Embed Size (px)
Citation preview
2018-19 Kindergarten Enrollment
Kindergarten is an exciting and important step in your child’s success in school. The Bellevue School District is committed to providing a variety of experiences and
opportunities so that your child’s educational experience is productive as well as enjoyable. Our goal is for each child to become a life-long learner.
To register for Kindergarten
Your child must be 5 years old
on or before August 31, 2018
You will need to submit:Completed enrollment packet
Residency verification
Certified copy of birth certificateor Current passport
Child’s immunization RecordsSchool Nurse Health Information
Home Language Survey
Bellevue School District Early Learning and After School Programs
Kindergarten - 5th Grade Fun and Learning Come Together Convenience at your school
Social opportunities with friends
Academic support
Recreational activities
Project based learning and classes
Programs available during school breaks and summer from 6:30 am—6:00 pm
Preschool Counts Every year of school counts—children who attend preschool do better in math and reading, are more likely to graduate, and work in jobs with higher earnings.
Development and Learning Come Together
Kindergarten readiness
Research based curricula which places emphasis on all aspects of learning
Opening the World of Learning (OWL)—literacy/reading readiness
RULER - social/emotional skills
Dreambox - math
Handwriting without Tears
Choice Programs ORCA - Introduction to Spanish Mandarin - Introduction to Mandarin Head Start/ECEAP - No cost income qualified PALS - Integrated and inclusive
All documents required for enrollment are on the Bellevue School Districtwebsite; http://www.bsd405.org/schools/registration/
Full-Day Kindergarten is available for all Bellevue School District students at no charge.
Knows letters and numbers are different
Names most letters of the alphabet
Makes many of the letter sounds
Enjoys reading books or being read to
Can hold a book carefully
Can draw most of the letters in their name
Understands letters can be made into words
Knows that words are a way that we can communicate with others
Plays well with other children
Says a child that they play with is their friend
Shares with others and is able to take turns
Can let an adult know if they need help
Tries to use words to solve a conflict
Gets from one place to another using different types of movement
Can hold a pencil
Goes to the bathroom without help
Washes hands after going to the bathroom
Can put on his or her own coat and shoes
Eats and drinks independently
Speaks clearly so other people can understand their words
Is able to have a conversation
Can tell a simple story in any language
Is curious about new things or ideas
Can come up with ideas to solve a problem
Sorts objects by one or more feature
Remembers and retells a family activity
Counts the number of items in a group
Uses words like “all” and “some” to describe an amount of items
Kindergarten Readiness
Children grow and develop in different ways and at different speeds. If you have concerns about your child’s development talk to your preschool
teacher, pediatrician or contact ChildFind at (425) 456 - 4171. For more information visit www.bsd405.org/kindergarten
How can I help my child prepare for Kindergarten?
Get to Know Your School
Take your child to the school they will be attending for orientation, welcome events or just to play on the playground.
Visit the building with your child (before the 1st day if possible) to find important places together so you will both know what to expect.
Take a walk to the bus stop before the 1st day so your child gets familiar with the routine.
Be Ready for the School Day
Help your child to have a good day by keeping a regular schedule. Ensure they are getting enough sleep and start their day with a nutritious breakfast.
Check your child’s backpack after school for notes and homework.
Check in with your child about homework but let them do the work themselves.
Set Expectations
Be a good role model by showing your child a positive attitude about school and learning.
Answer questions and talk about your child’s feelings about going to Kindergarten.
Talk to your child about making new friends and meeting people who are different from them.
Tell your child how you expect them to behave at school and the importance of respecting teachers and other students.
Help your child to think of solutions if they have a problem or talk about what they could do in a situation that comes up unexpectedly.
Practice Skills at Home
Read to your child every day.
Teach your child their full name, phone number, address and parents’ names.
Use everyday situations to practice taking turns and sharing.
Get plenty of exercise and spend time outdoors every day.
Teach and model good hygiene—washing hands after using the restroom, brushing teeth and covering your mouth when coughing or sneezing.
Help your child learn skills to calm themselves (like taking deep breaths or counting to 10) if they are upset. Help them learn to use words to solve problems with others.
3120P – Exhibit A
Bellevue School District 8/2/2017
Welcome to the Bellevue School District
ESTABLISHING AND VERIFYING RESIDENCY
State law requires that a student reside within the District boundaries and be able to prove residency or have been approved for an Interdistrict transfer in order to enroll in school. In order to establish or reestablish residency in the Bellevue School District you will need to complete the steps below.
STEP ONE: ESTABLISH RESIDENCY – If you live within the Bellevue School District, before your student may be enrolled, you must establish residency within the attendance boundaries of your neighborhood school. Residency is defined as the physical location where the student spends the majority of their time, at a minimum, where they consistently spend four nights a week. Parents/guardians must supply documentation as listed in one of the options below:
To verify residency, you must provide two of the items listed below; each bullet counts as one item.
All addresses on the documents must match the address of your residence
STEP TWO: RESIDENCY VERIFICATION – During the Enrollment Process, you will be required to carefully read, agree to, and sign a Residency Verification Form.
Misrepresentation of residency information or failure to follow through with the statements on theResidency Verification Form will result in your student's withdrawal from the District, and may resultin referral to the District Attorney’s office for further action.
STEP THREE: ENROLLMENT PROCESS -- Once you have established your student’s residency and have agreed to the terms on the Residency Verification form, you may enroll your student at the local school.
Redacted 1099 or W-2 (Social Security Number and dollar amounts blacked out)
Government Mail (e.g. car registration; Good to Go! bill or letter; letter from Social Security,immigration, unemployment, health finder exchange or DMV; USPS Change of Address form; electionballot. Correspondence from the Bellevue School District does not qualify as Government Correspondence)
Homeowner’s Insurance Policy Declaration
Property Tax bill (must have been received in the mail, not printed off a website)
Unexpired Lease Agreement (must be signed by both parties with 2 months cancelled checks or proof ofonline banking payment of lease)
Utility Bills (2 consecutive utility bills from the same utility company dated within the last 3 months –accepted utilities include water, sewer, gas, electricity, or garbage; the mailing and service address mustbe the residence address. Cable, internet and phone bills are not accepted.)
If you are part of the Washington State Address Confidentiality Program, an official letter from theAddress Confidentiality Program stating the attendance area school fulfills the requirement to establishresidency in the Bellevue School District. You must submit a renewed letter to the school each year.
If you are unable to provide any of the above items, please contact the District Student Placement office at [email protected] or at 425-456-4200 to create and sign a Residency Agreement. This Agreement will give you extra time to collect the needed documents.
