Embed Size (px)
Citation preview

Asthma Research 2002 - 2008
NEW APPROACHES IN AK
FOR THE TREATMENT OF
CHRONIC ASTHMA
By Tracy S Gates, D.O., DIBAK

Asthma Research 2002 - 2008
IntroductionAsthma is a disease of the air passages, characterised clinically by episodes of breathlessness, wheezing and cough as a result of bronchiolar constriction, oedema of the bronchial mucosa and secretion of thick viscous fluid.
Remodelling occurs over time as a result of these physiologic reactions, leading to a permanent thickening of the airway passages. This thickening, when prolonged, will cause irreversible pathological damage, resulting in a state of chronic obstructive pulmonary disease (COPD).
The incidence of asthma is increasing at an alarming rate – an estimated 2% of the population of the United States were believed to suffer with asthma in either its allergic of idiosyncratic form in 1982; in 2002, the figure is believed to be in the region of 11% and still increasing.

Asthma Research 2002 - 2008
Asthma UK – Key facts
5.2 million people in the UK are currently receiving treatment for asthma: 1.1million children (1 in 10) and 4.1 million adults (1 in 12). There were just under 1,400 deaths (1,381) from asthma in the UK in 2004 (40 were children aged 14 years or under). On average, 4 people per day or 1 person every 6 hours dies from asthma

Asthma Research 2002 - 2008
USA (American Lung Association) – Based on the 2004 NHIS sample
An approximate 30.2 million American citizens, or 104.7 per 1,000 citizens, has been diagnosed with asthma. Children / teenagers age 5-17 years have the highest prevalence rates. In 2004, 140.1 per 1,000 children were diagnosed with asthma. Females have had consistently higher rates than males in the USA. In 2004, females were approximately 6% more likely than males to be diagnosed with asthma.

Asthma Research 2002 - 2008
Annual Economic Cost of Asthma to the USA in 2004:
$16.1 billion via indirect costs in lost productivity. $5 billion via the direct medical expenditure of Prescription drugs. The value of lost productivity due to death represented the largest single indirect cost at $1.7 billion. Total annualized estimated cost in 2004 = $22.8billion

Asthma Research 2002 - 2008
Causation
The breathing difficulty associated with asthma is in the expiratory phase of respiration, since the exhaled air must be expelled against the restriction of the narrowed airways and occluding mucous. This results in an escalating state of hyperventilation, which in turn has the following consequences:

Asthma Research 2002 - 2008
Causation contd:
Hyperventilation → Constriction of blood vessels, impairing blood supply to the brain, causing dizziness Tightness in the chest caused by constriction of the airways Increase in heart rate Paraesthesia Eventually, fainting
A state of chronic hyperventilation generally develops in asthmatics, with a minimal manifestation of the above clinical signs and symptoms.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
The Buteyko method of Respiratory Control was first devised by Buteyko over 40 years ago, whilst he was involved in research as a medical student. The method was endorsed by the Soviet Academy of Science in 1985. It is a method employing simple breathing techniques to overcome symptoms related to asthma, as well as emphysema, bronchitis, sleep apnoea, panic attacks and anxiety.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Controlled studies have shown that: After 6 weeks, use of bronchodilators was reduced by 90% After 12 weeks, use of steroid inhalers was reduced by 30% In comparison, the control group was able to reduce intake by less than 5%.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Functions of Carbon dioxide: Helps to utilise oxygen in the body, so that the more the person breathes, the more carbon dioxide is expired, and therefore the less oxygen there is available Regulates acid/alkali balance in the body Acts as a bronchodilator

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
The average person exhales 17,000 times in each 24 hour period. Hyperventilation develops when the respiration becomes too fast or too deep (or both). Asthmatics chronically hyperventilate, breathing up to 4 – 5 times deeper than is required by the body; leading to spasms and increased mucous production. This low-grade hyperventilation is further increased in response to activity, infection, emotion and exposure to allergen.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
During an attack, the body tries to prevent the person from over-breathing in order to prevent further carbon dioxide loss. This is a life-saving defence mechanism.
Normalising the breathing pattern helps reduce or eliminate an asthma attack.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Evaluating the patient’s current status:
Are you breathing through your mouth? Do you feel your chest moving? Does your abdomen move less than your chest? Are your shoulders moving up and down while you breathe? Is your breathing being interrupted by sighs? Establish the number of breaths/min

