-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
1/8
RESPIRATORY SYSTEM (Gross)
Objectives:
Describe the gross features of the tracheobronchial treeo
Identify important structures related to the trachea
and primary bronchi
o Ramifications of the bronchial treeo Orientation of the
primary bronchi and anatomical
basis of the location of aspirated foreign bodies
o Features of bronchopulmonary segments and theirclinical
sig.
Describe gross features of the lungso Surfaces, lobes and
fissureso Differentiate right and left lungso Impressions made on
the mediastinal surfaceo Composition of the root of the lung
Surface projection of the borders and fissures of the lungs
onthe chest wall
Blood supply, innervations, lymphatics Embryologic development
of the tracheobronchial tree (?!?!?!) Describe normal radiologic
features
THE RESPIRATORY SYSTEM (RS)
Component parts:
A. Anatomic divisions1. Upper RS- nose, pharynx and larynx2.
Lower RS- trachea, bronchi, lungs
B. Functional divisions1. Conducting portion
Nasal cavities, pharynx, larynx, trachea,bronchi [can be
extrapulmonary
(primary/main bronchus) or
intrapulmonary(secondary/lobar)],
bronchiole-terminal
2. Respiratory portion Respiratory bronchiole, alveolar
ducts,
alveolar sacs, alveoli
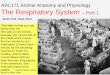
GROSS ANATOMY OF THE LUNGS
conical in shape; reflect space of pleural cavity(except for
costodiaphragmatic andcostomediastinal recesses)
each has an apex, root and base apex aka cupula
o blunt superior end of the lungascending above the level of
the1st rib into the root of the neck for
September 8, 2009
Collapsed Lung Inflated LungCervical part
Costa
part
Pleural cavity
Visceral pleura
Diaphragmaticpart
Parietal Pleura
Mediastinal Part
Gross Respiratory
Dr. Esguerra
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
2/8
about 1 in. (2.5 cm) above theclavicle
o covered by cervical pleurao separated from the neck by
suprapleural membrane or Sibsons
fasciao can be mapped out on the anterior
surface of the body by drawing a
curved line, convex upward, from
the sternoclavicularjoint to a point1 above the junction of the
medialand intermediate thirds of theclavicle.
rooto aka hilum/hiluso point of entry of lymph nodes,
bronchi and pulmonary vesselso structures pass from the neck
to
abdomen (esophagus, bloodvessels, vagus nerve, thoracicanterior
to the root: phrenic nerve
(found within the pericardial lning) base
o concave in shape; conforms todiaphragm
diaphragm on right T8 level
diaphragm on left IVdisc level of T8/T9
o right is higher than the left,because of the liver
o it then follows that the right lung isshorter
o the heart pushes the left lung,therefore right lung is
broader
each has 3 surfaces: costal( related to theribs), mediastinal
(beside the heart)anddiaphragmatic (inferior)
each also has anterior and inferior borders(no posterior border
because at the back, themediastinal surface is continuous to
costal
surface without any edge) Fissures:
Oblique fissureo At the posterior surface, about
2.5 inches from the apex, itfollows the course of 6th ribdown to
inferior border of the
lungo Divides lower lobe of right lung
from the upper and middle
lobes
Horizontal fissureo Divides the middle and upper
lobe of the right lungo Follows the plane of 4th rib as it
attaches to the sternum Formation: each lung bud invaginates the
wall
of the coelomic cavity and then grows to fill a
greater part of the cavity in life, light, soft, spongy and
elastic that it
recoils to about one third their size when the
thoracic cavity is opened in children, they are pink; in adults,
dark and
molted due to inhalation of dust particles
(carbon)
Occupy the thoracic cavity except for the ff:Costodiapharagmatic
recessoSlit-like spaces between the costal and
diaphragmatic parietal pleurae that areseparated only by a
capillary layer of pleural
fluidoLower area of the pleural cavity into which
the lung expands on inspiration
oDuring expiration, the lower margins of thelungs ascend so that
the costal anddiaphragmatic pleurae come together again.
o2 (5 cm) deep in the scapular lineposteriorly
o3 to 3.5 (8-9 cm) in the midaxillary lineo1 to 1.5 (2.5 to 4
cm) in the midclavicular
line
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
3/8
Costomediastinal recess (left)opotential space in the pleural
cavity between
the costal pleura and mediastinal pleura atthe level of the 5th
intercostal space on theleft side in which the lingula expands
into
during inspirationo structures pass the thoracic cavity
posteriorly except the phrenic nerve
which passes anteriorly to the root of the
lung to the pericardium of the heart
*Lingula is a tongue like projection on the left lung analogous
to the
middle lobe of the right lung* 3R, 2L number of lobes, lobar
bronchi and bronchial arteries.*Segue: Amazingly, same trend in the
heart. Right: tricuspid valve,left: bicuspid valve.
