Embed Size (px)
Citation preview

2008 National HREC 2008 National HREC
Chairs RoundtableChairs Roundtable

WelcomeAims of the day:
• To identify examples of good practice in strategies and procedures of
research ethics review; and
2. To facilitate and promote exchange of opinion, experience and ideas among HREC Chairs


Roles of review body chairs in human research ethics review in Australia
Professor Colin ThomsonChair
Australian Health Ethics CommitteeNational Health and Medical Research Council

Australia’s human research ethics review system
Australia has had active human research ethics review committees for more than three decades
1976 IEC review required by NHMRC1987 114 IECs2008 238 HRECs
Despite Ministerial review (1996), criticism in House of Representatives Cloning Inquiry report (2001), Essentially Yours (2003), & Latrobe and QuT instances in 2006/2007,
In 2004-5, HRECs reviewed 21,177 proposals and reported only 93 complaints (0.44%)(NHMRC)

HREC CHAIRS
Chairs of HRECs essential to established strengths
Central role in maintaining quality Accumulated experience indispensable source
of information and understanding Round Table celebrates this in treating all
chairs as equal in responsibility To promote ethically good human research –
accord respect and protection due to participants foster research of benefit to the community

Roles of HREC chairs
Assist institutions to fulfill responsibilities
Fulfill responsibilities, explicit & implicit, as Chair
Fulfill role as HREC members

Assist institutions to fulfil responsibilities
Institutions: must see any human research they
conduct/are responsible is ethically reviewed & monitored in accordance with National Statement. (NS 5.1.1)
may establish own processes for ethical review or use those of another institution. (NS 5.1.3)
satisfied that processes are in place for:(a) managing conflicts of interest (Chapter 5.4);(b) monitoring research (Chapter 5.5);(c) handling complaints (Chapter 5.6), and(d) ensuring accountability (Chapter 5.7) (NS 5.1.4)

Assist institutions to fulfil responsibilities
To enable assessment, prepare & make accessible regular reports on all ethical review processes. (NS 5.1.16)
To have auditing process to confirm that: research is being reviewed at levels of review their
criteria require (NS 5.1.17) To ensure their HRECs
established/operate in accordance with NS (NS 5.1.25) have access to expertise necessary to address ethical
issues from categories of research it is likely to consider, including from outside HREC. (NS 5.1.33)

As Chair - experience & commitment
To have suitable experience
Other responsibilities will not impair the HREC’s capacity to meet obligations under NS (NS 5.1.30)
Good ethical review requires shared commitment to the review process,
Institutions to encourage shared commitment by promoting:
awareness of this NS among researchers; and ready accessibility of review bodies and their
staff to researchers. (NS 5.2.13)

As Chair: communication
Good ethical review requires open communication between review bodies and researchers, non-adversarial process.
As misunderstandings often arise when only written communication used, review bodies should: encourage informal communication with researchers, and consider face-to-face meetings to resolve issues not resolved by
written/telephone communication. (NS 5.2.14) Review body to clearly communicate decision to researcher/s:
Where approved, communication in writing (include email) & include explicit statement that proposal meets requirements NS.
Where amendments requested, communication written or informal & reasons for requested amendments.
Where proposal rejected, communication in writing (include email) and include reasons linked to NS (NS 5.2.22)

As Chair: meetings
To enable at least one member in each specified category to attend.
Papers enough in advance to enable members fully informed. (NS 5.2.28)
Decisions informed by exchange of opinions from each of minimum membership,
Ideally at meeting with those members present. (NS 5.2.29)
Where less than full attendance of minimum membership, Chairperson should be satisfied, before a decision is reached, that the views of minimum membership absent have been received and considered. (NS 5.2.30)
Endeavour to reach decisions by general agreement, not necessarily unanimity. (NS 5.2.31)
All documents/material used in recruiting potential research participants should be approved (NS 5.2.23)

As Chair: advocates, researchers, experts
Review body consider consulting participant advocate to assess if a proposal adequately provides for participants’ decision making and understanding. 5.2.17
Review body may invite researcher/s, and researchers may request, to be present for discussion of proposed research. 5.2.18
Review body may seek advice from experts to help
Experts bound by confidentiality & conflicts of interest requirements as review body members. NS 5.2.19