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
First stage in helping to control the breathing pattern:
Establish a Control Pause:
The Control Pause is the period of time until the patient really needs to inhale again after full expiration:
Inhale – Exhale – Hold the nose until a sensation of lack of air is experienced.A healthy length is 40 – 60 seconds - this corresponds to the percentage of carbon dioxide in the lungs.5.5% = 40 secs6.5% = 60 secs4.5% = 20 – 30 secs4% = 0 secs
Below 3% concentration is insufficient to maintain life.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Correction And Control
Factors which influence control: Posture Relaxation Concentration on other factors decreases respiratory rate Closure of the eyes reduces respiratory rate

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
“Shallow Breathing”
The desire to breathe deeply is, of course, caused by lack of oxygen to the brain. In response to the decreasing partial pressure of oxygen, chemoreceptors in the brain initiate the process of reflex breathing which increases the volume of air inhaled, thereby increasing the volume of oxygen available to feed the brain. At the same time, the body reflexly increases lung expansion and diaphragmatic movement. However, if the potential to exhale is reduced, this scenario rapidly leads to the onset of hyperventilation. This can be controlled by shallow breathing, whereby the patient holds on expiration, and then inhales without increasing the depth of the breath accordingly. The objective is to have the patient get used to a feeling of lack of air.
Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Maximum Pause
This increases carbon dioxide.
Have the patient inhale – exhale – hold breath. On resuming breathing, resist the urge to gulp air by taking several short breaths, rather than one deep one. If the patient is forced to gulp air, this implies that the Maximum Pause was too long and it must be reduced.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Contra-indications for Maximum Pause: Heart disease Increased Blood Pressure Epilepsy Diabetes Kidney Disease Anxiety attacks
The Maximum Pause is an exercise only to be used to overcome the symptoms of asthma, not as a prophylactic exercise.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
General rules for a Exercise Routine:
Should be practiced 20 – 30 mins twice daily Always wait 2 hours after eating Measure cardiac pulse every 3 – 5 mins during exercise. Shallow breathing leads to an increase in carbon dioxide concentration, causing dilatation and increased circulation of blood – hence a decreased pulse rate and warmth in the face. If the pulse increases, this is an indication that the breathing has been reduced too much. With the shallow breathing, the patient should continue to feel a light lack of air, but should not tolerate extreme discomfort.

Asthma Research 2002 - 2008
The Buteyko Eucapnic Method
Remember:
Bronchodilators impair the progress by: Increasing respiratory rate Decreasing carbon dioxide reserves Interfering with defence mechanisms

Asthma Research 2002 - 2008
Clinical Application
- A group of 90 patients was taken, age range 6 years to 43 years.
- 3 subgroups were randomly formed, each of 30 people with varying range of ages and debility and the following applications made.
Asthma Research 2002 - 2008
Clinical ApplicationGROUP 1:Undertook no treatment for 8 weeks, other than ongoing use of inhalers and steroids.
GROUP 2:Undertook practice of the Buteyko Method without any additional treatment for a period of 8 weeks.
GROUP 3:Undertook practice of the Buteyko method, together with fortnightly attendance at the practice, whereby treatment was administered accordingly to need using muscle testing.

Asthma Research 2002 - 2008
Clinical Application
Each of the 90 participants were asked to fill in a questionnaire** on a fortnightly basis.
** questionnaire available upon request – [email protected]
The results were as follows:

Asthma Research 2002 - 2008
Group 1-control
Subjective symptoms
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
After 2 weeks: After 4 weeks: After 6 weeks: After 8 weeks:
No Change
Worst
Improved
Imp Worse No Chg
2 wks: 3 5 22
4 wks: 4 7 19
6 wks: 5 5 20
8 wks: 6 2 22

Asthma Research 2002 - 2008
Drug Intake
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
After 2 weeks: After 4 weeks: After 6 weeks: After 8 weeks:
No Change
Worst
Improved
Imp Worse No Chg
2 wks: 3 1 26
4 wks: 3 3 24
6 wks: 5 1 24
8 wks: 3 1 26
Group 1-control

Asthma Research 2002 - 2008
Group 2 –Buteyko only
Subjective Symptoms
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
After 2 weeks: After 4 weeks: After 6 weeks: After 8 weeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 11 2 17
4 wks: 9 3 18
6 wks: 14 2 14
8 wks: 19 1 10

