Embed Size (px)
DESCRIPTION
identify the needs of the population we serve, to improve the cancer health disparities and to identify gaps in the resources available to the cancer patients in our community
Citation preview


PAG
E 2
PAGE 2………………………….TABLE OF CONTENTS
PAGE 3……..…….INTRODUCTION/ COMMITTEE
PAGE 4….…….INCIDENCE OF CANCER IN MEN
PAGE 5…….INCIDENCE OF CANCER IN WOMEN
PAGE 6 …………....INCIDENCE GRAPHS BY RACE
PAGE 7…….….LOCAL INCIDENCE COMPARISON
PAGE 8………..…...2011 US DEATH ESTIMATES
PAGE 9……...US DEATH RATES FOR MEN & WOMEN
PAGE 10………………………….…..BREAST CANCER
PAGE 11………….TEXARKANA BREAST CANCER
PAGE 12………...KOMEN COMMUNITY PROFILE
PAGE 13…….....KOMEN COMMUNITY PROFILE
PAGE 14………..KOMEN COMMUNITY PROFILE
PAGE 15…….…..KOMEN COMMUNITY PROFILE
PAGE 16……………………..COLORECTAL CANCER
PAGE 17……………………..COLORECTAL CANCER
PAGE 18…………………………….……LUNG CANCER
PAGE 19…………......TEXARKANA LUNG CANCER
PAGE 20…………………….…….PROSTATE CANCER
PAGE 21…………………...…….PROSTATE CANCER
PAGE 22……………………….….CERVICAL CANCER
PAGE 23……………………..HEAD & NECK CANCER
PAGE 24………….……..…..BREAST CANCER GOAL
PAGE 25……………..…..CERVICAL CANCER GOAL
PAGE 26………………COLORECTAL CANCER GOAL
PAGE 27………………………….LUNG CANCER GOAL
PAGE 28………………….PROSTATE CANCER GOAL
PAGE 29………OBESITY-RELATED CANCER GOAL
PAGE 30………………………..CANCER PREVENTION
PAGE 31..…...NUTRITION & PHYSICAL ACTIVITY
PAGE 32…...NUTRITION FOR CANCER PATIENTS
PAGE 33…TOBACCO CONTROL & PREVENTION
PAGE 34…………………….…...CANCER RESOURCES
PAGE 35………………...……….CANCER RESOURCES
PAGE 36…...COMMUNITY CANCER RESOURCES
PAGE 37…...COMMUNITY CANCER RESOURCES
PAGE 38…….COMMUNITY CANCER RESOURCES
PAGE 39…..OTHER CANCER-RELATED RESOURCES

“To identify the needs of the population we serve; to improve cancer
health disparities, and to identify gaps in the resources available to the
cancer patients in our community.”
The Texarkana Community Needs Assessment Committee is pleased to present to you the findings of this committee as
we have tried to identify the needs of the population we serve, to improve the cancer health disparities and to identify
gaps in the resources available to the cancer patients in our community.
Assessment Objectives:
Determine incidence rates; Identify risks; Identify screenings & prevention activities
Identify treatments available in this community
Identify the cancer related resources we have available in this community
Identify the barriers cancer patients face as they navigate the journey of diagnosis, treatment and survivorship
The committee was also charged with the task of identifying screenings and treatments available in the community as
well as the cancer related resources available. The committee identified barriers cancer patients face as they navigate
the journey of diagnosis, treatment and survivorship. This report contains recent data from the CoC Joint Cancer
Programs of CHRISTUS St. Michael Health System and Wadley Regional Medical Center. The CoC Approved Cancer
Programs data is collected through the UAMS AHEC Southwest Cancer Registry for these facilities. The data identifies
disparities in cancer incidence by race, gender, age and AJCC stage at diagnosis. Geographic data is shown by the Texas
Cancer Registry data as well as Arkansas Cancer Registry data. This publication is intended to assist healthcare
organizations and health care professionals in the pursuit of improving the health and support of the cancer patients in
the Texarkana area.
PLANNING COMMITTEE MEMBERS
Dianne Ketchum, Co-Chair, Editor, UAMS AHEC Southwest
Gary Miller, Co-Chair, Design & Layout, UAMS AHEC Southwest
Shelby Brown, Wadley Regional Medical Center
Tonya Domokos, BEAT Tobacco Control
Patti Finley, Texarkana Affiliate of the Susan G. Komen for the Cure
Kim Lewis, Wadley Regional Medical Center
Julie Huntley, Arkansas Department of Health
Tammy McKamie, CHRISTUS St. Michael Health System
Mary Miller, CHRISTUS St. Michael Health System
Ashley Price, Wadley Regional Medical Center
Jackie Rollins, CHRISTUS St. Michael Health System
Jena Teer, Wadley Regional Medical Center
Brenda Thompson, Wadley Regional Medical Center
Gary Upp, CHRISTUS St. Michael Health System
Lakecia Washington, CHRISTUS St. Michael Health System
REPORT CONTRIBUTORS
Tonya Domokos—Tobacco Report
Alyssa Haley—Susan G. Komen for the Cure Texarkana Community Profile
Julie Huntley—Cervical & Breast Cancer Goals
James Hutcheson, MD—Head & Neck Cancer
Tammy McKamie —Colorectal Cancer
Tammy McKamie, Gary Miller, Brenda Thompson —Patient Navigation
Mary Miller, Jena Teer, Lakecia Washington—Patient Resources
Ashley Price—Obesity Report
Malcolm Smith, MD—Lung Cancer
Gary Upp—Prostate Cancer
*Cover Photo provided by Destiny Carter, UAMS AHEC Southwest
PAG
E 3

PAG
E 4
A graph has been provided to depict the incidence of the most frequent sites of cancers for men diagnosed in the previous five years (Y2007-2011). The total number of this group of incidence of male cancers were 2,676.
Incidence rates of prostate cancer have changed substantially over the last 20 years: rapidly increasing from 1988 to 1992, declining sharply from 1992 to 1995, remaining stable from 1995 to 2000, and de-creasing from 2000 to 2007, due, in part, to changes in prostate cancer screening with the prostate-specific antigen (PSA) blood testing. Incidence rates for both lung and colorectal cancers in men have been declining for many decades.

A graph created shows the incidence of the most frequent sites of cancers for women diagnosed in the previous five years (Y2007-2011). The total number of this group of incidence of female cancers were 2,372.
Breast cancer incidence rates in women decreased by 1.6% per year from 1998 to 2007, likely due in part to a reduction in use of hormone replacement therapy and a slight decline in mammography uti-lization from 2003 to 2005. However, close inspection of the data show that after dramatically de-creasing from 2002 to 2003, breast cancer incidence rates remained relatively unchanged from 2003 to 2007. Similarly, although incidence of lung cancer has increased slightly by 0.4% per year since 1991, rates in the most recent several years have plateaued; in fact, analysis of a larger data set (that only goes back to 1992) shows a significant decrease of 0.3% per year in lung cancer incidence rates in women from 2003 to 2007. Colorectal cancer incidence rates have been decreasing rapidly by 2.2% per year since 1998.
PAG
E 5

PAG
E 6
Cancer incidence rates are consistently higher in African American men than Caucasian men. In con-trast, overall cancer incidence rates are generally higher in Caucasian women than African American women, largely driven by higher breast cancer incidence rates in Caucasians.
Cancer incidence rates are higher in men than women in each racial/ethnic population. Among men, African Americans have the highest incidence followed by Caucasians, Hispanics, American Indians/Alaska Natives, and Asian Americans/Pacific Islanders. Racial differences in cancer incidence among women are less pronounced; Caucasian women have the highest incidence rates followed by African American, American Indian/Alaskan Native, Hispanic, and Asian American/Pacific Islander women.
Important Note: Rates for populations other than Caucasian and African American may be affected by problems in ascertaining race/ethnicity information from medical records. This is likely to result in re-ported rates that are lower than true incidence rates.

