR
%ARF aftercardiacsurgery
Even milder degrees of ARF after OHS (i.e., GFR drop >50%) lead to increased mortality rates. The critical point appears to be a reduction in kidney function of �0% or more.

18 | Nephrology and Hypertension 2006
As we serve an ever increasing elderly population with a high co-morbidity burden, the occurrence of acute kidney injury (AKI) following open heart surgery remains about the same. The roles of several preoperative conditions which influence the development of postoperative renal dysfunction have been developed and reconfirmed. Do these same preoperative risk factors used in predicting acute kidney injury have an influence on postoperative mortality? Also, will this burden of disease influence the outcome of patients who develop acute renal dysfunction?
When the time frames from 199�-1997 were compared with 1998-2002, data showed mortality associated with AKI actually declined by 20% over time (61% vs. 49%, p<0.001). Indeed, the reduction in mortality was seen in patients with AKI despite an increase in comorbid conditions. Preoperative risk factors for developing AKI did not seem to influence the mortality in patients with AKI. This can be attributed to improved dialytic techniques and dose deliveries.
80
40
02000 2001 2002
ARF-D
> 50% decline in GFR
%
Yearly Mortality Rates in ARF at Cleveland Clinic

Nephrology and Hypertension | 19
The figures compare outcomes of five centers who participated in the Program to Improve Care in Acute Renal Disease (PICARD) NIH Trial, as well as the internal data of post open heart AKI outcome over time. (Published in Kidney International 2004;66:161�-1621.
In 2006, the European Heart Journal presented a review and meta-analysis of 19 preoperative risk stratification models for OHS (Eur Heart J 2006;27:867-874). We are pleased to report the Cleveland Clinic predictive model was one of only three models recognized as accurate and predictive of mortality in the ICU following OHS.
100
80
60
40
20
0All CC MMC VU
Dialysis Modality
UCSD UCSF
NoneIHD only* CRRT only**Combined initially, IHDCombined, initially CRRT%
MortalityRates
CC - Cleveland Clinic, MMC - Maine Medical Center, VU - Vanderbilt University,
UCSD - University of California San Diego, UCSF - University of California San Francisco
* IHD - Intermittent Hemodialysis** CRRT - Continuous Renal Replacement Therapy
Dialysis Modality

20 | Nephrology and Hypertension 2006
100
80
60
40
20
0No AKI AKI
ExpiredDischarged on Dialysis
%
Alive
In 2006, the combined efforts of the nephrology and cardiac teams developed a predictive score for acute kidney injury (AKI) that would require hemodialysis following cardiac transplantation. Recipients of 756 cardiac transplants between 199� and 2004 formed the basis for this study. The primary outcome was postoperative AKI requiring hemodialysis. Overall, 5.8% of patients developed AKI requiring dialysis. As shown in the figure below, the mortality rate of patients with AKI requiring dialysis was substantial (50% vs. 1.4% without AKI). (Boyle, JM, et al. American Journal of Kidney Disease. Risks and outcomes of acute kidney injury requiring dialysis after cardiac transplantation. 2006;48:87-796). AKI was associated with greater frequencies of cardiac, neurological and serious infection morbidities. By means of multivariate analysis, were independent predictors of postoperative AKI requiring dialysis increased serum creatinine levels, lower serum albumins, insulin-requiring diabetes, and longer cardiopulmonary bypass times. Investigators are working to develop a risk stratification which may assist in implementing strategies to prevent or limit posttransplant kidney injury which may offer a survival benefit.
Nephrology and Hypertension | 21
Transplant
Our department looks forward to a unique transplant collaboration that will occur with the move to the Glickman Urological and Kidney Institute housed within the new Glickman Tower. To optimize the care and treatment of kidney/kidney pancreas transplant patients, surgical kidney transplant will be integrated with the Department of Nephrology and Hypertension in the same geographic area. The integration has immense implications for collegiality, coordination of patient services and discovery. Renal transplantation has a long and storied history since 196�, and the transplant theme area envisions synergistic participation (medicine, surgery) across multiple different areas (e.g., clinical transplant research protocols and immunology). Over the past three decades, diligent clinical care of our ESRD patients made the possibility of transplant a reality.
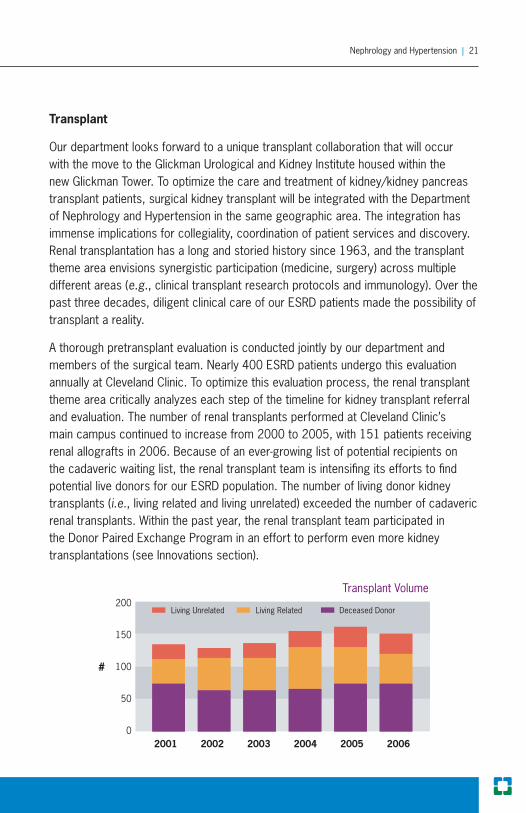
A thorough pretransplant evaluation is conducted jointly by our department and members of the surgical team. Nearly 400 ESRD patients undergo this evaluation annually at Cleveland Clinic. To optimize this evaluation process, the renal transplant theme area critically analyzes each step of the timeline for kidney transplant referral and evaluation. The number of renal transplants performed at Cleveland Clinic’s main campus continued to increase from 2000 to 2005, with 151 patients receiving renal allografts in 2006. Because of an ever-growing list of potential recipients on the cadaveric waiting list, the renal transplant team is intensifing its efforts to find potential live donors for our ESRD population. The number of living donor kidney transplants (i.e., living related and living unrelated) exceeded the number of cadaveric renal transplants. Within the past year, the renal transplant team participated in the Donor Paired Exchange Program in an effort to perform even more kidney transplantations (see Innovations section).
Transplant Volume200
150
100
50
02001 2002 2003 2004 2005 2006
Living Unrelated Living Related
#
Deceased Donor