BORDERS Anterior
o costal and mediastinal surfaces meetanteriorly and overlap the
heart
o RIGHT LUNG Relatively straight Begins behind the
sternoclavicular
joint and runs downward, almost
reaching the midline behind thesterna angle, then continues
downward reaching the xiphisternaljoint
Thin and overlaps the hearto LEFT LUNG
Similar course as the right lung, butdeviates laterally at the
level of the4th costal cartilage to extend for avariable distance
beyond the lateral
margin of the sternum to form thecardiac notch
Cardiac Notchnotch produced by the heartdisplacing the lung to
the left, creating a thin,
tongue-like process of the superior lobe,LINGULA, which extends
below the cardiacnotch and slides in and out of the
costomediastinal recess during inspiration andexpiration
Posterioro extends downward from the spinousprocess of C7 to the
level of T10 and lies
1.5 (4 cm) from the midlineo thick and lies beside the vertebral
column
Inferioro In the midinspiration, follows a curving
line, which crosses the 6th rib in the
midlavicular line; 8th rib in themidaxillary line and 10th rib
adjacent tothe vertebral column posteriorly
o Level of this border changes duringinspiration and
expiration
RADIOGRAPHY
Chest X-ray: PA Projection (PosteroanteriorView)
For babies: AP Pojection (Anteropsterior) To obtain a
posteroanterior radiograph, the X-
ray are projected from behind the patient to a
plate that is touching the patients chest;structures close to
the plate appear very close tothe actual size, and the structures
further away
appear larger
Hearto In anteroposterior view, it appears much
larger (and less distinct) than in posteroanteriorview
Right Lung Left Lung
# of Lobes 3 2
At the root of the
lung
Azygos arch
impressionAortic arch impression
Pulmonary ligament (mesopneumonium)
double layer of pleura below theroot
covers the root and attaches thelung to the mediastinum
Pulmonary vein posteriorly and inferiorly
located
Lobar bronchi posterior and central
Pulmonary arteries anterior to bronchiPulmonary arteries always
the most
superior structure
Special feature
in some cases,
eparterial bronchus
appears above the
artery
Lingula*
Fissures Oblique, Horizontal Oblique
# of
Bronchopulmonary
segments
10 8
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
4/8
Lungsodense shadows caused by the presence of the
blood-filled pulmonary and bronchial vessels, thelarge bronchi,
and the lymph nodes
olungs are more translucent on full inspirationthan on
expiration
opulmonary blood vessels are seen as a series ofshadows
radiating from the lung root. They
appear as small, round, white shadows
olarge bronchi also cast round shadowsosmaller bronchi are not
seen
Bonesothoracic vertebrae are imperfectly seenocostal cartilages
are not usually seen, but if
calcified, they will be visible
oclavicles are clearly seen crossing the upper partof each lung
field
omedial borders of the scapulae may overlap theperiphery of each
lung field
Diaphragmodiaphragm casts dome-shaped shadows on each
side; the one on the right is slightly higher thanthe one on the
left
ocostophrenic angle,- area where the diaphragmmeets the thoracic
wall
obeneath the right dome is the homogeneous,dense shadow of the
liver
obeneath the left dome a gas bubble may beseen in the fundus of
the stomach
*on x-rays, black-color signifies presence of air. More dense
structuresappear as white (bones). Radiopaque materials (coins,
pins, wire, etc.)
also appear white.
GROSS ANATOMY OF the TRACHEOBRONCHIALTREE
Tracheastarts from larynx (C6 level-lower border of
cricocartilage) up to its bifurcation (carina*)5 in. long, 1 in.