PAG
E 7

PAG
E 8
Lung cancer is by far the most common fatal cancer in men (28%), followed by prostate (11%), and colon & rectum (9%). In women, lung (26%), breast (15%), and colon & rectum (8%) are the leading sites of cancer death. The death rate for all cancers combined decreased by 1.9% per year from 2001 to 2007 in men and 1.5% per year from 2002 to 2007 in women. Compared to the peak rates -- in 1990 for men and 1991 for women -- the cancer death rate for all sites combined in 2007 was 22.2% lower in men and 13.9% lower in women.
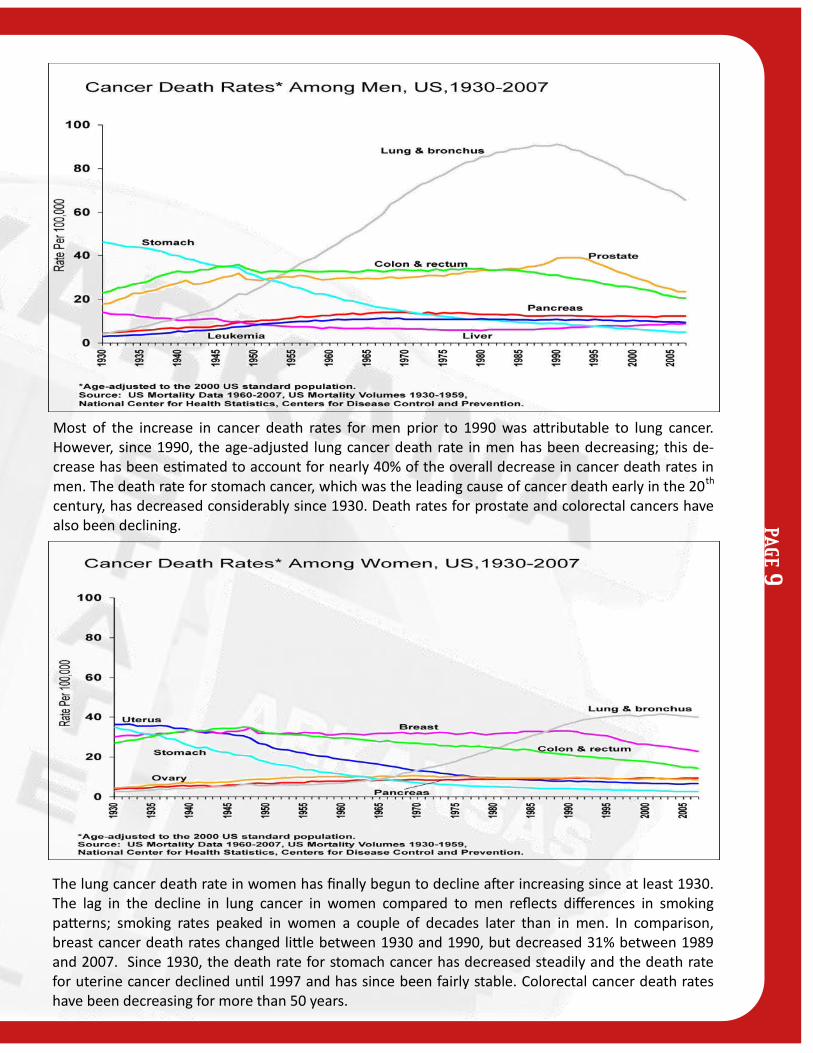
Most of the increase in cancer death rates for men prior to 1990 was attributable to lung cancer. However, since 1990, the age-adjusted lung cancer death rate in men has been decreasing; this de-crease has been estimated to account for nearly 40% of the overall decrease in cancer death rates in men. The death rate for stomach cancer, which was the leading cause of cancer death early in the 20th century, has decreased considerably since 1930. Death rates for prostate and colorectal cancers have also been declining.
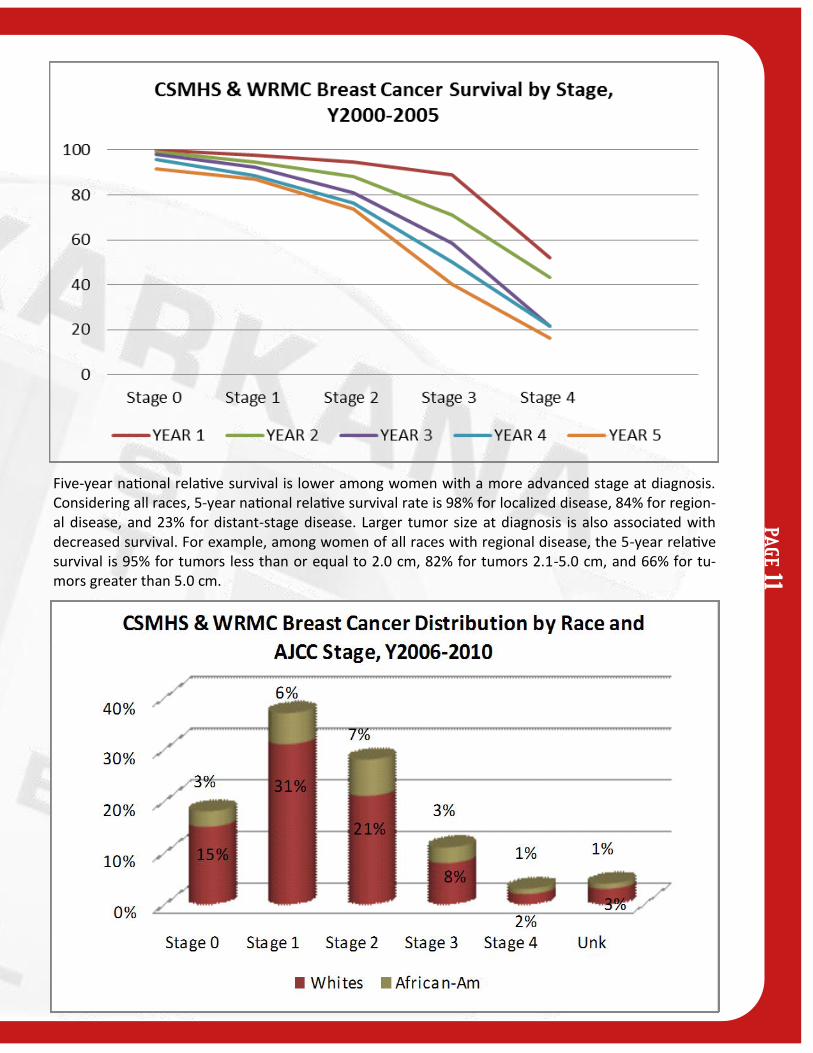
The lung cancer death rate in women has finally begun to decline after increasing since at least 1930. The lag in the decline in lung cancer in women compared to men reflects differences in smoking patterns; smoking rates peaked in women a couple of decades later than in men. In comparison, breast cancer death rates changed little between 1930 and 1990, but decreased 31% between 1989 and 2007. Since 1930, the death rate for stomach cancer has decreased steadily and the death rate for uterine cancer declined until 1997 and has since been fairly stable. Colorectal cancer death rates have been decreasing for more than 50 years.
PAG
E 9

