Embed Size (px)
Citation preview

ANEURX STENT GRAFT SYSTEM2010 ANNUAL PHYSICIAN CLINICAL UPDATE (VOL VII)January 28, 2011

2
Table of Contents
ABSTRACT .............................................................................................................................. 3 DEVICE DESCRIPTION ......................................................................................................... 4 INTRODUCTION .................................................................................................................... 6 1.0 Clinical Study Experience ............................................................................................. 8
1.1 Primary Safety Analyses ......................................................................................... 10 1.1.1 Ruptures: Kaplan-Meier Analysis................................................................... 10 1.1.2 Surgical Conversion: Kaplan-Meier Analysis ................................................ 11 1.1.3 Aneurysm-Related Death: Kaplan-Meier Analysis ........................................ 12 1.1.4 Mortality (all cause): Kaplan-Meier Analysis ................................................ 15
1.2 Primary Effectiveness Analyses ............................................................................. 16 1.2.1 Prosthesis Migration ....................................................................................... 18 1.2.2 Core Lab (Phase II Patients)/Hospital Observations (Phases II and III) for Device Integrity .............................................................................................................. 22
2.0 AneuRx Stent Graft Post Market Surveillance Study Update ................................... 24 2.1 Principal Safety Results .......................................................................................... 25 2.2 Principal Effectiveness Results ............................................................................... 34
2.2.1 Endoleaks ........................................................................................................ 34 2.2.2 Other Effectiveness Outcomes ........................................................................ 35
3.0 Worldwide Commercial Experience ........................................................................... 38 4.0 Explant Analysis ......................................................................................................... 43
4.1.1 Explant Summary of Observations ................................................................. 44 5.0 Notes to Clinicians ...................................................................................................... 49 6.0 Brief Summary of Indications for Use, Warnings and Precautions ........................... 51

3
ABSTRACT Medtronic Vascular is pleased to present you with our seventh edition of this report. The purpose of this report is to provide physicians with current information on clinical study and post- market commercial experience of the AneuRx Stent Graft System. While the Clinical and Post- market sections of the report contains important information, particularly relevant data is included in the cumulative clinical trial and commercial experience (Section 2 and Section 3) – involving more than 91,000 patients treated with the AneuRx Stent Graft System.
The clinical study experience (Section 1) presented in this report incorporates the final clinical data through study closure for the AneuRx Clinical Study (IDE), which was completed and closed on September 24, 2008. The results from the clinical study continue to support the safety and effectiveness of the AneuRx Stent Graft System. Patients treated with the AneuRx Stent Graft in the study had a 5-year freedom from rupture rate of 96.8 % and a 5-year freedom from conversion to surgical repair rate of 92.2%. This report also includes AneuRx Post-Market Surveillance Registry data (Section 2). The AneuRx Post-Market Surveillance Registry was closed on March 5, 2009. Furthermore, this report includes data relating to the worldwide commercial experience data between 1997 and June 2010. The report also includes analysis of explants data from patients who were implanted between 1996 and 2010.
Our hope is that the information provided in this report will help you make informed decisions regarding your patients with abdominal aortic aneurysms (AAA) who have been treated with the AneuRx Stent Graft System or who may be considering the AneuRx Stent Graft System as their treatment option. The results published in this report continues to support that the AneuRx stent graft is a safe and effective therapy option for appropriately selected patients.

4
DEVICE DESCRIPTION The AneuRx AAAdvantage® Stent Graft with the Xcelerant® Hydro Delivery System (HDS) is designed to treat infrarenal abdominal aortic or aorto-iliac aneurysms using an endovascular approach. When placed within the aneurysm, the graft provides an alternative conduit for blood flow within the patient’s vasculature by excluding the aneurysmal sac from blood flow and pressure.
ANEURX AAADVANTAGE STENT GRAFT
The AneuRx AAAdvantage Stent Graft (Figure 0-1) is constructed from self-expanding nickel-titanium (Nitinol) alloy stent rings and woven polyester graft material. Each stent ring is a series of diamond-shaped segments connected side-to-side in the circumferential direction to form a ring. The diamond-shaped segments are laser cut from a single piece of Nitinol tubing.
The AneuRx AAAdvantage Stent Graft includes:
• a stent graft (either bifurcated stent graft, iliac limb stent graft, iliac extender cuff stent graft or aortic extender cuff stent graft) that is modular and fully stented along its length;
• radiopaque markers placed in the stent graft proximally and distally; the markers are visualized under fluoroscopy.
Figure 0-1: AneuRx AAAdvantage Stent Graft

5
XCELERANT HYDRO DELIVERY SYSTEM (HDS)
The stent graft is loaded inside the Xcelerant HDS. The Xcelerant HDS is a hydrophilic coated delivery system, which facilitates the placement of the stent graft via the arterial vasculature (e.g., femoral arteries). Using fluoroscopic guidance, the Xcelerant HDS is properly positioned within the patient’s vasculature and the stent graft is deployed from the Xcelerant HDS.
The Xcelerant HDS consists of:
• a single use, disposable system with an integrated handle intended to provide the user with controlled deployment.
• a flexible catheter assembly compatible with a 0.035” guidewire. • three concentric single lumen polymer shafts (an outer graft cover shaft with
hydrophilic coating, an inner member shaft, and a guidewire lumen). • runners attached to the distal end of the inner member shaft intended to reduce
friction between the stent graft and the graft cover. • a polymeric, atraumatic tip attached at the distal end intended to facilitate tracking
through tortuous and calcified vessels. • a radiopaque tip, a marker at the distal end of the stent graft, and a marker on the
distal end of the graft cover intended to aid in fluoroscopic visualization. • o-rings contained within the delivery system intended to maintain hemostasis during
the procedure. Retraction of the graft cover allows deployment of the self-expanding stent grafts. Post deployment, the physician will recapture the runners and tip of the delivery system by retracting the inner member.
Figure 0-2: AneuRx AAAdvantage Stent Graft with Xcelerant HDS
1. Tapered Tip 8. Handle Disassembly Ports 2. RO Marker Band 9. Front Grip 3. Runners 10. Trigger 4. AneuRx AAAdvantage Stent Graft
11. Slider
5. Distal RO Marker 12. Rear Grip 6. Graft Cover 13. Quick Disconnect 7. Strain Relief 14. Touchy Burst
A B
Detail A
Detail B
12 10 9 7
11 8 6
4 3 2
1 5
13
14

6
INTRODUCTION This report is divided into six sections:
• Section I contains final clinical data results from the entire U.S. IDE cohort, and data collected through five years on 1193 patients. These data include safety endpoints (patient mortality, rupture, surgical conversion) as well as key endovascular effectiveness measures (endoleak, aneurysm size, migration, graft kinking and device integrity).
• Section II contains final clinical data results from the AneuRx Stent Graft Post Market Surveillance studies.
• Section III summarizes information regarding aneurysm rupture, surgical conversion, and aneurysm-related death from combined global commercial experience.
• Section IV summarizes the results from Medtronic’s explant analysis,
• Section V provides notes to clinicians,
• Section VI provides summary comments.
DEVICE DEVELOPMENT HISTORY Device Development History
The current device commercially available in the United States is the AneuRx AAAdvantage Stent Graft with the Xcelerant Hydro Delivery System. The device and delivery system underwent several modifications since its conception and the current system is the 7th generation. The changes that the device underwent are briefly explained below.
Modifications to the AneuRx Stent Graft System
In reviewing this report, it is important to remember that the AneuRx Stent Graft has undergone a number of technology improvements since the original clinical trial. Based on the evolving results of the IDE trial, our experience with over 68,000-update US bifurcated implants, and valuable feedback from physicians, we have continued to build upon the success of the initial AneuRx platform by incorporating new design elements and more advanced technologies.
The AneuRx AAA Stent Graft has been in clinical use since June of 1996; however, since that time, there have been many changes to the stent graft. The first generation of the AneuRx stent graft was designed with a “stiff body”, which consisted of a 5 cm stent structure that limited conformability in tortuous anatomy. The design of the stent graft was updated during the Phase II US Clinical Trial to include individual one cm stent rings to assist in conformability; additionally, the graft material was changed to a “Reduced Porosity Material” (RPM) during this time.

7
In 2000, an update to the delivery system was made, which incorporated a tapered proximal tip, replacing the original “bullet” tip delivery system used during the clinical trial. In 2002, the delivery system was further changed to add a lubricious coating on the inner aspect of the graft cover to aid in deployment of the stent graft; this iteration is the Xpedient Delivery System. The delivery system was further enhanced in 2004. This new delivery system (the Xcelerant Delivery System) was introduced in January 2005 following approval by FDA on October 28, 2004. Modifications to the delivery system include an integrated handle and a radiopaque marker on the distal end of the graft cover to aid in the accuracy of stent graft placement.
In 2004, explant findings prompted a further change in the graft material from the RPM graft material to a greater density graft material (“Resilient”). The latest modifications to the AneuRx Stent Graft were implemented after FDA approval on March 17, 2006. The seventh generation, the AneuRx AAAdvantage Stent Graft System with the Xcelerant Hydro Delivery System, was approved by FDA on December 6, 2007. This is the currently commercialized design of the delivery system.

8
1.0 Clinical Study Experience From 1996 through 1999, 1193 subjects participated in the AneuRx Stent Graft System clinical study at 19 U.S. investigational sites, in which subjects were enrolled in three phases.
Phase I enrolled forty (40) subjects between June 3, 1996 and April 8, 1997. The Phase II pivotal stent graft cohort enrolled four hundred twenty-four (424) subjects between April 9, 1997 and September 30, 1998. The 424 subjects enrolled in Phase II include additional patients which were enrolled after the submission of the PMA. The PMA submission included the initial 416 subjects from Phase II and 66 open surgical treatment control subjects, both with one (1) year of clinical follow-up. The Phase III cohort enrolled six hundred thirty-nine (639) subjects between August 21, 1998 and September 30, 1999. Ninety (90) additional subjects who did not meet the study’s inclusion criteria were enrolled in the Emergency Use/ Miscellaneous/ High-risk (EU/ Misc/ HR) arm of the study. The subject enrollment described above is summarized in Table 1-1 below.
The date of data cut-off for the results contained in the IDE clinical study close out report is March 18, 2008. All final clinical data was presented to FDA on May 22, 2008 within an AneuRx Clinical Study Final Report, which was subsequently closed by FDA on September 24, 2008.
Table 1-1: IDE Study Subject Enrollments
IDE Study Enrollment Dates Subjects (Device Design)
EU/Misc/ HR Arm (Device Design) Total
Phase I 03 June 1996 – 08 April 1997
40 (all stiff body design) N/A 40
Phase II 09 April 1997 – 30 September 1998
424 (134 with stiff body design and 290 with flex body design)
46 (flex body design) 470
Phase III 21 August 1998 – 30 September 1999
639 (all with flex body) 44 (flex body 683
Total 1103 90 1193 As indicated in Table 1-1, 40 patients in Phase I and 134 patients in Phase II (for a total of 174 patients) received an early device design which incorporated a unibody “stiff” stent in the aortic body of the device. The remaining 1019 patients were implanted with a device design that incorporated a multi-segmented “flexible” aortic body. This “flexible” device design is incorporated into the currently marketed endograft, which is commercially available today. Additionally, the delivery system used in the clinical study when all 1193 patients were enrolled was the older generation “Bullet” delivery system which has since been modified into the “Xpedient” delivery system in 2002 and ultimately the “Xcelerent” delivery system in 2005.

