Embed Size (px)
Citation preview

Slide 1
2007 New Data ItemsData Due in:
Days
In this presentation we will discuss five new data items that were introduced with the 2007 MPH Coding Rules.

Slide 2
2
5 New Data Items
• Ambiguous Terminology• Date of Conclusive Terminology
• Multiplicity Counter • Date of Multiple Tumors • Type of Multiple Tumors Reported as One
Primary
To help document and describe some of the situations that result from the new rules, for example two breast tumors abstracted as a single primary, it was determined it would be best to do this with a few new data items. There are five new data items. There are 3 new data items used directly with the Multiple Primary Rules to help describe when there was more than one tumor abstracted as a single primary. These data items are: •Multiplicity Counter •Date of Multiple Tumors (plus the Flag field) •Type of Multiple Tumors Reported as One Primary The other two new data items are not part of the multiple primary rules but were introduced at the same time. They have more to do with the basis of how the tumor was diagnosed. These data items are: •Ambiguous Terminology •Date of Conclusive Terminology (plus the Flag field)

Slide 3
3
Rational for new data items
• Identify cases in which the diagnosis was based on ambiguous terminology.– Prostate: probably adenocarcinoma– Prostate: Adenocarcinoma
• Identify cases in which there was more than one tumor abstracted as a single primary.
When there is a statement of diagnosis, physicians may use terms to describe how conclusive they feel the diagnosis is. These terms are considered to be ambiguous and include terms such as probable, possible, suspects, and suggests. The terms probable and suspects are ambiguous terms that DO constitute a diagnosis, probably adenocarcinoma, for example. The terms possible and suggests are ambiguous terms that DO NOT constitute a diagnosis. Other times, ambiguous terms are not used at all. There is just a strict statement of cancer, prostate adenocarcinoma, for example. These data items help let the user of the data know if the diagnosis was based on ambiguous or conclusive terminology. This information is helpful when considering whether to include a case in special studies or to contact patients for follow-up. If there are two or more tumors, the physician may say this is a multiple primary, especially if only one of the tumors was biopsied. However, when you apply this case to the rules, the instructions state this would be one primary. The word “primary” is used in two different ways. Physicians don’t always mean a new primary the way a cancer registrar uses the term. A new primary to the registrar means de novo, or one is not a metastasis from another tumor. The tumors started growing independently of each other. When we talk about a new primary we are using it in the epidemiological sense. If there are two infiltrating duct primaries there are two de novo tumors. Even though these did start growing independent of each other, the epidemiological interpretation says these should be coded as a single primary. The new multiplicity data item would identify this as a single primary, but with two separate tumors. The benefit of this data item is that this information is still available to the physician and for studies.

Slide 4
4
New Data Items
• Code only for cases diagnosed on or after 1/1/2007
• What if the date of diagnosis is before 1/1/2007?– Leave these 5 data items blank
These data items are only collected for cases diagnosed on or after January 1, 2007. For cases diagnosed prior to 2007, these data items should be left blank. Your software vendor may instruct you to handle these differently. If so, that’s ok. But, as a general instruction, these should be left blank. There is no benefit in collecting them because they were not collected consistently for all cases diagnosed prior to 2007.

Slide 5
5
Ambiguous Terminology
• Identifies all cases accessioned based on ambiguous terminology. Includes:– Death Clearance only– Autopsy only
• Allows identification of cases in database– Cases excluded from research studies – Direct patient contact not recommended
Page 335
The coding instructions for these data items begin on page 335 of the MPH Coding Rules Manual. It is recommended that you follow along in your manual as we discuss these data items. The first data item we will discuss is the Ambiguous Terminology data item. This data item identifies all cases, including Death Clearance only (in central registries) and autopsy only cases, that were accessioned based on ambiguous terminology.

Slide 6
6
• Ambiguous Terms– Reportable case when an ambiguous term is used as
basis for a diagnosis– Only use terms listed on page 337
• Conclusive Terms– A clear and definite statement of cancer – Statement may be from:
• Physician (clinical diagnosis)• Laboratory test• Autopsy, cytologic findings, and/or pathology
Ambiguous Terminology
This data items looks at two elements. • Was the diagnosis made using ambiguous terms or conclusive terms? • And, if it was an ambiguous term, at any time later did they confirm the diagnosis with a conclusive
term? Only the ambiguous terms provided with this data item are to be used to say that the basis for the
diagnosis used ambiguous terminology. These terms are listed on page 337.

