Embed Size (px)
Citation preview

2012 Meaningful Use and Health Care Innovations Conference
Keeping the main thing the main thingDavid Ehrenberger MD
Chief Medical Officer, Integrated Physician Network
Cincinnati, Ohio 16 March 2012

The future:Exceptional Care
PCMH, Meaningful Use, population health management, data warehouses, performance
improvement, business intelligence…What is the connection?
What is it?

What if…?
What if the moment you walked into your primary care team’s office, everyone really knew you and was ready to meet your needs?
What if your health was as important to your care team between visits as it was when you were in the office?
What if, at every visit for healthcare, your provider was relaxed, seemed to have plenty of time to listen, understand and to connect?
What if, after an office visit, you consistently felt better informed and more capable —even energized—to promote your own health?
What if your elderly grandparent, living alone yet frail, could count on her care team to make home visits?
Patients’ view
What if…?What if a busy PCP schedule was 12 patients/ day?
What if each PCP was supported by a team of 2 MAs?...and that the MAs did as much clinical care as the provider?
What if pre-visit planning (huddling) was the key to a relaxed day and superior population-based care…and technology was a gateway not a barrier to effective and efficient huddling?
What if, aside from indicated physical exams and Pap smears, PCPs never did prevention, screening or routine chronic care management?...but could prove that the care their panel of patients received was in the 90th percentile nationally?
What if your typical patient encounter was focused mainly your relationship and on tackling interesting diagnostic challenges?
What if you loved coming to work…every day, no matter who was on your schedule?
Providers’ view
The Patient Centered Medical Home is the Mojo
of Exceptional Care!
National demonstration projects, multi-payer, multi-stakeholder pilots, integrated delivery
systems…all prove it
1. Better outcomes for chronic care
2. Better performance on prevention and screening
3. Better patient experience and access
4. Decreased cost, avoidable hospitalizations and ED use
5. Better staff and provider satisfaction
6. …thru the reinvention of primary care

The Connection (between PCMH, Meaningful Use and
Exceptional Care)
…TWO simple Rules…

Rule # 1:
Patients are persons first.

An uncalled for house call…Worried about Jim, pt of 10 yrs…diabetes,
some depression, non-compliant with Rx, f/u office visits. Mom died…
Made the time, end of a busy day…Rang the doorbell.
Jim was poor, one room apartment, disheveled
“May I check your medicine cabinet?” “Here it is doc”…plastic bag.
“Good to see you’re taking your fluoxetine.” “Yeah doc, but I can’t afford that therapist you sent me to. Don’t have a car anymore.”
Bottles of vodka, empty, full and half empty.
“Have any family around?” “Sure, in Iowa, my sister, she hates me.”
No time in business model
Economic barriers
Powerless, disengaged
No access: behavioral health
Nutritional impact, closet alcohol abuse
Poor social network, support
Translation

Rule # 2:
We are in the business of Health Care.
…not just sick care…

LA Police Department

“You call, we brawl.”
“In God we trust, all others are suspects.”
“To arrest and incarcerate.”
“We’ll kick your butt and take your donuts too!”
LAPD Motto contest in 1955

“To serve and protect”
Officer Joseph S Dorobeck won:
“As a team, my family, my community, my country”
LAPD Motto contest in 1955

Innovating the Patient Centered Medical Home…
Becoming a Health Home centered on Persons and our Community
The new normal
• Health Care vs. sick care– Care of both the patient (ill) and the person (psychosocial, family
and community context, wellness)– Contiguous accountability for health care: at time of encounter
and the other 99.99%...
• Top of license and “meta” teamwork• Skilled commitment to activation and engagement• Beyond the pejorative…patient as teammate in their care
and their care team• Examples: Group Visits, Performance Improvement
Team, Self Management, Population Health Management
Health Home centered on Persons and our Community

Weight and Hgb A1c
200
220
240
260
280
300
320
Wei
ght
456789101112
Hbg
A1c Weight
Hgb A1c
Ruben’s MessageThe voice for “Exceptional Care”

Primary Care:“Life as I knew it…”
R. Hernandez: presents for 30 min routine Complete Physical Exam:• 60 yrs old, engineer, single father of 3• Diabetes, A1c 10%• Obesity• Bladder cancer• Coronary artery disease• Hypertension and dyslipidemia• “By the way, I have a total knee replacement scheduled
in 2 weeks.”

Teamwork and Practice Transformation
Broomfield Family Practice Performance Improvement Team
Meaningful WorkSkills of CQI
A new culturePatient presence
Top of license

Diabetes Poor Control
0%
10%
20%
30%
40%
Mar-10 Apr-10 May-10
Jun-10 Jul-10 Aug-10
Sep-10
% P
atie
nts
w/
DM Hgb A1c >9% or None
% 423 Patients w/ DM
System Culture: barrier to better diabetes care?
Group Visits: Diabetes

Exceptional care…What the heck?
• New tool to focus on outliers, high risk, chronic care, vexations…
• Content Thread (vs content box)
• Group Self-Management (vs orders)
• Team-based care led by MAs
• Facilitation (vs didactic)

