Embed Size (px)
Citation preview
A Sponsored Supplement To Science
MEDICINE
SELE C TE D PR E S E NTAT I O N S FROM TH E
ON CLINICAL AND TR ANSL ATIONAL
2011 SINO -AMER I C AN SYMPOSIUM
Sponsored by
Global MD OrganizationProduced by the
Science/AAAS Custom Publishing Office

ScienceCareers.org
Get a Career Plan that Works.An exceptional career requires insightful planning and management. That’s where Science Careers comes in. From job search to career enhancement, Science Careers has the tools and resources to help you achieve your goals. Get yourself on the right track today and get a real career plan that works. Visit ScienceCareers.org.
LabNote_full.indd 1 2/15/11 3:00 PM

Cancer: From Basic Science to Clinical Research
30 Translational Strategies in Gastric
Cancer ResearchYongzhan Nie, Yongquan Shi, Zhiping Yang, et al.
31 Cell Cycle Regulators and Malignant Tumor Biomarkers Tong Tong, Yongmei Song, Shujuan Shao, et al.
33 Translational Medicine for Myeloid Leukemia Sai-Juan Chen
35 Translational Medicine in Oral Cancer Lai-ping Zhong, Zhi-yuan Zhang
36 Translational Science for Targeted Personalized Medicine Treatments Ákos Végvári, Melinda Rezeli, Balázs Döme, et al.
four:
Promoting Effective Communication and Enabling “Constraint" Research
16 From Genome to 4P Medicine
Shengli Yang
17 The Value of Dedicated Research Units to Reproducible Clinical InvestigationDonald A. McClain
18 Development of a Training Program for Physicians and Researchers to Advance Global Standardization in Clinical Research Tim Z. Shi, Carol B. Collado, Xiaokun Liang, et al.
20 A Novel Approach to Teaching Clinical and Translational Science Using Adult Learning Principles, Learner-Centered Outcomes, and Hierarchical CompetenciesDeborah Helitzer, Jeff Norenberg, Kristina Wittstrom
22 Center for Translational Research in Biomedical Sciences, Chang Gung Memorial Hospital–Kaohsiung Medical Center, Taiwan Samuel H. H. Chan
23 New Commercialization Models for Early Stage Health Research Natalie Dakers, Barry Gee, Michel Roberge
two:
Table of Contents 1
Synergism: Cooperation Between Industry, Investors, Government, and Academia
24 Keeping the End Goal in Mind: Multinational Collaborative Research ProgramsRobert M. Califf
26 Personalized MedicineVicki Seyfert-Margolis
27 Business and Commercial Aspects of InnovationRobert Go
29 Validating Government Investment in Biological ResearchRegis B. Kelly
three:
Defining the Vision and Strategies for Collaboration: Institutional and International
7 National Plan on Translational Medicine in China: Promoting Health Care Reform and Improving People’s Health
Zhu Chen
8 Global Outreach in Clinical Research by the NIH Clinical Center: Building Training Partnerships with ChinaFrederick P. Ognibene, Tim Z. Shi, John I. Gallin
10 Developing Rational Antiplatelet Agents: From Bedside to Bench and Back Barry S. Coller
11 The NIH Vision on Advancing Translational Medicine and Therapeutics: Role of International Collaborations for CTSA Member Institutions in the United StatesAnthony Hayward
13 From Medical Research to Public Health Policy: An Integral Part of Translational MedicineXiaoming Shen
15 The Development Strategy of Translational Research Based on China’s Current National SituationKerong Dai
one:
prefaces: 3 A Healthier Future for All Through
Enhanced China-U.S. Cooperation on Translational Medicine
Zhu Chen, Minister of Health, China
4 Report on 2011 Sino-American Symposium on Clinical and Translational Medicine
John I. Gallin, Director, NIH Clinical Center
5 A Developmental View: The Sino- American Symposium on Clinical and Translational Medicine
Tim Z. Shi, Executive Director, Global MD Organization
6 Fostering Collaboration and Cooperation
Alan Leshner, CEO, AAAS
Drug Development and Innovative Research: The Principles of Clinical Trials
62 How to Optimize Personalized Medicine R&D and Commercialization Decision-MakingSean Xinghua Hu, Edward Abrahams
64 Ethnic Differences in Genetic Polymorphism in Asian Populations Should Not be Neglected in Clinical Trials Yu Cheng, Wei Zhang, Cheng-Xian Guo, et al.
66 Antibody-Based Biopharmaceuticals and Translational Research Zhi-Nan Chen
68 Biochips for Translational Medicine Jing Cheng
nine:
2
This booklet was produced by the Science/AAAS Custom Publishing Office and sponsored by GlobalMD. Materials that appear in this booklet were commissioned, edited, and published by the Science/AAAS Custom Publishing Office and were not reviewed or assessed by Science Editorial staff. Articles can be cited using the following format [AUTHOR NAME(S)] in Selected Presentations from the 2011 Sino-American Symposium on Clinical and Translational Medicine, S. Sanders Ed. (Science/AAAS, Washington, DC, 2011), pp. [xx-xx].
Editor: Sean Sanders, Ph.D.; Design: Amy Hardcastle; Proofing: Yuse Lajiminmuhip
© 2011 by The American Association for the Advancement of Science. All rights reserved. 23 December 2011
Cerebro- and Cardiovascular Diseases: Collaborations Between Basic and Clinical Studies
38 Advanced Rescue for Acute Ischemic Stroke Feng Ling, Peng Gao
40 The NIH NHLBI/UHG Centers of Excellence: A Model for International CollaborationCristina Rabadan-Diehl
five:
Infectious Diseases: From Basic to Clinical Translational Medical Research
42 ExploringDifficult-to-TreatChronicHepatitis B Patients: From Bench to BedsideQin Ning, Meifang Han, Tao Chen, et al.
44 AIDS Vaccine Research, from Basic Research to Clinical StudyYiming Shao, Ying Liu, Jing Xu, et al.
46 Strategy and Practice of Translational Medicine in Therapeutic VaccinesYu-Mei Wen, Zheng-hong Yuan, Xuan-Yi Wang
48 Perspectives from an Investigational Site on Global Trials in China—Building Up Clinical Research Platforms for Chronic Liver Disease Mao Yimin
six:
Neurological System Diseases: Clinical and Translational Research
50 Translational Magnetic Resonance Imaging Research of Mental DisordersQiyong Gong, Qizhu Wu, Andrea Mechelli, et al.
51 Suicide Screening in Children and Adolescents in the Clinical and Research Setting Maryland Pao
53 Reprogrammed Astrocytes as a Potential Therapy for Neurodegenerative DisordersChanghai Tian, Jialin C. Zheng
seven:
Regenerative Medicine and Stem Cell Therapeutics: Basic and Clinical Research
55 Translating Stem Cell Research into Patient Care: Hype or Reality?Yufang Shi, Xiaodong Chen, Liying Zhang, et al.
56 Histone Methylation and MicroRNA-Mediated Regulation of the Multipotential State of Flk1+ Mesenchymal Stem CellsHongling Li, Jianhe Chen, Qin Han, et al.
58 Translational Research and the Treatment of Skin Wounds in China Xiaobing Fu
60 Autologous Cell Therapy for Tendon Tissue Reconstruction Ming H. Zheng, Gerard Hardisty, William Breidahl, et al.
eight:
Table of Contents
ACKNOWLEDGMENTS:Special thanks to co-organizers of the 2011 Sino-American Symposium on Clinical and Translational Medicine: the Chinese Academy of Engineering, the Chinese Academy of Medical Sciences, the U.S. NIH Clinical Center, and the Global MD Organization. Thanks to Johnson & Johnson Medical (Shanghai) Ltd. for their partial sponsorship of this booklet.

3
preface:
A Healthier Future for All Through Enhanced China-U.S. Cooperation on Translational Medicine
On June 24 this year, scientists, physicians, and officers from the United States and China gathered
in Shanghai for the 2011 Sino-American Symposium on Clinical and Translational Medicine.
The per capita expenditure on health in China is much less than that in the United States, and the two nations’ health care systems are quite different. However, both countries face the same challenge: To meet the growing health needs and ex-pectations of their citizens, while facing an increasingly restrictive financing environ-ment. We think that translational medicine is one of the best solutions to tackle this challenge.
Thanks to the efforts of the journal Science and the Global MD Organization (GlobalMD), the ideas and recommenda-tions of the participants in the clinical and translational medicine symposium can be presented in this special supplement. The content covers all phases of translational medicine, including policy and decision-making related to capacity and formation of a “constraint-free” environment, synergism
of collaborations and partnerships between all stakeholders, examples of successful translational research on different specific diseases and within a variety of disciplines, and the commercialization of different prod-ucts. Also discussed is the development of translational medicine over the next 5 to 10 years and what measures will be effective in breaking through the major barriers be-tween basic research and clinical applica-tion as well as how best to foster interna-tional cooperation.
This is the second Sino-American Sym-posium on Clinical and Translational Medi-cine. I believe the timely and close coop-eration and exchange between colleagues from China and the United States will pro-mote the development of translational med-icine not only in our two countries, but also in other parts of the world. I sincerely hope that the U.S.-Sino cooperation on clinical and translational medicine soon will bring about true results and make lasting contri-butions to the healthy future of the world.
Zhu Chen, Ph.D. Minister of Health, China
4
preface:
Report on 2011 Sino- American Symposium on Clinical and Translational Medicine
I was honored to co-chair the first two Sino-American Symposia on Clinical and Translational Medicine. The first
was held in Beijing, in June 2010, and the second in Shanghai, in June 2011. Both symposia illustrated the potential for bring-ing investigators from China and the United States together to pursue opportunities for new partnerships. At these sessions it was clear that the Chinese are committed to im-proving their clinical research infrastructure and becoming leaders in the international clinical research community. This commit-ment was demonstrated by attendance of Chinese leaders, including the Minister of Health, Dr. Zhu Chen (see preface on page 3); joint co-sponsorship by the Chinese Academy of Engineering and the Chinese Academy of Medical Sciences; and partici-pation by leaders and translational investi-gators from many Chinese hospitals and academic institutions.
The United States had representatives from the National Institutes of Health, the Food and Drug Administration, and senior investigators from the National Academy of Sciences and Institute of Medicine. Many participants came from American universi-ties, academic medical centers, industry, and non-profit organizations. The relatively new U.S. Society of Clinical and Transla-tional Sciences was also well represented by its membership and the first two Presi-dents of the Society, Dr. Barry Coller and Dr. Harry Selker. The first Lasker Founda-
tion Chinese lecture, which paired Lasker Laureate Dr. Brian Druker from the United States and Dr. Sijuan Chen from China, featured exciting presentations of the latest approaches to treating chronic myeloid leu-kemia. The Lasker lecture was followed by vibrant open discussion with young Chinese investigators led by Dr. Zhu Chen.
It has been gratifying to witness the re-cent progress made by the Chinese scien-tific community in translational research. The quality of science, as reflected by the articles in this supplement to Science, is first rate. I was very impressed by the prog-ress in training clinical investigators (see article by Ognibene et al. on page 8) and to learn that in 2011, the first accreditation of a Chinese hospital by the Association for the Accreditation of Human Research Pro-tection Programs was awarded to Beijing’s YouAn Hospital led by Dr. Ning Li. The sec-ond Sino-American Symposium on Clinical and Translational Medicine was a significant step in promoting Chinese and U.S. part-nerships, as highlighted in this supplement. The shared hope is that these partnerships will lead to better and faster discoveries to improve human health and serve as exam-ples of how to build academic partnerships across the world.
John I. Gallin, M.D.Director of the NIH Clinical Center Bethesda, MD, USA [email protected]

5
preface:
A Developmental View: The Sino-American Symposium on Clinical and Translational Medicine (SAS-CTM)
This symposium is a seed, planted in fertile ground and having all of the environmental conditions needed
to grow and flourish. The Sino-American Symposium (SAS) was born of both a need and a vision. As a unique initiative to pro-mote scientific collaboration on clinical and translational medicine, its timing was pre-cise, the participants committed, and the growth strong. Like a child, her develop-ment is continuing.
A simple idea to develop an event to facilitate sharing and communication of expertise among the U.S. and Chinese health care practitioners and researchers, the SAS-CTM came about quite naturally. GlobalMD had been active in bringing the National Institutes of Health (NIH) Clinical Center-designed courses on the principles and practice of clinical research to China. As the cadre of trained persons grew, the need arose to find a way to further promote true international collaborations that would permit a global vision for fighting deadly diseases together.
Since this idea coincided with the mis-sion of GlobalMD “to improve global health care through professional development, re-search and collaboration without borders,” we pursued and developed possibilities for organizing an international symposium. With generous support and encouragement from individual physicians, researchers, and health care leaders, as well as respected academicians, institutions, universities, and government agencies, SAS became a real-ity. We have begun to build up a virtual plat-form for effective and meaningful communi-cation between health care practitioners and
researchers in the United States, China, and around the globe, focusing on clinical and translational medicine.
We have seen that Sino-American col-laboration encourages each party to capi-talize on the strengths of the other, the United States with advanced biomedical knowledge and technological resources, and China with its fast economic growth, large research capacity, and vast resources in the biomedicine field. SAS is continu-ally expanding ways of learning and acting within its remit: To motivate scientists and researchers to collaborate. We now have a venue to share multidisciplinary work; to break through the fences and walls created by social ideologies, and to cross borders in the scientific quest so as to provide benefits to both the researchers and the societies in which they live.
Recently, the final flight of the Space Shuttle Atlantis marked not only the end of the 30-year historic space shuttle program in the United States, but also a milestone for humankind as this revolutionary space transportation program came to a close. Similarly, progress in the development of SAS leads us to believe that, 10 years from now, this symposium will play a significant role in both biomedical science and health care driven by translational sciences. Work-ing together, globally, we can anticipate the many positive outcomes that will result from the powerful creativity brought together and harnessed for the future of medicine.
Tim Z. Shi, M.D., Ph.D.Executive Director for Global MD Organization (GlobalMD)
6
preface:
Fostering Collaboration and Cooperation
The efforts to advance Sino-American collaboration in clinical and trans-lational research described in this
booklet reflect both great needs and great opportunities. As we all know, far too many patients throughout the world are suffering from a wide array of seemingly intractable diseases, both infectious and noncommu-nicable. Moreover, fragmented health care systems and high costs for medical care and medications make these problems even more daunting.
To even partially address these problems, clinicians and other treatment providers are in dire need of greater understanding of the pathophysiology of disorders as well as new prevention and treatment approaches based on that understanding. Leaders of pharmaceutical and biotechnology indus-tries are also calling for new therapeutic targets that would increase the effective-ness and accelerate the pace of medication development.
Meeting global medical needs also re-quires a broadening and strengthening of the clinical and translational science com-munity of scholars. There are far too few individuals trained as physician-scientists, and the system for producing them is cum-bersome and very time consuming, both for the trainees and their mentors. The situa-tion with translational science is particularly
worrisome, since there are no established best practices for training physician scien-tists in this relatively newly emerging phase of the research continuum. Training trans-lational scientists is particularly complex because they need grounding in both basic science and clinical research. That combina-tion can require long training periods, which often is a disincentive for younger scientists eager to establish laboratories of their own. Hopefully, combining the lessons learned in training programs in the United States and China will yield new and better training para-digms and protocols that can help expand the number of high quality individuals work-ing in this domain.
The ultimate goal, of course, is to produce the best translational science, but we have few best practice paradigms for achiev-ing this. Fortunately, both the American and Chinese clinical and translational re-search enterprises are gaining experience and improving the quality of their work all the time. Combining United States and Chi-nese efforts in collaborative partnerships, as reflected in this collection, will surely yield more and better outcomes than either alone.
Alan Leshner, Ph.D.CEO, AAASExecutive Publisher, Science
sec t ion one 7sect ion one
In past three decades, China’s average annual growth in gross do-mestic product (GDP) has remained above 9%, which is considered as an economic miracle in the history of the mankind. In mid-2010, China became the second largest economy in the world (1). The
sustained growth of revenue has allowed the Chinese government to be more self-confident and rational in its policymaking, and China has started to place more emphasis on the transformation of the economic growth mode and put substantial investment into social services, in-cluding health.
China’s new round of health care reform was initiated in 2009 (2). The Chinese government decided, despite the global financial crisis, to invest 850 billion RMB ($133 billion) in health, in addition to the regu-lar annual budget for government health expenditure (3). In past two years, the basic health insurance systems have been extended to cover 1.27 billion people, or 94.8% of the population, and the out-of pocket health expenditure for individuals was cut to 35.5% (4); a pilot reform project was launched in public hospitals in 17 cities and 300 county public hospitals; 1,877 county hospitals, 5,169 central township health centers, and 2,382 community health centers have been refurbished; and two million health professionals have been trained. The collection of 15% commission on prescription drug costs is no longer being prac-ticed in the government-run primary health care system, and 307 drugs regarded as national essential medicines are now available in all grass-roots-level institutions. Access to basic public health services has been improved, nine categories of basic programs were implemented, and eight major programs were 100% completed for 2010 (5). The progress of health reform is impressive, but the medical safety net is still limited compared with some countries that have similar GDP per capita (6).
Closing the gap between the increasing challenges of population health, rising public expectations, and relatively stringent financing has yet to be achieved in any country. Along with the fast economic growth in China, comes rapid urbanization and aging of the population. The epidemiological and demographic transitions lead to a complex health burden: Emerging infectious diseases in tandem with rising chronic, noncommunicable diseases (NCDs) and mental illness, as well as phys-ical injuries, affect all age groups. In a rapid changing world, even “pri-mary health care for all” (7) seems a mission impossible if we cannot find a solution to fill the above mentioned gap. I believe that science and technology, coupled with evidence-based policymaking, are key to finding the solution and that translational medicine in particular must play a major role in health care reform.
The concept of translational medicine was first proposed by the U.S. National Institutes of Health (NIH). Described as bi-directional, “B(ench) to B(edside)” is regarded as the natural progression from evidence-based medicine, and is the process of turning appropriate biological discoveries into medical technologies (including drugs, vac-cine, and devices) that can be used in the treatment of patients and the prevention of diseases (8). It integrates research from the basic scienc-es, social sciences, and political sciences with the aim of optimizing people’s health. Promotion of translational medicine will streamline the
translation of basic discoveries into new diagnostics, treatments, and cures. Therefore, it will also foster an innovative and competitive bio-medical industry, which will accrue the double benefit of alleviating the nation’s health burden while also stimulating revenue growth.
With its large population, diversified disease spectrum, and ex-perience in both Western medicine and traditional Chinese medicine (TCM), China is in a uniquely advantageous position to develop translational medicine. The recent surge in research—China is ranked world number two in the number of papers published, second only to the United States (9)—provides unprecedented opportunities for ac-celerating translational research. The Chinese government has made a political commitment to further increase the investment in health care reform and foster innovation. By 2015, the proportion of R&D funding will increase to 2.2% of GDP, and the government will further promote health-related science and technology—making translational medicine the centerpiece—and continue to strengthen capacity in key disciplines in order to speed up health care reform.
The expansion of translational medicine in China—a developing country—must include key elements inspired by the reform of the health care system. First, translational research should benefit the ma-jority of people, not just a small minority. Second, the emphasis of the research should be on both public health (prevention and health promo-tion) and on diagnosis and treatment of disease. Third, in view of the challenges of NCDs, the future focus for the application of translational medicine should be in the community.
In China, there is no health research organization with an equivalent role to the NIH. Therefore, it would be preferable to form a network of translational medicine centers. Among these centers, two geographic focal points are worth mentioning: One center was founded by Peking Union Medical University and another by Shanghai Jiaotong Universi-ty School of Medicine/Shanghai Ruijin Hospital. The two centers have their unique expertise in the three phases of translational medicine, but will play similar roles as local conveners, catalysts, and common resources for collaborative interactions and partnerships. Both centers currently pay more attention to the fostering of complex talents and capacity building. I’d like to suggest that more emphasis should be placed on the study of translational medicine–related policy and health resources management so that they may serve as think-tanks to enhance the support to the central and local authorities in developing robust pol-icies, strategies, and plans.
Guided by the concept of “cure a disease before its onset” estab-lished long ago in TCM, China’s translational medicine efforts will put more emphasis on public health. One of the major tasks should be the prevention of, and intervention in, NCDs. Dozens of interven-tion networks will be implemented nationwide and rooted in commu-nities. The government will continue to increase access to the public health services.
It is clearly stated in the National 12th Five-Year Plan (2011–2015) that, by 2015, China should significantly reduce the disparity in health care and increase the average life expectancy by one year (estimated to
Def ining the Vision and Strategies for Collaboration: Institutional and International
National Plan on Translational Medicine in China: Promoting Health Care Reform and Improving People’s HealthZhu Chen, Ph.D. Minister of Health, China
sect ion one
8
reach 74.5 years old) relative to that of 2010. The governmental invest-ment in health care reform will be ensured and will grow steadily. Inter-national collaborations and partnerships will be warmly welcomed, and I believe the results of translational medicine research and application will promote health care reform and improve people’s health not only in China but also in other countries.
REFERENCES 1. D. Barboza, “China Passes Japan as Second-Largest Economy”
(The New York Times, New York, 2010; http://www.nytimes.com/2010/08/16/business/global/16yuan.html).
2. Y. Yuan, G. C. Jiang, “China unveils health-care reform guidelines” (Xinhua News Agency, Beijing, 2009; http://news.xinhuanet.com/english/2009-04/06/content_11138643.htm).
3. J. B. WEN, “Report on the Work of the Government” (People’s Publishing House, Beijing, 2009; http://www.china.org.cn/government/NPC_CPPCC_2009/2009-03/13/content_17440331.htm).
4. J. Shan, “China ramps up healthcare spending” (China Daily, Beijing, 2011; http://www.chinadaily.com.cn/bizchina/2011-03/10/content_12151446.htm).
5. “Assessment Report on the National Human Rights Action Plan of China (2009–2010)” (Information Office of the State Council, Beijing, 2011; http://www.gov.cn/english/official/2009-04/13/content_1284128.htm).
6. “Global Health Observatory Data Repository” (WHO, 2011; http://apps.who.int/ghodata/).
7. “The World Health Report 2008 - primary Health Care (Now More Than Ever)” (WHO, 2008; http://www.who.int/whr/2008/en/index.html).
8. F. M. Marincola, Translational Medicine: A two-way road. J. Transl. Med. 1, 1 (2003).
9. “Knowledge, Networks and Nations” (The Royal Society, 2011; http://royalsociety.org/uploadedfiles/royal_society_content/influencing_policy/reports/2011-03-28-knowledge-networks-nations.pdf).
In order for clinical research to be carried out efficiently and ef-fectively, members of clinical research teams need the knowledge, skills, and experience to safely and ethically conduct the highest quality research. Historically, there has been little formal education
in clinical research for U.S. medical students, more advanced physician trainees, or other research team members (1, 2). Such training depended on mentors sharing their knowledge and experience. However, clini-cal trials have become more complex, training in clinical research is more sophisticated, and the scope of research networks has evolved to include universities, academic centers and privately funded entities, community-based practitioners, and those conducting clinical research internationally.
Advances in information technology have led to significant oppor-tunities for analyzing massive amounts of data. Additionally, ethical and regulatory concerns are critical, and there is an expectation of ac-countability among researchers, absolute transparency in our processes, and a commitment to patient/research subject safety and privacy. These are critical issues affecting the global clinical research enterprise, and as such, contemporary approaches to teaching how to conduct clinical research are necessary (3).
In 1995, the National Institutes of Health Clinical Center (NIH CC) recognized that formal training in clinical research was essential. A series of three courses was developed and comprised the core curriculum in clinical research at the Clinical Center (4, 5). These courses are taught
locally and are also available via long-distance learning around the world. Archived lectures are available online, and abbreviated versions of the three courses have been taught in live formats internationally. Distance learning and academic collaborations with centers around the world have allowed access both by individuals and by institutions that do not have well-developed curricula in clinical research.
The first course in the core curriculum, “Introduction to the Prin-ciples and Practice of Clinical Research,” was established in 1995 and provides content ranging from trial design to ethical and regu-latory issues. Participants learn how to design a successful clini-cal trial focusing on epidemiologic methods, study design, protocol preparation, patient monitoring, quality assurance, FDA regula-tions, data management, and ethical issues. Since its inception the course has been offered to over 11,000 students, with 50% at long-distance sites in 23 countries on five continents. An accompanying textbook, Principles and Practice of Clinical Research, is used for the course (6).
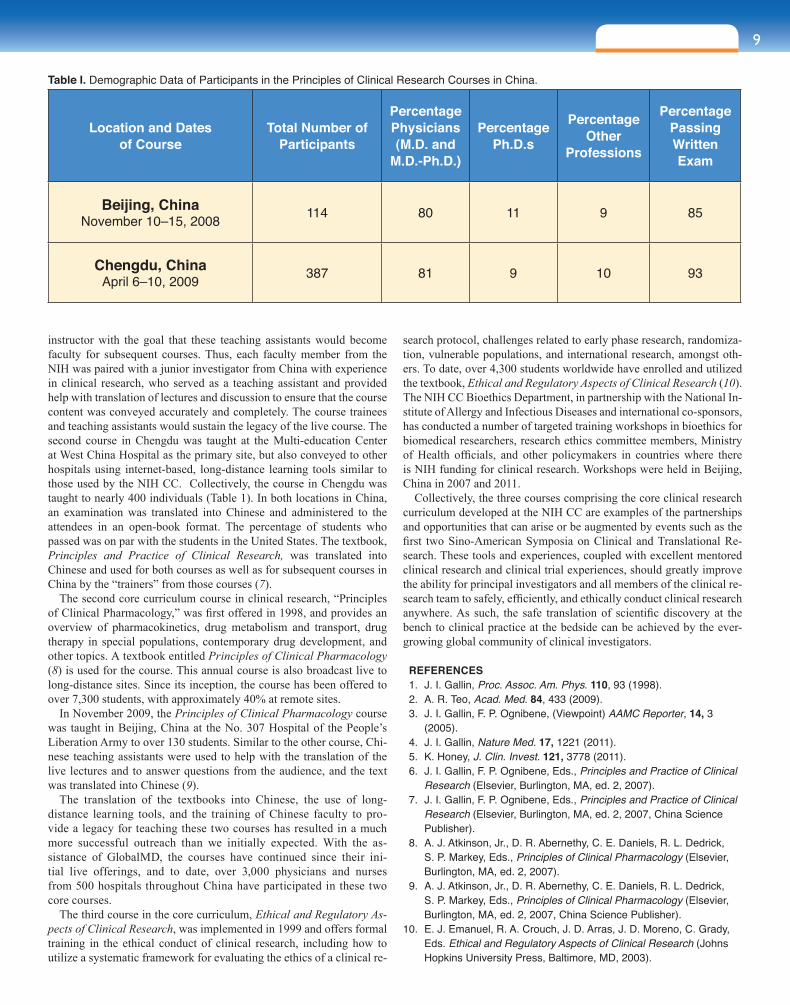
Two modified live versions of the course have been taught in China. The first was in Beijing in November 2008 and the second in Chengdu in April 2009, both in partnership with the not-for-profit Global MD Organization. It was evident that our Chinese colleagues not only wanted the content of the course, but they were eager to ensure that there would be a legacy and some sustainability for the course materials. In Beijing, the course was taught at Peking Capital Medical University to 114 trainees from a number of hospitals in Beijing who agreed to not only use the knowledge gained to enhance their clinical research skills, but also convey that knowledge to their hospital colleagues (Table 1). It was a model designed to “train the trainer.” The NIH CC course leaders insisted that a Chinese teaching assistant work with each
1National Institutes of Health Clinical Center, Bethesda, MD, USA2Global MD Organization Network Corp (GlobalMD), Catonsville, MD, USA*Corresponding Author: [email protected]
Global Outreach in Clinical Research by the NIH Clinical Center: Building Training Partnerships with ChinaFrederick P. Ognibene, M.D.1, Tim Z. Shi, M.D., Ph.D.2, and John I. Gallin, M.D.1,*
9sect ion one
instructor with the goal that these teaching assistants would become faculty for subsequent courses. Thus, each faculty member from the NIH was paired with a junior investigator from China with experience in clinical research, who served as a teaching assistant and provided help with translation of lectures and discussion to ensure that the course content was conveyed accurately and completely. The course trainees and teaching assistants would sustain the legacy of the live course. The second course in Chengdu was taught at the Multi-education Center at West China Hospital as the primary site, but also conveyed to other hospitals using internet-based, long-distance learning tools similar to those used by the NIH CC. Collectively, the course in Chengdu was taught to nearly 400 individuals (Table 1). In both locations in China, an examination was translated into Chinese and administered to the attendees in an open-book format. The percentage of students who passed was on par with the students in the United States. The textbook, Principles and Practice of Clinical Research, was translated into Chinese and used for both courses as well as for subsequent courses in China by the “trainers” from those courses (7).
The second core curriculum course in clinical research, “Principles of Clinical Pharmacology,” was first offered in 1998, and provides an overview of pharmacokinetics, drug metabolism and transport, drug therapy in special populations, contemporary drug development, and other topics. A textbook entitled Principles of Clinical Pharmacology (8) is used for the course. This annual course is also broadcast live to long-distance sites. Since its inception, the course has been offered to over 7,300 students, with approximately 40% at remote sites.
In November 2009, the Principles of Clinical Pharmacology course was taught in Beijing, China at the No. 307 Hospital of the People’s Liberation Army to over 130 students. Similar to the other course, Chi-nese teaching assistants were used to help with the translation of the live lectures and to answer questions from the audience, and the text was translated into Chinese (9).
The translation of the textbooks into Chinese, the use of long-distance learning tools, and the training of Chinese faculty to pro-vide a legacy for teaching these two courses has resulted in a much more successful outreach than we initially expected. With the as-sistance of GlobalMD, the courses have continued since their ini-tial live offerings, and to date, over 3,000 physicians and nurses from 500 hospitals throughout China have participated in these two core courses.
The third course in the core curriculum, Ethical and Regulatory As-pects of Clinical Research, was implemented in 1999 and offers formal training in the ethical conduct of clinical research, including how to utilize a systematic framework for evaluating the ethics of a clinical re-
search protocol, challenges related to early phase research, randomiza-tion, vulnerable populations, and international research, amongst oth-ers. To date, over 4,300 students worldwide have enrolled and utilized the textbook, Ethical and Regulatory Aspects of Clinical Research (10). The NIH CC Bioethics Department, in partnership with the National In-stitute of Allergy and Infectious Diseases and international co-sponsors, has conducted a number of targeted training workshops in bioethics for biomedical researchers, research ethics committee members, Ministry of Health officials, and other policymakers in countries where there is NIH funding for clinical research. Workshops were held in Beijing, China in 2007 and 2011.
Collectively, the three courses comprising the core clinical research curriculum developed at the NIH CC are examples of the partnerships and opportunities that can arise or be augmented by events such as the first two Sino-American Symposia on Clinical and Translational Re-search. These tools and experiences, coupled with excellent mentored clinical research and clinical trial experiences, should greatly improve the ability for principal investigators and all members of the clinical re-search team to safely, efficiently, and ethically conduct clinical research anywhere. As such, the safe translation of scientific discovery at the bench to clinical practice at the bedside can be achieved by the ever-growing global community of clinical investigators.
REFERENCES 1. J. I. Gallin, Proc. Assoc. Am. Phys. 110, 93 (1998). 2. A. R. Teo, Acad. Med. 84, 433 (2009). 3. J. I. Gallin, F. P. Ognibene, (Viewpoint) AAMC Reporter, 14, 3
(2005). 4. J. I. Gallin, Nature Med. 17, 1221 (2011). 5. K. Honey, J. Clin. Invest. 121, 3778 (2011). 6. J. I. Gallin, F. P. Ognibene, Eds., Principles and Practice of Clinical
Research (Elsevier, Burlington, MA, ed. 2, 2007). 7. J. I. Gallin, F. P. Ognibene, Eds., Principles and Practice of Clinical
Research (Elsevier, Burlington, MA, ed. 2, 2007, China Science Publisher).
8. A. J. Atkinson, Jr., D. R. Abernethy, C. E. Daniels, R. L. Dedrick, S. P. Markey, Eds., Principles of Clinical Pharmacology (Elsevier, Burlington, MA, ed. 2, 2007).
9. A. J. Atkinson, Jr., D. R. Abernethy, C. E. Daniels, R. L. Dedrick, S. P. Markey, Eds., Principles of Clinical Pharmacology (Elsevier, Burlington, MA, ed. 2, 2007, China Science Publisher).
10. E. J. Emanuel, R. A. Crouch, J. D. Arras, J. D. Moreno, C. Grady, Eds. Ethical and Regulatory Aspects of Clinical Research (Johns Hopkins University Press, Baltimore, MD, 2003).
Table I. Demographic Data of Participants in the Principles of Clinical Research Courses in China.
Location and Dates of Course
Total Number of Participants
Percentage Physicians (M.D. and
M.D.-Ph.D.)
Percentage Ph.D.s
Percentage Other
Professions
Percentage Passing Written Exam
Beijing, China November 10–15, 2008 114 80 11 9 85
Chengdu, ChinaApril 6–10, 2009 387 81 9 10 93
10
Platelets play a crucial role in hemostasis by adher-ing to damaged endo-thelium (adhesion) and
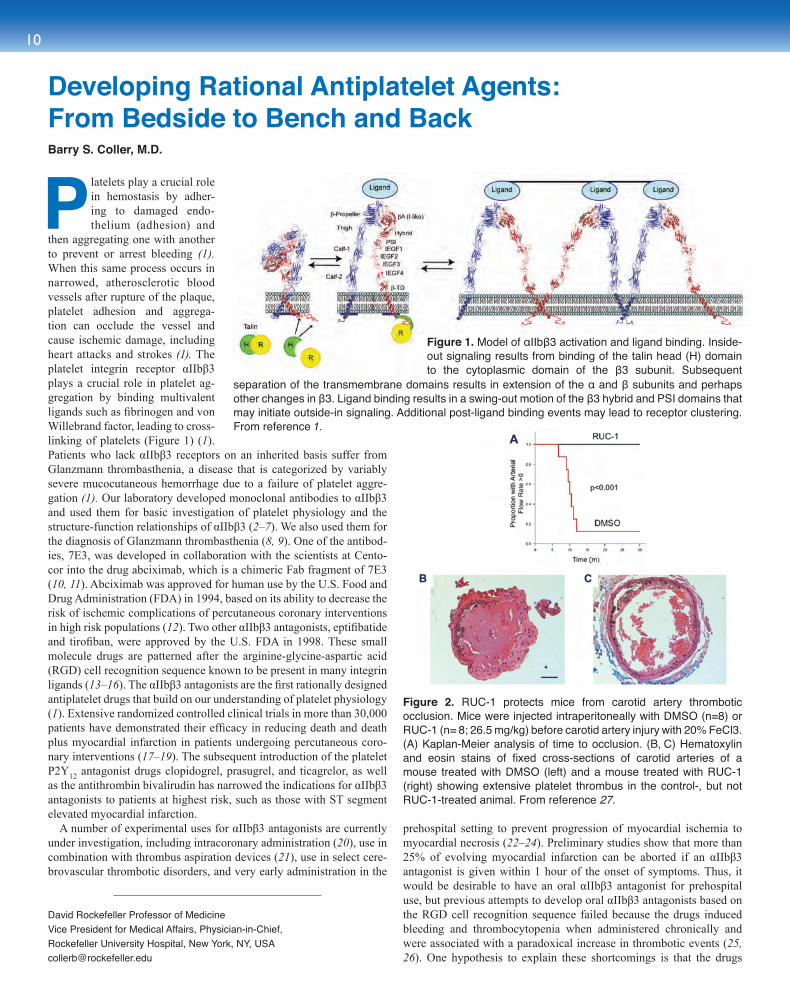
then aggregating one with another to prevent or arrest bleeding (1). When this same process occurs in narrowed, atherosclerotic blood vessels after rupture of the plaque, platelet adhesion and aggrega-tion can occlude the vessel and cause ischemic damage, including heart attacks and strokes (1). The platelet integrin receptor αIIbβ3 plays a crucial role in platelet ag-gregation by binding multivalent ligands such as fibrinogen and von Willebrand factor, leading to cross-linking of platelets (Figure 1) (1). Patients who lack αIIbβ3 receptors on an inherited basis suffer from Glanzmann thrombasthenia, a disease that is categorized by variably severe mucocutaneous hemorrhage due to a failure of platelet aggre-gation (1). Our laboratory developed monoclonal antibodies to αIIbβ3 and used them for basic investigation of platelet physiology and the structure-function relationships of αIIbβ3 (2–7). We also used them for the diagnosis of Glanzmann thrombasthenia (8, 9). One of the antibod-ies, 7E3, was developed in collaboration with the scientists at Cento-cor into the drug abciximab, which is a chimeric Fab fragment of 7E3 (10, 11). Abciximab was approved for human use by the U.S. Food and Drug Administration (FDA) in 1994, based on its ability to decrease the risk of ischemic complications of percutaneous coronary interventions in high risk populations (12). Two other αIIbβ3 antagonists, eptifibatide and tirofiban, were approved by the U.S. FDA in 1998. These small molecule drugs are patterned after the arginine-glycine-aspartic acid (RGD) cell recognition sequence known to be present in many integrin ligands (13–16). The αIIbβ3 antagonists are the first rationally designed antiplatelet drugs that build on our understanding of platelet physiology (1). Extensive randomized controlled clinical trials in more than 30,000 patients have demonstrated their efficacy in reducing death and death plus myocardial infarction in patients undergoing percutaneous coro-nary interventions (17–19). The subsequent introduction of the platelet P2Y12 antagonist drugs clopidogrel, prasugrel, and ticagrelor, as well as the antithrombin bivalirudin has narrowed the indications for αIIbβ3 antagonists to patients at highest risk, such as those with ST segment elevated myocardial infarction.
A number of experimental uses for αIIbβ3 antagonists are currently under investigation, including intracoronary administration (20), use in combination with thrombus aspiration devices (21), use in select cere-brovascular thrombotic disorders, and very early administration in the
prehospital setting to prevent progression of myocardial ischemia to myocardial necrosis (22–24). Preliminary studies show that more than 25% of evolving myocardial infarction can be aborted if an αIIbβ3 antagonist is given within 1 hour of the onset of symptoms. Thus, it would be desirable to have an oral αIIbβ3 antagonist for prehospital use, but previous attempts to develop oral αIIbβ3 antagonists based on the RGD cell recognition sequence failed because the drugs induced bleeding and thrombocytopenia when administered chronically and were associated with a paradoxical increase in thrombotic events (25, 26). One hypothesis to explain these shortcomings is that the drugs
Developing Rational Antiplatelet Agents: From Bedside to Bench and BackBarry S. Coller, M.D.
David Rockefeller Professor of MedicineVice President for Medical Affairs, Physician-in-Chief, Rockefeller University Hospital, New York, NY, [email protected]
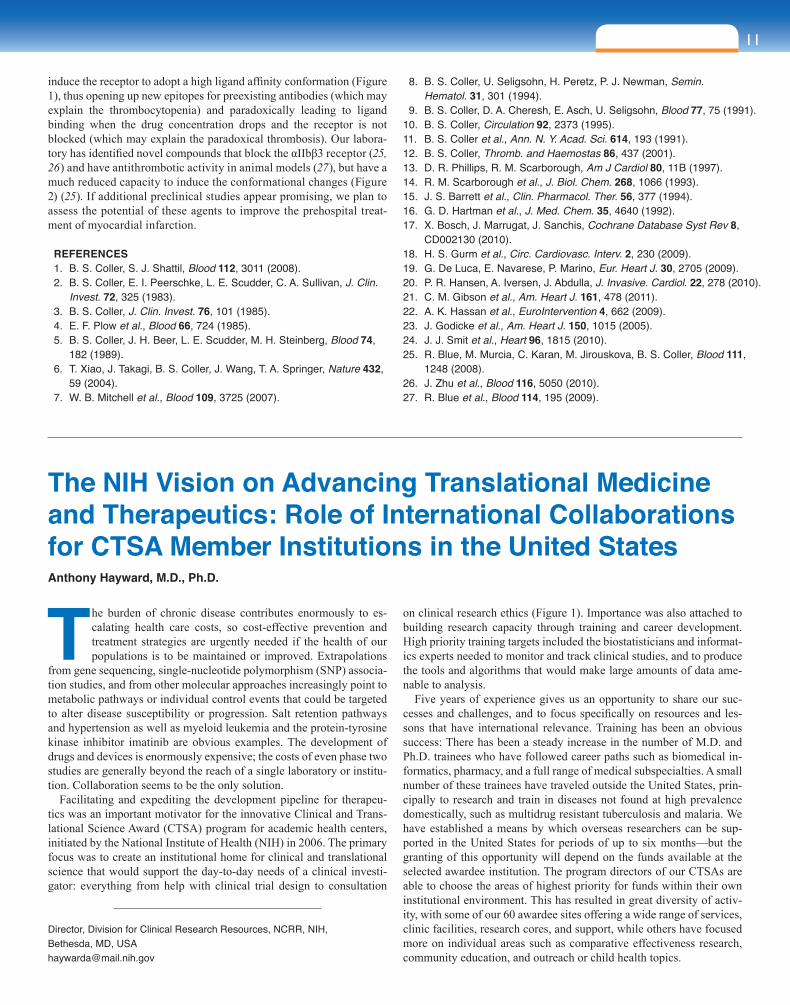
Figure 2. RUC-1 protects mice from carotid artery thrombotic occlusion. Mice were injected intraperitoneally with DMSO (n=8) or RUC-1 (n= 8; 26.5 mg/kg) before carotid artery injury with 20% FeCl3. (A) Kaplan-Meier analysis of time to occlusion. (B, C) Hematoxylin and eosin stains of fixed cross-sections of carotid arteries of a mouse treated with DMSO (left) and a mouse treated with RUC-1 (right) showing extensive platelet thrombus in the control-, but not RUC-1-treated animal. From reference 27.
Figure 1. Model of αIIbβ3 activation and ligand binding. Inside-out signaling results from binding of the talin head (H) domain to the cytoplasmic domain of the β3 subunit. Subsequent
separation of the transmembrane domains results in extension of the α and β subunits and perhaps other changes in β3. Ligand binding results in a swing-out motion of the β3 hybrid and PSI domains that may initiate outside-in signaling. Additional post-ligand binding events may lead to receptor clustering. From reference 1.
11sect ion one
The burden of chronic disease contributes enormously to es-calating health care costs, so cost-effective prevention and treatment strategies are urgently needed if the health of our populations is to be maintained or improved. Extrapolations
from gene sequencing, single-nucleotide polymorphism (SNP) associa-tion studies, and from other molecular approaches increasingly point to metabolic pathways or individual control events that could be targeted to alter disease susceptibility or progression. Salt retention pathways and hypertension as well as myeloid leukemia and the protein-tyrosine kinase inhibitor imatinib are obvious examples. The development of drugs and devices is enormously expensive; the costs of even phase two studies are generally beyond the reach of a single laboratory or institu-tion. Collaboration seems to be the only solution.
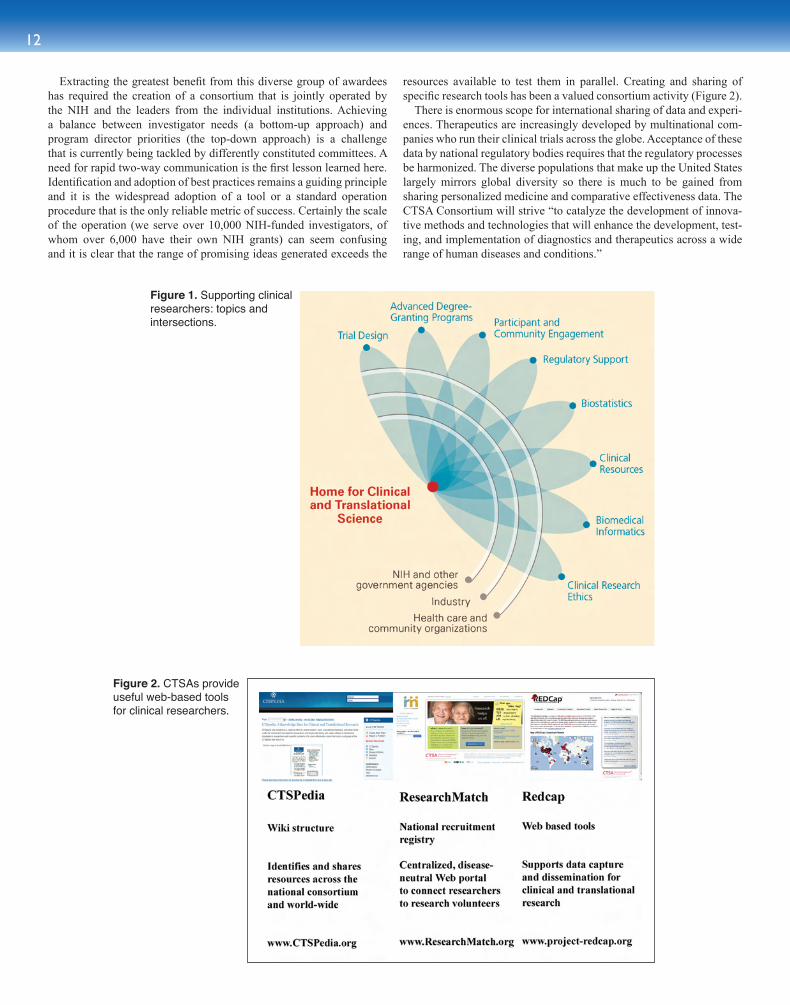
Facilitating and expediting the development pipeline for therapeu-tics was an important motivator for the innovative Clinical and Trans-lational Science Award (CTSA) program for academic health centers, initiated by the National Institute of Health (NIH) in 2006. The primary focus was to create an institutional home for clinical and translational science that would support the day-to-day needs of a clinical investi-gator: everything from help with clinical trial design to consultation
on clinical research ethics (Figure 1). Importance was also attached to building research capacity through training and career development. High priority training targets included the biostatisticians and informat-ics experts needed to monitor and track clinical studies, and to produce the tools and algorithms that would make large amounts of data ame-nable to analysis.
Five years of experience gives us an opportunity to share our suc-cesses and challenges, and to focus specifically on resources and les-sons that have international relevance. Training has been an obvious success: There has been a steady increase in the number of M.D. and Ph.D. trainees who have followed career paths such as biomedical in-formatics, pharmacy, and a full range of medical subspecialties. A small number of these trainees have traveled outside the United States, prin-cipally to research and train in diseases not found at high prevalence domestically, such as multidrug resistant tuberculosis and malaria. We have established a means by which overseas researchers can be sup-ported in the United States for periods of up to six months—but the granting of this opportunity will depend on the funds available at the selected awardee institution. The program directors of our CTSAs are able to choose the areas of highest priority for funds within their own institutional environment. This has resulted in great diversity of activ-ity, with some of our 60 awardee sites offering a wide range of services, clinic facilities, research cores, and support, while others have focused more on individual areas such as comparative effectiveness research, community education, and outreach or child health topics.
The NIH Vision on Advancing Translational Medicine and Therapeutics: Role of International Collaborations for CTSA Member Institutions in the United StatesAnthony Hayward, M.D., Ph.D.
Director, Division for Clinical Research Resources, NCRR, NIH, Bethesda, MD, [email protected]
induce the receptor to adopt a high ligand affinity conformation (Figure 1), thus opening up new epitopes for preexisting antibodies (which may explain the thrombocytopenia) and paradoxically leading to ligand binding when the drug concentration drops and the receptor is not blocked (which may explain the paradoxical thrombosis). Our labora-tory has identified novel compounds that block the αIIbβ3 receptor (25, 26) and have antithrombotic activity in animal models (27), but have a much reduced capacity to induce the conformational changes (Figure 2) (25). If additional preclinical studies appear promising, we plan to assess the potential of these agents to improve the prehospital treat-ment of myocardial infarction.
REFERENCES 1. B. S. Coller, S. J. Shattil, Blood 112, 3011 (2008). 2. B. S. Coller, E. I. Peerschke, L. E. Scudder, C. A. Sullivan, J. Clin.
Invest. 72, 325 (1983). 3. B. S. Coller, J. Clin. Invest. 76, 101 (1985). 4. E. F. Plow et al., Blood 66, 724 (1985). 5. B. S. Coller, J. H. Beer, L. E. Scudder, M. H. Steinberg, Blood 74,
182 (1989). 6. T. Xiao, J. Takagi, B. S. Coller, J. Wang, T. A. Springer, Nature 432,
59 (2004). 7. W. B. Mitchell et al., Blood 109, 3725 (2007).
8. B. S. Coller, U. Seligsohn, H. Peretz, P. J. Newman, Semin. Hematol. 31, 301 (1994).
9. B. S. Coller, D. A. Cheresh, E. Asch, U. Seligsohn, Blood 77, 75 (1991).10. B. S. Coller, Circulation 92, 2373 (1995).11. B. S. Coller et al., Ann. N. Y. Acad. Sci. 614, 193 (1991).12. B. S. Coller, Thromb. and Haemostas 86, 437 (2001).13. D. R. Phillips, R. M. Scarborough, Am J Cardiol 80, 11B (1997).14. R. M. Scarborough et al., J. Biol. Chem. 268, 1066 (1993).15. J. S. Barrett et al., Clin. Pharmacol. Ther. 56, 377 (1994).16. G. D. Hartman et al., J. Med. Chem. 35, 4640 (1992).17. X. Bosch, J. Marrugat, J. Sanchis, Cochrane Database Syst Rev 8,
CD002130 (2010).18. H. S. Gurm et al., Circ. Cardiovasc. Interv. 2, 230 (2009).19. G. De Luca, E. Navarese, P. Marino, Eur. Heart J. 30, 2705 (2009).20. P. R. Hansen, A. Iversen, J. Abdulla, J. Invasive. Cardiol. 22, 278 (2010).21. C. M. Gibson et al., Am. Heart J. 161, 478 (2011).22. A. K. Hassan et al., EuroIntervention 4, 662 (2009).23. J. Godicke et al., Am. Heart J. 150, 1015 (2005).24. J. J. Smit et al., Heart 96, 1815 (2010).25. R. Blue, M. Murcia, C. Karan, M. Jirouskova, B. S. Coller, Blood 111,
1248 (2008).26. J. Zhu et al., Blood 116, 5050 (2010).27. R. Blue et al., Blood 114, 195 (2009).
12
Extracting the greatest benefit from this diverse group of awardees has required the creation of a consortium that is jointly operated by the NIH and the leaders from the individual institutions. Achieving a balance between investigator needs (a bottom-up approach) and program director priorities (the top-down approach) is a challenge that is currently being tackled by differently constituted committees. A need for rapid two-way communication is the first lesson learned here. Identification and adoption of best practices remains a guiding principle and it is the widespread adoption of a tool or a standard operation procedure that is the only reliable metric of success. Certainly the scale of the operation (we serve over 10,000 NIH-funded investigators, of whom over 6,000 have their own NIH grants) can seem confusing and it is clear that the range of promising ideas generated exceeds the
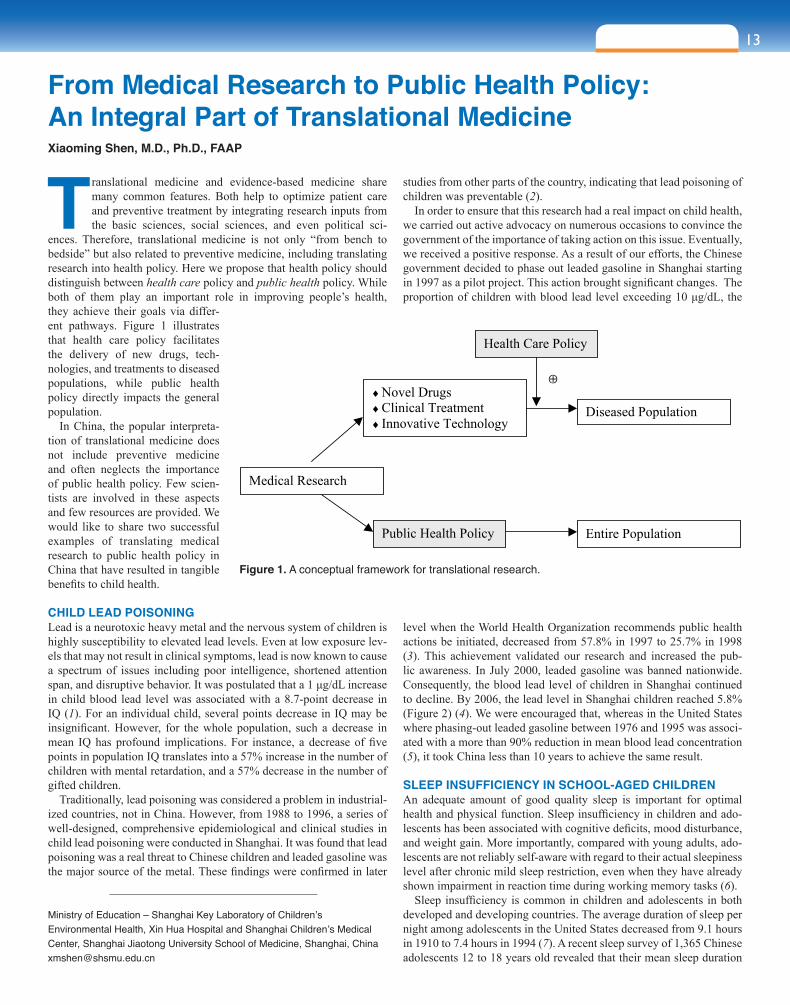
resources available to test them in parallel. Creating and sharing of specific research tools has been a valued consortium activity (Figure 2).
There is enormous scope for international sharing of data and experi-ences. Therapeutics are increasingly developed by multinational com-panies who run their clinical trials across the globe. Acceptance of these data by national regulatory bodies requires that the regulatory processes be harmonized. The diverse populations that make up the United States largely mirrors global diversity so there is much to be gained from sharing personalized medicine and comparative effectiveness data. The CTSA Consortium will strive “to catalyze the development of innova-tive methods and technologies that will enhance the development, test-ing, and implementation of diagnostics and therapeutics across a wide range of human diseases and conditions.”
Figure 2. CTSAs provide useful web-based tools for clinical researchers.
Figure 1. Supporting clinical researchers: topics and intersections.
13sect ion one
Translational medicine and evidence-based medicine share many common features. Both help to optimize patient care and preventive treatment by integrating research inputs from the basic sciences, social sciences, and even political sci-
ences. Therefore, translational medicine is not only “from bench to bedside” but also related to preventive medicine, including translating research into health policy. Here we propose that health policy should distinguish between health care policy and public health policy. While both of them play an important role in improving people’s health, they achieve their goals via differ-ent pathways. Figure 1 illustrates that health care policy facilitates the delivery of new drugs, tech-nologies, and treatments to diseased populations, while public health policy directly impacts the general population.
In China, the popular interpreta-tion of translational medicine does not include preventive medicine and often neglects the importance of public health policy. Few scien-tists are involved in these aspects and few resources are provided. We would like to share two successful examples of translating medical research to public health policy in China that have resulted in tangible benefits to child health.
CHILD LEAD POISONINGLead is a neurotoxic heavy metal and the nervous system of children is highly susceptibility to elevated lead levels. Even at low exposure lev-els that may not result in clinical symptoms, lead is now known to cause a spectrum of issues including poor intelligence, shortened attention span, and disruptive behavior. It was postulated that a 1 μg/dL increase in child blood lead level was associated with a 8.7-point decrease in IQ (1). For an individual child, several points decrease in IQ may be insignificant. However, for the whole population, such a decrease in mean IQ has profound implications. For instance, a decrease of five points in population IQ translates into a 57% increase in the number of children with mental retardation, and a 57% decrease in the number of gifted children.
Traditionally, lead poisoning was considered a problem in industrial-ized countries, not in China. However, from 1988 to 1996, a series of well-designed, comprehensive epidemiological and clinical studies in child lead poisoning were conducted in Shanghai. It was found that lead poisoning was a real threat to Chinese children and leaded gasoline was the major source of the metal. These findings were confirmed in later
studies from other parts of the country, indicating that lead poisoning of children was preventable (2).
In order to ensure that this research had a real impact on child health, we carried out active advocacy on numerous occasions to convince the government of the importance of taking action on this issue. Eventually, we received a positive response. As a result of our efforts, the Chinese government decided to phase out leaded gasoline in Shanghai starting in 1997 as a pilot project. This action brought significant changes. The proportion of children with blood lead level exceeding 10 μg/dL, the
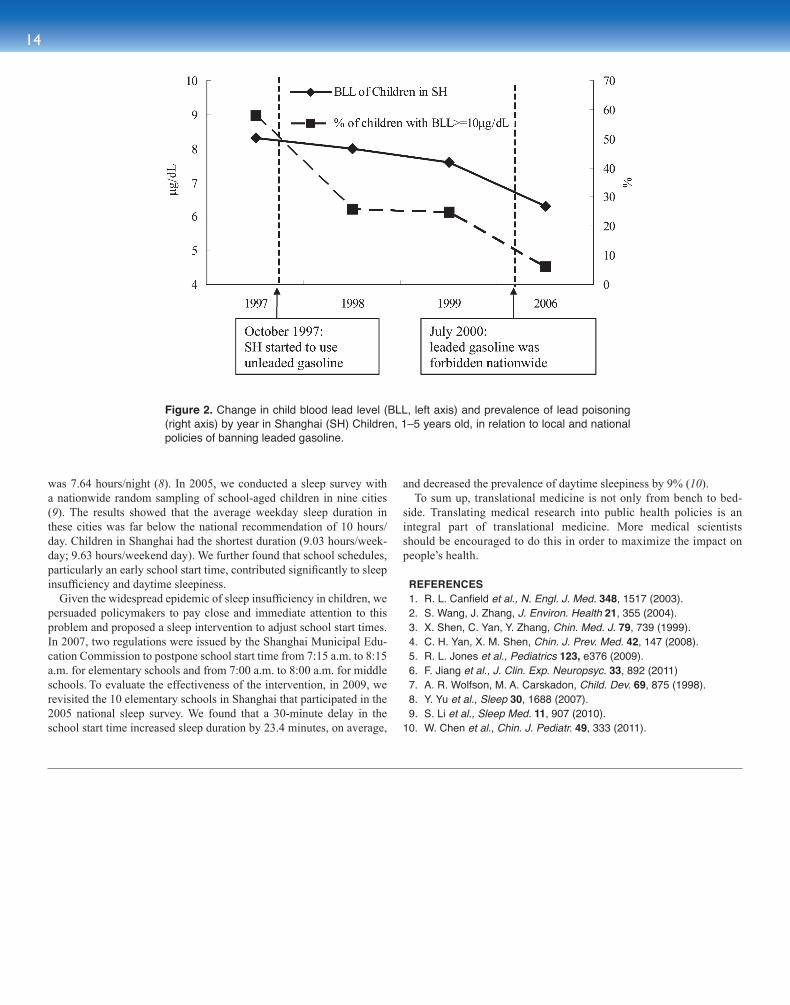
level when the World Health Organization recommends public health actions be initiated, decreased from 57.8% in 1997 to 25.7% in 1998 (3). This achievement validated our research and increased the pub-lic awareness. In July 2000, leaded gasoline was banned nationwide. Consequently, the blood lead level of children in Shanghai continued to decline. By 2006, the lead level in Shanghai children reached 5.8% (Figure 2) (4). We were encouraged that, whereas in the United States where phasing-out leaded gasoline between 1976 and 1995 was associ-ated with a more than 90% reduction in mean blood lead concentration (5), it took China less than 10 years to achieve the same result.
SLEEP INSUFFICIENCY IN SCHOOL-AGED CHILDRENAn adequate amount of good quality sleep is important for optimal health and physical function. Sleep insufficiency in children and ado-lescents has been associated with cognitive deficits, mood disturbance, and weight gain. More importantly, compared with young adults, ado-lescents are not reliably self-aware with regard to their actual sleepiness level after chronic mild sleep restriction, even when they have already shown impairment in reaction time during working memory tasks (6).
Sleep insufficiency is common in children and adolescents in both developed and developing countries. The average duration of sleep per night among adolescents in the United States decreased from 9.1 hours in 1910 to 7.4 hours in 1994 (7). A recent sleep survey of 1,365 Chinese adolescents 12 to 18 years old revealed that their mean sleep duration
6
Legends:
Figure 1. A conceptual framework for translational research
Figure 2. Change in child blood lead level (BLL, left axis) and prevalence of lead
poisoning (right axis) by year in Shanghai (SH) Children, 1-5 years old, in relation to
local and national policies of banning leaded gasoline.
Health Care Policy
Diseased Population
Medical Research
♦ Novel Drugs
♦ Clinical Treatment
♦ Innovative Technology
Public Health Policy Entire Population
From Medical Research to Public Health Policy: An Integral Part of Translational MedicineXiaoming Shen, M.D., Ph.D., FAAP
Ministry of Education – Shanghai Key Laboratory of Children’s Environmental Health, Xin Hua Hospital and Shanghai Children’s Medical Center, Shanghai Jiaotong University School of Medicine, Shanghai, [email protected]
Figure 1. A conceptual framework for translational research.
14
was 7.64 hours/night (8). In 2005, we conducted a sleep survey with a nationwide random sampling of school-aged children in nine cities (9). The results showed that the average weekday sleep duration in these cities was far below the national recommendation of 10 hours/day. Children in Shanghai had the shortest duration (9.03 hours/week-day; 9.63 hours/weekend day). We further found that school schedules, particularly an early school start time, contributed significantly to sleep insufficiency and daytime sleepiness.
Given the widespread epidemic of sleep insufficiency in children, we persuaded policymakers to pay close and immediate attention to this problem and proposed a sleep intervention to adjust school start times. In 2007, two regulations were issued by the Shanghai Municipal Edu-cation Commission to postpone school start time from 7:15 a.m. to 8:15 a.m. for elementary schools and from 7:00 a.m. to 8:00 a.m. for middle schools. To evaluate the effectiveness of the intervention, in 2009, we revisited the 10 elementary schools in Shanghai that participated in the 2005 national sleep survey. We found that a 30-minute delay in the school start time increased sleep duration by 23.4 minutes, on average,
and decreased the prevalence of daytime sleepiness by 9% (10). To sum up, translational medicine is not only from bench to bed-
side. Translating medical research into public health policies is an integral part of translational medicine. More medical scientists should be encouraged to do this in order to maximize the impact on people’s health.
REFERENCES 1. R. L. Canfield et al., N. Engl. J. Med. 348, 1517 (2003). 2. S. Wang, J. Zhang, J. Environ. Health 21, 355 (2004). 3. X. Shen, C. Yan, Y. Zhang, Chin. Med. J. 79, 739 (1999). 4. C. H. Yan, X. M. Shen, Chin. J. Prev. Med. 42, 147 (2008). 5. R. L. Jones et al., Pediatrics 123, e376 (2009). 6. F. Jiang et al., J. Clin. Exp. Neuropsyc. 33, 892 (2011) 7. A. R. Wolfson, M. A. Carskadon, Child. Dev. 69, 875 (1998). 8. Y. Yu et al., Sleep 30, 1688 (2007). 9. S. Li et al., Sleep Med. 11, 907 (2010).10. W. Chen et al., Chin. J. Pediatr. 49, 333 (2011).
Figure 2. Change in child blood lead level (BLL, left axis) and prevalence of lead poisoning (right axis) by year in Shanghai (SH) Children, 1–5 years old, in relation to local and national policies of banning leaded gasoline.
15sect ion one
Starting in 2006, translational research centers began to spon-taneously appear in China. Since 2009, more and more have been set up. In 2009, nine new centers were built, while in 2010, another 16 were established, and in only the first six
months of 2011, nine more were founded. Geographically, these cen-ters are located mainly in Shanghai (14), Beijing (5), Shenzhen (3), and other large cities in southeastern China. The translational research centers are mostly led by university hospitals (or medical colleges) and universities, which account for 39% and 32% of the total, respectively. 26% of them are led by research institutions, while only one is headed by private enterprise. The research carried out at these centers includes the fields of stem cells, regenerative medicine, drug discovery, cancer, orthopedics, cardiovascular disease, pediatrics, and diabetes. These centers have already achieved a certain level of academic proficiency within the research fields above, and have favorable research and clini-cal infrastructure.
There is a huge gap between basic research and clinical applica-tion, which urgently needs to be bridged. Based on data from PubMed, those papers published by Chinese researchers related to stem cell re-search have increased rapidly in recent years. The number of the papers indexed by the Science Citation Index exceeded 1,000 in 2007, and reached 2,085 in 2010. But there is still no national standard for the regulation of stem cell isolation, purification, or amplification. Com-pared with the United States and Europe, there are some bottlenecks in the development of translational research in China, such as lack of macroplanning within government, flawed systems of policies and reg-ulations, lack of professionals with experience in essential disciplines, and lack of knowledge and mechanisms necessary for translation of important research. Additionally, interdisciplinary integration is not sufficiently robust. Take, for example, the patent situation in Shanghai Ninth People’s Hospital: Eighty-two patents were approved between 2005 and 2009 by the Department of Orthopaedics, Plastic Surgery, and Stomatology. As of the start of 2011, only 7% of them had realized clinical translation.
Based on the current situation in China, the national development strategies for translational research should emphasize the establishment of overall strategies, multidisciplinary integration, the shift of transla-tional mode, project appraisal and approval as well as the training of professionals in translational research.
Currently, translational centers are founded mostly independently by provinces, cities, or universities. Although they take advantage of their research strengths, improvements in certain aspects like policy support and guidance, funding support, and resource shar-ing are still needed. These will depend on the establishment of ro-bust and overarching national development strategies for transla- tional research.
Interdisciplinary integration is the motivation for translational re-search. In the United States, for example, 46 translational centers fund-ed by the CTSA had integrated 738 cooperative institutions of multi-disciplinary research by 2011. China does not require such extensive integration, however. A fewer participants and research collaboration on a smaller scale will likely be better for establishing effective coop-eration and coordination in the country.
In China, the most common practice is to commit to the process of translating the research only after the basic research has already been completed, and then starting patent applications, preclinical animal studies, clinical trials, enterprise partner searches, production and med-ical license applications, and finally moving to clinical applications. The main shortcoming of this process is that it is passive and arbitrary: The translation decisions are made after the discovery. By this time, researchers are already involved in new research projects, and may be put off by the low chance of successful translation to the clinic. A better approach in China, particularly because there are many translational research centers led by hospitals or medical colleges, is an active mod-el: Formulating clinical issues and patient requirements into scientific projects, forming multidisciplinary research programs to solve these challenges, and at the same time starting the translational proposal. This model will attract the interest of industry partners involved in the clinical trial process at the very beginning of the study. With a clearer purpose and goal, efficiency will be improved.
Appraisal and approval of these projects are essential. At the start of a project, a comprehensive evaluation should be carried out to avoid wasting valuable resources. Risk assessment, the significance of the clinical application, maturity and stability of the technology, and diffi-culties of clinical promotion should all be considered. In addition, intel-lectual property protection should be strengthened.
Those carrying out translational research should be familiar with the development trends of basic research as well as the urgent clinical is-sues to be addressed, related technologies, and policies and regulations. They should also have knowledge of statistics, epidemiology, ethics, economics, clinical trials, and potential legal issues. Many Chinese researchers and clinical staff lack this knowhow, but through the es-tablishment of a sound education system and a well-planned training program, this deficit can be addressed.
The Development Strategy of Translational Research Based on China’s Current National SituationKerong Dai, M.D.
Ninth People’s Hospital, Shanghai Jiao Tong University School of MedicineClinical Translational Center of Stem Cell and Regenerative Medicine, Shanghai, [email protected]

