-
8/20/2019 2013 IDF.pdf
1/160
IDF DIABETES ATLASSixth edition
-
8/20/2019 2013 IDF.pdf
2/160
02 I IDF Diabetes Atlas I Sixth edition
© I st o c k ph ot o. c om
-
8/20/2019 2013 IDF.pdf
3/160
IDF Diabetes Atlas I Sixth edition I 03
→
T A B L E O F C O N T E N T S
Chapter 1
Chapter 2
Chapter 3
Chapter 4
Chapter 5
Chapter 6
Table of contents
Acknowledgements 05Foreword 07Introduction 09Executive summary
11
What is diabetes? 19Type 1 diabetes 22Type 2 diabetes
23Gestational diabetes 23Impaired glucose tolerance and impaired
fasting glucose 24Diabetes complications 24Other complications
26
The global burden 29Diabetes and impaired glucose tolerance
32
2.1 Diabetes 342.2 Undiagnosed diabetes 382.3 Impaired glucose
tolerance 402.4 Diabetes in young people 422.5 Hyperglycaemia in
pregnancy 442.6 Mortality 462.7 Health expenditure 48
Regional overviews 51A global perspective 543.1 Africa 563.2
Europe 583.3 Middle East and North Africa 603.4 North America and
Caribbean 62
3.5 South and Central America 643.6 South-East Asia 663.7
Western Pacific 68
Global issues in diabetes 714.1 A global review of diabetic
retinopathy 764.2 Rates of diabetic ketoacidosis at diagnosis in
children with type 1 diabetes 784.3 Diabetes in Indigenous peoples
804.4 Diabetes in rural communities 82
Linking local to global 855.1 Driving the global agenda on
diabetes 885.2 Including diabetes in development 905.3 The IDF
Diabetes Scorecard 925.4 Training health professionals in diabetes
94
Resources and Solutions 996.1 Diabetes in older people 1026.2
IDF programmes and campaigns 1046.3 Clinical guidelines and
Position Statements 1066.4 About the International Diabetes
Federation 110
Appendices and references 113Country summary table: estimates
for 2013 114Country details table: estimates for 2013
128Abbreviations and acronyms 142Glossary 143References 146List of
tables, maps and figures 153
-
8/20/2019 2013 IDF.pdf
4/160
04 I IDF Diabetes Atlas I Sixth edition
© International Diabetes Federation, 2013No part of this
publication may be reproduced, translated, or transmitted in any
form or by any meanswithout the prior written permission of the
International Diabetes Federation.
First published, 2000Second edition, 2003Third edition,
2006Fourth edition, 2009Fifth edition, 2011Sixth edition, 2013
Online version of IDF Diabetes Atlas :
www.idf.org/diabetesatlas
ISBN: 2-930229-85-3
Design and layout: De Visu Digital Document DesignCover photos:
© istockphoto.com – © Tim Nolan
-
8/20/2019 2013 IDF.pdf
5/160
IDF Diabetes Atlas I Sixth edition I 05
→
A C K N O W L E D G E M E N T S
Acknowledgements
Corporate sponsorsIDF would like to express its thanks to the
followingsponsors for their generous support of the
sixthedition:
Diabetes Atlas,sixth edition committeeNam Han Cho (chair), David
Whiting (deputy chair),Leonor Guariguata, Pablo Aschner Montoya,
NitaForouhi, Ian Hambleton, Rui Li, Azeem Majeed,Jean Claude
Mbanya, Ayesha Motala, K.M. VenkatNarayan, Ambady Ramachandran,
WolfgangRathmann, Gojka Roglic, Jonathan Shaw, MartinSilink, D.R.R.
Williams, Ping Zhang.
Editorial teamLeonor Guariguata, Tim Nolan, Jessica Beagley,Ute
Linnenkamp, Olivier Jacqmain.
ContributorsThe International Diabetes Federation (IDF)
wouldlike to thank the following core contributors:
Florencia Aguirre, Alex Brown, Nam Han Cho,Gisela Dahlquist, the
Diabetes EducationConsultative Section (DECS), Sheree Dodd,
TrishaDunning, Sir Michael Hirst, Christopher Hwang,
Dianna Magliano, Chris Patterson, Courtney Scott,Jonathan Shaw,
Gyula Soltész, Juliet Usher-Smith,David Whiting.
