Embed Size (px)
DESCRIPTION
2011 Annual Report
Citation preview

.
ParentProjectMD.org
Our MissiOnTo improve the treatment, quality of life, and long-term outlook for all individuals affected by Duchenne muscular dystrophy through research, education, advocacy, and compassion.
Parent Project Muscular Dystrophy401 Hackensack Ave., 9th FloorHackensack, New Jersey 07601
T. 800.714.5437
crea
ted
by
Big
Duc
k
TogeTher we are...
PROGRESS REPORT

LeaDINg The FIghT To eND DUCheNNe
Dear friends, families, and supporters,
My son has Duchenne muscular dystrophy.
When Sam was first diagnosed, like so many
Duchenne families, we went through a period of
mourning. But then it was time to focus and put
together a team that would help us fight this disease.
We convened doctors, therapists, nutritionists, and anyone else who
would play a role in his day-to-day care. We talked to teachers, coaches,
and community-members so that everyone knew what Sam would be
dealing with and what they could do to help.
Several years later, this team has become part of the Killian family.
In a way, our journey has been like PPMD’s journey. In 1994, when a
determined group of parents and grandparents began working to raise
awareness, increase research efforts, and expand care in Duchenne, the
key was collaboration and teamwork.
Today, as a result of collaborations with scientists, government agencies,
physicians, and families, PPMD is the largest nonprofit in the world
dedicated to fighting Duchenne—and we are closer than ever to a cure.
The PPMD team is led by Pat Furlong, Kimberly Galberaith, and Sharon
Hesterlee. They work tirelessly to move us all toward a cure, while at the
same time earning PPMD the highest ratings attainable from nonprofit
watchdogs like the Better Business Bureau and Charity Navigator.
This is not the life I imagined for Sam, for myself, or for my family.
But now that we are all on this journey, I cannot imagine our lives without
Parent Project Muscular Dystrophy.
Best,
John Killian Board Chair Parent Project Muscular Dystrophy
DE
AR
FRIEN
DS...
Dear PPMD Family,
It’s no secret that for the last few years, countless
families have struggled economically. And yet, because
of you—our dedicated, passionate community—even
during the worst financial period in recent American
history, our fight against Duchenne has not stopped. It
has not slowed. Because of you, we at Parent Project
Muscular Dystrophy are stronger and more determined than ever to
stop Duchenne in its tracks.
Because of you, we are filled with hope, promise, and momentum.
Exciting research is moving into the clinical trial pipeline. With the
publication of the Care Considerations, we now have a standard by
which physicians and caregivers can treat our children. The MD-CARE
Act has been reauthorized, and our voices continue to be heard in
Congress. We continue to raise money and awareness through
national programs like Coach To Cure MD and Run For Our Sons,
and through hundreds of grassroots events around the country.
Because of you, we continue to seek innovative ways to use social
media to build our community and bring us closer to a cure. We
have created a thriving Duchenne community site. We have an ever-
evolving presence on Facebook. We host webinars that respond to
pressing issues in our community.
Because of you, we can continue to expand our investments in
research, advocacy, care, and education.
Because of you, we will all win this fight. We will end Duchenne.
Warm regards,
Pat Furlong President, Chief Executive Officer Parent Project Muscular Dystrophy
DE
AR
PPM
D F
AM
ILY

PAR
ENT
PRO
JECT
MU
SCU
LAR
DY
STRO
PHY
Parent Project Muscular Dystrophy (PPMD) is the largest nonprofit
organization in the United States focused entirely on Duchenne muscular
dystrophy. We are the only Duchenne organization:
• To invest in a broad research
portfolio;
• To successfully leverage $15.4
million from the National Institutes
of Health (NIH) into a new drug
discovery program;
• To accelerate research through
a partnership with the NIH to
ensure that support continues
for promising research that would
otherwise fail to receive further
funding from the NIH;
• To consistently lobby the federal
government for muscular
dystrophy funding, thus far helping
to leverage $434 million into
muscular dystrophy research, with
$162 million specific to Duchenne;
• To convene topic-specific, care-
related workshops to better
understand the spectrum of issues
faced by those diagnosed with
Duchenne;
• To host a Duchenne-specific annual
conference in the United States;
• To receive the seal-of-approval from
the Better Business Bureau’s Wise
Giving Alliance;
• To receive a four-star rating from
Charity Navigator several years
running.
Since 1994, PPMD has improved the treatment, quality of life, and long-term
outlook for all individuals affected by Duchenne through research, advocacy,
care, and education. Because of our efforts, families affected by Duchenne
have better access to state-of-the-art care information, research is moving
forward at an accelerated pace, and legislation now exists to fund Duchenne
research and outreach programs.
The name of our organization
reflects our grassroots origins,
our parent-led focus, and
our passion. Parent Project
Muscular Dystrophy is now a name recognized around the world as the leader
in the Duchenne community. We hold the highest ethical standards and
consistently receive high marks from watchdog organizations.
We take a comprehensive approach in the fight against Duchenne—funding
research, promoting advocacy, connecting the community, broadening
treatment options, and raising awareness. Only this comprehensive approach
will lead to the day that 100% of those diagnosed can turn to a treatment that
will end Duchenne muscular dystrophy.
Duchenne muscular dystrophy (Duchenne) is the most common fatal genetic
disorder diagnosed in childhood, affecting approximately one in every 3,500
live male births (about 20,000 new cases each year). Because the Duchenne
gene is found on the X-chromosome, it primarily affects boys; however, it
occurs across all races and cultures.
Duchenne can be passed from parent to child, but approximately 35% of
cases occur because of a random spontaneous mutation. In other words,
Duchenne can affect any family. Although there are medical treatments that
may help slow its progression, there is currently no cure for Duchenne, and
young men with Duchenne typically live only into their late twenties.