PAG
E 1
0
The American Cancer Society (ACS) estimated 39,840 breast cancer deaths in women are anticipated in 2010. Breast cancer ranks second among cancer deaths in women, exceeded only by the number of lung cancer deaths in women which are expected to be 71,080 in 2010. Breast cancer incidence and death rates generally increase with age. According to the ACS, 95% of new cases and 97% of breast can-cer deaths occurred in women aged 40 and older. Caucasian women have a higher incidence of breast cancer than African American women beginning at age 45. In contrast, African American women have a higher incidence rate before age 45 and are more likely to die from breast cancer at every age. Besides being female, age is the most important risk factor for breast cancer.
Breast cancer remains the most common site of cancer seen in women in Texarkana in 2010. This can-cer totals 37% of the total cancers seen at CHRISTUS St. Michael and Wadley Regional Medical Center. Excluding cancers of the skin, breast cancer, accounting for nearly 1 in 4 cancers in women, is the most common cancer among women in the U.S. Local statistics on breast cancer have revealed 1,014 female breast cancer cases in the last five years, with 14 cases being males. There were 83% early stage and 14% late stage cancers, and 3% unknown/not applicable stage. Distribution of cases by race were 79% Caucasian, 20% African-American women and 1% other in 2010.
Many of the known breast cancer risk factors, such as age, family history, age at first full-term pregnan-cy, early menarche, late menopause, and breast density, are not easily modifiable. However, other fac-tors associated with increased breast cancer risk (postmenopausal obesity, use of combined estrogen and progestin menopausal hormones, alcohol consumption, and physical inactivity) are modifiable. Gene expression analysis has led to the identification of molecularly defined subtypes of breast cancer that are distinct biological features, clinical outcomes, and responses to chemotherapy. Treatment strategies are now being developed based on an individual’s tumor characteristics .
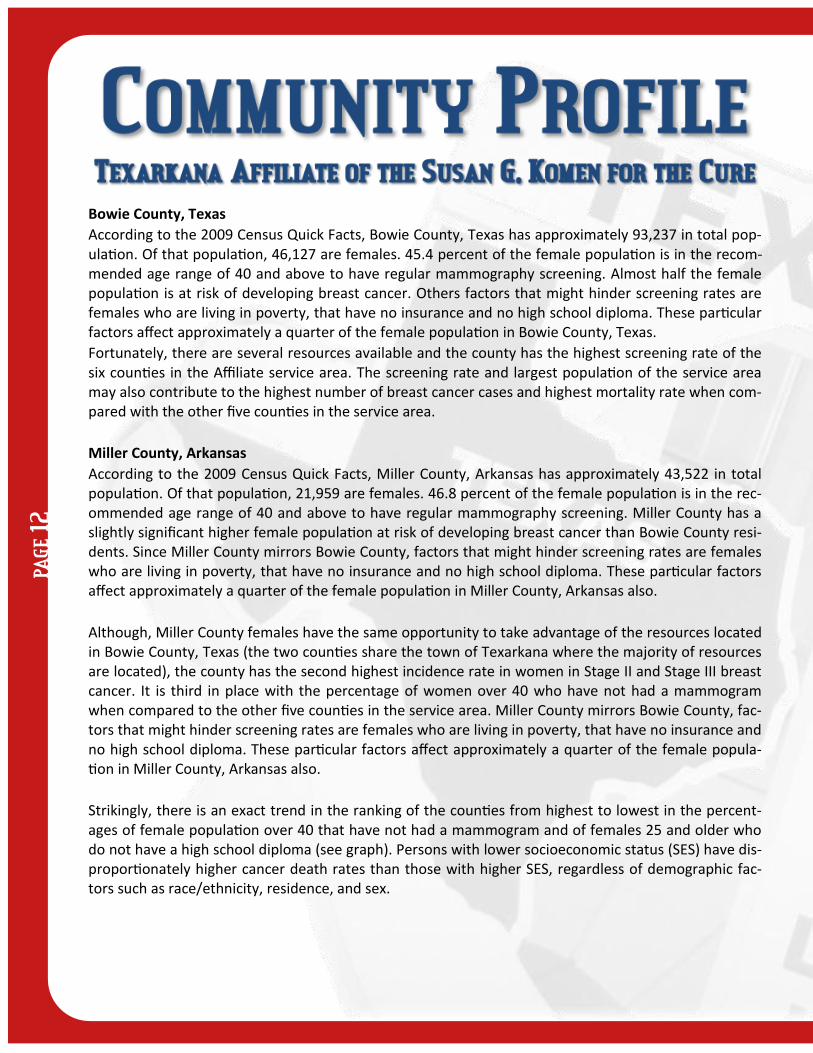
Five-year national relative survival is lower among women with a more advanced stage at diagnosis. Considering all races, 5-year national relative survival rate is 98% for localized disease, 84% for region-al disease, and 23% for distant-stage disease. Larger tumor size at diagnosis is also associated with decreased survival. For example, among women of all races with regional disease, the 5-year relative survival is 95% for tumors less than or equal to 2.0 cm, 82% for tumors 2.1-5.0 cm, and 66% for tu-mors greater than 5.0 cm.
PAG
E 11
PAG
E 1
2
Bowie County, Texas
According to the 2009 Census Quick Facts, Bowie County, Texas has approximately 93,237 in total pop-ulation. Of that population, 46,127 are females. 45.4 percent of the female population is in the recom-mended age range of 40 and above to have regular mammography screening. Almost half the female population is at risk of developing breast cancer. Others factors that might hinder screening rates are females who are living in poverty, that have no insurance and no high school diploma. These particular factors affect approximately a quarter of the female population in Bowie County, Texas.
Fortunately, there are several resources available and the county has the highest screening rate of the six counties in the Affiliate service area. The screening rate and largest population of the service area may also contribute to the highest number of breast cancer cases and highest mortality rate when com-pared with the other five counties in the service area.
Miller County, Arkansas
According to the 2009 Census Quick Facts, Miller County, Arkansas has approximately 43,522 in total population. Of that population, 21,959 are females. 46.8 percent of the female population is in the rec-ommended age range of 40 and above to have regular mammography screening. Miller County has a slightly significant higher female population at risk of developing breast cancer than Bowie County resi-dents. Since Miller County mirrors Bowie County, factors that might hinder screening rates are females who are living in poverty, that have no insurance and no high school diploma. These particular factors affect approximately a quarter of the female population in Miller County, Arkansas also.
Although, Miller County females have the same opportunity to take advantage of the resources located in Bowie County, Texas (the two counties share the town of Texarkana where the majority of resources are located), the county has the second highest incidence rate in women in Stage II and Stage III breast cancer. It is third in place with the percentage of women over 40 who have not had a mammogram when compared to the other five counties in the service area. Miller County mirrors Bowie County, fac-tors that might hinder screening rates are females who are living in poverty, that have no insurance and no high school diploma. These particular factors affect approximately a quarter of the female popula-tion in Miller County, Arkansas also.
Strikingly, there is an exact trend in the ranking of the counties from highest to lowest in the percent-ages of female population over 40 that have not had a mammogram and of females 25 and older who do not have a high school diploma (see graph). Persons with lower socioeconomic status (SES) have dis-proportionately higher cancer death rates than those with higher SES, regardless of demographic fac-tors such as race/ethnicity, residence, and sex.
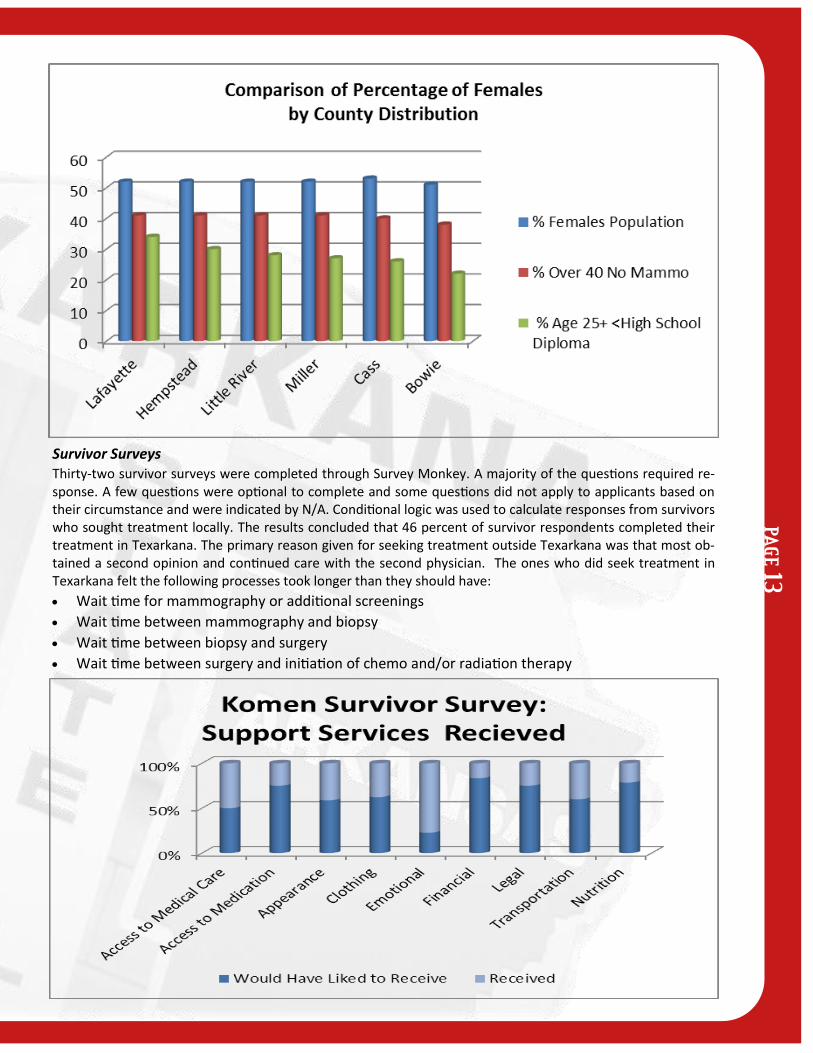
Survivor Surveys Thirty-two survivor surveys were completed through Survey Monkey. A majority of the questions required re-sponse. A few questions were optional to complete and some questions did not apply to applicants based on their circumstance and were indicated by N/A. Conditional logic was used to calculate responses from survivors who sought treatment locally. The results concluded that 46 percent of survivor respondents completed their treatment in Texarkana. The primary reason given for seeking treatment outside Texarkana was that most ob-tained a second opinion and continued care with the second physician. The ones who did seek treatment in Texarkana felt the following processes took longer than they should have:
Wait time for mammography or additional screenings
Wait time between mammography and biopsy
Wait time between biopsy and surgery
Wait time between surgery and initiation of chemo and/or radiation therapy
PAG
E 13