16
Since the beginning of this century, translational medicine has been paid more attention and has become a reemerging hot topic in medicine. Both the changing practice of medicine and health care reform have contributed to the rapid development
of translational medicine.Translational medicine is the bridge from the human genome to
predictive medicine, preventive medicine, personalized medicine, and participatory medicine (4P medicine). Genomic medicine and digital medicine are two of the main drivers in the transformation process from the genomics to 4P medicine.
GENOMIC MEDICINEGenomic medicine includes high-quality annotation of the human ge-nome, systems experimental analysis, and bioinformatics. This field will offer extensive insight into the relationship between genotype and phenotype—particularly the relationship of the functionally important genes and their variants to health and disease—and the dynamic net-works and mathematic models of disease initiation and progression.
In the past 10 years, annotation of human genome has advanced rap-idly. Genome-wide association studies (GWAS) and single-nucleotide polymorphism (SNP) research have identified many useful biomark-ers—more than 1,400 genes have been identified that are directly re-lated to disease. Discovery and validation of susceptibility genes offers encouraging signs that predictive and preventive medicine is possible.
Systems biology analysis is now focusing on “omics” research, pre-dominantly transcriptomics, proteomics, and metabolomics. The gen-eration and integration of multiomic data is key in biomarker discovery, dynamic network construction, and elucidation of the mechanism of disease development. Bioinformatics plays an important role in the data generation, integration, storage, processing, and in the translation of results from discovery to knowledge and the application of that knowl-edge for predictive medicine.
Elucidating the relationship between genotype and phenotype is a challenging task due to the multiple factors, besides just the DNA se-quence, that might affect phenotype. These factors include epigenetics, physiological state, lifestyle, and environment. In 1892, Sir William Osler wrote, “If it were not for the great variability among individuals, medicine might as well be a science and not an art.” The time is ripe to transform medicine from art to science. Addressing the heterogeneity in
both disease and patient requires personalized medicine: A personalized preventive strategy, personalized drugs, and personalized treatments will all benefit society.
The biggest challenge in translational medicine is how to rapidly and efficiently apply the knowledge and technology gained from research to the promotion of health and prevention of disease. Currently, the ap-plication of biomarkers in the clinic is slow and inefficient because of inadequate, or no, validation. It is important that both biological valida-tion and clinicopathological validation be performed. Only after these validation steps are complete can the biomarker under study be consid-ered for clinical application.
DIGITAL MEDICINEDigital medicine is a new strategy and engine of translational medicine, encompassing electronic health record keeping, mobile medical device use, hospital information systems, laboratory information systems, and nationwide medical information architecture. These systems and net-works connect patients, community health service centers, hospitals, remote clinics, and education centers to improve the quality and effi-ciency of health care. There are certain deficiencies in digital medicine, including a lack of data standards, slow data processing, limits for data storage, problems with information sharing policies, and lack of good infrastructure. However, mobile medical devices combined with wire-less communication systems have the ability to create a new medical paradigm and a cost-effective, efficient health care system. Diseases where constant monitoring or rapid treatment is critical will especially benefit, including asthma, diabetes, heart failure, hypertension, and sleep disorders.
In the past 10 years, translational medicine has clearly advanced quickly, with positive gains in predicting and preventing disease. Some examples include personalized drugs, gene chips for predicting drug metabolism and disease susceptibility, a synthetic retina generated from stem cells, engineered blood vessels, broad spectrum influenza vaccines, epidermal electronic sensors, implantable glucose sensors, and the artificial pancreas for treating diabetics. But most translational processes still remain an expensive, slow, and failure-prone endeavor and the expected breakthroughs in prevention and treatment methods have not been seen. Possibly it is still too early to expect such results, considering the relatively extended timeline for medical research and development.
As translational medicine advances, it promises to accelerate the process of applying what is learned from the genome to 4P medicine. The hope is that 4P medicine will be widely applied, making disease prevention, control, and treatment more effective. In the near future, translational medicine will be not just a dream with great potential, but rather a reality benefiting humankind and society.
Division of Medicine and Health, Chinese Academy of Engineering, Beijing, ChinaShanghai Institute of Biological Sciences, Chinese Academy of Sciences, Shanghai, [email protected]
From Genome to 4P MedicineShengli Yang, Ph.D.
Promoting Ef fective Communication and Enabling "Constraint" Research
sect ion two
17sect ion two
The National Center for Research Resources (NCRR) was founded in 1962 to provide shared research infrastructure resources to the research community. One of these programs supported the General Clinical Research Centers (GCRC),
a network of over sixty units at major academic centers throughout the United States. GCRCs were intended to provide highly trained research nursing services and hospital beds for clinical research studies that required specialized facilities or intensive protocols. These units functioned as the laboratories for clinical investigators, and their funding by NCRR could be seen as analogous to the support given basic investigators for their laboratories through indirect costs from National Institutes of Health (NIH) grants. Studies performed at GCRCs included not only NIH-funded studies but also pilot projects and industry-sponsored studies.
When the Clinical and Translation Science Awards (CTSA) were cre-ated in 2006, GCRCs were folded into that program. Currently, a CTSA site is not required to include one of these research units, although most CTSAs have retained them as so-called Clinical Services Cores (CSCs). Under the CTSA program, the units have also been given greater flex-ibility of mission, and many of the current CSCs include the capability to support studies throughout their parent medical centers as well as in the surrounding communities.
In a survey of these units conducted in 2010, it was found that they supported $1.6 billion annually in NIH-funded studies across a broad spectrum of areas that includes internal medicine, pediatrics, sur-gery, obstetrics and gynecology, and most or all of their subspecial-ties. It was estimated in this survey that, had the GCRC investigators instead been forced to pay bed and nursing charges for using stan-dard hospital beds, $200 to $300 million annually would have been added to the budgets of the supported NIH grants. Thus, the support of GCRCs was highly cost effective, if not actually cost saving, to the NIH.
The benefits of the GCRC/CSC program extend beyond cost effec-tiveness:
• Training: In 2010 CSCs supported approximately 700 NIH-funded pre- and postdoctoral trainees and approximately 200 CTSA Pilot Projects.
• Support of research networks and multicenter trials: In the survey described above, support of over 700 multicenter stud-ies and 32 collaborative networks was indicated, encompassing a variety of medical disciplines. The CSC network facilitates com-munication among such groups and helps ensure uniform stan-dards and strict protocol adherence.
• Ability to undertake highly complex studies: Complex disease phenotyping studies often include multiple diagnostic mo-dalities—functional imaging, complex infusions, and tissue and biospecimen sampling, for example—that are often performed
under stringent time constraints. Such studies essentially would be impossible without the dedicated space and specialized staff of a CSC. Many units include facilities that offer special support in the areas of nutrition, exercise, imaging, and others.
• Data reproducibility and precision: Another benefit that is difficult to quantify but is nonetheless generally accepted is that the units afford much greater reproducibility of research data than could be achieved if the studies were undertaken throughout a medical center and without the consistent supervision of a support staff that is familiar with the study and the special requirements of research studies in general.
• Safety: It is highly likely that the units increase research subject safety and are more attuned to maintaining research data confidentiality.
• Efficiency: Several CSCs are moving toward uniform and shared reviews of protocols for scientific validity and subject safety. As is the case for federated Institutional Review Boards, such review processes will hasten the completion of clinical trials.
Studies undertaken in these units have resulted in findings that have changed the practice of medicine. Numerous publications citing in-dispensable support by CSCs have appeared in recent years that have changed our understanding of human physiology and informed current state-of-the-art clinical care in nearly every specialty. A few examples of such studies illustrate their breadth and significance:
• Identification and importance of brown adipose tissue in adult hu-mans, a finding with significant implications for the understanding and treatment of obesity and diabetes (1);
• Demonstration of a reduction in long-term mortality after gastric bypass surgery (2);
• A series of studies from the ACCORD Study Group that define current optimal treatment for type 2 diabetes (3, 4);
• Discovery of a gene (SCN9A) that contributes to the risk of febrile seizures, one of many gene finding studies that made use of the CSCs for clinical phenotyping and that are providing the basis for rational therapy of diseases across the spectrum of medical specialties (5);
• Studies on genetic contributions to dementia (6);• Defining optimal treatment of chronic hepatitis C (7);• New approaches to the treatment of sickle cell disease (8);• Defining the appropriate treatment of gestational diabetes (9);• Treatment for locally advanced breast cancer (10);• Treatment of angiomyolipoma in tuberous sclerosis complex or
lymphangioleiomyomatosis (11);• Defining novel pathogenic features in cystic fibrosis that open the
door to potential new therapies (12);• Defining biomarkers for acute appendicitis to speed diagnosis and
prevent unnecessary surgery (13);• Defining biomarkers, pathogenesis, and therapeutic targets for
major depressive disorders (14);• Preexposure chemoprophylaxis for HIV prevention in men who
have sex with men (15).In addition to clinical research trials themselves, CSCs are also play-
ing a key role in “process engineering,” that is, changing the way those studies are designed and executed. As just one example, CSCs played a
Professor of Medicine and BiochemistryAssociate Vice President for Clinical ResearchDirector, Center for Clinical and Translational ScienceUniversity of Utah School of Medicine,Salt Lake City, UT, [email protected]
The Value of Dedicated Research Units to Reproducible Clinical InvestigationDonald A. McClain, M.D., Ph.D.

18
INTRODUCTIONClinical research using populations in different parts of the world pres-ents challenges in applying the principles and practices of research as well as in maintaining data quality (1–4). Multinational clinical re-search and drug trials conducted in China have increased substantially in recent years, with increasing amounts of data being collected and submitted to the U.S. Food Drug Administration (FDA) from these multisite trials and postmarketing surveys (5).
Since the majority of clinical research and trials are conducted by clinicians, the quality of their training is critical. However, medical education worldwide remains oriented towards managing patients and diseases (6). Little attention is given to understanding clinical research concepts and practices. Often, opportunities for formal courses and certification in clinical research are limited, and without recognized international standards, global sharing and cooperation will be more difficult (4).
GlobalMD identified a specific need for standardization in training, which could facilitate communication and collaboration across cultures and among the various sectors, including academia, health care servic-es, and bio-industry. Since 2008, professional development programs in China have been put in place to meet this need.
PROPOSED SOLUTIONS AND METHODSIt was realized that Chinese health care practitioners at local hospitals did not have easy access to advanced knowledge and systematic training opportunities in the international standards of clinical research. To address this issue, the U.S. National Institutes of Health Clinical Center (NIH CC) course on the principles and practice of clinical research (PPCR) was selected as a core training component
due to its professional acclaim and international validation (20,000 professionals certified globally since 1995) (7). The content was synthesized into a five-day intensive course. As additional needs were identified, courses in the Principles of Clinical Pharmacology (five days, 30 hours), and Bioethics (two days, 12 hours) were added.
A number of different teaching methods were used, including on-site lectures in China by NIH faculty, web-based courses through the website www.ChinaGlobalMD.cn, and scientific workshops on specific topics. Additionally, textbooks and lectures were translated into Chinese for self-study by trainees, and changes to the curriculum were made as needed. A combination of teaching methods proved most ef-fective and courses now include lectures, online videos, and group study sessions on specific issues as well as one-on-one mentoring.
PARTICIPANTSBetween 2008 and 2011, approximately 3,000 clinicians, researchers, and nurses from 500 hospitals and research institutions across China participated in the different clinical research training courses organized by GlobalMD, NIH CC, and leading hospitals in China.
Forty-eight percent of participants were clinicians, 28% were project assistants, and the remaining 24% were administrative staff, residents, or M.D. or Ph.D. candidates. The majority (76%) of par-ticipants have been directly involved in clinical research and/or drug trials in their daily practice. Their motivations for participa-tion were principally knowledge acquisition, career development, and promotion.
EVALUATION OF RESULTS Trainees took pre- and posttraining tests and an anonymous survey. A random sample follow-up survey was conducted after 18 months. While the pre- and posttraining examinations concentrated on what the train-ees knew, the surveys examined the impact of the classes on clinical re-search knowledge, skills, and abilities, as well as course design, and the usefulness of the lectures and training methodologies. Questionnaires
crucial role in the development of statistical tools to facilitate the analy-sis of gene sequence data to find disease-causing mutations among a large number of inconsequential sequence variants (16).
The CSCs are likely to continue to play a crucial role in transla-tional science. For example, the dawning era of “personalized medi-cine” will rely on these units for the complex physiologic phenotyping studies necessary for genotype/phenotype correlation and the discov-ery and testing of therapies tailored to those specific situations. Such studies would be difficult or even impossible in the usual clinic or hospital setting.
REFERENCES 1. A. M. Cypess et al., N. Engl. J. Med. 360, 1509 (2009). 2. T. D. Adams et al., N. Engl. J. Med. 357, 753 (2007).
3. G. Mancia, Circulation 122, 847 (2010). 4. M. C. Riddle, Circulation 122, 844 (2010). 5. N. A. Singh et al., PLoS Genet. 5, e1000649 (2009). 6. A. E. Sanders et al., JAMA 303, 150 (2010). 7. A. M. Di Bisceglie et al., N. Engl. J. Med. 359, 2429 (2008). 8. G. F. Atweh et al., Blood 93, 1790 (1999). 9. M. B. Landon et al., N. Engl. J. Med. 361, 1339 (2009).10. J. Baar et al., Clin. Cancer Res. 15, 3583 (2009).11. J. J. Bissler et al., N. Engl. J. Med. 358, 140 (2008).12. M. Makam et al., Proc. Natl. Acad. Sci. U.S.A. 106, 5779 (2009).13. A. Kentsis et al., Ann. Emerg. Med. 55, 62 (2010).14. V. Vaccarino et al., Biol. Psychiatry 64, 476 (2008).15. R. M. Grant et al., N. Engl. J. Med. 363, 2587 (2010).16. A. F. Rope et al., Am. J. Hum. Genet. 89, 28 (2011).
Development of a Training Program for Physicians and Researchers to Advance Global Standardization in Clinical ResearchTim Z. Shi, M.D., Ph.D.1,*, Carol B. Collado, R.N., Ph.D.1, Xiaokun Liang, R.N., Ph.D.2, Fei Fei, M.D.2, and Xiaolei Zhao, M.PH.2
1Global MD Organization Network Corp (GlobalMD), Catonsville, MD, USA2Global MD (China office), Beijing, China*Corresponding Author: [email protected]
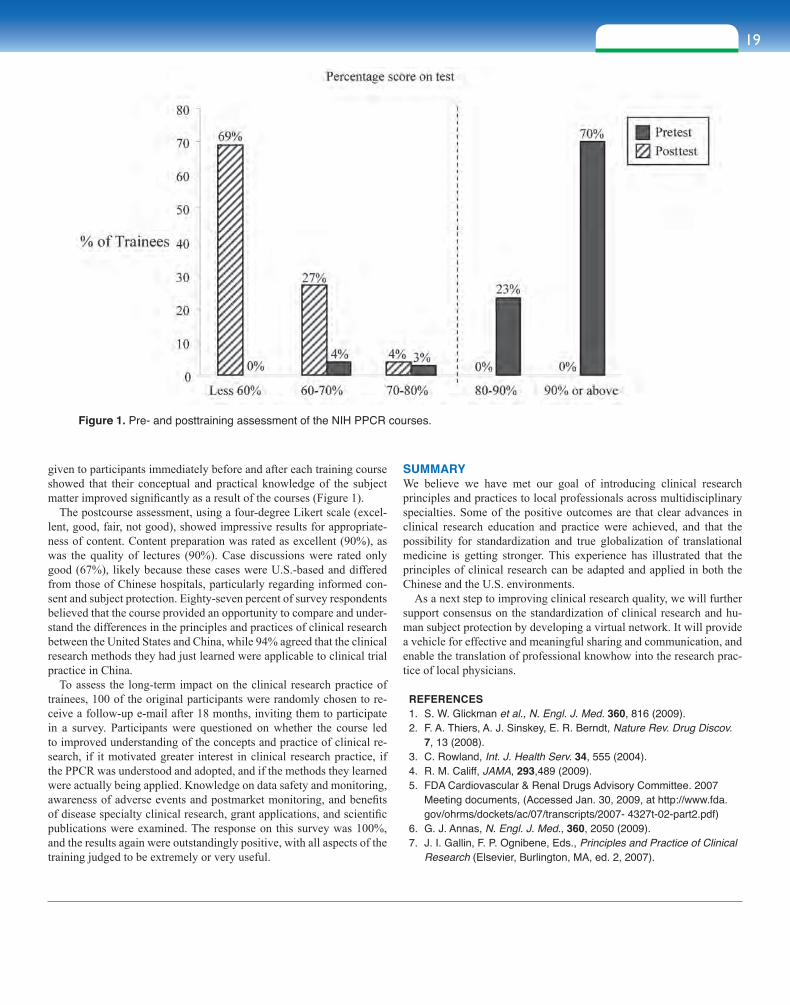
19sect ion two
given to participants immediately before and after each training course showed that their conceptual and practical knowledge of the subject matter improved significantly as a result of the courses (Figure 1).
The postcourse assessment, using a four-degree Likert scale (excel-lent, good, fair, not good), showed impressive results for appropriate-ness of content. Content preparation was rated as excellent (90%), as was the quality of lectures (90%). Case discussions were rated only good (67%), likely because these cases were U.S.-based and differed from those of Chinese hospitals, particularly regarding informed con-sent and subject protection. Eighty-seven percent of survey respondents believed that the course provided an opportunity to compare and under-stand the differences in the principles and practices of clinical research between the United States and China, while 94% agreed that the clinical research methods they had just learned were applicable to clinical trial practice in China.
To assess the long-term impact on the clinical research practice of trainees, 100 of the original participants were randomly chosen to re-ceive a follow-up e-mail after 18 months, inviting them to participate in a survey. Participants were questioned on whether the course led to improved understanding of the concepts and practice of clinical re-search, if it motivated greater interest in clinical research practice, if the PPCR was understood and adopted, and if the methods they learned were actually being applied. Knowledge on data safety and monitoring, awareness of adverse events and postmarket monitoring, and benefits of disease specialty clinical research, grant applications, and scientific publications were examined. The response on this survey was 100%, and the results again were outstandingly positive, with all aspects of the training judged to be extremely or very useful.
SUMMARYWe believe we have met our goal of introducing clinical research principles and practices to local professionals across multidisciplinary specialties. Some of the positive outcomes are that clear advances in clinical research education and practice were achieved, and that the possibility for standardization and true globalization of translational medicine is getting stronger. This experience has illustrated that the principles of clinical research can be adapted and applied in both the Chinese and the U.S. environments.
As a next step to improving clinical research quality, we will further support consensus on the standardization of clinical research and hu-man subject protection by developing a virtual network. It will provide a vehicle for effective and meaningful sharing and communication, and enable the translation of professional knowhow into the research prac-tice of local physicians.
REFERENCES 1. S. W. Glickman et al., N. Engl. J. Med. 360, 816 (2009). 2. F. A. Thiers, A. J. Sinskey, E. R. Berndt, Nature Rev. Drug Discov.
7, 13 (2008). 3. C. Rowland, Int. J. Health Serv. 34, 555 (2004). 4. R. M. Califf, JAMA, 293,489 (2009). 5. FDA Cardiovascular & Renal Drugs Advisory Committee. 2007
Meeting documents, (Accessed Jan. 30, 2009, at http://www.fda.gov/ohrms/dockets/ac/07/transcripts/2007- 4327t-02-part2.pdf)
6. G. J. Annas, N. Engl. J. Med., 360, 2050 (2009). 7. J. I. Gallin, F. P. Ognibene, Eds., Principles and Practice of Clinical
Research (Elsevier, Burlington, MA, ed. 2, 2007).
Figure 1. Pre- and posttraining assessment of the NIH PPCR courses.
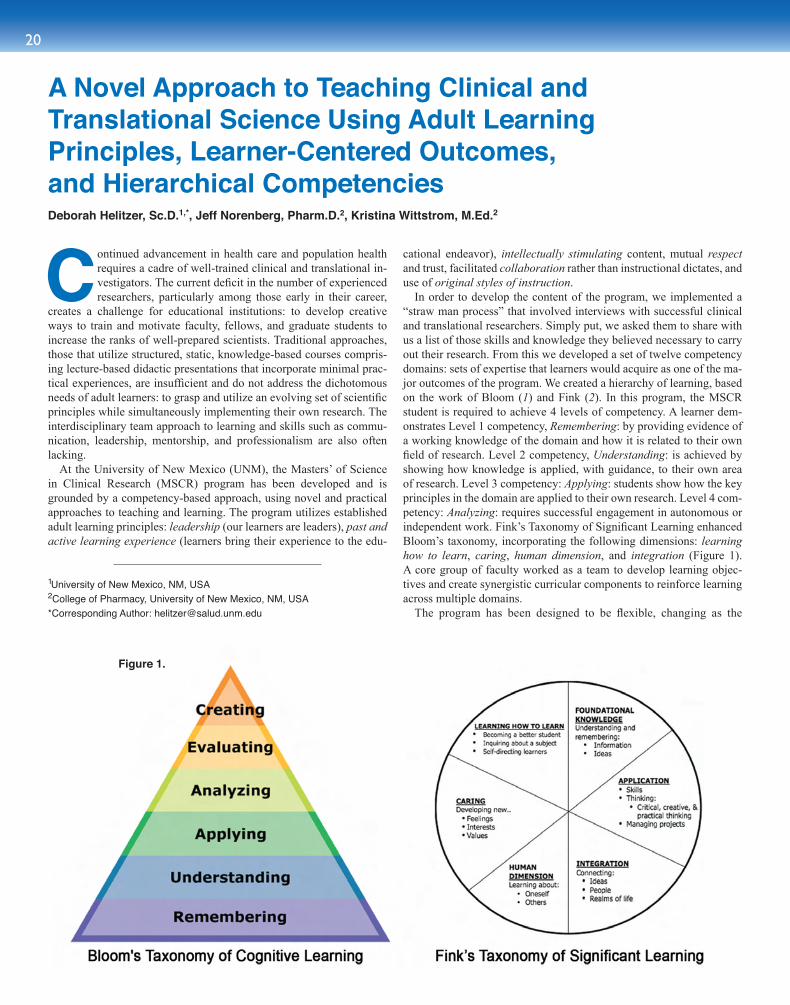
20
Continued advancement in health care and population health requires a cadre of well-trained clinical and translational in-vestigators. The current deficit in the number of experienced researchers, particularly among those early in their career,
creates a challenge for educational institutions: to develop creative ways to train and motivate faculty, fellows, and graduate students to increase the ranks of well-prepared scientists. Traditional approaches, those that utilize structured, static, knowledge-based courses compris-ing lecture-based didactic presentations that incorporate minimal prac-tical experiences, are insufficient and do not address the dichotomous needs of adult learners: to grasp and utilize an evolving set of scientific principles while simultaneously implementing their own research. The interdisciplinary team approach to learning and skills such as commu-nication, leadership, mentorship, and professionalism are also often lacking.
At the University of New Mexico (UNM), the Masters’ of Science in Clinical Research (MSCR) program has been developed and is grounded by a competency-based approach, using novel and practical approaches to teaching and learning. The program utilizes established adult learning principles: leadership (our learners are leaders), past and active learning experience (learners bring their experience to the edu-
cational endeavor), intellectually stimulating content, mutual respect and trust, facilitated collaboration rather than instructional dictates, and use of original styles of instruction.
In order to develop the content of the program, we implemented a “straw man process” that involved interviews with successful clinical and translational researchers. Simply put, we asked them to share with us a list of those skills and knowledge they believed necessary to carry out their research. From this we developed a set of twelve competency domains: sets of expertise that learners would acquire as one of the ma-jor outcomes of the program. We created a hierarchy of learning, based on the work of Bloom (1) and Fink (2). In this program, the MSCR student is required to achieve 4 levels of competency. A learner dem-onstrates Level 1 competency, Remembering: by providing evidence of a working knowledge of the domain and how it is related to their own field of research. Level 2 competency, Understanding: is achieved by showing how knowledge is applied, with guidance, to their own area of research. Level 3 competency: Applying: students show how the key principles in the domain are applied to their own research. Level 4 com-petency: Analyzing: requires successful engagement in autonomous or independent work. Fink’s Taxonomy of Significant Learning enhanced Bloom’s taxonomy, incorporating the following dimensions: learning how to learn, caring, human dimension, and integration (Figure 1). A core group of faculty worked as a team to develop learning objec-tives and create synergistic curricular components to reinforce learning across multiple domains.
The program has been designed to be flexible, changing as the
A Novel Approach to Teaching Clinical and Translational Science Using Adult Learning Principles, Learner-Centered Outcomes, and Hierarchical CompetenciesDeborah Helitzer, Sc.D.1,*, Jeff Norenberg, Pharm.D.2, Kristina Wittstrom, M.Ed.2
Figure 1.
1University of New Mexico, NM, USA2College of Pharmacy, University of New Mexico, NM, USA*Corresponding Author: [email protected]