Slide 7
7
Ambiguous Terms that are Reportable
• Apparent(ly)• Appears*• Comparable with*• Compatible with*• Consistent with• Favor(s)• Malignant appearing*
• Most likely• Presumed• Probable• Suspect(ed)• Suspicious (for)• Typical (of)
* Effective with cases diagnosed 1/1/1998 and later
Listed here are the valid terms. Notice that “consistent with” is considered ambiguous terminology for assigning this data item.

Slide 8
8
Code Label Definition Time Frame0 Conclusive term There was a conclusive diagnosis
within 60 days of the original diagnosis. Case was accessioned based on conclusive terminology. Includes all diagnostic methods such as clinical diagnosis, cytology, pathology, etc.
Within 60 days of the date of initial diagnosis.
1 Ambiguous term only
The case was accessioned based only on ambiguous terminology. There was no conclusive terminology during the first 60 daysfollowing the initial diagnosis. Includes all diagnostic methods except cytology.Note: Cytology is excluded because registrars are not required to collect cases with ambiguous terms describing a cytology diagnosis.
N/A
Use Code 0 when a case is accessioned based on conclusive terminology. The diagnosis had clear and definite terminology describing the malignancy within two months of the original diagnosis. Note: Usually the patient undergoes a diagnostic work-up because there is a suspicion of cancer (ambiguous terminology). For example, a mammogram may show calcifications suspicious for carcinoma. The date of the mammogram is still the date of initial diagnosis. When there is a clear and definite diagnosis within two months of that mammogram (date of initial diagnosis) such as the pathology from an excisional biopsy showing intraductal carcinoma, assign a code 0. Examples of a conclusive diagnosis: 1. Adenocarcinoma in TURP chips. 2. Mammogram suspicious
for DCIS. Excisional biopsy 1 week later positive for DCIS.
Use Code 1 when a case is accessioned based on ambiguous terminology and there is no clear and definite terminology used to describe the malignancy within 60 days
of the date of initial diagnosis. The diagnosis may be from a pathology report, a radiology report, an imaging report, or on the medical record.
Examples of an ambiguous diagnosis: 1. Chest MRI shows a malignant appearing
2. Pt with elevated PSA admitted for TRUS Biopsy. Pathology: Prostatic chips
lesion in the right upper lobe. Patient refused further workup or treatment.
consistent with
adenocarcinoma. No further information is available.

Slide 9
9
Code Label Definition Time Frame
2 Ambiguous term followed by conclusive term
The case was originally assigned a code 1 (was accessioned based only on ambiguous terminology). More than 60 days after the initial diagnosis the information is being updated to show that a conclusive diagnosis was made by any diagnostic method including clinical diagnosis, cytology, pathology, autopsy, etc.
60 days or more after the date of diagnosis
9 Unknown term
There is no information about ambiguous terminology.
N/A
Use Code 2 when a case was originally accessioned based on ambiguous terminology, but was then followed by clear and definite terminology more than 60 days
after the initial diagnosis.
For example, follow-back to a physician or in a subsequent readmission (following the initial 60 day period) may eventually confirm the cancer using a conclusive cancer term. If so, change the code of 1 to a Code 2.
Examples: A biopsy of the thyroid reads: most likely thyroid cancer. Three months later
a biopsy is positive for papillary follicular cancer. The case would have been coded 1 Ambiguous term only when originally abstracted because of the use of the ambiguous terminology “most likely”. The code should be changed 2 - Ambiguous term followed by conclusive term.

Slide 10
10
Date of Conclusive Terminology
• Date of definite statement of malignancy
• Abstractor must enter the valid date that the malignancy was described conclusively
• May have to change the code in the “Ambiguous Terminology” field from 1 to 2
Page 338
The next data item is the Date of Conclusive Terminology. This data items describes the date that a definite statement of malignancy was made. This will only apply when the “Ambiguous Terminology” was originally a code 1 but then changed to a code 2 when conclusive terminology was used more than 60 days after the date of diagnosis. These data items are followed and updated over time and will be something that you will have to remember to look for and update if appropriate.