Asthma Research 2002 - 2008
Drug Intake
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
After 2 weeks: After 4 weeks: After 6 weeks: After 8 weeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 5 1 24
4 wks: 6 1 23
6 wks: 9 1 20
8 wks: 13 0 17
Group 2 –Buteyko only

Asthma Research 2002 - 2008
Group 3 –Buteyko & TTT
Subjective Symptoms
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
After 2 weeks: After 4 weeks: After 6 weeks: After 8 weeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 15 3 12
4 wks: 18 5 7
6 wks: 21 2 7
8 wks: 23 0 7

Asthma Research 2002 - 2008
Drug Intake
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
After 2 weeks: After 4 weeks: After 6 weeks: After 8 weeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 5 2 23
4 wks: 9 2 19
6 wks: 15 2 13
8 wks: 17 0 13
Group 3 –Buteyko & TTT
Asthma Research 2002 - 2008
Note:
After completion of the study, the control group were then put through a treatment regime, together with the study and application of the Buteyko Method.

Asthma Research 2002 - 2008
CONCLUSION
Treatment utilising the Buteyko method allowed for a significant improvement in both subjective and objective symptomology over the control group where no active external support was provided. However, the group receiving the combination of Buteyko training, together with manual treatment and orthomolecular support showed the greatest overall improvement of all groups.

Asthma Research 2002 - 2008
UPDATE 2008
Since the completion of this project in 2002, 36 of the original group were re-entered into further research – 17 of whom were ongoing periodic-review patients and 19 of whom agreed to return to take part in the research.
*All 36 people in the study were specifically chosen as having continued to use the Buteyko method as part of their ongoing treatment protocol.

Asthma Research 2002 - 2008
UPDATE 2008
Two phases of research were undertaken –
the first using the Powerbreathe™ as an additional adjunct to the existing treatment regime.
The second phase of the research was to implement a strict dietary control, restricting histamine.

Asthma Research 2002 - 2008
Asthma Research 2002 - 2008
POWERBREATHE DATA:
The magnitude of the breathing effort and dyspnoea is proportional to the magnitude of the motor drive to the inspiratory muscles. The weaker a muscle is, or the greater the impedance it must overcome, the higher is the motor drive required to bring about a given action, and vice versa. Accordingly, strengthening the inspiratory muscles has a universally beneficial effect upon motor drive and dyspnoea...

Asthma Research 2002 - 2008
POWERBREATHE DATA:
Thus, irrespective of its pathophysiological origin, dyspnoea can be ameliorated by specific strength training of the inspiratory muscles. Interestingly, the presence of weakness is not a pre-requisite for this effect, as inspiratory muscle training has been shown to reduce breathing effort in healthy young athletes (McConnell & Romer, 2004b), as well as patients.

Asthma Research 2002 - 2008
MT (Muscle Training) in AsthmaThe role of IMT in the management of asthma has been less widely studied than in COPD, but the data that exists from five randomised controlled trials are unanimously supportive (Weiner et al., 1992; McConnell et al., 1998; Weiner et al., 2000; Weiner et al., 2002a; Weiner et al., 2002b). Patients experience a reduction in dyspnoea, as well as improvements in quality of life. Most striking are the observations that IMT reduces absence from school/work (by ~95%), use of healthcare resources (by ~75%), and the consumption of medication (by ~79%, see figure 4) (Weiner et al., 1992).

Asthma Research 2002 - 2008
Fig.4 Reduction in ß2-agonist use

Asthma Research 2002 - 2008
MT (Muscle Training) in Asthma
Presented at the Medical Research Society, August 1998 Clinical Science: 95: 4P, 1998 Inspiratory muscle training improves lung function and reduces exertional dyspnoea in mild/moderate asthmatics AK McCONNELL, MP CAINE, KJ DONOVAN, AK TOOGOOD and *MR MILLER Sports Medicine & Human Performance Unit, School of Sport & Exercise Sciences & *Department of Medicine, The University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK

Asthma Research 2002 - 2008
CLINICAL APPLICATION
Once again, 3 subgroups were randomly formed, each of 12 people with varying range of ages and debility and the following applications made:

Asthma Research 2002 - 2008
Clinical Application
GROUP 1:Undertook no additional input for the 6 weeks duration of the research.
GROUP 2:Undertook use of the Powerbreathe in place of the Buteyko Method for a period of 6 weeks.
GROUP 3:Undertook use of the Powerbreathe in addition to the Buteyko Method for a period of 6 weeks.