9
The data presented below and throughout this report includes all 1193 patients implanted with both stiff-body and flexible devices using the “Bullet” delivery system, and includes patients that were followed through March 19, 2008. One patient is not included in the rupture, survival, and aneurysm-related death analyses because this patient received a conversion device. The conversion device was approved as a treatment arm of the IDE and is intended for use with the bifurcated device.
Table 1-2 below provides a summary of clinical results relating to rates of rupture, conversion, aneurysm-related death, and all-cause mortality. Two sets of aneurysm related data (per Medtronic clinical definition and per FDA’s suggested definition as denoted in footnotes 3 & 4) are presented in the table. Please see Section 1.1.3 of the update for detailed information on the aneurysm-related death.
Kaplan-Meier summaries are provided for endpoints for each year of follow-up, out to five years. A breakdown of the number of patients followed through each follow-up period for the clinical data presented in this report is provided in Appendix A.
Table 1-2: Rupture, Conversion, and Death1
Number (m/n) & percent (%)
Number only (m/n) 5 Kaplan-Meier Summaries
Kaplan-Meier Estimates (%)
Intra-op
<30 Days2
>30 Days
Total 1 Year
2 Years
3 Years
4 Years
5 Years
Aneurysm Rupture
2/1193 (0.17%)
3/1193 (0.25%)
21/1193 26/1193 Freedom from Aneurysm Rupture
99.5 98.7 98.4 97.4 96.8
Conversion to Surgical Repair
11/1193 (0.92%)
4/1193 (0.34%)
52/1193 67/1193 Freedom from Conversion
98.5 96.9 95.3 93.4 92.2
Aneurysm Related Death
MDT3 0 23/1193 (1.93%)
15/1193 38/1193 Freedom from Aneurysm Related Death
MDT3 98.0 97.6 97.2 96.8 96.0
FDA4 0 23/1193 (1.93%)
27/1193 50/1193 FDA4 97.6 97.0 96.7 95.7 94.6
Death (all- cause)
0 23/1193 (1.93%)
379/1193 402/1193 Probability of Survival (based on all-cause mortality)
91.5 82.7 77.0 68.6 60.1
1 Includes final patient data approved on September 24, 2008. 2 Post-operative,but within 30 days. 3 Aneurysm related death as defined in the AneuRx Clinical Study (MDT), is any death occurring within 30 days of the initial procedure, a rupture, a conversion, or any other secondary procedure of the specific aneurysm that is being treated with the AneuRx Stent Graft System. Excluded are aneurysms in other anatomical areas. 4 Aneurysm-related death (ARD) is currently defined as deaths from rupture of the AAA or from any procedure intended to treat the AAA. If death occurred within one month of any procedure to treat the AAA, it was presumed to be aneurysm-related, unless there was evidence to the contrary. 5 Patients within this group are at a variety of follow-up periods; therefore rates are not given for these columns. Please refer to Kaplan-Meier estimates for specific projections for patients >30 days post procedure.

10
Table 1-3 below outlines the primary causes of the 67 conversions to open surgery among the 1193 patients reported in Table 1-1 above.
Table 1-3: Primary Causes and Reasons For Conversion
Reasons for Conversions Rupture 18 Endoleak with AAA Expansion 13
Endoleak 12 Failure to Access 10 AAA Expansion 6 Migration/Displacement of modular component 5 Other 3 Total Reasons 67
1.1 Primary Safety Analyses The following pages contain Kaplan-Meier analyses of outcomes during the U.S. IDE trial, along with a detailed data summary provided for each Kaplan-Meier curve.
1.1.1 Ruptures: Kaplan-Meier Analysis As demonstrated in the analysis below, patients treated with the AneuRx Stent Graft have a 5-year freedom from rupture rate of 96.8%.
Time in Months
Free
dom
from
Rup
ture
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Figure 1-1: Freedom from Ruptures

11
1.1.1.1 Summary of Kaplan-Meier Curve For additional information on the number of patients followed at these time intervals, please refer to Appendix A.
Table 1-4: Summary of Kaplan-Meier Curve for Ruptures
Summary of Kaplan-Meier Curve
Treatment to
30 days 31 days to
1 year 1 year to 2 years
2 years to 3 years
3 years to 4 years
4 years to 5 years
# at risk1 1193 1163 1046 900 769 599
# of events 5 1 8 2 7 3
# censored2 25 116 138 129 163 237
Cumulative Censored3
25 141 279 408 571 808
Kaplan-Meier estimate4
0.996 0.995 0.987 0.984 0.974 0.968
Standard Error
0.002 0.002 0.004 0.004 0.006 0.006
95% Confidence Interval
0.992 - 1.000 0.991 - 0.999 0.979 - 0.995 0.976 - 0.992 0.962 - 0.986 0.956 - 0.980
1The number of patients at risk at the beginning of interval (based on actual implantation duration). 2Patients are censored due to insufficient implant duration or loss to follow-up. 3The total censored for all time intervals up to and including that specific time interval. 4Estimate made at end of time interval.
1.1.2 Surgical Conversion: Kaplan-Meier Analysis As demonstrated in the analysis below, patients treated with the AneuRx Stent Graft have a 5-year freedom from surgical conversion rate of 92.2%. Ten of the 67 surgical conversions experienced immediate conversion at the time of surgery due to failure to access.
Time in Months
Free
dom
from
Surg
ical C
onve
rsion
s
0 10 20 30 40 50 60
0.00.2
0.40.6
0.81.0
Figure 1-2: Freedom from Surgical Conversion

12
1.1.2.1 Summary of Kaplan Meier-Curve For additional information on the number of patients followed at these time intervals, please refer to Appendix A
Table 1-5: Summary of Kaplan-Meier Curve for Surgical Conversion
Summary of Kaplan-Meier Curve
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
4 years to 5 years
# at risk1 1193 1152 1042 897 769 600 # of events 15 3 15 14 14 6 # censored2 26 107 130 114 155 235 Cumulative Censored3
26 133 263 377 532 767
Kaplan-Meier estimate4
0.987 0.985 0.969 0.953 0.934 0.922
Standard Error
0.003 0.004 0.005 0.007 0.008 0.009
95% Confidence Interval
0.981 - 0.993 0.977 - 0.993 0.959 - 0.979 0.939 - 0.967 0.918 - 0.950 0.904 - 0.940
1The number of patients at risk at the beginning of interval (based on actual implantation duration). 2Patients are censored due to insufficient implant duration or loss to follow-up. 3The total censored for all time intervals up to and including that specific time interval. 4Estimate made at end of time interval.
1.1.3 Aneurysm-Related Death: Kaplan-Meier Analysis Aneurysm-related death was initially defined (per the initial Medtronic AneuRx clinical study) as any death occurring within 30 days of the initial treatment, a rupture, a conversion, or any other secondary stent graft procedure. The Kaplan-Meier analysis as illustrated in Figure 1-3 below uses this clinical study definition. As demonstrated in the Table 1-6 below, patients treated with the AneuRx Stent Graft have a 5-year freedom from aneurysm-related death rate of 96.0%.
In collaboration with the FDA, the definition of aneurysm-related death has been updated to include deaths from rupture of the AAA or from any procedure intended to treat the AAA. If death occurs within one month of any procedure to treat the AAA, it is presumed to be aneurysm-related, unless there is evidence to the contrary. Using this broader definition, an additional evaluation of all deaths resulted in seven patients with deaths that may be considered as aneurysm-related even though they expired after 30 days of the initial procedure. In addition, there were five deaths for which the underlying cause of death is unknown. These 12 patients do not meet the clinical study definition for aneurysm-related death; however, they are added to this category when using the broader definition. Therefore, using this definition, the 5-year freedom from aneurysm-related death rate would be 94.6% as shown in Figure 1-4 and Table 1-7. Refer to Table 1-2 and its related footnotes for aneurysm related death calculations using this alternate FDA definition.

13
1.1.3.1 Aneurysm-Related Death: Kaplan-Meier Analysis- Medtronic definition
Time in Months
Free
dom
from
Ane
urys
m-R
elat
ed D
eath
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Figure 1-3: Freedom from Aneurysm-Related Death – Medtronic Definition
1.1.3.2 Summary of Kaplan-Meier Curve
For additional information on the number of patients followed at these time intervals, please refer to Appendix A.
Table 1-6: Summary of Kaplan-Meier Curve for ARD (Medtronic definition)
Summary of Kaplan-Meier Curve
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
4 years to 5 years
# at risk1 1193 1165 1048 902 771 601 # of events 23 1 4 3 3 4 # censored2 5 116 142 128 167 238 Cumulative Censored3
5 121 263 391 558 796
Kaplan-Meier estimate4
0.981 0.980 0.976 0.972 0.968 0.960
Standard Error
0.004 0.004 0.005 0.005 0.006 0.007
95% Confidence Interval
0.973 - 0.989 0.972 - 0.988 0.966 - 0.986 0.962 - 0.982 0.956 - 0.980 0.946 - 0.974
1The number of patients at risk at the beginning of interval (based on actual implantation duration). 2Patients are censored due to insufficient implant duration or loss to follow-up. 3The total censored for all time intervals up to and including that specific time interval. 4Estimate made at end of time interval.

14
1.1.3.3 Aneurysm -Related Death: Kaplan-Meier Analysis- FDA definition
Time in Months
Free
dom
from
Ane
urys
m-R
elat
ed D
eath
(FD
A D
efin
ition
)
0 10 20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Figure 1-4: Freedom from Aneurysm-Related Death – FDA Definition

15
1.1.3.4 Summary of Kaplan-Meier Curve
For additional information on the number of patients followed at these time intervals, please refer to Appendix A.
Table 1-7: Freedom from Aneurysm-Related Death – FDA Definition
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
4 years to 5 years
# at risk1 1193 1165 1048 902 771 601
# of events 23 6 5 3 7 6
# censored2 5 111 141 128 163 236
Kaplan-Meier estimate3 0.981 0.976 0.970 0.967 0.957 0.946
Standard Error 0.004 0.004 0.005 0.005 0.007 0.008
95% Confidence Interval
0.973 - 0.989
0.968 - 0.984
0.960 - 0.980
0.957 - 0.977
0.943 - 0.971
0.930 - 0.962
1 The number of subjects at risk at the beginning of interval (based on actual implantation duration). 2 Subjects are censored due to insufficient implant duration or loss to follow-up. 3 Estimate made at end of time interval.
1.1.4 Mortality (all cause): Kaplan-Meier Analysis As demonstrated in the analysis below, patients treated with the AneuRx Stent Graft have a 5-year probability of survival (based on all-cause mortality) of 60.1%.
Time in Months
Free
dom
from
Death
0 10 20 30 40 50 60
0.00.2
0.40.6
0.81.0
Figure 1-5: Freedom from Mortality (all cause)

16
1.1.4.1 Summary of Kaplan-Meier Curve
For additional information on the number of patients followed at these time intervals, please refer to Appendix A.
Table 1-8: Summary of Kaplan-Meier Curve for Mortality (all cause)
Summary of Kaplan-Meier Curve
Treatment to 30 days
31 days to 1year
1 year to 2 years
2 years to 3 years
3 years to 4 years
4 years to 5 years
# at risk1 1193 1165 1048 902 771 601 # of events 23 77 98 60 78 66 # censored2 5 40 48 71 92 176 Cumulative Censored3
5 45 93 164 256 432
Kaplan-Meier estimate4
0.981 0.915 0.827 0.770 0.686 0.601
Standard Error 0.004 0.008 0.011 0.013 0.014 0.016 95% Confidence Interval
0.973 - 0.989
0.899 - 0.931 0.805 - 0.849 0.745 - 0.795 0.659 - 0.713 0.570 - 0.632
1The number of patients at risk at the beginning of interval (based on actual implantation duration). 2Patients are censored due to insufficient implant duration or loss to follow-up. 3The total censored for all time intervals up to and including that specific time interval. 4Estimate made at end of time interval.
1.2 Primary Effectiveness Analyses Below Table 1-9 contains effectiveness data for the entire AneuRx clinical cohort (N=1193), as defined and reported by the investigating physician at each time interval on the case report form (CRF). The decrease in denominators could be attributed to the data point not having been collected at the visit or the patient missing the follow up visit. Effectiveness outcomes were not always confirmed by an imaging study due to the method of data collection required by the CRFs. Medtronic Vascular would like to stress that imaging is required to adequately assess effectiveness outcomes. Please refer to Appendix A for corresponding site reported imaging compliance.