Slide 11
Date and Date Flag Fields
• Read pages 7-8 in the FORDS (Coding Dates)
• See next slide for special codes that can be used in this course.
• Flag fields will not be included in the exercises in this lesson.
11
Begin by reading the section on Coding Dates in the FORDS, pages 7-8. Beginning with the FORDS 2010 (implemented with cases diagnosed 1/1/2010 and after), the format for transmitting dates in the abstract were revised. Prior to FORDS 2010, special codes were used in the date fields if treatment was not given (00000000), the date was unknown (code 99999999) or if the treatment was recommended but unknown if given (code 88888888). Now, only valid dates can be transmitted in the date fields and the Flag fields are used to describe these other situations. The FORDS says that the "Interoperable" format will be used for TRANSMITTING data. For example, when the data is sent from the hospital registry to the NCDB. Each cancer registry software vendor will determine how the date is to be ENTERED. If the date is entered in the traditional format, the software computer programs will convert the format to the interoperable format for the transmission of data. Because there may be a choice of how the date is to be entered when using actual cancer registry software systems, it is important to learn what format must be used at the particular facility in which you work. IMPORTANT INSTRUCTIONS FROM THE INSTRUCTOR: Using the Flag fields will be discussed in more detail in the Oncology Treatment and Coding course. The FORDS does not specify a specific format to be used for the date fields, but rather states that the cancer registry software providers will provide the instructions for the format to be used. For the purposes of this course and the CRM program
, all dates will use the TRADITIONAL format (MMDDYYYY). When completing exercises and answering quiz questions, use the traditional format.
If any part of the date information is unknown, it should be filled in with 9's (99999999 if the entire date is unknown, 99992010 if only the year is known, 06992010 if only the month and year are known, etc.) for unknown if an estimated date cannot be determined. If the date does not apply, such as that particular type of treatment was not given, then the date field is filled in 0's (00000000). The Flag field will not be collected in lesson as detailed instructions for the flag fields will not be discussed until the Oncology Treatment and Coding course. If you are working in a cancer registry, you should check with your software provider to determine the appropriate format to be used for data entry in your cancer registry software system.