diameterFrom the lower border of the cricoids cartilage
until the level of the 6thcervical vertebra (C6)Bifurcates into
right and left main stem bronchi
(extrapulmonary) at T4and T5
Carina: bifurcation. It is the keel-like ridgebetween the two
openings of the main stembronchi
Main bronchi branch will form the bronchial tree(secondary
intrapulmonary lobar bronchi)
has fibroelastic wall in which are embedded aseries of U-shaped
bars of hyaline cartilagethat keep the lumen patent
posterior free ends are connected by thetrachealis
muscle(regulated by therecurrent laryngeal nerve-branch of
vagus)
*normally located at T4/t5; in deep inspiration, the carina
descends up to the T6 level because the lungs go down
BronchusRight Main Bronchus Left Main Bronchus
Wider Narrower
shorter longer
More vertical More horizontal/lateral
Branches: superior and
intermediate lobar
bronchus
Superior and inferior lobar
bronchus
Latter divides into: middle
and inferior lobar bronchus
*Primary or main stem bronchus divides into*
Lobar Bronchi (secondary bronchi)*Each lobar bronchus divides
into*
Segmental Bronchi (tertiary bronchi)Supply the bronchopulmonary
segmentsName would correspond to the segment it
supplies
THE BRONCHOPULMONARY SEGMENT
pyramidal shaped segment of the lungs with theapex facing the
lung root and the base at the pleura
surface largest subdivision of a lobe anatomic, functional, and
surgical unit of the lungs separated from adjacent segments by
connective
tissue septa
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
5/8
supplied independently by a segmental or tertiarybronchus and a
tertiary branch of a pulmonary
artery named according to the segmental bronchus that
supplies it
drained by pulmonary veins along the connectivetissue septa
(intersegmental drainage)
surgically resectable (Segmentectomy) functionally and
independent unit of the lung with its
own segmental bronchus and artery
Aspiration Pneumonia particles aspirated by an adult in an
upright position will most likely fall tothe right main bronchus
(may go
further to the posterior basal segment) paricles aspirated by an
adult lying on
his right side will most likely fall to the
right main bronchus (may go tofurther to posterior or middle
lobe)
particles aspirated by an adult lying onhis left side will most
likely fall to theleft main bronchus (may go further tolingular
segments)
particles aspirated by an adult lying onhis backwill most likely
fall to the rightmain bronchus (may go further to
superior bronchopulmonary segment ofthe right lower lobe)
particles aspirated by a baby goes toright upper lobe (more
often)
Bronchioles Where cartilage disappearsbronchioles
possess no cartilage in their walls and
are lined with columnar ciliated
epithelium
Arise from the division of the smallestbronchi
Are less than 1mm in diameter Terminal bronchioles
The bronchioles divide and give rise toterminal bronchioleswhich
show
delicate outpouchings from their walls.
Respiratory bronchiole Start of respiratory portion Associated
with alveoli on the walls Gaseous exchange between blood and
air takes place in the walls of these
outpouchings
Alveolar duct The respiratory bronchioles end by
branching into alveolar ducts which lead
into tubular passages with numerous
thin-walled out-pouchings called alveola
sacs
Alveolar Sac Consist of several alveoli opening into a
single chamber
Alveolus The alveolar sacs consist of several
alveoli opening into a single chamber.
Each alveolus is surrounded by a richnetwork of blood
capillaries. Gaseous
exchange takes place between the air in
the alveolar lumen through the alveolar
wall into the blood within the
surrounding capillaries
PULMONARY CIRCULATION (refer to Appendix A)s
Deoxygenated blood form the terminal branches of thepulmonary
arteries is received by the alveoli. The
oxygenated blood leaving the alveolar capillaries drainsinto the
tributaries of the pulmonary veins, which followthe intersegmental
connective tissue septal to the lungroot. Two pulmonary veins leave
each lung root to
empty into the left atrium of the heart.
Segmental bronchus
Pulmonary artery
Pulmonary vein in
intersegmental
connective tissue
Autonomic nerves
Lymphatic vessel
Pulmonary vein
Terminal
bronchiole
Respiratory
bronchiole
Alveolar sac
alveolus
Tracheopulmonary segment
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
6/8
Arteries Pulmonary Artery
- follows the lobes (bronchial branching)and carries
unoxygenated blood fromthe heart
- Upper and lower pulmonary arteriesare drained by one Upper
Pulmonary
Vein Bronchial Artery
-Branch of descending bronchiole
-Trachea to bronchi to respiratorybronchiole-Supplies the
bronchi, connective tissue
to the lung and the visceral pleura-Carries oxygenated
blood-Right Lung: 1(posterior intercostal
artery arises from the left bronchialarteries)-Left Lung:
2(superior and inferior branches of descending thoracic
aorta)-Eventually anastomose with withpulmonary arteries
Veins Pulmonary Vein
- All drain to posterior aspect (LeftAtrium)- Primary drainage
of blood frombronchial artery- NOT the bronchial venous system