17
Table 1-9: Effectiveness Outcomes (Site Reported)
Site Reported Effectiveness Table - Phases I, II, III, EU/Misc/HR (n = 1193) 1
Pre-Discharge
1 Month 6 Months 1 Year 2 Years 3 Years 4 Years 5 Years
Endoleak2 27.88% (310/1112)
14.13% (151/1069)
15.20% (152/1000)
15.07% (145/962)
17.86% (147/823)
15.92% (110/691)
15.43% (83/538)
14.98% (62/414)
Enlarged Aneurysm3
N/A 8.82% (48/544)
5.23% (39/746)
7.07% (51/721)
8.94% (55/615)
11.71% (61/521)
13.73% (56/408)
19.06% (61/320)
Migration4 0.45% (5/1103)
0.31% (3/961)
1.17% (11/937)
2.40% (22/916)
5.87% (46/784)
7.44% (52/699)
9.61% (52/541)
7.99% (33/413)
Patency 99.82% (1111/1113)
99.34% (1048/1055)
99.39% (985/991)
99.38% (957/963)
99.27% (811/817)
98.85% (685/693)
98.70% (531/538)
99.27% (410/413)
1All 1193 patients were treated with the older generation device. The graft material was Reduced Porosity graft Material (RPM) and the currently commercialized AneuRx graft material uses the “Resilient” High Density Material (HDM). The commercially available device also has strategically placed RO markers and an extended aortic body for enhanced proximal seal. 2 Specific types of endoleak were not reported. 3 Aneurysm Enlargement uses both site and Core Lab data. This endpoint is defined as any increase >5mm as compared to pre-discharge measurement. 4 Prosthesis migration was defined as any post implantation movement reported by the Investigator.
Table 1-10 below contains core lab reported effectiveness data for Phase II (N=424) of the AneuRx clinical study. Core lab data collection was not required for any other Phases of the clinical study. Please refer to Appendix A for corresponding core lab imaging compliance.
Table 1-10: Effectiveness Outcomes (Core Lab Reported)
CoreLab Reported Effectiveness Table - Phase II (n=424) 1
Pre-
Discharge 1 Month 6 Months 1 Year 2 Years 3 Years 4 Years 5 Years Endoleak 2 49.72%
(177/356) 47.97% (59/123)
25.00% (81/324)
21.50% (63/293)
22.22% (52/234)
21.08% (39/185)
19.05% (24/126)
14.52% (9/62)
Enlarged3
Aneurysm N/A 0.79%
(1/126) 1.85% (6/325)
3.91% (12/307)
9.33% (25/268)
11.07% (27/244)
12.70% (24/189)
17.11% (26/152)
Migration4 0.00% (0/375)
0.00% (0/295)
1.38% (5/362)
1.45% (5/346)
4.63% (13/281)
4.66% (11/236)
6.25% (10/160)
0.00% (0/105)
Patency 99.46% (371/373)
99.26% (134/135)
99.13% (341/344)
98.40% (307/312)
98.41% (248/252)
97.64% (207/212)
97.81% (134/137)
96.20% (76/79)
1.All 424 patients were treated with the older generation Reduced Porosity graft Material (RPM). Currently commercialized AneuRx graft material uses the “Resilient” High Density Material (HDM). 134 of the 424 Phase II patients received the 1st generation “stiff body” stent design, all remaining patients received the newer “flex-body” stent design. 2 Endoleak was defined by the CoreLab as any evidence for contrast outside the endovascular prosthesis. Specific types of endoleak were not reported. 3 Aneurysm Enlargement uses both site and CoreLab data. This endpoint is defined as any increase >5mm as compared to pre-discharge measurement. 4 Migration was defined by the CoreLab as any evidence for device migration.

18
1.2.1 Prosthesis Migration Medtronic Vascular is dedicated to understanding the risk and root causes for migration associated with the AneuRx Stent Graft. Migration is defined as any post implantation movement reported by the investigator. As shown above in Table 1-9, there were a total of 224 reports of migration from pre-discharge through five years post treatment. These 224 reports of migration occurred in 163 patients
Of the 163 patients with reported migration, secondary procedures related to migration were performed in 48 patients. The predominant secondary procedure was insertion of an aortic cuff or graft limb extension which was required in forty (40) of these forty-eight patients. A total of eight patients were successfully converted to surgery, two of whom were reported to have suffered an aneurysm rupture. None of the 48 secondary procedures resulted in death. The remaining 115 patients did not require a secondary procedure to treat migration.
As shown in Section II, AneuRx Stent Graft Post Market Surveillance Study Update, (Refer to Table 2-12) there was one report of migration was documented in the Lifeline Registry at two years and three reports of migration reported in the Post Market Surveillance Registry. One report of migration was noted at the one year follow-up interval, and two instances were reported at the four year follow-up interval.
A comparison was performed evaluating field complaints when migration was reported. Based on complaints reported as of July 1, 2008, the primary conclusion is that reported commercial migration complaints versus implant duration appears to be steady over time based on results from similar KM curves for those implanted between 2000-2002 and those implanted between 2003-2005. The freedom from migration rate based on reported migration events was estimated as 99.4% (lower C.I. 99.0%) at 2.7 years.
In July 2006, the AneuRx Migration Questionnaire was introduced to physicians to promote the documentation of specific information related to the occurrence of migration as part of Medtronic Vascular’s ongoing quality assurance program. When a migration was reported, information using the questionnaire includes the distance of the device migration, the duration of implant to migration, secondary procedures, achieved fixation of neck length compared with available fixation neck length, length of distal iliac fixation, migration associated with neck angle, and documentation of potential root causes. These results are then compared with published results. After one hundred and forty seven (147) responses to date, results are consistent with reported literature.

19
An extensive review of published literature regarding migration with the AneuRx Stent Graft was performed. A wide range of migration rates (1%-40%)1-7 were reported from single center experiences based on a variety of migration definitions, and some with small sample sizes and short-term follow-up durations that may have influenced the rates. Due to the inconsistency in reporting migration, only those articles that met the Society Vascular Surgery (SVS)/ American Association for Vascular Surgery (AAVS) reporting standard definition8 for migration and included greater than 23 months mean follow-up were included in the publication summary. The SVS/AAVS reporting standards definition for migration is 1) device movement of greater than 10 mm; or 2) movement of 10 mm or less resulting in a secondary intervention or producing symptoms. The literature did not provide results to distinguish between the two definitions for device movement. Table 1-11 below provides a summary of publications that discuss migration rates, potential causes, clinical consequences, and aneurysm-related death.

20
Table 1-11: Migration Rates from the Published Literature
Publication # Implants Migration Rate
Mean Follow-
Up (Month)
Migration Definition
Potential Causes
Clinical Consequences # Aneurysm
Related Death
Cao, et.al, 20029
113 15% (17) 28 >10 mm -27 (24%) oversizing <10% -AAA diameter >5.5 cm (15%) -Neck enlargement >10%
8 required secondary intervention; 6 cuff placement, 2 conversions, including 1 rupture.
0
Azizzadeh, et al, 200510
365 4% (15) 23.7 >10 mm -Neck angulation 45º -Neck thrombus -Reverse neck taper -Short necks <15 mm
20/365 (5.5%) with prox. attachment failure required reintervention. 15/20 had proximal migration and 5/20 had suboptimal attachment. >90% treated with cuffs. 2/365 (0.05%) required conversion.
0
Heikkinen, et al, 200511
173 I:Good aortic/good iliac= 45 II:Intermediate/bad aortic/good iliac=18 III:Good aortic/ intermediate/ bad iliac=58 IV:Intermediate/bad aortic/ intermediate/ bad iliac=52
10% (17) Group I: 0% Group II: 0% Group III: 8.6% (5/58) Group IV: 23.1% (12/52)
23 >10 mm Poor iliac fixation, where iliac limbs were >10 mm from the iliac bifurcation
9 patients required secondary intervention; 5 patients required both proximal and distal ext. cuffs and 4 patients distal ext. cuffs. Group III: 1 elective conversion. Group IV: 1 rupture with subsequent conversion; 2 elective conversions.
0
Fulton, et al, 200612
FNA 59 (70%) (Favorable Neck Anatomy)
6.1% (4) 40.3 > 10 mm None given for FNA group.
3 Secondary interventions with cuff placement. No conversions.
0

21
Publication # Implants Migration Rate
Mean Follow-
Up (Month)
Migration Definition
Potential Causes
Clinical Consequences # Aneurysm
Related Death
UFNA 25 (30%) (Unfavorable Neck Anatomy)
42% (10) -> 45º neck angulation -Longer initial graft to renal artery distance -Proximal neck length <15 mm -Endograft sizing <10%
7 Secondary interventions with cuff placement. No conversions.
0
Abbruzzese, et al, 200813
277 3.25% (9) 31.3 >5mm 23.8% of grafts were placed outside of at least one IFU Parameter 21.3% oversizing
6 required proximal cuff placement One required AUI conversion with fem-fem bypass
102
Van Herwaarden, et al, 200714
212 12.3% (26) 52.0 Any movement
None given 22 secondary interventions due to migration with 16 cuff placements and 6 Talent aorto-monoiliac devices placed
131
1 Number listed is overall aneurysm-related death as deaths due to or following noted migration was not available.