3120P – Exhibit B
Page 1 of 2 Bellevue School District 7/17/2017
(Please complete one form for each student)
HOME OWNER RENTER CO-RESIDENT (Complete Co-Residency Form)
OTHER (Specify)
Washington law generally requires schools to be open to the admission of all persons between the ages of 5 and 21 residing in that school district. (RCW 28A.225.160). The Bellevue School District("District") is required to take appropriate steps to ensure that students attending our schoolssatisfy applicable laws. This Residency Verification Form must be completed, signed and submitted with appropriate documentation demonstrating compliance with Washington’s residency laws.
Student: Last Name First Name School Date of Birth Grade
(Effective Year)
Parent/Guardian: ________________________________________________________________________ Phone 1:
Parent/Guardian Email: Phone 2:
Address: Number Street City Zip Code
NOTE: The District presumes that the person who enrolls a student in school is the residential parent/guardian of the student. (Board Policy No. 3126). In circumstances of divorce in which legal and physical custody of the studentis shared between two parents, parents must provide a certified copy of the court order (parenting plan) identifying eachparent’s respective legal and physical custody rights. You also must inform the District of any changes to the court order within five (5) days.
Student:
Student:
Student:
Student:
Please list below the names of additional students at this address who attend the Bellevue School District:
(Last Name) (First Name) School Date of Birth Grade
(Last Name) (First Name) School Date of Birth Grade
(Last Name) (First Name) School Date of Birth Grade
(Last Name) (First Name) School Date of Birth Grade
Welcome to the Bellevue School District
RESIDENCY VERIFICATION FORM
Unit #
Cell Home Work
Cell Home Work
3120P – Exhibit B
______ My student (listed above) resides with me at least four (4) nights per week at the address listed above, (Initial) which is my primary residence.
NOTE: If your child does not reside with you at least four (4) nights per week at the above-listed address, please initial here_______, and attach a written explanation of where and with whom your child resides each day of the week.
_______I agree to notify the District/School within (5) days when I change my residence or that of my student to a (Initial) new address, either within or outside the District.
_______Home visitation and/or other residency verification is part of a periodic process to confirm current residency (Initial) status.
_______The District will investigate all cases where it has reason to believe that residency status has changed and/or (Initial) false information has been provided, which may include the use of private investigators to verify residency
status. Verification may include home visits.
_______Investigations that reveal students have enrolled on the basis of providing false information will be cause for (Initial) revocation of the student’s school assignment and disenrollment from the District.
I certify the foregoing information to be true and correct, and that any and all copies of documents submitted to verify my residency are true and correct copies of the original documents, and that any and all documents submitted have not been altered except for the redaction of dollar amounts and account numbers, which is permitted for the purposes of this Residency Verification Form. Furthermore, I recognize that falsification or omission of information could result in modification of the school or program placement for this student including withdrawal from school.
Signature of Parent/Guardian Date
I acknowledge and agree to the following: (initial each statement below):
Bellevue School District
RESIDENCY VERIFICATION FORM
Page 2 of 2 Bellevue School District 7/17/2017
DO NOT SIGN THIS FORM IF ANY OF THE STATEMENTS ARE INCORRECT. Evidence that false information was provided will be cause for immediate revocation of the student’s school assignment and withdrawal from the District, and may lead to criminal and/or financial penalties.
Legal last name: Legal first /middle initial name:
Gender: Male Female
Entering grade level:
Mo Day Year
Birthdate: __________________ ______________________ _______ __________________
* This form is available in the following languages: Chinese, Japanese, Korean, Russian, Spanish, and Vietnamese
Preferred last name: Preferred first name
Has your student gone by any other name?
yes no
If yes, what was the previous name?
_____________________________________
BSD ID#_________________
DATE RECEIVED______________
Home Address:_____________________________________________Unit#________City_______________________Zip__________
Mailing address: _____________________________Unit #______PO Box____________City______________________Zip__________ (If different from above)
School Experience Data: Has this student:
previously attended the Bellevue School District (BSD)? been enrolled in any special education program (served with
an Individual Education Plan, IEP )? had a 504 Plan? had an IHP to address known medical issues? been enrolled in ELL programs? ever been suspended or expelled for disciplinary reason(s)? had a history of violent or criminal behavior? had any history of weapons possession?
yes
yes yes yes yes yes yes yes
no
no no no no no no no
If yes, school_______________Year________
If yes, school_______________ Year_______
If yes, school ______________ Year _______
Dates Grade From School City State Zip To Levels
Last school attended:__________________________________ Dates: from__________ to ___________ Grade level(s)___________
Street___________________________________________ City________________________ State_____________ Zip_________ Other schools attended (list most recent first)
yes noother preschool playgroup childcare with family, friends, neighbors