PAG
E 1
4
Key informant interviews were conducted in person and by email questionnaire to gain a better in-sight to breast health resources and barriers through a channel of community organizations: from ex-isting grantees to potential partners in the target counties. The interviews revealed a strong willingness to partner to alleviate the identified barriers, shown below, and bridge the gaps in communication.
Education: All respondents listed a need for more education through brochures, seminars/conferences and health fairs to reach underserved individuals, uneducated individuals, and rural county individuals.
Financial Assistance: The interviewees who were not existing grantees suggested making financial as-sistance available to women with no insurance. For those with insurance, they suggested having finan-cial assistance available for high deductibles or co-pays.
Transportation: All agreed it would help to offer assistance for transportation such as bus tickets, cab fares or gas cards available to bring women to screening facilities. Also, to have a mobile mammogra-phy van available consistently to reach underserved individuals, uneducated individuals, and rural county individuals.
The key informant interviews, provider and survivor surveys and focus groups all echoed the same needs for our community regardless of ethnicity; more education, financial assistance, and help with transportation. While Bowie County, Texas and Miller County, Arkansas have access to three major breast resources (Arkansas BreastCare, Texas Breast and Cervical Cancer services, and Komen) and a fully accredited, comprehensive cancer center at CHRISTUS St. Michael Health System, the screening rates, stage at diagnosis statistics and high mortality rates may indicate not enough women are being reached through existing educational methods. Several of the key informants and focus group partici-pants were not aware of financial resources in any of the three counties.
Conclusions: What We Learned & What We Will Do
Statistical data reviewed reported the counties of interest had high mortality rates in African Ameri-cans in Bowie County, Texas. Caucasian females had a higher incidence rates and local cancer cases in Miller County, Arkansas. Stage III and IV incidence rates in Caucasian females companied with high lev-els of poverty, low levels of education and higher percentages of uninsured females plagued Lafayette County, Arkansas.
Research of programs and services revealed all three target areas were either partially or fully desig-nated as health professional shortage areas. Even with the concentration of medical providers and fi-nancial assistance in Texarkana, Texas, many women still cannot access necessary screenings and/or treatment because of barriers such as low educational levels, cultural beliefs and transportation.
After conducting focus groups and key informant interviews, we learned the women of the community and the community leaders were not aware of all breast health resources available. This is an oppor-tunity for Komen to increase visibility and presence not only in the target area but in the service area as a whole.
Gaps in communication could be addressed by holding forums or symposiums for resource providers. Community leaders can learn about existing resources and partner to bridge gaps such as transporta-tion or develop an implementation of nurse navigators.
In addition, African American females were more culturally sensitive than Caucasian women when it came to body image after treatment. Both races were equally concerned with the perception of look-ing normal afterwards. However, the cultural pride of African American female is what will prevent those women from seeking treatment. Komen can partner with non-medical providers such as the Texarkana Housing Authority and predominately African American churches to address these deadly concerns and help decrease mortality rates in African American females.
Provider surveys confirmed breast information was available at all OB/GYN offices but limited in other provider offices as stated in the focus groups. This one factor may contribute to the high incidence rate of Stage III and Stage IV diagnoses and high mortality rates in Bowie County, Texas and Miller County, Arkansas. Komen can reach out to local educational institutions to develop literature that is appropriate reading level in our service area. Komen can also partner with local healthcare facilities in Lafayette County to assist with transportation expenses through means of gas cards.
Texarkana Affiliate of the Susan G. Komen for the Cure Action Plan
Priority #1: Education/Awareness Goal #1: Increase breast cancer education and awareness to African American females in Bowie County, Texas by 2012.
Objective 1.1: To decrease late stage diagnosis and high mortality rates by increasing partnerships with community based organizations that predominantly serve African American females.
Objective 1.2: Support the development of culturally appropriate marketing materials to increase education and awareness about breast cancer among African American women of a low socioeconomic status.
Goal #2: Increase breast cancer education and awareness among medical providers in Affiliate service area.
Objective 2.1: Hold Komen sponsored provider education workshops about breast health guidelines and resources available in the target communities by January 2012.
Objective 2.2: Improve statistical gathering methods in our community by requesting that all grantees provide the Can-cer Registry with yearly data on all breast screenings by January 2012.
Priority #2: Access Goal #1: Increase funding for breast cancer prevention and screening services Bowie County, Texas and Miller County and Lafayette County in Arkansas by 2012.
Objective 1.1: Hold at least one grant writing workshop in the target areas by January 2012.
Objective 1.2: Explore partnerships with non-medical organizations in target areas to reach women by non-traditional means immediately.
Priority #3: Coordination of Resources Goal #1: Hold at least one breast health resource symposium every year that facilitate knowledge-sharing of programs and resources among organizations.
PAG
E 15
PAG
E 1
6
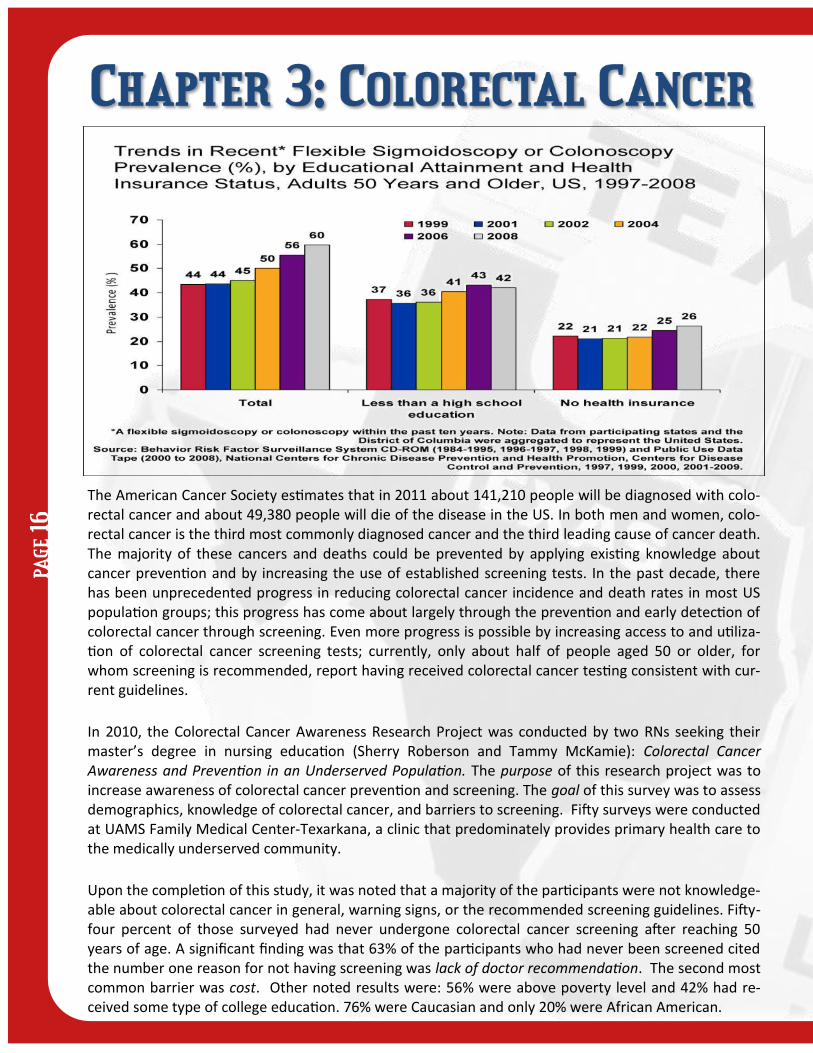
The American Cancer Society estimates that in 2011 about 141,210 people will be diagnosed with colo-rectal cancer and about 49,380 people will die of the disease in the US. In both men and women, colo-rectal cancer is the third most commonly diagnosed cancer and the third leading cause of cancer death. The majority of these cancers and deaths could be prevented by applying existing knowledge about cancer prevention and by increasing the use of established screening tests. In the past decade, there has been unprecedented progress in reducing colorectal cancer incidence and death rates in most US population groups; this progress has come about largely through the prevention and early detection of colorectal cancer through screening. Even more progress is possible by increasing access to and utiliza-tion of colorectal cancer screening tests; currently, only about half of people aged 50 or older, for whom screening is recommended, report having received colorectal cancer testing consistent with cur-rent guidelines.
In 2010, the Colorectal Cancer Awareness Research Project was conducted by two RNs seeking their master’s degree in nursing education (Sherry Roberson and Tammy McKamie): Colorectal Cancer Awareness and Prevention in an Underserved Population. The purpose of this research project was to increase awareness of colorectal cancer prevention and screening. The goal of this survey was to assess demographics, knowledge of colorectal cancer, and barriers to screening. Fifty surveys were conducted at UAMS Family Medical Center-Texarkana, a clinic that predominately provides primary health care to the medically underserved community.
Upon the completion of this study, it was noted that a majority of the participants were not knowledge-able about colorectal cancer in general, warning signs, or the recommended screening guidelines. Fifty-four percent of those surveyed had never undergone colorectal cancer screening after reaching 50 years of age. A significant finding was that 63% of the participants who had never been screened cited the number one reason for not having screening was lack of doctor recommendation. The second most common barrier was cost. Other noted results were: 56% were above poverty level and 42% had re-ceived some type of college education. 76% were Caucasian and only 20% were African American.

BARRIERS
Cost of Colonoscopy – estimated at $2,000.00 out of pocket
Lack of education in the community
Miller County Health Clinic only offers Digital Rectal Exams on a limited bases
Bowie County Health Clinic does not offer any type of colorectal testing
Lack of agencies providing funding for screenings
SUGGESTIONS TO IMPROVE EDUCATION &ACCESS
Apply for grants that help subsidize education & screenings
Ask GI physicians to provide reduced cost for recommended screenings to under/uninsured pts.
Ask hospitals to provide reduced cost for recommended screenings to under and uninsured pts.
Ask County Clinics to provide Hemoccult testing to pts. 50 years old & older.
Colorectal educational symposium for healthcare providers and the public
Involve colorectal-focused healthcare providers to join local task force.
RISK FACTORS
Age
Family history
Genetics-Personal history of breast, ovarian, or uterine cancer
Dietary habits
PREVENTION
Screening digital rectal exam
Colonoscopy beginning at age 50
Earlier if strong family history or symptoms
Removal of polyps (adenomas) in the colon
Following a low fat high fiber diet
Fecal occult blood testing
RESOURCES AVAILABLE
Genetic Education & Testing
Community Health Worker/Nurse Navigator
Local Health Fairs
Three separate G. I. Clinics
Two County Clinics
Two Community Hospitals
One For-profit
One Non For-profit
University-based, satellite primary care clinic
PAG
E 17
PAG
E 1
8
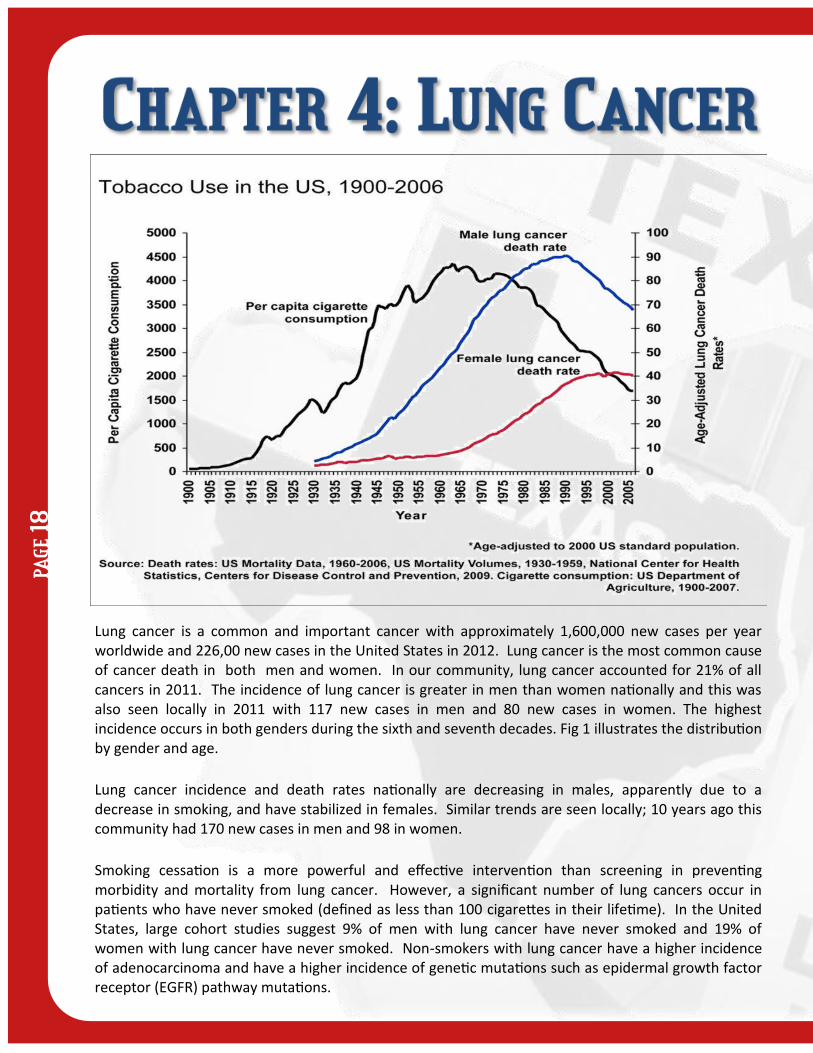
Lung cancer is a common and important cancer with approximately 1,600,000 new cases per year worldwide and 226,00 new cases in the United States in 2012. Lung cancer is the most common cause of cancer death in both men and women. In our community, lung cancer accounted for 21% of all cancers in 2011. The incidence of lung cancer is greater in men than women nationally and this was also seen locally in 2011 with 117 new cases in men and 80 new cases in women. The highest incidence occurs in both genders during the sixth and seventh decades. Fig 1 illustrates the distribution by gender and age.
Lung cancer incidence and death rates nationally are decreasing in males, apparently due to a decrease in smoking, and have stabilized in females. Similar trends are seen locally; 10 years ago this community had 170 new cases in men and 98 in women.
Smoking cessation is a more powerful and effective intervention than screening in preventing morbidity and mortality from lung cancer. However, a significant number of lung cancers occur in patients who have never smoked (defined as less than 100 cigarettes in their lifetime). In the United States, large cohort studies suggest 9% of men with lung cancer have never smoked and 19% of women with lung cancer have never smoked. Non-smokers with lung cancer have a higher incidence of adenocarcinoma and have a higher incidence of genetic mutations such as epidermal growth factor receptor (EGFR) pathway mutations.