Slide 12
12
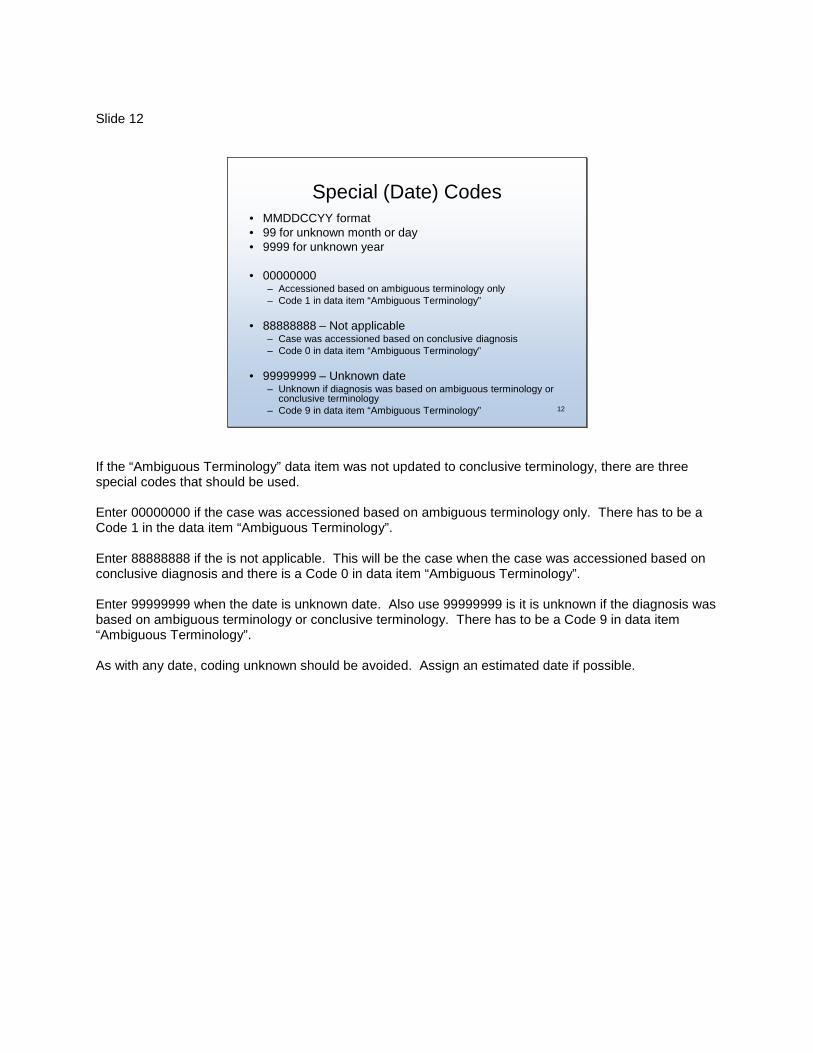
Special (Date) Codes• MMDDCCYY format• 99 for unknown month or day • 9999 for unknown year
• 00000000 – Accessioned based on ambiguous terminology only – Code 1 in data item “Ambiguous Terminology”
• 88888888 – Not applicable – Case was accessioned based on conclusive diagnosis – Code 0 in data item “Ambiguous Terminology”
• 99999999 – Unknown date– Unknown if diagnosis was based on ambiguous terminology or
conclusive terminology – Code 9 in data item “Ambiguous Terminology”
If the “Ambiguous Terminology” data item was not updated to conclusive terminology, there are three special codes that should be used. Enter 00000000 if the case was accessioned based on ambiguous terminology only. There has to be a Code 1 in the data item “Ambiguous Terminology”.
Enter 88888888 if the is not applicable. This will be the case when the case was accessioned based on conclusive diagnosis and there is a Code 0 in data item “Ambiguous Terminology”.
Enter 99999999 when the date is unknown date. Also use 99999999 is it is unknown if the diagnosis was based on ambiguous terminology or conclusive terminology. There has to be a Code 9 in data item “Ambiguous Terminology”. As with any date, coding unknown should be avoided. Assign an estimated date if possible.
Slide 13
13
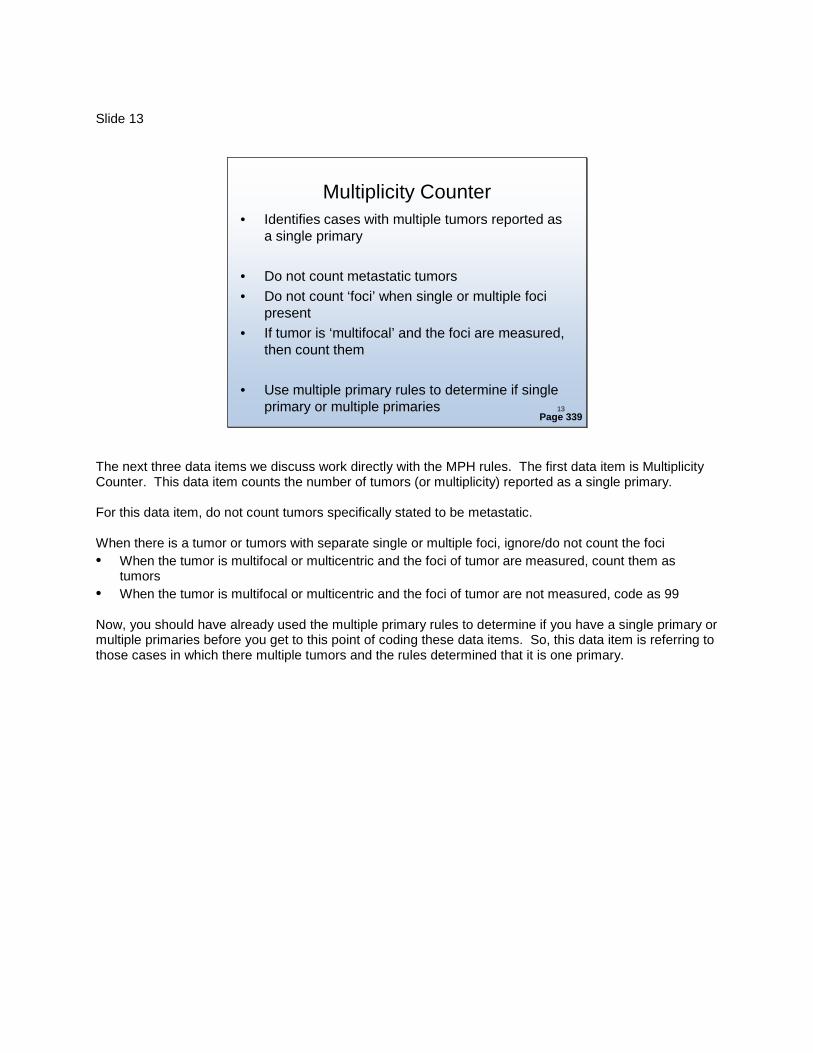
Multiplicity Counter• Identifies cases with multiple tumors reported as
a single primary
• Do not count metastatic tumors• Do not count ‘foci’ when single or multiple foci
present• If tumor is ‘multifocal’ and the foci are measured,
then count them
• Use multiple primary rules to determine if single primary or multiple primaries
Page 339
The next three data items we discuss work directly with the MPH rules. The first data item is Multiplicity Counter. This data item counts the number of tumors (or multiplicity) reported as a single primary. For this data item, do not count tumors specifically stated to be metastatic. When there is a tumor or tumors with separate single or multiple foci, ignore/do not count the foci • When the tumor is multifocal or multicentric and the foci of tumor are measured, count them as
tumors • When the tumor is multifocal or multicentric and the foci of tumor are not measured, code as 99 Now, you should have already used the multiple primary rules to determine if you have a single primary or multiple primaries before you get to this point of coding these data items. So, this data item is referring to those cases in which there multiple tumors and the rules determined that it is one primary.