Asthma Research 2002 - 2008
Clinical Application
As before, each of the 36 participants were asked to fill in a questionnaire on a fortnightly basis.
The results were recorded as follows:

Asthma Research 2002 - 2008
Subjective Symptoms
0%
20%
40%
60%
80%
100%
Af ter 2 weeks: Af ter 4 weeks: Af ter 6 weeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 1 4 7
4 wks: 1 7 4
6 wks: 3 2 7
Group 1 –control
Asthma Research 2002 - 2008
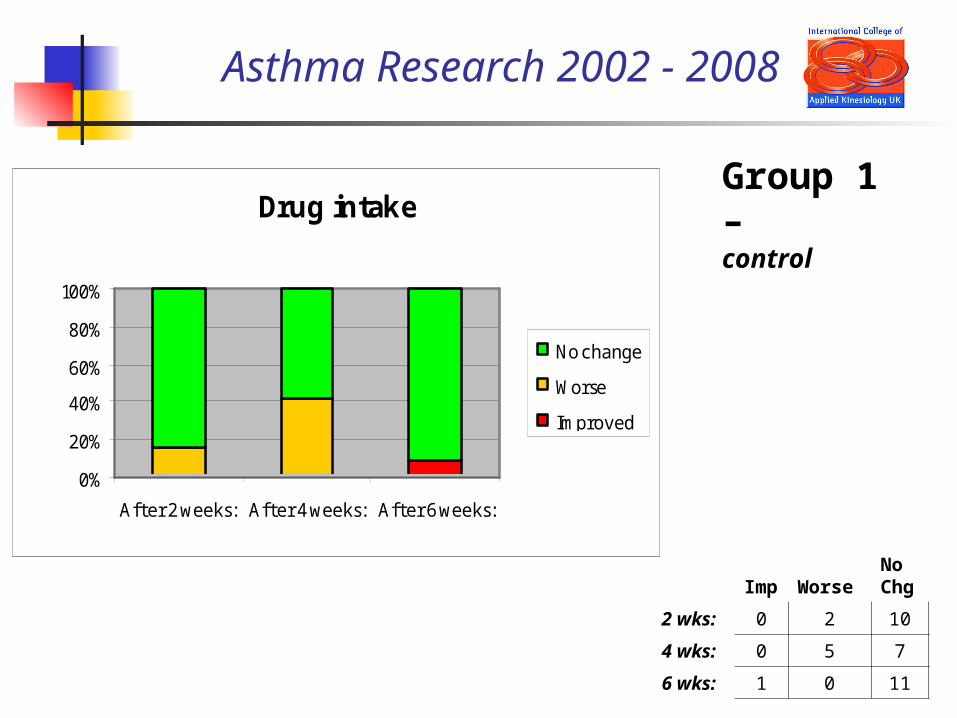
Drug intake
0%
20%
40%
60%
80%
100%
After 2 weeks: After 4 weeks: After 6 weeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 0 2 10
4 wks: 0 5 7
6 wks: 1 0 11
Group 1 –control

Asthma Research 2002 - 2008
Group 2 –Powerbreathe only
Subjective Symptoms
0%
20%
40%
60%
80%
100%
After 2w eeks:
After 4w eeks:
After 6w eeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 0 3 9
4 wks: 3 4 5
6 wks: 5 1 6