PAG
E 19

PAG
E 2
0
According to the American Cancer Society (ACS), as published in their Cancer Facts and Figures 2012 there will be an estimated 241,740 new cases of prostate cancer in the United States in 2012, making it the most frequently diagnosed form of cancer among men other than skin cancer. For reasons that are unclear, the incidence rates are significantly higher among African Americans than in the Cauca-sian population, 241 per 100,000 men compared to 149 per 100,000 men respectively (2008 data). Prostate cancer has been shown to have the highest incidence rate of all cancers among males in both Arkansas and Texas. As noted in the graph above, prostate cancer remains the highest incidence among men in the U.S. Data from both the Texas and Arkansas Cancer Registry Query Systems to obtain five-year data for the Texarkana Health Systems Primary and Secondary Markets, consisting of Bowie, Cass, Morris and Red River Counties in Texas and Columbia, Hempstead, Howard, Lafayette, Little River, Miller, Nevada and Sevier Counties in Arkansas. Considered a Secondary Market area, the data for McCurtain County in Oklahoma was not obtained for the purpose of this study. The data from the states of Texas and Ar-kansas correlate closely with what is seen on the national level.

EARLY DETECTION
Historically, there has been insufficient data to recommend for or against routine screening for pros-tate cancer with the PSA (prostate specific antigen) test. The ACS recommends that men at age 50 should receive information about the benefits and limitations of testing, if they have an expected life expectancy of at least 10 years. For those at a higher risk, defined as being African American or hav-ing a close relative diagnosed before age 65, the same process should begin at age 45. If several rela-tives have been diagnosed at an early age, screenings should begin at age 40. The information provid-ed should allow them to make an informed decision based upon their personal values and prefer-ences.
Earlier this year, the United States Preventive Services Task Force recommended that doctors and patients not screen for prostate cancer because the potential benefits do not outweigh the potential harm, stating that evidence shows that screening prevents less than one death from prostate cancer for every 1,000 men tested. It is their opinion that most of the cancers identified by screening would not have caused problems for the patients. Side effects of treatment include sexual dysfunction, bowel and bladder incontinence, and even death. This determination has been rebuked by profes-sional organizations, including the American Urologic Association and Large Urology Group Practice Association, with the opinions that there are studies that demonstrate the efficacy of screening tests, focus on education of Primary Care Physicians on targeted screening and education, and that men should still be given the choice.
DATA SUMMARY
Counties in the Service area with the largest number of cases over a five-year period:
Bowie County, TX= 321
Miller County, AR= 167
Cass County, TX= 151
Columbia County, AR= 109
Counties with the highest overall Incidence:
Columbia County, AR= 185.3
Nevada County, AR= 178.4
Miller County, AR= 160.7
Hempstead County, AR= 160.6
Counties with the highest incidence in Caucasian population:
Columbia County, AR= 169.0
Red River County, TX= 143.2
Cass County, TX= 142.5
Howard County, AR= 141.5
Counties with the highest incidence in the African American population:
Hempstead County, AR= 236.1
Miller County, AR= 230.2
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Stage 1 Stage 2 Stage 3 Stage 4
White 7.5% 83.9% 3.9% 4.6%
Black 4.5% 84.5% 4.5% 6.5%
Hispanic 100.0%
Pe
rce
nta
ge
CHRISTUS ST. Michael & Wadley Prostate Cancer Distribution by Race and AJCC Stage, Y 2007-2011
PAG
E 21

PAG
E 2
2
The American Cancer Society estimated 12,710 new cases of cervical cancers are expected to be diag-nosed in 2011 and the incidence of this cancer have decreased in the past several decades in both Caucasian and African-American women. Mortality rates continue to decline due to the prevention and early detection message and the result of PAP testing. The death rates have remained stable since 2003.
Prevention: There are two vaccines approved for the prevention of the most common types of HPV infection that cause cervical cancer; Gardasil is recommended for use in females 9 to 26 years of age, and Cervix in females 10 to 25 years of age. In December 2010, Gardasil was also approved for use in males 9 to 26 years of age to prevent anal cancer and associated precancerous lesions; approximately 90% of anal cancers have been linked to HPV infection. These vaccines cannot protect against estab-lished infections, nor do they protect against all HPV types. Screening can prevent cervical cancer by detecting precancerous lesions.
Screening: As screening has become more common, pre-invasive lesions of the cervix are detected far more frequently than invasive cancer. The PAP test is the most widely used cervical cancer screening method. Fortunately, most cervical pre-cancers develop slowly, so nearly all cancers can be prevented if a woman is screened regularly. It is important for all women, even those who have received the HPV vaccine, to follow cervical cancer screening guidelines.
Survival: The one (1) and five (5)- year survival rates for cervical cancer patients are 87% and 70% re-spectively. The 5 year survival rate for patients diagnosed with localized disease is 97%. Cervical can-cer is diagnosed more frequently in Caucasians (50%) than in African Americans (43%). Our local data reveals Caucasians have a 67% incidence of cervical cancer and African Americans have a 30% rate.
0%
5%
10%
15%
20%
25%
30%
Stage0
Stage I Stage2
Stage3
Stage4
UnkStage
Per
cen
tage
CHRISTUS ST. Michael & Wadley Regional Medical Center Cervical Cancer Distribtuion by AJCC Stage, Y2007-2011
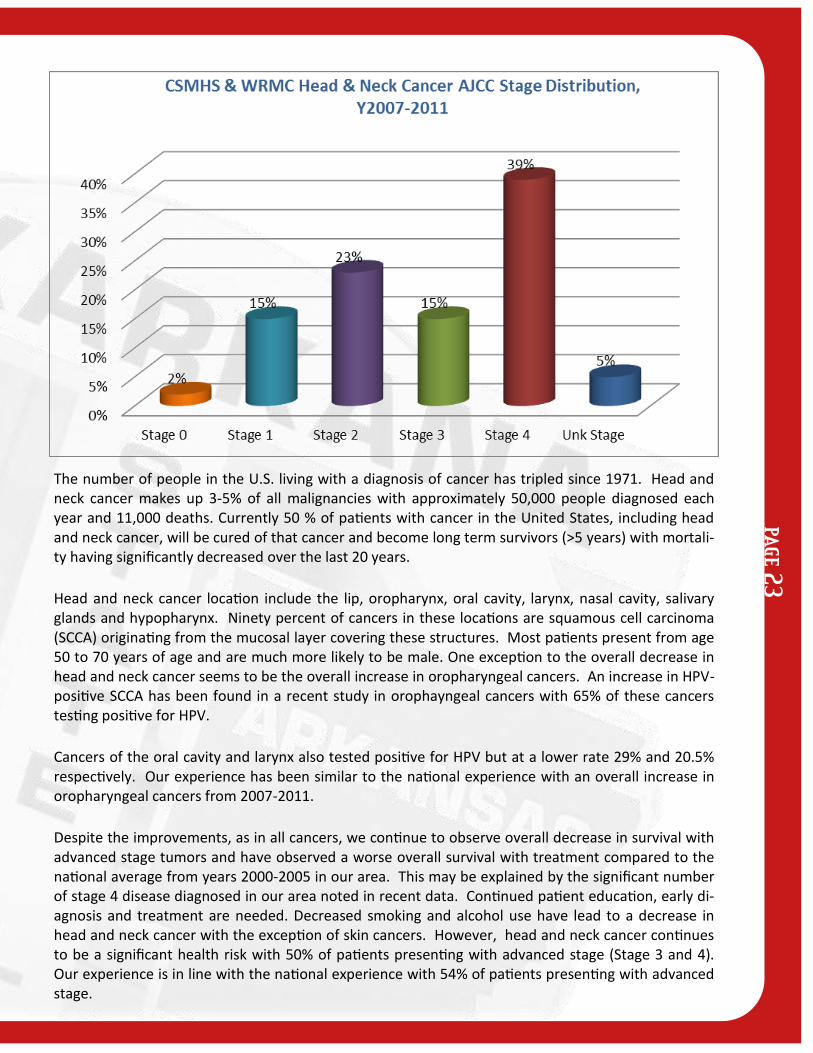
The number of people in the U.S. living with a diagnosis of cancer has tripled since 1971. Head and neck cancer makes up 3-5% of all malignancies with approximately 50,000 people diagnosed each year and 11,000 deaths. Currently 50 % of patients with cancer in the United States, including head and neck cancer, will be cured of that cancer and become long term survivors (>5 years) with mortali-ty having significantly decreased over the last 20 years.
Head and neck cancer location include the lip, oropharynx, oral cavity, larynx, nasal cavity, salivary glands and hypopharynx. Ninety percent of cancers in these locations are squamous cell carcinoma (SCCA) originating from the mucosal layer covering these structures. Most patients present from age 50 to 70 years of age and are much more likely to be male. One exception to the overall decrease in head and neck cancer seems to be the overall increase in oropharyngeal cancers. An increase in HPV-positive SCCA has been found in a recent study in orophayngeal cancers with 65% of these cancers testing positive for HPV.
Cancers of the oral cavity and larynx also tested positive for HPV but at a lower rate 29% and 20.5% respectively. Our experience has been similar to the national experience with an overall increase in oropharyngeal cancers from 2007-2011.
Despite the improvements, as in all cancers, we continue to observe overall decrease in survival with advanced stage tumors and have observed a worse overall survival with treatment compared to the national average from years 2000-2005 in our area. This may be explained by the significant number of stage 4 disease diagnosed in our area noted in recent data. Continued patient education, early di-agnosis and treatment are needed. Decreased smoking and alcohol use have lead to a decrease in head and neck cancer with the exception of skin cancers. However, head and neck cancer continues to be a significant health risk with 50% of patients presenting with advanced stage (Stage 3 and 4). Our experience is in line with the national experience with 54% of patients presenting with advanced stage.
PAG
E 23