21sect ion two
science of clinical translational research evolves. New domains of competency can be added, existing ones can be changed, and some can be dropped.
The original twelve domains of competency are: biomedical infor-matics, biomedical ethics, biostatistics, research design, epidemiology, instrument and measurement design (both quantitative and qualita-tive), cultural competence, patient outcomes research, research in health care settings, study implementation and management, current and emerging technologies, and grantsmanship. As an example of the programmatic flexibility, competencies related to regulatory aspects of clinical and translational research were recently added to support en-hanced interaction among teams of basic, clinical, and practice-based scholars. These competency domains comport with the recommenda-tions for core competencies for Masters programs recently developed by the CTSA national education and career development key function group (3).
We engaged over 60 faculty members from the Schools of Medicine, Nursing, and Pharmacy to participate as course leaders and domain team experts. These faculty members are experienced basic, clinical, and translational researchers who evidence proficiency in their own scientific disciplines. A fortuitous benefit of the program is that learners have unusual access to very senior mentors. It is believed that facili-tating connections between learners and senior scientists early in their career will be instrumental both for their scientific accomplishments and their career advancement.
The coursework is divided according to competency level. Level 1 competency is attained through participation in structured face-to-face class sessions. Much of the content is delivered in seminar-style in-struction using Socratic methods of inquiry and debate to stimulate crit-ical thinking. Students are asked to share research articles in their area of scientific interest and the discussions focus on the ways in which
the domain is expressed in the article. Within the domain of biomedical informatics, students engage in discussions about search strategies as well as inclusion and exclusion criteria. Within the domain of research design, discussions address the choices made by the authors in their research approach. Within the biostatistics domain, students consider the analyti-cal approach to the research data. Focus is placed on commu-nication and attainment of terminology. The majority of work is completed by learners outside of the traditional classroom setting. The purpose of the face-to-face sessions is to share knowledge, clarify understanding, identify gaps and resources, provide opportunities to demonstrate leadership, and to model the implementation of team science.
All students complete a clinical research appraisal inventory (CRAI) (4), which enables them and their research mentor to identify areas of strength and opportunities for additional skill building. Each student develops an individual learning plan and a committee on studies comprising the student’s research mentor, at least one faculty with subject matter expertise, and an MSCR steering committee member as chair. Level 2 com-petencies and higher are attained through independent study, although some learners identify learning objectives that they prefer to address in learning teams. Learners complete course contracts with the domain leader and their research mentor that reflect the ongoing growth in competency attainment through Levels 2 and higher.
The program runs for 12 consecutive months and is divided into six 8-week modules, each offering two to three courses. Learners are expected to complete the program in 2–2.5 years. In addition to coursework, requirements include a research thesis, a manuscript, and a grant proposal.
At the writing of this brief report, we have enrolled five cohorts to-taling 27 students. Table 1 shows the relevant demographics. Notably, in 10 of 12 domains, the original faculty directors continue to lead the instruction in their subject areas.
This approach to curriculum design has proven to be universally effective and respectful of adult learning needs. The hierarchical ap-proach to competency development acknowledges that learning new skills is a process as much as it is an outcome. The UNM MSCR is a successful model that engages learners in a “need to know” approach, which becomes increasingly focused as the learner approaches higher levels of skill development. The program is very learner intensive, but entirely adaptable to local conditions owing to its use of local tal-ent and skill as a foundation for learning. In addition to producing important learner outcomes, this approach to program development benefits the instructor pool engaging instructors in a team-based, mul-tidisciplinary approach to program design and implementation that requires knowledge and language acquisition in all domains among all instructors.
REFERENCES 1. L. W. Anderson, D. R. Krathwohl, Eds., A Taxonomy for Learning,
Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives (Longman, New York, 2001).
2. L. D. Fink, Creating Significant Learning Experiences: An Integrated Approach to Designing College Courses (Jossey-Bass, San Francisco, 2003), pp. 27-59.
3. Clinical and Translational Science Awards: Core Competencies in Clinical and Translational Research. Available at http://www.ctsaweb.org/index.cfm?fuseaction=home.showCoreComp.
4. E. A. Mullikin, L. L. Bakken, N. E. Betz, J. Career Assess. 15, 367 (2007).
*Includes Basic Science, Exercise Science, Biomedical Informatics.Table 1.
Cohort 2007 2008 2009 2010 2011 Total 5 years
DisciplineMedicine (63%) 2 3 3 4 5 17Pharmacy (7%) 1 0 0 0 1 2Nursing (11%) 2 0 0 0 1 3Other* (19%) 0 0 1 3 1 5
GenderFemale (48%) 1 0 4 2 6 13Male (52%) 4 3 0 5 2 14
EthnicityMinority (56%) 3 2 3 4 3 15Majority (44%) 2 1 1 3 5 12
RankFellow (59%) 2 1 2 5 6 16Faculty (41%) 3 2 2 2 2 11
DegreeM.D. (63%) 2 3 3 4 5 17Ph.D. (23%) 2 0 1 2 1 6Pharm.D. (7%) 1 0 0 0 1 2Other (7%) 0 0 0 1 1 2
Total 5 3 4 7 8 27
22
A new model for translational research has been created at the Center for Translational Research in Biomedical Sciences (CTRBS) at Chang Gung Memorial Hospital-Kaohsiung Medical Center in the southern city of Kaohsiung in Taiwan.
Commissioned in December 2007 by Mr. Yung-Ching Wang, the late chairman of the board of the Formosa Plastic Group, and with gen-erous funding from the Chang Gung Medical Foundation, this center was officially inaugurated in February 2009. Under the directorship of Professor Samuel H.H. Chan, Ministry of Education National Chair Professor and editor of the monograph series Translational Research in Biomedicine (S. Karger AG), this center aspires to set an example of how translational research in a medical center should be carried out and strives to be a center of research excellence with international repute.
INTERPRETATIONS OF TRANSLATIONAL MEDICINEAs the brainchild of Professor Chan, the uniqueness of the CTRBS re-sides in his two interpretations of translational medicine. First, transla-tional medicine is about solutions to health problems. If one subscribes to the philosophical belief that medical research is for the betterment of humankind, then one should realize that there is no real demarca-tion between clinical (bedside) and preclinical (bench) research. The only difference between these studies is that in the former, human subjects are used rather than animals, tissues, or cells. Nonetheless, because these studies are governed by the same ethical principles and guidelines, all will reveal information in some aspects of biomedi-cine. Translational research in biomedicine therefore transcends the boundaries between bench and bedside research. It is the synthesis of ideas, technologies, and research outcomes that are associated with a particular health theme. Second, translational medicine is about communication. The word “translation” is most commonly defined as expression of words in another language. Its definition can be ex-tended to include using simpler language and uncomplicated interpre-tations. Translational research in biomedicine therefore encompasses the presentation of knowledge in a fashion accessible to nonexperts. A molecular biologist is a nonexpert when it comes to interpretation of the clinical ramifications of acute myocardial infarction; a cardiolo-gist is a nonexpert when it comes to interpretation of the intricacies of DNA repair. Communication in simple, understandable language will bridge the intellectual gap between laboratory scientists and clinical practitioners.
THE PHILOSOPHY AND GOALStemming from these two interpretations of translational medicine, the governing philosophy of the CTRBS is that clinical and laboratory scientists must work together to tackle health-oriented problems. Under this philosophy, the goal of the CTRBS is to foster a congenial
environment where M.D.s and Ph.D.s can interact freely in terms of addressing meaningful research problems and generating solutions without the worry of the availability of facilities, know how, or clinical significance.
THE STRATEGIESSeveral strategies have been put forth to achieve this goal. First, the CTRBS has a provision for state-of-the-art facilities and technical sup-port. During the past 32 months, the CTRBS has completed its Phase I refurbishment of approximately 3,000 m2 of laboratory space, and purchased, installed, and tested over 3,000 pieces of equipment. Fa-cilities for physiological and biochemical experiments at the molecular, cellular, tissue, and whole-animal levels are currently available to com-plement modern clinical facilities in the medical center. In addition, an AAALAC International-accredited Center for Laboratory Animals provides excellent support for experimental animals, including ge-netically manipulated mice. To befit translational research, compatible clinical and laboratory facilities have been installed. For example, the presentation of images from animal ultrasonographs or MRIs and their analysis programs are compatible with those used in the medical cen-ter, making cross-interpretation between disease symptoms and pheno-types from animal models easily accessible. To ensure proper handling of the facilities, the center has held more than 60 training sessions on major equipment.
Second, the CTRBS has a provision to provide scientific and clinical advice. State-of-the-art facilities notwithstanding, the quality of labo-ratory research resides in employing the most appropriate and sensi-tive methodology to address the scientific issues. In addition to their individual research endeavors, Ph.D.s at the CTRBS routinely provide consultations to M.D.s on the best methods to answer mechanistic ques-tions. Likewise, M.D.s provide input to Ph.D.s on the validity of, for example, an animal model, based on whether the stipulated phenotypes are actually manifested by patients with the targeted disease. In the end, this is a win-win situation for both the clinical and laboratory scientists.
Third, and most importantly, is the provision of financial support. The principal concern on research projects at the CTRBS is whether the study is of clinical significance. Beyond that, funds for manpower and supplies are not an issue, and facilities are already available. The practice is to make use of the grant application as a means to solidify the scientific problems, and more often, to put the know-how of clinical and laboratory scientists together to provide comprehensive answers. Members of the CTRBS are also encouraged to seek external fund-ing; a matching fund amounting to 50% of the grant is awarded as an enticement.
Finally, despite the massive financial investment, the orientation of research projects is always towards solving a health problem rather than towards a marketable product. Nevertheless, regular meetings with two other members of the Chang Gung Group (Chang Gung Biotechnology Corporation and Chang Gung Medical Technology Company) offer a channel for the development of potential commercial products or di-agnostic tools.
Center for Translational Research in Biomedical Sciences, Chang Gung Memorial Hospital– Kaohsiung Medical Center, TaiwanSamuel H.H. Chan, Ph.D.
Director, Center for Translational Research in Biomedical Sciences, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, [email protected]

23sect ion two
Governments around the world have made large investments in academic health research, investments that play a criti-cal role in building strong scientific cultures and knowledge economies, and that have immense potential to be the gen-
esis of new therapies. However, countries continue to struggle with how to successfully translate academic discoveries into actual new medicines for patients. A significant factor influencing this struggle, exacerbated by the current difficult economic environment, is that ven-ture capital firms have become more risk averse and less willing to invest in early technology opportunities arising straight from academia. Global pharmaceutical companies are also facing challenges, including impending patent expirations on blockbuster drugs, the increasing cost of bringing new drugs to market, and today’s regulatory hurdles—all leading to the reorganization and redirecting of their research and de-velopment strategies. To rebuild its pipeline of drug candidates, pharma is increasingly interested in accessing innovative academic discover-ies. However, academic research laboratories can rarely advance their discoveries to the proof-of-concept stage that marks the transition be-tween an interesting discovery and a commercially viable investment opportunity for the private sector. As a consequence, we have seen a number of translational centers and initiatives launched to try to fill this commercialization gap.
A wide variety of models and structures are being explored world-wide, ranging from virtual centers that outsource all research and de-velopment activities to those that are fully equipped and staffed to sup-port such activities, and from centers led by academic institutions or government agencies to those driven exclusively by the private sector, while numerous combinations thereof are also emerging in the form of hybrid organizations. Irrespective of the model being pursued, these centers face multiple common challenges, including how to bridge the significant differences in scientific culture and values that exist between academia and industry, how to identify therapeutically and commer-cially promising projects from highly innovative and extremely early discoveries, and how to fund drug discovery activities that align neither with the traditional mandate of public granting agencies nor with cur-rent funding strategies of the private sector.
In Canada, the Federal Government has created the Centres of Excel-lence for Commercialization and Research Program with an investment of CAN$285 million over five years (2007–2012) to support centers that advance research and facilitate the commercialization of technolo-gies. To date, 17 centers have been established including the Centre for Drug Research and Development (CDRD) headquartered in Vancouver.
CDRD is a “bricks and mortar” organization with 85 employees and trainees with scientific, business, and project management expertise. It is equipped for drug screening, therapeutic antibody generation, drug target evaluation, medicinal chemistry, and drug delivery as well as in vitro and in vivo pharmacology, toxicology, and ADME studies. CDRD is a not-for-profit organization that operates fully independently of any academic institution or private sector company. Instead, it
has affiliations with major universities and health sciences research centers across Canada as well as select international centers, which enable researchers at all of these institutions to access its capabilities and resources.
CDRD aims to bring together, in as many ways as possible, the best drug development practices of both academia and industry. It was founded by academic researchers and business leaders with established track records in commercializing discoveries from university laborato-ries, and in founding successful biotech companies, thereby possessing first-hand knowledge of the challenges of early-stage drug discovery and development. This type of direct industry experience was a key criterion in building CDRD’s senior management and entire team.
CDRD’s team collaborates with principal investigators to undertake projects with the highest level of commercial potential, screened against rigorous scientific and business criteria to optimally design them for commercial success. Milestone-driven, outcomes-focused drug devel-opment under professional project management is then undertaken, as the projects are carried out according to industry practices with more strictly defined experiments, budgets, timelines, and reporting than is commonly employed in academia. The objective of the research plan is to develop early drug candidates to the proof-of-principle stage with demonstration of efficacy in animal models of human disease. And with most projects being very early stage in nature, they often require several iterations before the true commercial potential can be fully evaluated. The projects with the more promising data are continued at CDRD, and those that require further research can be then returned to the investiga-tor’s laboratory for further exploration, should they choose.
To support the projects, CDRD facilitates the leveraging of external funding via granting agencies such as the Canadian Institutes for Health Research Proof-of-Principle program, and through funds raised via CDRD’s established partnership with international industry. This struc-ture enables CDRD to carry out key experiments on a number of proj-ects per year, enhancing their data packages to identify those showing therapeutic and commercialization potential, and making them increas-ingly attractive to potential commercialization partners. Commercial-ization is enabled through licensing by the academic researcher’s in-stitution technology transfer office. In addition, CDRD has established a commercial arm, CDRD Ventures Inc. (CVI), to act as an interface between CDRD and industry, in-license selected intellectual property generated from CDRD projects directly from the affiliated institution or inventor, and form strategic partnerships with pharmaceutical and bio-tech companies to further develop and commercialize the technologies. Profits from CVI will flow back to the not-for-profit CDRD to support ongoing drug development projects.
The work of translational centers such as CDRD will significantly increase the prospects of health research discoveries being further de-veloped by commercialization partners, therein fueling the global life sciences industry with a robust pipeline of more fully validated and de-risked technologies. As the array of strategies being employed by translational centers around the world continues to mature, it is impor-tant for us all to communicate our respective knowledge on successful (and unsuccessful) ways to bridge the gaps in the commercialization process, maximize societal returns on public research investment, and ultimately benefit patients around the world.
New Commercialization Models for Early Stage Health ResearchNatalie Dakers, Barry Gee, and Michel Roberge, Ph.D.*
The Centre for Drug Research and Development (CDRD),Vancouver, BC, Canada*Corresponding Author: [email protected]
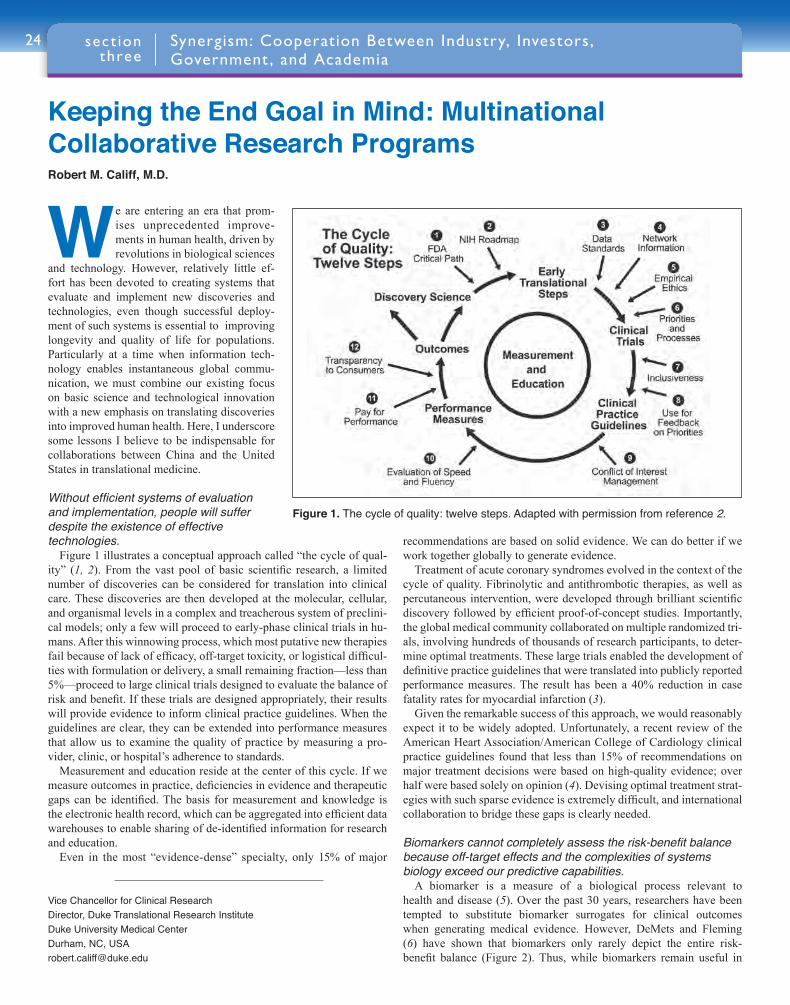
24
We are entering an era that prom-ises unprecedented improve-ments in human health, driven by revolutions in biological sciences
and technology. However, relatively little ef-fort has been devoted to creating systems that evaluate and implement new discoveries and technologies, even though successful deploy-ment of such systems is essential to improving longevity and quality of life for populations. Particularly at a time when information tech-nology enables instantaneous global commu-nication, we must combine our existing focus on basic science and technological innovation with a new emphasis on translating discoveries into improved human health. Here, I underscore some lessons I believe to be indispensable for collaborations between China and the United States in translational medicine.
Without efficient systems of evaluation and implementation, people will suffer despite the existence of effective technologies.
Figure 1 illustrates a conceptual approach called “the cycle of qual-ity” (1, 2). From the vast pool of basic scientific research, a limited number of discoveries can be considered for translation into clinical care. These discoveries are then developed at the molecular, cellular, and organismal levels in a complex and treacherous system of preclini-cal models; only a few will proceed to early-phase clinical trials in hu-mans. After this winnowing process, which most putative new therapies fail because of lack of efficacy, off-target toxicity, or logistical difficul-ties with formulation or delivery, a small remaining fraction—less than 5%—proceed to large clinical trials designed to evaluate the balance of risk and benefit. If these trials are designed appropriately, their results will provide evidence to inform clinical practice guidelines. When the guidelines are clear, they can be extended into performance measures that allow us to examine the quality of practice by measuring a pro-vider, clinic, or hospital’s adherence to standards.
Measurement and education reside at the center of this cycle. If we measure outcomes in practice, deficiencies in evidence and therapeutic gaps can be identified. The basis for measurement and knowledge is the electronic health record, which can be aggregated into efficient data warehouses to enable sharing of de-identified information for research and education.
Even in the most “evidence-dense” specialty, only 15% of major
recommendations are based on solid evidence. We can do better if we work together globally to generate evidence.
Treatment of acute coronary syndromes evolved in the context of the cycle of quality. Fibrinolytic and antithrombotic therapies, as well as percutaneous intervention, were developed through brilliant scientific discovery followed by efficient proof-of-concept studies. Importantly, the global medical community collaborated on multiple randomized tri-als, involving hundreds of thousands of research participants, to deter-mine optimal treatments. These large trials enabled the development of definitive practice guidelines that were translated into publicly reported performance measures. The result has been a 40% reduction in case fatality rates for myocardial infarction (3).
Given the remarkable success of this approach, we would reasonably expect it to be widely adopted. Unfortunately, a recent review of the American Heart Association/American College of Cardiology clinical practice guidelines found that less than 15% of recommendations on major treatment decisions were based on high-quality evidence; over half were based solely on opinion (4). Devising optimal treatment strat-egies with such sparse evidence is extremely difficult, and international collaboration to bridge these gaps is clearly needed.
Biomarkers cannot completely assess the risk-benefit balance because off-target effects and the complexities of systems biology exceed our predictive capabilities.
A biomarker is a measure of a biological process relevant to health and disease (5). Over the past 30 years, researchers have been tempted to substitute biomarker surrogates for clinical outcomes when generating medical evidence. However, DeMets and Fleming (6) have shown that biomarkers only rarely depict the entire risk-benefit balance (Figure 2). Thus, while biomarkers remain useful in
Vice Chancellor for Clinical ResearchDirector, Duke Translational Research InstituteDuke University Medical CenterDurham, NC, USA [email protected]
Keeping the End Goal in Mind: Multinational Collaborative Research ProgramsRobert M. Califf, M.D.
Synergism: Cooperation Between Industry, Investors, Government , and Academia
sect ion three
Figure 1. The cycle of quality: twelve steps. Adapted with permission from reference 2.
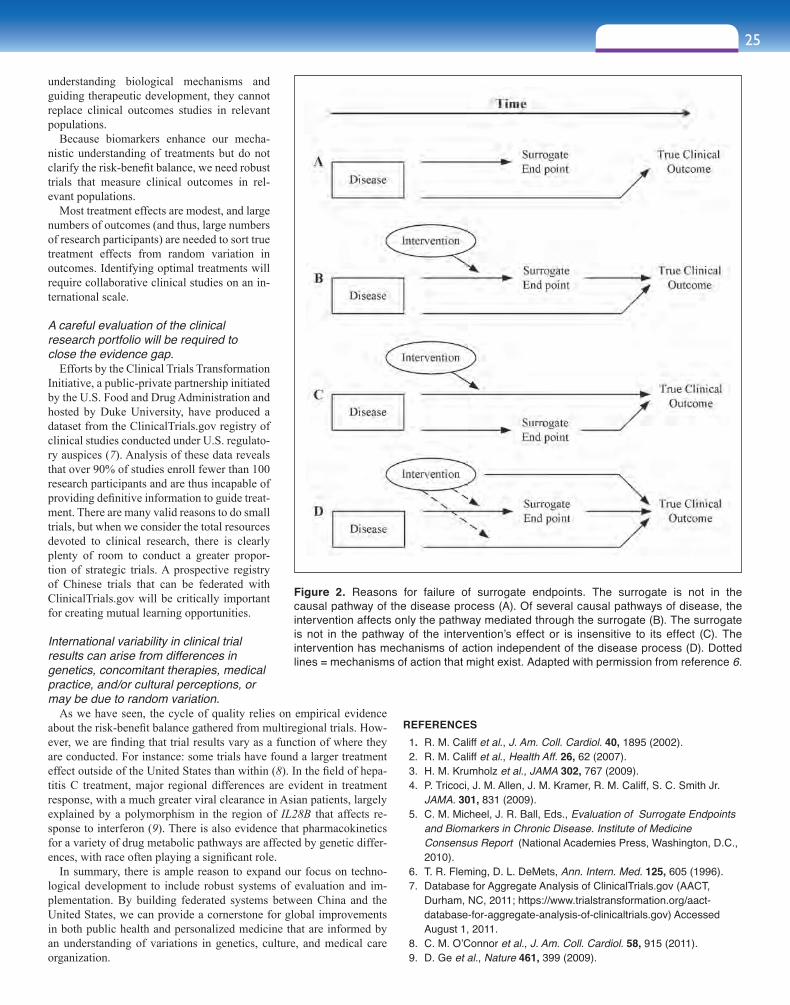
understanding biological mechanisms and guiding therapeutic development, they cannot replace clinical outcomes studies in relevant populations.
Because biomarkers enhance our mecha-nistic understanding of treatments but do not clarify the risk-benefit balance, we need robust trials that measure clinical outcomes in rel-evant populations.
Most treatment effects are modest, and large numbers of outcomes (and thus, large numbers of research participants) are needed to sort true treatment effects from random variation in outcomes. Identifying optimal treatments will require collaborative clinical studies on an in-ternational scale.
A careful evaluation of the clinical research portfolio will be required to close the evidence gap.
Efforts by the Clinical Trials Transformation Initiative, a public-private partnership initiated by the U.S. Food and Drug Administration and hosted by Duke University, have produced a dataset from the ClinicalTrials.gov registry of clinical studies conducted under U.S. regulato-ry auspices (7). Analysis of these data reveals that over 90% of studies enroll fewer than 100 research participants and are thus incapable of providing definitive information to guide treat-ment. There are many valid reasons to do small trials, but when we consider the total resources devoted to clinical research, there is clearly plenty of room to conduct a greater propor-tion of strategic trials. A prospective registry of Chinese trials that can be federated with ClinicalTrials.gov will be critically important for creating mutual learning opportunities.
International variability in clinical trial results can arise from differences in genetics, concomitant therapies, medical practice, and/or cultural perceptions, or may be due to random variation.
As we have seen, the cycle of quality relies on empirical evidence about the risk-benefit balance gathered from multiregional trials. How-ever, we are finding that trial results vary as a function of where they are conducted. For instance: some trials have found a larger treatment effect outside of the United States than within (8). In the field of hepa-titis C treatment, major regional differences are evident in treatment response, with a much greater viral clearance in Asian patients, largely explained by a polymorphism in the region of IL28B that affects re-sponse to interferon (9). There is also evidence that pharmacokinetics for a variety of drug metabolic pathways are affected by genetic differ-ences, with race often playing a significant role.
In summary, there is ample reason to expand our focus on techno-logical development to include robust systems of evaluation and im-plementation. By building federated systems between China and the United States, we can provide a cornerstone for global improvements in both public health and personalized medicine that are informed by an understanding of variations in genetics, culture, and medical care organization.
25sect ion three
REFERENCES 1. R. M. Califf et al., J. Am. Coll. Cardiol. 40, 1895 (2002). 2. R. M. Califf et al., Health Aff. 26, 62 (2007). 3. H. M. Krumholz et al., JAMA 302, 767 (2009). 4. P. Tricoci, J. M. Allen, J. M. Kramer, R. M. Califf, S. C. Smith Jr.
JAMA. 301, 831 (2009). 5. C. M. Micheel, J. R. Ball, Eds., Evaluation of Surrogate Endpoints
and Biomarkers in Chronic Disease. Institute of Medicine Consensus Report (National Academies Press, Washington, D.C., 2010).
6. T. R. Fleming, D. L. DeMets, Ann. Intern. Med. 125, 605 (1996). 7. Database for Aggregate Analysis of ClinicalTrials.gov (AACT,
Durham, NC, 2011; https://www.trialstransformation.org/aact-database-for-aggregate-analysis-of-clinicaltrials.gov) Accessed August 1, 2011.
8. C. M. O’Connor et al., J. Am. Coll. Cardiol. 58, 915 (2011). 9. D. Ge et al., Nature 461, 399 (2009).
Figure 2. Reasons for failure of surrogate endpoints. The surrogate is not in the causal pathway of the disease process (A). Of several causal pathways of disease, the intervention affects only the pathway mediated through the surrogate (B). The surrogate is not in the pathway of the intervention’s effect or is insensitive to its effect (C). The intervention has mechanisms of action independent of the disease process (D). Dotted lines = mechanisms of action that might exist. Adapted with permission from reference 6.

26
Recent biomedical breakthroughs, such as the sequencing of the human genome and a deeper understanding of the un-derpinnings of disease, have laid the scientific foundation for changes in the way drugs will be developed and used.
The result is a movement toward personalized medicine, which tailors treatments to individual patients based on each person’s genetic char-acteristics. This new approach to medicine has the potential to optimize targeted delivery and dosing of treatments so that patients will receive better therapies with more accurate dosing and fewer side effects.
While personalized medicine may provide patients with a new era of therapy, it also holds the potential to revitalize the biomedical industry. Although American pharmaceutical and biotech companies maintain a competitive advantage in the global marketplace and make up two of the few U.S. manufacturing sectors with a positive trade balance (1), there are some signs that the ability of these industries to continue to innovate may be at risk. The return on investments for biomedical prod-ucts continues to drop, development costs are increasing, timelines are long, and rates of failure are high. And while the promise of personal-ized medicine has great potential for treating patients more effectively, it necessitates a business model that is different from the traditional blockbuster approach (2).
Shifting to a model based on personalized medicine will not only introduce a more sustainable development approach for industry, but it will also revolutionize the way in which patients are treated. And we are already seeing some successes from this model. Trastuzumab (trade name Herceptin) is the best-known case of a tailored drug, relying on the use of genetic-based tests for assessing overexpression of the HER2 gene, the target of the drug (3). A very recent example of a tailored therapy is the U.S. Food and Drug Administration (FDA) approval of Vemurafenib (trade name Zelboraf), which is a new treatment for pa-tients with metastatic melanoma who also have the genetic mutation BRAF V600E (4). Vemurafenib was co-developed and approved with a diagnostic test for this mutation.
Although there have been early returns on investments in personal-ized medicine in the form of these and several other therapies, there is still a long way to go. Realizing the potential of personalized medicine requires a sustained commitment to advancing our understanding of the science underlying the human genome and the underlying basis of disease, as well as how individual genetic variations affect a particular patient’s response to therapy. It also requires an efficient pathway to translate new scientific findings into marketable products; this includes more investment in sound regulatory science that will facilitate getting more personalized therapies to the market more quickly, without com-promising patient safety.
At the FDA, we believe that regulatory science—the knowledge, tools, standards, and approaches necessary to assess the safety, efficacy, quality, and performance of FDA-regulated products—is the critical bridge between basic scientific research discoveries and new, mar-keted medical products. Commissioner Margaret Hamburg, M.D., has placed a high priority on regulatory science at the FDA, and released a Strategic Plan for Regulatory Science in August 2011 that outlines the agency’s investment priorities to expand the FDA’s science capacity and allow the agency to keep pace with emerging scientific advances,
particularly at the forefront of personalized medicine (5). The FDA’s Regulatory Science Initiative has agency-wide impact, and several key pieces promote the movement toward personalized medicine.
The use of clinical biomarkers in drug development holds much promise for the future of medicine and the biomedical industries. By identifying and qualifying biomarkers, companies can decrease costs by pinpointing patients who will respond better to drugs, reducing trial sample size, excluding patients early in the process by predicting ad-verse response through toxicity biomarkers, shortening end-point ob-servation times, and providing important information for data mining.
Predictive toxicology is another important piece of regulatory sci-ence necessary to drive and successfully regulate personalized medi-cine. Toxicity is the most common reason for failure in drug develop-ment (6), due in large part to the lack of predictive power in animal models. Yet, we are still using the same toxicology models of 60 years ago. The FDA is currently working in collaboration with the Nation-al Institutes of Health to implement a major shift that will transform toxicology from being observational to being predictive, thus allowing companies to determine which drugs to reject earlier in the process.
Finally, information technology has the potential to transform health care and drive personalized medicine. The FDA houses the largest known repository of clinical data, including all the safety, efficacy, and performance data submitted to the agency for new products as well as an increasing volume of postmarket safety surveillance data. The abil-ity to integrate and analyze these data could revolutionize the develop-ment of new treatments. It would allow us to address fundamental sci-entific questions about patient responses to therapeutics and to acquire information on disease parameters, such as determining meaningful measures of disease progression and identifying biomarkers for assess-ing drug safety and responses that could only be gained by analyzing large, pooled sets of data. The FDA is currently in the process of build-ing the information technology infrastructure necessary to harness the potential of data mining.
We are entering a new era of medicine—one that will revolutionize how diseases are treated by tailoring therapies to individual patients’ genetic and biological profiles. It is clear that personalized medicine is the medicine of the future, and it is important that we continue to focus our efforts and investments on understanding the science necessary to develop this field and bring safe, effective therapies to patients around the world.
REFERENCES 1. FDA internal data for 2007–2010 compiled from tariff and trade data
from the U.S. Department of Commerce and the U.S. International Trade Commission.
2. Tufts Center for the Study of Drug Development, Biopharmaceutical Approvals Up Dramatically (Tufts CSDD, 2011), vol.13, no. 3.
3. For additional information on the approval of Herceptin to treat HER2-positive breast cancer patients, see: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2006/ucm108788.htm.
4. For additional information on Zelboraf to treat patients with BRAF V600E, see: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm268241.htm.
5. U.S. Food and Drug Administration, Advancing Regulatory Science at FDA: A Strategic Plan (FDA, 2011; http://www.fda.gov/ScienceResearch/SpecialTopics/RegulatoryScience/ucm267719.htm).
6. L. Safinia, Drug Discovery Today: Fail Early, Fail Cheaply - Improving Drug Discovery Output with Early ADME/Tox Tests (Frost & Sullivan, 2008; http://www.frost.com/prod/servlet/market-insight-top.pag?docid=135570876).
Senior Advisor for Science, U.S. Food and Drug Administration, Washington, D.C., [email protected]
Personalized MedicineVicki Seyfert-Margolis, Ph.D.

27sect ion three
Over the last decade, the number of approved product launch-es in the life sciences industry has been overshadowed by the growth in research and development (R&D) expendi-ture. As a result, life sciences companies have become more
focused on the value of their R&D investments and are looking for ways to assess the true return on investment as well as for ways to im-prove that return. As the focus on return on investment has increased, the emphasis on improving R&D processes, appropriate virtualization of R&D activities, and carefully designed collaborative development have also increased, and translational medicine can play a key role in these efforts.
Although the life sciences industry continues to innovate relative to sectors such as telecom, finance, automotive/aerospace, and manu-facturing industries, its value is lagging expectations. Biopharma is at an inflection point: The industry faces higher scientific and regulatory hurdles to innovation, an increased cost burden in R&D activities [the total cost to bring a new drug to market now approaches $1 billion (1)], and decreased probability of success. More importantly, R&D output is not keeping up with rising R&D investment, as R&D expen-ditures have not been matched by a proportional increase in approved product launches.
Concerns about this gap in R&D return on investment are prompting life sciences companies to scrutinize R&D budgets, to seek increased management transparency, and look at investments with almost the same intensity as venture capital fund managers. Executives are looking to assess the internal rate of return on these investments, utilizing traditional portfolio management processes as well as other tools to curtail unproductive expenditures earlier in the product lifecycle.
As the focus on return on investment has increased, improving R&D processes, appropriate virtualization of R&D activities, and carefully designed collaborative development have increased in importance. They hold the promise of improving productivity of invested resources and the likelihood that successful new therapies can reach the market more expeditiously.
To generate sustained shareholder value, life sciences organizations need to focus on key levers that can drive change in the R&D process. Using a tool such as Deloitte’s Enterprise Value Map (EVM) offers a way for life sciences organizations to identify those R&D levers that could help transform performance (Figure 1).
TRANSLATIONAL MEDICINE: LEVER TO IMPROVE R&D PRODUCTIVITYOne of the challenges in improving R&D effectiveness is the need for better collaboration, connectivity, and sharing of information across various silos in the health care value chain. Translational medicine con-cepts and approaches can play a key role in addressing this challenge. Translational medicine integrates research information, clinical results, and other data. This helps to bridge the gap between basic science re-search and clinical practice to create an integrated “bench and bedside” model where clinicians and researchers collaborate and exchange criti-cal data. This integrated “bench to bedside and back” approach to shar-ing information across clinical research, clinical practice, patients, and ultimately broader community participants, can enable improvements across the entire health care value chain, and specifically in some of the most “value-sensitive” areas of the R&D model such as success rates and attrition management. Translational medicine, and the collabora-tion implicitly associated with it, can be used as a lever to ultimately re-engineer the R&D process and reduce R&D cycle times and unit costs (Figure 2).
Translational medicine has the potential to improve efficiency in the overall health care value chain. For example, it could facilitate lower R&D costs, greater sales and marketing efficiency, and more rapid adoption of targeted therapies. It also may enable a more successful product pipeline through earlier termination of unsuccessful com-
Global Managing DirectorLife Sciences and Health CareDeloitte Touche Tohmatsu LimitedDetroit, MI, [email protected]
Business and Commercial Aspects of InnovationRobert Go
Figure 1. Life Sciences R&D Value Map: Transforming R&D Performance. IRR, internal rate of return.
© 2011 Deloitte Global Services Limited. Private and confidential.
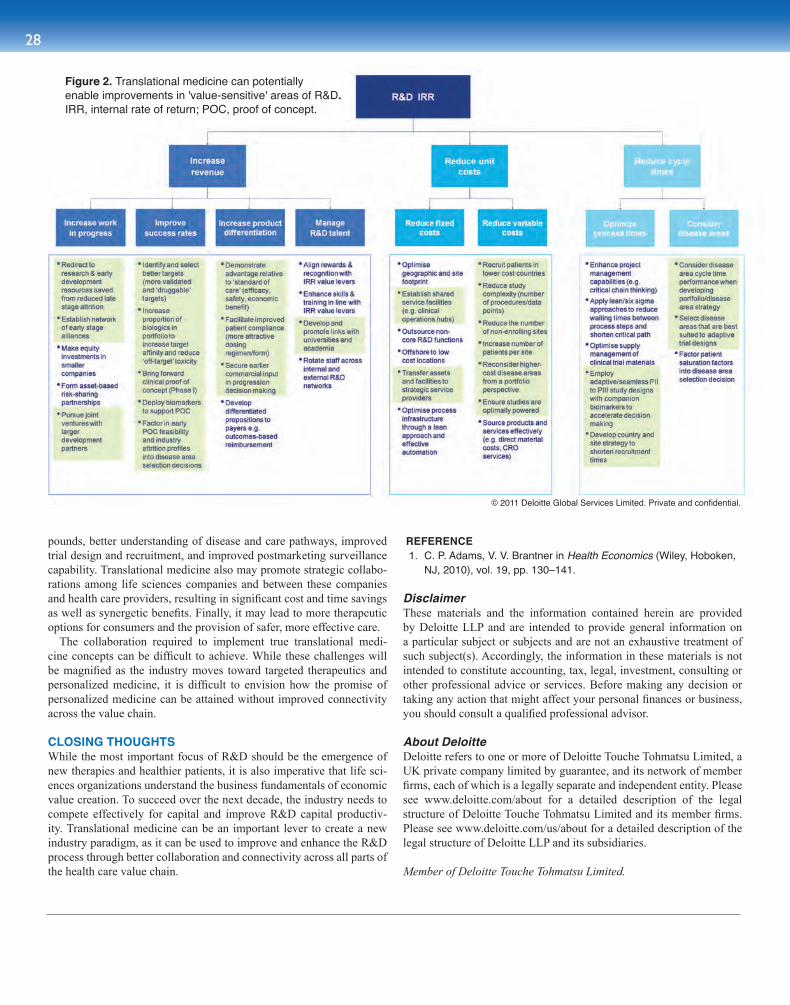
28
pounds, better understanding of disease and care pathways, improved trial design and recruitment, and improved postmarketing surveillance capability. Translational medicine also may promote strategic collabo-rations among life sciences companies and between these companies and health care providers, resulting in significant cost and time savings as well as synergetic benefits. Finally, it may lead to more therapeutic options for consumers and the provision of safer, more effective care.
The collaboration required to implement true translational medi-cine concepts can be difficult to achieve. While these challenges will be magnified as the industry moves toward targeted therapeutics and personalized medicine, it is difficult to envision how the promise of personalized medicine can be attained without improved connectivity across the value chain.
CLOSING THOUGHTSWhile the most important focus of R&D should be the emergence of new therapies and healthier patients, it is also imperative that life sci-ences organizations understand the business fundamentals of economic value creation. To succeed over the next decade, the industry needs to compete effectively for capital and improve R&D capital productiv-ity. Translational medicine can be an important lever to create a new industry paradigm, as it can be used to improve and enhance the R&D process through better collaboration and connectivity across all parts of the health care value chain.
REFERENCE 1. C. P. Adams, V. V. Brantner in Health Economics (Wiley, Hoboken,
NJ, 2010), vol. 19, pp. 130–141.
DisclaimerThese materials and the information contained herein are provided by Deloitte LLP and are intended to provide general information on a particular subject or subjects and are not an exhaustive treatment of such subject(s). Accordingly, the information in these materials is not intended to constitute accounting, tax, legal, investment, consulting or other professional advice or services. Before making any decision or taking any action that might affect your personal finances or business, you should consult a qualified professional advisor.
About DeloitteDeloitte refers to one or more of Deloitte Touche Tohmatsu Limited, a UK private company limited by guarantee, and its network of member firms, each of which is a legally separate and independent entity. Please see www.deloitte.com/about for a detailed description of the legal structure of Deloitte Touche Tohmatsu Limited and its member firms. Please see www.deloitte.com/us/about for a detailed description of the legal structure of Deloitte LLP and its subsidiaries.
Member of Deloitte Touche Tohmatsu Limited.
Figure 2. Translational medicine can potentiallyenable improvements in 'value-sensitive' areas of R&D.IRR, internal rate of return; POC, proof of concept.
© 2011 Deloitte Global Services Limited. Private and confidential.