AB
OU
T D
UC
HEN
NE
310

• Continued to invest in research and potential treatments that will benefit the entire Duchenne community;
• Partnered with the National Institutes of Health to launch the End Duchenne Grant Award Program (GAP), the first-ever Duchenne-specific bridging program, and the first NIH bridge- funding program presented in the rare disease category;
• Expanded PPMD’s scientific leadership by bringing in Sharon Hesterlee, Ph.D., as the new Senior Director of Research and Advocacy, and by establishing a new Scientific Advisory Board to review metrics in order to maximize research funding and its impact on this generation of boys;
• Led the advocacy initiative in the muscular dystrophy community, which resulted in the reauthorization of the MD-CARE Act;
• Hosted and expanded the PPMD annual Advocacy Conference, ensuring that our voice continues to be heard in Washington, DC;
• Expanded outreach and education initiatives with the Centers for Disease Control and Prevention (CDC) to help Duchenne patients receive earlier diagnosis and access to care;
• Worked alongside the CDC and other Duchenne authorities to help create the Care Considerations, the first published document in the Duchenne community outlining acceptable guidelines for care;
• Hosted our Annual Connect Conference, which continues to see 20% growth each year, with more than 50 scientific and medical professionals and hundreds of family members in attendance;
• Initiated the first-ever Duchenne Therapeutic Development Meeting in the United States, which runs in parallel with PPMD’s Annual Connect Conference;
• Expanded PPMD’s website to include a Duchenne-specific community site (community.parentprojectmd.org) that helps connect families from around the world;
• Supported and expanded DuchenneConnect.org, a community resource for families, healthcare professionals, researchers, industry, and policymakers to learn about clinical trials and treatments (in English and Spanish);
• Developed and launched FACES (Families Advocating, Connecting, Educating, and Supporting), the official parent-led outreach initiative of PPMD;
• Partnered with the American Football Coaches Association to develop Coach To Cure MD, a national one-day awareness event for Duchenne muscular dystrophy;
• Expanded the Run For Our Sons program to include more national marathon programs, as well as local 5K and 10K events;
• Capitalized on the growing social media network to expand PPMD’s visibility and awareness for Duchenne muscular dystrophy.R
ECEN
T A
CH
IEV
EMEN
TS
Behind the compounds in clinical testing now lies a full “pipeline” of compounds in the
preclinical stage. Thanks to the tremendous efforts of everyone involved, our flagship
Project Catalyst program with PTC Therapeutics has produced two drug candidates, a
utrophin upregulator and a myostatin inhibitor. Each has entered the final phase of
optimization in preparation for clinical development. Our funds have also supported the
preclinical development of “biglycan,” another compound that stimulates utrophin upregulation.
Our new End Duchenne Grant Award Program (GAP), which provides additional funding
to investigators who just miss the National Institutes of Health (NIH) pay-line so that they
can gather additional data to bolster their resubmission, also noted its first successes in
2010. GAP recipients Justin Fallon and Krista Vandenborne parlayed their PPMD awards
into winning re-applications at the NIH.
Our grantees understand that we are not just a source of funding, but rather a committed
partner. We bring the right scientific and clinical advisors to the table; we meet with
companies and regulatory authorities; we advocate for research funds; and we ensure
that the voice of the family is heard in the process.
RE
SEA
RC
H
5
These are just some of our recent accomplishments in our fight to end Duchenne:
PPMD’s research program has kicked into high gear, and investments in therapy
development are starting to bear fruit. Never before have there been so many
promising drug candidates either in clinical testing or headed to the clinic in the
near term, and many of them have benefited from our funding:
• PTC Therapeutic’s Ataluren completed a Phase IIb study;
• AVI and Prosensa each conducted studies of systemic compounds to skip exon 51;
• Prosensa began clinical development of a compound to skip exon 44;
• Biomarin began testing of its utrophin up-regulating compound in healthy volunteers;
• Acceleron launched its first study of a muscle enhancer in Duchenne;
• Nationwide Children’s Research Hospital in Columbus, Ohio, began enrollment for a study to compare losartan and ACE inhibitors;
• Two academic groups began planning for an initial study of sildenafil, a nitric oxide upregulator.
PrOject catalyst Established in 2004, Project Catalyst is a first-of-its-kind research initiative designed to identify new
drugs to treat the present generation of young men with Duchenne. Project Catalyst is a collaboration
between PPMD and PTC Therapeutics, Inc., a biopharmaceutical company focused on the discovery,
development, and commercialization of small-molecule drugs. Our initial $3 million investment in
Project Catalyst helped leverage an additional $18 million into this drug discovery program. Project
Catalyst continues to be a leading program in the Duchenne research arena, one that is swiftly moving
closer to the development of treatments for every young man diagnosed with Duchenne.