22 | Nephrology and Hypertension 2006
To learn more about the pioneering studies of renal transplant immunology directed by Drs. Peter Heeger (Mt. Sinai Hospital, New York, NY) and Emilio Poggio, please see the Innovations section of the transplant theme area. The Innovations section also documents the pioneering clinical research of the nephrology and transplant teams in examining donor kidney volume and function upon outcomes following live donor kidney transplantation.
100
75
50
25
06 months 1 year 2 years
%
Kidney Graft Survival* 2002-2006
*Includes kidney/pancreas, kidney/liver and kidney/heart
Our patients continue to enjoy excellent patient and allograft survival. Over the past five years, data from more than 600 kidney transplants resulted in 95% patient survival and 90% allograft survival at one year.
100
75
50
25
06 months 1 year 2 years
%
Kidney Translant Patient Survival* 2002-2006

Nephrology and Hypertension | 2�
Hypertension
The hypertension theme area is organized as a center for investigation and management of patients with problematic hypertension issues. Focus is placed upon refractory hypertension, both primary and secondary in nature. Hypertension specialists have particular interest in secondary forms of hypertension that result from renovascular disease, primary aldosteronism and pheochromocytoma. Also, significant interest has been generated by identifying patients with “pre-hypertension” and the risks associated with this diagnosis.
The hypertension area is currently enrolling patients in a NIH-funded trial on renal artery stenosis and hypertension, entitled Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL). This randomized, controlled trial compares medical therapy versus renal artery stenting. Key clinical criteria for inclusion into the trial include:
Hypertension requiring two or more medications
Unilateral or bilateral renal artery stenosis angiographically
Serum creatinine <�.0 mg/dL
Referrals may be made to Drs. Pohl or Nally at 216.444.6776.
In a recent retrospective study of renal artery stenting in patients with impaired renal function (serum creatinine >1.5 mg/dL), the vascular surgery and nephrology investigators observed that 67% of patients demonstrated stabilization or improvement (>10% increase in eGFR) of renal function and blood pressure decreased significantly (J Vasc Surg 2007;45:101-109). A rapid decline in eGFR before intervention correlated with improvement after renal artery stenting.
Dr. Emmanuel L. Bravo and colleagues have a longstanding interest in the evaluation and management of patients with primary aldosteronism. After a comprehensive diagnostic evaluation, patients are offered management strategies
•
•
•
24 | Nephrology and Hypertension 2006
that include up-to-date surgical intervention and/or medical therapy. Dr. Bravo and hypertension colleagues collaborate closely with Dr. Inderbir Gill (Glickman Urological Institute) who has advanced the frontier of laparoscopic adrenal surgery. If medical therapy is elected, the team has extensive experience in the use of aldosterone antagonists and additional antihypertensive therapy.
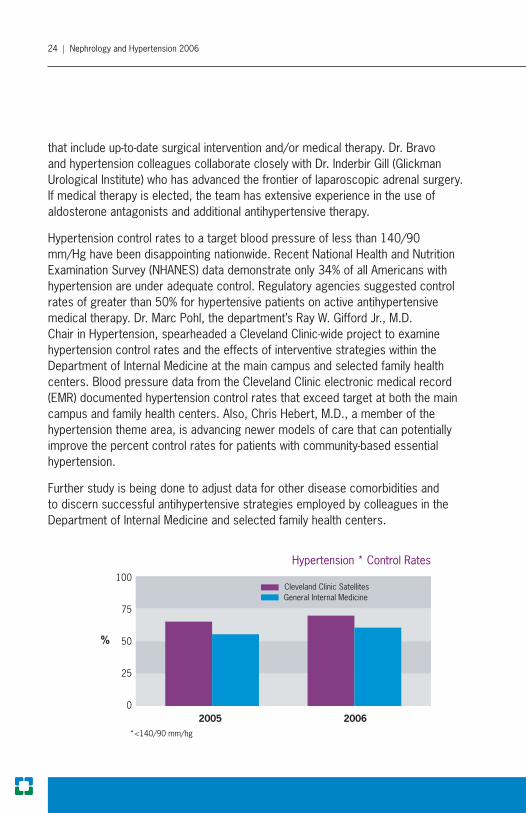
Hypertension control rates to a target blood pressure of less than 140/90 mm/Hg have been disappointing nationwide. Recent National Health and Nutrition Examination Survey (NHANES) data demonstrate only �4% of all Americans with hypertension are under adequate control. Regulatory agencies suggested control rates of greater than 50% for hypertensive patients on active antihypertensive medical therapy. Dr. Marc Pohl, the department’s Ray W. Gifford Jr., M.D. Chair in Hypertension, spearheaded a Cleveland Clinic-wide project to examine hypertension control rates and the effects of interventive strategies within the Department of Internal Medicine at the main campus and selected family health centers. Blood pressure data from the Cleveland Clinic electronic medical record (EMR) documented hypertension control rates that exceed target at both the main campus and family health centers. Also, Chris Hebert, M.D., a member of the hypertension theme area, is advancing newer models of care that can potentially improve the percent control rates for patients with community-based essential hypertension.
Further study is being done to adjust data for other disease comorbidities and to discern successful antihypertensive strategies employed by colleagues in the Department of Internal Medicine and selected family health centers.
Hypertension * Control Rates 100
75
50
25
02005 2006
Cleveland Clinic SatellitesGeneral Internal Medicine
%
*<140/90 mm/hg
Nephrology and Hypertension | 25
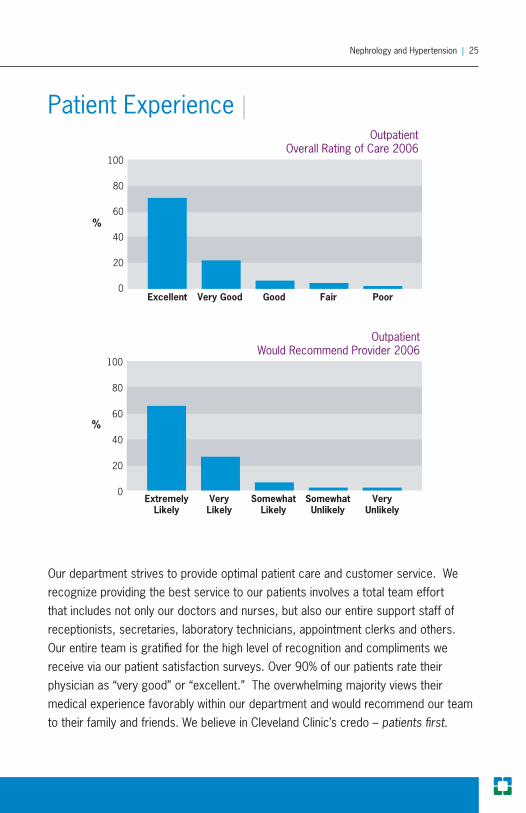
Our department strives to provide optimal patient care and customer service. We recognize providing the best service to our patients involves a total team effort that includes not only our doctors and nurses, but also our entire support staff of receptionists, secretaries, laboratory technicians, appointment clerks and others. Our entire team is gratified for the high level of recognition and compliments we receive via our patient satisfaction surveys. Over 90% of our patients rate their physician as “very good” or “excellent.” The overwhelming majority views their medical experience favorably within our department and would recommend our team to their family and friends. We believe in Cleveland Clinic’s credo – patients first.
Patient Experience | Outpatient
Overall Rating of Care 2006100
80
60
40
20
0Excellent Very Good Good Fair Poor
%
Outpatient Would Recommend Provider 2006
100
80
60
40
20
0Extremely
LikelyVeryLikely
SomewhatLikely
SomewhatUnlikely
VeryUnlikely
%