22
Significant predictors of migration for the AneuRx Stent Graft System were reported in the published literature as short proximal and distal fixation lengths, proximal neck angulation, incorrect stent graft sizing, and aortic neck dilatation.1-4 Based upon the literature review, it is probable that migration is related to suboptimal anatomy. As shown in Table 1-11, the clinical consequences were comprised primarily of secondary inventions (5.4%) requiring cuff placement. There were a low number of migrations that led to conversion (1.1%) and/or rupture (0.3%) and zero deaths were reported. Device migration rates were within range of the published literature (5-42%) when compared with the overall results from the IDE clinical trial (7.99%), however, direct comparisons are limited due to the use of different definitions of migration. The difference may also be partially explained by differences in patient selection during the clinical study as compared to after commercialization. The clinical consequences reported in the published literature for migration were similar to those reported earlier for the IDE clinical trial group.
Since the first use of the AneuRx Stent Graft System in 1996, several design improvements have been made including two major delivery system and graft material upgrades. The latest enhancement provided with the AneuRx AAAdvantage included an extended aortic body and strategically-placed radiopaque markers to facilitate accurate placement, as well as the addition of hydrophilic coating to the Xcelerant Delivery System. As stated in the AneuRx AAAdvantage IFU, precise stent graft placement, coupled with appropriately selected patients with infrarenal abdominal aneurysms, are critical factors that lead to successful clinical outcomes.
1.2.2 Core Lab (Phase II Patients)/Hospital Observations (Phases II and III) for Device Integrity
Medtronic Vascular required an independent Core Lab to analyze images for the Phase II (IDE Cohort) patients. As part of the clinical study and routine follow-up, data were analyzed for “Device Integrity”. This endpoint was based on Core Lab determination of whether devices displayed a stent fracture or (probable/possible) suture break.
A total of 111 Phase II and III clinical trial patients had one or more device integrity reports, as compared to 91 patients in the 4th edition of this clinical update. Prior to closure of the AneuRx Clinical Trial (FDA closure was granted on 24 September 2008), a reconciliation project of Core Lab films took place, which has influenced this number.
Table 1-12: Clinical Trial Patients with One or More Device Integrity Reports
Clinical Trial Patients With One or More Device Integrity Reports
Phase II (n=424)
Phase III (n=639)
Total (n=1063)
Core Lab Reported 1, 2 71 N/A 71 Hospital Reported 18 22 40 Total 111
1Core Lab evaluations were based on review of plain abdominal X-rays (protocol requirement) 2Core Lab evaluations were not required for Phase III patients.
23
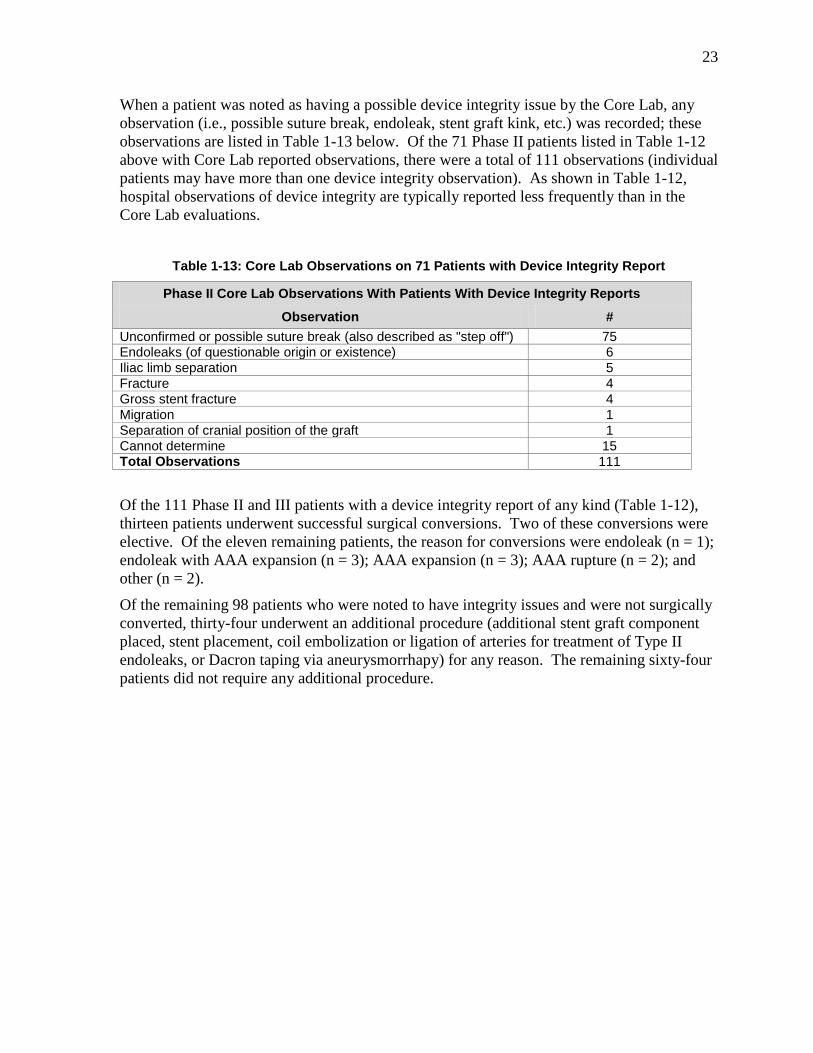
When a patient was noted as having a possible device integrity issue by the Core Lab, any observation (i.e., possible suture break, endoleak, stent graft kink, etc.) was recorded; these observations are listed in Table 1-13 below. Of the 71 Phase II patients listed in Table 1-12 above with Core Lab reported observations, there were a total of 111 observations (individual patients may have more than one device integrity observation). As shown in Table 1-12, hospital observations of device integrity are typically reported less frequently than in the Core Lab evaluations.
Table 1-13: Core Lab Observations on 71 Patients with Device Integrity Report
Phase II Core Lab Observations With Patients With Device Integrity Reports
Observation # Unconfirmed or possible suture break (also described as "step off") 75 Endoleaks (of questionable origin or existence) 6 Iliac limb separation 5 Fracture 4 Gross stent fracture 4 Migration 1 Separation of cranial position of the graft 1 Cannot determine 15 Total Observations 111
Of the 111 Phase II and III patients with a device integrity report of any kind (Table 1-12), thirteen patients underwent successful surgical conversions. Two of these conversions were elective. Of the eleven remaining patients, the reason for conversions were endoleak (n = 1); endoleak with AAA expansion (n = 3); AAA expansion (n = 3); AAA rupture (n = 2); and other (n = 2).
Of the remaining 98 patients who were noted to have integrity issues and were not surgically converted, thirty-four underwent an additional procedure (additional stent graft component placed, stent placement, coil embolization or ligation of arteries for treatment of Type II endoleaks, or Dacron taping via aneurysmorrhapy) for any reason. The remaining sixty-four patients did not require any additional procedure.
24
2.0 AneuRx Stent Graft Post Market Surveillance Study Update
The AneuRx Stent Graft Post-Market Surveillance Plan provides information on prospective data collection from the commercially-available AneuRx Stent Graft System in two registries: the Lifeline Registry of Endovascular Aneurysm Repair sponsored by The American Vascular Association: A Foundation of the Society for Vascular Surgery (SVS) and the Post-Market Surveillance Registry (PS Registry) sponsored by Medtronic Vascular.
The data collected on commercial use of the AneuRx device have the purpose of ensuring appropriate labeling of the device for use in the designated subject populations for which the risk-benefit profile is known to be favorable and to confirm the appropriate and necessary training and experience for users of the device. The post-market surveillance study was also designed to assist in identifying factors that contribute to the likelihood of both favorable and unfavorable subject outcomes, such as subject demographics and anatomical characteristics, procedural methods, and physician training. FDA granted approval to close the Post-Market Surveillance Registry (PS Registry) on February 5, 2009 (data collected through February 28, 2008). The Lifeline Registry has been closed by SVS since July 2005. As such, this section provides final results for the two registries.
Enrollment Table 2-1 provides a summary of the registry enrollment.
Table 2-1: Summary of Registry Enrollment
# Centers # Enrolled Lifeline Registry 5 189 PS Registry 8 160
TOTAL 13 349 Demographics and Anatomic Characteristics Table 2-2 provides the Lifeline Registry and PS Registry subject demographics and anatomical characteristic information and provides the percentage of the concomitant factors associated with each subject enrolled. It must be noted that subjects who had more than one concomitant factor in their medical history at the time of enrollment (baseline) were counted in each category.

25
Table 2-2: Lifeline and PS Registry Baseline Demographics and Characteristics
Lifeline (n = 189)
PS Registry (n = 160)1
Gender-Male 84.1%(159/189) 86.9%(139/160)
Gender-Female 15.9%(30/189) 13.1% (21/160) Age (mean, years) 75.1 ± 8.53 74.3 ± 7.31 AAA Diameter (mean, mm) 2 55.0 ± 9.62 53.6 ± 8.50 Neck Diameter (mean, mm) 3 22.0 ± 2.40 No Data Neck Length (mean, mm) 4 27.0 ± 14.51 30.9 ± 11.30 Neck Angulation ≥ 45° (%) 27.2% (22/81) 0.0% (0/1)
Proximal Neck Length < 10 mm 5.8% (5/86) 1.4% (1/71) History of Tobacco Use 22.6% (37/164) 17.6% (28/159) ASA Grade < 3 6.0% (11/182) 14.4% (23/160) ASA Grade ≥ 3 94.0% (171/182) 85.6% (137/160)
History of Cancer 20.5% (38/185) 25.9% (41/158) History of Hypertension 67.9% (127/187) 73.8% (118/160) Heart Issues5 47.6% (89/187) 57.5% (92/160) History of Diabetes 10.7% (20/187) 17.0% (27/159)
History of Creatinine ≥ 3.0 mg/dL(%)
6.1% (5/82) 0.0% (0/160)
History of COPD 17.2% (32/186) 34.0% (53/156) History of PVD 9.1% (17/186) 18.1% (29/160) 1 One subject at site #115 was consented prior to IRB approval. Subject was removed per IRB instructions. This subject was reported in previous reports and has been removed from this year’s dataset. 2 AAA diameter was not collected for 104 Lifeline subjects, and 88 PS Registry subjects 3 Neck diameter was not collected for 105 Lifeline subjects, and all PS Registry subjects. 4 Neck length was not collected for 103 Lifeline subjects, and 89 PS Registry subjects. 5 Heart issues defined as history of Coronary Artery Disease, Myocardial Infarction, Valvular Heart Disease or Congestive Heart Failure
2.1 Principal Safety Results
Results – Primary Safety Outcomes The analyses for Death, Aneurysm-Related Death, Ruptures, and Surgical Conversions are being provided in a subject-month format. These analyses are provided in Table 2-3 for the Lifeline Registry and PS Registry.

26
Table 2-3: Subject-Month Follow-up for Principal Safety Results1
Event Lifeline Registry PS Registry Total Deaths 21 20 Aneurysm-Related Deaths 0 3 Ruptures 0 1 Total Surgical Conversions 1 22
Failure to Access: (0) (1) 1 Day Post-op to 30 Days: (0) (0)
> 30 Days: (1) (1) Total Subject-Months of Follow-Up3 2794.94 3764.76 Mean Follow-Up (months) 14.8 23.5
1 Data reported through 5 years of follow up for the Lifeline Registry and through 4 years of follow up for the PS Registry. 2 One subject was previously reported as a surgical conversion in error. The total number of surgical conversions in PS Registry is 2 which was inadvertently reported as 3 in the previous version 3 The calculation used to determine the subject-month analyses is subject month = 12 x [date of last visit- procedure date (or event date, i.e., Death, Surgical Conversion or Rupture)] ÷ 365.25. The mean follow-up = the total subject-months of follow-up divided by the number of subjects.
The date a subject is removed from the study is actually the date the clinical research coordinator completes the case report form. This does not necessarily guarantee the subject was known to be alive at that date. For this reason, the subject-month calculation is based on the last known follow-up date, rather than the date the subject was removed from the study.
Lifeline and PS Registry Safety Data The principal safety (Death, Aneurysm-Related Death, Rupture, and Surgical Conversion) results are provided in Figure 2-1and Figure 2-2 using Kaplan-Meier estimates for the Lifeline Registry and PS Registry. Results are only provided through 4 years of follow-up due to the limited amount of data available between 4 and 5 years. Standard error bars are included and illustrate a higher rate of variability due to the relatively smaller number of patients with longer-term follow up in the registries. Kaplan-Meier estimates are not provided for aneurysm-related death in the Lifeline Registry, as there were no reports of aneurysm-related death in the registry.

27
Time in Months
Free
dom
from
Dea
th
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Lifeline
Figure 2-1: Freedom from Death in the Lifeline Registry
Table 2-4: Lifeline Registry Summary of Kaplan-Meier Curve-Freedom from Death
Intra-operative
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
# at risk 189 188 141 74 51 35 # of events 0 3 10 2 2 2 # censored 1 44 57 21 14 17 Kaplan-Meier estimate
1.000 0.982 0.885 0.856 0.812 0.743
Standard Error 0.000 0.011 0.031 0.036 0.046 0.063 95% Confidence Interval
N/A 0.960 - 1.000
0.824 - 0.946
0.785 - 0.927
0.722 - 0.902 0.620 - 0.866

28
Time in Months
Free
dom
from
Dea
th
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
PS Registry
Figure 2-2: Freedom from Death in the PS Registry
Table 2-5: PS Registry Summary of Kaplan-Meier Curve-Freedom from Death
Intra-operative
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
# at risk 160 160 145 120 83 37 # of events 0 1 8 5 5 1 # censored 0 14 17 32 41 30 Kaplan-Meier estimate
1.000 0.993 0.935 0.889 0.813 0.784
Standard Error 0.000 0.007 0.021 0.028 0.043 0.050 95% Confidence Interval
N/A 0.979 - 1.000
0.894 - 0.976
0.834 - 0.944
0.729 - 0.897
0.686 - 0.882

29
Time in Months
Free
dom
from
Dea
th
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
PS Registry
Figure 2-3: Freedom from Aneurysm-Related Death in the PS Registry
Table 2-6: PS Registry Summary of Kaplan-Meier Curve Freedom from Aneurysm-Related
Death
Intra-
operative Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
PS Registry # at risk 160 160 145 120 83 37 # of events 0 1 2 0 0 0 # censored 0 14 23 37 46 31 Kaplan-Meier estimate
1.000 0.993 0.979 0.979 0.979 0.979
Standard Error
0.000 0.007 0.012 0.012 0.012 0.012
95% Confidence Interval
N/A 0.979 - 1.000
0.955 - 1.000
0.955 - 1.000
0.955 - 1.000
0.955 - 1.000

30
Time in Months
Free
dom
from
AA
A R
uptu
re
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Lifeline
Figure 2-4: Freedom from AAA Rupture in the Lifeline Registry
Table 2-7: Lifeline Registry Summary of Kaplan-Meier Curve-Freedom from Rupture
Intra-operative
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
# at risk 189 188 141 74 51 35 # of events 0 0 0 0 0 0 # censored 1 47 67 23 16 19 Kaplan-Meier estimate
1.000 1.000 1.000 1.000 1.000 1.000
Standard Error 0.000 0.000 0.000 0.000 0.000 0.000 95% Confidence Interval
N/A N/A N/A N/A N/A N/A

31
Time in Months
Free
dom
from
AAA
Rup
ture
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
PS Registry
Figure 2-5: Freedom from AAA Rupture in the PS Registry
Table 2-8: PS Registry Summary of Kaplan-Meier Curve-Freedom from Rupture
Intra-operative
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
# at risk 160 160 145 120 83 37 # of events 0 0 1 0 0 0 # censored 0 15 24 37 46 31 Kaplan-Meier estimate
1.000 1.000 0.993 0.993 0.993 0.993
Standard Error 0.000 0.000 0.007 0.007 0.007 0.007 95% Confidence Interval
N/A N/A 0.979 - 1.000
0.979 - 1.000
0.979 - 1.000
0.979 - 1.000