As Chair: conflicts of interest
Of researchers: disclosure to participants & in report (except details?
5.4.6) independent approach to participants or alternative
researcher disapproval
Of HREC members: disclose actual or potential CoI personal involvement/participation in research or
competing research financial interest, affiliation
Manage CoI’s of HREC members: e.g exclusion

As Chair: records
Review body to retain copy of each research proposal & application for ethical
approval, including all documents & relevant correspondence, in approved form 5.2.25
Review body to record specified details of all research proposals received & reviewed
NS 5.2.24 decisions of, & reasons linked to NS for, approval, amendment or
rejection in written or electronic form NS 5.2.26
Where more than one review body has reviewed proposal, each body to record
details of other review body/ies involved; the decision/s of each other review body; and details of any amendments required by each other review body.
5.2.27

As an HREC member
Each member responsible for deciding whether, in his or her judgement, a proposal
submitted to the review body meets the requirements of NS and is ethically acceptable. (NS 5.2.2)
becoming familiar with NS & consult other guidelines relevant to specific proposals,
preparing for & attending scheduled meetings of review body,
if unavailable, providing opinions on ethical acceptability of proposals before meetings, subject to institutional policies on absences,
attending continuing education/training in research ethics at least every three years. (NS 5.2.3)
disclosing to review body any actual or potential conflict of interest, that bears on any research coming before the review body (NS 5.2.4)

Roundtable
• Recognizes the community to which you belong
• Offers opportunity to – discuss - and be instructed by - experience– explore ways to meet responsibilities


How do you sustain a HREC?
Lead Facilitator: A/Prof Lyn Angel

• Why we chose this session to open the program
• Nuts and bolts session
• About management practices
• Adapting to trends and changes – what have you done in the last two years which has altered the way you run and sustain your committee?
• New and Senior Chairs attending with variable experience
• Acknowledging the collective wisdom of Chairs with opportunities to tap into this wisdom.

Which of the following issues created difficulty in sustaining a HREC?
Prioritise 3 and discuss
• Workload of secretariat• Workload of the HREC• Circulating increasingly large
agendas to all members• Massive amounts of paper
required to distribute• Length of meetings • Timing and frequency of
meetings
• Venue eg videoconferencing facilities
• Membership• Communication between
meetings• Training• Succession planning• Institutional support• Others? Eg. Food.

What strategies did you employ to overcome them?
• How do you justify the strategies?
• What principles do you use in developing strategies to overcome issues around ethical management?
• Why do you do it this way?
• Can it be applied across other sections or HREC’s or is it just going to work in your institution?

Conflict of Interests: real and perceived
Lead Facilitator: Dr Garry Pearce

A conflict of interest exists where there is a divergence between the individual interests of a person and their professional responsibilities such that an independent observer might reasonably conclude that the professional actions of that person are unduly influenced by their own interests (Section 7)
The Code defines conflict of interest as follows:

While a conflict may relate to financial interests, it can also relate to other private, professional or institutional
benefits or advantages that depend significantly on the research outcomes. (Section 5.4).
The National Statement states that:

Institutions should establish transparent processes to identify and manage actual and perceived conflicts of
interests involving:(a) the institution itself;(b) the researchers; or(c) ethical review bodies,
their members or advisors.
Section 5.4.1 of the National Statement requires that:
Sometimes a researcher who discloses the fact that he or she has a conflict of interest may have an ethically acceptable reason for not disclosing what the conflict is, for example, that this might breach another person’s privacy. The researchers may then remain involved in the research only if the review body is satisfied that the conflict can be managed without its nature being disclosed. (National Statement 5.4.6).
For a researcher, the National Statement notes that:

Researchers frequently have a conflict of interest that cannot be avoided………An individual researcher should therefore expect to be conflicted from time to time, and be ready to acknowledge the conflict and make disclosures as appropriate. (Section 7.2).
In relation to disclosing a conflict of interest the Code notes that:

1. “Identify a COI as a presentation from the table for case discussion- what it was, how it was dealt with”.
2. What systems are in place to deal with COI at the institutional level and at the HREC level?
• Whom do COI involve – sponsors, institutions, researchers, HREC members?
• When do they get the COI declaration forms signed?
• How are COI best managed at the HREC level?• When do they get a person to leave the room and
when do they bring them back? Do they always have to leave the room? Who decides?
• How do Universities deal with COI arising from the commercial realities of research?
• How do Health entities deal with pharmaceutical sponsorship COI in research?
• Should a person from the same department review a study given that they are not participating in the study?
• How detailed should COI declarations be?• Should we be doing more? How should this best be
done?• Institutional support – what policies should be in
place to assist the process?


Low Risk Research Review
Lead Facilitator: A/Prof Lyn Angel

How do the various institutions manage LRRR?
• Is it (ie LRRR) a growing workload for universities and health sectors? We have no trend data to inform the discussion
• What barriers are there to reviewing LRRR?• How are Institutions overcoming these barriers?• What is the least costly way of dealing with LRRR.• What systems have been put in place?• Related questions/issues:
i Undergraduate projects issues: how are these managed? Approved? By whom?ii Honors students, projects undertaken by students on placement (clinical/education)?
• What is the membership of LRRR oversight groups? Separate committee? Executive of the HREC?
• Is training required?• How is this best done? • Should it be necessary for the HREC to ratify the LRR? (National
Statement 2007 does not say that LRRR has to be ratified)• How much in the way of extra resources and workload is required to
deal with LRRR?• What extra help is required in this area by Institutions to deal more
effectively with LRRR?


Human research ethics review in Australia - where we’ve been, where we are and
where we might go.Professor Colin Thomson
Chair,Australian Health Ethics Committee
National Health and Medical Research Council

A history of Australian human research ethics review
1936 Medical Research Endowment Fund Act creates Medical Research Endowment Fund. Minister for Health determines use of fund for
medical research & training receives advice from National Health and Medical Research Council (NHMRC).
1964 World Medical Assembly issues Declaration of Helsinki
1966 NHMRC issues Statement on Human Experimentation that expressly draws on Declaration of Helsinki.
A history
1972 NHMRC Ethics in Clinical Research Subcommittee revises Statement & recommends medical ethics committee review - one outside member - of NHMRC grants involving human subjects.
1976 Supplementary Note 1 added to the Statement, requires review by institutional ethics committee (IEC).
Scope of the Statement extended to all human subject research: medical, social and behavioural research.
IEC minimum membership:• Layman and laywoman not associated with institution• Minister of religion• Lawyer• Medical graduate with research experience

A history
1982 Council established Medical Research Ethics Committee (MREC) to
keep under review ethical principles in human experimentation
facilitate, review & report on the work of IECs, & respond to questions raised by them.
1985 Council policy that, to be eligible for Council research funds, institutions must conform to Supplementary Note 1 to Statement.
1987 114 IECs in Australia

A history
1987 - 1991 Research Ethics Newsletter (MREC)Annual one-day IEC workshops
1991 TGA legislation permits CTN trials to commence if favourable advice from IEC that would
undertake monitoring1992 NHMRC Act - statutory corporation
• AHEC formed• issue of "guidelines for the conduct of medical
research involving humans”, • precisely as developed by Australian Health Ethics
Committee (AHEC).

A history
1994 - concerns about adequacy of ethical review under de-
centralized drug research regimemonitoring by AHEC of IECsadequacy of guidelinestrials about reproductive technologyinnovative use of growth hormone

1996 Ministerial review recommends revision of national guidelinesmanual or procedures for IECs IECs address
• multi-centre review &• procedures for information & voluntary
consent• annual reports
institutions to appoint complaints officers, resource IECs
researchers use plain language in consent documentation
A history

1997 NHMRC/AVCC Joint Statement on Scientific Misconduct guides institutions on
handling research misconduct allegations.
1999 National Statement on Ethical Conduct in Research Involving Humans
(NationalStatement)
IECs now human research ethics committees (HRECs)
2001 Parliamentary report on Human Cloning criticizes IECs as lacking public
accountability, “in-house” National forum identifies urgent need to address duplication of ethical review
A history