Slide 14
14
Multiplicity Counter - Codes
• 01 One tumor only • 02 Two tumors present • 03 Three tumors present• :• 88 Information on multiple tumors not
collected/not applicable for this site • 99 Multiple tumors present, unknown how
many
And, here are some examples of the codes that you will use. Use code 01 when:
• There is a single tumor in the primary site being abstracted • There is a single tumor with separate unmeasured foci of tumor
Use code 02 when there were two tumors present and the rules said to abstract as a single primary. Use code 03 when there are three tumors present, and so on. Code 88 is used when information on multiple tumors is not collected or is not applicable for that primary
site. This includes: • Leukemia • Lymphoma • Immunoproliferative disease • Unknown primary Use code 99 when you know there are multiple tumors present, but the exact number is unknown. This
includes situations when: • The original pathology report is not available and the documentation does not specify whether there
was a single or multiple tumors in the primary site. • The tumor is described as diffuse. • The operative or pathology report describes multiple tumors but does not give an exact number. • It is unknown if there is a single tumor or multiple tumors and the multiple primary rules instructed you
to default to a single tumor.

Slide 15
15
Date of Multiple Tumors
• Identifies the date patient diagnosed with multiple tumors
• Use multiple primary rules to determine if single primary or multiple primaries
• May or may not be the same date as date of diagnosis– Only when multiple tumors are present at diagnosis
• Change Multiplicity Counter to 02 and enter the date the second tumor was diagnosed when subsequent tumor(s) are counted as same primary
Page 341
The next data item identifies the month, day and year the patient was diagnosed with multiple tumors that were reported as a single primary. Again, you would have already used the multiple primary rules to determine if it is a single primary or a multiple primary. The date the patient was diagnosed with multiple tumors may or may not be the same as the date of diagnosis. Obviously, if there were multiple tumors present at diagnosis, then this date will be the same as the date of diagnosis. Don’t forget: You will also need to remember to change the Multiplicity Counter data item from code 01 to code 02 and enter the date the second tumor was diagnosed if the subsequent tumor(s) are considered as same primary according to the MPH rules.

Slide 16
16
Special (Date) Codes
• MMDDCCYY format• 99 for unknown month or day • 9999 for unknown year
• 00000000 – Single tumor• 88888888 – Information on multiple tumors not
collected/not applicable for this site • 99999999 – Unknown date
Although coding 9’s for any part of a date that is unknown is allowed, it is recommended that you investigate further prior to coding unknown. If possible, estimating a date is preferred to coding unknown. Assign 00000000 when there is only a single tumor. Assign 88888888 when information on multiple tumors is not collected or is not applicable for this site. Assign 99999999 if the date of multiple tumors is unknown.