Other ContributorsCarlos Aguilar Salinas, Riyadh
Alshamsan,Tabassum Ambia, Carmen Gloria Aylwin, CarolineBaan,
Juliana Chan, Adel A. El-Sayed, LaercioFranco, Juan José
Gagliardino, Jody Grundman,Lucy Hadley, Christian Herder, Hak C.
Jang, PiliKamenju, Andre Pascal Kengne, Tawfik Khoja,Mandana
Kooijmans, Silvia Lapertosa, Kerry
Lydon, Ronald Ching Wan Ma, Lydia Makaroff, ChrisMillett, Graham
Ogle, Martijn Parker, NasheetaPeer, Lorenzo Piemonte, Salman Rawaf,
JoachimRosenbauer, Segundo Seclén, ChamukuttanSnehalatha, Anne
Mieke Spijkerman, TeresaTamayo, Sean Taylor, Sara Webber, Sarah H.
Wild,Mary Vinocour, Bernard Zinman.
Lilly Diabetes
Merck and Co, Inc.
Novo Nordisk A/S – Supportedthrough an unrestricted grant by the
NovoNordisk Changing Diabetes® initiative
Pfizer, Inc.
Sanofi Diabetes
-
8/20/2019 2013 IDF.pdf
6/160
06 I IDF Diabetes Atlas I Sixth edition
-
8/20/2019 2013 IDF.pdf
7/160
IDF Diabetes Atlas I Sixth edition I 07
→
F O R E W O R D
Despite the grim picture painted by the newfigures, we already
have the knowledge andexpertise to begin creating a brighter future
forgenerations to come. We must increase awarenessof the importance
of a healthful diet and physicalactivity, especially for children
and adolescents.Crucially though, environments have to be
createdthat lay the foundations for healthy living. Thesemeasures
are most pressing in low- and middle-income countries, precisely
those which are leastprepared to confront this huge-scale
pandemic,and whose very development will be thwarted in
itsaftermath. It is essential that health professionals
– particularly the primary care practitioners –receive adequate
and appropriate training to beable to perform effectively on the
front line againstdiabetes.
In the last two years, progress has been madetoward driving
political change for diabetes.Building on the momentum of the 2011
UN PoliticalDeclaration on non-communicable diseases(NCDs), the
66th World Health Assembly in May 2013saw the unanimous
adoption by Member States ofa voluntary Global Action Plan for the
preventionand control of NCDs. Diabetes is now prominent
on the global health agenda, with specific targetsfor access to
essential medicines and for haltingthe growth of obesity and
diabetes. Still, we mustnot miss this opportunity. Governments and
policy-makers, health professionals and those affected bythe
disease must remain engaged in the fight sothat IDF may achieve its
vision of living in a worldwithout diabetes.
Sir Michael HirstPresident,
International Diabetes Federation
It is a bittersweet pleasure to be presiding over
theInternational Diabetes Federation upon the launchof this sixth
edition of the IDF Diabetes Atlas . Theevidence published
herein on the millions of peopleswept up by the diabetes pandemic
vindicates theFederation’s relentless efforts to promote
solutionsto this worldwide health crisis. Previous editionsof the
Atlas were a crucial tool in the successfulcampaign for a UN
Resolution on diabetes andour figures informed the subsequent
politicaldeclaration on non-communicable diseases. Wehave achieved
much: diabetes is now firmly onthe highest of decision-making
agendas. But the
figures in this edition are a harsh reminder of howfar we still
have to go.
Today, there are 382 million people living withdiabetes. A
further 316 million with impairedglucose tolerance are at high risk
from thedisease – an alarming number that is set to reach471
million by 2035. Diabetes is on the rise all overthe world and
countries are struggling to keeppace. The misconception that
diabetes is ‘a diseaseof the wealthy’ is still held by some – to
the detri-ment of desperately needed funding to combat thepandemic.
But the evidence published in the IDF
Diabetes Atlas disproves that delusion: a stag-gering 80%
of people with diabetes live in low- andmiddle-income countries,
and the socially disad-vantaged in any country are the most
vulnerable tothe disease. Today’s emerging diabetes hotspotsinclude
countries in the Middle East, WesternPacific, sub-Saharan Africa
and South-East Asiawhere economic development has
transformedlifestyles. These rapid transitions are
bringingpreviously unheard of rates of obesity and
diabetes;developing countries are facing a firestorm of illhealth
with inadequate resources to protect their
population.By the end of 2013, diabetes will have caused5.1
million deaths and cost USD 548 billion inhealthcare spending.