29sect ion three
Academic scientific research is well funded in the United States to the tune of about $50 billion per year (1). China is behind but is catching up fast (2). With investments in aca-demic research of that magnitude, we have the responsibility
to ask if these governments are getting their money’s worth. Several major academic centers within the United States are therefore ques-tioning whether the conversion of university discoveries into products and services that benefit society could be made more efficient. These products and services emerge from the private sector, not universities; yet universities in general interface poorly with the private sector. The pipeline between academia and industry must be short and unclogged if good ideas coming out of academia are to have practical benefits for the public.
California Institute for Quantitative Biosciences (QB3) is an aca-demic, health-related scientific institution based in the United States that is consciously acting as an interface between universities and the private sector (1). QB3 is one of four Institutes for Science and Innova-tion created by the California Legislature in 2000 to capture the value of University of California research to benefit its citizens and to foster economic growth. It the only one of the four devoted exclusively to the life sciences. QB3’s vision is to create an Academic Health Center appropriate for the 21st century that not only includes the conventional basic and clinical academic communities, but also engages partners from existing life science companies and life science startups. The goal is to create a conscious and energetic bioinnovation ecosystem. Modest investments in university-based interface organizations such as QB3 should significantly enhance the value to society of government invest-ment in research and development.
To achieve its goals QB3 offers services to its academic scientists and its entrepreneurs that include:
Market Analysis: A key challenge is identifying the best appli-cation for new discoveries. This requires the institution to identify a potential application, evaluate whether there is a need for it and the size of the market, assess potential competitors and partners in that space, and determine the intellectual property position. If licensing is appropriate, QB3 staff prepares the scientist/inventor to interact suc-cessfully with their university’s technology transfer office. Academic scientists can also access the services of the institute’s scientific and legal interns.
De-risking research facilities: The private sector—both the life science industries and the investment communities—often find po-tential investment interests in academic research but are unwilling to partner unless the commercial value can be validated first through pre-commercial development research. QB3 has created facilities equipped for industrial-grade high throughput screening, medicinal chemistry, and microfabrication to help meet these needs.
Bridging-the-gap funding: QB3 has a small Catalyst Fund that
enables its scientists to “bridge the gap” between government-funded discovery research and commercial adoption.
Mentorship: QB3 offers both an Entrepreneurs-in-Residence Pro-gram and a College of Mentors to aid academic scientists who do not have the training to assess whether their discoveries have commercial applications and, if so, whether to license them to an industry part-ner or start a new company. Scientists often need advice on sources of capital, equity sharing, building a team, developing a business plan, and formulating an exit strategy, should they choose to start their own company.
Start-up-in-a-box: If an academic scientist decides to launch their own company, QB3’s Start-up-in-a-box allows the entrepreneur to identify corporate and patent lawyers, small business funding oppor-tunities, and other services to help simplify forming a new company.
Incubator facilities: QB3 provides incubator space for new com-panies down to a few hundred square feet, enough to start a company but also minimize burn rate. QB3 also offers opportunities for its incu-bator tenants to socialize with each other and those with entrepreneurial expertise. The goal is to remove as many distractions as possible to allow the entrepreneurs to focus on their milestones.
Locating industry partners: QB3 helps to identify collaborators within the life science industry for both our academic scientists and the entrepreneurs in our incubator.
Venture funding: With help from local venture capitalist talent, QB3 has created its own $11 million venture fund, Mission Bay Capi-tal, which is now funding six companies.
QB3 created these initiatives to import the “Lean Start-Up” model, now prevalent in the information technology industry, into the biotech-nology industry (3). After four years of operation, QB3 now has 43 companies in its incubator and continues to receive a steady stream of requests from potential tenants. Several tenants have already left the incubator after being awarded significant Series A funding from larger venture firms or being acquired by an existing company. What is most important, however, is that the institution has raised the consciousness of our creative faculty to the importance of identifying discoveries that could potentially help society. QB3 has also made it easier for scien-tists to develop their discovery into a product without disrupting their scientific careers.
Governments of both developing and developed countries face the constant challenge of assessing how much of their limited resources to put into the support of fundamental scientific research. Government in-vestment in academic research is more likely if there are clear pathways to job creation and economic growth. Academic organizations such as QB3 can provide effective tools to ensure the ongoing government sup-port of basic research.
REFERENCES 1. R. B. Kelly, D. Crawford, Mol. Biol. Cell, 22, 1807 (2011). 2. H. Yang, Nature Biotechnol. 29, 779 (2011). 3. E. Reis, The Lean Startup: How Today’s Entrepreneurs Use
Continuous Innovation to Create Radically Successful Businesses. (Crown Publishing Group, New York, NY, 2011).
Validating Government Investment in Biological ResearchRegis B. Kelly, Ph.D.
Director of the California Institute for Quantitative Biosciences (QB3), UCSF, San Francisco, CA, [email protected]

30
1. What are the most dangerous precancerous lesions of gastric cancer?
At one time, gastric diseases with prolonged recovery periods, such as gastric ulcers, gastric polyps, and some forms of chronic atrophic gastritis, were considered to be precancerous lesions. Results from our studies using the immunohistochemical techniques showed that
intestinal metaplasia and atypical hyperplasia of gastric mucosa had a high coincidence with gastric cancer in spatial distribution of gastric epithelial tissue. As a result, we drew the preliminary conclusion that for the abovementioned precancerous lesions, intestinal metaplasia and atypical hyperplasia should be considered more likely to become cancerous.
2. Are there currently biomarkers that accurately predict the malignancy potential of precancerous lesions?
Precancerous lesions expressing certain tumor antigens may be more likely to become cancerous than those without these antigens.
Gastric cancer is one of the leading malignant diseases in China. Currently, the causes of gastric cancer have not been conclusively determined, so instead of etiological treatment, early detection of gastric cancer has become an important strategy for reducing mortality from this disease. Our laboratory has been devoted to researching gastric cancer for more than 33 years, including the exploration of pathogenesis and preclinical/clinical applications of diagnosis and treatment (1).
Our Research Institution—Xijing Hospital of Digestive Diseases in Xi’an, China.
State Key Laboratory of Cancer Biology, Xijing Hospital of Digestive Diseases, Fourth Military Medical University, Xi’an, China*Corresponding Author: [email protected]
Cancer: From Basic Science to Clinical Research
Translational Strategies in Gastric Cancer Research Yongzhan Nie, M.D., Ph.D., Yongquan Shi, M.D., Ph.D., Zhiping Yang, M.D., Yanglin Pan, M.D., Ph.D., Liu Hong, M.D., Ph.D., Jie Liang, M.D., Ph.D., Xiaohua Li, M.D., Ph.D., Kaichun Wu, M.D., Ph.D., and Daiming Fan, M.D., Ph.D.*
30 sect ion four

31sect ion four
To examine whether this is the case, we determined whether important tumor antigens such as CEA, CA19-9, CA50, CA125, CA 153, Lewx, Lewy, T, and Tn were associated with cancerous and precancerous lesions. No correlation was found, and these antigens presented little contribution to a diagnosis. Therefore, it is clear that alternative tumor antigen biomarkers of greater diagnostic value are needed.
3. Seeking gastric cancer antigen biomarkers.The identification of gastric cancer antigen markers that are of high
diagnostic value for histology, cytology, and particularly serology sam-ples is a long and arduous process. Starting in 1984, our group began to improve on traditional immunological techniques and design new methods for antigen expression. We have obtained 12 monoclonal an-tibodies (mAbs; MG series) from 28561 hybridomas using the lym-phocyte hybridizing technique. We named these previously unreported antigens, against which these mAbs were raised, MGAgs (2). The MG mAbs produced have high specificity for MGAgs, which are highly expressed in gastric cancer tissue, but rarely expressed in normal tissue. Immunohistochemical staining using MG mAbs confirmed that over 90% of gastric cancer histology samples tested positive. The discovery of MGAgs has laid a significant foundation for our subsequent research.
4. Are MGAgs valuable for clinical diagnosis of gastric cancer?Beginning in 1987, we have been collaborating closely with more
than 10 domestic hospitals and scientific research institutes to evalu-ate the clinical diagnostic value of MGAgs for gastric cancer. Using various methods and focusing on different aspects such as histology, cytology, and serology, we have reached the consensus that MGAgs have a number of clinical applications. First, they can assist patholo-gists in carrying out differential diagnoses of ambiguous cases. Second, MGAgs can be used as markers for monitoring precancerous lesions suspected to be high risk for becoming true tumors. Third, using im-munofluorescence to detect MGAgs in cell membranes can raise the detection rate of cancer cells from hydrothorax, hydroperitoneum, and other types of body fluids. Fourth, MGAgs are valuable in radioim-munoimaging. Finally, an immunoradiometric assay reagent-box, made of isotope-labeled antibodies, can be used to detect MGAgs in the blood of patients in order to carry out serological diagnosis of gastric cancer.
5. Polymerase chain reaction has enhanced the serological diagnosis of gastric cancer.
Compared with other methods, the serological diagnostic method described above has significant clinical diagnostic value. However, we found many cases of gastric cancer that failed to be detected using this technique due to low levels of MGAg expression in blood samples. Though highly expressed in gastric cancer tissue, MGAgs are primarily released into gastric lumen instead of into the blood. The small amount of MGAgs released into blood are either destroyed or metabolized by the immune system or biochemical factors of the body (3). To address this issue, we established the immune polymerase chain reaction (PCR) technique, which combined the high specificity of mAbs with the high sensitivity of PCR (4). When this technique was used to detect MGAgs in serum from gastric cancer patients, the positive detection rate in-creased to over 70%. Further, some early gastric cancers could also be detected. We next applied this technique to test whether MGAgs were correlated with gastric cancer incidence in high-risk groups in China. We found that gastric cancer was detected in those patients positive for MGAgs in their serum. Patients with early gastric cancers and who were positive for MGAgs showed a 30% occurrence of cancer within five years, whereas those patients who lacked MGAgs rarely developed cancer (5). These results indicate that the detection of MGAgs may help predict whether gastric mucosa will become cancerous and could po-tentially be used as a marker to identify which patients will develop gastric cancer. This technique has been patented and received certifica-tion to be used for testing the efficacy of new drugs.
Gastric cancer is a complex disease, and our research is still in the beginning stages. We are far from achieving ultimate success; however, we are interested in sharing our experiences with other translational researchers to advance the field. There is still much to learn as we con-tinue to research the underlying causes, and search for diagnostic mark-ers, in gastric cancer.
REFERENCES 1. D. Fan et al. J. Gastroenterol. Hepatol. 20, 360 (2005). 2. D. Zhang, Y. Chen, D. Fan, Exp. Rev. Vaccines 5, 223 (2006). 3. L. Hong, D. Fan, Exp. Opin. Ther. Targets 12, 749 (2008). 4. J. Ren et al., Cancer 88, 280 (2000). 5. J. Liu et al., Int. J. Clin. Pract. 56, 169 (2002).
Cell Cycle Regulators and Malignant Tumor BiomarkersTong Tong, M.D., Yongmei Song, M.D., Shujuan Shao, Ph.D., M.D., Xiaoxia Wang, Ph.D., Lihui Zou, Ph.D., M.D., Dan Li, Ph.D., Qimin Zhan, M.D.*
The control of cell cycle progression has been shown to be as-sociated with the maintenance of genomic fidelity. Defects in the regulation of cell cycle progression may result in genomic instabilities, including gene mutations, amplifications, or
chromosomal aberrations, which are associated with malignant trans-formation and tumorigenesis. The inactivation of cell cycle control can also have dramatic consequences on therapeutic sensitivity. A better un-derstanding of the machinery that controls cell cycle progression may lead to the discovery of clinical biomarkers for early diagnosis, predic-tion of therapeutic sensitivity, and better prognosis (1).
Mitosis in mammalian cells involves the generation of two genetically identical daughter cells. Successful mitosis requires the assembly of a strictly bipolar mitotic apparatus that ensures chromosomes are distributed equally between the daughter cells. This process is controlled by centrosomes. These are small cytoplasmic nonmembraneous organelles involved in the nucleation and organization of microtubules, and are required for spindle formation and function. They establish polarity and orientation of microtubules during interphase, and contribute to the assembly of the spindle and chromosomal segregation. Centrosomes may also serve as a central site that anchors important

32
molecules and regulates fundamental cellular functions, such as cell motility and adhesion. Multiple studies have shown that centrosome activity is also important for completing cytokinesis and for the progression of the cell cycle from the G1 to the S phase. Amplification of centrosomes leads to chromosomal missegregation and generation of aneuploidy, both of which are closely associated with cell transformation and tumorigenesis. Centrosome abnormalities are frequently observed in different types of human tumors and are often correlated with a poor clinical prognosis (2).
The machinery that controls centrosome stability still needs to be fully defined and likely involves multiple important cellular proteins, including p53, BRCA1, Gadd45, p21, Aurora-A, Cdk2/cyclin E, and Cdc2/cyclin B1. Precise coordination of these regulatory proteins maintains normal centrosome duplication and stability. Most recently, we found that the tumor suppressor BRCA1 physically interacts and co-localizes with the centrosomal protein, Ninein-like protein (Nlp). The localization of Nlp at the centrosome is likely dependent on normal cellular BRCA1 function, since cells containing BRCA1 mutations or that have silenced their endogenous BRCA1 reveal disrupted Nlp-cen-trosome colocalization. Suppressed endogenous Nlp expression using siRNA results in aberrant spindle formation, a failure of chromosomal segregation, and aneuploidy (3). Nlp is overexpressed in human breast, lung, and esophageal carcinomas, and the NLP gene is amplified in lung cancer (4). Interestingly, Nlp is phosphorylated by Cdc2 and Aurora-B, and such protein modifications contribute to Nlp stability and its regulation of cytokinesis (5, 6). Importantly, Nlp is strongly oncogenic and can induce transformation of NIH3T3 fibroblasts. Additionally, transgenic mice overexpressing Nlp mimic the phenotype of disrupted BRCA1, including centrosome amplification and spontaneous tumor formation. It appears that Nlp may act in cooperation with BRCA1 in the mitotic machinery and overexpression of Nlp leads to genomic in-stability and tumorigenesis (4). Thus, our findings have defined Nlp as a potent oncogenic protein, and provide a new potential molecular biomarker and therapeutic target for cancer.
Cyclin B1, a key component in the control of cell cycle progression from G2 through the M phase, has been implicated in tumorigenesis and malignant transformation. We have shown that Cyclin B1 is de-regulated in human esophageal squamous cell carcinoma (ESCC) and that overexpression of Cyclin B1 is closely associated with a malignant tumor phenotype and poor prognosis for patients. Isogenic ESCC cells overexpressing Cyclin B1 show highly invasive growth and have a high potential for metastasizing to the lungs in mouse models. Suppressing Cyclin B1 expression using siRNA in high-metastatic esophagus carci-noma cells specifically inhibits their ability to metastasize to the lungs. Notably, the expression of epithelial markers is altered and mesenchy-mal markers are induced in high Cyclin B1-expressing tumor cells,
suggesting that Cyclin B1 likely contributes to metastasis by promoting an epithelial-mesenchymal transition. These results establish a mecha-nistic link between Cyclin B1and the metastasis of ESCC cells into the lungs. Further, these data provide novel insight into understanding the role of Cyclin B1 in the development of tumor malignancy (7).
Aurora-A/STK15/BTAK, another centrosome-associated oncogenic protein, has been implicated in the control of mitosis. The overexpres-sion of Aurora-A results in chromosomal aberrations and genomic instability in both cell culture and animal models. Multiple lines of evidence indicate that Aurora-A induces malignant transformation of cells. Recently, we have found that Aurora-A expression is elevated in ESCC and is closely associated with tumor invasion, suggesting that overexpression of this protein might contribute to the occurrence and progression of ESCC (8). We are currently interested in defining the molecular mechanism(s) underlying the involvement of Aurora-A in the development of tumor malignancies. To do this, we first established isogenic cell lines, which expressed high levels of exogenous Aurora-A. These cells show increased proliferation and migration properties. Consistent with these observations, xenografts generated from ESCC cells expressing Aurora-A in nude mice grow faster than those from ESCC cells transfected with empty vector. In some cases, increased Aurora-A expression also appears to promote the invasive growth and metastasis of ESCC cells. Next, we examined the expression profiles for multiple proteins related to tumorigenesis and tumor malignancy in these cells. The overexpression of Aurora-A resulted in an altered expression profile for all of these proteins (9). In addition, we exam-ined the gene expression profiles in the isogenic cells overexpressing Aurora-A using a microarray assay. Aurora-A transfected ESCC cells showed about 200 upregulated genes, compared to the parental control cells. Further, our studies showed that the presence of Aurora-A en-hanced Cyclin B1 protein stability through their physical interactions and reduced the stability of AP2, a tumor suppressor-like transcription factor (10).
Taken together, these findings indicate that the dysregulation of the cell cycle regulating proteins Nlp, Cyclin B1, and Aurora-A significant-ly contribute to the development of malignant tumors, and that expres-sion levels of these proteins may be used as biomarkers for clinical diagnosis and prediction of clinical therapeutic sensitivity.
REFERENCES 1. L. H. Hartwell, T. A. Weinert, Science 246, 629 (1989). 2. S. J. Doxsey, Nature Cell Biol. 3, E105 (2001). 3. S. Q. Jin et al., J. Biol. Chem. 284, 22970 (2009). 4. S. Shao et al., J. Clin. Invest. 120, 498 (2010). 5. X. Zhao, S. Jin, Y. Song, Q. Zhan, Cancer Biol. Ther. 10, 945 (2010). 6. J. Yan, S. Jin, J. Li, Q. Zhan, J. Biol. Chem. 285, 40230 (2010). 7. Y. Song et al., Carcinogenesis 29, 307 (2008). 8. T. Tong et al., Clin. Cancer Res. 10, 7304 (2004). 9. X. X. Wang, R. Liu, S. Q. Jin, F. Y. Fan, Q. M. Zhan, Cell Res. 16,
356 (2006).10. L. Zou, Y. Sun, M. Wang, Q. Zhan, PLoS One 6, e23110 (2011),
doi:10.1371/journal.pone.0023110.
State Key Laboratory of Molecular OncologyCancer Hospital and Institute, Chinese Academy of Medical Sciences and Peking Union Medical college, Beijing, China*Corresponding Author: [email protected]
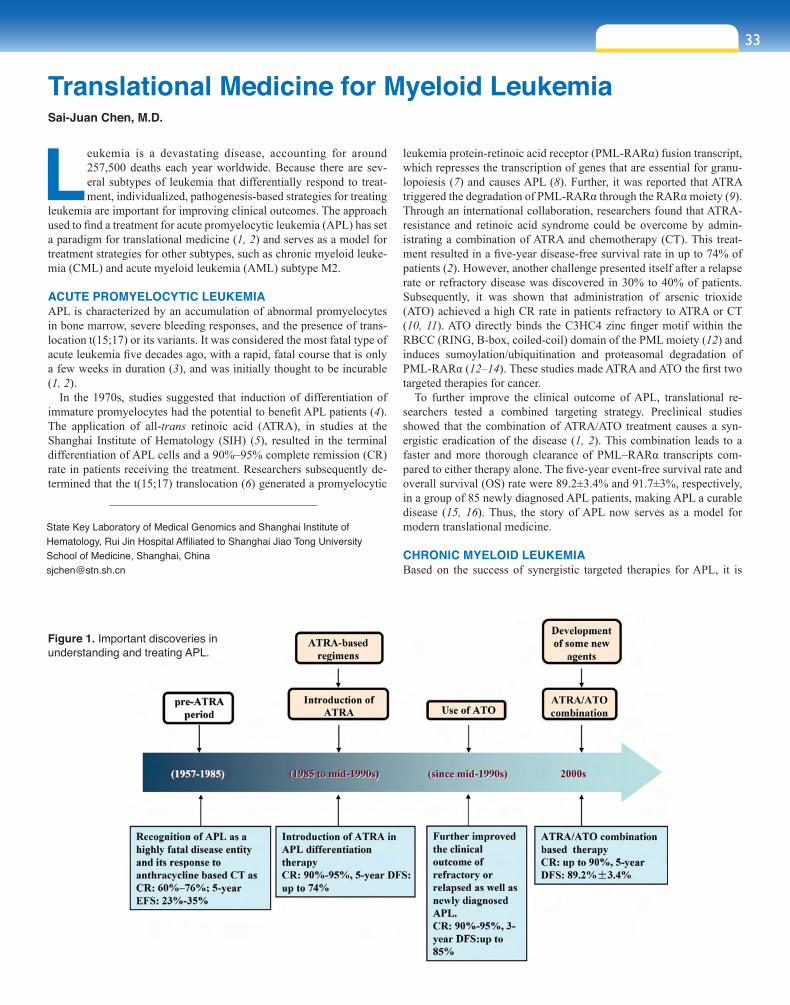
33sect ion four
Leukemia is a devastating disease, accounting for around 257,500 deaths each year worldwide. Because there are sev-eral subtypes of leukemia that differentially respond to treat-ment, individualized, pathogenesis-based strategies for treating
leukemia are important for improving clinical outcomes. The approach used to find a treatment for acute promyelocytic leukemia (APL) has set a paradigm for translational medicine (1, 2) and serves as a model for treatment strategies for other subtypes, such as chronic myeloid leuke-mia (CML) and acute myeloid leukemia (AML) subtype M2.
ACUTE PROMYELOCYTIC LEUKEMIA APL is characterized by an accumulation of abnormal promyelocytes in bone marrow, severe bleeding responses, and the presence of trans-location t(15;17) or its variants. It was considered the most fatal type of acute leukemia five decades ago, with a rapid, fatal course that is only a few weeks in duration (3), and was initially thought to be incurable (1, 2).
In the 1970s, studies suggested that induction of differentiation of immature promyelocytes had the potential to benefit APL patients (4). The application of all-trans retinoic acid (ATRA), in studies at the Shanghai Institute of Hematology (SIH) (5), resulted in the terminal differentiation of APL cells and a 90%–95% complete remission (CR) rate in patients receiving the treatment. Researchers subsequently de-termined that the t(15;17) translocation (6) generated a promyelocytic
leukemia protein-retinoic acid receptor (PML-RARα) fusion transcript, which represses the transcription of genes that are essential for granu-lopoiesis (7) and causes APL (8). Further, it was reported that ATRA triggered the degradation of PML-RARα through the RARα moiety (9). Through an international collaboration, researchers found that ATRA-resistance and retinoic acid syndrome could be overcome by admin-istrating a combination of ATRA and chemotherapy (CT). This treat-ment resulted in a five-year disease-free survival rate in up to 74% of patients (2). However, another challenge presented itself after a relapse rate or refractory disease was discovered in 30% to 40% of patients. Subsequently, it was shown that administration of arsenic trioxide (ATO) achieved a high CR rate in patients refractory to ATRA or CT (10, 11). ATO directly binds the C3HC4 zinc finger motif within the RBCC (RING, B-box, coiled-coil) domain of the PML moiety (12) and induces sumoylation/ubiquitination and proteasomal degradation of PML-RARα (12–14). These studies made ATRA and ATO the first two targeted therapies for cancer.
To further improve the clinical outcome of APL, translational re-searchers tested a combined targeting strategy. Preclinical studies showed that the combination of ATRA/ATO treatment causes a syn-ergistic eradication of the disease (1, 2). This combination leads to a faster and more thorough clearance of PML–RARα transcripts com-pared to either therapy alone. The five-year event-free survival rate and overall survival (OS) rate were 89.2±3.4% and 91.7±3%, respectively, in a group of 85 newly diagnosed APL patients, making APL a curable disease (15, 16). Thus, the story of APL now serves as a model for modern translational medicine.
CHRONIC MYELOID LEUKEMIA Based on the success of synergistic targeted therapies for APL, it is
Translational Medicine for Myeloid LeukemiaSai-Juan Chen, M.D.
Figure 1. Important discoveries in understanding and treating APL.
State Key Laboratory of Medical Genomics and Shanghai Institute of Hematology, Rui Jin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, [email protected]

34
possible other subtypes of leukemia, such as CML could benefit from this type of strategy. CML is a malignant my-eloproliferative disease characterized by a t(9;22)(q34;q11) translocation, which results in a BCR-ABL oncoprotein with constitutively active tyrosine kinase activity (17). Re-searchers have designed an inhibitor, imatinib (IM), of BCR-ABL’s kinase activity, and clinical studies have shown that this treatment elicits a five-year OS rate up to 89% (18). However, tyrosine kinase inhibitors alone do not completely conquer CML, therefore targeted therapies that work in syn-ergy would be beneficial. PML is one possible target since it enables leukemia-initiating cells (LICs) to maintain a qui-escent state and avoid destruction by therapeutics. Interest-ingly, ATO is able to target PML and eradicate quiescent LICs (19). Further, arsenic binds c-CBL which promotes the ubiquitination and proteasomal degradation of BCR-ABL (20). Taken together, these studies suggest that testing an ar-senic (such as ATO)/IM combination therapy may be a good candidate for eliciting synergistic therapeutic effects against CML (21–23).
ACUTE MYELOID LEUKEMIA SUBTYPE M2 WITH T(8;21)(Q22;Q22)Sixty percent of AML patients with t(8;21)/acute myeloid leukemia-1 transcription factor and the eight-twenty-one corepressor (AML1-ETO) show poor long-term survival rates. While AML1-ETO is not sufficient to induce a full-blown leukemia, C-KIT abnormalities, which are frequently found along with this AML (24), plus AML1-ETO causes a fatal leukemia in mice (25). We recently demonstrated that oridonin selectively induces apoptosis of t(8;21) leukemia cells and results in AML1-ETO cleavage. One of the cleaved fragments, a large portion of which is similar to wild-type ETO (26), interacts with and antagonizes parental AML1-ETO, which suppresses tumor activity and mediates oridonin’s anti-leukemia effects. Our preliminary studies show that oridonin induces partial clinical remission and sensitizes chemotherapy. Based on the multi-hit model of pathogenesis for leukemia, a combinatory targeted therapy of oridonin and C-KIT inhibitor could further improve the clinical outcome of patients and is a good candidate for testing in clinical trials.
CONCLUSIONS Elucidating the mechanisms underlying leukemogenesis is crucial for developing new therapeutic strategies for leukemia. This information can provide new targets for which molecularly synergistic, targeted therapies can be created. These types of therapies have already proven to be powerful tools. How well leukemia can be controlled in the 21st century will be determined by how quickly research advances, espe-cially in areas that bridge basic research and clinical practice, can be brought from bench to bedside.
REFERENCES 1. S. J. Chen et al., Blood 117, 6425 (2011). 2. Z. Y. Wang, Z. Chen, Blood 111, 2505 (2008). 3. L. K. Hillestad, Acta. Med. Scand. 159, 189 (1957). 4. L. Sachs, Nature 274, 535 (1978). 5. M. E. Huang et al., Blood 72, 567 (1988). 6. J. D. Rowley, H. M. Golomb, C. Dougherty, Lancet 1, 549 (1977). 7. K. Wang et al., Cancer Cell 17, 186 (2010). 8. H. de The, C. Chomienne, M. Lanotte, L. Degos, A. Dejean, Nature
347, 558 (1990). 9. J. Zhu et al., Proc. Natl. Acad. Sci. U.S.A. 96, 14807 (1999).10. Z. X. Shen et al., Blood 89, 3354 (1997).11. H. D. Sun, L. Ma, X. C. Hu, T. D. Zhang, Chin. J. Integr. Med. 12,
170 (1992).12. X. W. Zhang et al., Science 328, 240 (2010).13. G. Q. Chen et al., Blood 89, 3345 (1997).14. M. Jeanne et al., Cancer Cell 18, 88 (2010).15. J. Hu et al., Proc. Natl. Acad. Sci. U.S.A. 106, 3342 (2009).16. Z. X. Shen et al., Proc. Natl. Acad. Sci. U.S.A. 101, 5328 (2004).17. R. Ren, Nature Rev. Cancer 5, 172 (2005).18. B. J. Druker et al., N. Engl. J. Med. 355, 2408 (2006).19. K. Ito et al., Nature 453, 1072 (2008).20. J. H. Mao et al., Proc. Natl. Acad. Sci. U.S.A. 107, 21683 (2010).21. Q. Y. Zhang et al., Proc. Natl. Acad. Sci. U.S.A. 106, 3378 (2009).22. T. Yin et al., Blood 104, 4219 (2004).23. R. P. La, K. Johnson, M. E. O’Dwyer, B. J. Druker, Exp. Hematol.
30, 729 (2002).24. Y. Y. Wang et al., Proc. Natl. Acad. Sci. U.S.A. 102, 1104 (2005).25. Y. Y. Wang et al., Proc. Natl. Acad. Sci. U.S.A. 108, 2450 (2011).26. G. B. Zhou et al., Blood 109, 3441 (2007).
Figure 2. A potential synergistic targeted therapy for CML (A). Mechanism of action of oridonin in t(8;21) AML (B).

35sect ion four
Translational medicine is a popular term for the bench-to-bed-side ‘translation’ of basic scientific research into practicable diagnostic procedures and therapies, with meaningful im-provements in physical, mental, or social health outcomes.
Translational research is the underlying basis for translational medi-cine, which hopes to turn evidence-based medicine into sustainable solutions for public health problems. Both basic and clinical scientists are committed to moving translational research from the laboratory to clinical application, although there may be some differences in how they define the tenants of “from bench-to-bedside” and “from bedside-to-bench-to-bedside.” Basic scientists who want to translate their ba-sic research results into clinical practice can find it a frustratingly long process, often taking 10 to 20 years. It is a real challenge to shorten this timeframe. For clinical scientists, translational research begins at the bedside before going to the bench; their main focus is therefore on benefitting the patient’s well-being. However, some phenomena cannot be explained only through clinical data. For example, before starting a clinical trial, hypotheses are formed based on epidemiologi-cal investigation, and a trial is designed with the hope of improving a patient’s prognosis. The trials are then planned and carried out using strict protocols and rigorous testing; however, the results are not always what one expects. It can be difficult to determine the reasons behind the discrepancies, and researchers often need to turn back to basic research to solve these issues, come up with new ideas, and design another trial in hopes of resolving the issues.
Oral cancer is one of the most common cancers of the head and neck region, with about 300,000 new cases worldwide each year, and the incidence continues to increase. The five-year survival rate for patients diagnosed with oral cancer is 50%–60%, and even lower for patients diagnosed in the later clinical stages. Early discovery, early diagno-sis, and early treatment are keys to improving a patient’s prognosis. Even though efforts have been made to improve the prognosis for oral cancer, few have been successful. More clinical trial studies looking at better management of treatment protocols are currently under way, focusing on induction chemotherapy, new drugs, and new techniques, amongst others.
We focus our translational research primarily on the optimization of treatment protocols as well as on early diagnosis of oral cancer. Developing clinical trial treatment protocols and biobanking (collection of tissue, blood, and saliva samples) in collaboration with basic researchers are some of the most important aspects of our
research. For example, we have started a clinical trial using targeted induction chemotherapy as a presurgical treatment for localized, advanced oral squamous cell carcinoma; the control group receives surgery plus postoperative radiotherapy. We plan to evaluate the presurgical treatment response and correlate these effects with genomic and proteomic studies, with the aim of finding markers that predict the response of preoperative treatment and help guide clinicians in choosing the best preoperative regimens. We hope this will improve the prognosis for patients with oral cancer.
As surgeons, our strategies focus on early diagnosis, optimization of personalized treatment protocols, and prognosis prediction. We’ve started clinical trials to optimize clinical treatment protocols for oral cancer, as described above. Initial results indicate that the local and regional recurrence rate is 4% higher in the induction chemotherapy group than the control group. We’ve now turned to basic research to help elucidate why this is the case and plan to compare genomic, pro-teomic, and metabolic analysis with follow-up patient data, such as lo-cal recurrence and survival rates.
Personalized treatment protocols based on an individual patient’s needs could ideally enhance their prognosis. We hope our basic research studies might uncover new biomarkers for early diagnosis and prognos-tic prediction, which could then help guide the selection of treatment protocols. An ideal cancer biomarker could be used to screen healthy or high-risk populations, diagnose the specific type of cancer, predict the patient’s prognosis, and monitor remission during recovery or while receiving surgery, radiation, chemotherapy, or biotherapy. Our strategy for the early diagnosis of oral cancer will be based on genomic, tran-scriptomic, proteomic, peptidomic, and metabolomic studies to identify potential biomarkers using serum, tissue, saliva, or urine. For treatment protocols, we want to identify potential biomarkers that are predictive of treatment response and prognosis. Using the results from these stud-ies, we will design new clinical trials to confirm whether the biomarkers are useful for predicting treatment response and guiding the selection of treatment protocols. We have established a biobank of more than 3,500 oral cancer samples from fresh tissue, serum, and saliva from oral cancer patients; more than 2,000 samples from pre-cancer patients from fresh lesion, serum, and saliva; and more than 4,000 formalin-fixed tis-sue samples are added each year from oral and maxillofacial tumors. We have also established a database of follow-up studies for clinical researchers that is more than 95% complete.
In summary, translational medicine plays a critical role in bridging the gap between basic and clinical research. For oral cancer, our translational medicine strategy is based on our clinical expertise and using basic research methods to search for biomarkers that can be useful in early diagnosis and treatment response, and prognosis prediction, with the aim of enhancing treatment protocols and improving patient outcomes.
Translational Medicine in Oral CancerLai-ping Zhong, M.D., Ph.D. and Zhi-yuan Zhang, M.D.*
Department of Oral and Maxillofacial SurgeryNinth People’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China*Corresponding Author: [email protected]
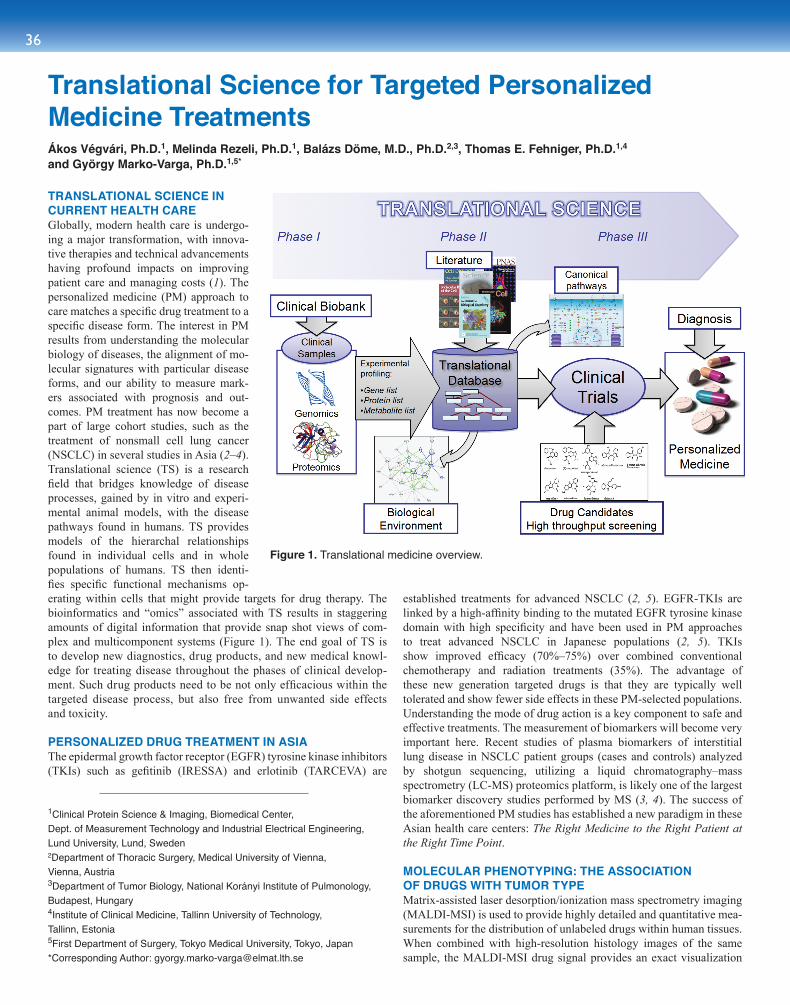
36
TRANSLATIONAL SCIENCE IN CURRENT HEALTH CARE Globally, modern health care is undergo-ing a major transformation, with innova-tive therapies and technical advancements having profound impacts on improving patient care and managing costs (1). The personalized medicine (PM) approach to care matches a specific drug treatment to a specific disease form. The interest in PM results from understanding the molecular biology of diseases, the alignment of mo-lecular signatures with particular disease forms, and our ability to measure mark-ers associated with prognosis and out-comes. PM treatment has now become a part of large cohort studies, such as the treatment of nonsmall cell lung cancer (NSCLC) in several studies in Asia (2–4). Translational science (TS) is a research field that bridges knowledge of disease processes, gained by in vitro and experi-mental animal models, with the disease pathways found in humans. TS provides models of the hierarchal relationships found in individual cells and in whole populations of humans. TS then identi-fies specific functional mechanisms op-erating within cells that might provide targets for drug therapy. The bioinformatics and “omics” associated with TS results in staggering amounts of digital information that provide snap shot views of com-plex and multicomponent systems (Figure 1). The end goal of TS is to develop new diagnostics, drug products, and new medical knowl-edge for treating disease throughout the phases of clinical develop-ment. Such drug products need to be not only efficacious within the targeted disease process, but also free from unwanted side effects and toxicity.
PERSONALIZED DRUG TREATMENT IN ASIAThe epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) such as gefitinib (IRESSA) and erlotinib (TARCEVA) are
established treatments for advanced NSCLC (2, 5). EGFR-TKIs are linked by a high-affinity binding to the mutated EGFR tyrosine kinase domain with high specificity and have been used in PM approaches to treat advanced NSCLC in Japanese populations (2, 5). TKIs show improved efficacy (70%–75%) over combined conventional chemotherapy and radiation treatments (35%). The advantage of these new generation targeted drugs is that they are typically well tolerated and show fewer side effects in these PM-selected populations. Understanding the mode of drug action is a key component to safe and effective treatments. The measurement of biomarkers will become very important here. Recent studies of plasma biomarkers of interstitial lung disease in NSCLC patient groups (cases and controls) analyzed by shotgun sequencing, utilizing a liquid chromatography–mass spectrometry (LC-MS) proteomics platform, is likely one of the largest biomarker discovery studies performed by MS (3, 4). The success of the aforementioned PM studies has established a new paradigm in these Asian health care centers: The Right Medicine to the Right Patient at the Right Time Point.
MOLECULAR PHENOTYPING: THE ASSOCIATION OF DRUGS WITH TUMOR TYPE Matrix-assisted laser desorption/ionization mass spectrometry imaging (MALDI-MSI) is used to provide highly detailed and quantitative mea-surements for the distribution of unlabeled drugs within human tissues. When combined with high-resolution histology images of the same sample, the MALDI-MSI drug signal provides an exact visualization
Translational Science for Targeted Personalized Medicine Treatments Ákos Végvári, Ph.D.1, Melinda Rezeli, Ph.D.1, Balázs Döme, M.D., Ph.D.2,3, Thomas E. Fehniger, Ph.D.1,4 and György Marko-Varga, Ph.D.1,5*
1Clinical Protein Science & Imaging, Biomedical Center, Dept. of Measurement Technology and Industrial Electrical Engineering, Lund University, Lund, Sweden2Department of Thoracic Surgery, Medical University of Vienna, Vienna, Austria3Department of Tumor Biology, National Korányi Institute of Pulmonology, Budapest, Hungary4Institute of Clinical Medicine, Tallinn University of Technology, Tallinn, Estonia5First Department of Surgery, Tokyo Medical University, Tokyo, Japan*Corresponding Author: [email protected]
Figure 1. Translational medicine overview.
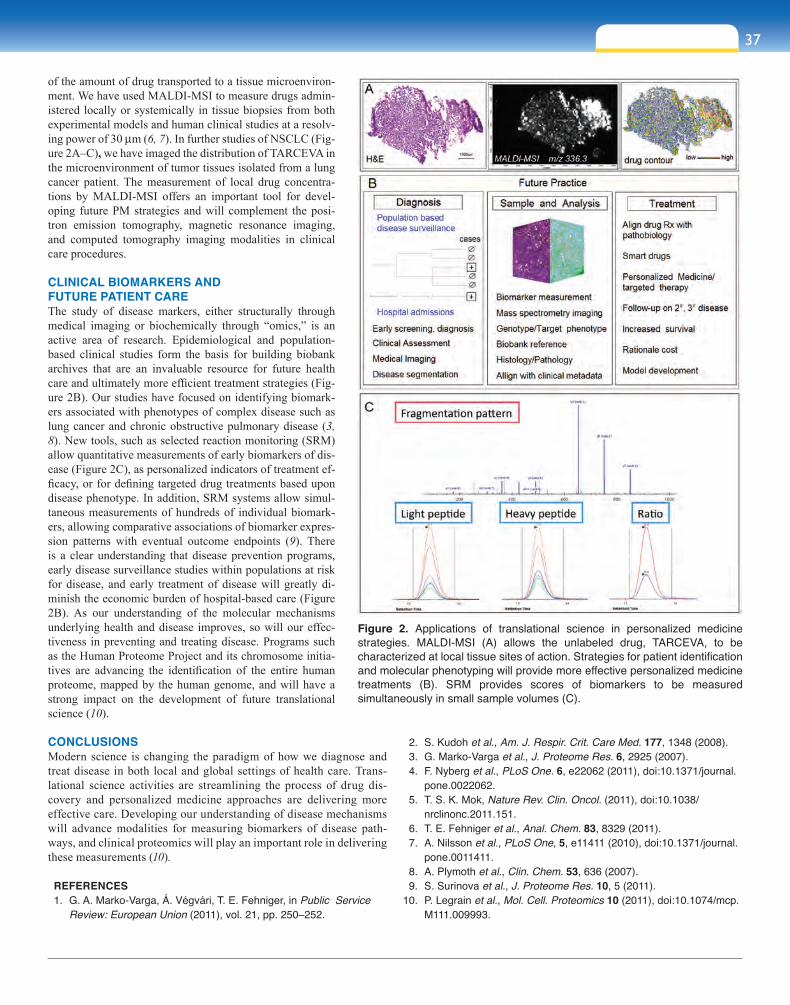
37sect ion four
of the amount of drug transported to a tissue microenviron-ment. We have used MALDI-MSI to measure drugs admin-istered locally or systemically in tissue biopsies from both experimental models and human clinical studies at a resolv-ing power of 30 mm (6, 7). In further studies of NSCLC (Fig-ure 2A–C), we have imaged the distribution of TARCEVA in the microenvironment of tumor tissues isolated from a lung cancer patient. The measurement of local drug concentra-tions by MALDI-MSI offers an important tool for devel-oping future PM strategies and will complement the posi-tron emission tomography, magnetic resonance imaging, and computed tomography imaging modalities in clinical care procedures.
CLINICAL BIOMARKERS AND FUTURE PATIENT CAREThe study of disease markers, either structurally through medical imaging or biochemically through “omics,” is an active area of research. Epidemiological and population-based clinical studies form the basis for building biobank archives that are an invaluable resource for future health care and ultimately more efficient treatment strategies (Fig-ure 2B). Our studies have focused on identifying biomark-ers associated with phenotypes of complex disease such as lung cancer and chronic obstructive pulmonary disease (3, 8). New tools, such as selected reaction monitoring (SRM) allow quantitative measurements of early biomarkers of dis-ease (Figure 2C), as personalized indicators of treatment ef-ficacy, or for defining targeted drug treatments based upon disease phenotype. In addition, SRM systems allow simul-taneous measurements of hundreds of individual biomark-ers, allowing comparative associations of biomarker expres-sion patterns with eventual outcome endpoints (9). There is a clear understanding that disease prevention programs, early disease surveillance studies within populations at risk for disease, and early treatment of disease will greatly di-minish the economic burden of hospital-based care (Figure 2B). As our understanding of the molecular mechanisms underlying health and disease improves, so will our effec-tiveness in preventing and treating disease. Programs such as the Human Proteome Project and its chromosome initia-tives are advancing the identification of the entire human proteome, mapped by the human genome, and will have a strong impact on the development of future translational science (10).
CONCLUSIONSModern science is changing the paradigm of how we diagnose and treat disease in both local and global settings of health care. Trans-lational science activities are streamlining the process of drug dis-covery and personalized medicine approaches are delivering more effective care. Developing our understanding of disease mechanisms will advance modalities for measuring biomarkers of disease path-ways, and clinical proteomics will play an important role in delivering these measurements (10).
REFERENCES 1. G. A. Marko-Varga, Á. Végvári, T. E. Fehniger, in Public Service
Review: European Union (2011), vol. 21, pp. 250–252.
2. S. Kudoh et al., Am. J. Respir. Crit. Care Med. 177, 1348 (2008). 3. G. Marko-Varga et al., J. Proteome Res. 6, 2925 (2007). 4. F. Nyberg et al., PLoS One. 6, e22062 (2011), doi:10.1371/journal.
pone.0022062. 5. T. S. K. Mok, Nature Rev. Clin. Oncol. (2011), doi:10.1038/
nrclinonc.2011.151. 6. T. E. Fehniger et al., Anal. Chem. 83, 8329 (2011). 7. A. Nilsson et al., PLoS One, 5, e11411 (2010), doi:10.1371/journal.
pone.0011411. 8. A. Plymoth et al., Clin. Chem. 53, 636 (2007). 9. S. Surinova et al., J. Proteome Res. 10, 5 (2011).10. P. Legrain et al., Mol. Cell. Proteomics 10 (2011), doi:10.1074/mcp.
M111.009993.
Figure 2. Applications of translational science in personalized medicine strategies. MALDI-MSI (A) allows the unlabeled drug, TARCEVA, to be characterized at local tissue sites of action. Strategies for patient identification and molecular phenotyping will provide more effective personalized medicine treatments (B). SRM provides scores of biomarkers to be measured simultaneously in small sample volumes (C).