Slide 17
17
Type of Multiple TumorsReported as one Primary
• Identifies the type(s) of multiple tumors abstracted as a single primary
• Example: both in situ, both invasive, one in situ and the other invasive, etc.
• Do not count metastatic tumors
Page 342
The last data item identifies the type of multiple tumors abstracted as a single primary. That is, were the tumors all invasive, all in situ, or both. Again, we are not looking at tumors stated to be metastatic.
Slide 18
18
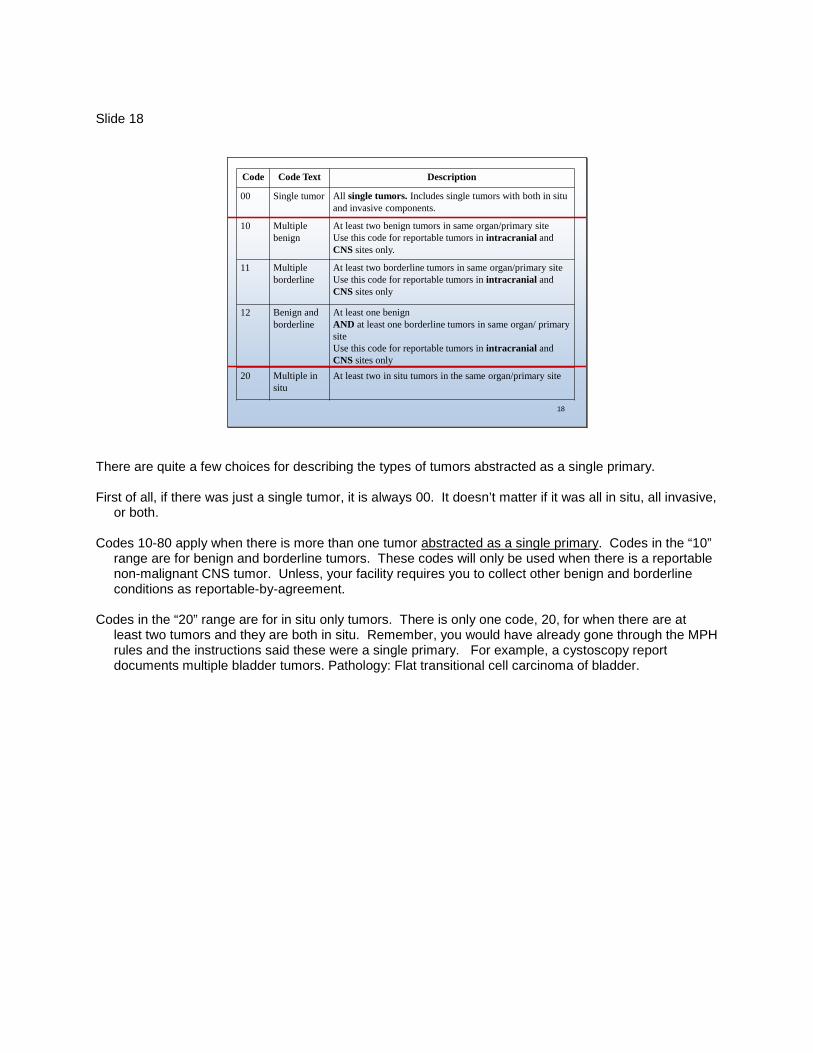
Code Code Text Description
00 Single tumor All single tumors. Includes single tumors with both in situ and invasive components.
10 Multiple benign
At least two benign tumors in same organ/primary siteUse this code for reportable tumors in intracranial and CNS sites only.
11 Multiple borderline
At least two borderline tumors in same organ/primary siteUse this code for reportable tumors in intracranial and CNS sites only
12 Benign and borderline
At least one benign AND at least one borderline tumors in same organ/ primary site Use this code for reportable tumors in intracranial and CNS sites only
20 Multiple in situ
At least two in situ tumors in the same organ/primary site
There are quite a few choices for describing the types of tumors abstracted as a single primary. First of all, if there was just a single tumor, it is always 00. It doesn’t matter if it was all in situ, all invasive,
or both. Codes 10-80 apply when there is more than one tumor abstracted as a single primary
. Codes in the “10” range are for benign and borderline tumors. These codes will only be used when there is a reportable non-malignant CNS tumor. Unless, your facility requires you to collect other benign and borderline conditions as reportable-by-agreement.
Codes in the “20” range are for in situ only tumors. There is only one code, 20, for when there are at least two tumors and they are both in situ. Remember, you would have already gone through the MPH rules and the instructions said these were a single primary. For example, a cystoscopy report documents multiple bladder tumors. Pathology: Flat transitional cell carcinoma of bladder.