2003 NHMRC Research Ethics Conference and Training Day
(ALRC/NHMRC Essentially Yours; The Protection of Human Genetic Information in Australia, 2003, p 446
“The Inquiry has concluded that there is a need to improve consistency, efficiency,
transparency and accountability in HREC review . . “
2004 NHMRC research ethics training program2005 NHMRC 2nd research ethics conference 1st. HREC Chairs Rpundtable
A history

2006 LaTrobe University: phone interviews that revealed intimate details of the lives of partners of interviewees led to complaint that the
review failed to identify some risks. http://www.abc.net.au/rn/healthreport/stories/2006/1680645.htm
(at12/08/08)
2nd HREC Chairs Roundtable2007 QUT: research participation of people with
intellectual disability led to complaints that HREC failed to protect participants from risks.
http://www.abc.net.au/news/opinion/items/200706/s1953217.htm (at 12/08/08)
3rd NHMRC Research Ethics Conference, Continuing Education Day and 3rd HREC Chairs Roundtable
A history

2007 Revised National Statement on Ethical Conduct in Human Research
Australian Code for Responsible Conduct of Research replaces Joint Statement
232 HRECs
A history

Another history
• Research on Aboriginal and Torres Strait Islander people since early 1900’s
• Perceived risks to white settlers of exotic tropical diseases
• Testing theories about blood type & race & physiological reactions and capacities
• No consent - identification by numbers on bodies or cards around necks
• Helicopter studies; data raids
• No alleviation of deepening disadvantage

• Research designed to meet needs of researchers, not participants
• Exploitation of cultural property• Shared memories poisoned & deep suspicion of
research and science1985 - fiery conference in Central Australia• Recognition of need to protect cultural integrity• Draft guidelines emphasised consultation, benefit and
ownership• Used prescriptive rules to control investigator conduct
in order to protect culture
Another history

2000-2003• Maturing Aboriginal organizations, cultural
confidence and resilience • Aboriginal organizations recognised potential
value of research to address disadvantage• More Aboriginal researchers• Developing vision of cultural values• Engagement with research where those values
realised
Another history

Emerging approaches:• For research to be ethically and culturally
acceptable, must be of benefit to those involved• Benefit - and burden - to be of their definition and
agreement• To be reciprocal with benefit to others from
research• Essential prior consultation with involved people• Negotiated research plan
Another history

Confidence that• participants can assert research needs &
protect themselves through relationship with researchers
• best participant protection through negotiated relationship - and not only from approval from HREC.
• researchers accept that only through relationship would they achieve research goals.
Another history

Human research ethics review in Australia - where we’ve been, where we are and
where we might go.Professor Colin Thomson
Chair,Australian Health Ethics Committee
National Health and Medical Research Council

1970 1980 1990 2000
Statement on Human Experimentation & IEC review
Ministerial review
National Statement
1st Research Ethics Conference
&Training Day
HREC training program
2nd Research Ethics Conference, training day & HREC Chairs roundtable
3rd Research Ethics Conference, training day & 3rd HREC Chairs Roundtable
2nd HREC Chairs Roundtable
NHMRC Act, AHEC
Revised Statement + SuppNotes
NHMRC policy decision
MREC formed, IEC support
IEC newsletter, annual IEC workshops
Cloning Report criticises HRECs
ALRC/NHMRC questions HRECs
LaTrobe
QuT
National Statement
CTN/CTX


1920 1930 1940 1950 1960 1970 1980 1990 2000
ALICE SPRINGS
CONFERENCE
Interim Guidelinesprotect cultural integrityconsultation, benefit & ownershipprescriptive rules to control investigators to protect culture
Values & Ethics
Keeping
Research on
Track
Aboriginal & Torres Islander health research
Risks to white settlers of exotic diseasesTheories about blood type & race & physiological reactions and capacitiesNo consent - identification by numbers on bodies or cards around necksResearch meet researchers needsShared memories poisoned & deep suspicion of research and scienceNo alleviation of deepening disadvantage
State protection, access conditions, consent