76
RE
SEA
RC
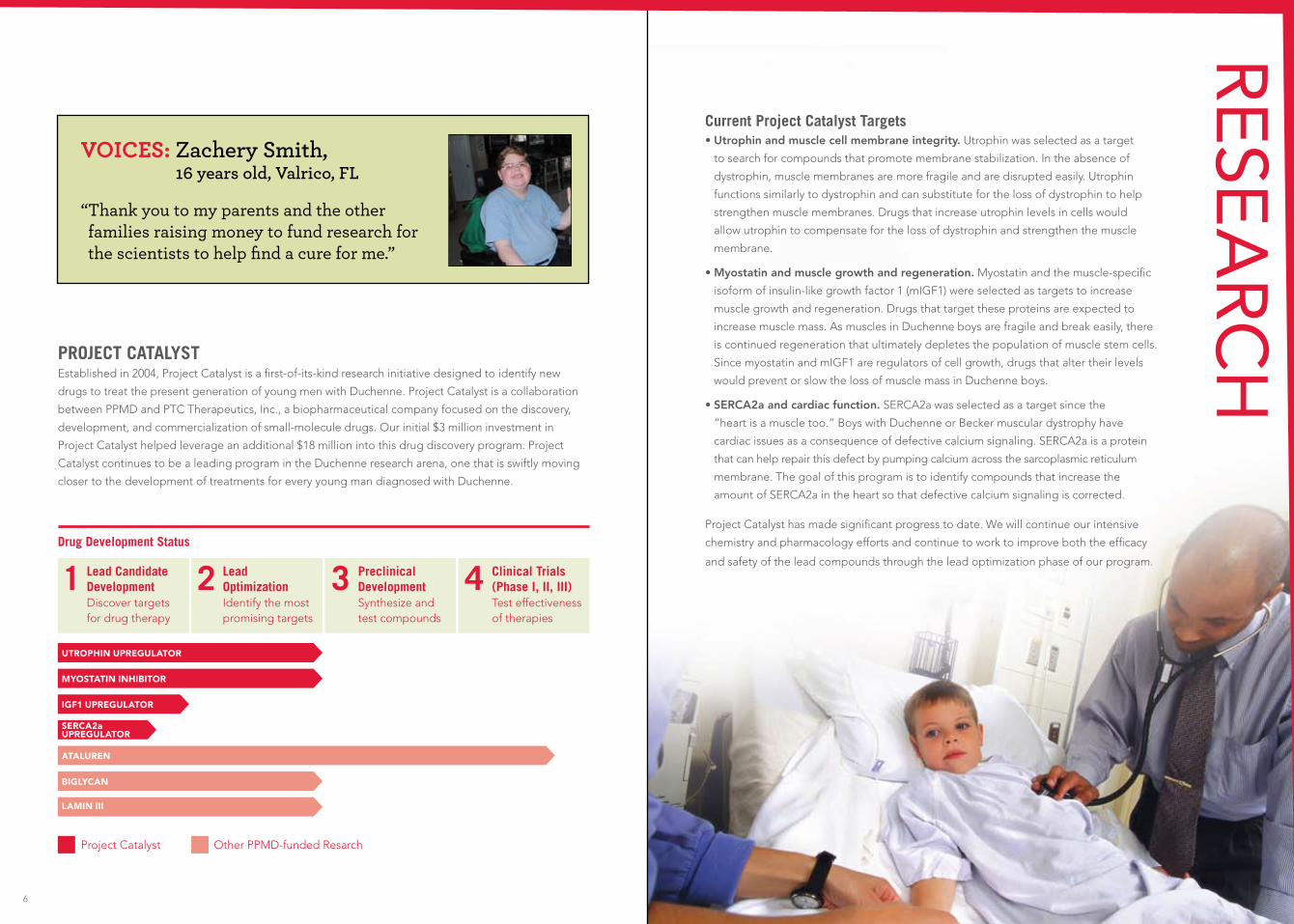
HVOICES: Zachery Smith,
16 years old, Valrico, FL “ Thank you to my parents and the other families raising money to fund research for the scientists to help find a cure for me.”
current Project catalyst targets • Utrophin and muscle cell membrane integrity. Utrophin was selected as a target
to search for compounds that promote membrane stabilization. In the absence of
dystrophin, muscle membranes are more fragile and are disrupted easily. Utrophin
functions similarly to dystrophin and can substitute for the loss of dystrophin to help
strengthen muscle membranes. Drugs that increase utrophin levels in cells would
allow utrophin to compensate for the loss of dystrophin and strengthen the muscle
membrane.
• Myostatin and muscle growth and regeneration. Myostatin and the muscle-specific
isoform of insulin-like growth factor 1 (mIGF1) were selected as targets to increase
muscle growth and regeneration. Drugs that target these proteins are expected to
increase muscle mass. As muscles in Duchenne boys are fragile and break easily, there
is continued regeneration that ultimately depletes the population of muscle stem cells.
Since myostatin and mIGF1 are regulators of cell growth, drugs that alter their levels
would prevent or slow the loss of muscle mass in Duchenne boys.
• SERCA2a and cardiac function. SERCA2a was selected as a target since the
“heart is a muscle too.” Boys with Duchenne or Becker muscular dystrophy have
cardiac issues as a consequence of defective calcium signaling. SERCA2a is a protein
that can help repair this defect by pumping calcium across the sarcoplasmic reticulum
membrane. The goal of this program is to identify compounds that increase the
amount of SERCA2a in the heart so that defective calcium signaling is corrected.
Project Catalyst has made significant progress to date. We will continue our intensive
chemistry and pharmacology efforts and continue to work to improve both the efficacy
and safety of the lead compounds through the lead optimization phase of our program.
Drug Development status
lead candidate Development Discover targets for drug therapy
1 2 lead Optimization Identify the most promising targets
3 Preclinical Development Synthesize and test compounds
4 clinical trials (Phase i, ii, iii) Test effectiveness of therapies
utrophin upregulator
lamin iii
biglycan
ataluren
igf1 upregulator
myostatin inhibitor
Project Catalyst Other PPMD-funded Resarch
serca2a upregulator

RE
SEA
RC
H
98
Edward Tenthoff, Piper Jaffray
Jeff Molkentin, Ph.D., Cincinnati Children’s Hospital Medical Center
Jody Puglisi, Ph.D., Stanford University
Katherine D. Mathews, M.D., University of Iowa
Kathryn Wagner, M.D., Ph.D., Kennedy Krieger Institute
Lee Sweeney, Ph.D., University of Pennsylvania
Lorenzo Puri, M.D., Ph.D., Burnham Institute
Ronald Meyer, Ph.D., Michigan State University
enD Duchenne Grant awarD PrOGraM (GaP) We developed the End Duchenne Grant Award Program in partnership with the National Institutes
of Health (NIH) to ensure that funding continues for promising research that would otherwise fail to
receive further funding from the NIH. Our bridge funding accelerates research and strengthens the
possibility that researchers will receive future federal dollars toward the development of new treatments
for Duchenne.
summary of year-1 Funded Grants1. Brown University/Justin Fallon—Biglycan as a potential therapeutic treatment for Duchenne
muscular dystrophy. Outcome: NIH Award granted.