Slide 19
19
Code Code Text Description
30 In situ and invasive
One or more in situ tumor(s) AND one or more invasive tumors in the same organ/primary site
31 Polyp and adenocarcinoma
One or more polyps with either• In situ carcinoma or • Invasive carcinoma AND one or more frank adenocarcinoma(s) in the same segment of colon, rectosigmoid, and/or rectum
32 FAP with carcinoma
Familial polyposis (FAP) AND carcinoma (in situ or invasive) is present in at least one of the polyps
40 Multiple invasive
At least two invasive tumors in the same organ
80 Unk in situ or invasive
Multiple tumors present in the same organ/primary site, unknown if in situ or invasive
88 NA Information on multiple tumors not collected/not applicable for this site
99 Unk Unknown
Codes in the “30” range are for in situ and invasive tumors. One tumor is invasive and one tumor in in situ. There are two special codes that apply to polyps in the colon and rectum. Use code 31 if there is a polyp and a frank adenocarcinoma abstracted as a single primary. Use code 32 if there is FAP with carcinoma in at least one polyp. Codes in the “40” range are for invasive only tumors. There is only one code, 40, for there is more than one tumor and they are all invasive.

Slide 20
CaseScenarios
The next three slides include audio narrations. Each slide runs for approximately 3 minutes. Before you advance the presentation to the next slide, check to make sure your speakers or headphones are connected and adjusted to an appropriate volume.
If you are not able to listen to the narration, complete instructors notes are provided with the slide.
At this time, we are going to go through 3 case scenarios together. The case scenarios are narrated. If you do not have the ability to listen to the narration, complete speakers notes have been provided as well.

Slide 21
21
Case Scenario 1January 4, 2007 - Bladder cystectomy, final diagnosis:A. Poorly differentiated transitional cell carcinoma of the
bladder trigone, 3.2cm, extending through muscular wall, margins free of tumor.
B. Two separate, 1.0cm moderately differentiated papillary transitional cell carcinomas of the bladder within the dome of the bladder.
Data Item Answer RationaleAmbiguous Terminology
Date of Conclusive Terminology
Multiplicity Counter
Date of Multiple Tumors
Type of Multiple Tumors
0
03
40
88888888
01042007
Conclusive dx w/in 60 days of original dxN/A – Case accessioned based on conclusive dxThree tumors presentMultiple tumors at orig dx, abstracted as single primaryMultiple invasive tumors
In this case, there are 3 tumors in the bladder, one in the trigone and two in the dome. If you were to take this case through the multiple primary rules, you would see this is one primary with multiple tumors. The first data item we are going to determine is ambiguous terminology. What we are looking for is was the case abstracted based on the use of ambiguous terminology. The list of ambiguous terms can be found on page 337. We looking for words such as apparently, consistent with, probable, etc. In this case, there was no use of such words. It just states straight out transitional cell carcioma and papillary transitional cell carcinoma. It doesn’t say probably transitional carcinoma or anything like that. So, this case was abstracted based on the use of a conclusive diagnosis. So, we will assign code 0 for the ambiguous terminology data item. The next data item is the date of the conclusive diagnosis (if there was one) IF the case was originally abstracted using ambiguous terminology. Since the original diagnosis statement used conclusive terminology, this date is not applicable. So, we should record 8’s for the date. Multiplicity counter: Use to count the number of tumors reported as a single primary (not metastatic lesions). There were three primary tumors present in the bladder at the time of diagnosis. The MP rules told us this is a single primary. So, we will record 03 in this data item. Date of multiple tumors: And, now we need to record the date the multiple tumors were diagnosed. Using the only information we have in the case scenario, this was determined on January 4, 2007. So, we will record 01042007. And the last data item is the type of multiple tumors: What we are looking for is was one invasive and the other in situ, or were all in situ or all invasive. In this example, all three tumors were invasive. So, the appropriate code is 40. There were two or more invasive tumors in the same organ.