Previously enrolled in an early learning program? If yes, check all that apply: BSD preschool
If yes, preschool attended:_______________________ # of years:_____
Is your student a foster child? yes noFor this purpose, a foster child is a child whose care and placement is the responsibility of the State or local Welfare agency ORwho is placed by a court with a caretaker household.
STUDENT INFORMATION
STUDENT ENROLLMENT FORM 1 of 5 Bellevue School District 8/15/17
Please Print Cleary
Month Day Year Birth City State Country
If your student was NOT born in the United States, date first entered:_______________________Has your student lived outside the United States during the last 12 months? yes no If yes, which country?:_______________________
STUDENT ENROLLMENT FORM
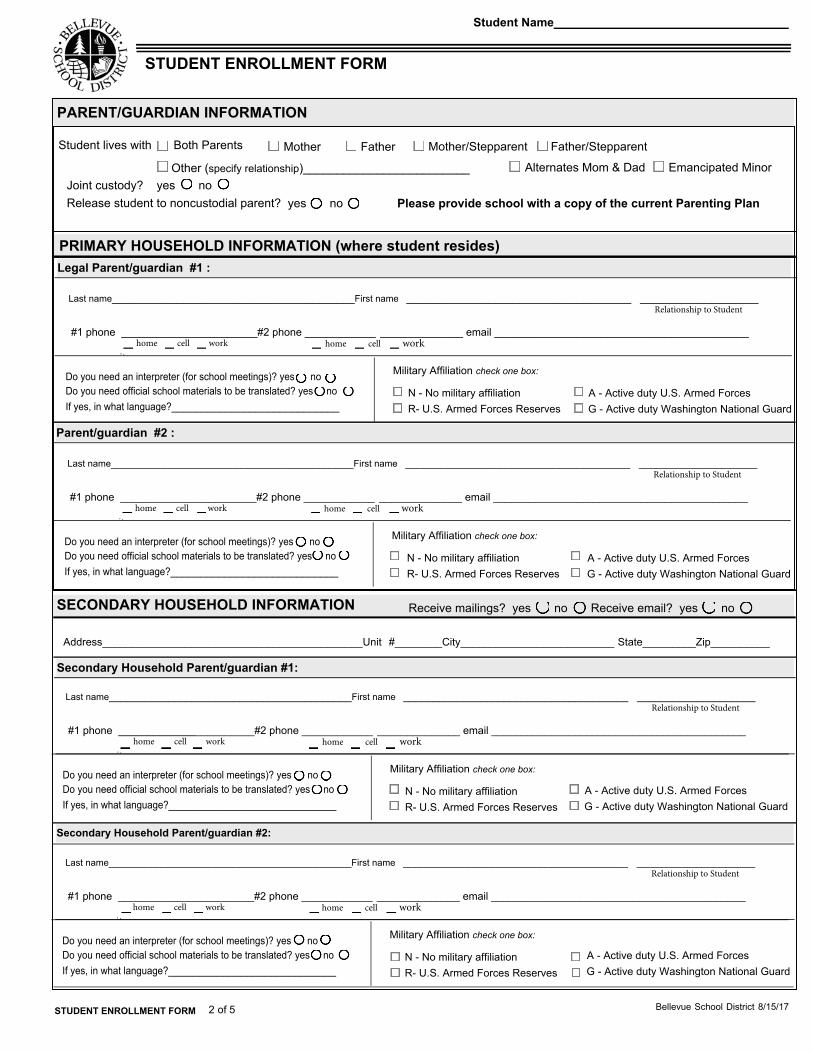
Student lives with Both Parents Mother Father Mother/Stepparent Father/Stepparent
Other (specify relationship)_________________________ Alternates Mom & Dad Emancipated Minor
Please provide school with a copy of the current Parenting PlanJoint custody? yes no Release student to noncustodial parent? yes no
Address____________________________________________Unit #________City__________________________ State_________Zip__________
N - No military affiliationR- U.S. Armed Forces Reserves
A - Active duty U.S. Armed ForcesG - Active duty Washington National Guard
Military Affiliation check one box:
Last name_________________________________________First name ______________________________________ ____________________
PRIMARY HOUSEHOLD INFORMATION (where student resides)
SECONDARY HOUSEHOLD INFORMATION Receive mailings? yes no Receive email? yes no
#1 phone _______________________#2 phone ____________ ______________ email ___________________________________________
Relationship to Student
Do you need an interpreter (for school meetings)? yes no Do you need official school materials to be translated? yes no If yes, in what language?____________________________
home cell work home cell work
Secondary Household Parent/guardian #2:
N - No military affiliationR- U.S. Armed Forces Reserves
A - Active duty U.S. Armed ForcesG - Active duty Washington National Guard
Military Affiliation check one box:
Last name_________________________________________First name ______________________________________ ____________________
#1 phone _______________________#2 phone ____________ ______________ email ___________________________________________
Relationship to Student
Do you need an interpreter (for school meetings)? yes no Do you need official school materials to be translated? yes no If yes, in what language?____________________________
home cell work home cell work
Secondary Household Parent/guardian #1:
N - No military affiliationR- U.S. Armed Forces Reserves
A - Active duty U.S. Armed ForcesG - Active duty Washington National Guard
Military Affiliation check one box:
Last name_________________________________________First name ______________________________________ ____________________
#1 phone _______________________#2 phone ____________ ______________ email ___________________________________________
Relationship to Student
Do you need an interpreter (for school meetings)? yes no Do you need official school materials to be translated? yes no If yes, in what language?____________________________
home cell work home cell work
Parent/guardian #2 :
N - No military affiliationR- U.S. Armed Forces Reserves
A - Active duty U.S. Armed ForcesG - Active duty Washington National Guard
Military Affiliation check one box:
Last name_________________________________________First name ______________________________________ ____________________
#1 phone _______________________#2 phone ____________ ______________ email ___________________________________________
Relationship to Student
Do you need an interpreter (for school meetings)? yes no Do you need official school materials to be translated? yes no If yes, in what language?____________________________
home cell work home cell work
Legal Parent/guardian #1 :
PARENT/GUARDIAN INFORMATION
STUDENT ENROLLMENT FORM
Student Name
STUDENT ENROLLMENT FORM 2 of 5 Bellevue School District 8/15/17
Student Name
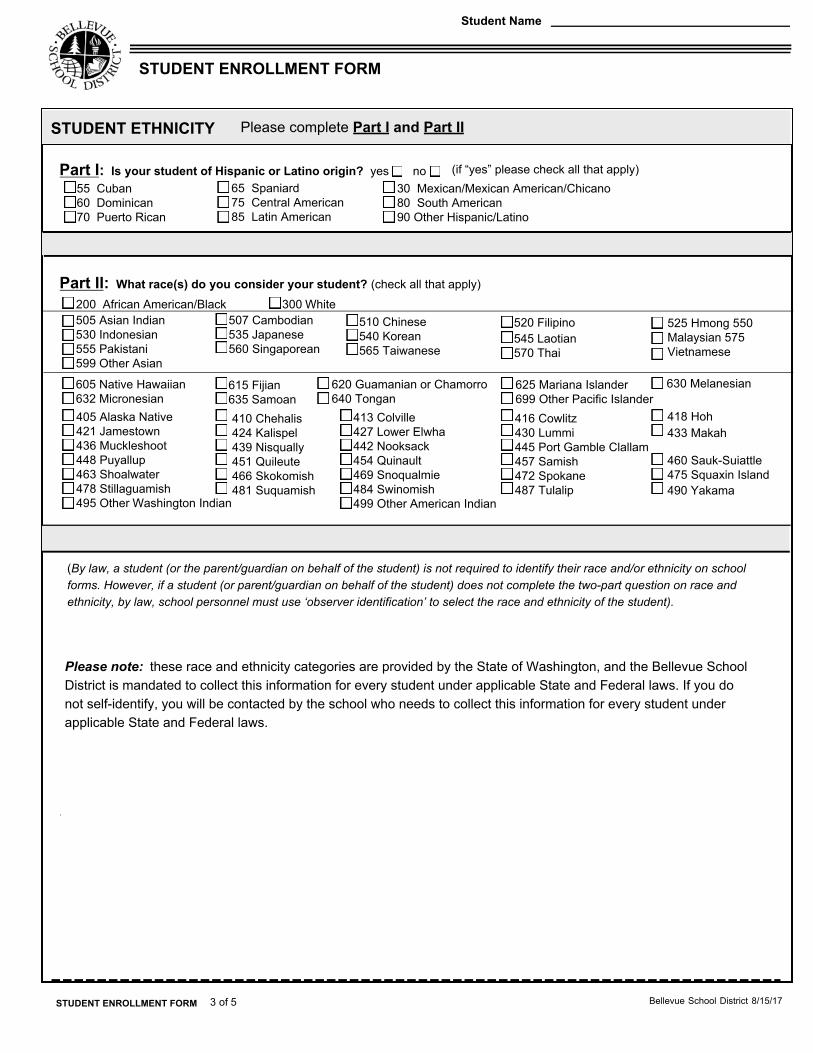
Part I: Is your student of Hispanic or Latino origin? yes no (if “yes” please check all that apply) 55 Cuban60 Dominican 70 Puerto Rican
65 Spaniard 75 Central American 85 Latin American
30 Mexican/Mexican American/Chicano 80 South American90 Other Hispanic/Latino
Part II: What race(s) do you consider your student? (check all that apply)
510 Chinese 540 Korean 565 Taiwanese
525 Hmong 550 Malaysian 575 Vietnamese
505 Asian Indian 530 Indonesian 555 Pakistani 599 Other Asian
615 Fijian 635 Samoan
605 Native Hawaiian 632 Micronesian
620 Guamanian or Chamorro 640 Tongan
625 Mariana Islander 699 Other Pacific Islander
520 Filipino545 Laotian 570 Thai
507 Cambodian 535 Japanese 560 Singaporean
200 African American/Black 300 White
630 Melanesian
418 Hoh 433 Makah
410 Chehalis 424 Kalispel 439 Nisqually 451 Quileute 466 Skokomish 481 Suquamish
416 Cowlitz 430 Lummi 445 Port Gamble Clallam 457 Samish 472 Spokane 487 Tulalip
460 Sauk-Suiattle 475 Squaxin Island 490 Yakama
405 Alaska Native 421 Jamestown 436 Muckleshoot 448 Puyallup 463 Shoalwater 478 Stillaguamish 495 Other Washington Indian
413 Colville 427 Lower Elwha 442 Nooksack 454 Quinault 469 Snoqualmie 484 Swinomish 499 Other American Indian
STUDENT ETHNICITY Please complete Part I and Part II
3 of 5 Bellevue School District 8/15/17 STUDENT ENROLLMENT FORM
STUDENT ENROLLMENT FORM
Please note: these race and ethnicity categories are provided by the State of Washington, and the Bellevue School District is mandated to collect this information for every student under applicable State and Federal laws. If you do not self-identify, you will be contacted by the school who needs to collect this information for every student under applicable State and Federal laws.