Effectiveness of Values & Ethics guidelines depends on establishing, between researchers & Aboriginal and Torres Strait Islander participants, a relationship through which the scope, methods & outcomes of research
are negotiated & determined.
Another history

Influence of another history
In National Statement, experience of potential participants should be used in determination of research merit in some
cases (1.1(a))assessment of research risk (2.1.6) planning some consent processes (2.2.15) institutional assessment of low risk review
(5.1.14)deciding if research adequately provides for
decision-making and understanding (5.2.17)

The present – and the future
Criticisms that Australian HREC review system is :
invisible ineffective inefficient
Inconsistent
Future of human ethics review needs to include responses to these criticisms

“invisible”
Faceless, lacking transparency and accountability
To whom accountable: Participants? Funders? Institutions? Government? The public?
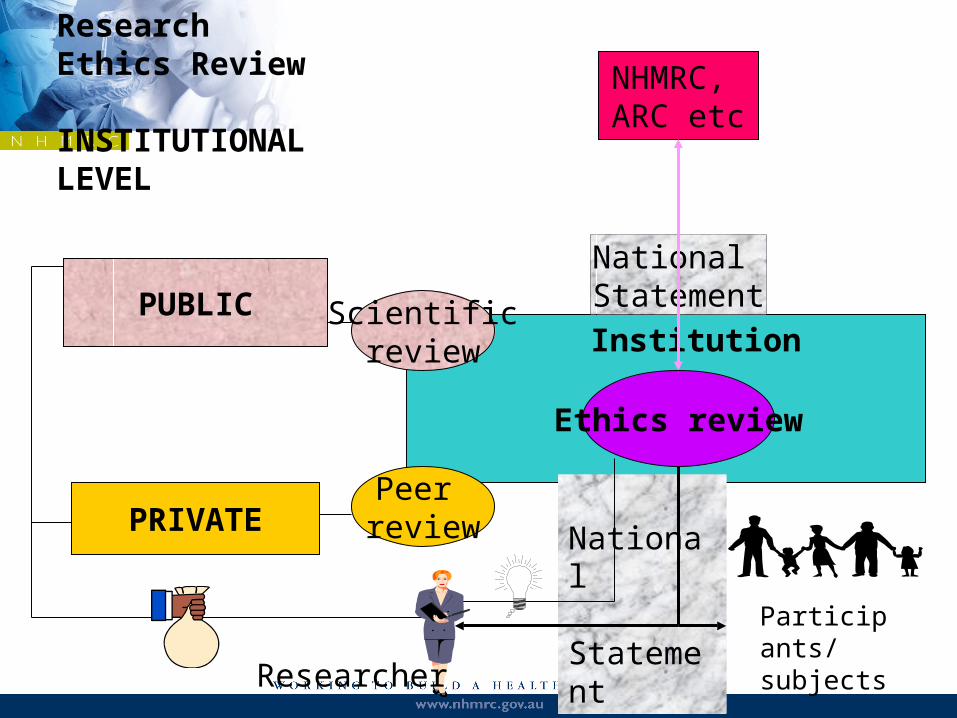
Institution
Ethics review
National Statement
Participants/subjects
NHMRC, ARC etc
PUBLIC
National Statement
Scientificreview
PRIVATEPeer
review
Research Ethics Review
INSTITUTIONALLEVEL
Researcher

NHMRC, ARC, UA
National Statement
I n s t i t u t i o n s
Researchers
Participants
GOVERNMENT
ResearchEthics ReviewSYSTEMLEVEL
Accountability
Responses to “invisible”
Challenging Ethical Issues in Contemporary Research on Human Beings, Repot to Minister (NHMRC website)
Recognition or accreditation (later)Strengthen the annual report

Annual report
At present, no questions about how HRECs use NS clauses that protect participants, e.g. consent & waiver, risk assessment .
Does accountability = demonstration that NS process followed, or that outcomes achieve goals of NS?How could an HREC show that : NS process followed? NS outcomes achieved?Annual repot revision related to broader NHMRC goals &
functions & AHEC advisory role