2. U. Florida/Krista Vandenborne—Magnetic Resonance Imaging and Biomarkers for Muscular
Dystrophy. This proposal intends to validate the potential of noninvasive magnetic resonance
imaging (MRI) and spectroscopy (MRS) to monitor disease progression and to serve as an outcomes
measure for clinical trials in Duchenne muscular dystrophy. Outcome: NIH Award granted.
3. UCLA/Melissa Spencer—Osteopontin (OPN) as a Therapeutic Target. This proposal will evaluate
the validity of Osteopontin as a therapeutic target in Duchenne muscular dystrophy. OPN appears to
regulate the immune milieu of dystrophic muscle and its ablation generates a more immunologically
favorable anti-inflammatory environment.
4. UCLA/Carmen Bertoni—High throughput screening (HTS) to identify chemical compounds that
increase the efficiency of oligonucleotide-mediated (ssODN) gene correction in Duchenne and that
can be advanced into a clinical application for the treatment of Duchenne muscular dystrophy. This
proposal will screen the Prestwick library, a collection of all of the FDA-approved drugs, to identify
compounds that can significantly enhance the ssODN mediated gene repair and that are already
approved for use in humans, thus increasing the chances of moving this technology into a clinical
scenario in a relatively short period of time.
5. Prothelia/Bradley Hodges—IV-based protein therapy approach to treat Duchenne muscular
dystrophy. Prothelia has an exclusive license to the protein therapeutic PRT-01. This approach is
evaluated to understand the potential to stabilize both skeletal and cardiac muscles by enhancing
the activity of non-dystrophin surrogates.
PPMD end Duchenne GaP scientific advisory Board
aDDitiOnal PrOjects FunDeD By PPMD Project: Gene therapy/myostatin inhibition in mice and dogs Myostatin inhibition is an attractive therapeutic target because inhibition relates to
how well muscle mass is maintained in a variety of disorders, including the muscular
dystrophies, cachexia, and sarcopenia. This project was funded to understand the
degree of benefit in skeletal muscle, and the possible positive and/or negative effects
on the heart. These experiments are ongoing and should give a realistic view of the
pros and cons of myostatin inhibition as a potential treatment for Duchenne.
Project: influence of long-term myostatin inhibition on dystrophic cardiomyopathy This is a follow-on project to the gene therapy/myostatin inhibition to further
investigate the effect on heart function. An unexpected finding in dystrophic (mdx) mice
following long-term myostatin inhibition is an inhibitor-dose-dependent increase in heart
weight and a decline in systolic function. This project was developed to perform serial
echocardiograms on these animals to precisely track alterations in heart function.
Project: increasing calcium buffering in mdx mice with over-expression of serca1a It has been well documented that dystrophin deficiency in muscle results in excess
calcium influx following contraction, and that this ultimately leads to muscle damage
through multiple maladaptive mechanisms. Additionally, experimental evidence indicates
there may be a calcium-pumping deficit due to the loss of expression of SERCA1a in fast
fibers (Divet A 2005). These experiments could validate that altering calcium handling in
skeletal muscle in Duchenne patients is a reasonable therapeutic approach.
Project: investigation of PGc-1a as a target and sirt1 activators Increased utrophin expression has repeatedly been shown to reduce pathology in dystrophic
skeletal muscle. In addition, dystrophic muscle demonstrates mitochondrial abnormalities
(likely due to oxidative free radical damage). Recently, PGC-1 activation has been shown to
increase oxidative genes, and transgenic mdx mice over-expressing PGC-1 had increased
utrophin mRNA and improved histology. While it was not shown in previous studies, if
over-expression of PGC-1 in post-natal mdx mice increases utrophin, then the dystrophic
muscles should be more resistant to damage caused by lengthening contractions.
Project: continuing examination of the Bowman-Birk inhibitor (BBi) in dystrophic mice BBI improves the overall phenotype of the muscles of the mdx mouse, including
increasing mass and strength and decreasing necrosis. However, as expected, BBI does
not treat the underlying increased sensitivity damage that is due to loss of dystrophin.
Nevertheless, it is likely the increased force production and decreased necrosis will slow
the progress of disease and lead to an improved quality of life for those afflicted with
Duchenne. This project will evaluate the effects of administering pure BBI compared to
the effects of using different purification processes.

aDDitiOnal PrOjects FunDeD By PPMD (cOnt’D)
1110
Project: aaV-mediated cardiac gene therapy in the dog model of Duchenne muscular dystrophy Virtually all patients with Duchenne develop cardiomyopathy, but clinical signs associated with the
cardiovascular system may be masked by severe skeletal muscle weakness. Gene replacement therapy
is a promising technique that may result in direct myocardial and skeletal muscle improvement.
Although there are two strategies currently under investigation using AAV vectors to provide dystrophin
expression in skeletal muscle in Duchenne patients, it is unknown whether the myocardial response to
therapy will mirror the skeletal muscle response. This project compares AAV-directed exon-skipping (U7)
in the GRMD dog (which creates a nearly full-length dystrophin protein), to the delivery of a micro-
dystrophin, which will fail to rescue a number of components of the cardiac DGC, including NOS.