26 | Nephrology and Hypertension 2006
Since 1959, the Department of Nephrology and Hypertension has been integral to the care of patients with renal disease and hypertension. Brilliant scientists and clinicians paved the way for us to provide the very best care for individuals suffering from renal disease and hypertension. William J. Kolff developed the artificial kidney in 1948. Later, Harriet P. Dustan and Irving H. Page unraveled the causes of hypertension and developed the “mosaic theory” of hypertension, clarifying the realization that hypertension is rarely due to a single mechanism.
In 196�, kidney dialysis moved from research to clinical service in our department. Louise Spade received Cleveland Clinic’s first kidney transplant in January 196�, and Richard Crowley received the �,000th kidney transplant in 2005. A number of different teams have been instrumental in caring for patients, from treating this chronic disease and initiating cures for acute insults, to shepherding patients awaiting transplantation to dialysis to keep them in optimal condition for surgery. Patients suffering from acute injuries perioperatively have benefited immensely from the innovation, courage and hard work of physicians such as Magnus Magnusson, Kathryn Popowniak, Sat Nakamoto and Emil Paganini, as well as the scores of nurses and technicians who have made Cleveland Clinic’s acute dialysis service one of the best in the world.
We are grateful to our patients who have impelled us to seek answers, together forging treatment plans that, years ago, were barely dreams. Moving forward, only by questioning how we can do it better will we set the stage for future advancements that will predict, prevent and treat disease, adding quality-life years to people who, only a decade ago, faced low chances of survivals.
Advances in Nephrology & Hypertension
1935 Dr. I.H. Page announced the discovery of a substance released by the brain that causes hypertension.
1940s Dr. Page arrived at Cleveland Clinic and uncovered the link between high blood pressure and heart disease. He isolated the peptide angiotensin and serotonin – key players in hypertension1.
1943 Dr. Willem J. Kolff developed the first widely used and practical artificial kidney2.
1. The drug is hydrazo-phtalazine. Credit is given to earlier work of Dr. Francoise Reubi of Basle, Switzerland, as being the first to show the drug might be useful in essential hypertension. 2. Dr. Kolff’s work with the “tin-can” kidney prompted ideas that led to the improvement of the heart-lung machine, which, in the 1950s, led to the groundbreaking stopped-heart surgery at Cleveland Clinic.
Innovations |

Nephrology and Hypertension | 27
1945 Dr. Kolff was responsible for the first long-term survivor of ARF. Research Division was formally established.
1950s Drs. Harriet P. Dustan and Eugene F. Poutasse originated renovascular surgery for the treatment of high blood pressure.
1950 Dr. Kolff joined Cleveland Clinic’s Research Foundation.
1955 Dr. Kolff performed the first dialysis.
1956 More than 1�5 Cleveland Clinic patients were repaired with transplanted major human arteries (approximately one per day), saving lives of victims of ` malignant hypertension. Dr. Page was named director of the Research Division.
1957 Cleveland Clinic researchers reported chlorothiazide promoted kidney function and caused increased secretion of salt and water, an oral agent not requiring injection.
1957 Dr. Ray W. Gifford played a key role in classifying Raynaud’s disease and introduced a simplified method for evaluating hypertensive patients.
1958 Selection of Dr. David C. Humphrey as the first chairman of the Hypertension and Renal Disease Department.
1959 20,000 doctors heard Expert Panel telecast on hypertension featuring Drs. Page and Dustan.
1960s Dr. Magnus O. Magnusson pioneered kidney preservation research, lengthening the period available to seek suitable recipients and donors for transplantation.
1963 Dr. Kolff developed the twin coil artificial kidney. Dr. Kolff is named head of the Department of Artificial Organs�.
1963 The first cadaver kidney transplant was performed at Cleveland Clinic.
1964 Peritoneal dialysis (PD) was introduced at Cleveland Clinic, primarily as a holding procedure for hemodialysis.
�. Other kidney transplants had been done elsewhere on an experimental basis, but the main accomplishment at Cleveland Clinic was getting good enough results that the operation became an established and accepted treatment. Drs. Ralph A. Straffon, Eugene F. Poutasse and Willem J. Kolff pioneered kidney transplantation and revascularization.

28 | Nephrology and Hypertension 2006
1966 Dr. Kolff developed a dialysis machine and, later, a portable dialyzer. Dr. Page retired and edited the blood pressure “bible.”
1967 Drs. Subha Sen, F. Merlin Bumpus and Robert Smeby isolated a hormone-like phospholipid renin inhibitor.
1968 Dr. William Braun started the Histocompatibility Laboratory for kidney transplantation.
1969 Drs. Dustan, Page, M Ulrych and RC Tarazi discovered the association between renal hypertension and cardiac output. Drs. Page, Bumpus and Hans J. Schwarz discovered angiotensin controlled blood pressure and sought a way to inhibit the rennin-angiotensin system.
1970 Cleveland Clinic’s Board of Governors officially established the Department of Hypertension & Nephrology.
1970 Dr. Emmanuel L. Bravo joined Cleveland Clinic’s Research Division and established the Endocrine-Hypertension Research Laboratory. He continued Dr. Gifford’s research in pheochromocytoma and primary aldosteronism. Cleveland Clinic became the facility with the largest single-center clinical experience in diagnosing and treating these complex conditions.
1972 Dr. Braun was appointed Chief of Renal Transplant Section; the 450th kidney transplant was performed.
1972 The first glomerular filtration rate (GFR) test was performed in the Renal Function Lab at Cleveland Clinic, becoming the gold standard for renal function measurements.
1973 The new ambulatory Kidney Dialysis Center opened.
1974-76 Dr. Braun became the first president of the American Society of Histocompatibility and Immunogenetics.
1977 Drs. Sen and Bumpus discovered aldosterone stimulating factor (ASF), a hormone-like brain substance that affects aldosterone secretion in the adrenals.
Cleveland Clinic is the first in the United States to perform continuous dialysis therapy parallel with doctors in Germany.
Drs. Dustan and Gifford serve on the Executive Committee of JNC VI.