Asthma Research 2002 - 2008
Drug intake
0%
20%
40%
60%
80%
100%
After 2w eeks:
After 4w eeks:
After 6w eeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 0 2 10
4 wks: 0 3 9
6 wks: 3 0 9
Group 2 –Powerbreathe only
Asthma Research 2002 - 2008
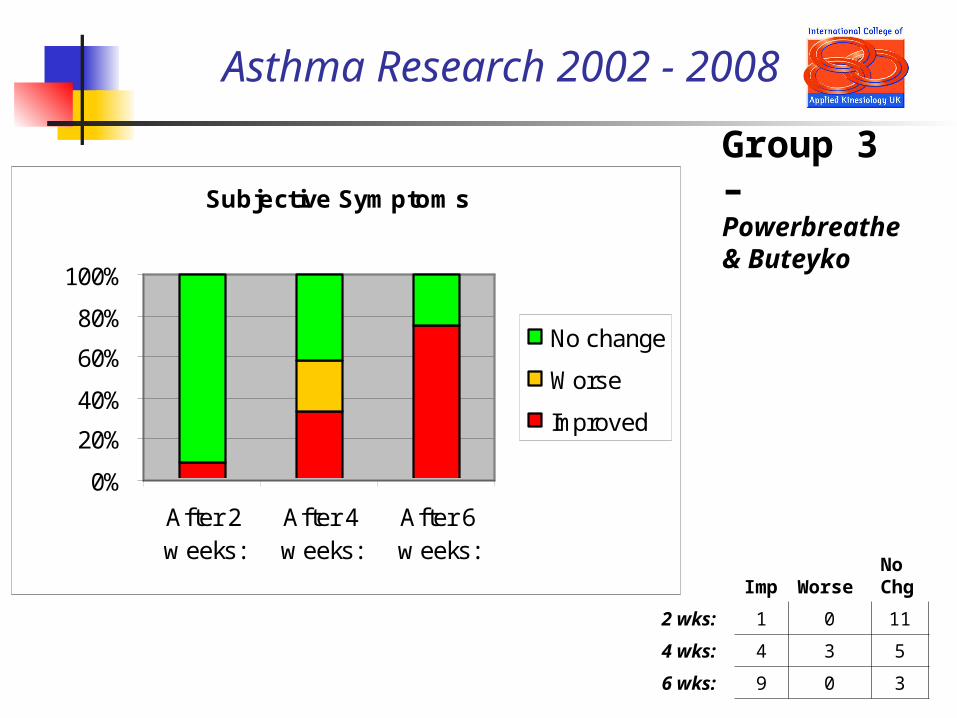
Group 3 –Powerbreathe & Buteyko
Subjective Symptoms
0%
20%
40%
60%
80%
100%
After 2w eeks:
After 4w eeks:
After 6w eeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 1 0 11
4 wks: 4 3 5
6 wks: 9 0 3

Asthma Research 2002 - 2008
Drug intake
0%
20%
40%
60%
80%
100%
After 2w eeks:
After 4w eeks:
After 6w eeks:
No change
Worse
Improved
Imp Worse No Chg
2 wks: 1 0 11
4 wks: 2 1 9
6 wks: 8 0 4
Group 3 –Powerbreathe & Buteyko
Asthma Research 2002 - 2008
Clinical Application
N. B. There was an interesting period between week 4 and week 6, during which time there was a significant deterioration in many of the subjects, but this coincided with a deleterious environmental impact, where there was very high barometric pressure, together with a high pollen count; which probably explained the increased need for inhalers by a large number of the group during this period.
Asthma Research 2002 - 2008
Clinical Application
A two month period was allowed to lapse, during which time all volunteers returned to their regime as it was before the onset of the first trial.
Asthma Research 2002 - 2008
Clinical Application
The second phase of the research was to implement a strict dietary control, whereby the volunteers were divided into two groups of 18. The control group made no changes to their daily routine. The second group were placed on a strict dietary control, whereby all high histamine containing foods were removed from the diet.
Each group was then evaluated after 4 weeks and again after 8 weeks, with the following results recorded:

Asthma Research 2002 - 2008
Group 1 –control
Subjective Symptoms
0%
20%
40%
60%
80%
100%
After 4w eeks:
After 8w eeks:
No change
Worse
Improved
Imp Worse No Chg
4 wks: 2 4 12
8 wks: 2 3 13

Asthma Research 2002 - 2008
Drug intake
0%
20%
40%
60%
80%
100%
After 4w eeks:
After 8w eeks:
No change
Worse
Improved
Imp Worse No Chg
4 wks: 0 2 16
8 wks: 1 3 14
Group 1 –control