32
Time in Months
Free
dom
from
Con
vers
ion
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
Lifeline
Figure 2-6: Freedom from Surgical Conversion in the Lifeline Registry
Table 2-9: Lifeline Registry Summary of Kaplan-Meier Curve-Freedom from
Surgical Conversion
Intra-operative
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
# at risk 189 188 141 74 51 35 # of events 0 0 0 0 0 1 # censored 1 47 67 23 16 18 Kaplan-Meier estimate
1.000 1.000 1.000 1.000 1.000 0.957
Standard Error 0.000 0.000 0.000 0.000 0.000 0.043 95% Confidence Interval
N/A N/A N/A N/A N/A 0.873 - 1.000

33
Time in Months
Free
dom
from
Con
vers
ion
0 10 20 30 40
0.0
0.2
0.4
0.6
0.8
1.0
PS Registry
Figure 2-7: Freedom from Surgical Conversion in the PS Registry
Table 2-10: PS Registry Summary of Kaplan-Meier Curve-Freedom from
Surgical Conversion
Intra-operative
Treatment to 30 days
31 days to 1 year
1 year to 2 years
2 years to 3 years
3 years to 4 years
# at risk 160 159 145 120 83 37 # of events 1 0 1 0 0 0 # censored 0 14 24 37 46 31 Kaplan-Meier estimate
0.994 0.994 0.986 0.986 0.986 0.986
Standard Error 0.006 0.006 0.010 0.010 0.010 0.010 95% Confidence Interval
0.982 - 1.000
0.982 - 1.000
0.966 - 1.000
0.966 - 1.000
0.966 - 1.000
0.966 - 1.000

34
2.2 Principal Effectiveness Results
2.2.1 Endoleaks Table 2-11 provides reported rates of endoleaks in the Lifeline and PS Registries, as defined and reported by the investigating physician at each time interval on the case report form (CRF).The reported endoleak rate includes all types, including Type IV transgraft leaks. Endoleaks are typically identified through imaging at subject follow-up visits, and not necessarily at the time of occurrence. In the case of the registries, when an endoleak is observed, it is noted on the case report form related to the time when the subject had imaging performed. Endoleaks were not always confirmed by an imaging study due to the method of data collection required by the CRFs. Medtronic Vascular would like to stress that imaging is required to adequately assess endoleaks.
Table 2-11: Reported Endoleaks- Lifeline and PS Registries
PS Registry Lifeline Registry
Intra-Operative
# of subjects with visits 160 189
Unknown/No response 0.6% (1/160) 1.1% (2/189)
Endoleak1 26.4% (42/159) 22.5% (42/187)
New 100.0% (42/42) 100.0% (42/42)
At 30 day Follow-Up
# of subjects with visits 146 162
Unknown/No response 0.0% (0/146) 4.9% (8/162)
Endoleak1 13.7% (20/146) 14.3% (22/154)
New 75.0% (15/20) 54.5% (12/22)
Continuing 25.0% (5/20) 45.5% (10/22)
At 1 Year Follow-Up
# of subjects with visits 105 78
Unknown/No response 1.0% (1/105) 17.9% (14/78)
Endoleak1 16.3% (17/104) 12.5% (8/64)
New 47.1% (8/17) 50.0% (4/8)
Continuing 52.9% (9/17) 50.0% (4/8)
At 2 Year Follow-Up
# of subjects with visits 84 55
Unknown/No response 0.0% (0/84) 14.5% (8/55)
Endoleak1 19.0% (16/84) 14.9% (7/47)
New 43.8% (7/16) 14.3% (1/7)
Continuing 56.3% (9/16) 85.7% (6/7)

35
PS Registry Lifeline Registry
At 3 Year Follow-Up
# of subjects with visits 47 36
Unknown/No response 0.0% (0/47) 16.7% (6/36)
Endoleak1 6.4% (3/47) 23.3% (7/30)
New 0.0% (0/3) 28.6% (2/7)
Continuing 100.0% (3/3) 71.4% (5/7)
At 4 Year Follow-Up
# of subjects with visits 21 19
Unknown/No response 0.0% (0/21) 31.6% (6/19)
Endoleak1 9.5% (2/21) 15.4% (2/13)
New 100.0% (2/2) 0.0% (0/2)
Continuing 0.0% (0/2) 100.0% (2/2) 1 The decrease in denominators from the total number of subjects with visits to the denominators for the total number of endoleaks answered on the CRF are attributed to the data point not having been collected on the CRF or the physician indicated “does not know” on the CRF at the time of the visit.
2.2.2 Other Effectiveness Outcomes Table 2-12 provides reported rates of migration in the Lifeline and PS Registries, as defined and reported by the investigating physician at each time interval on the case report form (CRF).Migration was defined for both registries as longitudinal movement of all or part of a stent or attachment system for a distance of >5 mm relative to anatomical landmarks determined at the time of the initial endovascular procedure.
Table 2-12: Reported Migration for PS and Lifeline Registries
PS Registry Lifeline Registry
Intra-Operative
At 30 day Follow-Up
# of subjects with visits 146 162
Unknown/No response 0.0% (0/146) 12.3% (20/162)
Migration1 0.0% (0/146) 0.0% (0/142)
At 1 Year Follow-Up
# of subjects with visits 105 78
Unknown/No response 0.0% (0/105) 24.4% (19/78)
Migration1 1.0% (1/105) 0.0% (0/59)
At 2 Year Follow-Up

36
PS Registry Lifeline Registry
# of subjects with visits 84 55
Unknown/No response 0.0% (0/84) 29.1% (16/55)
Migration1 0.0% (0/84) 2.6% (1/39)
At 3 Year Follow-Up
# of subjects with visits 47 36
Unknown/No response 0.0% (0/47) 44.4% (16/36)
Migration1 0.0% (0/47) 0.0% (0/20)
At 4 Year Follow-Up
# of subjects with visits 21 19
Unknown/No response 0.0% (0/21) 42.1% (8/19)
Migration1 9.5% (2/21) 0.0% (0/11) 1 The decrease in denominators from the total number of subjects with visits to the denominators for the total number of migrations answered on the CRF are attributed to the data point not having been collected on the CRF or the physician indicated “does not know” on the CRF at the time of the visit. Table 2-13 provides reported changes in aneurysm diameter in the Lifeline and PS Registries, as defined and reported by the investigating physician at each time interval on the case report form (CRF).
Aneurysm enlargement was defined for both registries as an increase in the diameter of the aneurysm sac, greater than or equal to 5 mm since the last follow-up. Aneurysm enlargement data was derived from actual maximum aneurysm diameter measurements entered on the CRF.

37
Table 2-13: Reported Changes in Aneurysm Diameter for Lifeline and PS Registries
Lifeline Registry PS Registry 1 Month to 6 Months # of subjects with both visits 92 70
Increased > 5 mm1 0.0% (0/39) 7.1% (4/56) Decreased > 5 mm1 0.0% (0/39) 25.0% (14/56) No Change in Size1 100.0% (39/39) 67.9% (38/56)
6 Months to 1 Year # of subjects with both visits 76 59
Increased > 5 mm1 0.0% (0/30) 9.3% (5/54) Decreased > 5 mm1 0.0% (0/30) 22.2% (12/54) No Change in Size1 100.0% (30/30) 68.5% (37/54)
1 Year to 2 Years # of subjects with both visits 53 70
Increased > 5 mm1 5.0% (1/20) 10.6% (7/66) Decreased > 5 mm1 0.0% (0/20) 18.2% (12/66) No Change in Size1 95.0% (19/20) 71.2% (47/66)
2 Years to 3 Years # of subjects with both visits 33 41
Increased > 5 mm1 0.0% (0/21) 2.8% (1/36) Decreased > 5 mm1 0.0% (0/21) 16.7% (6/36) No Change in Size1 100.0% (21/21) 80.6% (29/36)
3 Years to 4 Years # of subjects with both visits 17 15
Increased > 5 mm1 8.3% (1/12) 23.1% (3/13) Decreased > 5 mm1 0.0% (0/12) 7.7% (1/13) No Change in Size1 91.7% (11/12) 69.2% (9/13)
4 Years to 5 Years # of subjects with both visits 9
Increased > 5 mm1 0.0% (0/7) Decreased > 5 mm1 0.0% (0/7) No Change in Size1 100.0% (7/7)
1 The decrease in denominators from the total number of subjects with both visits to the denominators for the number of changes in the aneurysm diameter (indicated as Increased, Decreased or No Change) answered on the CRF are attributed to the data point not having been collected on the CRF or the physician indicated “does not know” on the CRF at the time of the visit.

38
3.0 Worldwide Commercial Experience As of June 30, 2010, over 91,000 AneuRx Stent Grafts have been distributed worldwide (over 87,000 stent grafts in the United States and over 3,500 stent grafts outside the United States). From this commercial experience, Medtronic gathers product performance reports via field reports and our explant analysis program.
The data presented in Table 3-1 summarizes reports of adverse events from worldwide commercial experience with the AneuRx Stent Graft through June 30, 2010. The data in this table includes both acute and chronic reported events for devices implanted since 1997 (OUS) and 1999 (USA). As per the current AneuRx Instructions for Use (IFU), regular patient follow-up (including imaging) is required. Imaging should be scheduled based on the physician’s clinical assessment of the patient pre- and post-implantation of the stent graft. Both the type of imaging modality and the frequency of imaging should be individualized to meet the patient’s specific needs.
Table 3-1: Summary of Commercial Experience
Adverse Event Type US
(September 28, 1999 to June 30, 2010)
International (November1997
to June 30, 2010) Rupture 275 18 Conversion 643 30 Aneurysm-related Death* 242 8 *Aneurysm-related death is defined as any death occurring within 30 days of the initial treatment, a rupture, a conversion, or any other secondary stent graft procedure
The data presented in Table 3-2 summarize adverse events from worldwide commercial experience from July 2009 through June 30, 2010. All the complaints reported were noted to be US based as no complaints were received from outside of US. Additional details for these adverse event types are presented in the information that follows Table 3-2.

39
Table 3-2: Summary of Reported Adverse Events from Worldwide Commercial Experience
Adverse Event Type* US (July 1, 2009 to June 30,2010)
Ruptures (Post-implant) 26
Surgical Conversion 57
Aneurysm-Related Death 27
Migration (ANY movement)** 121
Integrity (fractures) 31 *The majority of these reported events were observed at time points spanning the duration of the implant (1,2,3,4 years, etc). As recommended in the AneuRx Instructions for Use, regular patient follow up and imaging is required **The majority of the migration events were observed to be for patients also having disease progression and/ or neck angulation. Summary of Aneurysm –Related Mortality Events
A total of 27 aneurysm related deaths have been reported worldwide between July 2009 and June 2010 in subjects treated with the AneuRx Stent Graft devices.
Table 3-3: Summary of Aneurysm Related Mortality
Cause for Aneurysm Related Mortality1 Number of Cases Ruptures: Post Implant Aneurysm Rupture Pre- Op Rupture
6 2 4
Severe blood loss due to pre-exisiting patient condition 4
Unknown2 6 Others3 11 1Aneurysm-related mortality is defined as any death occurring within 30 days of the index procedure, or due to a rupture, conversion or secondary procedure. 2 This category includes an event where adequate information is not received from the site in order to determine cause of death. 3 These events include infrequent events where the cause of death is not stent graft related such as MI, cardiac event, multi- organ failure, aspiration, patient condition, or arthro- emoli shower along with liver and kidney failure.