Nephrology and Hypertension | 29
1977-78 Drs. Paganini and Nakamoto performed the first SCUF/Ultrafiltration in the ICU.
1979 Cleveland Clinic’s Nephrology & Hypertension Department, represented by Dr. Marc A. Pohl, became a founding member of the Lupus Nephritis Study Group (LNSG), organized by Dr. Edmund J. Lewis.
1979 The West Side Dialysis Unit opened, the first satellite outpatient dialysis unit.
1986 The LNSG published results in the New England Journal of Medicine on plasmapheresis for treatment of lupus nephritis.
1989 Dr. Braun was elected president of the American Society of Transplantation.
1993 The LNSG became the Collaborative Study Group and studied the use of the ACE inhibitor captopril for treating Type I diabetic nephropathy. This landmark trial, in which Cleveland Clinic was a participating center, revolutionized the treatment of kidney disease.
2000 Drs. Charuhas Thakar and Paganini developed the risk assessment score for predicting renal failure in the ICU.
2001 The Collaborative Study Group studied the effects of irbesartan on Type II diabetes (IDNT), publishing again in the New England Journal of Medicine with international participation. Again, Cleveland Clinic was a participating center.
2001 Dr. Paganini inaugurated the Renal Assist Device (RAD) (bioartificial kidney) Study with Dr. H.D. Hume.
2003 Dr. Donald Vidt serves on the writing committee for JNC4 VII.
2004 RAD study results of the bioartificial kidney in ICU patients with acute renal failure published in Kidney International.
2006 More than 15,000 GFR measurements have been performed to date.
4. Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure.
�0 | Nephrology and Hypertension 2006
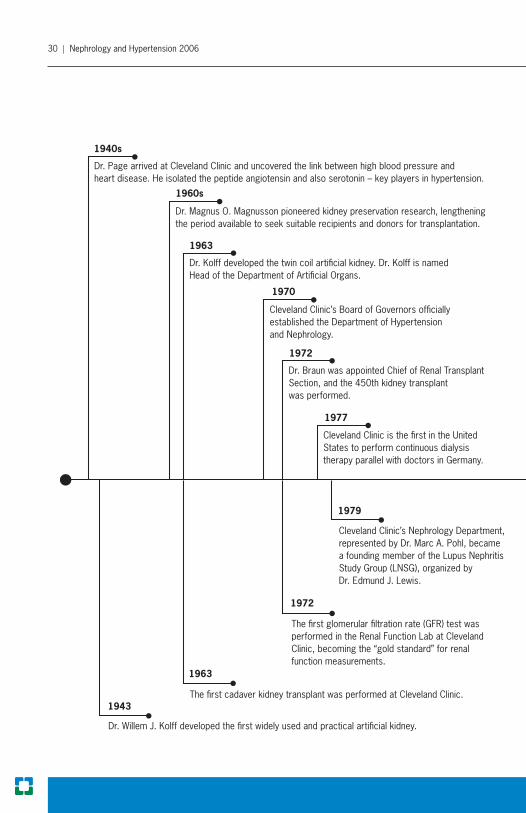
Dr. Page arrived at Cleveland Clinic and uncovered the link between high blood pressure and heart disease. He isolated the peptide angiotensin and also serotonin – key players in hypertension.
Dr. Magnus O. Magnusson pioneered kidney preservation research, lengthening the period available to seek suitable recipients and donors for transplantation.
Dr. Kolff developed the twin coil artificial kidney. Dr. Kolff is named Head of the Department of Artificial Organs.
Cleveland Clinic’s Board of Governors officially established the Department of Hypertension and Nephrology.
Dr. Braun was appointed Chief of Renal TransplantSection, and the 450th kidney transplant was performed.
Cleveland Clinic is the first in the United States to perform continuous dialysis therapy parallel with doctors in Germany.
The LNSG became the Collaborative Study Group and studied the use of the ACE inhibitor captopril for treating Type I diabetic nephropathy. This landmark trial, in which Cleveland Clinic was a participating center, revolutionized the treatment of kidney disease.
RAD study results of the bioartificial kidney in ICU patients with acute renal failure published in Kidney International.
More than 15,000 GFR measurements performed to date.
Drs. Charuhas Thakar and Paganini developed the risk assessment score for predicting renal failure in the ICU.
Cleveland Clinic’s Nephrology Department, represented by Dr. Marc A. Pohl, becamea founding member of the Lupus Nephritis Study Group (LNSG), organized by Dr. Edmund J. Lewis.
The first glomerular filtration rate (GFR) test wasperformed in the Renal Function Lab at ClevelandClinic, becoming the “gold standard” for renal function measurements.
The first cadaver kidney transplant was performed at Cleveland Clinic.
Dr. Willem J. Kolff developed the first widely used and practical artificial kidney.
1940s
1960s
1963
1970
1972
1977
1993
1943
1963
1972
1979
2000
2006
2004

Nephrology and Hypertension | �1
Dr. Page arrived at Cleveland Clinic and uncovered the link between high blood pressure and heart disease. He isolated the peptide angiotensin and also serotonin – key players in hypertension.
Dr. Magnus O. Magnusson pioneered kidney preservation research, lengthening the period available to seek suitable recipients and donors for transplantation.
Dr. Kolff developed the twin coil artificial kidney. Dr. Kolff is named Head of the Department of Artificial Organs.
Cleveland Clinic’s Board of Governors officially established the Department of Hypertension and Nephrology.
Dr. Braun was appointed Chief of Renal TransplantSection, and the 450th kidney transplant was performed.
Cleveland Clinic is the first in the United States to perform continuous dialysis therapy parallel with doctors in Germany.
The LNSG became the Collaborative Study Group and studied the use of the ACE inhibitor captopril for treating Type I diabetic nephropathy. This landmark trial, in which Cleveland Clinic was a participating center, revolutionized the treatment of kidney disease.
RAD study results of the bioartificial kidney in ICU patients with acute renal failure published in Kidney International.
More than 15,000 GFR measurements performed to date.
Drs. Charuhas Thakar and Paganini developed the risk assessment score for predicting renal failure in the ICU.
Cleveland Clinic’s Nephrology Department, represented by Dr. Marc A. Pohl, becamea founding member of the Lupus Nephritis Study Group (LNSG), organized by Dr. Edmund J. Lewis.
The first glomerular filtration rate (GFR) test wasperformed in the Renal Function Lab at ClevelandClinic, becoming the “gold standard” for renal function measurements.
The first cadaver kidney transplant was performed at Cleveland Clinic.
Dr. Willem J. Kolff developed the first widely used and practical artificial kidney.
1940s
1960s
1963
1970
1972
1977
1993
1943
1963
1972
1979
2000
2006
2004