PAG
E 2
4
Strategic Action Conduct educational campaigns in the service area
-Articles in local newspapers
-Health fairs
-Radio announcements
-Collaborate with Churches, women’s groups and community service agencies
Expand and promote access to women in rural areas by increasing alternative screening opportunities.
Improve health care professional knowledge, practice behaviors and support related to Breast Cancer screening guidelines and develops appropriate follow-up for those who receive abnormal cancer screen-ing results.
Implement evidence-based strategies to decrease disparities in gen-der, racial/ethic populations, and rural communities related to inci-dence and mortality of Breast Cancer.
OBJECTIVES:
1. Increase breast cancer education and awareness to increase early detection of breast cancer through screening.
2.Increase breast cancer education and awareness among Health Care provid-ers on the resources and appropriate screening guidelines.
3. Recommend developing a multidisciplinary team approach to Breast Care.
4. To increase awareness and knowledge of potential Hereditary Cancer Syn-dromes.
RISKS:
Age
Family History
Early menarche
Late menopause
Post menopausal obesity
Use of combined estrogen and progestin menopausal hormones
Alcohol consumption
Physical activity
Genetics
Late age at first full time pregnancy
No full-term pregnancies

OBJECTIVES:
1. Increase knowledge and empower women in regards to im-portance of cervical cancer screening and cervical cancer.
2. Educate Health Care providers on the re-sources and cervical cancer risks to eliminate barriers to cervical can-cer screening and treat-ment.
3. Explore the possibil-ity of recruiting a gyne-cological oncologist to the service area so women do not have to travel to see a special-ist.
RISKS
· History of abnormal
Pap test
· HPV
· Multiple partners in a
lifetime
· Early age at first inter-course (before age 16)
· HIV/AIDS/immunocompromised
· DES Exposure
· Smoking
Strategic Action Conduct educational campaigns in the service area.
-Articles in local newspaper
-Health Fairs
-Radio announcements
-Collaborate with Churches, women’s groups and community service agencies
Improve health care professional’s knowledge, practice behaviors and support related to Cervical Cancer screening guidelines, HPV testing, diagnosis and prevention including vaccination.
Provide education to women in our service area to include available resources, screening guidelines, HPV testing, diagnosis and preven-tion, including vaccination.
PAG
E 25

PAG
E 2
6
Strategic Action Educate communities on the importance of colorectal screenings,
helping to reduce myths and fears centered around screening op-tions.
Expand capacity for colon and rectal cancer screening and follow-up.
Increase and improve access to care by reducing structural and fi-nancial barriers.
Using evidence-based interventions, provide education on colon and rectal cancer and promote screening guidelines and awareness of insurance coverage options, including all underserved populations.
Improve health professional knowledge, practice behaviors, and sys-tems support related to improving service delivery.
OBJECTIVES:
1. Increase proportion of adults who receive colon and rectum cancer screening according to national guidelines.
2. Reduce the rate of invasive colon and rec-tum cancer
3. To increase awareness and knowledge of poten-tial Hereditary Cancer Syndromes.
RISKS:
Age
Family History
Personal History
Race
High Dietary Fat Intake
Lifestyle Factors
Smoking
Body Mass Index
Ethanol Consumption
Diabetes
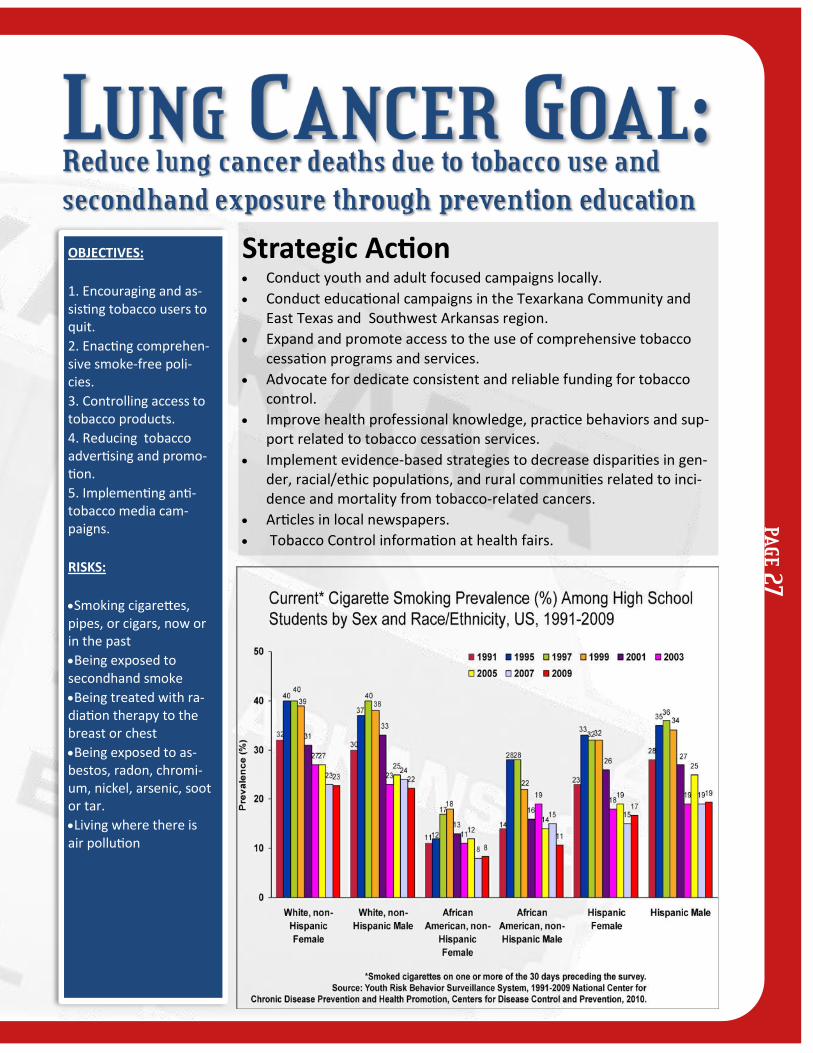
Strategic Action Conduct youth and adult focused campaigns locally.
Conduct educational campaigns in the Texarkana Community and East Texas and Southwest Arkansas region.
Expand and promote access to the use of comprehensive tobacco cessation programs and services.
Advocate for dedicate consistent and reliable funding for tobacco control.
Improve health professional knowledge, practice behaviors and sup-port related to tobacco cessation services.
Implement evidence-based strategies to decrease disparities in gen-der, racial/ethic populations, and rural communities related to inci-dence and mortality from tobacco-related cancers.
Articles in local newspapers.
Tobacco Control information at health fairs.
OBJECTIVES:
1. Encouraging and as-sisting tobacco users to quit.
2. Enacting comprehen-sive smoke-free poli-cies.
3. Controlling access to tobacco products.
4. Reducing tobacco advertising and promo-tion.
5. Implementing anti-tobacco media cam-paigns.
RISKS:
Smoking cigarettes, pipes, or cigars, now or in the past
Being exposed to secondhand smoke
Being treated with ra-diation therapy to the breast or chest
Being exposed to as-bestos, radon, chromi-um, nickel, arsenic, soot or tar.
Living where there is air pollution
PAG
E 27

PAG
E 2
8
OBJECTIVES:
1. Identify the popula-tions in the Service Area that are at the highest risk for Prostate Cancer.
2. Determine most effi-cient methodologies for disseminating Prostate Cancer educational ma-terials.
3. Increase the number of men who obtain needed screening pro-cedures at appropriate times.
4. Identify methodolo-gies that will increase compliance with recom-mended screenings.
RISKS
African- American de-scent
Over 50 years of age
Family history
Strategic Action Establish screening events in high incidence areas with a strong focus
upon the African-American population.
Collaborate with multiple community organizations to meet the needs in rural medically underserved areas.
Educational focus on September as Prostate Cancer Awareness Month
Provide physician education in high incidence areas.
Provide education materials to African-American Community through churches.
Age-adjusted five-year prostate cancer incidence
rates per 100,000 men
All Caucasian African American
Arkansas 157.0 148.0 210.3
Texas 141.8 140.1 206.4

Strategic Action Increase evidence-based nutrition behaviors to reduce obesity rates
locally.
Increase physical activity behaviors shown to reduce cancer risk
Eat more fruits & vegetables
Provide healthy foods in vending machines and cafeterias
OBJECTIVES:
1. Encourage regular screenings for cancer detection
2. Encourage employers to provide opportunity for physical activity at work
RISKS:
Certain cancer types
Breast
Colon & Rectum
Endometrium
Esophagus
Kidney
Pancreas
Overweight Raises Risk
Gallbladder
Liver
Non-Hodgkin Lympho-ma
Multiple Myeloma
Cervix
Ovary
Aggressive forms of Prostate Cancer
PAG
E 29

PAG
E 3
0
This slide highlights the obesity epidemic as mentioned in the previous slide. In 2009, over 55% of adults in all states, except District of Columbia, were overweight or obese, compared to none in 1992.
Achieve and maintain a healthy weight throughout life.
Be as lean as possible throughout life without being underweight.
Avoid excess weight gain at all ages. For those who are overweight or obese, losing even a small amount of weight has health benefits and is a good place to start.
Get regular physical activity and limit intake of high-calorie foods and drinks as keys to help maintain a healthy weight.
Be physically active.
Adults: Get at least 150 minutes of moderate intensity or 75 minutes of vigorous intensity activity each week (or a combination of these), preferably spread throughout the week.
Children and teens: Get at least 1 hour of moderate or vigorous intensity activity each day, with vigorous activity on at least 3 days each week.
Limit sedentary behavior such as sitting, lying down, and watching TV.