38
Stroke is emerging as the second most common cause of pre-ventable death and disability in adults around the world (1). It is now well-recognized that stroke is a major cause of death in developing countries, and that approximately 80% of all
deaths by stroke occur in these nations (2–4). China has the largest global population, and experiences 40% of all stroke deaths in develop-ing countries; stroke is a leading cause of death and disability.
Stroke is characterized by high incidence, mortality, morbidity, and recurrence. It is estimated that over 1.5 million people in China will have a stroke or transient ischemic attack (TIA) each year. The mortal-ity rate after the first stroke is nearly one-third. Among stroke survivors, nearly 90% will have a neurological deficit. Within the following three months, nearly 20% of patients who experienced a TIA will have a stroke (5-7). Ischemic stroke accounts for ap-proximately 80% of all the stroke sub-types. Early restoration of the ischemic penumbra plays a key role in the salva-tion of brain function.
Acute ischemic stroke can be treated in the emergency room of a hospital. Time is of the essence in stroke care. Current stroke treatment strategy has two modality suggestions available: in-travenous thrombolysis (IVT) that can be applied within 4.5 hours from onset of symptoms, and intra-arterial throm-bolysis (IAT) which will work within an extended time window of up to 12 hours. For IVT, a recent meta-analysis systematically reviewed the current cost-effectiveness data on thromboly-sis by IVT with recombinant tissue plasminogen activator (rtPA) for acute ischemic stroke, and confirmed that rtPA is effective for acute stroke within 4.5 hours (8). For IAT, a combination of multiple modalities can be used includ-ing microcatheter drug infusion, direct stent implantation, stent/balloon an-gioplasty, and endovascular thrombec-tomy. IAT has advantages over IVT, including a smaller dose require-ment to reach a high local concentration, a treatment window that can be appropriately extended, and higher recanalization rates. However, IAT largely depends on technical expertise, and carries additional risks and expense.
In the past decade, new endovascular thrombectomy devices have been developed and widely used in the treatment of acute ischemic stroke, including the Microwire, MERCI, Phonon Clot Retriever, Alli-gator Retrieval Device, Catch, and Solitaire retriever. Based on our 10-
year data set of 527 IAT cases, overall recanalization was 71% (internal carotid artery/middle cerebral artery occlusion: 257 cases; and vertebral artery/basilar artery occlusion: 270 cases). Post-IAT complications pre-sented as intracranial hemorrhage in 58 cases (11%), stroke/death after 30 days in 72 cases (13.7%), and stroke/death after 30 days to one year in 14 cases (2.7%). In light of the high complication rate, the role of these devices must be vigorous evaluated and the use of thrombolysis for acute ischemic stroke must be considered, that is, should thromboly-sis be a primary treatment or more of a disease management solution?
Good care of patients after a stroke starts with the organization of the entire stroke chain from the prehospital scene, through the emer-gency room, to the stroke unit. Therefore, a novel management system
for acute ischemic stroke thrombolysis was conceived and introduced, based on actual clinical treatment at the stroke center of Xuanwu Hos-pital (9). The most important concepts in this novel management sys-tem were the thrombolysis chain and thrombolysis unit. This model aims to integrate all of these clinical resources and establish an effec-tive management system, which is critical for the safety and efficacy of thrombolysis for acute ischemic stroke (Figure 1).
Since the 1980s, China has made huge progress in both social and economic status; however, with economic development, inequalities emerge. There are many factors associated with socioeconomic im-balances that may lead to differences in the public health service and education. In China, among all 13,600 medical centers, only 117 are qualified to carry out emergency interventional thrombolysis (10). Over 95% of these medical centers are located in Eastern China. Both the
China International Neuroscience Institute (CHINA-INI)Beijing Xuanwu hospital, Beijing Capital Medical University, Beijing, China*Corresponding Author: [email protected]
Cerebro- and Cardiovascular Diseases: Collaborations Between Basic and Clinical Studies
Figure 1.
sect ion f i ve
Advanced Rescue for Acute Ischemic StrokeFeng Ling, M.D. and Peng Gao, M.D.
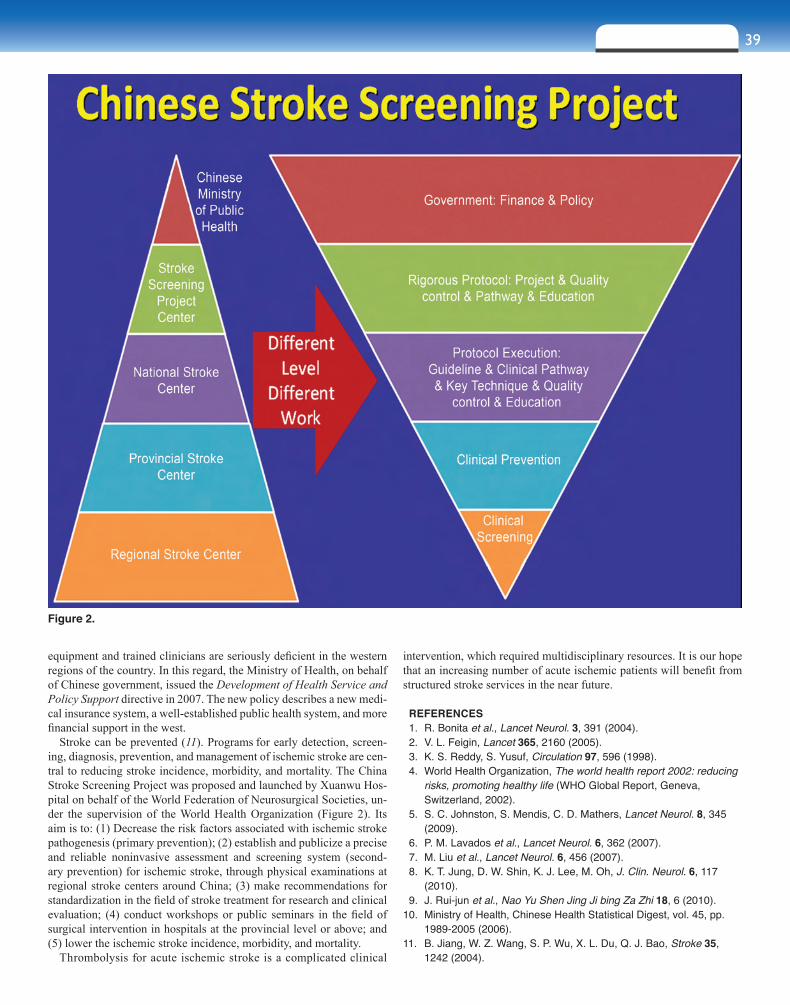
sec t ion f i ve 39
equipment and trained clinicians are seriously deficient in the western regions of the country. In this regard, the Ministry of Health, on behalf of Chinese government, issued the Development of Health Service and Policy Support directive in 2007. The new policy describes a new medi-cal insurance system, a well-established public health system, and more financial support in the west.
Stroke can be prevented (11). Programs for early detection, screen-ing, diagnosis, prevention, and management of ischemic stroke are cen-tral to reducing stroke incidence, morbidity, and mortality. The China Stroke Screening Project was proposed and launched by Xuanwu Hos-pital on behalf of the World Federation of Neurosurgical Societies, un-der the supervision of the World Health Organization (Figure 2). Its aim is to: (1) Decrease the risk factors associated with ischemic stroke pathogenesis (primary prevention); (2) establish and publicize a precise and reliable noninvasive assessment and screening system (second-ary prevention) for ischemic stroke, through physical examinations at regional stroke centers around China; (3) make recommendations for standardization in the field of stroke treatment for research and clinical evaluation; (4) conduct workshops or public seminars in the field of surgical intervention in hospitals at the provincial level or above; and (5) lower the ischemic stroke incidence, morbidity, and mortality.
Thrombolysis for acute ischemic stroke is a complicated clinical
intervention, which required multidisciplinary resources. It is our hope that an increasing number of acute ischemic patients will benefit from structured stroke services in the near future.
REFERENCES 1. R. Bonita et al., Lancet Neurol. 3, 391 (2004). 2. V. L. Feigin, Lancet 365, 2160 (2005). 3. K. S. Reddy, S. Yusuf, Circulation 97, 596 (1998). 4. World Health Organization, The world health report 2002: reducing
risks, promoting healthy life (WHO Global Report, Geneva, Switzerland, 2002).
5. S. C. Johnston, S. Mendis, C. D. Mathers, Lancet Neurol. 8, 345 (2009).
6. P. M. Lavados et al., Lancet Neurol. 6, 362 (2007). 7. M. Liu et al., Lancet Neurol. 6, 456 (2007). 8. K. T. Jung, D. W. Shin, K. J. Lee, M. Oh, J. Clin. Neurol. 6, 117
(2010). 9. J. Rui-jun et al., Nao Yu Shen Jing Ji bing Za Zhi 18, 6 (2010).10. Ministry of Health, Chinese Health Statistical Digest, vol. 45, pp.
1989-2005 (2006).11. B. Jiang, W. Z. Wang, S. P. Wu, X. L. Du, Q. J. Bao, Stroke 35,
1242 (2004).
Figure 2.
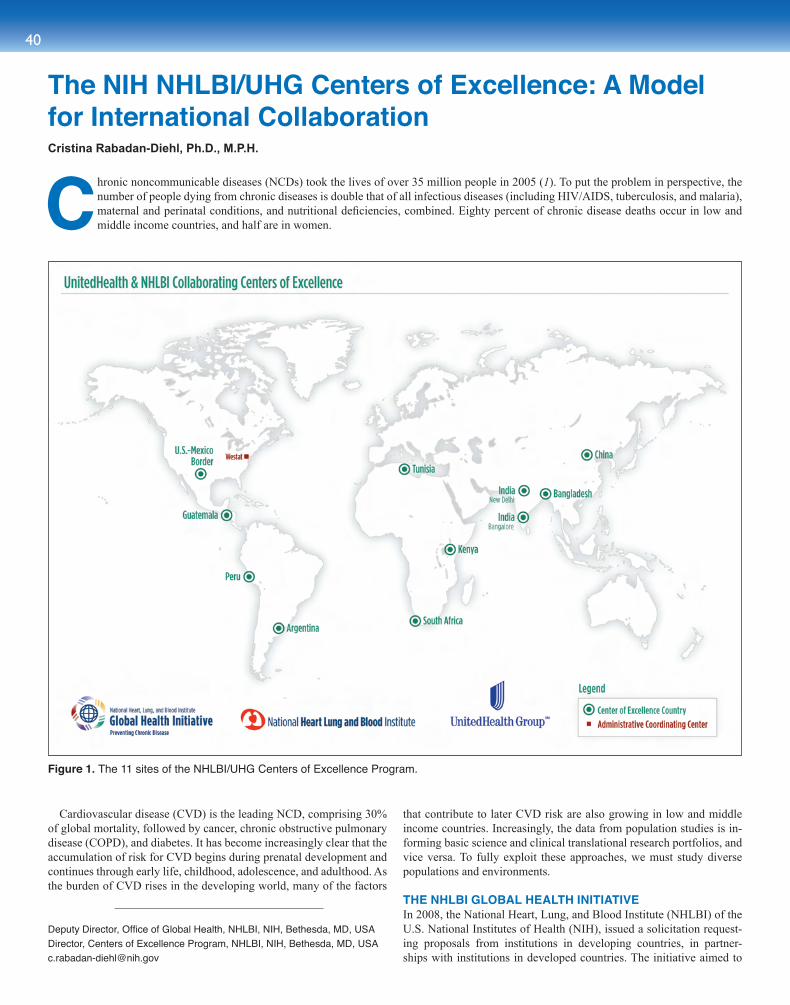
40
Cardiovascular disease (CVD) is the leading NCD, comprising 30% of global mortality, followed by cancer, chronic obstructive pulmonary disease (COPD), and diabetes. It has become increasingly clear that the accumulation of risk for CVD begins during prenatal development and continues through early life, childhood, adolescence, and adulthood. As the burden of CVD rises in the developing world, many of the factors
that contribute to later CVD risk are also growing in low and middle income countries. Increasingly, the data from population studies is in-forming basic science and clinical translational research portfolios, and vice versa. To fully exploit these approaches, we must study diverse populations and environments.
THE NHLBI GLOBAL HEALTH INITIATIVEIn 2008, the National Heart, Lung, and Blood Institute (NHLBI) of the U.S. National Institutes of Health (NIH), issued a solicitation request-ing proposals from institutions in developing countries, in partner-ships with institutions in developed countries. The initiative aimed to
The NIH NHLBI/UHG Centers of Excellence: A Model for International CollaborationCristina Rabadan-Diehl, Ph.D., M.P.H.
Figure 1. The 11 sites of the NHLBI/UHG Centers of Excellence Program.
Chronic noncommunicable diseases (NCDs) took the lives of over 35 million people in 2005 (1). To put the problem in perspective, the number of people dying from chronic diseases is double that of all infectious diseases (including HIV/AIDS, tuberculosis, and malaria), maternal and perinatal conditions, and nutritional deficiencies, combined. Eighty percent of chronic disease deaths occur in low and middle income countries, and half are in women.
Deputy Director, Office of Global Health, NHLBI, NIH, Bethesda, MD, USA Director, Centers of Excellence Program, NHLBI, NIH, Bethesda, MD, [email protected]

sec t ion f i ve 41
establish collaborating Centers of Excellence for Cardiovascular and Pulmonary research in developing countries. In June 2009, NHLBI, in collaboration with UnitedHealth Group (UHG), established a network of 11 Centers of Excellence (COE) across the globe (Figure 1). The goals of this 11-center network program are to enable research capac-ity building, train future chronic cardiovascular and pulmonary disease investigators, and conduct research, programs, and measures to prevent or treat chronic cardiovascular and pulmonary diseases (2). Network members include institutions and researchers from developing coun-tries (Argentina, Bangladesh, China, Guatemala, two India centers, Kenya, Peru, South Africa, Tunisia, and the U.S.-Mexico Border); aca-demic and research institutions in the United States, Canada, Australia, United Kingdom, and Finland; and a coordinating Center (Westat) in the United States. Each COE conducts research and training activities. The research activities, while focused on the specific country’s needs and populations, are extremely relevant to many other countries, in-cluding developed countries such as the United States. Some of the research involves questions related to epidemiological surveillance, dietary factors, effects of indoor air pollution, primary and secondary prevention, and the validation of better and more cost-effective screen-ing tools for identifying high-risk patients for CVD. Many of the COEs are leveraging their expertise and infrastructures built in the arenas of maternal/child health and infectious diseases, to develop and carry out the NCD agenda. This approach opens tremendous opportunities for future research and partnerships with other stakeholders.
The COEs are not only engaging in research collaborations across their regions and the world, but are in close communication with local, state, and national governments and policymakers. Training and capac-ity building is an important pillar of this program. Training programs include short training courses in chronic disease epidemiology, clinical research biostatistics, mentorship programs, scholarships, and Master’s degree programs.
THE CHINA INTERNATIONAL CENTER FOR CHRONIC DISEASE PREVENTION Cardiovascular diseases are currently the leading cause of death in both urban and rural China, responsible for about 2.6 million deaths annu-ally. By 2020, this figure is projected to increase to 4 million deaths per year. A recent report from the World Bank (3) addresses the importance of controlling chronic disease in China, not only from the health and social perspectives, but also highlighting the economic consequences if no immediate action is taken.
Elevated blood pressure is the single most important determinant of CVD in China and its importance is greatest in rural and northern regions, where salt consumption and the incidence of stroke are both very high. The NHLBI/UHG-funded Center of Excellence in China
is located at the George Institute in Beijing (4). In collaboration with Peking University Health Science Center, the China COE is an interna-tional network with partners in five different provinces in China (Hebei, Liaoning, Ningxia, Shaanxi, and Shanxi), the United States (Duke Uni-versity), United Kingdom (Imperial College of London), and Australia (The George Institute for International Health, The University of Syd-ney, and the University of Queensland).
The China COE is funded to implement the China Rural Health Ini-tiative (CRHI). The CRHI is evaluating the effects of two interventions: (1) a primary care–based high cardiovascular risk management package delivered by village doctors, and (2) a community-based sodium reduc-tion program, delivered by community health educators with a local supply of low-sodium salt. The community-based sodium reduction program has recently received additional funding from the U.S. Cen-ters for Disease Control and Prevention (CDC) through an interagency agreement with the NHLBI. In addition to research, the China COE provides local research training, has developed programs for visiting local and international fellows and scholars, and has mechanisms to strengthen capacity in human subject regulatory affairs. Once a year the COE sponsors a Forum on Chronic Disease and Health Policy Round Tables, in partnership with the China Ministry of Health, targeted main-ly to policymakers and key opinion leaders.
SUMMARYThe NHLBI/UnitedHealth Group Centers of Excellence network is a model for NCDs research and training in developing countries. The program is receiving domestic and international attention and it is con-sidered a unique and innovative model of research collaboration at the global level. Given the current epidemic of NCDs worldwide, there is a need to develop and provide effective, feasible, and sustainable approaches aimed at the prevention and control of NCDs. The COE program is designed to serve as a platform to develop research-based evidence for strategies that can be implemented not only in developing countries, but can also inform research agendas across the world.
REFERENCES 1. World Health Organization, Preventing chronic diseases: a vital
investment (WHO Global Report, Geneva, Switzerland, 2005; http://www.who.int/chp/chronic_disease_report/part2_ch1/en/index4.html).
2. http://www.nhlbi.nih.gov/about/globalhealth/centers/index.htm 3. The World Bank, Toward a healthy and harmonious life in China:
the rising tide of non-communicable diseases (World Bank Report 62318-CN, 2011; http://www.worldbank.org/content/dam/Worldbank/document/NCD_report_en.pdf).
4. http://www.georgeinstitute.org.cn/our-work-china/CICCDP
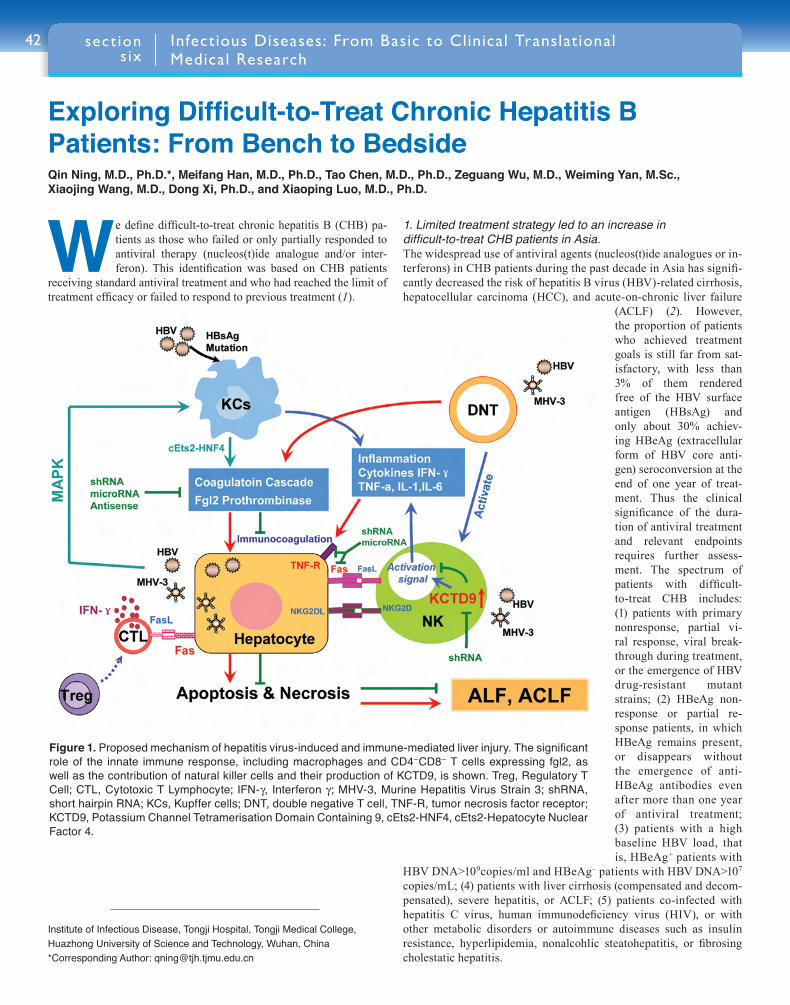
42
We define difficult-to-treat chronic hepatitis B (CHB) pa-tients as those who failed or only partially responded to antiviral therapy (nucleos(t)ide analogue and/or inter-feron). This identification was based on CHB patients
receiving standard antiviral treatment and who had reached the limit of treatment efficacy or failed to respond to previous treatment (1).
1. Limited treatment strategy led to an increase in difficult-to-treat CHB patients in Asia.The widespread use of antiviral agents (nucleos(t)ide analogues or in-terferons) in CHB patients during the past decade in Asia has signifi-cantly decreased the risk of hepatitis B virus (HBV)-related cirrhosis, hepatocellular carcinoma (HCC), and acute-on-chronic liver failure
(ACLF) (2). However, the proportion of patients who achieved treatment goals is still far from sat-isfactory, with less than 3% of them rendered free of the HBV surface antigen (HBsAg) and only about 30% achiev-ing HBeAg (extracellular form of HBV core anti-gen) seroconversion at the end of one year of treat-ment. Thus the clinical significance of the dura-tion of antiviral treatment and relevant endpoints requires further assess-ment. The spectrum of patients with difficult-to-treat CHB includes: (1) patients with primary nonresponse, partial vi-ral response, viral break-through during treatment, or the emergence of HBV drug-resistant mutant strains; (2) HBeAg non-response or partial re-sponse patients, in which HBeAg remains present, or disappears without the emergence of anti-HBeAg antibodies even after more than one year of antiviral treatment; (3) patients with a high baseline HBV load, that is, HBeAg+ patients with
HBV DNA>109copies/ml and HBeAg– patients with HBV DNA>107
copies/mL; (4) patients with liver cirrhosis (compensated and decom-pensated), severe hepatitis, or ACLF; (5) patients co-infected with hepatitis C virus, human immunodeficiency virus (HIV), or with other metabolic disorders or autoimmune diseases such as insulin resistance, hyperlipidemia, nonalcohlic steatohepatitis, or fibrosing cholestatic hepatitis.
Figure 1. Proposed mechanism of hepatitis virus-induced and immune-mediated liver injury. The significant role of the innate immune response, including macrophages and CD4–CD8– T cells expressing fgl2, as well as the contribution of natural killer cells and their production of KCTD9, is shown. Treg, Regulatory T Cell; CTL, Cytotoxic T Lymphocyte; IFN-g, Interferon g; MHV-3, Murine Hepatitis Virus Strain 3; shRNA, short hairpin RNA; KCs, Kupffer cells; DNT, double negative T cell, TNF-R, tumor necrosis factor receptor; KCTD9, Potassium Channel Tetramerisation Domain Containing 9, cEts2-HNF4, cEts2-Hepatocyte Nuclear Factor 4.
Infectious Diseases: From Basic to Clinical Translational Medical Research
Institute of Infectious Disease, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China*Corresponding Author: [email protected]
sect ion s ix
ExploringDifficult-to-TreatChronicHepatitisBPatients: From Bench to BedsideQin Ning, M.D., Ph.D.*, Meifang Han, M.D., Ph.D., Tao Chen, M.D., Ph.D., Zeguang Wu, M.D., Weiming Yan, M.Sc., Xiaojing Wang, M.D., Dong Xi, Ph.D., and Xiaoping Luo, M.D., Ph.D.
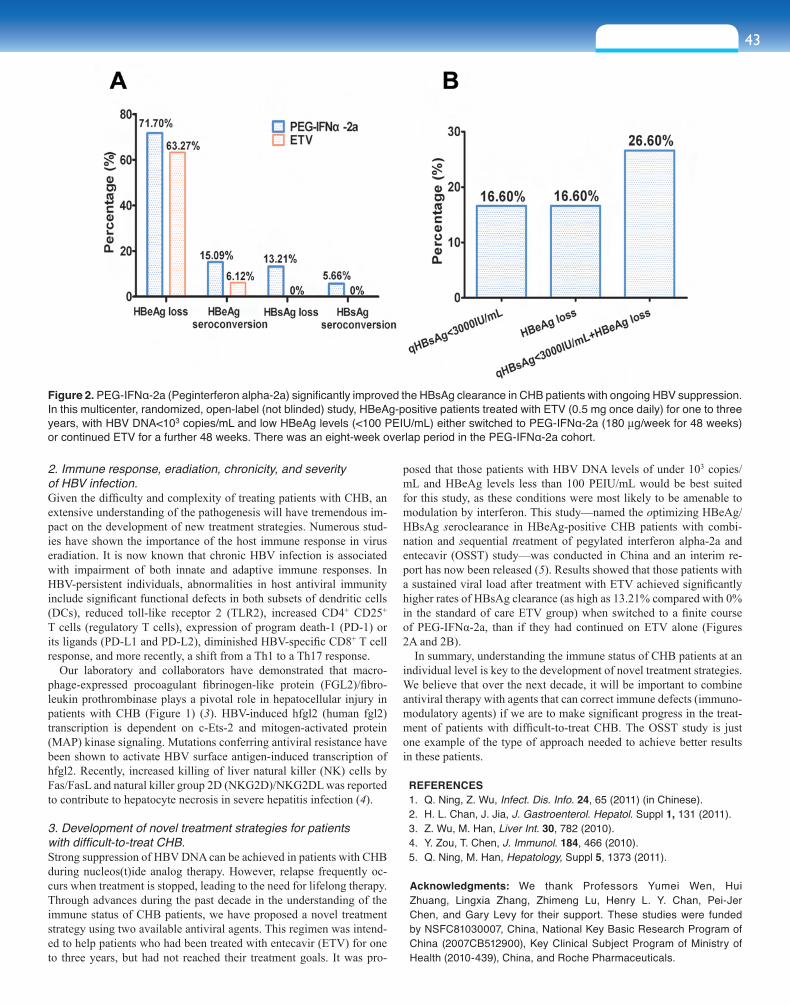
43sect ion s ix
2. Immune response, eradiation, chronicity, and severity of HBV infection.Given the difficulty and complexity of treating patients with CHB, an extensive understanding of the pathogenesis will have tremendous im-pact on the development of new treatment strategies. Numerous stud-ies have shown the importance of the host immune response in virus eradiation. It is now known that chronic HBV infection is associated with impairment of both innate and adaptive immune responses. In HBV-persistent individuals, abnormalities in host antiviral immunity include significant functional defects in both subsets of dendritic cells (DCs), reduced toll-like receptor 2 (TLR2), increased CD4+ CD25+ T cells (regulatory T cells), expression of program death-1 (PD-1) or its ligands (PD-L1 and PD-L2), diminished HBV-specific CD8+ T cell response, and more recently, a shift from a Th1 to a Th17 response.
Our laboratory and collaborators have demonstrated that macro-phage-expressed procoagulant fibrinogen-like protein (FGL2)/fibro-leukin prothrombinase plays a pivotal role in hepatocellular injury in patients with CHB (Figure 1) (3). HBV-induced hfgl2 (human fgl2) transcription is dependent on c-Ets-2 and mitogen-activated protein (MAP) kinase signaling. Mutations conferring antiviral resistance have been shown to activate HBV surface antigen-induced transcription of hfgl2. Recently, increased killing of liver natural killer (NK) cells by Fas/FasL and natural killer group 2D (NKG2D)/NKG2DL was reported to contribute to hepatocyte necrosis in severe hepatitis infection (4).
3. Development of novel treatment strategies for patients with difficult-to-treat CHB.Strong suppression of HBV DNA can be achieved in patients with CHB during nucleos(t)ide analog therapy. However, relapse frequently oc-curs when treatment is stopped, leading to the need for lifelong therapy. Through advances during the past decade in the understanding of the immune status of CHB patients, we have proposed a novel treatment strategy using two available antiviral agents. This regimen was intend-ed to help patients who had been treated with entecavir (ETV) for one to three years, but had not reached their treatment goals. It was pro-
posed that those patients with HBV DNA levels of under 103 copies/mL and HBeAg levels less than 100 PEIU/mL would be best suited for this study, as these conditions were most likely to be amenable to modulation by interferon. This study—named the optimizing HBeAg/HBsAg seroclearance in HBeAg-positive CHB patients with combi-nation and sequential treatment of pegylated interferon alpha-2a and entecavir (OSST) study—was conducted in China and an interim re-port has now been released (5). Results showed that those patients with a sustained viral load after treatment with ETV achieved significantly higher rates of HBsAg clearance (as high as 13.21% compared with 0% in the standard of care ETV group) when switched to a finite course of PEG-IFNα-2a, than if they had continued on ETV alone (Figures 2A and 2B).
In summary, understanding the immune status of CHB patients at an individual level is key to the development of novel treatment strategies. We believe that over the next decade, it will be important to combine antiviral therapy with agents that can correct immune defects (immuno-modulatory agents) if we are to make significant progress in the treat-ment of patients with difficult-to-treat CHB. The OSST study is just one example of the type of approach needed to achieve better results in these patients.
REFERENCES 1. Q. Ning, Z. Wu, Infect. Dis. Info. 24, 65 (2011) (in Chinese). 2. H. L. Chan, J. Jia, J. Gastroenterol. Hepatol. Suppl 1, 131 (2011). 3. Z. Wu, M. Han, Liver Int. 30, 782 (2010). 4. Y. Zou, T. Chen, J. Immunol. 184, 466 (2010). 5. Q. Ning, M. Han, Hepatology, Suppl 5, 1373 (2011).
Acknowledgments: We thank Professors Yumei Wen, Hui Zhuang, Lingxia Zhang, Zhimeng Lu, Henry L. Y. Chan, Pei-Jer Chen, and Gary Levy for their support. These studies were funded by NSFC81030007, China, National Key Basic Research Program of China (2007CB512900), Key Clinical Subject Program of Ministry of Health (2010-439), China, and Roche Pharmaceuticals.
Figure 2. PEG-IFNα-2a (Peginterferon alpha-2a) significantly improved the HBsAg clearance in CHB patients with ongoing HBV suppression. In this multicenter, randomized, open-label (not blinded) study, HBeAg-positive patients treated with ETV (0.5 mg once daily) for one to three years, with HBV DNA<103 copies/mL and low HBeAg levels (<100 PEIU/mL) either switched to PEG-IFNα-2a (180 mg/week for 48 weeks) or continued ETV for a further 48 weeks. There was an eight-week overlap period in the PEG-IFNα-2a cohort.