�2 | Nephrology and Hypertension 2006
A brief discussion of some of the innovations within each theme area offers an exciting glimpse into the frontiers of nephrology. As with the outcomes data, each of the innovations is presented in association with the appropriate theme area.
Chronic Kidney Disease (CKD): With the reorganization of the department, the most exciting innovation within CKD is the establishment of a formal CKD Clinic. The CKD Clinic will accept patients referred from Cleveland Clinic and outside physicians for the evaluation and management of CKD. Enrollment of patients in the CKD Clinic and use of the Electronic Medical Record (EMR) will permit the establishment of a CKD database that captures patients’ demographics, clinical parameters, treatments and outcomes (hospitalizations, achievement of clinical treatment targets, and survival years). The CKD database in the EMR will permit us to obtain outcomes data on important issues such as anemia management, blood pressure control, dialysis and transplant education, and dialysis access. In addition to providing these significant outcomes data, the CKD database will be fertile ground for identifying and enrolling patients in clinical research projects critical to understanding disease, deciding new therapeutic strategies, and preventing disease in future generations. Referring physicians may contact the CKD Clinic or Cleveland Clinic EMR’s referral system at 216/444-6771.
The anemia management project is one of our pioneering success stories, as patient numbers and the percentage of CKD patients brought to hemoglobin targets continue to grow. This clinical success fostered an investigative effort headed by Drs. Saul Nurko and Paul Fox at the Lerner Research Institute. Dr. Nurko and his team are investigating the role of hepcidin in the utilization of iron in a murine model of CKD anemia being treated with erythropoietin (EPO). In an effort to investigate the molecular mechanisms involved in CKD anemia, response to EPO and iron metabolism, the research team characterized the liver transcription profile of hepcidin, a novel iron regulatory hormone, in a model of CKD. Hepcidin may be regulated by three different pathways: iron, inflammation, and hypoxia and/or

Nephrology and Hypertension | ��
anemia. Most investigators believe hepcidin inhibits iron absorption, placental iron transfer and iron release from the reticuloendothelial macrophages. CKD is a pathological state wherein the inter-organ communication between EPOs need for iron and iron release from stores seems altered. The research has shown a �0% reduction in hepcidin expression in mice with CKD. A greater decrease (50%) was observed in mice treated with and responded to EPO. The team speculates a decreased hepatic hepcidin expression is probably necessary for EPO response, by facilitating the release of iron by the reticuloendothelial system. As Dr. Nurko demonstrated, hepcidin may be crucial in this experimental model and may play a substantial role in the clinical management of CKD anemia with EPO. Results of these preliminary studies are quite promising.
Under the guidance of Dr. Martin J. Schreiber, Jr., our department is participating in the NIH-sponsored Chronic Renal Insufficiency Cohort (CRIC) study, an observational trial of patients with CKD. This observational trial will collect pertinent data about progression of CKD and its complications over five years. Referring physicians or interested patients with questions about the CRIC study may contact Carol Horner, RN at 216/444-�56�.
Under the direction of Dr. William Braun, two randomized, controlled trials were initiated in patients with autosomal dominant polycystic kidney disease (ADPKD). In the Halt Progression of Polycystic Kidney Disease (HALT-PKD) trial, interruption of the renin angiotensin system with angiotensin-converting enzyme (ACE) inhibitors and/or angiotensin receptor blocker (ARB) therapy is compared to a placebo to examine the effect on progression of disease and cyst size detected by computer-assisted magnetic resonance imaging (MRI) studies. A second randomized, controlled trial uses similar technologies to determine the effect of Rapamune (Sirolimus) versus placebo upon disease progression. Referring physicians or interested patients who would like to learn more about these ADPKD trials can contact Dr. Braun or Rita Spirko, RN at 216/444-4680.