(which drains the proximal part of thelungs bronchi and CT
only)- Right Lung: One (1) upper and middle
and one (1) lower- Drain intersegmentally- Left Lung: One (1)
upper and one
lower
- Enters the heart via the left atriumcarrying oxygenated
blood
Bronchial Veins- Communicate with the pulmonaryveins
- Drain into the azygos vein whichcollects posterior intercostal
veins(right) and helmazygos veins (left)
RIGHTSIDE
LEFT SIDE
PulmonaryArtery
Locatedinferior to
theEparterialBronchus
Most superiorstructure (No
bronchus)
BronchialArtery
One (1)Right
bronchialartery
Two (2) LeftBronchial Arteries:
1. SuperiorLBA
2. Inferior LBABoth are branches
of the descendingaorta
BronchialVenousSystem
RBV drainsto theazygos vein
LBV drains to theleft accessoryhemiazygos/intercos
tal vein
Mixing of Oxygenated and Unoxygenated Blood
Occurs in the alveoli, along pleura andintersegmental CT
Bronchial artery with pulmonary vein from alveoliBlood supply
drained from the visceral pleura and thecapillaries
LYMPHATIC DRAINAGE AND NERVOUS SUPPLY
-Follow veins and arteries
-Lymph vessels originate in superficial and deepplexus-Up to
terminal bronchioles only (fluid absorbed
at this level)not present in alveolar walls
Superficial/ Subpleural Plexus- lies beneath the visceral
pleura- drains over the surface of the lung toward the
hilum (lymph vessels enter the bronchopulmonary nodes
Deep Plexus- travels along the bronchi and pulmonaryvessels
toward the hilum of the lung-passes through pulmonary nodes in the
hilum
-all the lymph from the lung leaves the hilumand drains into the
tracheobronchial nodes(superior and inferior tracheobronchial
CARINAL
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
7/8
Nodes paratracheal nodes) and then into thebronchiomedistinal
lymph trunks (along venous
circulation at the junction of subclavian vein andinternal
jugular vein
RIGHT LUNG LEFT LUNG
DRAINAGE RIGHT LYMPHATICDUCT
THORACIC DUCT
Lymph from Hilar
Nodes Carinal/Tracheobronchial Trunk
Right LymphaticTrunk
Subclavian Veinand Internal
Jugular Vein
(Upper lobe) Hilar
Node SuperiorTracheobronchialNodes Left
Paratracheal Nodes Thoracic Duct
(Lower Lobe) HilarNode
Carinal/InferiorTracheobrochial
Right Lung
THORACIC DUCT
- Collects all lymphatics from below the right andleft
diaphragm
- Located at the level of T12- Drains left side of the face and
arm and the left
upper lobe of the lung and below the diaphragm
- Begins in the abdomen as a dilated sac, theCISTERNA CHYLI
- Enters the AORTIC HIATUS (shares the sameforamen with the
aorta)
- 180 turn at C7- Terminates at the junction of the Left
Interna
Jugular Vein and the Left Subclavian Vein
Pulmonary Plexus- Supplies each lung-
Formed by branches of the sympathetic trunkand received
parasympathetic fibers from the- Vagus nerve (CNX): Innervation of
the smoot
muscle of the brachial tree, pulmonary vessels,and the glands of
the bronchial tree via the
pulmonary plexuses located anterior andposterior to the lung
roots
- Postganglionic Sympathetic Fibers from thesympathetic trunks
(bronchodilatorsvasoconstrictors, and inhibit glandular
excretion)
- Preganglionic Parasympathetic Fibers from theVagus Nerve (CNX)
bronchoconstrictorsvasodilators, and secretomotor to the glands
- Visceral Afferent Fibers follow sympathetic fibers carry
information involved in cough reflexesstretch reception, blood
pressurechemoreception, and nociception (also painreceptors
sympathetic over distention)
Left bronchomediastinal lymph
trunk drains into thoracic duct
Paratracheal nodes
Inferior tracheobronchial
(cardinal) nodes
Subpleural lymphatic plexus
Interlobar
lymphatic vessels
Drainage to
mediastinum
enough
pulmonary
ligaments
Deep
lymphatic
drainage
follows the
bronchial tree
Right bronchomediastinal lymph
trunk drains into right lymphatic duct
Superior tracheobronchial nodes
Bronchopulmonary
(hillar) nodes
nterpulmonary
nodes
Anterior
viewEsophageal
plexus
Left Vagus Nerve Left
Phrenic Nerve
Cervical Cardiac Branches
(Vagosympathetic)
Left Recurrent
Pharyngeal Nerve
Pulmonary Plexus
Pulmonary Trunk
Left
Vagus
Nerve
Right
Vagus
Nerve
Right Recurrent
Pharyngeal Nerve
Right Vagus Nerve
Right Phrenic Nerve
-
8/2/2019 2009-09-08 Ana Gross Respiratory 2013
8/8
TEST YOURSELF!1. All of the following commonly occur on
inhalation except:a. The diaphragm descendsb. The external
intercostal muscles
contractc. The abdominal muscles contract and
push the abdominal viscera cranially
d. The ribs are raisede. The visceral dimension of the
thoraciccavity increases
2. With a patient in the standing position, fluid inthe left
increases cavity tends to gravitate downto:
a. The oblique fissuresb. The cardiac notchc. The
costomediastinal recessd. The costodiapragmatic recesse. The
horizontal tissue
3. Which of the following statements is (are)correct regarding
the bronchopulmonary
![Z u ] v W · Gross Necropsy: Gross necropsy includes an external examination of the animal and an examination of the internal organs including those of the respiratory system, digestive](https://img.pdfslide.net/doc/110x75/604e2abb78e41e384932b30f/z-u-v-w-gross-necropsy-gross-necropsy-includes-an-external-examination-of-the.jpg)