44
After 30 years of unprec-edented global control efforts, there are still around three million
new HIV infections and two mil-lion AIDS deaths each year around the world (1). The global AIDS pan-demic is characterized by its wide range of HIV prevalence in various adult populations (from over 30% to less than 0.1%) and the genetic diversities (two sera-types, dozens of clades, and hundreds of circulat-ing recombinants forms). There is no single effective measure to con-trol HIV transmission. It is believed that an effective HIV vaccine is the only solution for achieving full con-trol of HIV/AIDS.
In the past 25 years, all conven-tional and modern vaccine tech-niques have been applied to HIV vaccine research. There remains neither a vaccine nor easy path to success in sight. Historically, the major hurdle in vaccine develop-ment has not been making the vac-cine itself, but rather finding the right pathogen, since traditional vaccines can be produced by follow-ing standardized procedures to kill or attenuate the original pathogens. There is no need for sophisticated vaccine design or to understand the mechanism of immune protection. However, conventional vaccine technologies work well only for the diseases that can induce protective immunity in humans during natural infection, so-called nature-born vaccines (Figure 1). Unfortunately, HIV falls into another category of infections, which do not induce enough protective immunity in the host. In natural hepatitis A or B virus infections, most adult humans can elim-inate the virus and become virus-free sera convertors (2, 3). So far, not a single virus-free sera convertor with HIV has ever been confirmed. The biggest barrier to a successful HIV vaccine is to empower the ineffec-tive human immune system to defend against HIV infection. Therefore, the key is not only to beat the virus, but to catch up with evolution.
HIV vaccine research at the Chinese Center for Disease Control and Prevention is based on the hypothesis that one can induce protective
immunity by either redesigning the HIV immunogen or modulating the host immune response to HIV infection. Practically, there are four working strategies to follow: (1) Systematically screening the circulat-ing HIV-1 strains to identify the predominant vaccine strain (4); (2) studying the correlation of immune protection of the world’s first len-tivirus vaccine, the equine infectious anemia virus (EIAV) vaccine, to shed light how to design an HIV vaccine (HIV is one of eight known lentiviruses) (5, 6); (3) improving HIV vaccine immunogenicity by re-designing conserved regions and utilizing novel immunization proto-cols (7); and (4) carefully selecting a vaccine vector with a balanced risk to benefit ratio. Based on these principles, the most predominant HIV-1 clade in China was found to be the CRF07 B’/C HIV-1 and this was used to build vaccine candidates. The replication competent Tian-tan vaccinia (TV) was chosen to be the major vector, due to its strong immunogenicity and good safety records throughout extended use in hundreds of millions of people in China during the smallpox eradica-tion campaign (8).
In collaboration with scientists who developed the EIAV vaccine, we found that the broader T cell and neutralizing antibody (nAb) responses are related to the vaccine’s protection (9). A string of amino acids in the conserved region of the envelope glycoprotein (env) of HIV-1 was genetically modified based on the same region in the env of highly im-munogenic EIAV vaccine strains, giving that HIV-1 env a similar con-formation to the EIAV vaccine strain env protein. The purpose of the modification was to enhance the immunogenicity of the HIV env pro-
AIDS Vaccine Research, from Basic Research to Clinical StudyYiming Shao, M.D., Ph.D.1,*, Ying Liu, Ph.D.1, Jing Xu, M.Med.2, Taisheng Li, M.D.3, Yong Liu, Ph.D.1, Yanling Hao, Ph.D.1, Hua Liang, M.D.1, Kunxue Hong, M.D.1, Lianxin Liu, Ph.D.1, Kaifan Dai, Ph.D.1, Li Ren, M.D.1, Xiang He, Ph.D.1, and Rongxian Shen, B.S.4
1National Center for AIDS/STD Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, China2National Vaccine and Serum Institute, Beijing, China3Peking Union Medical College Hospital, Beijing, China4Harbin Veterinary Research Institute, Chinese Academy of Agricultural Sciences, Beijing, China*Corresponding Author: [email protected]
Figure 1. A Tale of Two Cities—the fundamental differences between two types of vaccine research pathways.
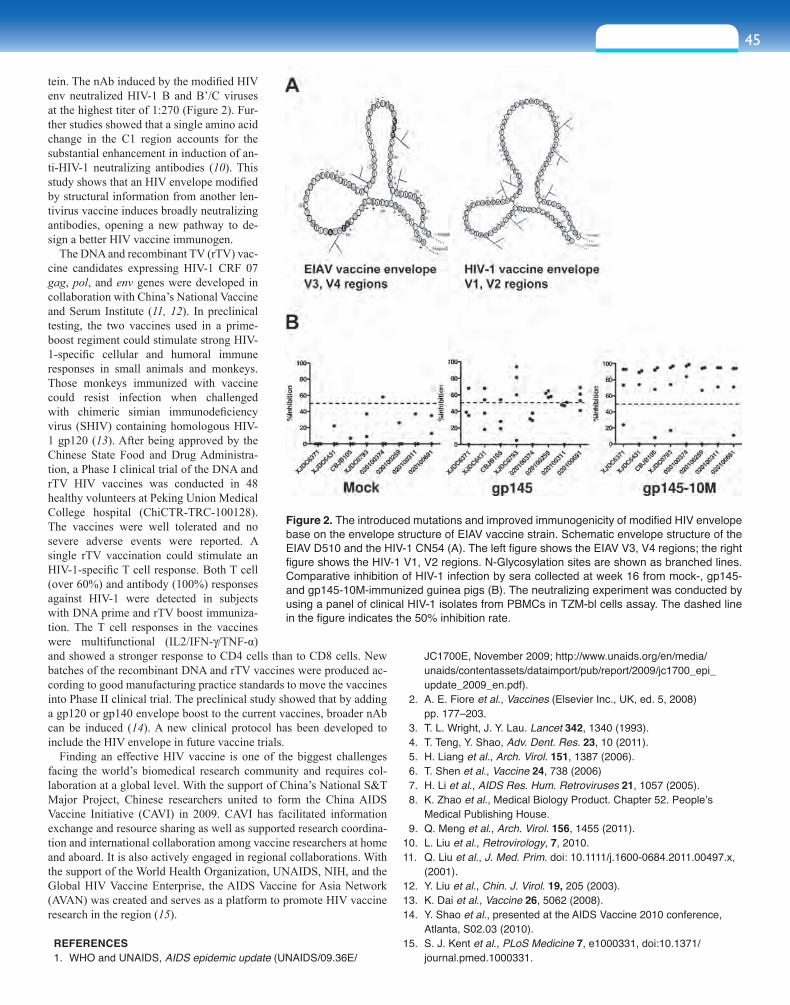
45sect ion s ix
tein. The nAb induced by the modified HIV env neutralized HIV-1 B and B’/C viruses at the highest titer of 1:270 (Figure 2). Fur-ther studies showed that a single amino acid change in the C1 region accounts for the substantial enhancement in induction of an-ti-HIV-1 neutralizing antibodies (10). This study shows that an HIV envelope modified by structural information from another len-tivirus vaccine induces broadly neutralizing antibodies, opening a new pathway to de-sign a better HIV vaccine immunogen.
The DNA and recombinant TV (rTV) vac-cine candidates expressing HIV-1 CRF 07 gag, pol, and env genes were developed in collaboration with China’s National Vaccine and Serum Institute (11, 12). In preclinical testing, the two vaccines used in a prime-boost regiment could stimulate strong HIV-1-specific cellular and humoral immune responses in small animals and monkeys. Those monkeys immunized with vaccine could resist infection when challenged with chimeric simian immunodeficiency virus (SHIV) containing homologous HIV-1 gp120 (13). After being approved by the Chinese State Food and Drug Administra-tion, a Phase I clinical trial of the DNA and rTV HIV vaccines was conducted in 48 healthy volunteers at Peking Union Medical College hospital (ChiCTR-TRC-100128). The vaccines were well tolerated and no severe adverse events were reported. A single rTV vaccination could stimulate an HIV-1-specific T cell response. Both T cell (over 60%) and antibody (100%) responses against HIV-1 were detected in subjects with DNA prime and rTV boost immuniza-tion. The T cell responses in the vaccines were multifunctional (IL2/IFN-g/TNF-α) and showed a stronger response to CD4 cells than to CD8 cells. New batches of the recombinant DNA and rTV vaccines were produced ac-cording to good manufacturing practice standards to move the vaccines into Phase II clinical trial. The preclinical study showed that by adding a gp120 or gp140 envelope boost to the current vaccines, broader nAb can be induced (14). A new clinical protocol has been developed to include the HIV envelope in future vaccine trials.
Finding an effective HIV vaccine is one of the biggest challenges facing the world’s biomedical research community and requires col-laboration at a global level. With the support of China’s National S&T Major Project, Chinese researchers united to form the China AIDS Vaccine Initiative (CAVI) in 2009. CAVI has facilitated information exchange and resource sharing as well as supported research coordina-tion and international collaboration among vaccine researchers at home and aboard. It is also actively engaged in regional collaborations. With the support of the World Health Organization, UNAIDS, NIH, and the Global HIV Vaccine Enterprise, the AIDS Vaccine for Asia Network (AVAN) was created and serves as a platform to promote HIV vaccine research in the region (15).
REFERENCES 1. WHO and UNAIDS, AIDS epidemic update (UNAIDS/09.36E/
JC1700E, November 2009; http://www.unaids.org/en/media/unaids/contentassets/dataimport/pub/report/2009/jc1700_epi_update_2009_en.pdf).
2. A. E. Fiore et al., Vaccines (Elsevier Inc., UK, ed. 5, 2008) pp. 177–203.
3. T. L. Wright, J. Y. Lau. Lancet 342, 1340 (1993). 4. T. Teng, Y. Shao, Adv. Dent. Res. 23, 10 (2011). 5. H. Liang et al., Arch. Virol. 151, 1387 (2006). 6. T. Shen et al., Vaccine 24, 738 (2006) 7. H. Li et al., AIDS Res. Hum. Retroviruses 21, 1057 (2005). 8. K. Zhao et al., Medical Biology Product. Chapter 52. People’s
Medical Publishing House. 9. Q. Meng et al., Arch. Virol. 156, 1455 (2011).10. L. Liu et al., Retrovirology, 7, 2010.11. Q. Liu et al., J. Med. Prim. doi: 10.1111/j.1600-0684.2011.00497.x,
(2001).12. Y. Liu et al., Chin. J. Virol. 19, 205 (2003).13. K. Dai et al., Vaccine 26, 5062 (2008).14. Y. Shao et al., presented at the AIDS Vaccine 2010 conference,
Atlanta, S02.03 (2010).15. S. J. Kent et al., PLoS Medicine 7, e1000331, doi:10.1371/
journal.pmed.1000331.
Figure 2. The introduced mutations and improved immunogenicity of modified HIV envelope base on the envelope structure of EIAV vaccine strain. Schematic envelope structure of the EIAV D510 and the HIV-1 CN54 (A). The left figure shows the EIAV V3, V4 regions; the right figure shows the HIV-1 V1, V2 regions. N-Glycosylation sites are shown as branched lines. Comparative inhibition of HIV-1 infection by sera collected at week 16 from mock-, gp145- and gp145-10M-immunized guinea pigs (B). The neutralizing experiment was conducted by using a panel of clinical HIV-1 isolates from PBMCs in TZM-bl cells assay. The dashed line in the figure indicates the 50% inhibition rate.
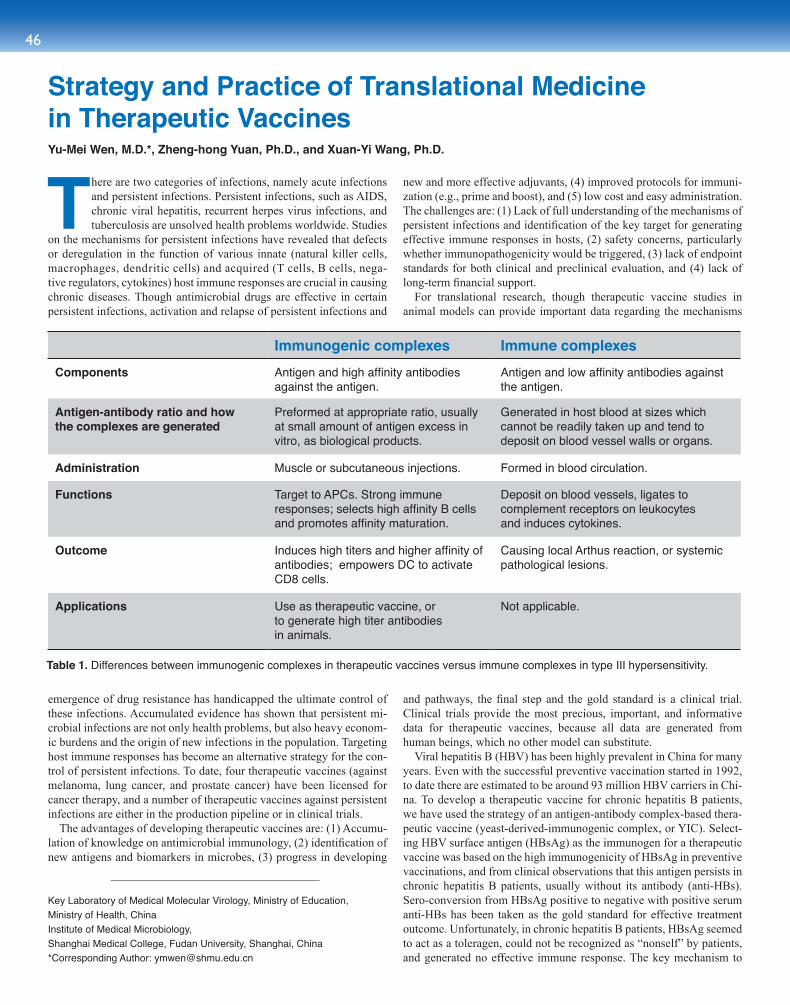
46
There are two categories of infections, namely acute infections and persistent infections. Persistent infections, such as AIDS, chronic viral hepatitis, recurrent herpes virus infections, and tuberculosis are unsolved health problems worldwide. Studies
on the mechanisms for persistent infections have revealed that defects or deregulation in the function of various innate (natural killer cells, macrophages, dendritic cells) and acquired (T cells, B cells, nega-tive regulators, cytokines) host immune responses are crucial in causing chronic diseases. Though antimicrobial drugs are effective in certain persistent infections, activation and relapse of persistent infections and
emergence of drug resistance has handicapped the ultimate control of these infections. Accumulated evidence has shown that persistent mi-crobial infections are not only health problems, but also heavy econom-ic burdens and the origin of new infections in the population. Targeting host immune responses has become an alternative strategy for the con-trol of persistent infections. To date, four therapeutic vaccines (against melanoma, lung cancer, and prostate cancer) have been licensed for cancer therapy, and a number of therapeutic vaccines against persistent infections are either in the production pipeline or in clinical trials.
The advantages of developing therapeutic vaccines are: (1) Accumu-lation of knowledge on antimicrobial immunology, (2) identification of new antigens and biomarkers in microbes, (3) progress in developing
new and more effective adjuvants, (4) improved protocols for immuni-zation (e.g., prime and boost), and (5) low cost and easy administration. The challenges are: (1) Lack of full understanding of the mechanisms of persistent infections and identification of the key target for generating effective immune responses in hosts, (2) safety concerns, particularly whether immunopathogenicity would be triggered, (3) lack of endpoint standards for both clinical and preclinical evaluation, and (4) lack of long-term financial support.
For translational research, though therapeutic vaccine studies in animal models can provide important data regarding the mechanisms
and pathways, the final step and the gold standard is a clinical trial. Clinical trials provide the most precious, important, and informative data for therapeutic vaccines, because all data are generated from human beings, which no other model can substitute.
Viral hepatitis B (HBV) has been highly prevalent in China for many years. Even with the successful preventive vaccination started in 1992, to date there are estimated to be around 93 million HBV carriers in Chi-na. To develop a therapeutic vaccine for chronic hepatitis B patients, we have used the strategy of an antigen-antibody complex-based thera-peutic vaccine (yeast-derived-immunogenic complex, or YIC). Select-ing HBV surface antigen (HBsAg) as the immunogen for a therapeutic vaccine was based on the high immunogenicity of HBsAg in preventive vaccinations, and from clinical observations that this antigen persists in chronic hepatitis B patients, usually without its antibody (anti-HBs). Sero-conversion from HBsAg positive to negative with positive serum anti-HBs has been taken as the gold standard for effective treatment outcome. Unfortunately, in chronic hepatitis B patients, HBsAg seemed to act as a toleragen, could not be recognized as “nonself” by patients, and generated no effective immune response. The key mechanism to
Immunogenic complexes Immune complexes Components Antigen and high affinity antibodies
against the antigen.Antigen and low affinity antibodies against the antigen.
Antigen-antibody ratio and how the complexes are generated
Preformed at appropriate ratio, usually at small amount of antigen excess in vitro, as biological products.
Generated in host blood at sizes which cannot be readily taken up and tend to deposit on blood vessel walls or organs.
Administration Muscle or subcutaneous injections. Formed in blood circulation.
Functions Target to APCs. Strong immune responses; selects high affinity B cells and promotes affinity maturation.
Deposit on blood vessels, ligates to complement receptors on leukocytesand induces cytokines.
Outcome Induces high titers and higher affinity of antibodies; empowers DC to activate CD8 cells.
Causing local Arthus reaction, or systemic pathological lesions.
Applications Use as therapeutic vaccine, or to generate high titer antibodies in animals.
Not applicable.
Strategy and Practice of Translational Medicine in Therapeutic VaccinesYu-Mei Wen, M.D.*, Zheng-hong Yuan, Ph.D., and Xuan-Yi Wang, Ph.D.
Key Laboratory of Medical Molecular Virology, Ministry of Education,Ministry of Health, China Institute of Medical Microbiology,Shanghai Medical College, Fudan University, Shanghai, China*Corresponding Author: [email protected]
Table 1. Differences between immunogenic complexes in therapeutic vaccines versus immune complexes in type III hypersensitivity.
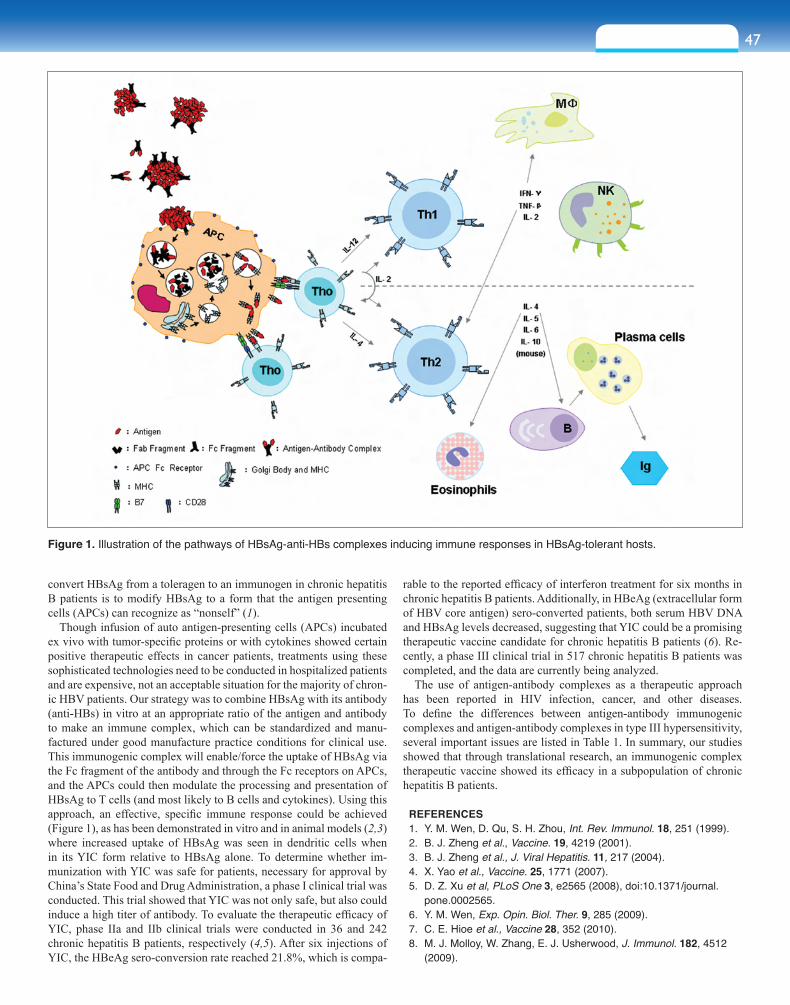
47sect ion s ix
convert HBsAg from a toleragen to an immunogen in chronic hepatitis B patients is to modify HBsAg to a form that the antigen presenting cells (APCs) can recognize as “nonself” (1).
Though infusion of auto antigen-presenting cells (APCs) incubated ex vivo with tumor-specific proteins or with cytokines showed certain positive therapeutic effects in cancer patients, treatments using these sophisticated technologies need to be conducted in hospitalized patients and are expensive, not an acceptable situation for the majority of chron-ic HBV patients. Our strategy was to combine HBsAg with its antibody (anti-HBs) in vitro at an appropriate ratio of the antigen and antibody to make an immune complex, which can be standardized and manu-factured under good manufacture practice conditions for clinical use. This immunogenic complex will enable/force the uptake of HBsAg via the Fc fragment of the antibody and through the Fc receptors on APCs, and the APCs could then modulate the processing and presentation of HBsAg to T cells (and most likely to B cells and cytokines). Using this approach, an effective, specific immune response could be achieved (Figure 1), as has been demonstrated in vitro and in animal models (2,3) where increased uptake of HBsAg was seen in dendritic cells when in its YIC form relative to HBsAg alone. To determine whether im-munization with YIC was safe for patients, necessary for approval by China’s State Food and Drug Administration, a phase I clinical trial was conducted. This trial showed that YIC was not only safe, but also could induce a high titer of antibody. To evaluate the therapeutic efficacy of YIC, phase IIa and IIb clinical trials were conducted in 36 and 242 chronic hepatitis B patients, respectively (4,5). After six injections of YIC, the HBeAg sero-conversion rate reached 21.8%, which is compa-
rable to the reported efficacy of interferon treatment for six months in chronic hepatitis B patients. Additionally, in HBeAg (extracellular form of HBV core antigen) sero-converted patients, both serum HBV DNA and HBsAg levels decreased, suggesting that YIC could be a promising therapeutic vaccine candidate for chronic hepatitis B patients (6). Re-cently, a phase III clinical trial in 517 chronic hepatitis B patients was completed, and the data are currently being analyzed.
The use of antigen-antibody complexes as a therapeutic approach has been reported in HIV infection, cancer, and other diseases. To define the differences between antigen-antibody immunogenic complexes and antigen-antibody complexes in type III hypersensitivity, several important issues are listed in Table 1. In summary, our studies showed that through translational research, an immunogenic complex therapeutic vaccine showed its efficacy in a subpopulation of chronic hepatitis B patients.
REFERENCES 1. Y. M. Wen, D. Qu, S. H. Zhou, Int. Rev. Immunol. 18, 251 (1999). 2. B. J. Zheng et al., Vaccine. 19, 4219 (2001). 3. B. J. Zheng et al., J. Viral Hepatitis. 11, 217 (2004). 4. X. Yao et al., Vaccine. 25, 1771 (2007). 5. D. Z. Xu et al, PLoS One 3, e2565 (2008), doi:10.1371/journal.
pone.0002565. 6. Y. M. Wen, Exp. Opin. Biol. Ther. 9, 285 (2009). 7. C. E. Hioe et al., Vaccine 28, 352 (2010). 8. M. J. Molloy, W. Zhang, E. J. Usherwood, J. Immunol. 182, 4512
(2009).
Figure 1. Illustration of the pathways of HBsAg-anti-HBs complexes inducing immune responses in HBsAg-tolerant hosts.
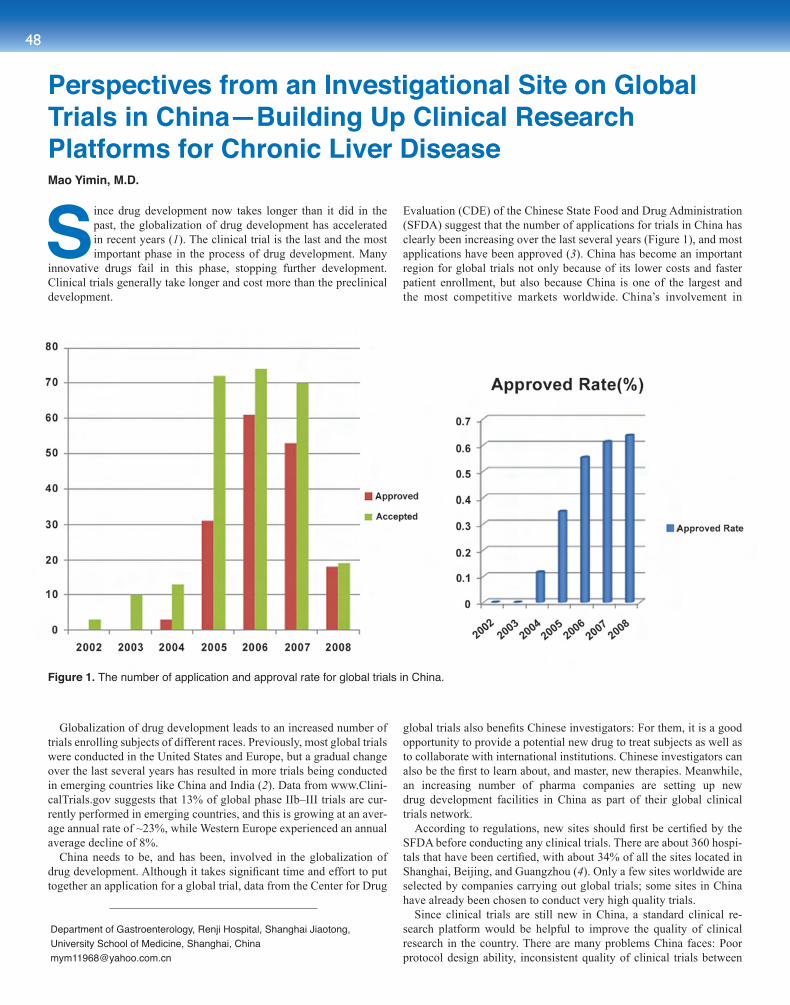
48
Since drug development now takes longer than it did in the past, the globalization of drug development has accelerated in recent years (1). The clinical trial is the last and the most important phase in the process of drug development. Many
innovative drugs fail in this phase, stopping further development. Clinical trials generally take longer and cost more than the preclinical development.
Globalization of drug development leads to an increased number of trials enrolling subjects of different races. Previously, most global trials were conducted in the United States and Europe, but a gradual change over the last several years has resulted in more trials being conducted in emerging countries like China and India (2). Data from www.Clini-calTrials.gov suggests that 13% of global phase IIb–III trials are cur-rently performed in emerging countries, and this is growing at an aver-age annual rate of ~23%, while Western Europe experienced an annual average decline of 8%.
China needs to be, and has been, involved in the globalization of drug development. Although it takes significant time and effort to put together an application for a global trial, data from the Center for Drug
Evaluation (CDE) of the Chinese State Food and Drug Administration (SFDA) suggest that the number of applications for trials in China has clearly been increasing over the last several years (Figure 1), and most applications have been approved (3). China has become an important region for global trials not only because of its lower costs and faster patient enrollment, but also because China is one of the largest and the most competitive markets worldwide. China’s involvement in
global trials also benefits Chinese investigators: For them, it is a good opportunity to provide a potential new drug to treat subjects as well as to collaborate with international institutions. Chinese investigators can also be the first to learn about, and master, new therapies. Meanwhile, an increasing number of pharma companies are setting up new drug development facilities in China as part of their global clinical trials network.
According to regulations, new sites should first be certified by the SFDA before conducting any clinical trials. There are about 360 hospi-tals that have been certified, with about 34% of all the sites located in Shanghai, Beijing, and Guangzhou (4). Only a few sites worldwide are selected by companies carrying out global trials; some sites in China have already been chosen to conduct very high quality trials.
Since clinical trials are still new in China, a standard clinical re-search platform would be helpful to improve the quality of clinical research in the country. There are many problems China faces: Poor protocol design ability, inconsistent quality of clinical trials between
Perspectives from an Investigational Site on Global Trials in China—Building Up Clinical Research Platforms for Chronic Liver Disease Mao Yimin, M.D.
Department of Gastroenterology, Renji Hospital, Shanghai Jiaotong,University School of Medicine, Shanghai, [email protected]
Figure 1. The number of application and approval rate for global trials in China.

49sect ion s ix
different sites/hospitals, a lack of clinical research coordinators and qualified nurses, limited accessibility to biostatisticians, underquali-fied clinical research associate teams, and different social and culture backgrounds. To establish a foundation for drug development by lo-cal Chinese pharmaceutical and biotech companies, and to respond to increasing international market demands, the Chinese government has invested 6.6 billion RMB (US$1.03 billion) through the National 11th Five-Year Plan (2006–2010) to set up a series of preclinical platforms and 24 global standard clinical research platforms that focus on differ-ent diseases.
Renji is one of the 24 clinical research platform sites, and its focus is chronic liver disease. The objectives of this program are: (1) To build an international normative technical platform for clinical research on new drugs for chronic liver disease, (2) to create a pilot project for the clinical development of new drugs for chronic liver disease, and (3) to establish a regional network with international research insti-tutes and to collaborate with leading global or domestic pharmaceutical companies.
The Renji clinical research platform for chronic liver disease con-sists of five subplatforms: (1) A platform for multicenter clinical re-search, which includes eight top hospitals for chronic liver disease na-tionwide; (2) a platform for data management and statistical analysis; (3) a platform for human biological and medical ethics, (4) a platform for a phase I unit; and (5) a platform for quality assurance and quality control.
The Renji platform has made great strides through this government-sponsored project. Over 750 technical regulations and standard operating procedures (SOPs) consistent with international standards have been enacted. To improve protocol design, technical guidelines for phase I to IV clinical trials of innovative drugs for chronic hepatitis B have been set up. As a leading center, and as the platform
that carries out the most trials for class I new drugs or global trials of liver disease, the Renji platform has successfully promoted drug development in China. About 50 global trials or trials for innovative drugs for liver diseases have been conducted in the platform, and most class I innovative drugs of liver diseases have received SFDA approval. The platform has also built up a clinical database with more than 10,000 different liver disease subjects. A sample bank with 4,000 blood samples and 1,000 tissue samples has also been set up.
In the National 12th Five-Year Plan (2011–2015), the Renji platform will further build upon the current platform of clinical research and translational medicine for liver diseases. Basic research including proteomics, genomics, and clinical research will be carried out for different liver diseases, such as liver fibrosis, nonalcoholic fatty liver disease/nonalcoholic steatohepatitis, and drug-induced liver disease (DILI). A technical evaluation system for DILI will be set up based on translational medicine research. Technical guidelines for phase I to IV clinical trials of innovative drugs for up to three liver diseases will be set up. The clinical database and the sample bank will be further expanded.
As China sets up more global standard clinical research platforms, it will play an increasingly important role in global trials.
REFERENCES 1. www.innovation.org/drug_discovery/drug_discovery_iframe.htm 2. F. A. Thiers, A. J. Sinskey, E. R. Berndt, Nature Rev. Drug Discov. 7, 13(2008). 3. www.cde.gov.cn (2008). 4. www.sfda.gov.cn (2010).
Acknowledgments: This work was supported by the National 11th Five-Year Plan of China 2008ZX09312-007.
FIRST ANNOUNCEMENT 2012 Sino-American Symposium on Clinical and Translational Medicine
The 3rd 2012 Sino-American Symposium on Clinical and Translational Medicine has been scheduled for June 27 - 29, 2012, in Shanghai and multiple other cities in China.
We sincerely invite distinguish speakers for 2012 SAS-CTM. All presentations will be in English. We warmly welcome all clinical and translational research experts and specialists to join us.
The Mission: Translational Medicine and Better Health Care
The core themes covered will be: 1. International Collaboration on Clinical and Translational Research Practice 2. Education and Professional Trainings on Clinical and Translational Medicine 3. Chronic Diseases and New Therapeutics Development 4. “4P” Medicine and Outcomes 5. Partnerships with Industry and Multidisciplinary Participation
For more details please visit www.ChinaCTS.org
or contact Dr. Tim Shi, international coordinator for the Co-Organizers’ Committee:
50
Mental disorders are one of the most significant causes of illness worldwide, with their human and economic costs exceeding those
of infectious, cardiovascular, or neoplastic diseases. The issue of mental illness has become particularly topical in China (1), where psychological examinations may even be introduced into the selection procedure for leaders of national industries. On the one hand, the recent surge in mental illness has been blamed on pressure resulting from the social transformation accompanying the country’s unprecedented economic growth. On the other hand, a series of recent major natural disasters may have contributed to the increasing number of certain psychiatric disorders, particularly posttraumatic stress disorder, depression, and anxiety. For instance, it has been shown that the Sichuan earthquake resulted in functional changes in the brains of survivors (Figure 1) (2). To date, the major obstacle to the more effective diagnosis and treatment of mental illnesses worldwide has been our poor understanding of the underlying neuropathophysiology, and in particular the lack of objective biomarkers for diagnosis and prognosis.
Magnetic resonance (MR) imaging allows the noninvasive investigation of brain structure and function in vivo, and is well-suited to the study of psychiatric patients. Using high-field MR imaging (i.e., 3.0 Tesla MR), a team at the Huaxi MR Research Center (HMRRC, www.hmrrc.org.cn) at the West China Hospital has been investigating the structural (3–5) and functional (2, 6–10) correlates of psychiatric disorders. By developing and applying a number of novel approaches and techniques for the acquisition and analysis of MR imaging data, the HMRRC group has carried out prospective studies on imaging biomarkers in populations that are at high-risk of developing mental disorders, and diagnostic biomarkers of mental disorders and underlying pathological mechanisms. The results provide the first step towards the translational use of high-field MR imaging for diagnosis, prediction of treatment response, and monitoring therapeutic effects.
A significant amount of work carried out by the HMRRC group has focused on depression, a common and debilitating psychiatric
disorder with an unclear etiology and com-plex and variable clinical manifestations. If objective diagnostic and prognostic markers of this disorder could be identified, the clini-cal management of patients would be markedly improved.
Research into depression has generally focused on two major clinical issues: suicidality (7) and refractoriness (6, 8). Studies have revealed microstructural abnormalities associated with suicidality amongst patients with major depression (7); more specifically, they have provided evidence for altered frontal-striatal circuits passing via the anterior limb of the internal capsule (Figure 2). These potentially disrupted connections are in areas regulating affect and behavior, and might trigger the onset of depression and confer a biological vulnerability, which in combination with environmental stressors could result in suicidal behaviors.
Secondly, the above studies have revealed differences in pathophysiology in patients who either do or do not respond to antidepressant treatment. About 30% of patients do not respond to standard antidepressant treatment and are classified as having refractory depression, while those who respond are
considered to have nonrefractory depression. Studies carried out by the HMRRC group revealed differences in functional connectivity related to treatment responsiveness, with the nonrefractory group showing a decrease mainly in the limbic-striatal-pallidal-thalamic circuits, and the refractory group showing a decrease mainly in thalamo-cortical circuits (8). Taken together, these findings suggest that refractory depression may be associated predominantly with disrupted connectivity in thalamo-cortical circuits. This may in part explain why patients with refractory depression are resistant to standard antidepressants but respond well to treatments targeting frontal areas (8).
More recently, the HMRRC team has revealed disrupted topological organization of intrinsic functional brain networks during rest in patients with depression (9). In light of the sensitivity of resting-state functional MR imaging to neuronal alterations associated with medication (10), further work needs to be done to investigate the therapeutic effect of antidepressants on the brains of patients with depression. In addition, the use of novel analytical methods that allow inferences to be made at an individual rather than group level may facilitate the translational impact of the results (5).
In summary, reflecting the greater awareness of mental illness in the Chinese population, there has been a significant growth in efforts to better understand and treat psychiatric disorders. This is best exemplified by the current imaging research that allows us to obtain various objective “radiological signs” of mental disorders, which
Translational Magnetic Resonance Imaging Research of Mental DisordersQiyong Gong, M.D., Ph.D.1,*, Qizhu Wu, Ph.D.1, Andrea Mechelli, Ph.D.2, Su Lui, M.D., Ph.D.1, Weihong Kuang, M.D.3, Wei Zhang, M.D.3, Zhiyun Jia, M.D., Ph.D.1, Junran Zhang, Ph.D.1, Hua Ai, Ph.D.1, Tao Li, M.D.3, and Xiaoqi Huang, M.D.1
Neurological System Diseases: Clinical and Translational Research
Figure 1. A clock, in a tower, surrounded by rubble, that was stopped at 2:28 p.m. by the Wenchuan earthquake on May 12, 2008. This was China's second deadliest quake, having caused at least 69,000 deaths and 37,000 injuries. The tower sits at the central square of Hanwang town, about 50 km from the epicenter. Work by the HMRRC team at the West China Hospital revealed an acute impact on the brains of physically healthy survivors (2).
1Huaxi MR Research Center (HMRRC), Departments of Radiology, West China Hospital of Sichuan University, Chengdu, China2Department of Psychosis Studies, Institute of Psychiatry, King’s College London, London, United Kingdom3Department of Psychiatry, State Key Lab of Biotherapy, West China Hospital of Sichuan University, Chengdu, China*Corresponding Author: [email protected]
sect ion seven
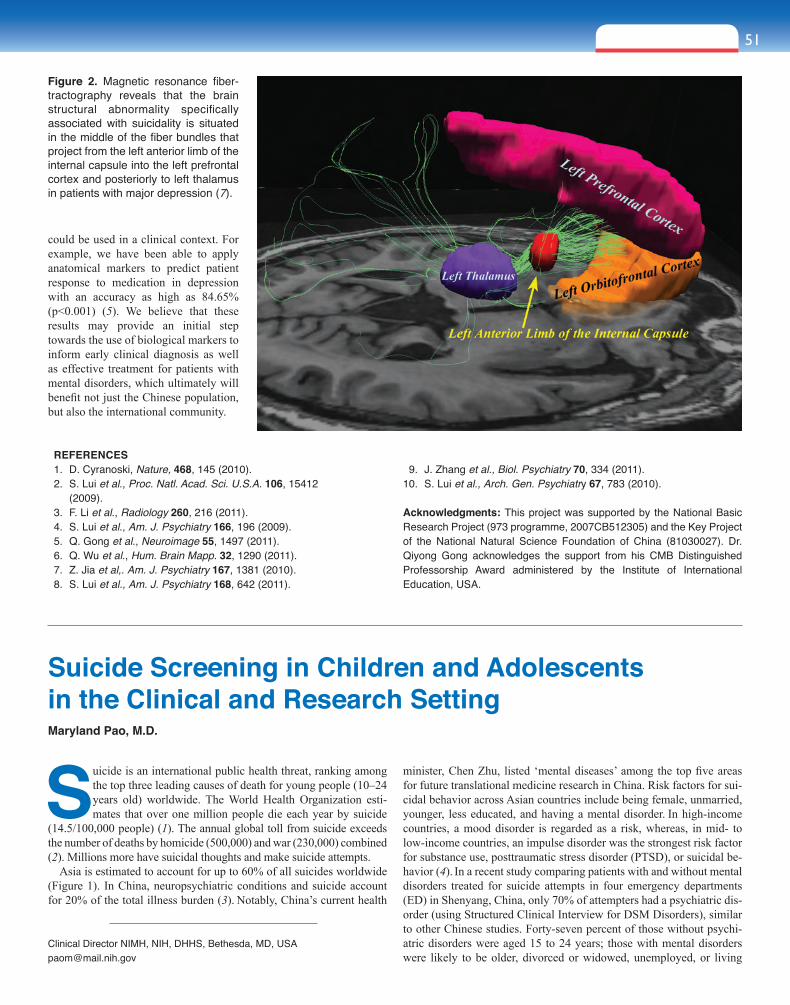
51sect ion seven
Figure 2. Magnetic resonance fiber-tractography reveals that the brain structural abnormality specifically associated with suicidality is situated in the middle of the fiber bundles that project from the left anterior limb of the internal capsule into the left prefrontal cortex and posteriorly to left thalamus in patients with major depression (7).
REFERENCES 1. D. Cyranoski, Nature, 468, 145 (2010). 2. S. Lui et al., Proc. Natl. Acad. Sci. U.S.A. 106, 15412
(2009). 3. F. Li et al., Radiology 260, 216 (2011). 4. S. Lui et al., Am. J. Psychiatry 166, 196 (2009). 5. Q. Gong et al., Neuroimage 55, 1497 (2011). 6. Q. Wu et al., Hum. Brain Mapp. 32, 1290 (2011). 7. Z. Jia et al,. Am. J. Psychiatry 167, 1381 (2010). 8. S. Lui et al., Am. J. Psychiatry 168, 642 (2011).
9. J. Zhang et al., Biol. Psychiatry 70, 334 (2011).10. S. Lui et al., Arch. Gen. Psychiatry 67, 783 (2010).
Acknowledgments: This project was supported by the National Basic Research Project (973 programme, 2007CB512305) and the Key Project of the National Natural Science Foundation of China (81030027). Dr. Qiyong Gong acknowledges the support from his CMB Distinguished Professorship Award administered by the Institute of International Education, USA.
could be used in a clinical context. For example, we have been able to apply anatomical markers to predict patient response to medication in depression with an accuracy as high as 84.65% (p<0.001) (5). We believe that these results may provide an initial step towards the use of biological markers to inform early clinical diagnosis as well as effective treatment for patients with mental disorders, which ultimately will benefit not just the Chinese population, but also the international community.
Suicide Screening in Children and Adolescents in the Clinical and Research Setting Maryland Pao, M.D.
Suicide is an international public health threat, ranking among the top three leading causes of death for young people (10–24 years old) worldwide. The World Health Organization esti-mates that over one million people die each year by suicide
(14.5/100,000 people) (1). The annual global toll from suicide exceeds the number of deaths by homicide (500,000) and war (230,000) combined (2). Millions more have suicidal thoughts and make suicide attempts.
Asia is estimated to account for up to 60% of all suicides worldwide (Figure 1). In China, neuropsychiatric conditions and suicide account for 20% of the total illness burden (3). Notably, China’s current health
minister, Chen Zhu, listed ‘mental diseases’ among the top five areas for future translational medicine research in China. Risk factors for sui-cidal behavior across Asian countries include being female, unmarried, younger, less educated, and having a mental disorder. In high-income countries, a mood disorder is regarded as a risk, whereas, in mid- to low-income countries, an impulse disorder was the strongest risk factor for substance use, posttraumatic stress disorder (PTSD), or suicidal be-havior (4). In a recent study comparing patients with and without mental disorders treated for suicide attempts in four emergency departments (ED) in Shenyang, China, only 70% of attempters had a psychiatric dis-order (using Structured Clinical Interview for DSM Disorders), similar to other Chinese studies. Forty-seven percent of those without psychi-atric disorders were aged 15 to 24 years; those with mental disorders were likely to be older, divorced or widowed, unemployed, or living
Clinical Director NIMH, NIH, DHHS, Bethesda, MD, [email protected]
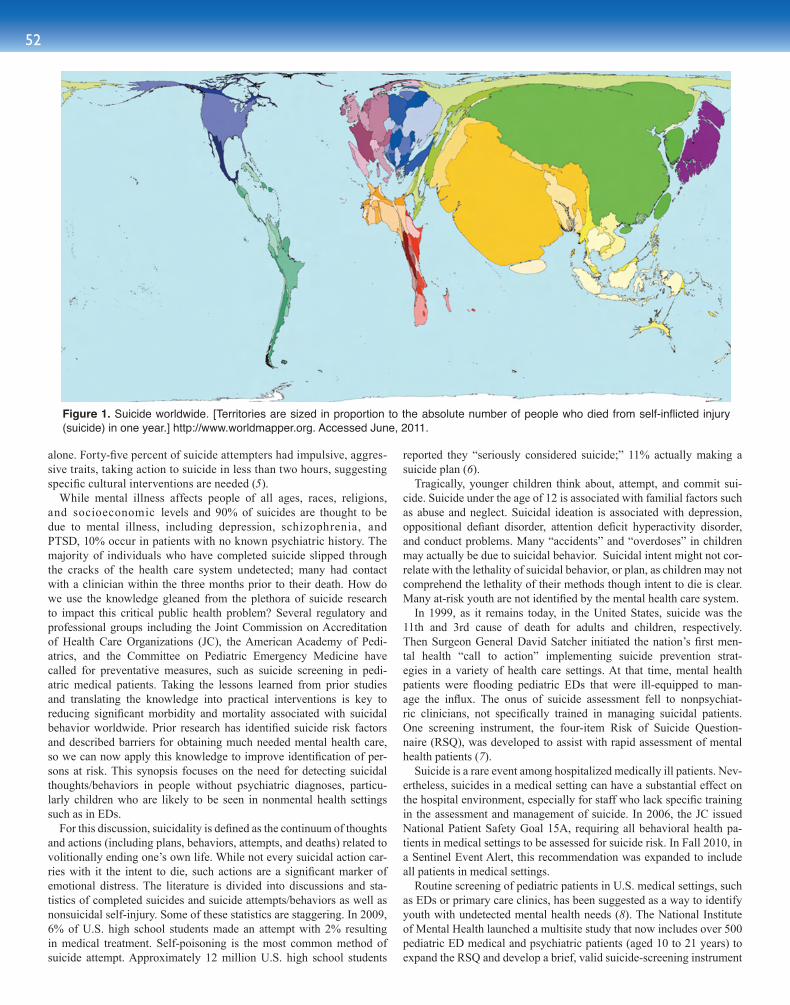
52
alone. Forty-five percent of suicide attempters had impulsive, aggres-sive traits, taking action to suicide in less than two hours, suggesting specific cultural interventions are needed (5).
While mental illness affects people of all ages, races, religions, and socioeconomic levels and 90% of suicides are thought to be due to mental illness, including depression, schizophrenia, and PTSD, 10% occur in patients with no known psychiatric history. The majority of individuals who have completed suicide slipped through the cracks of the health care system undetected; many had contact with a clinician within the three months prior to their death. How do we use the knowledge gleaned from the plethora of suicide research to impact this critical public health problem? Several regulatory and professional groups including the Joint Commission on Accreditation of Health Care Organizations (JC), the American Academy of Pedi-atrics, and the Committee on Pediatric Emergency Medicine have called for preventative measures, such as suicide screening in pedi-atric medical patients. Taking the lessons learned from prior studies and translating the knowledge into practical interventions is key to reducing significant morbidity and mortality associated with suicidal behavior worldwide. Prior research has identified suicide risk factors and described barriers for obtaining much needed mental health care, so we can now apply this knowledge to improve identification of per-sons at risk. This synopsis focuses on the need for detecting suicidal thoughts/behaviors in people without psychiatric diagnoses, particu-larly children who are likely to be seen in nonmental health settings such as in EDs.
For this discussion, suicidality is defined as the continuum of thoughts and actions (including plans, behaviors, attempts, and deaths) related to volitionally ending one’s own life. While not every suicidal action car-ries with it the intent to die, such actions are a significant marker of emotional distress. The literature is divided into discussions and sta-tistics of completed suicides and suicide attempts/behaviors as well as nonsuicidal self-injury. Some of these statistics are staggering. In 2009, 6% of U.S. high school students made an attempt with 2% resulting in medical treatment. Self-poisoning is the most common method of suicide attempt. Approximately 12 million U.S. high school students
reported they “seriously considered suicide;” 11% actually making a suicide plan (6).
Tragically, younger children think about, attempt, and commit sui-cide. Suicide under the age of 12 is associated with familial factors such as abuse and neglect. Suicidal ideation is associated with depression, oppositional defiant disorder, attention deficit hyperactivity disorder, and conduct problems. Many “accidents” and “overdoses” in children may actually be due to suicidal behavior. Suicidal intent might not cor-relate with the lethality of suicidal behavior, or plan, as children may not comprehend the lethality of their methods though intent to die is clear. Many at-risk youth are not identified by the mental health care system.
In 1999, as it remains today, in the United States, suicide was the 11th and 3rd cause of death for adults and children, respectively. Then Surgeon General David Satcher initiated the nation’s first men-tal health “call to action” implementing suicide prevention strat-egies in a variety of health care settings. At that time, mental health patients were flooding pediatric EDs that were ill-equipped to man-age the influx. The onus of suicide assessment fell to nonpsychiat-ric clinicians, not specifically trained in managing suicidal patients. One screening instrument, the four-item Risk of Suicide Question-naire (RSQ), was developed to assist with rapid assessment of mental health patients (7).
Suicide is a rare event among hospitalized medically ill patients. Nev-ertheless, suicides in a medical setting can have a substantial effect on the hospital environment, especially for staff who lack specific training in the assessment and management of suicide. In 2006, the JC issued National Patient Safety Goal 15A, requiring all behavioral health pa-tients in medical settings to be assessed for suicide risk. In Fall 2010, in a Sentinel Event Alert, this recommendation was expanded to include all patients in medical settings.
Routine screening of pediatric patients in U.S. medical settings, such as EDs or primary care clinics, has been suggested as a way to identify youth with undetected mental health needs (8). The National Institute of Mental Health launched a multisite study that now includes over 500 pediatric ED medical and psychiatric patients (aged 10 to 21 years) to expand the RSQ and develop a brief, valid suicide-screening instrument
Figure 1. Suicide worldwide. [Territories are sized in proportion to the absolute number of people who died from self-inflicted injury (suicide) in one year.] http://www.worldmapper.org. Accessed June, 2011.