(By law, a student (or the parent/guardian on behalf of the student) is not required to identify their race and/or ethnicity on school forms. However, if a student (or parent/guardian on behalf of the student) does not complete the two-part question on race and ethnicity, by law, school personnel must use ‘observer identification’ to select the race and ethnicity of the student).
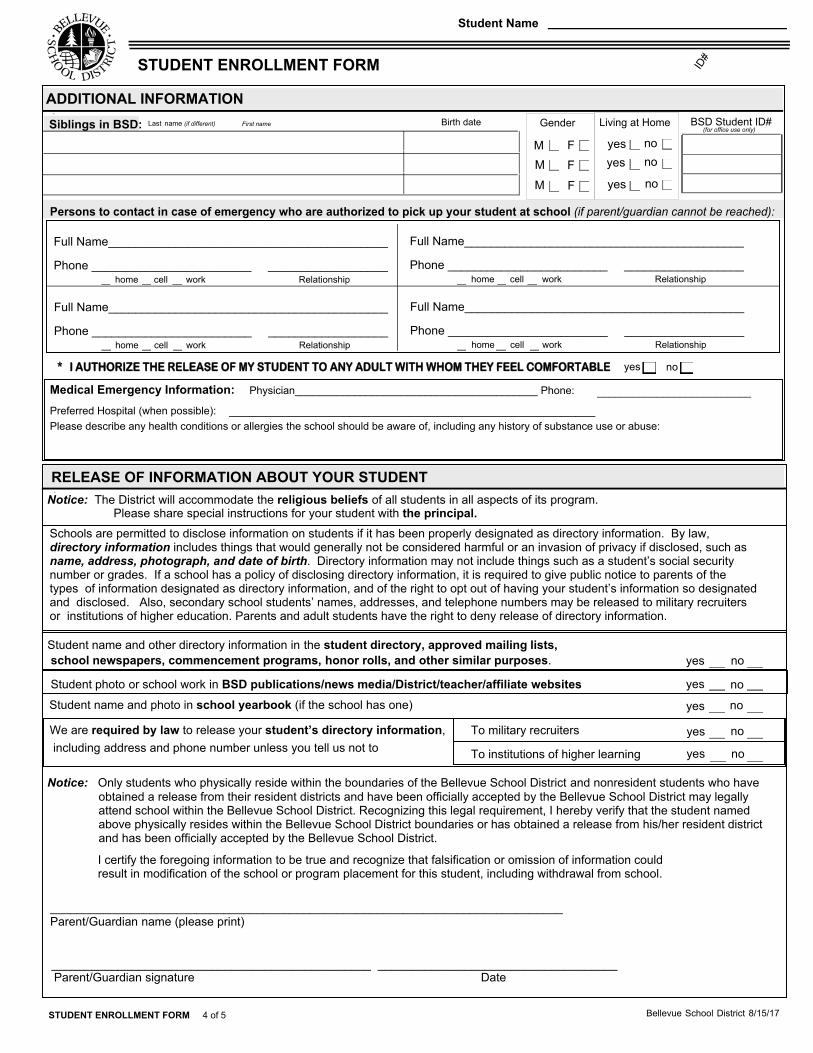
Schools are permitted to disclose information on students if it has been properly designated as directory information. By law, directory information includes things that would generally not be considered harmful or an invasion of privacy if disclosed, such as name, address, photograph, and date of birth. Directory information may not include things such as a student’s social security number or grades. If a school has a policy of disclosing directory information, it is required to give public notice to parents of the types of information designated as directory information, and of the right to opt out of having your student’s information so designated and disclosed. Also, secondary school students’ names, addresses, and telephone numbers may be released to military recruiters or institutions of higher education. Parents and adult students have the right to deny release of directory information.
Notice: Only students who physically reside within the boundaries of the Bellevue School District and nonresident students who haveobtained a release from their resident districts and have been officially accepted by the Bellevue School District may legally attend school within the Bellevue School District. Recognizing this legal requirement, I hereby verify that the student named above physically resides within the Bellevue School District boundaries or has obtained a release from his/her resident district and has been officially accepted by the Bellevue School District.
I certify the foregoing information to be true and recognize that falsification or omission of information could result in modification of the school or program placement for this student, including withdrawal from school.
_____________________________________________________________________________ Parent/Guardian name (please print)
________________________________________________ ____________________________________
including address and phone number unless you tell us not to To military recruiters
To institutions of higher learning
yes no
yes no
yes no
Student photo or school work in BSD publications/news media/District/teacher/affiliate websites
yes no Student name and other directory information in the student directory, approved mailing lists, school newspapers, commencement programs, honor rolls, and other similar purposes.
yes no
Notice: The District will accommodate the religious beliefs of all students in all aspects of its program. Please share special instructions for your student with the principal.