Project: Preconditioning stem cells in culture The delivery of muscle adult stem cells may provide a means to correct the skeletal muscle of patients
with a number of different forms of muscular dystrophy. The goal of this work is to develop technologies
that will promote and reinforce stem cell commitment to the myogenic lineage prior to implantation in
a diseased tissue. This project is a collaboration between the U.S. and France. An important objective
of the overall project is not only to understand to what extent external signals associated with disease
can be overridden in stem cells leading to the desired specification, but also to determine to what
extent the physical properties of the diseased matrix will interfere with specification and ultimately
differentiation into muscle.
RE
SEA
RC
HTo help expand our drug development
and advocacy efforts, Sharon Hesterlee,
Ph.D., has joined PPMD’s staff.
Dr. Hesterlee, whose background is
in neuroscience, comes to us after
11 years at the Muscular Dystrophy
Association, where she developed
MDA’s translational research and
venture philanthropy programs
and brokered $28 million worth of
biotechnology contracts.
President Pat Furlong welcomed
Dr. Hesterlee to PPMD in January
2010. “Sharon brings with her not only
expertise in the field of neuromuscular
disease and experience brokering
partnerships with industry, but she
also brings with her a passion for
fighting— fighting for the best
treatments, fighting to find a cure,
fighting to end Duchenne. Sharon
could have gone to any organization
working with any neuromuscular
disease. The fact that someone of her
talent and intelligence wanted to work
with PPMD is humbling, and it reinforces
the Duchenne community’s belief in
what we are doing.”
Dr. Hesterlee sees
a transition in
thinking around the
development of
new drugs. “For
so many years,
companies were
only interested in
developing drugs for big markets.
It’s amazing to see the amount of
interest Duchenne is getting now,”
said Dr. Hesterlee. “But the more
candidates we have in testing the
better, so we have to think creatively
about what we can do as a community
to provide incentives for industry. A
robust patient registry that allows us
to efficiently identify trial participants,
validated endpoints, and biomarkers
for clinical studies—these things can
all dramatically decrease the cost of
developing a new drug. PPMD has
made a good start with the
DuchenneConnect registry and the
Six-Minute Walk Test. Now we should
focus on developing good biomarkers.”
PPMD welcomes sharon hesterlee, Ph.D.

AD
VOC
AC
Y
AN
D IM
PAC
TFor years, Parent Project Muscular Dystrophy has facilitated interactions
between families and members of Congress through our annual Advocacy
Conference in Washington, DC, legislative roundtables, and more. Our
efforts have secured tens of millions of dollars for Duchenne research and
care centers, from the Centers for Disease Control and Prevention (CDC)
and from the National Institutes of Health (NIH).
• In 2001, Congress passed the MD-CARE Act, the first legislation for muscular dystrophy. It is also the only condition-specific legislation to become law in recent years. The bill was reauthorized
in 2008.
• Since passage of the MD-CARE Act, more than $434 million has been invested in muscular dystrophy research with more than $162 million going to
Duchenne-specific research.
• Six Wellstone Centers of Excellence have been established
as a result of the MD-CARE Act.
• Our annual Advocacy Conference unites hundreds of families from across the United States and is the largest organized Duchenne
advocacy event.
• Our advocates visit hundreds of congressional offices annually, urging an increase in funding at
the NIH and the CDC.
• We are represented on the Muscular Dystrophy Coordinating Committee; the committee was established with the MD-CARE Act and is charged with developing and executing the research agenda
for the muscular dystrophies.
• Pat Furlong is a committee member on the Collaboration in Education and Test Translation Program. She serves on the Institute of Medicine Committee on Accelerating Rare Diseases Research and Orphan Product Development. She also serves as a member of the National Task Force for the Early Identification of Childhood Neuromuscular Disorders. She is also on the data safety monitoring board for both the Rare Diseases Clinical Research Network and the Cooperative International Neuromuscular Research Group.
reauthOrizatiOn OF the MD-care act Since passage of the MD-CARE Act in 2001, major advancements have taken place in research, drug
trials, and care methods. In 2008, again due in large part to the leadership and commitment of our
advocacy campaign, Congress reauthorized the MD-CARE Act to continue funding vital research,
giving continued hope to families.
VOICES: Michael Gaglianone, 14 years old, Mt. Ephraim, NJ
“ When I went to Washington, DC, and talked, I felt like it was the most important thing I ever did. I felt like I was doing my part to let them know that me and other kids need their help so not as many kids have to go through not being able to walk.”
1312
PPMD’s annual aDVOcacy cOnFerence Every year, families from across the country gather in Washington, DC, for the largest annual Duchenne-
specific organized advocacy event. Advocates spend several days visiting hundreds of members of Congress
to make sure the voices of those living with Duchenne are heard throughout the halls of Capitol Hill. These
efforts have resulted in the MD-CARE Act (which included the establishment of six Wellstone Centers of
Excellence), the Reauthorization of the MD-CARE Act, and increased funding to the NIH and the CDC.
the MD-care act PPMD led the charge for the 2001 MD-CARE Act, the first muscular dystrophy legislation passed
by Congress. This critical piece of legislation directed the National Institutes of Health to establish
a government-wide Muscular Dystrophy Coordinating Committee, and it also directed the CDC
to expand data collection on muscular dystrophy. The MD-CARE Act also called for the creation
of scientific Centers of Excellence across the country to accelerate research on muscular dystrophy.
Named after the late Senator Paul D. Wellstone, the six centers are supported by collaborations
among the following:
• Promoting collaborations and providing shared
resources;
• Advancing basic research while stimulating
translational research;
• Fostering outreach activities;
• Developing greater patient awareness of
basic and clinical research and enabling their
participation in clinical trials;
• Facilitating the development of gene therapy for
the muscular dystrophies.