Slide 22
22
Case Scenario 2October 16, 2007 – Renal UltrasoundAssessment: Probably renal cell carcinoma
October 17, 2007 – R nephrectomyFinal diagnosis: Adenocarcinoma, probably clear cell
type of renal cell carcinoma.
Data Item Answer RationaleAmbiguous Terminology
Date of Conclusive Terminology
Multiplicity Counter
Date of Multiple Tumors
Type of Multiple Tumors
0
01
00
88888888
00000000
Conclusive dx w/in 60 days of original dxN/A – Case accessioned based on conclusive dx
One tumor only
Single tumor
Single tumor
Used to qualify the type of adenocarcinoma, not whether or not the case should be accessioned.
In this case, there was 1 tumors in the right kidney. There was an ultrasound that stated probably renal cell carcinoma on 10/16/07. Then, the next day, on resection, the final diagnosis was adenocarcinoma…probably clear cell type of renal cell carcinoma. The first thing I want to point out is the use of the phrase “probably clear cell type” is used to qualify the type adenocarcinoma. There is a definite statement of adenocarcinoma. There is no ambiguous terminology used to describe the fact that the patient does have cancer. So, we are not going to consider this as an ambiguous diagnosis. So, with that said. The first data item we are going to determine is ambiguous terminology. They did use “probably” renal cell on the ultrasound. However, the rules tell us there is a two month time frame in which there can be a conclusive diagnosis. And, there was. It was only the next day. So, in this case there was a conclusive diagnosis within two months of the original diagnosis. So, we will assign code 0 for the ambiguous terminology data item. Since the case was originally abstracted using conclusive terminology, this date is not applicable. So, we should record 8’s for the date. Multiplicity counter: There was one primary tumor present at the time of diagnosis. So, we will record 01 in this data item. Date of multiple tumors: And, since this case doesn’t have multiple tumors, the correct code for the date of multiple tumors data item is going to be 0’s to indicate that there was only one tumor. And, again, since this case does not have multiple tumors, the correct code is 00 to indicate that it was a single tumor only. So, the take home message with this case is not to just go scanning through the chart looking for any of the ambiguous terms listed on page 337. It has to be referring to the actual diagnosis.

Slide 23
23
Case Scenario 3June 2, 2007 – Prostate biopsyAssessment: Focal atypical small glands suspicious for minimal
prostatic adenocarcinoma associated with high grade PIN.
October 14, 2007 – ProstatectomyFinal diagnosis: Adenocarcinoma, well differentiated.
Data Item Codes when abstracted
Final codes
Ambiguous Terminology
Date of Conclusive Terminology
Multiplicity Counter
Date of Multiple Tumors
Type of Multiple Tumors
2
01
00
10142007
00000000
Go back andchange the code
1
01
00
00000000
00000000
And, we will do one more case together. In this case, there was a biopsy on June 2 that was suspicious for adenocarcinoma. So, there’s a flag there, “suspicious for adenocarcinoma”. Then, 4 months later (there’s another clue, it was more than 60 days later), a prostatectomy was done. The final diagnosis from that procedure was just straight out adenocarcinoma. The first data item we are going to determine is ambiguous terminology. This case was originally diagnosed in June and it did use ambiguous terminology “suspicious” for adenocarcinoma. So, when this case was originally accessioned, it would have been based on the ambiguous terminology. (in blue, column 2). The ambiguous terminology field would have been 1 for based on ambiguous terminology only and so on. Now, time goes on and the patient comes in for treatment and there is more information to add to your abstract. At this point in time, ambiguous terminology is not used. It is a conclusive diagnosis of adenocarcinoma. Now, this is probably the most cumbersome part of these data items. If you had already abstracted the case into your registry, you would have to remember to go back and update the codes based on the fact that there is now a conclusive diagnosis. Because it was more than 60 days later, we have to use a code of 2. And, the date the conclusive diagnosis was made was on 10142007, so we will record that in the date field. The rest of the date items will remain the same. Multiplicity counter: There was one primary tumor present at the time of diagnosis. So, we will record 01 in this data item. Date of multiple tumors: And, since this case doesn’t have multiple tumors, the correct code for the date of multiple tumors data item is going to be 0’s to indicate that there was only one tumor. And, again, since this case does not have multiple tumors, the correct code is 00 to indicate that it was a single tumor only.

So, you may want to make a note somewhere that you need to remember to change these data items if, at a later time, more than 60 days later, there is a conclusive diagnosis. Slide 24
This concludes this presentation.
Please return to the course content.
This concludes this presentation. Later in this lesson, you will have an opportunity to work on additional practice cases. Please return to the course to continue this lesson.





