Asthma Research 2002 - 2008
Group 2 – Histamine diet
Subjective Symptoms
0%
20%
40%
60%
80%
100%
After 4w eeks:
After 8w eeks:
No change
Worse
Improved
Imp Worse No Chg
4 wks: 13 0 5
8 wks: 15 1 2
Asthma Research 2002 - 2008
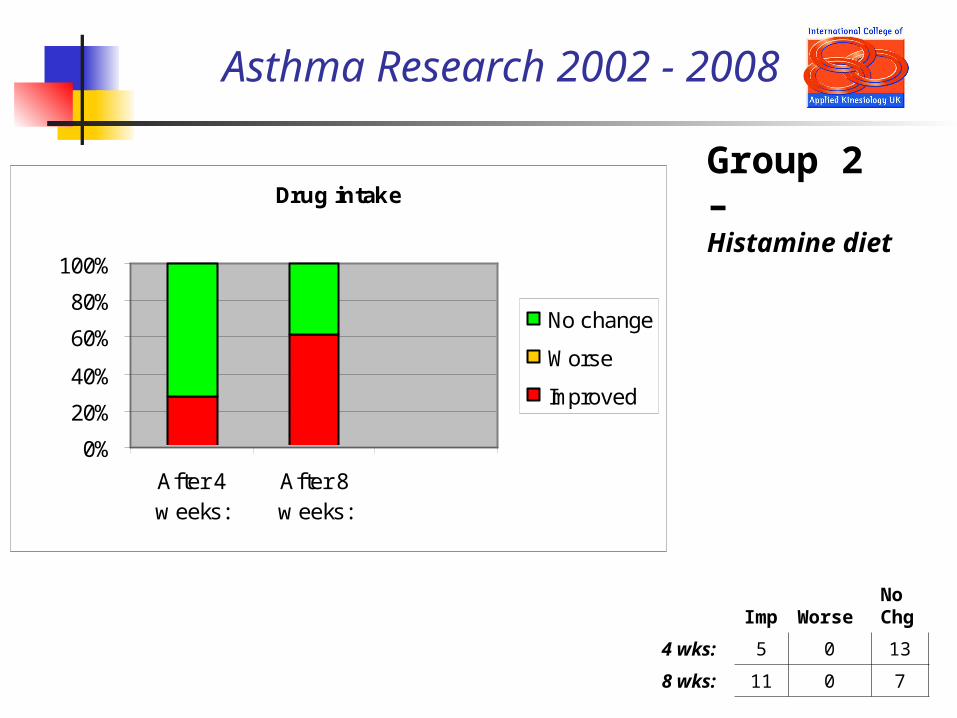
Group 2 –Histamine diet
Drug intake
0%
20%
40%
60%
80%
100%
After 4w eeks:
After 8w eeks:
No change
Worse
Improved
Imp Worse No Chg
4 wks: 5 0 13
8 wks: 11 0 7
Asthma Research 2002 - 2008
Clinical Application
Following on from this research period, each patient was then given a whole blood analysis and prescribed orthomolecular support according to both the results of the blood tests and muscle testing.

Asthma Research 2002 - 2008
Discussion:
IgE reactions resulting in degranulation of the mast cell and histamine release with its physiological consequences –
Contraction of the bronchial muscles, reducing the airway diameter Vasodilation of the blood vessels Increased fluid loss from the arterioles, allowing fluid and immune cells to escape into the surrounding areas oedema and irritation, leading to itching in the skin and blocked nasal passages
are of major significance in many cases of asthma.
. . . /

Asthma Research 2002 - 2008
Discussion:
Taking steps to reduce the overload of histamine in the body – both by reducing intake of high histamine-containing foods and by providing orthomolecular support to
a) inhibit mast cell degranulation and b) increase breakdown of histamine, can have significant subjective and clinical
benefits in chronic asthma patients.. .
. /

Asthma Research 2002 - 2008
Discussion:
All possible input of rehabilitative work to optimise respiratory efficiency and control, both on a conscious and a non-conscious level, has also shown in the research study to significantly improve overall well-being and reduce both subjective symptomology and clinical dependence on prescription medication.
. . . /

Asthma Research 2002 - 2008
Discussion:
This research study is by no means complete in its description of treatment of the asthmatic patient; as many factors are addressed on an individual-needs basis, according to clinical investigation and muscle testing.
However, such variabilities do not fit well into a research protocol and so have not been included in this paper.
Asthma Research 2002 - 2008
Conclusion:
Within this study, the Powerbreathe™ was shown to be an effective additional tool in helping people manage the symptoms of their asthma more effectively, thus allowing them to rely less heavily on prescription medication, with its well-acknowledged detrimental long-term side-effects.
. . . /

Asthma Research 2002 - 2008
Conclusion:
Additionally, the restriction of histamine-containing foods was shown to have a marked effect on presenting symptoms and this was increased further beyond the boundaries of this research study with the application of patient-specific orthomolecular support.
. . . /

Asthma Research 2002 - 2008
Conclusion:
Approaching both the physiological and metabolic deficiencies of patients diagnosed with asthma is of primary importance in providing the individual with a more effective management protocol and the opportunity to reduce or potentially withdraw dependence on
prescription medication.

Asthma Research 2002 - 2008
THANK YOU!





