Student name and photo in school yearbook (if the school has one)
We are required by law to release your student’s directory information,
RELEASE OF INFORMATION ABOUT YOUR STUDENT
Last name (if different) First name Birth date BSD Student ID#(for office use only)
Gender Living at Home
ID#
F yes no
F yes no
F yes no
MMM
Full Name__________________________________________
Phone ________________________ __________________ home cell work Relationship
__________________________ Medical Emergency Information: Physician_________________________________________ Phone:
Preferred Hospital (when possible): _______________________________________________________ Please describe any health conditions or allergies the school should be aware of, including any history of substance use or abuse:
Full Name__________________________________________
Phone ________________________ __________________ home cell work Relationship
Full Name__________________________________________
Phone ________________________ __________________ home cell work Relationship
Full Name__________________________________________
Phone ________________________ __________________ home cell work Relationship
* I AUTHORIZE THE RELEASE OF MY STUDENT TO ANY ADULT WITH WHOM THEY FEEL COMFORTABLE yes no
Siblings in BSD:
Persons to contact in case of emergency who are authorized to pick up your student at school (if parent/guardian cannot be reached):
ADDITIONAL INFORMATION
Parent/Guardian signature Date
Bellevue School District 8/15/17
Student Name
STUDENT ENROLLMENT FORM
STUDENT ENROLLMENT FORM 4 of 5
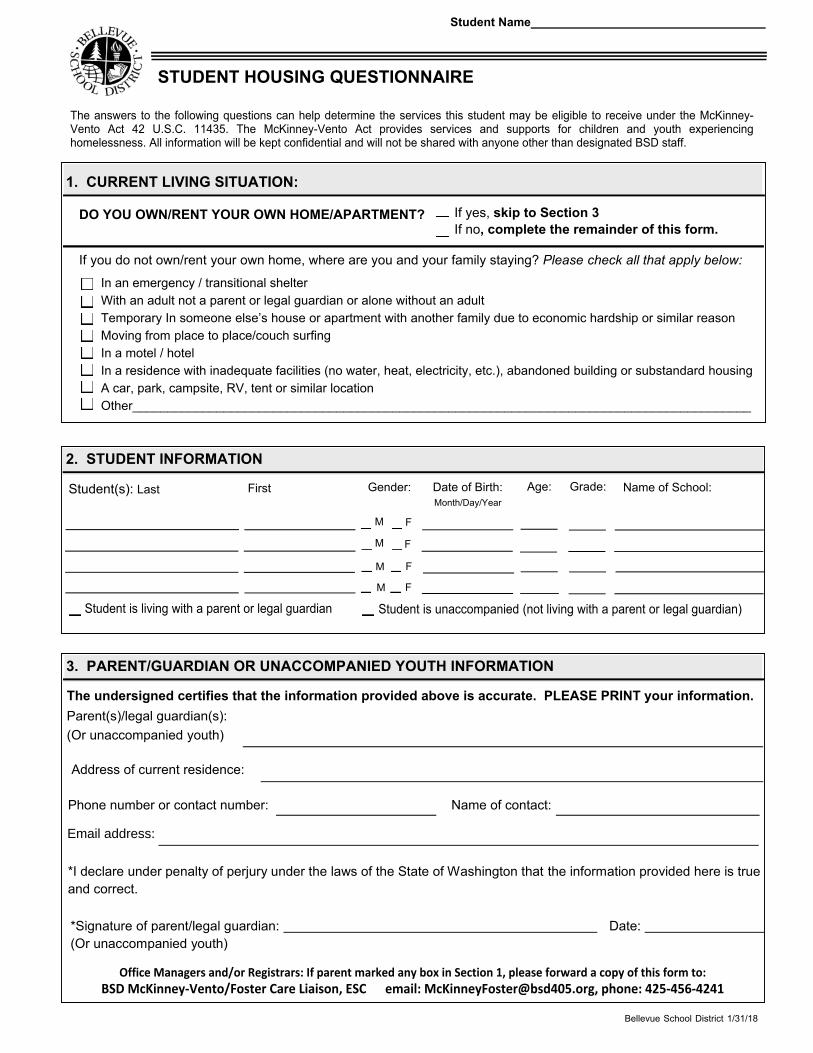
STUDENT HOUSING QUESTIONNAIRE
The answers to the following questions can help determine the services this student may be eligible to receive under the McKinney-Vento Act 42 U.S.C. 11435. The McKinney-Vento Act provides services and supports for children and youth experiencing homelessness. All information will be kept confidential and will not be shared with anyone other than designated BSD staff.
DO YOU OWN/RENT YOUR OWN HOME/APARTMENT? If yes, skip to Section 3If no, complete the remainder of this form.
If you do not own/rent your own home, where are you and your family staying? Please check all that apply below:
In an emergency / transitional shelter With an adult not a parent or legal guardian or alone without an adultTemporary In someone else’s house or apartment with another family due to economic hardship or similar reasonMoving from place to place/couch surfingIn a motel / hotelIn a residence with inadequate facilities (no water, heat, electricity, etc.), abandoned building or substandard housing A car, park, campsite, RV, tent or similar location Other________________________________________________________________________________________
Student(s): Last First Gender: Date of Birth: Age: Grade: Name of School:
Student is unaccompanied (not living with a parent or legal guardian)
Address of current residence:
Phone number or contact number: Name of contact:
The undersigned certifies that the information provided above is accurate. PLEASE PRINT your information. Parent(s)/legal guardian(s):(Or unaccompanied youth)
*Signature of parent/legal guardian: Date: (Or unaccompanied youth)
*I declare under penalty of perjury under the laws of the State of Washington that the information provided here is trueand correct.
Student Name
Office Managers and/or Registrars: If parent marked any box in Section 1, please forward a copy of this form to: BSD McKinney-Vento/Foster Care Liaison, ESC email: [email protected], phone: 425-456-4241
Month/Day/Year
Student is living with a parent or legal guardian
F
F
F
M
M
M
F M
2. STUDENT INFORMATION
3. PARENT/GUARDIAN OR UNACCOMPANIED YOUTH INFORMATION
Bellevue School District 1/31/18
1. CURRENT LIVING SITUATION:
Email address:
English/November 2016
Office of Superintendent of Public Instruction (OSPI)
Home Language Survey
The Home Language Survey is given to all students enrolling in Washington schools.
Student Name: Grade: Date:
Parent/Guardian Name Parent/Guardian Signature
Right to Translation and
Interpretation Services
Indicate your language preference so
we can provide an interpreter or
translated documents, free of
charge, when you need them.
All parents have the right to information about their child’s
education in a language they understand.
1. In what language(s) would your family prefer to communicate
with the school?
__________________________________
Eligibility for Language
Development Support
Information about the student’s
language helps us identify students
who qualify for support to develop
the language skills necessary for
success in school. Testing may be
necessary to determine if language
supports are needed.
2. What language did your child learn first?
__________________________________
3. What language does your child use the most at home?
__________________________________
4. What is the primary language used in the home, regardless of
the language spoken by your child?