Eat a healthy diet, with an emphasis on plant foods.
· Choose foods and drinks in amounts that help you get to and maintain a healthy weight.
Choose nutrient dense foods, not calorically dense foods.
Read food labels to become more aware of portion sizes and calories. Be aware that "low-fat" or "non-fat" does not necessarily mean "low-calorie." Eat smaller portions when eating high-calorie foods.
Choose vegetables, whole fruit, and other low-calorie foods instead of calorie-dense
foods such as French fries, potato and other chips, ice cream, donuts, and other sweets.
Limit your intake of sugar-sweetened beverages such as sodas and sports drinks
When you eat away from home, be especially mindful to choose food low in calories, fat, and added sugar, and avoid eating large portion sizes.
· Limit how much processed meat and red meat you eat.
Limit your intake of processed meats, i.e. bacon, sausage, lunch meats, and hot dogs.
Choose fish, poultry, or beans instead of red meat (beef, pork, and lamb).
If you eat red meat, choose lean cuts and eat smaller portions.
Prepare proteins by baking, broiling, or poaching rather than by frying or charbroiling.
· Eat at least 2½ cups (recommended 5 or more) of vegetables and fruits each day.
Eat a variety of vegetables and fruits each day.
Eat whole fruits and vegetables; choose 100% juice if you do drink juices.
Limit your use of creamy sauces, dressings, and dips with fruits and vegetables.
· Choose whole grains instead of refined grain products.
Choose 3 or more servings of whole-grain breads, pasta, brown rice and cereals instead of breads, cereals, and pasta made from refined grains, and white rice each day.
Limit your intake of refined carbohydrate foods, including pastries, candy, sugar-sweetened breakfast cereals, and other high-sugar foods.
Consume 3 cups of fat-free or low-fat milk or equivalent milk products every day.
If you drink alcohol, limit your intake.
· Drink no more than 1 drink per day for women or 2 per day for men.
BRFSS Prevalence and Trends Data
Arkansas & Texas Comparative Report
Overweight and Obesity (BMI)
Weight Classification by Body Mass Index (BMI)
Year: AR % CI n TX% CI n
1995 17.5 (15.4-19.6) 288 15.9 (13.8-18.0) 249
2000 23.3 (21.5-25.1) 676 23.1 (21.7-24.5) 1073
2005 28 (26.5-29.5) 1422 27 (25.5-28.5) 1585
2010 30.9 (28.5-33.2) 1186 31.7 (30.2-33.2) 5225
%=Weighted Pecentage, CI= Confidence interval, n=Cell size (Numerator)
BRFSS Survey Data
Centers for Disease Control and Prevention (CDC), Behavioral Risk Factor Surveillance
System Survey Data, Atlanta, GA; US Department of Health & Human Services, Center
For Disease Control and Prevention, Years 1995, 2000, 2005, 2010
PAG
E 31

PAG
E 3
2
Nutrition and Physical Activity in Cancer Treatment The diet is an important part of cancer treatment. Eating the right kinds of foods before, during, and after treatment can help the patient feel better and stay stronger. To ensure proper nutrition, a person has to eat and drink enough of the foods that contain key nutrients (vitamins, minerals, protein, carbohydrates, fat, and water). For many patients, however, some side effects of cancer and cancer treatments make it difficult to eat well. Symptoms that interfere with eating include anorexia, nausea, vomiting, diarrhea, constipation, mouth sores, trouble with swallowing, pain, depression, and anxiety. Appetite, taste, smell, and the ability to eat enough food or absorb the nutrients from food may be affected. Malnutrition (lack of key nutrients) can result, causing the patient to be weak, tired, and unable to resist infections or withstand cancer therapies. Eating too little protein and calories is the most common nutrition problem facing many cancer patients. Protein and calories are important for healing, fighting infection, and providing energy.
Prevent or correct malnutrition
Prevent wasting of muscle, bone, blood, organs, and other lean body mass
Help the patient tolerate treatment
Reduce nutrition-related side effects and complications.
Maintain strength and energy
Protect ability to fight infection
Help recovery and healing
Maintain or improve quality of life
Key Components of Education and Meal Planning
When side effects of cancer or cancer treatment interfere with normal eating, adjustments can be made to ensure the patient continues to get the necessary nutrition. Medications may be given to stimulate the appetite. Eating foods that are high in calories, protein, vitamins and minerals is usually advised. Other suggestions for meal planning include:
Some cancer-fighting foods include dark green, yellow, and orange fruits and vegetables, red grapes, cruciferous vegetables, orange juice, tomatoes, olive and canola oil, garlic, legumes, strong coffee, whole grains, soy, and other plant estrogens.
Patients should be encouraged to keep easy-to-eat foods, such as single portions of canned fruit, yogurt, pudding, or commercially available nutrition supplements on hand at all times.
For more nutritional information related to cancer treatment, talk to your oncology provider or visit the American Cancer Society website at www.cancer.org.

Why Is Preventing Tobacco Use Important?
Tobacco use is the single most preventable cause of death and disease in the United States. Each year, approximately 443,000 Americans die from tobacco-related illnesses. For every person who dies from tobacco use, 20 more people suffer with at least 1 serious tobacco-related illness. In addition, tobacco use costs the U.S. $193 billion annually in direct medical expenses and lost productivity.
Scientific knowledge about the health effects of tobacco use has increased greatly since the first Sur-geon General’s report on tobacco was released in 1964.
Tobacco use causes:
Cancer
Heart disease
Lung diseases (including emphysema, bronchitis, and chronic airway obstruction)
Premature birth, low birth weight, stillbirth, and infant death
There is no risk-free level of exposure to secondhand smoke. Secondhand smoke causes heart disease and lung cancer in adults and a number of health problems in infants and children, including:
Severe asthma attacks
Respiratory infections
Ear infections
Sudden infant death syndrome (SIDS)
Smokeless tobacco causes a number of serious oral health problems, including cancer of the mouth and gums, periodontitis, and tooth loss. Cigar use causes cancer of the larynx, mouth, esophagus, and lung.
Helping Smokers Quit
Preventing tobacco use and helping tobacco users quit can improve the health and quality of life for Americans of all ages. People who stop smoking greatly reduce their risk of disease and premature death. Benefits are greater for people who stop at earlier ages, but quitting tobacco use is beneficial at any age.
PAG
E 33

PAG
E 3
4
Patient Navigation Cancer is second only to cardiovascular disease as the most costly chronic disease in the United States. A cancer diagnosis often means lengthy, costly treatments. The financial costs in medical care and lost productivity are staggering, bankrupting families and burdening health care systems (Texas Cancer Plan 2012). Patients and their families diagnosed with cancer often feel “lost and over-whelmed” when trying to navigate the healthcare system.
One method of helping offset some these issues is the use of a patient navigator in the cancer care process. In simplest terms, the patient navigator is an individual (lay or health professional) that can help patients, families, and caregivers navigate the many systems needed during the cancer journey. The Colorado Patient Navigation Training Program further defines the role as:
“A patient navigator is a member of the healthcare team who helps patients ‘navigate’ the healthcare system and get timely care. Navigators work with patients to identify their barriers to healthcare and connect them to the resources they may need such as financial assistance, counseling, language translation or transportation.” (http://patientnavigatortraining.org)
Resources Several health care organizations in Texarkana offer patient navigation services, as well as support systems for accessing cancer detection and treatment methods. The Arkansas Department of Health Miller County Health Unit utilizes a Registered Nurse to provide case management for patients with an abnormal results obtained by a contracted provider in the area. Upon referral, the RN Case Man-ager contacts the patient within 72 hours to discuss their results, expected outcomes, and follow-up appointments. Assessment for Medicaid, patient education and identification of other referral needs are also provided. The RN Case Manager typically stays in contact with the patient until all treatment is completed, and contacts the patient annually to assess her needs. The RN Case Manager also helps patients enroll in the Arkansas Breast Care Program administered by ADH. The Miller County Health Unit provides clinical breast exams, mammography referrals, pelvic examinations and pap tests, digi-tal rectal exams and human papilloma virus testing, as indicated.
CHRISTUS ST. Michael Health System (CSMHS) W. Temple Webber Cancer Treatment Center employ-ees a Registered Nurse Patient Navigator to provide patient education and coordination of care once a patient is diagnosed. In addition, the Nurse Navigator works directly with the licensed clinical social worker at the center to assist the patient in accessing local resources. The Nurse Navigator at CSMHS has training in genetics counseling and can assist with determining the likelihood of cancer being di-agnosed among other family members. CSMHS is a grantee of the Susan G. Komen for the Cure Texar-kana Affiliate, a direct service provider for the Texas Breast and Cervical Program, and facilitates two support groups – the Power of Hope for all cancers survivors, and the Breast Cancer support group. CSMHS provides complete cancer screening, diagnostic and surgical services.
The University of Arkansas for Medical Sciences Area Health Education Center Southwest (UAMS AHEC Southwest) has a dedicated community education department that provides health information
to the community. One member of the community education team is a Community Health Worker (CHW) who works in a similar capacity as the defined patient navigator. The CHW takes information to the community about breast health services available in the area, and also helps set up appointments for patients needing clinical breast exams. UAMS AHEC Southwest is a grantee of the Susan G. Komen for the Cure Texarkana Affiliate and a contractual provider for Texas Breast and Cervical Program at CSMHS. UAMS AHEC Southwest provides clinical breast exams, cervical examinations, pap smears, pelvic exam, hemoccult screening, digital rectal exams/prostate specific antigen, oral cancer examina-tions, and skin cancer screenings. UAMS AHEC Southwest recently completed a pilot CHW training with plans to expand to a complete certificate program.
The Breast Health Center at Wadley Regional Medical Center (WRMC) staffs a patient coordinator who assists patients with abnormal mammogram and/or ultrasound results to the appropriate rec-ommended follow-up breast health services, to include; diagnostic mammography, ultrasound, and breast biopsy. The patient coordinator also connects patients with appropriate resources available in and outside of Texarkana. WRMC provides complete breast cancer screening, diagnostic and surgical services. Patients can access screening and diagnostic mammography services, breast ultrasound and biopsy services at Wadley utilizing Susan G. Komen for the Cure funding awarded through a grant to UAMS AHEC Southwest. In June of 2012, the Breast Health Center at Wadley began offering breast MRI services. Breast MRI is an extremely useful diagnostic tool and is recommended for women who have an increased risk of developing breast cancer. A National Cancer Institute (NCI) risk assessment tool is used at each screening mammogram performed at Wadley, giving the patient their lifetime risk of breast cancer based on the patient’s family medical history. A full service women’s health clinic is housed on the hospital’s third floor and serves women from all socio-economic environments. Clinic services are particularly available to low-income/Medicaid-eligible patients, including clinical breast exams, cervical and pelvic examinations, and cervical cancer screening with Pap smears.
Both hospitals offer various cancer-related screenings throughout the year at a reduced cost and par-ticipate in various health fairs to promote cancer-related services. Community-based screenings are provided at various times throughout the year by the Arkansas Prostate Foundation and the UAMS Mobile Mammography Unit. The ANGEL Fund Foundation offers medical financial assistance for quali-fied patients in the greater Texarkana area. Texarkana hosts two major cancer-related fundraising events – the Susan G. Komen Race for the Cure and the American Cancer Society Relay For Life.
Gaps
Despite the many available resources for cancer care, Texarkana faces certain barriers. There are no low-cost community-level colorectal cancer screening opportunities. While several health care organi-zations have a patient navigator, more lay and professional navigators are needed to assist patients and their families access cancer screenings, diagnostic and surgical services. Funding for cancer screening, diagnostic and treatment is limited to only a few of the major cancer sites. There is a lack of community awareness on certain cancer sites; therefore, more education is needed. Finally, there is limited local American Cancer Society presence. The American Cancer Society office recently closed and has limited staff capabilities. The Society has previously been a key provider of cancer education, navigation and basic cancer-care services in the community. This need creates a major barrier for the general public knowing and understanding cancer. Certain Society-sponsored programs (Look Good, Feel Better; Reach to Recovery) are offered on a limited basis in Texarkana.
PAG
E 35