40
Summary of Post-Implant Aneurysm Ruptures
There have been a total of 26 post-implant aneurysm ruptures reported to Medtronic between July 2009 and June 2010. As shown in the table below, the primary cause of aneurysm ruptures were endoleaks and migrations.
Table 3-4 below lists the causes of ruptures whereas Table 3-5 lists the time frame of each rupture
Table 3-4: Summary of Post-Implant Aneurysm Ruptures
Causes of Ruptures Number of Cases
Aneurysm Expansion
• Type I Endoleak (proximal and distal)
• Type III Endoleak
4
3
1
Endoleaks
• Type I
• Type II
• Type III (fabric)
• Unknown type
10
3
1
5
1
Migration 9
Others* 3
* Includes events where adequate information is not available in order to determine cause of rupture or when cause of rupture could not be determined by the site.
Table 3-5: Time frames for Ruptures
Time Period
Within 1 year post
implant
1 year post
implant
2 years post
implant
3 years post
implant
4 years post
implant
5 years post
implant
6 years post
implant
7 years post
implant
8 years post
implant
9 years post
implant
10 years post
implant Number of ruptures
0 0 61 32 43 14 25 46 17 18 19
1 The causes of the six ruptures included three migration, three endoleaks (distal type I, proximal type I, type III- junctional). 2 The causes of the three ruptures included two migration and one aneurysm enlargement. 3 The causes of the four ruptures included two migration, one type III (fabric) endoleak, and one due to another manufacturer’s stent graft falling out of the aortic neck. 4 The cause of rupture was due to an unknown type of endoleak.. 5 The causes of ruptures included one endoleak (type III- fabric) and one iliac artery aneurysm enlargement. 6 The cause of the rupture included two type I endoleaks, one migration and one unknown reason,. 7 The cause of the rupture was migration. 8 The cause of the rupture was aneurysm expansion. 9 The cause of the rupture was type III (junctional) endoleak. Note: There were three ruptures whose time frames are unknown and hence not listed in this table.

41
Summary of Conversions
Conversion to open repair has been reported between July 2009 and June 2010 in 57 patients treated with the AneuRx Stent Graft. The primary causes of these conversions are listed in the Table 3-6 below whereas Table 3-7 lists the time frame of each conversion.
Table 3-6: Summary of Conversions
Cause for Conversions Number of cases
Aneurysm Rupture
• Pre- operative
• Post- operative
9
1
8
Endoleaks
• Type I
• Type II
• Type III (junctional)
7
4
1
2
Implantation Difficulties1
• Inaccurate delivery
• Cannulation difficulties and deployment complications
• Positioning difficulties
• Delivery System Removal Difficulties
7
1
3
1
2
Aneurysm Enlargement
• Type I and type II
• Persistent type II
• Persistent unknown type of endoleak
• Migration
• unknown
11
1
4
1
2
3
Migrations 13
Unknown 1
Other2 9 1Problems associated with the implantation of components during the procedure 2Other less frequent events resulting in conversions such as calcifications and unsuitable anatomy.

42
Table 3-7: Time frames for Conversions
Time Period
Within 1 year post
implant
1 year post
implant
2 years post
implant
3 years post
implant
4 years post
implant
5 years post
implant
6 years post
implant
7 years post
implant 8 years post
implant
Number of ruptures
121 72 73 64 45 86 77 28 29
1 The causes of the twelve conversions included five implantation difficulties (one inaccurate delivery, one deployment difficulties, one positioning difficulties, two cannulation difficulties), one tamponade of the left common iliac artery, one perforation of the aorta, one type III (junctional), one due to no vessel for the stent graft to adhere to, one pre- operative rupture, two rupture of aorta due to excessive ballooning. 2 The causes of the seven conversions included two migration, two aneurysm enlargement (one due to persistent unknown type of endoleak and one due to both type I and type II endoleaks), one failed distal bypass, one removal difficulty, one stent graft infection,. 3 The causes of the seven conversions included two migration, one delivery catherter removal difficulty, two post- implant rupture, two endoleaks (one type II endoleak, one type III -junctional). 4 The causes of the six conversions were three migrations, three aneurysm expansions (one due to migration, one due to persistent type II endoleak, and one unknown reason). 5 The causes of four ruptures included one post- implant rupture, one disease progression and aortic neck angulation, one dissection of the aorta, and one migration. 6 The causes of the eight conversions included three migration, two aneurysm enlargement (one due to persistent type II endoleak), one post- implant rupture, one unknown reason, one type I endoleak . 7 The causes of the seven conversions were four aneurysm expansions (two due to persistent type II endoleak, one due to migration, and one due to unknown reason), two migrations, one post- implant rupture of iliac artery aneurysm. 8The causes of the two conversions were one migration and one persistent type I endoleak. 9The causes of the two conversions were one migration and one post- implant rupture. Note: There were 2 open surgical conversions whose time frames are unknown and hence not listed in this table.
Device Integrity (fractures)
A total of thirty one cases with stent graft fractures have been reported to Medtronic between July 2009 and June 2010. Of these thirty one cases, fourteen were converted to open surgery and two observed aneurysm expansion in the presence of broken suture and type III (fabric). The remaining fifteen cases observed endoleaks (two unknown type and thirteen type III) which were resolved using cuffs.
Migrations
For purposes of the commercial adverse event information, “stent graft migration” is defined as ANY reported movement of the stent graft post implantation. Migration has been reported to occur over the duration of the implant time. As such and per the AneuRx Instructions for Use, regular patient follow up and imaging is required. A total of 121 migrations were reported to Medtronic from July 1, 2009 to June 30, 2010. Of these 121 migrations, 82 also reported the presence of disease progression and/or neck angulations.

43
4.0 Explant Analysis Medtronic Vascular has collected and analyzed the AneuRx Stent Graft devices that were implanted and subsequently explanted either during conversion to open surgical repair or in conjunction with an autopsy. As of June 30, 2010, Medtronic Vascular completed explant analyses on 440 explant cases that encompass patients who were implanted over the period of time between 1996 and 2010. Data from the explant program are used to guide ongoing product development, improvement, and training programs.
The sources of explanted devices are listed below in Table 4-1.
Table 4-1: Sources of Explanted Devices
Number from Surgical Conversions
Number from Autopsies Following Rupture
Number from Incidental Autopsies
Total Number
From IDE clinical study (of 1,193 patients enrolled) 53 2 32 87
From US commercial sales (of 87,349 primary components distributed as of June 30, 2010)
293 2 10 305
From commercial sales outside of the United States (of 3885 primary components distributed as of June 30, 2010 )
41 0 7 48
Totals 387 4 49 440
Each explanted device received by Medtronic Vascular is scientifically evaluated by internal personnel and by outside technical experts when appropriate. The detailed findings are then analyzed in conjunction with the patient-specific clinical information in order to assess the potential clinical significance, if any, of the device findings. Patient anatomy and the procedural technique used by the physician are also assessed. Findings are presented to the implanting physician and appropriate regulatory bodies, including the FDA.
44
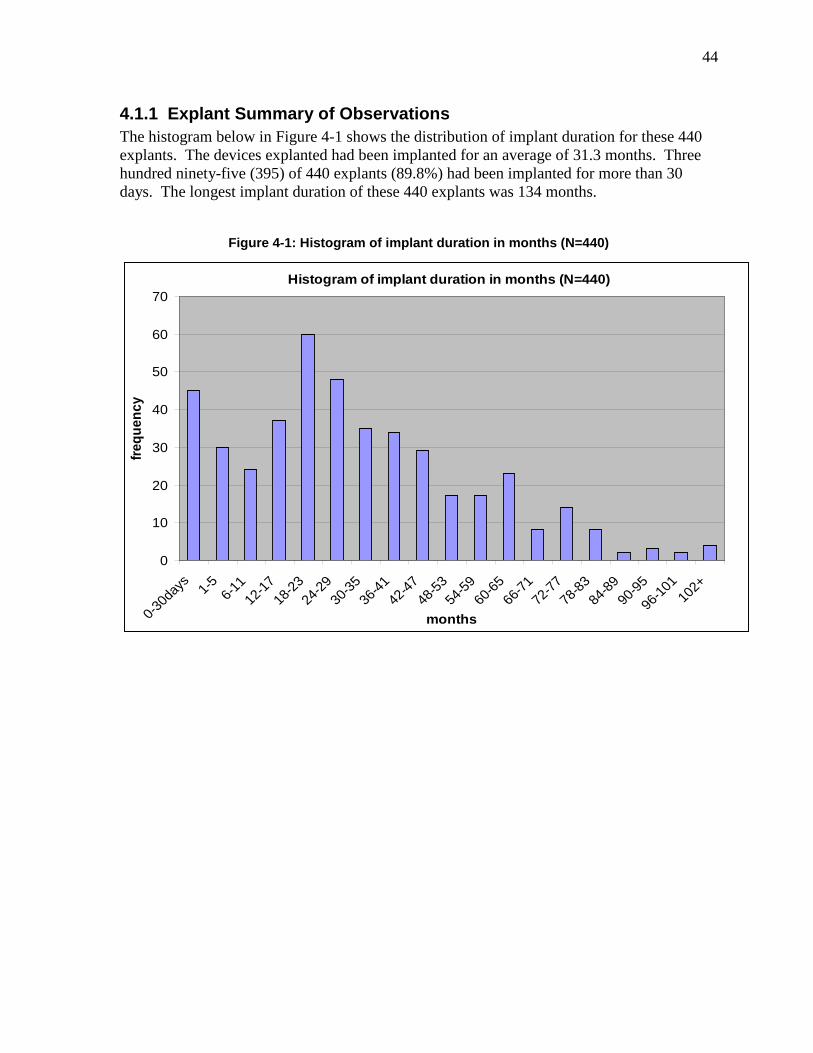
4.1.1 Explant Summary of Observations The histogram below in Figure 4-1 shows the distribution of implant duration for these 440 explants. The devices explanted had been implanted for an average of 31.3 months. Three hundred ninety-five (395) of 440 explants (89.8%) had been implanted for more than 30 days. The longest implant duration of these 440 explants was 134 months.
Figure 4-1: Histogram of implant duration in months (N=440)
Histogram of implant duration in months (N=440)
0
10
20
30
40
50
60
70
0-30d
ays
1-5 6-11
12-17
18-23
24-29
30-35
36-41
42-47
48-53
54-59
60-65
66-71
72-77
78-83
84-89
90-95
96-10
110
2+
months
frequ
ency

45
Table 4-2 below shows the reasons for explant as determined by the treating or explanting physician. Acute (≤ 30 day) and longer-term explants (> 30 day) are presented separately.
Table 4-2: Reasons for Explant – Primary Cause as Determined by Physician
Reason for Explant Number of Occurrences –
implant duration less than or
equal to 30 days
Number of Occurrences –
implant duration greater than 30
days
Number of Occurrences - Total
Aortoenteric Fistula 0 6 6 Disease Progression1 0 11 11 Endoleaks, Type I 3 39 42 Endoleaks, Type II 0 7 7 Endoleaks, Type III Junctional, including component separation
0 11 11
Implantation Difficulties 16 1 17 Incidental Autopsy 8 41 49 Infection 0 11 11 Increase in AAA Size 0 167 167 Limb Occlusion 4 10 14 Migration 0 20 20 Rupture • Post-implant • At time of implant
5 9
67 N/A
72 9
Symptomatic AAA 0 4 4 1 As defined by localized dilatation of the aortic neck
Explant Device Observations The Medtronic explant program serves as an important feedback element in our ongoing device research and development programs. In other words, the explant observations and data listed below were utilized to guide our decisions regarding device and implantation technique improvements.
As part of an individual analysis of each explanted device, the integrity of the components of the stent graft is examined. This examination includes the stents, graft material, and sutures. Of the 440 explanted cases, there were 374 cases examined in which the bifurcated stent graft was the primary component. These 374 examined cases (1261components) are mainly (329 cases; 1109 components) comprised of bifurcated devices with the Reduced Porosity Graft Material (RPM), which is no longer commercially available. A smaller number of devices (45 cases representing 152 components) which are comprised of bifurcated devices with the currently-available High Density Graft Material (HDM; Resilient Graft Material) have been explanted and analyzed. This is also explained in the Table 4-3 below:

46
Table 4-3: Explant Device Observations Summary
Bifurcated Stent Graft Material
Number of examined explanted cases
Number of components
Reduced Porosity Graft Material (RPM)
329 1109
High Density Graft Material (HDM; Resilient Graft Material)
45 152
Total 374 1261
Stent Observations Nitinol stent strut fractures have been observed in devices that have been surgically explanted as well as removed at autopsy. Fractures can be categorized as due to single event overload or fatigue. It is likely that the majority of single event overload fractures occur during the explant procedure itself.
Fatigue strut fractures appear to be clustered in the mid-aortic stent rings, generally outside the seal zones. Most fatigue strut fractures in the bifurcated components were found in aortic ring 3 (59.6%) and ring 4 (12.2%) in the area of transition between the circular and bi-oval cross section stent ring configuration, and at ring 1 (10.9%). The majority of fatigue fractures observed during explant analysis do not appear to be related to adverse clinical outcomes; however, it appears that severe aortic neck angulation may exacerbate the development of ring 3 fatigue strut fractures.
Modifications to the bifurcated stent graft (approved by FDA March 17, 2006) included changes to aortic rings 3 and 4, in order to improve the device’s fatigue resistance. The currently available version of the endograft, the AneuRx AAAdvantage Stent Graft system, incorporates these improvements.
Fourteen (14) of the 374 examined cases were configured with the AneuRx AAAdvantage Stent Graft system.
• A total of 44 stent strut fatigue fractures were observed on 8 bifurcates from these 14
cases. Twenty eight (28) of these fractures occurred on bifurcates from 2 cases in which the stent graft had migrated into the sac due to aortic neck dilatation from disease progression. These fractures were located outside the proximal seal zone in aortic ring 3 (N=2), ring 4 (N=17), ring 5 (N=5) and ring 6 (N=4), and the configuration of the explanted stent graft would suggest that the majority of these fractures had occurred after the stent graft had migrated.
• The remaining 6 AneuRx AAAdvantage cases with bifurcate fractures had a total of 16 fractures which were located in ring 1 (N=4), ring 4 (N=6), ring 5 (N=5) and ring 8 (N=1).