__________________________________
5. Has your child received English language development support
in a previous school? Yes___ No___ Don’t Know___
Prior Education
Your responses about your child’s
birth country and previous
education:
Give us information about the
knowledge and skills your child is
bringing to school.
May enable the school district to
receive additional federal funding
to provide support to your child.
This form is not used to identify
students’ immigration status.
6. In what country was your child born? ___________________
7. Has your child ever received formal education outside of the
United States? (Kindergarten – 12th grade) ____Yes ____No
If yes: Number of months: ______________
Language of instruction: ______________
8. When did your child first attend a school in the United States?(Kindergarten – 12th grade)
_______________________
Month Day Year
Thank you for providing the information needed on the Home Language Survey. Contact your school
district if you have further questions about this form or about services available at your child’s school.
Note to district: This form is available in multiple languages on http://www.k12.wa.us/MigrantBilingual/HomeLanguage.aspx. A response that includes a language other than English to question #2 OR question #3 triggers English language proficiency placement testing. Responses to questions #1 or #4 of a language other than English could prompt further conversation with the family to ensure that #2 and #3 were clearly understood. ”Formal education” in #7 does not include refugee camps or other unaccredited educational programs for children.
Forms and Translated Material from the Bilingual Education Office of the Office of Superintendent of Public Instruction are licensed under a Creative
Commons Attribution 4.0 International License.
SCHOOL NURSE HEALTH INFORMATION
2018-2019
To make school a safe and healthy place for your child this private form will be seen by the School
Nurse, school staff who help your child, and emergency medical personnel.
Name: Birthdate: Last First MI
School: Date:
SERIOUS HEALTH CONDITIONS (check box below):
If your child has a SERIOUS health condition, TELL YOUR SCHOOL NURSE NOW. State Law (RCW 28A.210.320) says medication, medical orders, and a health care plan must be in place before the start of school. ☐ My child does not have any SERIOUS health conditions that will affect them at school.☐ My child has the following SERIOUS health condition(s) – Check boxes below:
☐ Allergy (life threatening – requires an epinephrine prescription such as Epi Pen or Auvi-Q). Allergic to: Date of last reaction:
☐ Asthma – Will your child require a rescue inhaler (such as Albuterol) at school? Yes or no? ☐ Heart condition and restrictions (if any):
☐ Diabetes (Date of diagnosis: )☐ Insulin Pump ☐ Insulin Pen ☐ Insulin via syringe
☐ Seizure Disorder (Date of diagnosis:Type: Rescue Medication:
) (Date of last seizure: ) Yes or no?
☐ Other, including overnight hospitalizations in past 12 months: -- Please describe condition:
OTHER HEALTH CONDITIONS (check appropriate box below): ☐ My child does not have any other health conditions that will affect them at school. ☐ History of a Concussion (diagnosed by a health care provider) - Date of concussion
☐ Hearing concerns? ☐ Does your child wear hearing aids? ☐ Does your child have a known hearing loss?
☐ Vision concerns? ☐ Glasses ☐ Contacts
☐ Food sensitivity: ☐ Other Allergies (e.g. medication, pollen): __________________
☐ Other: _______________________________________________________________________________
MEDICATIONS: Prescription, supplements, over-the-counter (pills, eye drops, ointments, etc.): Does your child need to take medication every day at school? Yes ☐ No ☐Does your child need to take medication at school sometimes? Yes ☐ No ☐If Yes, a signed medical order form must be at school, for all medications (RCW 28A.210.206 and BSD Policy 4320).
CONTACT INFORMATION: Please provide correct & current contact numbers.
PARENT/GUARDIAN PARENT/GUARDIAN
Parents/Guardians:
Primary contact phone:
Email:
Signature (Parent/Guardian):____________________________________________Date:_______________
1-31-2018
Grade:
If you have a disability and need this document in another format, please call 1‐800‐525‐0127 (TDD/TTY call 711). DOH 348-295 November 2017
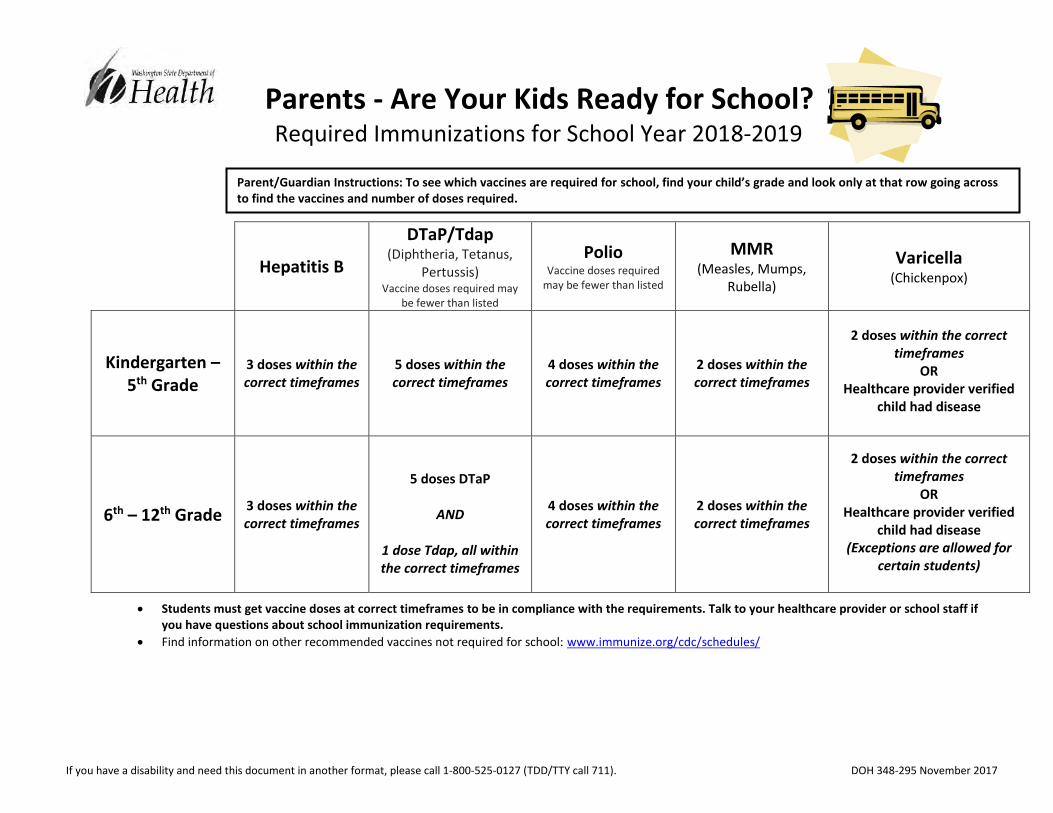
Parents - Are Your Kids Ready for School?