�4 | Nephrology and Hypertension 2006
As noted in the Outcomes section, the department has also been instrumental in validating the utility and limitations of estimates of GFR (eGFR) in various patient populations. Drs. Phillip Hall and Emilio Poggio, along with their GFR team, are also collaborating with national investigators to pursue the measurement of cystatin C as an improved estimate of GFR, especially in those with preserved or normal kidney function. A recent presentation of this collaborative group at the American Society of Nephrology in November 2006 suggests that combining both the serum creatinine and cystatin C measurement in an MDRD-type equation produces superior results across the entire spectrum of kidney function. Dr. Poggio and his collaborators will be further refining this exciting area of research.
Dialysis: Dr. Paganini and the ICU Nephrology Team continue to push the frontiers of acute renal failure (ARF) management in the critically ill patient. As noted in the departmental Outcomes section, Dr. Charuhas Thakar and colleagues developed an accurate predictive score to identify patients with a high likelihood of developing ARF following open-heart surgery. In addition to helping counsel patients and cardiac surgeons about potential ARF risk, the predictive score index identifies a subset of patients at high risk for perioperative ARF, who may be excellent candidates for preventive strategies and intervention trials. As can be seen in the departmental bibliography of “New Knowledge” section, Drs. Paganini, Thakar and national collaborators have further refined their predictive model and scoring system. Equally important, the Cleveland Clinic Nephrology and Cardiac Transplantation teams have developed a related risk stratification score for ARF requiring dialysis after cardiac transplantation.
The pleiotrophic effects of EPO administration to patients undergoing open heart surgery are being studied in patients at high risk for perioperative ARF. Dr. Sevag Demirjian was awarded an industry-funded grant to determine if EPO administration reduces the rates of ARF in a patient population deemed at high risk for ARF based on the previously predictive scoring system.
Nephrology and Hypertension | �5
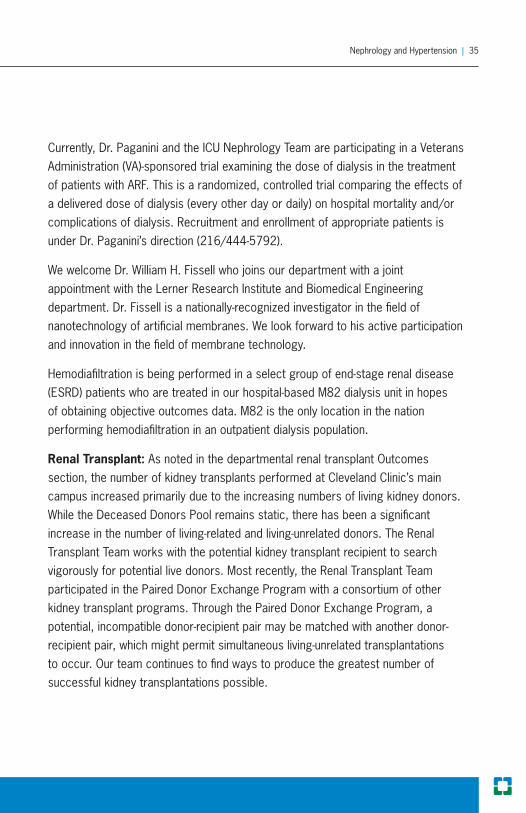
Currently, Dr. Paganini and the ICU Nephrology Team are participating in a Veterans Administration (VA)-sponsored trial examining the dose of dialysis in the treatment of patients with ARF. This is a randomized, controlled trial comparing the effects of a delivered dose of dialysis (every other day or daily) on hospital mortality and/or complications of dialysis. Recruitment and enrollment of appropriate patients is under Dr. Paganini’s direction (216/444-5792).
We welcome Dr. William H. Fissell who joins our department with a joint appointment with the Lerner Research Institute and Biomedical Engineering department. Dr. Fissell is a nationally-recognized investigator in the field of nanotechnology of artificial membranes. We look forward to his active participation and innovation in the field of membrane technology.
Hemodiafiltration is being performed in a select group of end-stage renal disease (ESRD) patients who are treated in our hospital-based M82 dialysis unit in hopes of obtaining objective outcomes data. M82 is the only location in the nation performing hemodiafiltration in an outpatient dialysis population.
Renal Transplant: As noted in the departmental renal transplant Outcomes section, the number of kidney transplants performed at Cleveland Clinic’s main campus increased primarily due to the increasing numbers of living kidney donors. While the Deceased Donors Pool remains static, there has been a significant increase in the number of living-related and living-unrelated donors. The Renal Transplant Team works with the potential kidney transplant recipient to search vigorously for potential live donors. Most recently, the Renal Transplant Team participated in the Paired Donor Exchange Program with a consortium of other kidney transplant programs. Through the Paired Donor Exchange Program, a potential, incompatible donor-recipient pair may be matched with another donor-recipient pair, which might permit simultaneous living-unrelated transplantations to occur. Our team continues to find ways to produce the greatest number of successful kidney transplantations possible.

�6 | Nephrology and Hypertension 2006
Loss of the allograft due to immune-mediated injury remains a major obstacle to long-term kidney transplant success. Drs. Peter Heeger and Emilio Poggio of the Transplant Immunology Team were awarded a collaborative NIH grant to study some innovative immune monitoring techniques. Their goal is to identify, and perhaps prevent, immune injury to the allograft. The Clinical Trial in Organ Transplantation (CTOT) is an ongoing, multi-center, NIH-sponsored trial to evaluate novel immune biomarkers for transplant rejection. Referring physicians or interested patients who would like to learn more about the CTOT can contact Dr. Poggio or Leslie Iosue, RN at 216/444-2991.
Employing cutting-edge technology, the Renal Transplant Team has also investigated the effect of living donor kidney volume on subsequent allograft function. By measuring living donor kidney volumes by �-D helical computed tomography (CT) scanning, the team showed large kidney volumes are associated with better GFR rates, post-transplant and less rejection. Donor volumes greater than 120 cc/1.7� m2, iGFR greater than 55 ml/min/1.7� m2, and age less than 45 years are all associated with better estimates of GFR following kidney transplantation.
75
60
45
302 years1 year6 monthsTaxed GFR
> 55ml/min/1.73m2< 55
MDRDeGFR
(ml/min/1.73m2)
75
60
45
302 years1 year6 monthsTaxed GFR
MDRDeGFR
(ml/min/1.73m2)
> 120cc/1.73m2< 120
p < 0.0001 for each time point
p < 0.0001 for each time point

Nephrology and Hypertension | �7
Hypertension: This theme area is organized as a consultative service to evaluate and manage patients with refractory hypertension. The Hypertension Research Team collaborated with an extramural company and Cleveland Clinic’s Vascular Surgery to investigate the electrical activation of the carotid body reflex in helping control resistant hypertension. As part of the CVRx Study design, selected patients will have a device similar to a pacemaker implanted. This device will send electrical signals to the carotid body reflex. In canine models, this device initiated a hemodynamic response to electrical activation of the carotid body reflex with a reduction in systolic blood pressure. The innovative Cleveland Clinic Hypertension Research Team will collaborate with vascular surgery to ascertain whether this device may be safely used in human subjects. Further studies are necessary to learn whether the electrical activation device can be used in combination with usual antihypertensive medications to produce a synergistic effect and control systemic hypertension. Referring physicians or interested patients who wish more information about the study may call Dr. Brian Stephany at 216/444-5�82.
The department is delighted to announce the arrival of Qingyu Wu, M.D., Ph.D. with a joint appointment to the Lerner Research Institute and Molecular Cardiology. Dr. Wu is a recognized research scientist in the field of hypertension and in the role of anatriuretic peptides (ANP) on blood pressure levels, especially in the African American patient.
75
60
45
302 years1 year6 monthsTaxed GFR
MDRDeGFR
(ml/min/1.73m2)
> 45 yo< 5
p = NS for the first two time points and p < 0.01 for the last two time points
�8 | Nephrology and Hypertension 2006
New Knowledge |
Selected Publication Highlights
Research and education are key ingredients in all our clinical activities. Here is a list of selected publications from our department that highlight some of our most recent activities.
Boyle JM, Moualla S, Arrigain S, Worley S, Bakri MH, Starling RC, Heyka R, Thakar CV. Risks and outcomes of acute kidney injury requiring dialysis after cardiac transplantation. American Journal of Kidney Diseases 2006;48:787-796.
Chertow GM, Soroko SH, Paganini EP, Cho KC, Himmelfarb J, Ikizler TA, et al. Mortality after acute renal failure: models for prognostic stratification and risk adjustment. Kidney International 2006;70:1120-1126.
Cho KC, Himmelfarb J, Paganini E, Ikizler TA, Soroko SH, Mehta RL, et al. Survival by dialysis modality in critically ill patients with acute kidney injury. J Am Soc Nephrol 2006;17:�1�2-�1�8.
Hix JK, Thakar CV, Katz EM, Yared JP, Sabik J, Paganini EP. Effect of off-pump coronary artery bypass graft surgery on postoperative acute kidney injury and mortality. Crit Care Med 2006;�4:2979-298�.
Liu KD, Himmelfarb J, Paganini E, Ikizler TA, Soroko SH, Mehta RL, Chertow GM. Timing of initiation of dialysis in critically ill patients with acute kidney injury. Clin J Am Soc Nephrol 2006;1:915-919.
Schreiber MJ, Jr. Minimizing perioperative complications in patients with renal insufficiency. Cleve Clin J Med 2006;7�(Suppl 1):S116-S120.