PAG
E 3
6
American Cancer Society
Road to Recovery – (limited availability)
Transportation assistance gas cards – (limited
amount and availability)
Gift Items
Wigs/ head coverings
Breast prosthesis/bras
Reach to Recovery – (limited availability)
Look Good—Feel Better (active)
Cancer Support Groups (active)
I Can Cope with Breast Cancer @ CSMHC –
meets 2nd Tuesday @ 5:30 PM
I Can Cope (Power of Hope) @ CSMHC – meets
1st Tuesday @ 12:00 PM
Phone Data Base
Insurance assistance
Link to financial assistance
Navigation
Medication assistance
Angel Fund Foundation
Financial assistance for cancer treatment
(excludes hospital charges)
Arkansas Breast and Cervical Care
Screenings and diagnostics for women
meeting eligibility criteria
CHRISTUS St. Michael Health System
Breast and Cervical Care Outreach Program
Spirit of St Michael
Cancer Screenings
Wellness Programs
Medication Assistance
Wigs and prosthetics
Community Education
Texarkana Affiliate of the Susan G. Komen
for the Cure
(Grants awarded to local service providers)
Angel Fund Foundation
Atlanta Memorial Hospital Foundation
CHRISTUS St Michael Health Care
Hospice of Texarkana
Little River Memorial Hospital
UAMS AHEC Southwest
UAMS AHEC Southwest
Cancer Screening
Community Education
Patient Navigation
Patient-Centered Medical Home
Prescription Assistance Program
Wadley Regional Medical Center
Cancer Screenings
Community Education
Wadley Scan Mobile
ACS Community Resource Center
Transportation Texarkana Volunteer Center
*Contact Joy @903-798-3211
*1-2 rides per week with 2 days notice
*Donations requested.
Opportunities, Inc.
*Contact 903-791-2295
*Transportation for Aged and Disabled
TRAXX
*Contact 866-575-9014 for Bowie, Cass, Morris counties
*Contact 877-633-8747 for Medicaid transportation
SW Arkansas Development Counsel

*Contact 870-772-5759
*Medicaid transportation in Arkansas
Hospices Dierksen – TX/AR
*Contact 903-793-6350
*Charity care available
Hospice of Texarkana – TX/AR
*Contact 903-794-4264
*Charity care available
*Grief Support available
Serenity – TX/AR
*Contact 903-255-0430
*Charity care available
Legacy – TX
*Contact 430-200-2830
*Grief Support available
Heritage – TX
*Contact 903-792-0716
*Grief Support available
Community Assistance
Friendship Center
*Contact 903-792-1301
*Assistance with food, $4.00 limit on RX
Salvation Army
*Contact 870-774-2701
*Assistance with utilities, rent, RX, short term shelter
Randy Sams Homeless Shelter
*Contact 903-792-7024
*Temporary shelter for homeless
Samaritan Charities
*Contact 903-793-0011
*Assistance with RX
*Resale shop clothing and household furnishings
Medication Assistance Good Samaritan Charities (limited to availabil-
ity of funds)
Friendship Center (limited to availability of funds)
Local churches (limited to availability of funds)
Shelter, utilities and Food Assistance Housing Authority – reduced rent for qualify-
ing applicants
Salvation Army – temporary shelter
Randy Sam’s Homeless Shelter – temporary shelter
North Texas Food Bank
Friendship Center
Local church pantries
Department of Human Service food stamp program
Home modification
Ark-La-Tex Council of governments – depends on situation and available funds
Arkansas Agency on Aging – depends on avail-ability of volunteers
Private contractors
Transportation American Cancer Society Reach to Recovery
(limited to availability of volunteer drivers)
CSMHC van (local transportation to facility for treatment)
T Line (discounts available for disabled)
Texarkana Volunteer Center (limited to availa-bility of volunteer drivers)
Medicaid Transportation for qualifying Medi-caid recipients
Grief Support Groups
Dierksen Hospice
Hospice of Texarkana
Serenity Hospice
Free or reduced clinics Grace Clinic 903-949-5571
PAG
E 37

PAG
E 3
8
Local Churches Central Christian 903-792-1915 Discount RX cards; gas vouchers
Chapel of Light 903-628-8718 Manna Kitchen
Church of the Living God 870-772-2579 Limited help with medications
Church on the Rock 903-794-8589 Limited help as funds available
Disciples Christian 903-838-0249 Limited help as food/funds available
First Baptist/New Boston 903-628-3395 Food Pantry/limited help
First Baptist/Moores Ln 903-831-6000 Limited help with RX, utilities
First Baptist/Nash 903-838-5104 Food Pantry 3rd Saturday
First Presbyterian 870-774-6453 Clothing, small house hold items
Landmark Pentecostal 903-794-6201 Food Pantry
Miles Chapel Church 870-772-8802 BC Support Gr, limited help
Sacred Heart Catholic 903-794-4444 Limited help with RX, utilities
St Edwards Catholic 870-216-2194 Daily lunch, limited help
Texarkana 7th Day Adventist 903-908-1988 Food, clothing, gas vouchers
Walnut Hill Church of Christ 903-223-0388 Limited help as funds available
Other Services Bowie County Clinical Services
903-614-5551/LaSondra Bailey
*Income guideline ($407 month single)
*$30,000 annual limit
Cass County Indigent 903-756-8392/Carolyn Jolly
Red River Indigent 903-428-0908/Muriel Shider
Morris County Indigent 903-645-3691/Sherry Ray
AR Health Care Access
Hill Burton
Opportunities
AR and TX Medicaid transporta-tion
Medicaid phone service
Habitat for Humanity
Housing Authority TX and AR
Texas Ramps in Texarkana
Multiple Myeloma group
References and Resources American Cancer Society, Cancer Facts and Figures, 2012
All ACS graphs and information s included in this publication are from the American Cancer Society, Cancer Statistics 2011; A presentation from the American Cancer Society.
Arkansas Cancer Facts and Figures, 2011
Center for Disease Control (CDC): Behavioral Risk Factor Surveillance
System, 2010
Texas Cancer Plan 2012- Cancer Prevention & Research Institute of Texas.
UAMS AHEC-SW Cancer Registry data collected from:
CHRISTUS ST. Michael Health System
Wadley Regional Medical Center
Susan G. Komen Texarkana Affiliate 2011 Community Profile
American Institute for Cancer Research- Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global Perspective 2012 (www.dietandcancerreport.org)
The Clinical Guide to Oncology Nutrition (2nd ed.) by Laura Elliott, Laura L. Molseed, and Paula Davis McCallum. American Dietetic Asso-ciation, 2006

Survivorship Promote overall health and well-being of people affected by cancer 1. Collaborate with other health care entities on an ongoing basis to develop and expand resources for cancer survivors. 2. Education for health care providers on the needs of survivors and the importance of a survivorship program. 3. Increase community awareness of survivorship through education and media exposure. Cancer Research Increase opportunities to access and participate in cancer research 1. Establish resources needed to provide access to clinical trials at the local level. 2. Provide educational resources in physician offices to increase public awareness of clinical trials. 3. Establish funding resources to assist patients and families with travel expenses for clinical trials when outside of our market area. 4. Investigate funding opportunities to assist medical groups in covering the cost of providing clinical trials in their offices. 5. Improve access to clinical trials for all patients regardless of demographic fingerprint. 6. Developing technologies to assist in patient identification. Clinical trials are research studies that involve people. They are the final step in a long process that begins with research in a lab and animal testing. Many treatments used today are the result of past clinical trials. In cancer, clinical trials are designed to answer questions about new ways to: Treat cancer Find and diagnose cancer Prevent cancer Manage symptoms of cancer or side effects from its treatment Clinical Trials Clinical trial participation involve people volunteer to take part in tests of new drugs or procedures. In Texas, only 3 to 5 percent of patients participate in clinical trials. This number is so low because patients are not often asked to participate because doctors either don’t know what trials are available or don’t have the systems in place to support patients participating on the trials. In Texarkana, as part of our accreditation process with the American College of Surgeons Commission on Cancer, we are required to report the number of patients who enroll in clinical trials. Up until 2012, the percentage of cases placed on clinical trials has been 2% to meet the Standard with 4% achieving Commendation. In 2012, the percentages increased to 4% to met the Standard and 6% needed for Commendation.
PAG
E 39

![Original Article Effects of high-intensity focused ... · lung cancer [1]. Breast cancer is treated in sev - eral ways. High-intensity focused ultrasound (HIFU) is a highly precise](https://img.pdfslide.net/doc/110x75/6002dc458183c45b33516b11/original-article-effects-of-high-intensity-focused-lung-cancer-1-breast-cancer.jpg)




