Required Immunizations for School Year 2018-2019
Hepatitis B
DTaP/Tdap (Diphtheria, Tetanus,
Pertussis) Vaccine doses required may
be fewer than listed
Polio Vaccine doses required
may be fewer than listed
MMR (Measles, Mumps,
Rubella)
Varicella (Chickenpox)
Kindergarten – 5th Grade
3 doses within the correct timeframes
5 doses within the correct timeframes
4 doses within the correct timeframes
2 doses within the correct timeframes
2 doses within the correct timeframes
OR Healthcare provider verified
child had disease
6th – 12th Grade 3 doses within the correct timeframes
5 doses DTaP
AND
1 dose Tdap, all within the correct timeframes
4 doses within the correct timeframes
2 doses within the correct timeframes
2 doses within the correct timeframes
OR Healthcare provider verified
child had disease (Exceptions are allowed for
certain students)
Students must get vaccine doses at correct timeframes to be in compliance with the requirements. Talk to your healthcare provider or school staff if you have questions about school immunization requirements.
Find information on other recommended vaccines not required for school: www.immunize.org/cdc/schedules/
Parent/Guardian Instructions: To see which vaccines are required for school, find your child’s grade and look only at that row going across to find the vaccines and number of doses required.
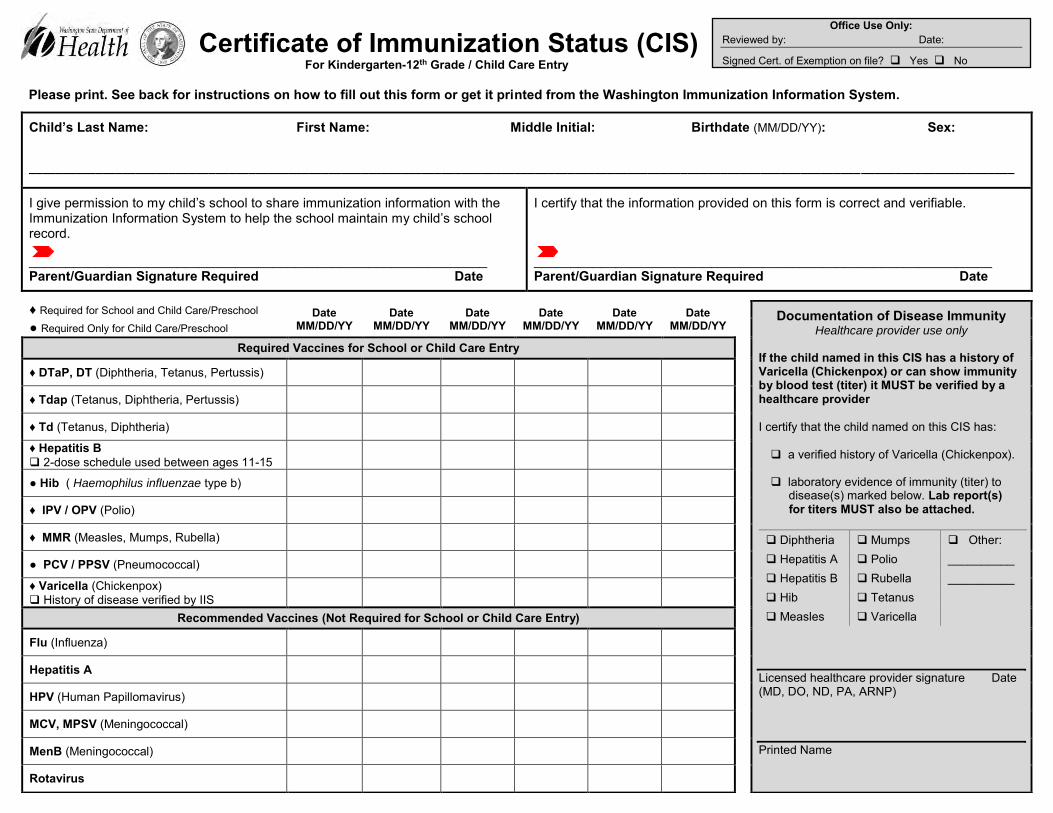
Certificate of Immunization Status (CIS) For Kindergarten-12th Grade / Child Care Entry
Please print. See back for instructions on how to fill out this form or get it printed from the Washington Immunization Information System.
Child’s Last Name: First Name: Middle Initial: Birthdate (MM/DD/YY): Sex:
____________________________________________________________________________________________________________________________________________________
I give permission to my child’s school to share immunization information with the Immunization Information System to help the school maintain my child’s school record.
______________________________________________________________ Parent/Guardian Signature Required Date
I certify that the information provided on this form is correct and verifiable.
______________________________________________________________ Parent/Guardian Signature Required Date
♦ Required for School and Child Care/Preschool Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Date MM/DD/YY
Documentation of Disease Immunity Healthcare provider use only
If the child named in this CIS has a history of Varicella (Chickenpox) or can show immunity by blood test (titer) it MUST be verified by a healthcare provider
I certify that the child named on this CIS has:
a verified history of Varicella (Chickenpox).
laboratory evidence of immunity (titer) to disease(s) marked below. Lab report(s)
for titers MUST also be attached.