53sect ion seven
for nonpsychiatric clinicians to use with all ED patients. Data is cur-rently being analyzed. In an early feasibility study from one site, 6% of medical patients were found to be at risk for suicide. Screening was deemed feasible, acceptable to parents, and nondisruptive to ED work-flow (9). Child opinion was favorable for screening with comments like “…a lot of kids, especially teenagers get sad and don’t have anyone to talk about it with, so if a kid/teen is already in the emergency room and with people who are trained, it is a good time to talk.” Additional analyses confirm that children under age 12 have suicidal thoughts and behaviors but their suicide attempt methods differ from adolescents or adults. Gender, past attempts, and health insurance status are risk factors being examined for association.
SUMMARYSuicide is an international public health threat. By translating research on suicide into practical application, suicidality can be detected in adults and youth if health care providers use direct language to in-quire. Nonpsychiatric clinicians on the frontlines could potentially detect unrecognized suicidality, but they require education and screen-ing instruments to guide them in assessment. Patients who screen positive will require effective interventions, suggesting the need for increased mental health resources in medical settings. Future research on screening and interventions in the medical setting is needed. As for global government involvement, World Suicide Prevention Day planners (10) suggest a comprehensive approach that includes a na-
tional suicide prevention plan focused on developing effective sui-cide prevention programs along with a strategy to measure the im-pact of these interventions on what could hopefully become declining suicide rates.
REFERENCES 1. World Health Organization, Suicide prevention: Live your life (WHO
Suicide Prevention Programme, 2004; http://www.who.int/mental_health/prevention/suicide/suicideprevent/en).
2. World Health Organization, Suicide huge but preventable public health problem (WHO Media Release, 2004; http://www.who.int/mediacentre/news/releases/2004/pr61/en).
3. K. C. Wei, H. C. Chua, Int. Rev. Psychiatry 20, 4354 (2008). 4. M. K. Nock et al., Br. J. Psychiatry 192, 98 (2008). 5. B. Bi et al., Gen. Hosp. Psychiatry 32, 549 (2010). 6. Centers for Disease Control and Prevention, Morbidity and
Mortality Weekly Report 57, 1–131 (2008). 7. L. M. Horowitz et al., Pediatrics 107, 1133 (2001). 8. C. A. King, R. M. O’Mara, C. N. Hayward, R. M. Cunningham,
Acad. Emerg. Med. 16, 1234 (2009). 9. L. M. Horowitz et al., Pediatr. Emerg. Care 26, 787 (2010).10. A. L. Beautrais, B. L. Mishara, Crisis 29, 59 (2008).
Acknowledgments: Thanks to L. Horowitz. This research was supported by the NIMH Intramural Research Program.
We sought to determine which parental cell type was best suited for creating reprogrammed induced pluripotent stem cells (iPSCs) and what differences might exist be-tween iPSCs generated from various tissues. To do this,
we reprogrammed primary mouse astrocytes, a central nervous system derived cell, into astrocyte-derived iPSCs (mAsiPSCs) using ectopic expression of Oct3/4, Sox2, Klf4, and c-Myc. These mAsiPSCs ex-pressed stem cell markers and formed teratomas. Importantly, mA-siPSCs grew more slowly and were more likely to differentiate into neuronal-type cells compared to mouse embryonic fibroblast-derived iPSCs (MEFsiPSCs), a noncentral nervous system-derived cell type. These results suggest that mAsiPSCs retain a “memory” of their central nervous system origin and may have a higher incidence of neuronal dif-ferentiation. Moreover, direct conversion of somatic cells into lineage-specific progenitor cells in one step, bypassing the intermediated plu-ripotent stage, provides an alternative strategy for generating promising cell types. We demonstrated the conversion of adult dermal fibroblasts into induced neural progenitor cells (iNPCs) using a novel combination
of genes different from those previously reported. These iNPCs exhibit typical NPC morphology and marker gene expression, and a normal capacity for proliferation, self-renewal, and differentiation. Our find-ings suggest new cell-replacement strategies that may be beneficial for studies involving neurodegenerative diseases, disease modeling, and neural development.
Somatic cells have been successfully reprogrammed to form iPSCs, altering their pattern of gene expression, and hence their fate, by ectopic expression of a defined set of factors including Oct3/4, Sox2, and either c-Myc and Klf4 or Nanog and LIN28 (1–4). It was recently reported that reprogrammed cells may retain a “memory” of their original cell type, potentially biasing their differentiation towards the cell’s original lineage and suggesting that iPSCs from different origins may exhibit distinct differentiation preferences (5–7). To elucidate the differences between cells originating from reprogramming ectoderm versus mesoderm origins, we used mouse astrocytes as the parental cell type to generate iPSCs, named mAsiPSCs. Astrocytes were chosen because they are the most abundant neural cell type in the brain and play a critical role in neurodegenerative disorders. Our results showed that mAsiPSCs exhibit morphologies, differentiation potential, and teratoma formation in severe combined immune deficiency (SCID) mice, with derivatives of all three germ layers. Expression profiling of stem cell markers in mAsiPSCs and MEFsiPSCs showed significant similarities. However, this comparison also suggested that the central nervous system-derived mAsiPSCs were more likely to become neuronal cell types
Reprogrammed Astrocytes as a Potential Therapy for Neurodegenerative DisordersChanghai Tian, Ph.D.1,2,4 and Jialin C. Zheng, M.D.1,2,3,4,*
1Laboratory of Neuroimmunology and Regenerative Therapy at the 2Departments of Pharmacology/Experimental Neuroscience and 3Pathology/Microbiology4University of Nebraska Medical Center, Omaha, NE, USA*Corresponding Author: [email protected]
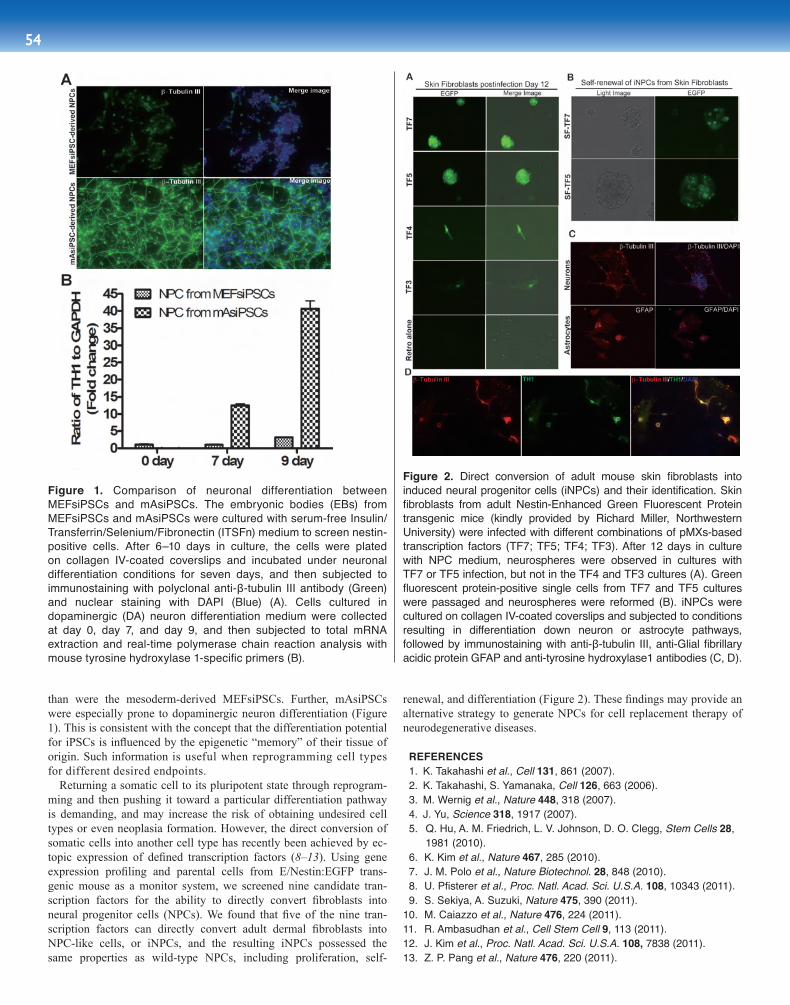
54
Figure 2. Direct conversion of adult mouse skin fibroblasts into induced neural progenitor cells (iNPCs) and their identification. Skin fibroblasts from adult Nestin-Enhanced Green Fluorescent Protein transgenic mice (kindly provided by Richard Miller, Northwestern University) were infected with different combinations of pMXs-based transcription factors (TF7; TF5; TF4; TF3). After 12 days in culture with NPC medium, neurospheres were observed in cultures with TF7 or TF5 infection, but not in the TF4 and TF3 cultures (A). Green fluorescent protein-positive single cells from TF7 and TF5 cultures were passaged and neurospheres were reformed (B). iNPCs were cultured on collagen IV-coated coverslips and subjected to conditions resulting in differentiation down neuron or astrocyte pathways, followed by immunostaining with anti-β-tubulin III, anti-Glial fibrillary acidic protein GFAP and anti-tyrosine hydroxylase1 antibodies (C, D).
Figure 1. Comparison of neuronal differentiation between MEFsiPSCs and mAsiPSCs. The embryonic bodies (EBs) from MEFsiPSCs and mAsiPSCs were cultured with serum-free Insulin/Transferrin/Selenium/Fibronectin (ITSFn) medium to screen nestin-positive cells. After 6–10 days in culture, the cells were plated on collagen IV-coated coverslips and incubated under neuronal differentiation conditions for seven days, and then subjected to immunostaining with polyclonal anti-β-tubulin III antibody (Green) and nuclear staining with DAPI (Blue) (A). Cells cultured in dopaminergic (DA) neuron differentiation medium were collected at day 0, day 7, and day 9, and then subjected to total mRNA extraction and real-time polymerase chain reaction analysis with mouse tyrosine hydroxylase 1-specific primers (B).
than were the mesoderm-derived MEFsiPSCs. Further, mAsiPSCs were especially prone to dopaminergic neuron differentiation (Figure 1). This is consistent with the concept that the differentiation potential for iPSCs is influenced by the epigenetic “memory” of their tissue of origin. Such information is useful when reprogramming cell types for different desired endpoints.
Returning a somatic cell to its pluripotent state through reprogram-ming and then pushing it toward a particular differentiation pathway is demanding, and may increase the risk of obtaining undesired cell types or even neoplasia formation. However, the direct conversion of somatic cells into another cell type has recently been achieved by ec-topic expression of defined transcription factors (8–13). Using gene expression profiling and parental cells from E/Nestin:EGFP trans-genic mouse as a monitor system, we screened nine candidate tran-scription factors for the ability to directly convert fibroblasts into neural progenitor cells (NPCs). We found that five of the nine tran-scription factors can directly convert adult dermal fibroblasts into NPC-like cells, or iNPCs, and the resulting iNPCs possessed the same properties as wild-type NPCs, including proliferation, self-
renewal, and differentiation (Figure 2). These findings may provide an alternative strategy to generate NPCs for cell replacement therapy of neurodegenerative diseases.
REFERENCES 1. K. Takahashi et al., Cell 131, 861 (2007). 2. K. Takahashi, S. Yamanaka, Cell 126, 663 (2006). 3. M. Wernig et al., Nature 448, 318 (2007). 4. J. Yu, Science 318, 1917 (2007). 5. Q. Hu, A. M. Friedrich, L. V. Johnson, D. O. Clegg, Stem Cells 28, 1981 (2010). 6. K. Kim et al., Nature 467, 285 (2010). 7. J. M. Polo et al., Nature Biotechnol. 28, 848 (2010). 8. U. Pfisterer et al., Proc. Natl. Acad. Sci. U.S.A. 108, 10343 (2011). 9. S. Sekiya, A. Suzuki, Nature 475, 390 (2011).10. M. Caiazzo et al., Nature 476, 224 (2011).11. R. Ambasudhan et al., Cell Stem Cell 9, 113 (2011).12. J. Kim et al., Proc. Natl. Acad. Sci. U.S.A. 108, 7838 (2011).13. Z. P. Pang et al., Nature 476, 220 (2011).
54
Stem cells are undifferentiated cells with the ability to undergo self-renewal for long periods without significant changes in their general proper ties. They can differentiate into various specialized cell types under certain physiological or experi-
mental conditions. Successful isolation of pluripotent embryonic stem cells (ESCs) from the inner cell mass of early embryos has provided a powerful tool for biological research. ESCs can give rise to almost any cell lineage and are currently considered the most promising cells for regenerative medicine. The ethical issues surrounding their isola-tion have promoted the development of induced pluripotent stem cells (iPSCs), which share many ESC properties, but which circumvent the ethical concerns. However, both ESCs and iPSCs have the potential for teratoma formation, which may seriously compromise their utility. Un-less differentiation protocols are developed that ensure the desired cell type is created, without any risk of teratoma formation, clinical appli-cation of these highly valuable cells remains impractical. Furthermore, some studies have suggested that iPSCs may retain epigenetic vestiges of their parental cell of origin, potentially leading to heterogeneity in the authenticity of their reprogramming into a desired differentiated fate (1). In recent years, great interest has developed in tissue mesen-chymal stem cells (MSCs). These cells are free of ethical concerns and have been isolated from a wide array of tissues and body fluids. They are thought to be responsible for growth, wound healing, and replacing cells that are lost through daily wear and tear, and likely contribute to the pathological responses to various disease states. Importantly, in a number of animal models and clinical trials, systemic or local admin-istration of MSCs has been demonstrated to have therapeutic effects on various diseases, including liver cirrhosis, heart disease, multiple sclerosis, rheumatoid arthritis, sys temic lupus erythematosus, severe combined immunodeficiency syndrome, Parkinson’s disease, and spi-nal cord injury (2, 3). Although the “gold rush” to use MSCs in clinical settings has started with high enthusiasm in many countries, numer-ous scientific issues remain to be resolved before clinical standards and governmental regulations can be established.
The primary mechanism proposed to be responsible for the thera-peutic effects of MSCs is that the stem cells differentiate and replace necessary cells at the site of tissue damage. MSCs, as multipotent stem cells, can be expanded and differentiated into a variety of tissue types in vitro. However, after in vivo infusion of MSCs, only a tiny propor-tion (or in some studies, none) of the infused cells have been found to engraft and differentiate in damaged tissues, notwithstanding the im-pressive curative effects observed following MSC administration (4). Recent studies have revealed that the therapeutic effects are likely due to the release of MSC-produced cytokines and other growth factors
that modulate the microenvironment at damaged tissue sites (4, 5). In fact, MSC-conditioned medium can elicit similar therapeutic effects to administration of the cells alone (6). This discovery has had a dra-matic impact on the design of stem cell therapy protocols.
The microenvironment at the site of damage is usually characterized by an abundance of pro-inflammatory factors produced by both innate and adaptive immune responses. These factors play a critical role in recruiting MSCs, whether they are of endogenous origin or exogenously administered. Once at the damaged tissue site, MSCs respond to signals from inflammatory cells, inflammatory cytokines, and chemokines. For example, interferon g (IFN-g), in the presence of either tumor necro-sis factor α (TNF-α) or interleukin 1 (IL-1), can induce robust MSC-associated effects in mice that modulate the immune response (5). In vitro, these cytokine-activated MSCs inhibit T cell receptor-triggered, T cell proliferation and cytokine production through production of large amounts of nitric oxide (NO) and chemokines, even at very low MSC to T cell ratios. In vivo, injection of as few as 106 MSCs attenuated graft-versus-host disease (GvHD) and increased tolerance to allogeneic skin transplants in mice (5, 7). This cytokine-induced immunosuppressive response by MSCs depends on inducible nitric oxide synthase (iNOS) in mice and on indoaleamine-2, 3-dihydrogenase (IDO) in humans (5, 8). Furthermore, the immunosuppressive effects of both murine and human MSCs correlate with a large increase in the production of chemokines, which are thought to recruit and retain lymphocytes near the MSCs, thus allowing NO or intracellular IDO to act on the immune cells locally (4, 5). It is noteworthy that the inflammatory environment not only enables MSCs to modulate immune responses by inducing iNOS, IDO, and chemokines, but also promotes MSC production of other growth fac-tors, metalloproteases, and adhesion molecules. These molecules serve to remodel the tissue’s microenvironment and attract de novo phago-cytes and stem cells that repair the tissue (9). Therefore, a better under-standing of the interactions between MSCs and immune cells in tissue microenvironments may lead to improved MSC-based cell therapies.
Histocompatibility and cell therapy rejection has been one of the biggest concerns with stem cell research. Because the allogeneic nature of ESCs is unavoidable, the possibility of histocompatible iPSCs has brought great hope to regenerative medicine. However, a recent report has demonstrated that, compared to derivatives of ESCs, altered gene expression in some cells derived from iPSCs can also lead to T cell-dependent immune responses in syngeneic recipients (10). On the other hand, MSCs can be derived autologously, from the patient themselves (with the exception of those with certain genetic disorders), meaning that this drawback could be avoided. Nonetheless, allogeneic MSCs have been shown to be effective for treating a variety of diseases, with negligible immune responses reported in recipients (11, 12). Indeed, if MSCs exert therapeutic effects through the secretion of trans-acting factors and modulation of tissue microenvironments, the use of allogeneic stem cells may be advantageous, as these cells will not persist due to allorejection and therefore, their tumorigenic potential would be dramatically reduced (13). In fact, for many diseases, the use of “cell-free” stem cell therapy, employing only the soluble products of stem cells, could be an effective option.
1Key Laboratory of Stem Cell Research, Institute of Health Sciences, Shanghai Institutes for Biological Sciences of Chinese Academy of Sciences and Shanghai Jiao Tong University of Medicine, Shanghai, China 2Child Health Institute of New Jersey, UMDNJ-Robert Wood Johnson Medical School, New Brunswick, NJ, USA*Corresponding Author: [email protected]
55Regenerative Medicine and Stem Cell Therapeutics: Basic and Clinical Research
sect ion e ight
Translating Stem Cell Research into Patient Care: Hype or Reality?Yufang Shi, Ph.D.1,2,*, Xiaodong Chen, B.Med.1, Liying Zhang, B.Med.2, Juanjuan Su, M.Sc.1, Arnold B. Rabson, M.D.2, and Guangwen Ren, Ph.D.2

56
Stem cells hold great potential for regenerative medicine. Ten years ago we hypothesized that there is an undefined subfrac-tion of embryonic-like stem cells left over in a number of tissues even after a fetus is formed and we defined them as
postembryonic pluripotent stem cells (PEPSCs). To prove this concept, the very first approach taken was to identify such cells from a variety of human fetal tissues. We have characterized this putative stem cell sub-population from human fetal pancreas, bone marrow, liver, skin, skeletal muscle, and many other tissues (1). These cells, named Flk1+-MSCs (Flk1+CD44+CD29+CD105+CD166+CD34-CD31-Lin-), are capable of multiorgan engraftment and multilineage differentiation. Multilineage differentiation of stem cells is regulated by both genetic and epigen-
etic factors. The regulation of stem cell and progenitor cell properties through the control of gene transcription has been studied extensively, but the role of epigenetic modifications is still not well understood.
Epigenetic modifications, including histone methylation, have be-come the focus of various studies recently. Two histone modifications in particular have been associated with regulating promoter expression: H3K4me3 is generally associated with active promoters, and H3K-27me3 is associated with silenced promoters. Genes with both modi-fications are defined to be in a bivalent state; they have relatively low levels of expression and are maintained in a ‘transcriptional ready’ state that allows rapid transcriptional activation or silencing upon the receipt of certain stimuli (2). This could be a model for an on/off switch for differentiation-associated genes in stem cells.
To explore the mechanisms underlying the multilineage state and lin-eage specification of Flk1+-MSCs, we performed a genome-wide inves-tigation on H3K4me3 and H3K27me3 profiles in these cells by ChIP-seq (n=3), and compared these results with those obtained in embryonic stem cells (ESCs), hematopoietic stem cells (HSCs), and hematopoietic progenitor cells (HPCs) (3,4). The pluripotent-associated gene, Klf4, was modified by the activating H3K4me3 modification; Sall4, Sox2, and Foxd3 were found to be bivalent; and Oct4 (Pou5f1) and Nanog exhibit-ed either a repressive state or no modification in Flk1+-MSCs. However,
Although significant progress has been made in stem cell research in recent years, regenerative medicine using stem cells is far from a mature clinical technology. Even if the issues of teratoma formation and the propagation of possible genetic abnormalities in the admin-istered cells are resolved, the stage and nature of differentiated cells of embryonic or induced pluripotent origin to be used for each dis-ease have to be determined, since their ability for engraftment and modification of tissue microenvironment varies greatly depending on their differentiation stage. Although MSCs are the most commonly used stem cells in current clinical applications, there are still several major hurdles to their widespread utility. While MSCs have been suc-cessfully isolated and expanded from various tissues, it is still not known which source should be used for which disease, which route of administration is best suited for a particular disease, and whether there are contraindications for their clinical use. Further, the param-eters for monitoring clinical effectiveness must still be established and are likely to vary for different diseases. Most importantly, most countries have yet to establish standards for cell expansion proto-cols, product characterization and quality, and safety. However, fur-ther scientific progress in answering these fundamental questions must occur before government agencies can establish regulatory polices to meet the challenges of this emerging and rapidly advanc-ing field, which promises to benefit patients suffering a wide array of diseases.
REFERENCES 1. K. Kim et al., Nature 467, 285 (2010). 2. A. Uccelli, L. Moretta, V. Pistoia, Nature Rev. Immunol. 8, 726
(2008). 3. J. Wagner, T. Kean, R. Young, J. E. Dennis, A. I. Caplan, Curr.
Opin. Biotechnol. 20, 531 (2009). 4. R. H. Lee et al., Cell Stem Cell 5, 54 (2009). 5. G. Ren et al., Cell Stem Cell 2, 141 (2008). 6. M. Gnecchi et al., Nature Med. 11, 367 (2005). 7. G. Xu et al., Cell Res. 17, 240 (2007). 8. G. Ren et al., Stem Cells 27, 1954 (2009). 9. N. G. Singer, A. I. Caplan, Annu. Rev. Pathol. 6, 457 (2011).10. T. Zhao, Z. N. Zhang, Z. Rong, Y. Xu, Nature 474, 212 (2011).11. K. Le Blanc et al., Lancet 363, 1439 (2004).12. L. Chen, E. E. Tredget, C. Liu, Y. Wu, PLoS One 4, e7119 (2009),
doi:10.1371/journal.pone.0007119.13. D. J. Prockop et al., Cytotherapy 12, 576 (2010).
Acknowledgments: This work was supported by grants from the Ministry of Science and Technology of China (2011DFA30630, 2010CB945600, 2009ZX09503-024), Scientific Innovation Project of the Chinese Academy of Science (XDA01040000), and grants from the National Institutes of Health of the United States of America (GM866889), and the Robert Wood Johnson Foundation (67038).
1Institute of Basic Medical Sciences & School of Basic Medicine, Center of Excellence in Tissue Engineering, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, China2Institute of Reproductive & Stem Cell Engineering, Central South University, Changsha, China3Department of Genetics, Rutgers University, Nelson Bio Labs, Piscataway, NJ, USA*Corresponding Author: [email protected]
Histone Methylation and MicroRNA-Mediated Regulation of the Multipotential State of Flk1+ Mesenchymal Stem CellsHongling Li, M.D., Ph.D.1, Jianhe Chen, M.D., Ph.D.1, Qin Han, M.D., Ph.D.1, Shihua Wang, M.D., Ph.D.1, Kanghua Li, M.D., Ph.D.1, Xuebin Qu, M.D., Ph.D.1, Jing Li, Ph.D.1, Yang Zeng, M.D., Ph.D.1, Jing Wang, M.D., Ph.D.1, Jing Li, B.S.1, Li Zhu, B.S.1, Xingxia Liu, M.D., Ph.D.1, Ge Lin, M.D.2, Changshun Shao, Ph.D.3, and Robert Chunhua Zhao, M.D., Ph.D.1, *
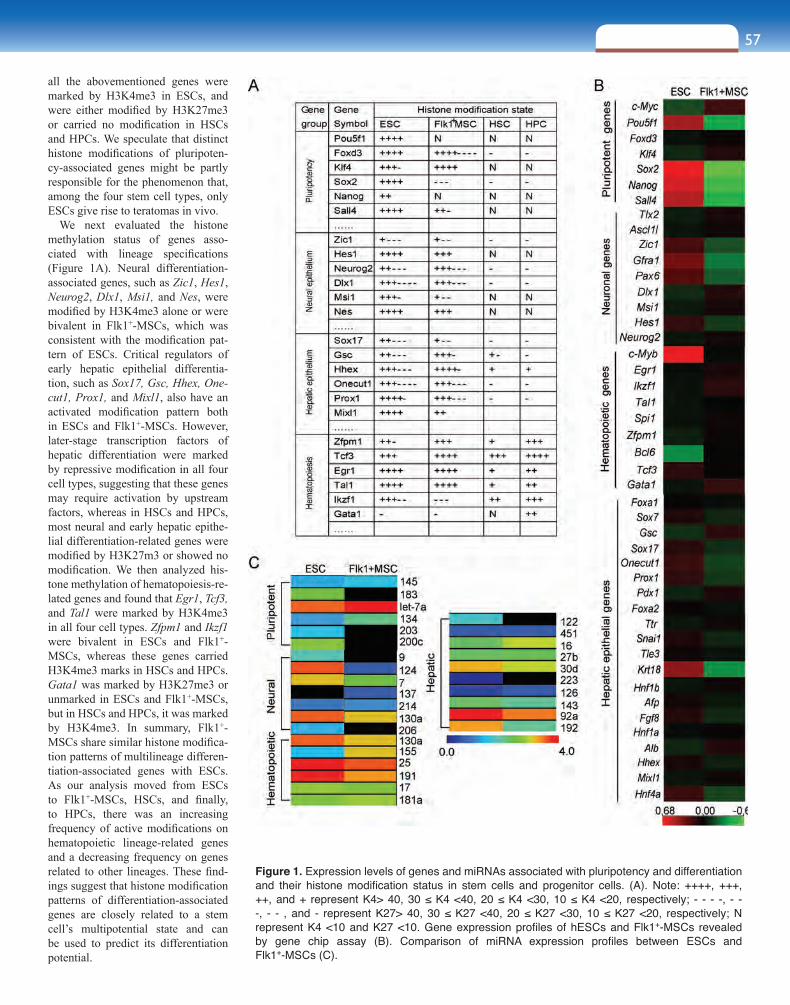
57sect ion e ight
all the abovementioned genes were marked by H3K4me3 in ESCs, and were either modified by H3K27me3 or carried no modification in HSCs and HPCs. We speculate that distinct histone modifications of pluripoten-cy-associated genes might be partly responsible for the phenomenon that, among the four stem cell types, only ESCs give rise to teratomas in vivo.
We next evaluated the histone methylation status of genes asso-ciated with lineage specifications (Figure 1A). Neural differentiation-associated genes, such as Zic1, Hes1, Neurog2, Dlx1, Msi1, and Nes, were modified by H3K4me3 alone or were bivalent in Flk1+-MSCs, which was consistent with the modification pat-tern of ESCs. Critical regulators of early hepatic epithelial differentia-tion, such as Sox17, Gsc, Hhex, One-cut1, Prox1, and Mixl1, also have an activated modification pattern both in ESCs and Flk1+-MSCs. However, later-stage transcription factors of hepatic differentiation were marked by repressive modification in all four cell types, suggesting that these genes may require activation by upstream factors, whereas in HSCs and HPCs, most neural and early hepatic epithe-lial differentiation-related genes were modified by H3K27m3 or showed no modification. We then analyzed his-tone methylation of hematopoiesis-re-lated genes and found that Egr1, Tcf3, and Tal1 were marked by H3K4me3 in all four cell types. Zfpm1 and Ikzf1 were bivalent in ESCs and Flk1+-MSCs, whereas these genes carried H3K4me3 marks in HSCs and HPCs. Gata1 was marked by H3K27me3 or unmarked in ESCs and Flk1+-MSCs, but in HSCs and HPCs, it was marked by H3K4me3. In summary, Flk1+-MSCs share similar histone modifica-tion patterns of multilineage differen-tiation-associated genes with ESCs. As our analysis moved from ESCs to Flk1+-MSCs, HSCs, and finally, to HPCs, there was an increasing frequency of active modifications on hematopoietic lineage-related genes and a decreasing frequency on genes related to other lineages. These find-ings suggest that histone modification patterns of differentiation-associated genes are closely related to a stem cell’s multipotential state and can be used to predict its differentiation potential.
Figure 1. Expression levels of genes and miRNAs associated with pluripotency and differentiation and their histone modification status in stem cells and progenitor cells. (A). Note: ++++, +++, ++, and + represent K4> 40, 30 ≤ K4 <40, 20 ≤ K4 <30, 10 ≤ K4 <20, respectively; - - - -, - - -, - - , and - represent K27> 40, 30 ≤ K27 <40, 20 ≤ K27 <30, 10 ≤ K27 <20, respectively; N represent K4 <10 and K27 <10. Gene expression profiles of hESCs and Flk1+-MSCs revealed by gene chip assay (B). Comparison of miRNA expression profiles between ESCs and Flk1+-MSCs (C).

58
To characterize the relationship between histone modification state and gene expression, we performed gene chip analysis and compared the expression profiles of genes associated with pluripotency and lineage specification in ESCs and Flk1+-MSCs (Figure 1B). The expression lev-el of pluripotency-associated genes is higher in ESCs. The expression of specific lineage-associated genes was low or even undetectable in ESCs and Flk1+-MSCs, despite the fact that these genes were marked by H3K4me3 or in a bivalent state. These findings are consistent with recent studies demonstrating that genes with the bivalent modification have relatively low levels of expression (5,6), suggesting that H3K4me3 and bivalent histone modifications in stem cells may mainly provide genes with transcriptional potential.
As microRNAs (miRNAs) play a major role in controlling stem cell differentiation, we obtained the miRNA profile of Flk1+-MSCs and compared it with that of ESCs. We found that expression of miRNAs associated with pluripotency was higher in ESCs than Flk1+-MSCs, while expression levels of most miRNAs associated with multilineage differentiation were similar between ESCs and Flk1+-MSCs (Figure 1C). Overall, the miRNA expression profile correlated well with the histone modification patterns of genes associated with pluripotency and lineage specification in ESCs and Flk1+-MSCs.
To better understand the properties of Flk1+-MSCs, we analyzed ex-pression profiles of lineage-specific genes during multilineage differ-entiation of Flk1+-MSCs. Interestingly, during adipogenic differentia-tion of Flk1+-MSCs, the histone modification profile of osteogenic and neuronal genes changed from an active to a repressive state. Similarly, during osteogenic differentiation, methylation states of adipogenic and neuronal genes were suppressed via repressive histone modifications.
These results suggest that when Flk1+-MSCs begin to differentiate to-ward a specific lineage, the specification-associated genes will be ac-tivated, whereas genes of other lineages will be silenced through epi-genetic changes initiated by as-yet unknown mechanisms. Dynamic changes in histone modification patterns may be prerequisites for stem cells to initiate differentiation toward a specific lineage.
These studies bridge a gap in our knowledge about the various fac-tors governing multipotency of Flk1+-MSCs—including histone meth-ylation, gene expression, and microRNAs—and illustrate some of the underlying mechanisms at both a transcriptional and posttranscriptional level. Our findings broaden the current understanding of stem cell mul-tipotency and provide new insight into how Flk1+-MSCs can be ma-nipulated in vitro for better clinical application.
REFERENCES 1. L. M. Liao, L. S. Li, R. C. Zhao, Philos. Trans. R. Soc. Lond. B.
Biol. Sci. 362, 1107 (2007). 2. B. E. Bernstein et al., Cell 125, 315 (2006). 3. M. Ku et al., PLoS Genet. 4, e1000242 (2008), doi:10.1371/journal.
pgen.1000242. 4. K. Cui et al., Cell Stem Cell 4, 80 (2009). 5. X. D. Zhao et al., Cell Stem Cell 1, 286 (2007). 6. T. S. Mikkelsen et al., Nature 448, 553 (2007).
Acknowledgments: This work was supported by grants from the “863 Projects” of Ministry of Science and Technology of China (2011AA020100) and the National Key Scientific Program of China (2011CB964901).
Translational Research and the Treatment of Skin Wounds in ChinaXiaobing Fu, M.D.
The skin is the largest and most easily injured organ in the human body. Skin wounds can be caused by acute injury, such as burns, or be a complication of diabetes. In China, diabetes is becoming the leading cause of chronic skin wounds (1,2),
making the prevention and management of skin wounds a major health care focus with considerable socioeconomic impact. Our team has been involved in studying wound-healing mechanisms, as well as growth-factor biology, for approximately two decades, examining the use of growth factors to accelerate wound healing and improve treatment in the field of skin trauma.
CHRONIC SKIN WOUNDS IN CHINAData are lacking on the epidemiology of all skin wounds in China; however, epidemiologic study of chronic skin wounds showed an in-cidence of 1.5% to 3.0% in surgical hospitalized patients undergoing surgery in 1998 (1). The principal causes of the chronic skin wounds were trauma or trauma plus infection (67.5%). Diabetic feet, venous
ulcers, and pressure ulcers (bed sores) accounted for 4.9%, 6.5%, and 9.2%, respectively (1). The wound sites differed by etiology: Of 580 wounds in 489 patients, 366 (63.1%) were in the lower extremities, and 214 (36.9%) were in other sites, such as the upper extremities (17.9%), thoracic and abdominal region (7.8%), back (4.8%), and head (6.4%). Farmers and manual workers showed a high incidence of these chronic skin wounds.
Ten years later, in 2008, a new epidemiologic study indicated an incidence of chronic skin wounds of about 1.7‰ among all hospitalized patients in China (2). Although the distribution of wounds was similar to that in 1998, the leading causes of the chronic skin wounds differed. The top cause was diabetes (32.6%), then trauma (23.8%), pressure ulcers (bed sores, 10.5%), iatrogenic factors (10.6%), and infections (9.3%). The median patient age was 58 years (range 18 days to 96 years), with the highest incidence among patients aged 40 to 60 years and 60 to 80 years (31% and 38%, respectively). Manual laborers (38.5% men, 29.3% women) and retirees (27.9% men, 23.5% women) accounted for more than half of the patients. Therefore, diabetes has recently become the leading cause of chronic cutaneous wounds in China, and the results are alarming in terms of prevention and management of these chronic skin wounds (2).
The Institute of Basic Medicine, PLA General Hospital, Beijing, China The First Affiliated Hospital, PLA General Hospital, Beijing, [email protected]

59sect ion e ight
REGULATION OF WOUND-HEALING MECHANISMS BY GROWTH FACTORS AND THEIR USE IN WOUND HEALINGIn response to clinical demand, we are studying the role of growth factors in regulating wound healing. Chronic skin wounds are characterized by defective remodeling of the ex-tracellular matrix (ECM), reepithelialization failure, and pro-longed inflammation (3,4). For deep chronic skin wounds, healing demands a complex process of angiogenesis, depo-sition of extracellular matrix, contraction, and epithelializa-tion. Chronic nonhealing wounds caused by infection, ve-nous diseases, and malnutrition in diabetics, or subsequent to chemotherapy or radiotherapy in cancer patients, are painful for patients and frustrating for physicians (3,4).
The dynamic biological process of wound healing involves a complex interaction of cellular and biochemical events and growth factors such as epidermal growth factor (EGF), fibroblast growth factor (FGF), transforming growth factor (TGF), and nerve growth factor (NGF), which all play key roles. Since 1990, pharmacological and toxicological studies have offered direct evidence of the relationship between growth factors and wound healing. Data are available on the use of growth factors in wound healing, including their dosage, most suitable administration time, and possible side effects. Our team of basic scientists, clinical physicians, and biopharmaceutical researchers has produced two kinds of genetically engineered growth factors for successfully translational use in skin wound repair and regeneration (5–8): recombinant human EGF (rhEGF) and recombinant bovine basic FGF (rbFGF). The topical application of these factors has accelerated wound healing and improved healing quality. A multicenter clinical trial revealed shorter wound healing time, by two to four days, for all superficial and deep second-degree burns and donor sites as compared with control treatment. Also, granulation tissue formation and epidermal regeneration was accelerated. In one study, 33 chronic skin wounds resulting from trauma, diabetes, bed sores, and radiation injuries were treated with rbFGF. The effective wound-healing rate within four weeks was 90%, and all wounds healed within 42 days (5–7). In some studies, the rate of healing was 84% to 94% for chronic skin ulcers treated with rbFGF or rhEGF (Figures 1 and 2, 5–8).
FUTURE TRENDS IN USE OF GROWTH FACTORS FOR SKIN WOUND HEALINGGrowth factor therapies have indeed accelerated the healing of acute or chronic skin wounds. However, some other methods, such as surgi-cal or enzyme débridement, wound bed preparation, infection control, dressing changes, tissue-engineered skin, and traditional medicine are also necessary or essential for skin wound management. Addition-ally, the mechanisms involved in the use of growth factors for wound healing should be studied in detail because of the complex biological process and the many biochemical factors involved. Although we have found no side effects or toxicity with use of growth factors, this pos-sibility should be more fully investigated. Short- and long-term effects must also be studied, and cost-benefit considerations examined. Physi-cians and dermatologists can expect that near-perfect skin wound heal-
ing is achievable through the use of comprehensive methods, including growth factors, stem cells, and other treatments that promote robust and complete skin repair and regeneration (9).
REFERENCES 1. X. B. Fu, Z. Y. Sheng, G. W. Cherry, Q. Y. Li, Wound Rep. Reg. 6,
21 (1998). 2. Y. F. Jiang et al., Wound Rep. Reg. 19, 181 (2011). 3. A. J. Singer, R. A. Clark, N. Engl. J. Med. 341, 738 (1999). 4. K. G. Harding, H. L. Morris, G. K. Patel, Br. Med. J. 324,
160 (2002). 5. X. B. Fu, Z. Y. Shen, Z. R. Guo, M. L. Zhang, Z. Y. Sheng, Chin.
Med. J. 115, 331 (2002). 6. X. B. Fu et al., Chin. Med. J. 113, 367 (2000). 7. X. B. Fu et al., Lancet 352, 1661 (1998). 8. X. B. Fu, X. K. Li, B. Cheng, W. Chen, Z. Y. Sheng, Wound Rep.
Reg. 13, 122 (2005). 9. X. B. Fu, H. H. Li, Cell Tissue Res. 335, 317 (2009).10. These works were supported in part by the National Basic Science
and Development Programme (973 Programme, 2005CB522603, 2012CB518105) and a grant from the National Natural Science Foundation of China (30730090).
Figure 1. A 30-year-old woman with chronic (present for at least 10 years) radiation-induced ulcers of the chest. Wounds were not healed with surgery, traditional medicine, or skin autografting (A). Healing was promoted with topical application of recombinant basic fibroblast growth factor for 42 days (B) (8).
Figure 2. A 24-year-old man with deep second-degree burns of the feet. The right foot was treated with recombinant human epidermal growth factor and the left with 1% silver sulfadiazine (A). Seven days after treatment, the right-foot wounds healed without scar formation or other side effects, but wound healing on the left foot was incomplete (B).
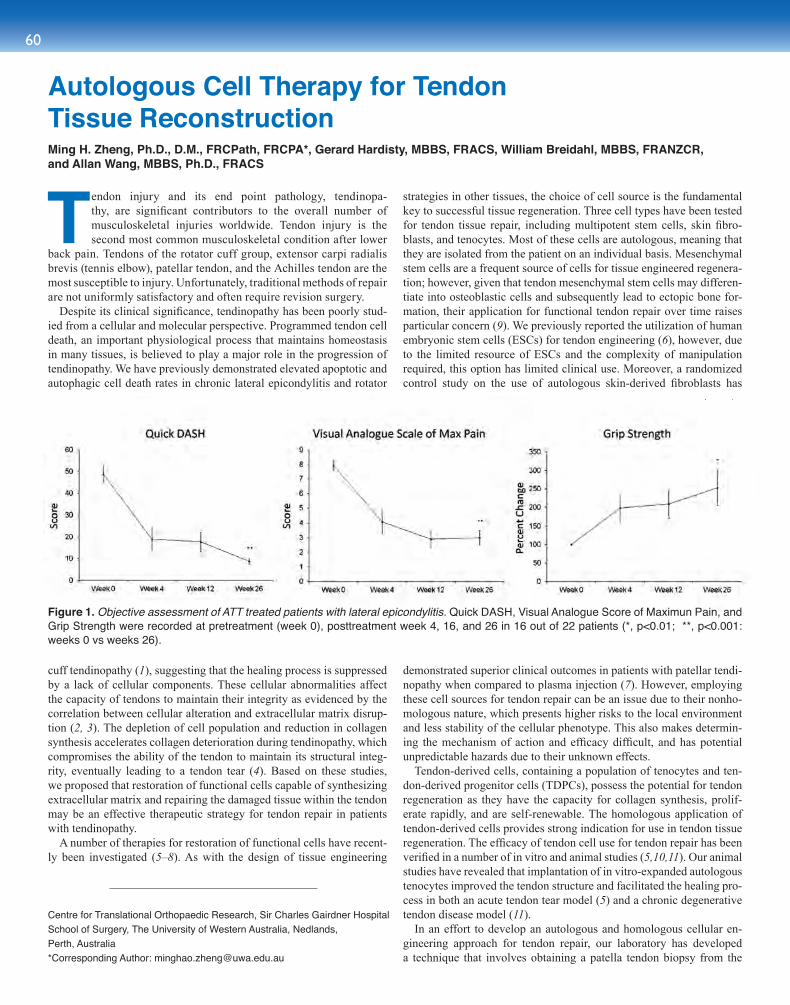
60
Tendon injury and its end point pathology, tendinopa-thy, are significant contributors to the overall number of musculoskeletal injuries worldwide. Tendon injury is the second most common musculoskeletal condition after lower
back pain. Tendons of the rotator cuff group, extensor carpi radialis brevis (tennis elbow), patellar tendon, and the Achilles tendon are the most susceptible to injury. Unfortunately, traditional methods of repair are not uniformly satisfactory and often require revision surgery.
Despite its clinical significance, tendinopathy has been poorly stud-ied from a cellular and molecular perspective. Programmed tendon cell death, an important physiological process that maintains homeostasis in many tissues, is believed to play a major role in the progression of tendinopathy. We have previously demonstrated elevated apoptotic and autophagic cell death rates in chronic lateral epicondylitis and rotator
cuff tendinopathy (1), suggesting that the healing process is suppressed by a lack of cellular components. These cellular abnormalities affect the capacity of tendons to maintain their integrity as evidenced by the correlation between cellular alteration and extracellular matrix disrup-tion (2, 3). The depletion of cell population and reduction in collagen synthesis accelerates collagen deterioration during tendinopathy, which compromises the ability of the tendon to maintain its structural integ-rity, eventually leading to a tendon tear (4). Based on these studies, we proposed that restoration of functional cells capable of synthesizing extracellular matrix and repairing the damaged tissue within the tendon may be an effective therapeutic strategy for tendon repair in patients with tendinopathy.
A number of therapies for restoration of functional cells have recent-ly been investigated (5–8). As with the design of tissue engineering
strategies in other tissues, the choice of cell source is the fundamental key to successful tissue regeneration. Three cell types have been tested for tendon tissue repair, including multipotent stem cells, skin fibro-blasts, and tenocytes. Most of these cells are autologous, meaning that they are isolated from the patient on an individual basis. Mesenchymal stem cells are a frequent source of cells for tissue engineered regenera-tion; however, given that tendon mesenchymal stem cells may differen-tiate into osteoblastic cells and subsequently lead to ectopic bone for-mation, their application for functional tendon repair over time raises particular concern (9). We previously reported the utilization of human embryonic stem cells (ESCs) for tendon engineering (6), however, due to the limited resource of ESCs and the complexity of manipulation required, this option has limited clinical use. Moreover, a randomized control study on the use of autologous skin-derived fibroblasts has
demonstrated superior clinical outcomes in patients with patellar tendi-nopathy when compared to plasma injection (7). However, employing these cell sources for tendon repair can be an issue due to their nonho-mologous nature, which presents higher risks to the local environment and less stability of the cellular phenotype. This also makes determin-ing the mechanism of action and efficacy difficult, and has potential unpredictable hazards due to their unknown effects.
Tendon-derived cells, containing a population of tenocytes and ten-don-derived progenitor cells (TDPCs), possess the potential for tendon regeneration as they have the capacity for collagen synthesis, prolif-erate rapidly, and are self-renewable. The homologous application of tendon-derived cells provides strong indication for use in tendon tissue regeneration. The efficacy of tendon cell use for tendon repair has been verified in a number of in vitro and animal studies (5,10,11). Our animal studies have revealed that implantation of in vitro-expanded autologous tenocytes improved the tendon structure and facilitated the healing pro-cess in both an acute tendon tear model (5) and a chronic degenerative tendon disease model (11).
In an effort to develop an autologous and homologous cellular en-gineering approach for tendon repair, our laboratory has developed a technique that involves obtaining a patella tendon biopsy from the
Figure 1. Objective assessment of ATT treated patients with lateral epicondylitis. Quick DASH, Visual Analogue Score of Maximun Pain, and Grip Strength were recorded at pretreatment (week 0), posttreatment week 4, 16, and 26 in 16 out of 22 patients (*, p<0.01; **, p<0.001: weeks 0 vs weeks 26).
Autologous Cell Therapy for Tendon Tissue ReconstructionMing H. Zheng, Ph.D., D.M., FRCPath, FRCPA*, Gerard Hardisty, MBBS, FRACS, William Breidahl, MBBS, FRANZCR, and Allan Wang, MBBS, Ph.D., FRACS
Centre for Translational Orthopaedic Research, Sir Charles Gairdner Hospital School of Surgery, The University of Western Australia, Nedlands, Perth, Australia*Corresponding Author: [email protected]