• National Institute of Arthritis and
Musculoskeletal and Skin Diseases;
• National Institute of Child Health and
Human Development;
• National Institute of Neurological Disorders
and Stroke.
The Centers’ goals are to provide an interactive environment that will advance knowledge of and
treatments for the muscular dystrophies by:

CA
RE
care cOnsiDeratiOns Care for Duchenne varies in the United States and around the world. In 2005, we began
working with leadership at the Centers for Disease Control and Prevention (CDC) to
establish a steering committee that would lead the effort for the development of Care
Considerations in Duchenne. Since our founding in 1994, PPMD has pushed to establish
clear, specific treatment guidelines for those with Duchenne. At last, we have them.
In February 2010, the DMD-Care Considerations Working Group published guidelines
in Lancet Neurology titled ”Diagnosis and Management of Duchenne Muscular
Dystrophy,” in which the group evaluated assessments and interventions used in the
management of Duchenne muscular dystrophy. The authors’ recommendations are
intended for the wide range of physicians and healthcare professionals who care for
individuals with Duchenne.
The publication of these important guidelines are the result of a three-year project to
provide a framework for recognizing the multisystem primary manifestations and
secondary complications of Duchenne; and for providing multidisciplinary care.
The Lancet guidelines represent an important part of the CDC’s commitment to
muscular dystrophy and will help healthcare providers better diagnose and care for the
Duchenne community. The Care Considerations were reviewed and rated by 84 national
and international experts representing 20 disciplines. The Care Considerations represent
an expert consensus about care, and they establish guidelines about what care should
be like, what tests should be given, and what medicines/treatments need to be added
and when. The Care Considerations discuss the need for multidisciplinary care
(coordinated care that involves many subspecialists), the need for genetic testing,
and the importance of family participation in global registries. Essentially, the Care
Considerations provide a roadmap for better care.
Better care translates into an improved quality of life and extended life span for our
children. It provides all of us—parents, children, researchers, and clinicians—with a level
of confidence about care. With the Care Considerations, we are able to highlight gaps
in care and point to what we need to think about in order to improve our base of
knowledge. This in turn prepares our sons for clinical studies; and it sets researchers,
clinicians, and industry on a path toward new and promising therapies.
VOICES: Seph Ware, 8 years old, West Monroe, LA
“ Better information means better doctors. Everyone needs a good doctor.”
1514

DuchenneConnect is a central
hub, linking patients, resources,
and industry professionals.
1,700 patient records
patients & families
doctors researcherspolicy
makersindustry
Duchenneconnect Patient Diagnosis
Duchenne
Becker
Unconfirmed
Confirmed Carrier
At Risk to be Carrier
Manifesting Carrier
81%
7%
6%
3%
2%
1%
Duchenneconnect Patient ambulation status
Walk without assistance
Do not walk
Use assistive devices
55%
30%
15%
60 countries
the natiOnal task FOrce FOr early iDentiFicatiOn OF chilDhOOD neurOMuscular DisOrDers To address the delay that families frequently experience between symptom onset and
diagnosis of neuromuscular disorders, in 2009 we convened The National Task Force for
Early Identification of Childhood Neuromuscular Disorders. The Task Force is funded by
a cooperative agreement from the CDC and includes representatives from:
• Parent Project Muscular Dystrophy;
• American Academy of Pediatrics;
• American Academy of Neurology;
• Childhood Neurology Society;
• American Academy of Physician Assistants;
• National Association of Pediatric Nurse Practitioners;
• National Society of Genetic Counselors;
• National Coalition for Health Professional Education in Genetics;
• Muscular Dystrophy Association;
• Cure CMD;
• SMA Foundation;
• Families of SMA.
EDU
CA
TIO
N A
ND
Aw
AR
ENE
SS
The Task Force aims to increase clinicians’ awareness of neuromuscular disease as a cause
of developmental delay in young children ages six months to five years, and to help health
care providers who see children in their early years of life become better at identifying
the early symptoms of neuromuscular disorders so they can make appropriate referrals.
Specifically, the Task Force is working towards a set of outcomes in which providers will:
• Perform developmental motor assessment, screening, and appropriate follow up and referral;
• Evaluate for motor weakness in all children with developmental delay, and consider obtaining CK testing;
• Be attentive to parents’ concerns about their children’s motor development;
• Be less inclined to “wait and see” and more inclined to act on motor delay;
• Appreciate that early signs of neuromuscular weakness may be more subtle, and different, than later signs.
To achieve these outcomes, we are developing a set of core educational messages that
will be incorporated into fact sheets, a series of case studies, and an online video library
illustrating early signs of neuromuscular weakness.
17
VOICES: Josh Winheld, passed away December 2009 at age 31, Mt. Ephraim, PA
“ I always felt that if I had to have this disease, some good ought to come from it. To that end it’s my sincere wish that my story will add to the wealth of knowledge that exists on living with serious illnesses.” –From Josh’s book: Worth the Ride
DuchennecOnnect Now that each child’s specific genetic mutation can be identified, the challenge remains to collect
enough data to understand the relationship between the mutation and the clinical course. That’s why
PPMD created DuchenneConnect.org, the central community resource for families, healthcare
providers, researchers, industry professionals, and policymakers.
DuchenneConnect.org is interactive, notifying families of promising clinical trials, and it offers
researchers/industry the opportunity to understand the progression of the disorder and the patient
population, thereby accelerating the development of new treatments.
The response to DuchenneConnect has been remarkable, reinforcing our belief that this online
resource meets a very real need within the clinical trial process. In its first three years, more than 1,700
individuals from 60 countries have registered with DuchenneConnect.org and reported their diagnoses
and ambulatory status.

PPMD’s annual cOnnect cOnFerence What started almost two decades ago as a small group of parents gathering to discuss
current Duchenne topics has evolved into the only annual conference focused entirely
on Duchenne muscular dystrophy: PPMD’s Annual Connect Conference.