Diphtheria Mumps Other: Hepatitis A Polio __________ Hepatitis B Rubella __________ Hib Tetanus Measles Varicella
Licensed healthcare provider signature Date (MD, DO, ND, PA, ARNP)
Printed Name
● Required Only for Child Care/Preschool
Required Vaccines for School or Child Care Entry
♦ DTaP, DT (Diphtheria, Tetanus, Pertussis)
♦ Tdap (Tetanus, Diphtheria, Pertussis)
♦ Td (Tetanus, Diphtheria)
♦ Hepatitis B 2-dose schedule used between ages 11-15
● Hib ( Haemophilus influenzae type b)
♦ IPV / OPV (Polio)
♦ MMR (Measles, Mumps, Rubella)
● PCV / PPSV (Pneumococcal)
♦ Varicella (Chickenpox) History of disease verified by IIS
Recommended Vaccines (Not Required for School or Child Care Entry)
Flu (Influenza)
Hepatitis A
HPV (Human Papillomavirus)
MCV, MPSV (Meningococcal)
MenB (Meningococcal)
Rotavirus
Office Use Only:
Reviewed by: Date:
Signed Cert. of Exemption on file? Yes No
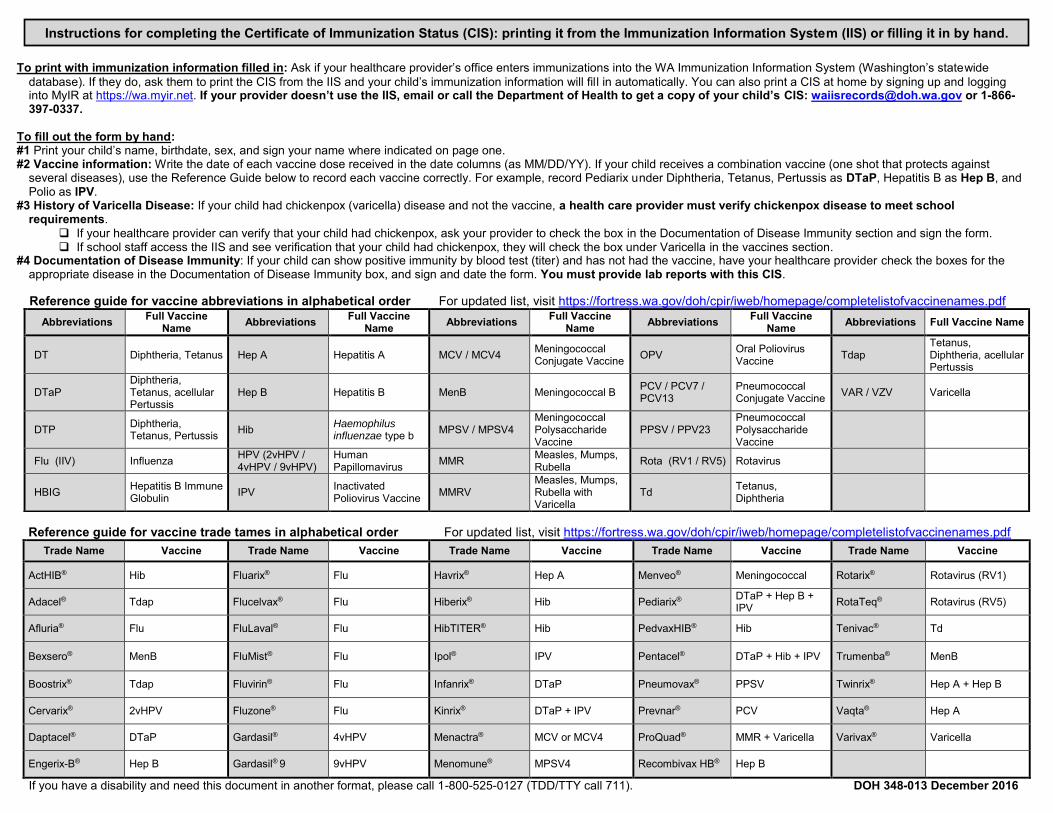
To print with immunization information filled in: Ask if your healthcare provider’s office enters immunizations into the WA Immunization Information System (Washington’s statewide database). If they do, ask them to print the CIS from the IIS and your child’s immunization information will fill in automatically. You can also print a CIS at home by signing up and logging into MyIR at https://wa.myir.net. If your provider doesn’t use the IIS, email or call the Department of Health to get a copy of your child’s CIS: [email protected] or 1-866-397-0337.
To fill out the form by hand: #1 Print your child’s name, birthdate, sex, and sign your name where indicated on page one. #2 Vaccine information: Write the date of each vaccine dose received in the date columns (as MM/DD/YY). If your child receives a combination vaccine (one shot that protects against
several diseases), use the Reference Guide below to record each vaccine correctly. For example, record Pediarix under Diphtheria, Tetanus, Pertussis as DTaP, Hepatitis B as Hep B, and Polio as IPV.
#3 History of Varicella Disease: If your child had chickenpox (varicella) disease and not the vaccine, a health care provider must verify chickenpox disease to meet school requirements.
If your healthcare provider can verify that your child had chickenpox, ask your provider to check the box in the Documentation of Disease Immunity section and sign the form. If school staff access the IIS and see verification that your child had chickenpox, they will check the box under Varicella in the vaccines section.
#4 Documentation of Disease Immunity: If your child can show positive immunity by blood test (titer) and has not had the vaccine, have your healthcare provider check the boxes for the appropriate disease in the Documentation of Disease Immunity box, and sign and date the form. You must provide lab reports with this CIS.
Reference guide for vaccine trade tames in alphabetical order For updated list, visit https://fortress.wa.gov/doh/cpir/iweb/homepage/completelistofvaccinenames.pdf Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine Trade Name Vaccine
ActHIB® Hib Fluarix® Flu Havrix® Hep A Menveo® Meningococcal Rotarix® Rotavirus (RV1)
Adacel® Tdap Flucelvax® Flu Hiberix® Hib Pediarix® DTaP + Hep B + IPV RotaTeq® Rotavirus (RV5)
Afluria® Flu FluLaval® Flu HibTITER® Hib PedvaxHIB® Hib Tenivac® Td
Bexsero® MenB FluMist® Flu Ipol® IPV Pentacel® DTaP + Hib + IPV Trumenba® MenB
Boostrix® Tdap Fluvirin® Flu Infanrix® DTaP Pneumovax® PPSV Twinrix® Hep A + Hep B
Cervarix® 2vHPV Fluzone® Flu Kinrix® DTaP + IPV Prevnar® PCV Vaqta® Hep A
Daptacel® DTaP Gardasil® 4vHPV Menactra® MCV or MCV4 ProQuad® MMR + Varicella Varivax® Varicella
Engerix-B® Hep B Gardasil® 9 9vHPV Menomune® MPSV4 Recombivax HB® Hep B
If you have a disability and need this document in another format, please call 1-800-525-0127 (TDD/TTY call 711). DOH 348-013 December 2016
Reference guide for vaccine abbreviations in alphabetical order For updated list, visit https://fortress.wa.gov/doh/cpir/iweb/homepage/completelistofvaccinenames.pdf Abbreviations Full Vaccine
Name Abbreviations Full Vaccine Name Abbreviations Full Vaccine
Name Abbreviations Full Vaccine Name Abbreviations Full Vaccine Name
DT Diphtheria, Tetanus Hep A Hepatitis A MCV / MCV4 Meningococcal Conjugate Vaccine OPV Oral Poliovirus
Vaccine Tdap Tetanus, Diphtheria, acellular Pertussis
DTaP Diphtheria, Tetanus, acellular Pertussis
Hep B Hepatitis B MenB Meningococcal B PCV / PCV7 / PCV13
Pneumococcal Conjugate Vaccine VAR / VZV Varicella
DTP Diphtheria, Tetanus, Pertussis Hib Haemophilus
influenzae type b MPSV / MPSV4 Meningococcal Polysaccharide Vaccine
PPSV / PPV23 Pneumococcal Polysaccharide Vaccine
Flu (IIV) Influenza HPV (2vHPV / 4vHPV / 9vHPV)
Human Papillomavirus MMR Measles, Mumps,
Rubella Rota (RV1 / RV5) Rotavirus
HBIG Hepatitis B Immune Globulin IPV Inactivated
Poliovirus Vaccine MMRV Measles, Mumps, Rubella with Varicella
Td Tetanus, Diphtheria
Instructions for completing the Certificate of Immunization Status (CIS): printing it from the Immunization Information System (IIS) or filling it in by hand.