61sect ion e ight
patient, isolating cells from the tendon tissue by enzymatic digestion, in vitro expansion of the cell population to a sufficient number in a GMP-certified laboratory, and finally delivering the cells to the defect site by an ultrasound-guided needle. Based on the preclinical evalua-tion, we conducted a phase I/IIa study of autologous tenocyte therapy (ATT) in Perth, Western Australia, for the treatment of lateral epicon-dylitis. In total, 23 patients (13 men, 10 women; mean age 50 years, ranging from 37–63) were recruited with refractory lateral epicondyli-tis. The mean duration of symptoms prior to the study was 14 months, with a range of 6 to 24 months. Two patients withdrew their consent and three were discontinued after commencement of the study. Tenocytes were successfully grown in culture at the Orthocell Pty. Ltd. GMP-cer-tified facility. Each patient received a single injection of cells. A safety assessment verified that no adverse events were reported for any patient at either the donor or recipient sites. No infection or excessive fibro-blastic reaction at the elbow implantation site was found in any of the patients injected with autologous tenocytes. One patient was subjected to surgery three months after the injection due to further injury, but had no adverse symptoms. Subjective evaluation data were collected prior to treatment, and then posttreatment at 4, 16, and 26 weeks. The aver-age pain score was 1.7/10 at four hours and 0/10 at four weeks after biopsy. One patient took paracetamol four hours after biopsy. Of the remaining 18 patients, 17 reached the six-month follow-up, and have shown at least 60% improvement in all scores when compared with pretreatment scores (Figure 1). Objective assessments by an MRI ex-amination showed infill of the tendon tear in the majority of patients but there was variation in the quality of regenerated tendon (Figure 2).
In short, the development of a novel therapeutic approach always
requires comparison with a conventional treatment to define its ben-eficial effect. Although in our first phase I/IIa trial ATT showed some degree of improvement in patient’s functional outcome, the efficacy of ATT for tendon regeneration still requires more solid evidence.
REFERENCES 1. J. Chen, A. Wang, J. Xu, M. H. Zheng, J. Shoulder Elbow Surg. 19,
355 (2010). 2. Y. Tuoheti et al., J. Shoulder Elbow Surg. 14, 535 (2005). 3. P. Sharma, N. Maffulli, J. Bone Joint Surg. (Am). 87, 187 (2005). 4. B. Wu et al., Arch. Orthop. Trauma Surg. 131, 405 (2010). 5. J. Chen, C. Willers, J. Xu, A. Wang, M. H. Zheng, Tissue Eng. 13,
1479 (2007). 6. X. Chen et al., Stem Cells 27, 1276 (2009). 7. A. W. Clarke et al., Am. J. Sports Med. 39, 614 (2011). 8. A. Crovace, L. Lacitignola, R. De Siena, G. Rossi, E. Francioso,
Vet. Res. Commun. Suppl 1, 281 (2007). 9. M.T. Harris et al., J. Orthop. Res. 22, 998 (2004).10. Y. Bi et al., Nature Med. 10, 1219 (2007). 11. J. Chen et al., Tissue Eng. Part A. 17, 2037 (2011).
Acknowledgments: We thank members of the Center for transla-tional Orthopedic Research and Professor David Lloyd and David Smith. Funding: supported in part by a grant from Australia Research Council linkage grant program. Competing interests: MHZ have been granted a patent in USA based on the work of autolougous teno-cyte culture method. The other authors declare that they have no competing interests.
Figure 2. MRI images before (A) and six month (B) after ATI showed improvement of tendon structure (repair) in 46-year-old female patient.
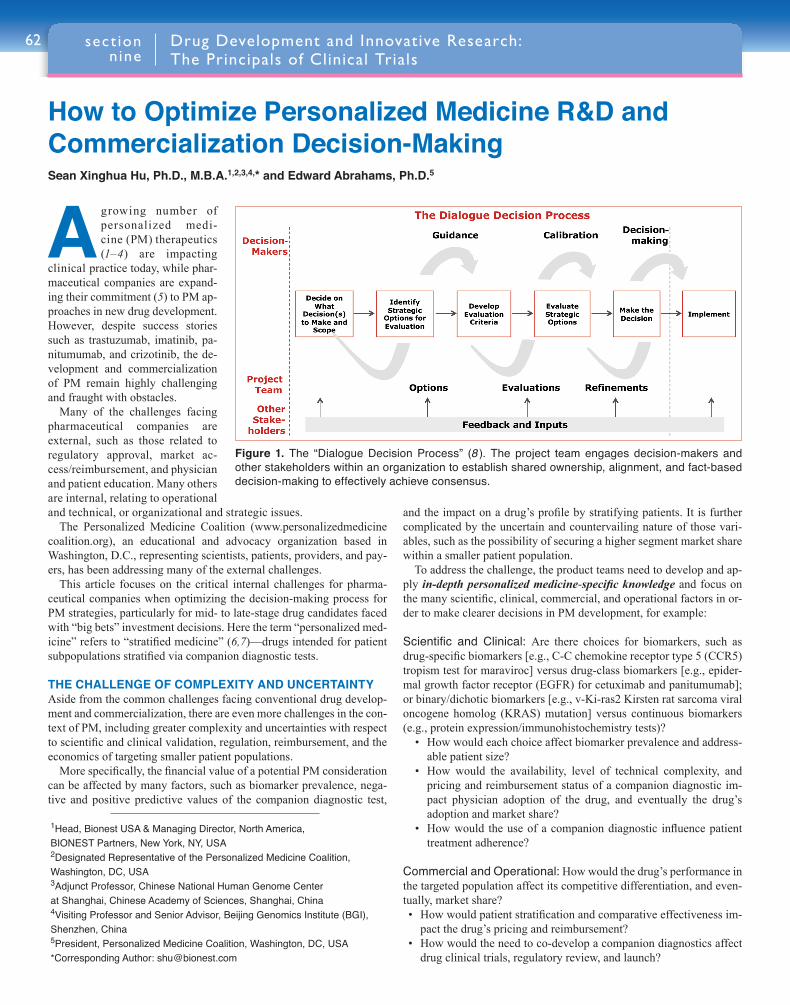
62
A growing number of personalized medi-cine (PM) therapeutics (1–4) are impacting
clinical practice today, while phar-maceutical companies are expand-ing their commitment (5) to PM ap-proaches in new drug development. However, despite success stories such as trastuzumab, imatinib, pa-nitumumab, and crizotinib, the de-velopment and commercialization of PM remain highly challenging and fraught with obstacles.
Many of the challenges facing pharmaceutical companies are external, such as those related to regulatory approval, market ac-cess/reimbursement, and physician and patient education. Many others are internal, relating to operational and technical, or organizational and strategic issues.
The Personalized Medicine Coalition (www.personalizedmedicine coalition.org), an educational and advocacy organization based in Washington, D.C., representing scientists, patients, providers, and pay-ers, has been addressing many of the external challenges.
This article focuses on the critical internal challenges for pharma-ceutical companies when optimizing the decision-making process for PM strategies, particularly for mid- to late-stage drug candidates faced with “big bets” investment decisions. Here the term “personalized med-icine” refers to “stratified medicine” (6,7)—drugs intended for patient subpopulations stratified via companion diagnostic tests.
THE CHALLENGE OF COMPLEXITY AND UNCERTAINTYAside from the common challenges facing conventional drug develop-ment and commercialization, there are even more challenges in the con-text of PM, including greater complexity and uncertainties with respect to scientific and clinical validation, regulation, reimbursement, and the economics of targeting smaller patient populations.
More specifically, the financial value of a potential PM consideration can be affected by many factors, such as biomarker prevalence, nega-tive and positive predictive values of the companion diagnostic test,
and the impact on a drug’s profile by stratifying patients. It is further complicated by the uncertain and countervailing nature of those vari-ables, such as the possibility of securing a higher segment market share within a smaller patient population.
To address the challenge, the product teams need to develop and ap-ply in-depth personalized medicine-specific knowledge and focus on the many scientific, clinical, commercial, and operational factors in or-der to make clearer decisions in PM development, for example:
Scientific and Clinical: Are there choices for biomarkers, such as drug-specific biomarkers [e.g., C-C chemokine receptor type 5 (CCR5) tropism test for maraviroc] versus drug-class biomarkers [e.g., epider-mal growth factor receptor (EGFR) for cetuximab and panitumumab]; or binary/dichotic biomarkers [e.g., v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS) mutation] versus continuous biomarkers (e.g., protein expression/immunohistochemistry tests)?
• How would each choice affect biomarker prevalence and address-able patient size?
• How would the availability, level of technical complexity, and pricing and reimbursement status of a companion diagnostic im-pact physician adoption of the drug, and eventually the drug’s adoption and market share?
• How would the use of a companion diagnostic influence patient treatment adherence?
Commercial and Operational: How would the drug’s performance in the targeted population affect its competitive differentiation, and even-tually, market share?• How would patient stratification and comparative effectiveness im-
pact the drug’s pricing and reimbursement?• How would the need to co-develop a companion diagnostics affect
drug clinical trials, regulatory review, and launch?
1Head, Bionest USA & Managing Director, North America, BIONEST Partners, New York, NY, USA 2Designated Representative of the Personalized Medicine Coalition, Washington, DC, USA3Adjunct Professor, Chinese National Human Genome Center at Shanghai, Chinese Academy of Sciences, Shanghai, China4Visiting Professor and Senior Advisor, Beijing Genomics Institute (BGI), Shenzhen, China 5President, Personalized Medicine Coalition, Washington, DC, USA*Corresponding Author: [email protected]
How to Optimize Personalized Medicine R&D and Commercialization Decision-MakingSean Xinghua Hu, Ph.D., M.B.A.1,2,3,4,* and Edward Abrahams, Ph.D.5
Drug Development and Innovative Research: The Principals of Clinical Trials
sect ion nine
Figure 1. The “Dialogue Decision Process” (8 ). The project team engages decision-makers and other stakeholders within an organization to establish shared ownership, alignment, and fact-based decision-making to effectively achieve consensus.
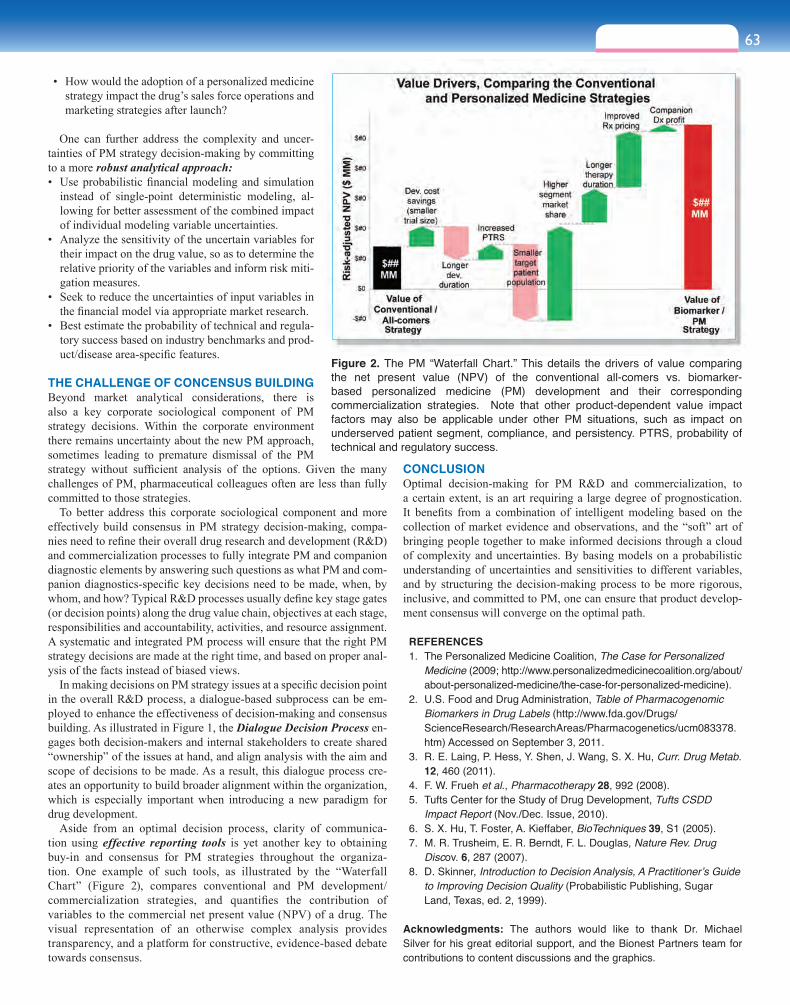
63sect ion nine
• How would the adoption of a personalized medicine strategy impact the drug’s sales force operations and marketing strategies after launch?
One can further address the complexity and uncer-tainties of PM strategy decision-making by committing to a more robust analytical approach:• Use probabilistic financial modeling and simulation
instead of single-point deterministic modeling, al-lowing for better assessment of the combined impact of individual modeling variable uncertainties.
• Analyze the sensitivity of the uncertain variables for their impact on the drug value, so as to determine the relative priority of the variables and inform risk miti-gation measures.
• Seek to reduce the uncertainties of input variables in the financial model via appropriate market research.
• Best estimate the probability of technical and regula-tory success based on industry benchmarks and prod-uct/disease area-specific features.
THE CHALLENGE OF CONCENSUS BUILDINGBeyond market analytical considerations, there is also a key corporate sociological component of PM strategy decisions. Within the corporate environment there remains uncertainty about the new PM approach, sometimes leading to premature dismissal of the PM strategy without sufficient analysis of the options. Given the many challenges of PM, pharmaceutical colleagues often are less than fully committed to those strategies.
To better address this corporate sociological component and more effectively build consensus in PM strategy decision-making, compa-nies need to refine their overall drug research and development (R&D) and commercialization processes to fully integrate PM and companion diagnostic elements by answering such questions as what PM and com-panion diagnostics-specific key decisions need to be made, when, by whom, and how? Typical R&D processes usually define key stage gates (or decision points) along the drug value chain, objectives at each stage, responsibilities and accountability, activities, and resource assignment. A systematic and integrated PM process will ensure that the right PM strategy decisions are made at the right time, and based on proper anal-ysis of the facts instead of biased views.
In making decisions on PM strategy issues at a specific decision point in the overall R&D process, a dialogue-based subprocess can be em-ployed to enhance the effectiveness of decision-making and consensus building. As illustrated in Figure 1, the Dialogue Decision Process en-gages both decision-makers and internal stakeholders to create shared “ownership” of the issues at hand, and align analysis with the aim and scope of decisions to be made. As a result, this dialogue process cre-ates an opportunity to build broader alignment within the organization, which is especially important when introducing a new paradigm for drug development.
Aside from an optimal decision process, clarity of communica-tion using effective reporting tools is yet another key to obtaining buy-in and consensus for PM strategies throughout the organiza-tion. One example of such tools, as illustrated by the “Waterfall Chart” (Figure 2), compares conventional and PM development/commercialization strategies, and quantifies the contribution of variables to the commercial net present value (NPV) of a drug. The visual representation of an otherwise complex analysis provides transparency, and a platform for constructive, evidence-based debate towards consensus.
CONCLUSION Optimal decision-making for PM R&D and commercialization, to a certain extent, is an art requiring a large degree of prognostication. It benefits from a combination of intelligent modeling based on the collection of market evidence and observations, and the “soft” art of bringing people together to make informed decisions through a cloud of complexity and uncertainties. By basing models on a probabilistic understanding of uncertainties and sensitivities to different variables, and by structuring the decision-making process to be more rigorous, inclusive, and committed to PM, one can ensure that product develop-ment consensus will converge on the optimal path.
REFERENCES 1. The Personalized Medicine Coalition, The Case for Personalized
Medicine (2009; http://www.personalizedmedicinecoalition.org/about/about-personalized-medicine/the-case-for-personalized-medicine).
2. U.S. Food and Drug Administration, Table of Pharmacogenomic Biomarkers in Drug Labels (http://www.fda.gov/Drugs/ScienceResearch/ResearchAreas/Pharmacogenetics/ucm083378.htm) Accessed on September 3, 2011.
3. R. E. Laing, P. Hess, Y. Shen, J. Wang, S. X. Hu, Curr. Drug Metab. 12, 460 (2011).
4. F. W. Frueh et al., Pharmacotherapy 28, 992 (2008). 5. Tufts Center for the Study of Drug Development, Tufts CSDD
Impact Report (Nov./Dec. Issue, 2010). 6. S. X. Hu, T. Foster, A. Kieffaber, BioTechniques 39, S1 (2005). 7. M. R. Trusheim, E. R. Berndt, F. L. Douglas, Nature Rev. Drug
Discov. 6, 287 (2007). 8. D. Skinner, Introduction to Decision Analysis, A Practitioner’s Guide
to Improving Decision Quality (Probabilistic Publishing, Sugar Land, Texas, ed. 2, 1999).
Acknowledgments: The authors would like to thank Dr. Michael Silver for his great editorial support, and the Bionest Partners team for contributions to content discussions and the graphics.
Figure 2. The PM “Waterfall Chart.” This details the drivers of value comparing the net present value (NPV) of the conventional all-comers vs. biomarker-based personalized medicine (PM) development and their corresponding commercialization strategies. Note that other product-dependent value impact factors may also be applicable under other PM situations, such as impact on underserved patient segment, compliance, and persistency. PTRS, probability of technical and regulatory success.
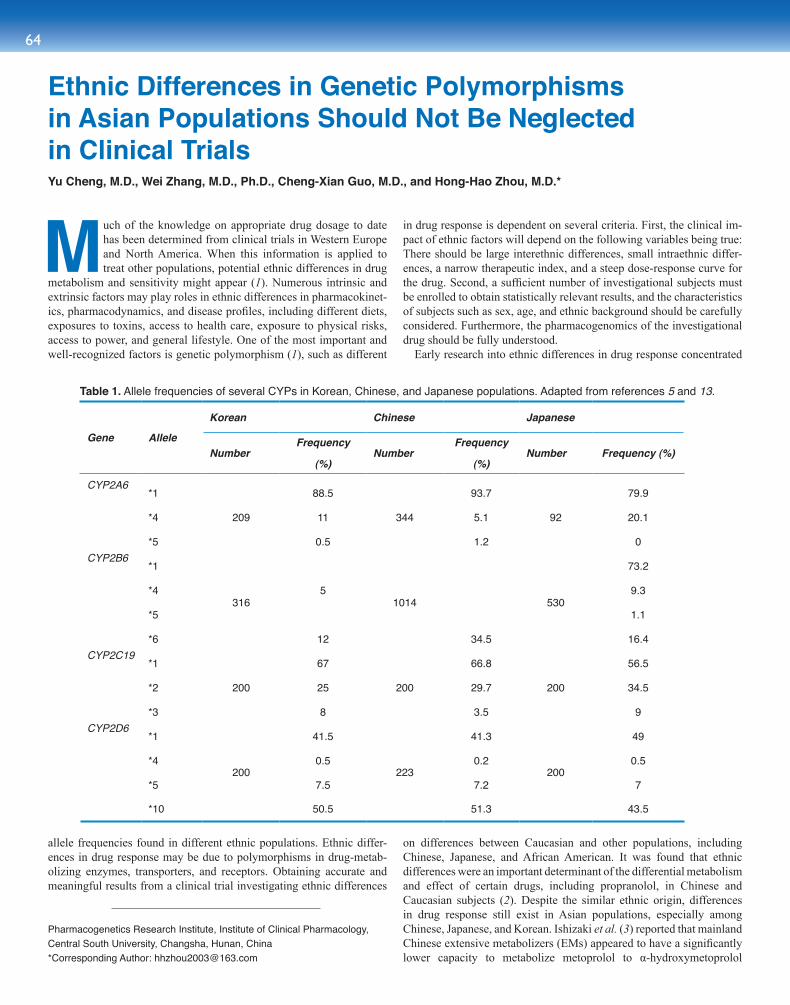
64
Much of the knowledge on appropriate drug dosage to date has been determined from clinical trials in Western Europe and North America. When this information is applied to treat other populations, potential ethnic differences in drug
metabolism and sensitivity might appear (1). Numerous intrinsic and extrinsic factors may play roles in ethnic differences in pharmacokinet-ics, pharmacodynamics, and disease profiles, including different diets, exposures to toxins, access to health care, exposure to physical risks, access to power, and general lifestyle. One of the most important and well-recognized factors is genetic polymorphism (1), such as different
allele frequencies found in different ethnic populations. Ethnic differ-ences in drug response may be due to polymorphisms in drug-metab-olizing enzymes, transporters, and receptors. Obtaining accurate and meaningful results from a clinical trial investigating ethnic differences
in drug response is dependent on several criteria. First, the clinical im-pact of ethnic factors will depend on the following variables being true: There should be large interethnic differences, small intraethnic differ-ences, a narrow therapeutic index, and a steep dose-response curve for the drug. Second, a sufficient number of investigational subjects must be enrolled to obtain statistically relevant results, and the characteristics of subjects such as sex, age, and ethnic background should be carefully considered. Furthermore, the pharmacogenomics of the investigational drug should be fully understood.
Early research into ethnic differences in drug response concentrated
on differences between Caucasian and other populations, including Chinese, Japanese, and African American. It was found that ethnic differences were an important determinant of the differential metabolism and effect of certain drugs, including propranolol, in Chinese and Caucasian subjects (2). Despite the similar ethnic origin, differences in drug response still exist in Asian populations, especially among Chinese, Japanese, and Korean. Ishizaki et al. (3) reported that mainland Chinese extensive metabolizers (EMs) appeared to have a significantly lower capacity to metabolize metoprolol to α-hydroxymetoprolol
Table 1. Allele frequencies of several CYPs in Korean, Chinese, and Japanese populations. Adapted from references 5 and 13.
Gene Allele
Korean Chinese Japanese
NumberFrequency
(%)Number
Frequency
(%)Number Frequency (%)
CYP2A6*1
209
88.5
344
93.7
92
79.9
*4 11 5.1 20.1
*5 0.5 1.2 0CYP2B6
*1
316 1014 530
73.2
*4 5 9.3
*5 1.1
*6 12 34.5 16.4CYP2C19
*1
200
67
200
66.8
200
56.5
*2 25 29.7 34.5
*3 8 3.5 9CYP2D6
*1
200
41.5
223
41.3
200
49
*4 0.5 0.2 0.5
*5 7.5 7.2 7
*10 50.5 51.3 43.5
Ethnic Differences in Genetic Polymorphisms in Asian Populations Should Not Be Neglected in Clinical Trials Yu Cheng, M.D., Wei Zhang, M.D., Ph.D., Cheng-Xian Guo, M.D., and Hong-Hao Zhou, M.D.*
Pharmacogenetics Research Institute, Institute of Clinical Pharmacology, Central South University, Changsha, Hunan, China*Corresponding Author: [email protected]
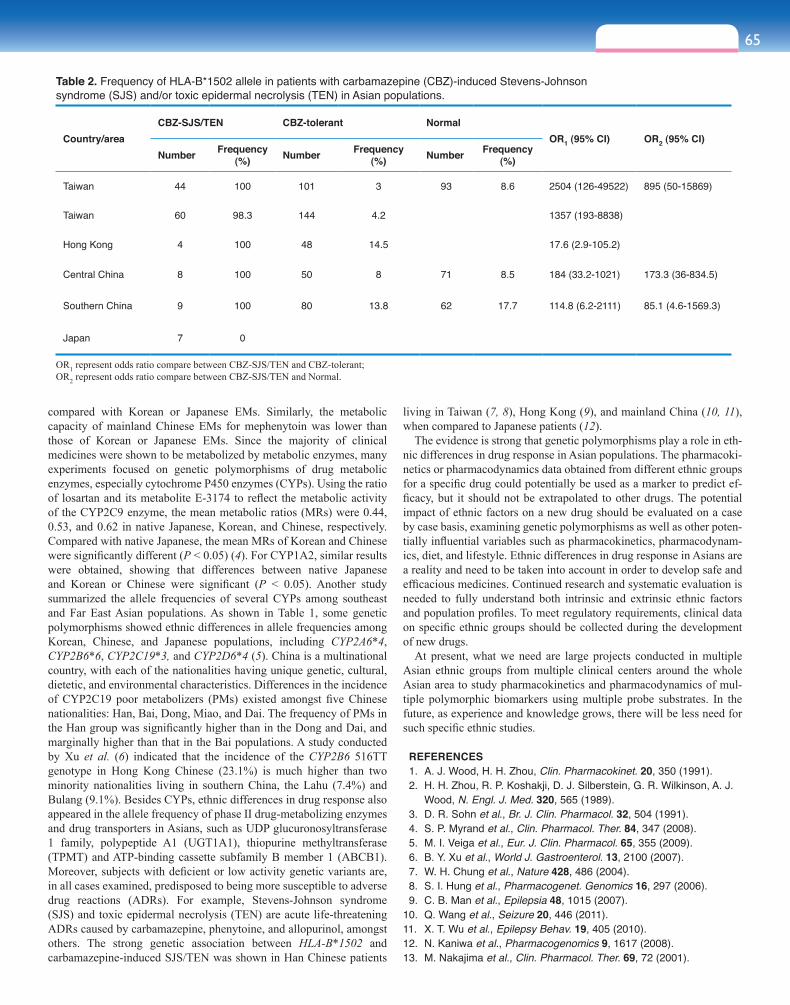
65sect ion nine
compared with Korean or Japanese EMs. Similarly, the metabolic capacity of mainland Chinese EMs for mephenytoin was lower than those of Korean or Japanese EMs. Since the majority of clinical medicines were shown to be metabolized by metabolic enzymes, many experiments focused on genetic polymorphisms of drug metabolic enzymes, especially cytochrome P450 enzymes (CYPs). Using the ratio of losartan and its metabolite E-3174 to reflect the metabolic activity of the CYP2C9 enzyme, the mean metabolic ratios (MRs) were 0.44, 0.53, and 0.62 in native Japanese, Korean, and Chinese, respectively. Compared with native Japanese, the mean MRs of Korean and Chinese were significantly different (P < 0.05) (4). For CYP1A2, similar results were obtained, showing that differences between native Japanese and Korean or Chinese were significant (P < 0.05). Another study summarized the allele frequencies of several CYPs among southeast and Far East Asian populations. As shown in Table 1, some genetic polymorphisms showed ethnic differences in allele frequencies among Korean, Chinese, and Japanese populations, including CYP2A6*4, CYP2B6*6, CYP2C19*3, and CYP2D6*4 (5). China is a multinational country, with each of the nationalities having unique genetic, cultural, dietetic, and environmental characteristics. Differences in the incidence of CYP2C19 poor metabolizers (PMs) existed amongst five Chinese nationalities: Han, Bai, Dong, Miao, and Dai. The frequency of PMs in the Han group was significantly higher than in the Dong and Dai, and marginally higher than that in the Bai populations. A study conducted by Xu et al. (6) indicated that the incidence of the CYP2B6 516TT genotype in Hong Kong Chinese (23.1%) is much higher than two minority nationalities living in southern China, the Lahu (7.4%) and Bulang (9.1%). Besides CYPs, ethnic differences in drug response also appeared in the allele frequency of phase II drug-metabolizing enzymes and drug transporters in Asians, such as UDP glucuronosyltransferase 1 family, polypeptide A1 (UGT1A1), thiopurine methyltransferase (TPMT) and ATP-binding cassette subfamily B member 1 (ABCB1). Moreover, subjects with deficient or low activity genetic variants are, in all cases examined, predisposed to being more susceptible to adverse drug reactions (ADRs). For example, Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are acute life-threatening ADRs caused by carbamazepine, phenytoine, and allopurinol, amongst others. The strong genetic association between HLA-B*1502 and carbamazepine-induced SJS/TEN was shown in Han Chinese patients
living in Taiwan (7, 8), Hong Kong (9), and mainland China (10, 11), when compared to Japanese patients (12).
The evidence is strong that genetic polymorphisms play a role in eth-nic differences in drug response in Asian populations. The pharmacoki-netics or pharmacodynamics data obtained from different ethnic groups for a specific drug could potentially be used as a marker to predict ef-ficacy, but it should not be extrapolated to other drugs. The potential impact of ethnic factors on a new drug should be evaluated on a case by case basis, examining genetic polymorphisms as well as other poten-tially influential variables such as pharmacokinetics, pharmacodynam-ics, diet, and lifestyle. Ethnic differences in drug response in Asians are a reality and need to be taken into account in order to develop safe and efficacious medicines. Continued research and systematic evaluation is needed to fully understand both intrinsic and extrinsic ethnic factors and population profiles. To meet regulatory requirements, clinical data on specific ethnic groups should be collected during the development of new drugs.
At present, what we need are large projects conducted in multiple Asian ethnic groups from multiple clinical centers around the whole Asian area to study pharmacokinetics and pharmacodynamics of mul-tiple polymorphic biomarkers using multiple probe substrates. In the future, as experience and knowledge grows, there will be less need for such specific ethnic studies.
REFERENCES 1. A. J. Wood, H. H. Zhou, Clin. Pharmacokinet. 20, 350 (1991). 2. H. H. Zhou, R. P. Koshakji, D. J. Silberstein, G. R. Wilkinson, A. J.
Wood, N. Engl. J. Med. 320, 565 (1989). 3. D. R. Sohn et al., Br. J. Clin. Pharmacol. 32, 504 (1991). 4. S. P. Myrand et al., Clin. Pharmacol. Ther. 84, 347 (2008). 5. M. I. Veiga et al., Eur. J. Clin. Pharmacol. 65, 355 (2009). 6. B. Y. Xu et al., World J. Gastroenterol. 13, 2100 (2007). 7. W. H. Chung et al., Nature 428, 486 (2004). 8. S. I. Hung et al., Pharmacogenet. Genomics 16, 297 (2006). 9. C. B. Man et al., Epilepsia 48, 1015 (2007).10. Q. Wang et al., Seizure 20, 446 (2011).11. X. T. Wu et al., Epilepsy Behav. 19, 405 (2010).12. N. Kaniwa et al., Pharmacogenomics 9, 1617 (2008).13. M. Nakajima et al., Clin. Pharmacol. Ther. 69, 72 (2001).
Table 2. Frequency of HLA-B*1502 allele in patients with carbamazepine (CBZ)-induced Stevens-Johnson syndrome (SJS) and/or toxic epidermal necrolysis (TEN) in Asian populations.
Country/areaCBZ-SJS/TEN CBZ-tolerant Normal
OR1 (95% CI) OR2 (95% CI)Number Frequency
(%) Number Frequency (%) Number Frequency
(%)
Taiwan 44 100 101 3 93 8.6 2504 (126-49522) 895 (50-15869)
Taiwan 60 98.3 144 4.2 1357 (193-8838)
Hong Kong 4 100 48 14.5 17.6 (2.9-105.2)
Central China 8 100 50 8 71 8.5 184 (33.2-1021) 173.3 (36-834.5)
Southern China 9 100 80 13.8 62 17.7 114.8 (6.2-2111) 85.1 (4.6-1569.3)
Japan 7 0
OR1 represent odds ratio compare between CBZ-SJS/TEN and CBZ-tolerant;OR2 represent odds ratio compare between CBZ-SJS/TEN and Normal.
Table 1. Allele frequencies of several CYPs in Korean, Chinese, and Japanese populations. Adapted from references 5 and 13.
Gene Allele
Korean Chinese Japanese
NumberFrequency
(%)Number
Frequency
(%)Number Frequency (%)
CYP2A6*1
209
88.5
344
93.7
92
79.9
*4 11 5.1 20.1
*5 0.5 1.2 0CYP2B6
*1
316 1014 530
73.2
*4 5 9.3
*5 1.1
*6 12 34.5 16.4CYP2C19
*1
200
67
200
66.8
200
56.5
*2 25 29.7 34.5
*3 8 3.5 9CYP2D6
*1
200
41.5
223
41.3
200
49
*4 0.5 0.2 0.5
*5 7.5 7.2 7
*10 50.5 51.3 43.5

66
Monoclonal antibodies (mAbs) have been widely applied in the diagnosis and treatment of human diseases, such as cancer, transplant rejection, and autoimmune diseases. Therapeutic antibodies represent one of the fastest growing
areas of the biopharmaceutical industry. Over 36 mAbs have thus far been approved by the U.S. Food and Drug Administration and Euro-pean Medicines Agency (1), and 16 mAbs have been approved by the Chinese State Food and Drug Administration (SFDA) for therapeutic applications, particularly for cancers (Table 1). One mode of cancer treatment currently being investigated involves using mAbs that bind specifically to tumor-associated antigens and induce an immunological response against the targeted cancer cell (2). Mechanisms employed to kill tumor cells in this treatment regimen include inhibition of signal transduction, amplification of immunological effects (such as antibody-dependent cell-mediated cytotoxicity and complement dependent cyto-toxicity), antibody neutralization, and immune regulation.
Although new technologies for the production of mAbs have been rapidly emerging in recent years—such as phage antibody libraries, transgenic mouse technology, and the human memory B cell sorting technology—most of the mAbs used today were originally prepared using traditional mouse hybridoma technology. However, under some conditions, mouse-derived whole-molecule antibodies have limita-tions for therapeutic applications because of the high risk for immu-nogenicity in humans (3,4). The primary methods for decreasing an antibody’s immunogenicity include complementarity-determining region/specificity-determining residues grafting, deimmunization, re-surfacing, framework shuffling, epitope-guided selection, and human string content maximization. Fully human mAbs can be expected to produce minimal, if any, immunogenic response in patients, and may be more suitable for the chronic treatment and management of cancer. Second-generation mAbs that address some of the limitations of current antibodies are currently under development. These are being designed to enhance antitumor efficacy through modifications of the antibody’s structure. For example, glycosylation plays a role in effector functions such as antibody-dependent cellular cytotoxicity (ADCC) (5,6). ADCC can be augmented through modification of the antibody Fc region to produce a more favorable binding profile for the Fc receptors expressed on monocytes and natural killer cells (3,5). These modifications include mutations in the amino acid structure of the Fc region as well as altera-tions in the Fc glycosylation pattern, such as in the MAGE 1.5 CHO cell line (Eureka Therapeutics, Inc.).
Design of large-scale fermentation technologies for mammalian cells is one of the most challenging frontiers in antibody production. However, it plays a vital role in biopharmaceutical manufacturing. To-day, the industrial production of antibodies is largely based on stirred-bioreactors for suspension cultures, with the most commonly used cell lines being CHO, BHK, HEK293, Per C6, SP2/0, and NSO as well as modified cell lines such as the ADCC-enhanced MAGE1.5 line. Per C6 is well-suited for the development and large-scale manufacturing of a wide range of biologics including vaccines, antibodies, therapeutic
proteins, and gene therapy products and has a productivity potential of up to 20 g/L coupled with cell densities up to 1.5×108 cell/L. It is note-worthy that improvements in cell fermentation modes of operation have been made over the years, including changes from adherent to suspen-sion cultures, from batch to perfusion, from culture medium containing serum to serum- and protein-free media, and from “black box” opera-tion to intelligent computer control of fermentation.
The HAb18 (IgG1) mAb was developed in our laboratory about 20 years ago using hybridoma technology (7,8). Its antigen, HAb18G, was identified by panning a hepatocellular carcinoma (HCC) cDNA expres-sion library (7). A Blast search of GenBank using the HAb18G gene sequence found it homologous to the CD147 gene (Emmprin, basigin). Thus HAb18G was named HAb18G/CD147 and now is known as a new member of the CD147 family, which belongs to the immunoglobu-lin superfamily (Protein Data Bank ID: 3B5H). Because the HAb18 mAb can bind to HCC cells with high affinity, we created Licartin [Ge-neric name: Iodine (131I) metuximab injection], an 131I-labeled HAb18 F(ab’)2, as a radioimmunotherapeutical agent capable of targeting tu-mors. Licartin has been proven in clinical trials to be a safe and effective agent for HCC treatment (9). In April 2005, Licartin was approved as a new drug for the clinical treatment of primary HCC by the SFDA. The antirecurrence and antitumor effects of Licartin were shown in postor-thotopic liver transplantation (OLT) HCC patients. Results showed that Licartin significantly decreased the cancer recurrence rate by 30.42% and increased HCC patients’ survival rate by 20.62%, compared with an untreated control group (10). The antigen HAb18G/CD147 has also been associated with a reduced survival and tumor recurrences, and can be used as a significant predictor of poor prognosis in HCC patients after tumor resection or liver transplantation (10). We also evaluated whether HAb18G/CD147 could be employed as a novel cancer-associ-ated biomarker. By immunohistochemical analysis of pathological sec-tions from 1672 tissue samples, HAb18G/CD147 was found to be pres-ent in 77.44% (858/1108) of tumors from various sources (liver, lung, esophagus, stomach, rectum, breast, ovary, and cervix), whereas, only 14.18% (80/564) of corresponding normal and benign tissue samples were HAb18G/CD147-positive (11). Therefore, HAb18G/CD147 could potentially be used as a novel universal cancer biomarker.
Antibody-based therapies have proven to be an excellent option for treating cancers, infectious diseases, and inflammatory diseases (12). The manufacturing of these therapeutic antibodies is becoming more financially advantageous for the biopharmaceutical industry in China and worldwide, and the demand for mAbs will likely increase for the foreseeable future.
The development of antibody-based therapies, such as the one de-scribed here, are good examples of the successful application of trans-lational policies and practices. Translational medicine has helped trans-form the process of bringing these types of laboratory-based scientific achievements to clinical application. Translational medicine research has also become a cross-disciplinary field, which is advocated by the international medical community. China, for example, has established about 24 regionally based translational medicine centers and one Inno-vation Alliance (China Innovation Alliance of Translational Medicine & Biotechnology, CIATMBT) since 2009. CIATMBT plans to establish a number of national translational medicine centers to collect innova-tive resources, form a national bio-industry chain, and accelerate the
Antibody-Based Biopharmaceuticals and Translational ResearchZhi-Nan Chen, M.D., Ph.D.
Cell Engineering Research Center and Department of Cell Biology, Fourth Military Medical University, Xi’an, [email protected]
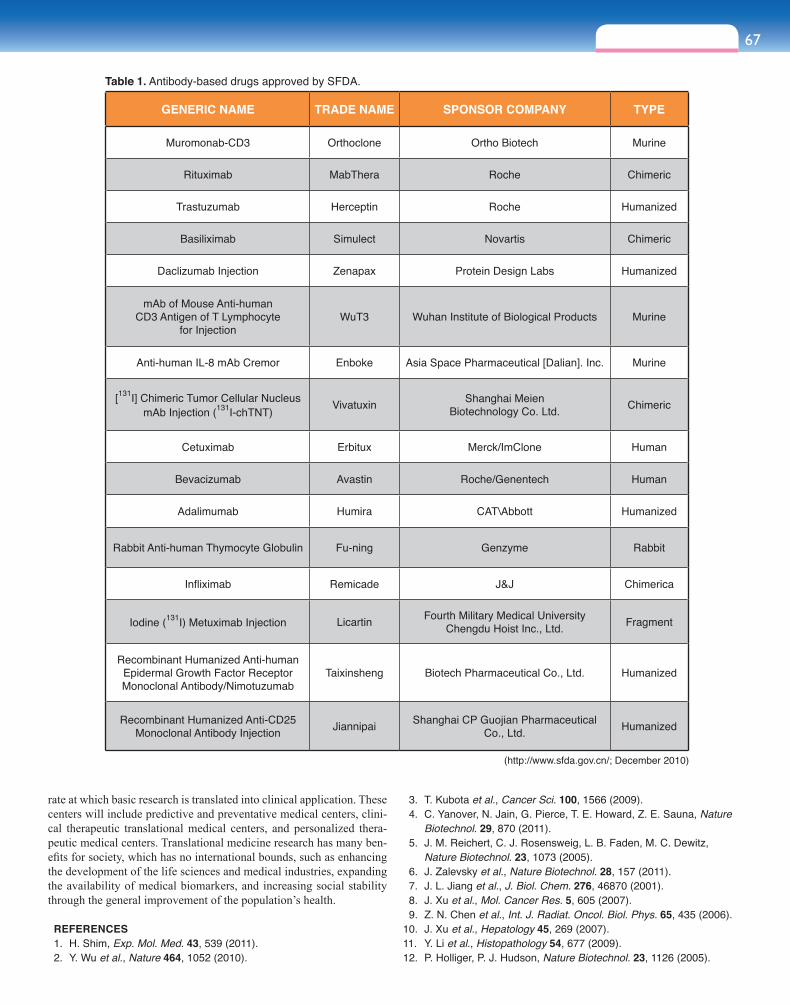
67sect ion nine
GENERIC NAME TRADE NAME SPONSOR COMPANY TYPE
Muromonab-CD3 Orthoclone Ortho Biotech Murine
Rituximab MabThera Roche Chimeric
Trastuzumab Herceptin Roche Humanized
Basiliximab Simulect Novartis Chimeric
Daclizumab Injection Zenapax Protein Design Labs Humanized
mAb of Mouse Anti-human CD3 Antigen of T Lymphocyte
for Injection WuT3 Wuhan Institute of Biological Products Murine
Anti-human IL-8 mAb Cremor Enboke Asia Space Pharmaceutical [Dalian]. Inc. Murine
[131I] Chimeric Tumor Cellular NucleusmAb Injection (131I-chTNT) Vivatuxin Shanghai Meien
Biotechnology Co. Ltd. Chimeric
Cetuximab Erbitux Merck/ImClone Human
Bevacizumab Avastin Roche/Genentech Human
Adalimumab Humira CAT\Abbott Humanized
Rabbit Anti-human Thymocyte Globulin Fu-ning Genzyme Rabbit
Infliximab Remicade J&J Chimerica
Iodine (131I) Metuximab Injection Licartin Fourth Military Medical University Chengdu Hoist Inc., Ltd. Fragment
Recombinant Humanized Anti-human Epidermal Growth Factor Receptor Monoclonal Antibody/Nimotuzumab
Taixinsheng Biotech Pharmaceutical Co., Ltd. Humanized
Recombinant Humanized Anti-CD25 Monoclonal Antibody Injection Jiannipai Shanghai CP Guojian Pharmaceutical
Co., Ltd. Humanized
(http://www.sfda.gov.cn/; December 2010)
Table 1. Antibody-based drugs approved by SFDA.
rate at which basic research is translated into clinical application. These centers will include predictive and preventative medical centers, clini-cal therapeutic translational medical centers, and personalized thera-peutic medical centers. Translational medicine research has many ben-efits for society, which has no international bounds, such as enhancing the development of the life sciences and medical industries, expanding the availability of medical biomarkers, and increasing social stability through the general improvement of the population’s health.
REFERENCES 1. H. Shim, Exp. Mol. Med. 43, 539 (2011). 2. Y. Wu et al., Nature 464, 1052 (2010).
3. T. Kubota et al., Cancer Sci. 100, 1566 (2009). 4. C. Yanover, N. Jain, G. Pierce, T. E. Howard, Z. E. Sauna, Nature
Biotechnol. 29, 870 (2011). 5. J. M. Reichert, C. J. Rosensweig, L. B. Faden, M. C. Dewitz,
Nature Biotechnol. 23, 1073 (2005). 6. J. Zalevsky et al., Nature Biotechnol. 28, 157 (2011). 7. J. L. Jiang et al., J. Biol. Chem. 276, 46870 (2001). 8. J. Xu et al., Mol. Cancer Res. 5, 605 (2007). 9. Z. N. Chen et al., Int. J. Radiat. Oncol. Biol. Phys. 65, 435 (2006).10. J. Xu et al., Hepatology 45, 269 (2007).11. Y. Li et al., Histopathology 54, 677 (2009).12. P. Holliger, P. J. Hudson, Nature Biotechnol. 23, 1126 (2005).

6868
The National Engineering Research Center for Beijing Biochip Technology (also known as CapitalBio Cor-poration, www.capitalbio.com), headed by Professor Jing Cheng, is based in Beijing and is one of China’s
most advanced diagnostics powerhouses. CapitalBio has been developing biochip technologies in collaboration with leading research hospitals in China to satisfy unmet demands from hos-pital bedsides for 10 years. For example, leading researchers from the Department of Otolaryngology and Genetic Testing Center for Deafness, Chinese People’s Liberation Army Gen-eral Hospital noted that nine mutations in four human genomic and mitochondrial genes (GJB2, GJB3, PDS, and 12sRNA) ac-count for approximately 80% of the causes of inherited deaf-ness, including susceptibility to deafness induced by exposure to aminoglycoside antibiotics. The hospital recognized that there was an urgent clinical need for a comprehensive and cost-effective test and approached CapitalBio to develop one. Cap-italBio supplied a multiplexed DNA microarray assay (Figure 1) that provides clinical answers in five hours, which, after four years of clinical trials, is now certified by the Chinese State Food and Drug Administration (SFDA) (1). This assay has been well received by hospitals and, as of March 2011, has been used to screen approximately 21,000 registered deaf persons and, as of January 2012, will be used to screen around 250,000 newborn babies each year in Beijing and Chengdu alone.
CapitalBio has also worked alongside professionals from Beijing Chest Hospital to develop two array-based tuberculosis (TB) test chips, which provide rapid sample-to-answer results in only six hours. One chip identifies 17 different mycobacteria, and the second chip detects the resistance to two first-line drugs, Rifampicin and Isoniazid (2, 3). Conventional plate methods can require up to one month for the results; however, the new array-based testing systems can provide answers on the same day as sampling and are highly accurate. These two multifac-eted TB tests are certified by both the Chinese SFDA and the European Community (the CE IVD mark) and are being used increasingly in Chi-nese hospitals. The drug-resistance chip is also currently undergoing independent evaluation at several sites across China, supported by the Bill and Melinda Gates Foundation.
A number of other products are also close to market, or are being released once they’ve been certified by the SFDA. Hepatitis B virus (HBV) infection is a serious disease in China, and CapitalBio has worked with the Liver Diseases Research Institute of People’s Hospital at Peking University to develop an HBV drug resistance detection array chip for Lamivudine and Adefovir. In addition, collaboration with the hospital’s respiratory department has resulted in the development of a microfluidics-based, rapid-detection platform that identifies 12 major bacterial-associated respiratory infections, including TB (Figure 2). This new detection platform is portable and can provide analysis from sample to results in less than 90 minutes. The platform is intended to be utilitarian in scope with additional assays to detect different pathogens and sample types currently in the research and development process.
Active biochip technologies are also being developed for personal-ized medicine applications, with several seminal advances being in-cluded in a package of fertility and reproductive health tools, which is close to being released to the market. These tools integrate several tests for sperm viability and physiological fitness, such as sperm motility, sperm chemotaxis, and thermotaxis capabilities (Figure 3). The tests will be coupled with on-chip oocyte fertilization and the subsequent on-chip development of the fertilized blastocyst, to provide a fully con-trolled, noninvasive automatic monitoring system for the evaluation of preimplantation embryos (4–6).
CapitalBio’s expertise in instrument technologies is being used to address the industry’s need for more sensitive, more accurate, and more reproducible assay platforms. The Biomixer, a hybridization station, and the Slidewasher, an automatic workstation for slide washing and drying, were all developed to aid the uniform application of standard-ized microarray protocols by clinical lab technicians. The Luxscan 10KB array scanner is an SFDA-certified single-laser confocal scan-ner. The Luxscan 10KA array scanner is a dual-laser confocal scanner that is also directed to clinical use and has recently received confor-mity assessment (CE) in vitro diagnostic medical device certification. The Luxscan Dx24 automatic array scanner (Figure 4) is designed for higher throughput clinical use and was SFDA certified and launched earlier this year. Other near-to-market instruments from CapitalBio in-clude an automated clinical sample preparation platform and a portable instrument for microfluidic chip-based nucleic acid amplification reac-tion and detection.
REFERENCES 1. C. Li et al., Hum. Mutat. 29, 306 (2008). 2. L. Zhu et al., J. Clin. Microbiol. 48, 3654 (2010). 3. Y. Guo et al., Int. J. Tuberculosis Lung Dis. 13, 914 (2009). 4. L. Xie et al., Clin. Chem. 56, 1270 (2010). 5. C. Han et al., Lab Chip 10, 2848 (2010). 6. R. Ma et al., Anal. Chem. 83, 2964 (2011).
Figure 2. Rapid respiratory infection detection chip.
Figure 1. Genetic deafness chip result.
Figure 4. LuxScan Dx24 confocal microarray scanner.
Figure 3. Sperm viability and oocyte fertilization assessment chip.
Biochips for Translational MedicineJing Cheng, Ph.D.
Cheung Kong Professor & Director, Medical Systems Biology Research CenterDepartment of Biomedical Engineering, Tsinghua University, School of Medicine, Beijing, [email protected]



















![MSc in Translational (Neuroscience) · PDF fileMSc in Translational Pathology [Neuroscience] Why Translational Pathology? The MSc Translational Pathology (Neuroscience) course combines](https://img.pdfslide.net/doc/110x75/5a7454947f8b9a0d558bb440/msc-in-translational-neuroscience-a-msc-in-translational-pathology-neuroscience.jpg)