Each year nearly 500 families from around the world gather to learn the latest progress
in the fight to end Duchenne. They also gather for support, strength, and camaraderie.
Our Annual Connect Conference is an opportunity for families, physicians, researchers,
and experts of all kinds to speak face-to-face about Duchenne. These discussions open
communication channels, lay the groundwork for future collaborations, and shape our
understanding of the Duchenne landscape.
The PPMD Annual Connect Conference features presentations on such topics as:
• The Basics of Duchenne: Understanding the Diagnosis;
• Genetic Testing and DNA Sequencing;
• Optimal Care: Understanding Steroids, Growth Hormone, Cardiac and Respiratory;
• Practical Physical Therapy sessions;
• Behaviors in Duchenne;
• Coping and Living in the Present;
• Updates on Current and Forthcoming Clinical Trials;
• The Community Impact in
Washington, DC;
• Reports from the FDA and NIH;
• Duchenne Research Strategies and Timelines;
• Approved Drugs and Their Use in Duchenne;
• Living with Duchenne: Our Expert Panel;
• Family Dynamics.
As part of our 2010 Connect Conference, we introduced the first Duchenne Therapeutic Development
Meeting, a scientific meeting that ran parallel with the Connect Conference. While we still provided
expert presentations regarding Duchenne research during the comprehensive Connect Conference,
we felt the need to also hold a scientific meeting that was exclusively dedicated to Duchenne research.
By providing a specific forum for researchers, we united the Duchenne research field and encouraged
research collaborations.
CO
MM
UN
ITY
• Representatives from eight biotech companies including AVI, GSK, Acceleron,
and PTC Therapeutics;
• Scientists representing every major therapeutic approach in development for Duchenne,
from exon-skipping to utrophin upregulation, from gene therapy to cell therapy.
scientific conference attendees of note:
1918

Duchenne Faces FACES stands for Families Advocating, Connecting, Educating, and Supporting. Duchenne
FACES is the official parent-led outreach initiative of PPMD. FACES outreach locations
offer families affected by Duchenne and Becker a regional PPMD point of contact and
serve as a volunteer extension of our central offices. FACES provides family mentoring,
supports national awareness and advocacy campaigns, and helps raise money for PPMD.
FACES groups continue to grow, with monthly meetings and events around the country.
cOach tO cure Parent Project Muscular Dystrophy has joined forces with the American Football Coaches
Association for the Coach to Cure MD program (CoachToCureMD.org). Coach to Cure MD
raises awareness during nationally-televised Saturday college football games and reaches
millions of people in the process. Coaches at more than 350 colleges and universities have
participated by wearing Coach To Cure MD armbands and by talking about Duchenne to
the press and raising awareness on campus. Thanks to their efforts, hundreds of articles
about Coach To Cure MD and Duchenne have appeared in national and local newspapers,
blogs, and websites.
Additionally, nearly 200 Coach To Cure MD events have taken place around the country—
from Alaska to Florida and everywhere in between. Combined with grassroots support
from local community high schools and junior leagues, Coach to Cure MD is a vital part of
our efforts to create exposure and raise funds to fight this devastating disorder.
sOcial MeDia: cOMMunity site, FaceBOOk, twitter, yOutuBe channel In 2008, PPMD launched www.Community.ParentProjectMD.org to unite families and
friends online in a virtual world that offers robust discussions and opportunities to
connect with people on similar Duchenne journeys. The community site—in combination
with our Facebook fan page, Twitter, YouTube channel, and RSS feed—reaches more
than 10,000 people and has become a critical communications tool and great fundraising
resource, winning $75,000 in online, social media contests. In a time of instantaneous
news, we have stayed at the forefront of technological advances to reach members of
the Duchenne community when they want, where they want, and how they want. Our
online community is a tremendous asset in our fight to end Duchenne.
VOICES: Joel Poysky, 7 years old, Katy, TX
“ The coaches [in Coach to Cure] are nice because they are raising money for boys like me. I think the coaches are cool. I hope it will help make a medicine so that my arms and legs will get better... I want the medicine to make me normal.”
2120
CO
MM
UN
ITY
run FOr Our sOns With thousands of runners and millions of dollars raised, Run For Our Sons is an important way for
members of the Duchenne community to come together and take action. Run For Our Sons teams
and fans participate in major marathons and half marathons around the country and inspire crowds
to go the distance to end Duchenne. In towns and cities all over America, families, friends,
churches, and schools host family fun runs, 5Ks, and 10Ks to raise awareness of Duchenne. Our
website, RunForOurSons.org, makes it easy for runners, “spirit” runners, families, and friends to go
the distance for Duchenne research and treatment.
GET
INVO
LVED Get involved today. There are so many simple, effective ways to support the work
of Parent Project Muscular Dystrophy:
• Make a donation;
• Join Striving to Impact Research (S.T.I.R.),
our monthly giving plan;
• Invite others to make donations;
• Host an event;
• Host a Coach To Cure MD event;
• Join or support a
Run For Our Sons team;
• Sign up at DuchenneConnect.org;
• Get active on the
PPMD community site;
• Contact your congressional
representative;
• Teach others about Duchenne;
• Attend the Annual Connect
Conference;
• Visit ParentProjectMD.org
to learn more.
raise yOur VOice— yOur VOice tO enD Duchenne Maybe you’re a parent or sibling of a young
man with Duchenne. Perhaps you’re a friend
of a family affected by Duchenne. Maybe
you’re a doctor, researcher, or caregiver.
Perhaps you even have Duchenne yourself.
Each of us has a voice in the fight to
end Duchenne. Each of us has a story to
tell. And every story is as unique as the person
telling it.