CEO
Operations Division
Knowledge Development Division
Program Management
Corporate Services
Research Investment
NICSHealth Evidence & Advice
Quality & Regulation
STRUCTURE OF THE NHMRC
Principal Committe
es [includes
AHEC]
Advice
Health & Research Ethics
Council

“ineffective”
Fail to protect participants?Fail to follow National Statement?Controversial studies in 2006, 2007, BUT:2004-5 HREC reviews 21,177
complaints about research conduct 62Responses:
Challenging Ethical Issues in Contemporary Research on Human Beings, Report to Minister, NHMRC websitefollow direction suggested by Values and Ethics National Ethics Application Form (NEAF)recognition or accreditation (later)

National Ethics Application Form (NEAF)
• Version 2 available 25 August 2008.• Reduced in length & detail• Revised sequence• Amended to suit revised National Statement• Information and familiarization sessions

“inefficient”
Slow, unpredictable, bureaucratic, pedantic.Duplication of review of multi-site research.
Responses: National Ethics Application Form (NEAF) Informal HREC recognitionsState level multi-site initiativesHarmonisation of Multi-centre Ethics Review
(HoMER)Recognition or accreditation (later)

I N S T I U T I O N SHREC HREC HREC HREC HREC
Research ethics review - multi-centre review I
N a t i o n a l S t a t e m e n t
Principal Researcher
A s s o c i a t e r e s e a r c h e r s
Problem method

I N S T I U T I O N S
HREC
HREC
HREC
HREC
HREC
Research ethics review - multi-centre review II
N a t i o n a l S t a t e m e n t
Mutual HREC recognitionPrincipal Researcher
Associate researchers Associate researchers

I N S T I U T I O N SHREC HREC
RecognisedHREC
HREC HREC
Research ethics review - multi-centre review III
National Statement
Institutional recognitionPrincipal Researcher
Associate researchers Associate researchers

HoMER
• AHMAC referral to NHMRC of task to develop a national harmonized system
• Of States/territories initiatives• Enable single scientific and ethical review of
national level studies• State/territory focus groups to
– Advise local progress– Clarify key elements

HoMER
Will need to deal with:• Recognition of HRECs
– scientific expertise– ethics– standards
• Procedures for scientific and ethical review• Training of institutional officials & researchers• Allocation of proposals for review• IT system• Monitoring of approved proposals• Insurance & indemnity arrangements

“inconsistent”
Contradictory or differing responses to same proposal
Applying different standards (institutional history) or the same standard differently.
Responses:Strengthen annual reportNational Ethics Application Form (NEAF)Recognition or accreditation

National Agency
Accreditation criteria
National Statement
Accreditation agency
I N S T I T U T I O N S
Research ethics review - accreditation

Accreditation criteria
National Statement
National Accreditation
agency
I N S T I T U T I O N S
Research ethics review - accreditation

Recognition or accreditation
1. To what should accreditation apply: (i) committee?(ii) institution?(iii) program or system?
2. What should standards be?3. Who should develop & determine standards?4. Who should implement standards & how?5. What should be consequences of non-
compliance?


Accreditation
Lead Facilitator: Dr Garry Pearce

• Some State Institutions eg NSW Health has already gone through an accreditation process as part of its single ethics review model 15/41 were accredited as “Lead Committees”.
• Should there be international accreditation of HREC’s for international multi site research?

choose 1 or 2 of these questions to discuss at each table.
1. To what should accreditation apply: institutions, programs, HRECs?
2. What future accreditation standards should apply?
3. Who should set the standards?
4. Who should implement the standards by checking and reporting compliance?
5. What should be the consequences of non-compliance?

1. How much support is there for an accreditation process?
2. Think of three arguments for and three arguments against accreditation.


Minimising / Eliminating duplication of review
Lead Facilitator: A/Prof Lyn Angel

1. What are local institutions doing to reduce duplication of review?
• Looking for practical experience • What do you think should happen at regional, State, and National levels
– should it be by choice ie voluntary or compulsion eg European Directive (all trials to be reviewed only once)? What would happen if the TGA used its powers to do similarly to Europeans?
• Where would the levers for change for this to happen best come from?i. Eg Working Party to review and develop recommendations?


Acknowledgement





