47
Graft Material and Suture Observations Abrasion induced holes occur predominately (73%) in the ipsilateral and contralateral iliac legs. Abrasion has also been observed, to a lesser extent, directly below the proximal aortic seal zone (13%), and along the aortic seal zone (8%). The presence of abrasion is typically observed in areas of increased vessel tortuosity.
In 329 examined explant cases where the bifurcated RPM device was the primary component of the stent graft, 171 explant cases exhibited 831 abrasion holes greater than 0.2 mm2 (the current manufacturing specification for maximum hole size). Graft holes were irregular in shape. The abrasion holes in the RPM explants averaged 0.82 mm2 in size, with a median size of 0.56 mm2 (range 0.21 – 10.0 mm2). Three devices from 3 cases exhibited four holes which are not typical (7.4 mm2, 9.5 mm2, 9.4 mm2 and 10.0 mm2), and were likely caused by excessive angulations. Another device exhibited a longitudinal tear approximately 20 mm in length (40 mm2 area) and did not exhibit typical abrasion factors. After removing these 4 holes, the average and range for the 171 RPM explant cases which exhibited abrasion holes was 0.78 mm2 and 0.21 – 6.0 mm2.
In 19 of the 45 explant cases in which the bifurcated HDM (Resilient) device was the primary component of the stent graft, 25 components (which included 13 bifurcates) exhibited a total of 106 abrasion holes greater than 0.2 mm2. The holes in this group averaged 0.63 mm2, with a median size of 0.47 mm2 (range 0.21 – 3.0mm2).
Table 4-4: Graft Material and Suture Observations Summary
Bifurcated Stent Graft Material
Number of examined explanted cases
Event
Reduced Porosity Graft Material (RPM)
171 of 329 cases (158 cases without holes)
831 abrasion holes >0.20mm2
High Density Graft Material (HDM; Resilient Graft Material)
19 of 45 cases (26 cases without holes)
106 abrasion holes >0.20mm2
Total 190 of 374 cases 1021 abrasion holes >0.20mm2
Transgraft flow is a process influenced by many factors such as anticoagulation, tissue incorporation and healing, pressure gradients, and collateral flow. Holes discovered during the explant analyses were normally exhibited in stent grafts in which no endoleaks were reported either via imaging or at the explant procedure.
Type IIIb endoleaks (or microleaks) are defined as holes in the fabric of the graft material and have been reported in the early generation abdominal aortic aneurysm endografts during long term follow-up. Long term surveillance, as recommended in the AneuRx AAAdvantage Instructions for Use, is crucial in the identification and treatment of endoleaks.
Broken sutures have also been observed in explanted AneuRx Stent Grafts. Abrasion of the suture against the nitinol stent appears to be the primary mode of the breakage. The breakage is typically seen at the junction (stent tip to stent tip connection) stitches, as opposed to the ‘node’ stitch that secures the stent ring to the graft fabric. Suture breaks occur in areas of angulation and stent ring overlap.

48
It is important to remember that earlier findings prompted a change to the graft material, which was introduced into commercial use following approval by FDA on January 30, 2004. The modification approved under this supplement was to a higher density weave pattern (Resilient Graft Material), and this improved graft material is on the AneuRx AAAdvantage Stent Graft. Please see the AneuRx AAAdvantage IFU for the most current recommendations and indications. Medtronic Vascular will continue to assess the potential for clinical impact as additional explants are received.
49
5.0 Notes to Clinicians The AneuRx AAAdvantage Stent Graft System is indicated for the endovascular treatment of infrarenal abdominal aortic or aorto-iliac aneurysms having:
• adequate iliac/femoral access; • infrarenal, non-aneurysmal neck length of greater than 1 cm at the proximal and distal
ends of the aneurysm and an inner vessel diameter approximately 10-20% smaller than the labeled device diameter;
• morphology suitable for endovascular repair; and • one of the following:
• aneurysm diameter > 5 cm; or • aneurysm diameter of 4-5 cm which has also increased in size by 0.5 cm in the last
6 months; or • aneurysm, which is twice the diameter of the normal infrarenal aorta
Patient Follow-Up and Selection Recommendations: As outlined in the AneuRx AAAdvantage Stent Graft Instructions for Use, critical factors for successful clinical outcomes include:
• Appropriate patient selection, including a 15 mm aortic seal zone and 25mm iliac seal zones and aortic neck angulation of <45 degrees
• 10-20% oversizing • Effective device deployment in accordance with the Instructions For Use • Appropriate and timely patient follow-up Patient follow-up should be individualized to meet patient specific needs. However, imaging should be scheduled based on the physician’s clinical assessment of the patient pre- and post-discharge. For example, periodic imaging should be performed every 3 to 6 months for patients in the enhanced surveillance group, and at least every 6 to 12 months for patients in the routine surveillance group.
Patient Selection: This device is not recommended in patients that have systemic infection, or are suspected of having systemic infection or with sensitivities or allergies to the device materials. Proper use of this device requires accurate fluoroscopic imaging. This device is not recommended for patients whose weight exceeds 350 lbs (150 kg) or whose weight may impede accurate fluoroscopic imaging. For additional details, please refer to the AneuRx AAAdvantage Stent Graft Systems Instructions of Use.

50
Adverse Event Reporting Instructions Below are the reporting instructions for adverse events:
• Report adverse events to Medtronic Vascular at 1-800-465-5533. This information may also be reported to FDA’s MedWatch reporting system by phone (1-800-FDA-1088), facsimile (1-800-FDA-0178), or to the MedWatch website at www. Fda.gov/medwatch. Form 3500 should be used for reporting adverse events.
• Forward patient films, explant data, and explant to Medtronic Vascular. • For additional information, contact your local Medtronic Vascular representative, or call
1-800-678-2500.

51
6.0 Brief Summary of Indications for Use, Warnings and Precautions
A brief summary of the warnings, precautions and contraindications is provided below. For detailed information, please refer to the AneuRx Stent Graft Systems Instructions for Use.
Indications for Use: The AneuRx AAAdvantage Stent Graft System is indicated for the endovascular treatment of infrarenal abdominal aortic or aorto-iliac aneurysms having:
• adequate iliac/femoral access;
• infrarenal, non-aneurysmal neck length of greater than 1 cm at the proximal and distal ends of the aneurysm and an inner vessel diameter approximately 10-20% smaller than the labeled device diameter
• morphology suitable for endovascular repair;
• one of the following:
• aneurysm diameter > 5 cm; or
• aneurysm diameter of 4-5 cm which has also increased in size by 0.5 cm in the last 6 months; or
• aneurysm, which is twice the diameter of the normal infrarenal aorta.
Contraindications: There are no known contraindications currently associated with this device.
Warnings and Precautions: The AneuRx AAAdvantage Stent Graft is intended to prevent rupture of abdominal aortic aneurysms. However, this risk is not completely eliminated. Based on reports received for patients enrolled in all phases of the clinical study through five years of follow up ruptures have occurred in 2/1193 (0.167%) patients during the operative period; in 3/1193 (0.251%) patients within 30 days of treatment; and in 21/1193 patients greater than 30 days after treatment. The one-year freedom from rupture rate for patients enrolled in all phases of the clinical study is 99.5%; the two-year freedom from rupture rate is 98.7%; the three-year freedom from rupture rate is 98.4%; the 4-year freedom from rupture rate is 97.4%; and the 5-year freedom from rupture rate is 96.8%.
The long term safety and effectiveness of this implant has not been established. All patients with endovascular aneurysm repair must undergo periodic imaging to evaluate the stent graft, aneurysm size, and occlusion of vessels in the treatment area. Significant aneurysm enlargement (>5 mm), the appearance of a new endoleak, evidence of perigraft flow, change in aneurysm pulsatility, or migration resulting in an inadequate seal zone should prompt further investigation and may indicate the need for additional intervention or surgical conversion.