Nephrology and Hypertension | �9
Poggio ED, Clemente M, Hricik DE, Heeger PS. Panel of reactive T cells (PRT) as a measure of cellular alloimmunity in kidney transplant candidates. Journal of the American Society of Nephrology. 2006;17: 564-572.
Poggio ED, Wang X, Weinstein DM, Issa N, Dennis VW, Braun WE, et al. Assessing glomerular filtration rate by estimation equations in kidney transplant recipients. Am J Transpl 2006;6:100-108.
Poggio ED, Hila S, Stephany B, Fatica R, Krishnamurthi V, del Bosque C, Braun WE, et al. Donor kidney volume and outcomes following live donor kidney transplantation. Am J Transpl 2006;6:616-624.
Poggio ED, Hila S, Stephany B, Fatica R, Krishnamurthi V, del Bosque C, Braun WE, et al. Donor kidney volume and outcomes following live donor kidney transplantation. Am J Transpl 2006;6:616-624.
Poggio ED, Hall PM. Estimation of glomerular filtration rate by creatinine-based formulas: Any room for improvement? Medical Knowledge Self-Assessment Program 2006;5:1�1-140.
Duclos AJ, Krishnamurthi V, Lard M, Poggio E, Kleeman M, Winans C, Fatica R, Nurko, S. Prevalence and clinical course of BK virus nephropathy in pancreas after kidney transplant patients. Transplantation Proceedings. 2006;�8:�666-�572.
Stephany BR, Augustine JJ, Krishnamurthi V, Goldfarb DA, Flechner SM, Braun WE, Hricik DE, Dennis VW, Poggio ED. Differences in qualitative proteinuria and graft function in de novo sirolimus-based versus calcineurin inhibitor-based immunosuppression in live donor kidney transplantation. Transplantation 2006;15:�68-�74.
40 | Nephrology and Hypertension 2006
Valujskikh A, Zhang Q, Heeger PS. CD8 T cells specific for a donor-derived, self-restricted transplant antigen are nonpathogenic bystanders after vascularized heart transplantation in mice. Journal of Immunology. 2006;176:2190-2196.
Kashyap VS, Sepulveda RN, Bena JF, Nally JV, Poggio ED, Greenberg RK, Yadav JS, Ouriel K. The management of renal artery atherosclerosis for renal salvage: Does stenting help? J Vasc Surg in press.
Nurko S. Anemia in chronic kidney disease: causes, diagnosis, treatment. Cleve Clin J Med 2006;7�:289-297.
Hall PM. Foreword: Hyponatremia: More to the story than disordered sodium homeostasis. Cleve Clin J Med 2006;7�(Suppl �):S2-S�.
Hall PM, ed. Hyponatremia and the role of vasopressin. Cleve Clin J Med. 2006;7�(Suppl �):S1-S��.
Hall PM. Prevention of progression in diabetic nephropathy. Diabetes Spectrum 2006;19:18-24.
Vootukuru V, Liew YP, Nally JV. Pemetrexed-induced acute renal failure, nephrogenic diabetes insipidus, and renal tubular acidosis in a patient with non-small cell lung cancer. Medical Oncology 2006;2�:419-22.
Davidson MB, Hix JK, Vidt DG, Brotman DJ. Association of impaired diurnal blood pressure variation with a subsequent decline in glomerular filtration rate. Arch Intern Med 2006;166:846-852.
Davidson MB, Hix JK, Vidt DG, Brotman DJ. Association of impaired diurnal blood pressure variation with a subsequent decline in glomerular filtration rate. Arch Intern Med 2006;166:846-852.

Nephrology and Hypertension | 41
Vidt DG, Harris S, McTaggart F, Ditmarsch M, Sager PT, Sorof JM. Effect of short-term rosuvastatin treatment on estimated glomerular filtration rate. Am J Cardiol 2006;97:1602-1606.
Bravo EL: Secondary hypertension: Mineralocorticoid excess states. In: Black HR, Elliott WJ, eds. Hypertension, A Companion to Braunwald’s Heart Disease. Philadelphia: Saunders; 2007:106-118.
Issa NS, Stephany B, Fatica R, Nurko S, Krishnamurthi V, Goldfarb DA, Braun WE, Dennis VW, Heeger PS, Poggio ED. Donor factors influencing graft outcomes in live donor kidney transplantation. In press.
Nally JV Jr. Management of renovascular hypertension. In: Izzo JL, Black HR, eds. Hypertension Primer. 4th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins,Transplantation; 2007; 8�:59�-599.
Pohl MA, Wilcox CS. Renal artery stenosis, renal vascular hypertension, and ischemic nephropathy. In: Schrier RW, ed. Diseases of the Kidney & Urinary Tract. 8th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2007:1272-1�25.
Pohl MA, Wilcox CS. Renovascular hypertension. In: Feehally J, Floege J, Johnson RJ, eds. Comprehensive Clinical Nephrology. �rd ed. New York: Elsevier; 2007, in press.
Goldfarb, DA, Nally, JV Jr, Schreiber, MJ Jr. Etiology, pathogenesis, and management of renal failure. In: Wein, AJ, Kavoussi, LR, Novick, AC, Partin, AW, Peters CA, eds Campbell-Walsh Urology. 9th ed. Philadelphia: Elsevier 2007.