Culture Shift…
• Group vs dyad Model of Care• Group Visits & meaningful work• “Wiki-learning” and expert
knowledge• Patient empowerment• Team-based/non-MD care• Value Based Health Care
– population-based – cheap and effective
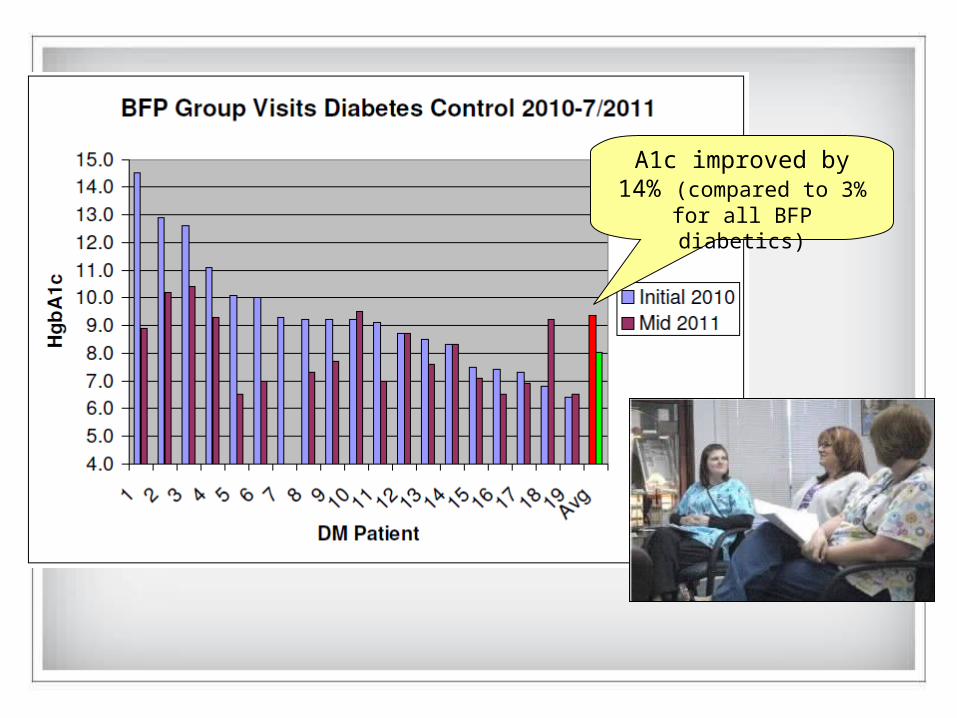
A1c improved by 14% (compared to 3% for all
BFP diabetics)

December 5, 2009:Diabetes for 10 years, Max weight 301#
December 2010:Weight loss now at 69#...HgbA1c down from 10.0 to 7.0
What Worke
d ?
Ruben’s Story…
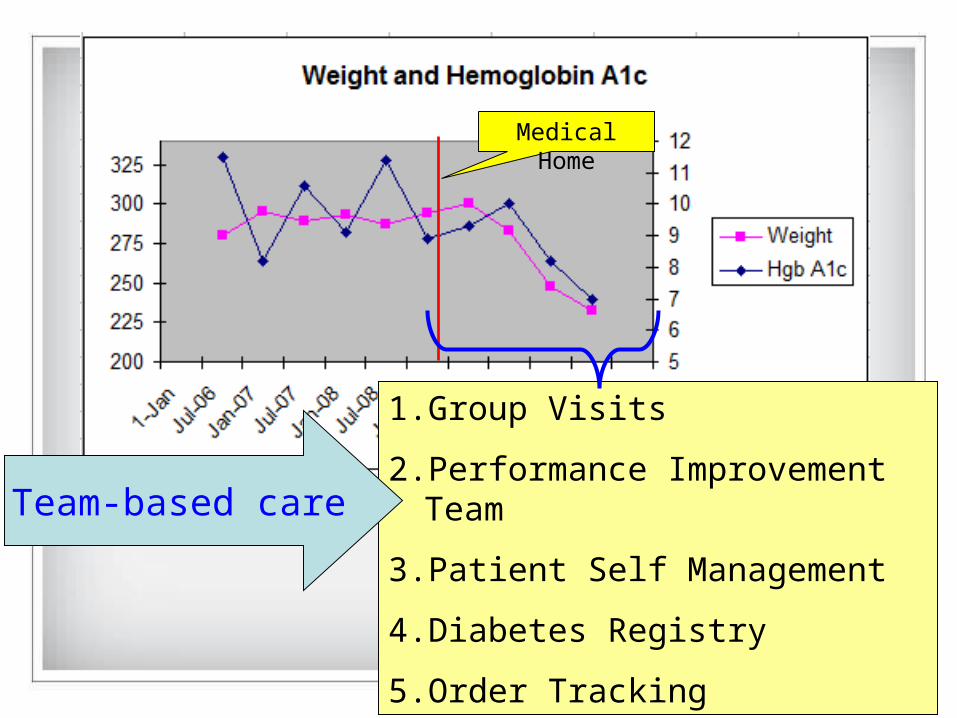
Medical Home
1. Group Visits
2. Performance Improvement Team
3. Patient Self Management
4. Diabetes Registry
5. Order Tracking
Team-based care

TARGET <=20%
Diabetes Poor Control
0%
10%
20%
30%
40%
Mar-10
Apr-10
May-10
Jun-10
Jul-10
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
A1c>9or notdone
423 pts w/DM
Introduction of the Group
Visit…
Culture change: new tools, better A1c’s

“Somebody has got to do something and
it is just incredibly pathetic that it has to
be us.”
Jerry Garcia