52
Exercise care in the handling and delivery technique to aid in the prevention of vessel rupture. The clinical study supporting approval of this device indicates that if an AneuRx Stent Graft is placed with less than one-centimeter length of non-aneurysmal tissue at the proximal or distal end attachment sites, there is potential for leaking or migration due to inadequate apposition of the stent graft. However, literature data available subsequent to approval indicate that patients with an aortic seal length of < 15 mm and an iliac seal length of < 25 mm may also have a higher likelihood of suboptimal outcomes.
• Inappropriate patient selection may contribute to poor device performance. Preliminary data indicate that patients with an aortic neck angle > 45 degrees may have a higher likelihood of suboptimal outcomes compared to patients with an aortic neck angle < 45 degrees. The same data indicate that patients with an aortic seal length of < 15 mm and an iliac seal length of < 25 mm may also have a higher likelihood of suboptimal outcomes.
• Do not attempt to use the AneuRx AAAdvantage Stent Graft System before completely reading and understanding the information contained in this booklet.
• The AneuRx AAAdvantage Stent Graft System should only be used by physicians and teams trained in vascular interventional techniques, including training in the use of the device. Specific training expectations are described in Section 10.1 PHYSICIAN TRAINING PROGRAM, of the AneuRx instructions for use.
• Do not use the AneuRx AAAdvantage Stent Graft in patients unable to undergo the necessary preoperative and postoperative imaging and implantation studies as described in Section 10.6 PREPARATION OF THE ANEURX AAADVANTAGE STENT GRAFT SYSTEM, of the AneuRx instructions for use.
• The results of the clinical studies indicated that patients who experience an unsuccessful endovascular repair attempt, and as a result undergo conversion to surgical Abdominal Aortic Aneurysm (AAA) repair, are likely to have increased complications arising from both procedures (i.e., cardiac complications, fever, infection, musculoskeletal complications, neurological complications, pulmonary complications, vascular disease, vessel dissection, wound healing issues, and mortality; reference Section 5 ADVERSE EVENTS for specific information on adverse event categories), of the AneuRx instructions for use.
• The safety and effectiveness of the AneuRx AAAdvantage Stent Graft System for the treatment of abdominal aortic aneurysms has not been evaluated in patients:
• with aneurysms pending rupture • with connective tissue disorder • with hypercoagulability • with mesenteric artery occlusive disease • with ilio-femoral, thoracic, or inflammatory aneurysms • with juxtarenal AAA • with pararenal AAA • with suprarenal or thorocoabdominal aneurysms • who are morbidly obese
53
• pregnant or nursing • less than 18 years old • with less than one-year life expectancy
• Always have a vascular surgery team available at institutions performing endovascular grafting in the event that conversion to open surgical repair is required.
MRI Safety and Compatibility: Non-clinical testing has demonstrated that the AneuRx AAAdvantage Stent Graft is MR conditional. It can be scanned safely under the following conditions: • Static magnetic field of 3-Tesla or less. • Spatial gradient field of 720 Gauss/cm or less. • Maximum whole-body-averaged specific absorption rate (SAR) of 3 W/kg for 15 minutes
of scanning. For additional information regarding MRI please refer to the product’s Instructions for Use.
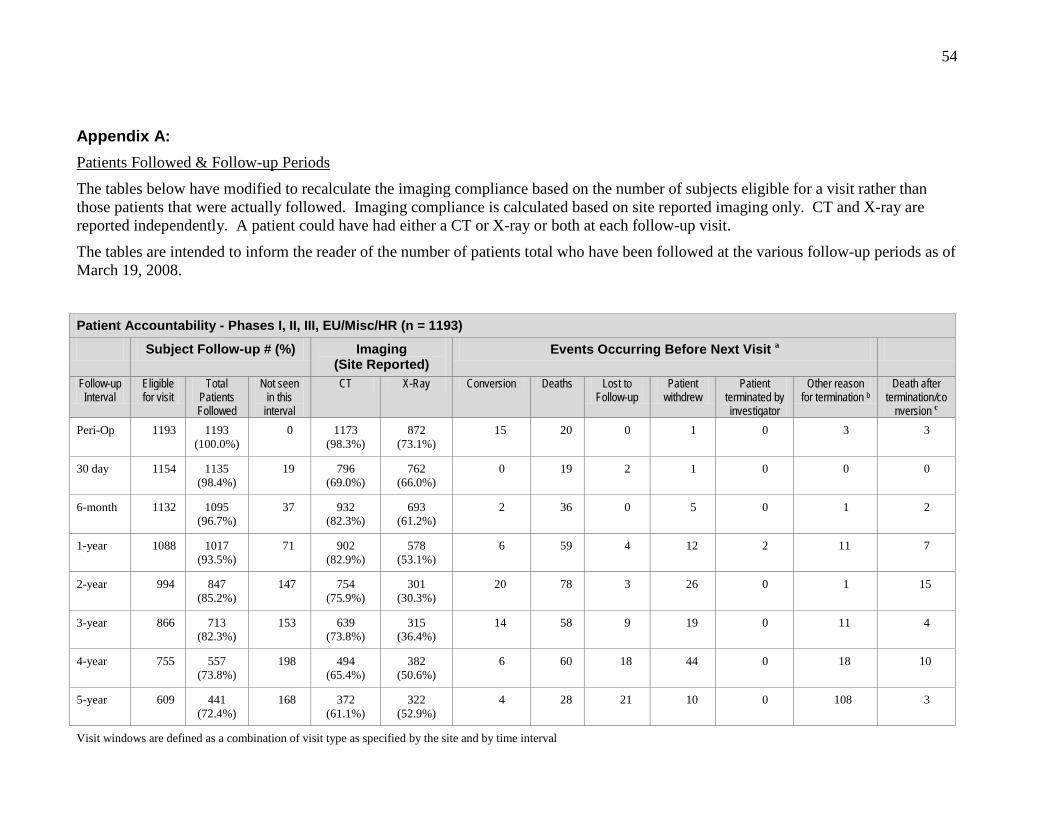
54
Appendix A: Patients Followed & Follow-up Periods
The tables below have modified to recalculate the imaging compliance based on the number of subjects eligible for a visit rather than those patients that were actually followed. Imaging compliance is calculated based on site reported imaging only. CT and X-ray are reported independently. A patient could have had either a CT or X-ray or both at each follow-up visit.
The tables are intended to inform the reader of the number of patients total who have been followed at the various follow-up periods as of March 19, 2008.
Patient Accountability - Phases I, II, III, EU/Misc/HR (n = 1193)
Subject Follow-up # (%) Imaging (Site Reported)
Events Occurring Before Next Visit a
Follow-up Interval
Eligible for visit
Total Patients Followed
Not seen in this
interval
CT X-Ray Conversion Deaths Lost to Follow-up
Patient withdrew
Patient terminated by investigator
Other reason for termination b
Death after termination/co
nversion c Peri-Op 1193 1193
(100.0%) 0 1173
(98.3%) 872
(73.1%) 15 20 0 1 0 3 3
30 day 1154 1135 (98.4%)
19 796 (69.0%)
762 (66.0%)
0 19 2 1 0 0 0
6-month 1132 1095 (96.7%)
37 932 (82.3%)
693 (61.2%)
2 36 0 5 0 1 2
1-year 1088 1017 (93.5%)
71 902 (82.9%)
578 (53.1%)
6 59 4 12 2 11 7
2-year 994 847 (85.2%)
147 754 (75.9%)
301 (30.3%)
20 78 3 26 0 1 15
3-year 866 713 (82.3%)
153 639 (73.8%)
315 (36.4%)
14 58 9 19 0 11 4
4-year 755 557 (73.8%)
198 494 (65.4%)
382 (50.6%)
6 60 18 44 0 18 10
5-year 609 441 (72.4%)
168 372 (61.1%)
322 (52.9%)
4 28 21 10 0 108 3
Visit windows are defined as a combination of visit type as specified by the site and by time interval

55
Patient Accountability - Phases I, II, III, EU/Misc/HR (n = 1193)
Subject Follow-up # (%) Imaging (Site Reported)
Events Occurring Before Next Visit a
Follow-up Interval
Eligible for visit
Total Patients Followed
Not seen in this
interval
CT X-Ray Conversion Deaths Lost to Follow-up
Patient withdrew
Patient terminated by investigator
Other reason for termination b
Death after termination/co
nversion c Time intervals are defined as: 30 day: 30 days - 3 months 6-month: 3 - 9 months 1-year: 9 - 18 months 2-year: 18 - 30 months 3-year: 30 - 42 months 4-year: 42 - 54 months 5-year: 54 - 66 months aPatients are only counted once in the following categories: Conversion, Death, and Termination even though a patient may have more than one of these events - ONLY the first event will be counted - Deaths that occurred after conversion or termination are included in the last column bOther reason for termination includes: Patient completed follow-up, Patient was surgically converted, Site terminated study, Device Explanted, Device not implanted, Patient enrolled in another study, and Physician discretion-medically necessary cImportant: This column should not be included in the calculation for the number of patients Eligible for visit in the next row

56
The following table is intended to inform the reader of the accountability for Phase II of the AneuRx IDE. The number of patients in the Phase II IDE cohort is as of March 18, 2008. The imaging compliance is calculated based on core lab reported imaging only.
Phase II IDE Patient Accountability Table (n = 424)
Subject Follow-up # (%) Imaging (Core Lab) Events Occurring Before Next Visit a Follow-
up Interval
Eligible for visit
Total Patients Followed
Not seen in this
interval
CT X-Ray Conversion Deaths Lost to Follow-up
Patient withdrew
Patient terminated
by investigator
Other reason for termination b
Death after termination/conversion c
Peri-Op 424 424 (100.0%)
0 417 (98.3%) 299 (70.5%) 6 7 0 0 0 2 0
30 day 409 405 (99.0%)
4 139 (34.0%) 261 (63.8%) 0 5 2 0 0 0 0
6-month
402 395 (98.3%)
7 353 (87.8%) 249 (61.9%) 1 6 0 1 0 0 1
1-year 394 377 (95.7%)
17 328 (83.2%) 266 (67.5%) 3 23 1 4 1 4 3
2-year 358 315 (88.0%)
43 273 (76.3%) 198 (55.3%) 10 20 1 8 0 1 7
3-year 318 274 (86.2%)
44 219 (68.9%) 171 (53.8%) 9 23 1 4 0 0 2
4-year 281 209 (74.4%)
72 148 (52.7%) 135 (48.0%) 3 18 4 12 0 5 4
5-year 239 173 (72.4%)
66 86 (36.0%) 98 (41.0%) 1 7 8 6 0 30 2
** Note to MDT - Visit windows are defined as a combination of visit type as specified by the site and by time interval Time intervals are defined as: 30 day: 30 days - 3 months 6-month: 3 - 9 months 1-year: 9 - 18 months 2-year: 18 - 30 months 3-year: 30 - 42 months 4-year: 42 - 54 months

57
5-year: 54 - 66 months aPatients are only counted once in the following categories: Conversion, Death, and Termination even though a patient may have more than one of these events - ONLY the first event will be counted - Deaths that occurred after conversion or termination are included in the last column. bOther reason for termination includes: Patient completed follow-up, Patient was surgically converted, Site terminated study, Device Explanted, Device not implanted, Patient enrolled in another study, and Physician discretion-medically necessary. cImportant: This column should not be included in the calculation for the number of patients Eligible for visit in the next row

58
Appendix B: Bibliography
1. Cao P, Verzini F, Zanetti S, De Rango P, Parlani G, Lupatelli L, Maselli A. Device migration after endoluminal abdominal aortic aneurysm repair: analysis of 113 cases with a minimum follow-up period of 2 years. J Vasc Surg 2002;35(2):229-35.
2. Azizzadeh A, Sanchez LA, Rubin BG, Parodi JC, et al. Aortic neck attachment failure and the AneuRx graft: incidence, treatment options, and early results. Ann Vasc Surg 2005;19:1-6.
3. Heikkinen MA, Alsac JM, Arko FR, et al. The importance of iliac fixation in prevention of stent graft migration. J Vasc Surg 2006;43:1130-7.
4. Fulton JJ, Farber MA, Sanchez LA, Godshall CJ, Marston WA, Mendes R, Rubin BG, Sicard GA, Keagy BA. Effect of challenging neck anatomy on mid-term migration rates in AneuRx endografts. J Vasc Surg 2006;44:932-7.
5. Chaikof EL, Blankensteijn JD, Harris PL, et al. Reporting standards for endovascular aortic aneurysm repair. J Vasc Surg 2002;35:1048-60.
6. Ebaugh JL, Eskandari MK, Finkelstein A, Matsumura JS, et. al. Caudal migration of endoprosthesis after treatment of abdominal aortic aneurysms. J Surg Res 2002;107(1):14-7.
7. Nolthenius RP, Herwaarden JA, van den Berg JC, et al. Three year single center experience with the AneuRx stent graft. Eur J Vasc Endovasc Surg 2001;22(3)257-64.
8. Tonnessen GH, Conners MS, Sternbergh WC, et al. Mid-term results of patients undergoing endovascular aortic aneurysm repair. Am J Surg 2002;184(6):561-6; discussion 567.
9. Greenberg RK, Turc A, Haulon S, et al. Stent-graft migration: a reappraisal of analysis methods and proposed revised definition. J Endovasc Ther 2004;11(4):353-63.
10. Biebl M, Hakaim AG, Oldenburg WA, et al. Midterm results of a single center experience with commercially available devices for endovascular aneurysm repair. Mt. Sinai J Med 2005;72(2):127-35.
11. Sampaio SM, Panneton JM, Mozez G, et al. AneuRx device migration: incidence, risk factors and consequences. Ann Vasc Surg 2005;19(2):178-85.
12. Sternberg WC, Carter G, York JW, et al. Aortic neck angulation predicts adverse outcome with endovascular abdominal aortic aneurysm repair. J Vasc Surg 2002;35:482-6.
13. Abbruzzese TA, Kwolek CJ, Brewster DC, Chung TK, Kang J, Conrad MF, LaMuraglia GM, Cambria RP. Outcomes following endovascular abdominal aortic aneurysm repair (EVAR): an anatomic and ecvice-specific analysis. J Vasc Surg. 2008 July; 48(1): 19-28.

59
14. Van Herwaarden JA, van de Pavoordt ED, Waasdorp DJ, Alber Vos J, Overtoom TT, Kelder JC, Moll FL, de Vries JP. Long-term single-center results with AneuRx endografts for endovascular repair abdominal aortic aneurysm repair. J Endovasc Ther. 2007 Jun; 14(3): 307-17.

Medtronic3576 Unocal PlaceSanta Rosa, CA 95403USATel: 707.525.0111
Product Services Tel: 888.283.7868 Fax: 800.838.3103
CardioVascular LifeLine Customer Support Tel: 877.526.7890 Tel: 763.526.7890
www.medtronic.com
© 2011 Medtronic, inc. All rights reserved. Printed in USA UC201201000 ENFor distribution in the USA only.