42 | Nephrology and Hypertension 2006
Martin J. Schreiber Jr., M.D. Chairman, Department of Nephrology and Hypertension
Appointed: 2005
Medical School: Bowman Gray School of Medicine, Winston-Salem, NC
Internship: Cleveland Clinic, Cleveland, OH
Residency: Cleveland Clinic, Cleveland, OH
Specialty Training: Massachusetts General Hospital, Boston, MA Other Education: B.S., John Carroll University, Cleveland, OH
Specialty Interests: Chronic kidney disease, end-stage renal disease and renal replacement therapies
Staff Listing | Chairman

Nephrology and Hypertension | 4�
Staff Listing |
Chairman Martin J. Schreiber Jr., M.D.
Quality Review Officer Joseph V. Nally Jr., M.D.
Staff Emil P. Paganini, M.D, Head, Section of Dialysis and Extracorporeal Therapy
Marc A. Pohl, M.D., Head, Section of Hypertension
William E. Braun, M.D.
Sevag Demirjian, M.D.
Richard A. Fatica, M.D.
Christopher Hebert, M.D. Robert J. Heyka, M.D.
Priya Kalahasti, M.D.
Saul Nurko, M.D.
Emilio Poggio, M.D.
James Simon, M.D. (July, 2007)
Brian R. Stephany, M.D.
Consultants Emmanuel L. Bravo, M.D.
Phillip M. Hall, M.D.
Physician Scientists
William Fissell, M.D.
Qingyu Wu, M.D., Ph.D.
Physician Extenders
Susan Busch, CNP
Amy Colbeck, CNP
Denise Coyner, MSN, CNP
Riana Naude, MSN, CNP
Jennifer Lyons, MSN, CNP
Karen Mallow, CNP
Caryl Richards, PA
Leslie Smith, MSN, CNP

44 | Nephrology and Hypertension 2006
Nephrology Appointment Line:
216.444.6771
For more details about Nephrology and Hypertension visit clevelandclinic.org/nephrology
Department Contacts | How to Refer Patients

Nephrology and Hypertension | 45
Main Campus Department of Nephrology and Hypertension 9500 Euclid Avenue / A51 Cleveland, Ohio 44195
Department Line 216.444.6766
Appointment Line 216.444.6771
Ohio Renal Care Group / Fresenius Medical Care Site of Service
Fresenius East (Fairhill) 1120� Stokes Blvd. Cleveland, Ohio 44142
Fresenius North Randall 4750 Northfield Rd. North Randall, Ohio 44128
Fresenius West 14670 Snow Rd. Brookpark, Ohio 44142
Fresenius Willoughby 5105 SOM Center Rd. Kaiser Building, �rd floor Willoughby, Ohio 4409�
Fresenius Solon 6020 Enterprise Parkway Solon, Ohio 441�9
Fresenius Farnsworth �764 Pearl Rd. Cleveland, Ohio 44109
Lake Erie
ClevelandClinicCleveland
Locations

46 | Nephrology and Hypertension 2006
Cleveland Clinic Overview |
Cleveland Clinic, founded in 1921, is a not-for-profit academic medical center that integrates clinical and hospital care with research and education. Today, 1,700 Cleveland Clinic physicians and scientists practice in 120 medical specialties and subspecialties.
Cleveland Clinic’s main campus, with 41 buildings on 1�0 acres in Cleveland, Ohio, includes a 1,000-bed hospital, outpatient clinic, subspecialty centers and supporting labs and facilities. Cleveland Clinic also operates 1� family health centers, eight community hospitals, two affiliate hospitals, and a medical facility in Weston, Florida.
At the Cleveland Clinic Lerner Research Institute, hundreds of principal investigators, project scientists, research associates and postdoctoral fellows are involved in laboratory-based research. Total annual research expenditures exceed $150 million from federal agencies, non-federal societies and associations, and endowment funds. In an effort to bring research from bench to bedside, Cleveland Clinic physicians are involved in more than 2,400 clinical studies at any given time.
In September 2004, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University opened and will graduate its first �2 students as physician- scientists in 2009.
For more details about Cleveland Clinic, visit clevelandclinic.org
Nephrology and Hypertension | 47
Online Services |
eCleveland Clinic
eCleveland Clinic uses state-of-the-art digital information systems to offer several services, including remote second opinions through a secure Web site to patients around the world; personalized medical record access for patients; patient treatment progress access for referring physicians (see below); and imaging interpretations by the Department of eRadiology’s subspecialty trained academic radiologists. For more information, please visit eclevelandclinic.org.
DrConnect
Online Access to Your Patient’s Treatment Progress
Whether you are referring from near or far, our new eCleveland Clinic service, DrConnect, can streamline communication from Cleveland Clinic physicians to your office. This new online tool offers you secure access to your patient’s treatment progress at Cleveland Clinic. With one-click convenience, you can track your patient’s care using the secure DrConnect Web site. To establish a DrConnect account, visit eclevelandclinic.org or e-mail [email protected].
MyConsult
MyConsult Remote Second Medical Opinion is a secure, online service providing specialist consultations and remote second medical opinions for more than 600 life-threatening and life-altering diagnoses. MyConsult remote second medical opinion service allows you to gather information from nationally recognized specialists without the time and expense of travel. For more information, visit eclevelandclinic.org/myconsult, e-mail [email protected] or call 800.22�.227�, ext 4�22�.

48 | Nephrology and Hypertension 2006
How to Refer Patients 24/7 Hospital Transfers or Physician Consults 800.55�.5056
General Information 216.444.2200
Hospital Patient Information 216.444.2000
Patient Appointments 216.444.227� or 800.22�.227�
Medical Concierge Complimentary assistance for out-of-state patients and families 800.22�.227�, ext. 55580, or email: [email protected]
International Center Complimentary assistance for international patients and families 216.444.6404 or visit www.clevelandclinic.org/ic
Cleveland Clinic in Florida 866.29�.7866
www.clevelandclinic.org
Cleveland Clinic Contact Numbers |

Cleveland Clinic is determined to exceed the expectations of patients,
families and referring physicians. In light of this goal, we are committed
to providing accurate and timely information about our patient care.
Through participation in national initiatives, we support transparent public
reporting of healthcare quality data and participate in the following public
reporting initiatives:
• Joint Commission Performance Measurement Initiative (www.qualitycheck.org)
• Centers for Medicare and Medicaid (CMS) Hospital Compare (www.hospitalcompare.hhs.gov)
• Leapfrog Group (www.leapfroggroup.org)
• Ohio Department of Health Service Reporting (www.odh.state.oh.us)
In addition, this publication was produced to assist patients and referring
physicians in making informed decisions. To that end, information about
care and services is provided, with a focus on outcomes of care. For
more information, please visit the Cleveland Clinic Quality Web site at
clevelandclinic.org/quality.
Cover photograph by Stephen Travarca





