We are many voices. But we all want one
thing: we want to end Duchenne. In this
fight, we are all one voice. Raise your
voice with us and support our efforts.
we must end Duchenne. and we will end Duchenne.
ParentProjectMD.org
ParentProjectMD.org
22

FINA
NC
IALS
STATEMENT OF ACTIVITIES For the Years Ended December 31, 2011 and 2010
Unrestricted Net Assets 2011 2010
Revenue and Other Support
Grants and Contributions $ 5,195,537 $ 5,638,319
Program Revenue 77,571 58,075
Investment Loss (9,469) (61,638)
Interest and Dividend Income 9,589 3,773
Fundraising Proceeds 1,059,625 1,031,973
(net of direct expenses of $333,208 and $422,775, respectively)
Total Revenue and Other Support 6,332,853 6,670,502
Expenses
Program Services 5,216,305 3,678,123
Management and General Expenses 417,787 423,984
Fundraising Expenses 585,946 484,017
Total Expenses 6,220,038 4,586,124
Increase (decrease) in Unrestricted Net Assets 112,815 2,084,378
Net Assets
Net Assets, Beginning of Period 2,735,521 651,143
Net Assets, End of Period $ 2,848,336 $ 2,735,521
Copies of the full 2011 and 2010 audits are available upon request. See reverse side for Statement of Functional Expenses.
Parent P
roject M
uscular Dystro
phy ParentProjectM
D.org

STATEMENT OF FUNCTIONAL EXPENSES For the Year Ended December 31, 2011 with Comparative Totals for 2010
Research Education Advocacy Mgmt. & Fundraising 2011 2010 General Total Total
Salaries $ 591,720 273,818 504 65,379 91,802 1,023,223 976,972
Payroll Taxes 53,705 21,073 – 6,077 8,533 89,388 75,391
Employee Benefits – – – 25,080 – 25,080 23,198
Accounting Fees – – – 101,291 16,500 117,791 86,703
Conferences
Legal Fees
7,675 – – 2,140 – 9,815 4,342
Bank Charges – – – 6,554 154,455 161,009 99,390
Interest Expense – – – 2 – 2 14
Fees and Permits 5,367 335 100 – 140,755 146,557 94,467
Insurance – 8,394 – 84,635 – 93,029 93,753
Outside Services 47,357 – – 5,224 25 52,606 2,750
Office and Computer
Technology 5,500 56,593 – 23,769 – 85,862 70,364
Rent 87,718 10,302 1,231 9,926 13,937 123,114 115,198
Postage and Shipping – 24,772 – 3,539 7,078 35,389 25,014
Printing and
Publications – 10,620 – 4,059 17,062 31,741 55,154
Consulting Fees
Telephone – 26,045 376 3,721 7,441 37,583 41,585
Utilities – – – 14,758 – 14,758 8,073
Merchandise – – – – 15,582 15,582 17,994
Travel 163,888 13,506 – 19,561 20,830 217,785 216,590
Meals and
Translation
– – – – – – 317,757
NIH Activity 2,244 – – – – 2,244 –
CDC Activity – 461,035 – – – 461,035 228,791
Total Before Grants
and Depreciation 1,133,030 1,224,018 193,211 414,685 583,455 3,548,399 3,343,663
Grants 2,663,480 – – – – 2,663,480 1,229,504
Depreciation – 2,491 75 2,491 2,491 7,548 12,797
Total Functional
Expenses
$ 3,796,510
1,226,509
193,286
417,787
585,946
6,220,038
4,586,124
Parent P
roject M
uscular Dystro
phy ParentProjectM
D.org
and Meetings 10,918 251,119 84,280 – 346,317 279,588
Expenses 1,813 3,184 – 25,273 13,854 44,124 63,534
136,386 45,150 106,720 59,057 347,313 364,006
Meals and
Entertainment 18,739 18,072 – 13,697 16,544 67,052 83,035
Loss on Disposal
of Equipment – – – 611 – 611 160
–
–

BO
AR
D
AN
D STA
FFBOARD OF DIRECTORS Robert J. McDonald, MD, Chairman, Jefferson City, MO
John Killian, Treasurer, Dallas, TX
Daniel Garofalo, Secretary, Middlesex, NJ
Neil Brandom, Newport Beach, CA
David Drohan, Bluffton, SC
Anessa Gaydou-Fehsenfeld, Rockford, MI
John Hiatt, Chicago, IL
Howard Kaplan*, Riverwoods, IL
Martin Karlin, Naperville, IL
Heinrich Meermann, The Woodlands, TX
Robert Nutt, Darien, IL
Christine L. Piacentino*, Rochester, NY
James Poysky, PhD, Katy, TX
Donna Saccomano*, New Rochelle, NY
* lifetime, non-voting board member
STAFF
Pat Furlong, President, Chief Executive Officer
Kimberly Galberaith, Chief Operating Officer
Sharon Hesterlee, Ph.D., Senior Director of Research and Advocacy
Holly Peay, MS, CGC, Senior Director of Outreach and Education
Will Nolan, Director of Communications and Administration
Ryan Fischer, Director of Community Outreach and Advocacy
Laurie Cicalo
Brian Denger
Danielle Garrigan
Janet Krakowski
Stephanie Matthes
Cecilia Matthes-Petersen
Nicole Rottino
Parent P
roject M
uscular Dystro
phy ParentProjectM
D.org
Catherine Jones Collins, New York, New York
Bob Getler, Louisville, KY
Lance Hester, Gig Harbor, WA
Jasbir Seehra, PhD, Lexington, MA
Ann Martin, MS, CGC, Genetic Counselor & DuchenneConnect Coordinator
Jody Gabbard





