Without concerted actionto prevent diabetes, in less than 25 years’
timethere will be 592 million people living with thedisease. Most
of those cases would be preventable.However, without a
multi-sectoral, all-of-societyapproach, the disturbing projections
in this editionof the IDF Diabetes Atlas will be
realised.
Foreword
-
8/20/2019 2013 IDF.pdf
8/160
08 I IDF Diabetes Atlas I Sixth edition
© I st o c k ph ot o. c om
-
8/20/2019 2013 IDF.pdf
9/160
IDF Diabetes Atlas I Sixth edition I 09
→
E X E C U T I V E
S U M M A R Y
For the first time, the IDF Diabetes Atlas hasproduced
estimates of high blood glucose in preg-nancy. This serious and
underreported conditionis affecting many women and infants – an
esti-mated 21.4 million live births in 2013. Not onlydoes diabetes
pose a grave threat to the health ofa mother and her child but
evidence shows highblood glucose levels during pregnancy can leadto
an increased risk of type 2 diabetes later in lifefor the child,
further contributing to the alreadydevastating epidemic.
More high-quality studies than ever before havecontributed to
the estimates in this edition of theIDF Diabetes Atlas .
Nevertheless, more studiesare needed to describe the burden of
diabetes inorder to improve the precision of the estimates,and
contribute to an evidence base that is funda-mental in driving
powerful advocacy for peoplewith diabetes.
Professor Nam Han ChoChair,
IDF Diabetes Atlas Committee, 6th Edition
This 6th edition of the IDF Diabetes Atlas onceagain
sets the standard for evidence on the globalepidemiology of
diabetes. The new estimates buildon the groundwork laid by previous
editions, andconfirm the precipitous rise in diabetes overthe last
few years. An astounding 382 millionpeople are estimated to have
diabetes, withdramatic increases seen in countries all over
theworld. The overwhelming burden of the diseasecontinues to be
shouldered by low- and middle-income countries, where four out of
five peoplewith diabetes are living. Socially and
economicallydisadvantaged people in every country carry the
greatest burden of diabetes and are often the mostaffected
financially.
The new estimates show an increasing trendtowards younger and
younger people developingdiabetes, a trend that is very worrisome
for futuregenerations. If current demographic patternscontinue,
more than 592 million people will beaffected with diabetes within a
generation. Thisfigure takes into account changes only in the
popu-lation and patterns of urbanisation, and is almostcertainly an
underestimate. Estimates of type 1diabetes in young people also
show unexplained
and rapid increases in several regions along withthe rise in
type 2 diabetes in younger populations.
The burden of diabetes is reflected not only in theincreasing
numbers of people with diabetes, butalso in the growing number of
premature deathsdue to diabetes. In 2013, roughly half of all
deathsdue to diabetes in adults were in people underthe age of 60,
and in less-developed regions likesub-Saharan Africa, that
proportion climbs to 75%.As life expectancy increases, while the
infectiousdisease burden decreases, and development drivesrapid
changes in lifestyles, it is the developing
regions that will see the greatest increases in theburden of
diabetes.
Introduction
-
8/20/2019 2013 IDF.pdf
10/160
10 I IDF Diabetes Atlas I Sixth edition
© I st o c k ph ot o. c om
-
8/20/2019 2013 IDF.pdf
11/160
IDF Diabetes Atlas I Sixth edition I 11
→
E X E C U T I V E
S U M M A R Y
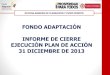
IDF’s most recent estimates indicate that 8.3% ofadults – 382
million people – have diabetes, andthe number of people with the
disease is set to risebeyond 592 million in less than 25 years.
Yet, with175 million of cases currently undiagnosed, a vastamount
of people with diabetes are progressingtowards complications
unawares. Moreover, with80% of the total number affected living in
low- andmiddle-income countries, where the epidemic isgathering
pace at alarming rates, the IDF DiabetesAtlas ’ latest figures
provide a worrying indicationof the future impact of diabetes as a
major threatto global development.
Diabetes in all its forms imposes unacceptably highhuman, social
and economic costs on countriesat all income levels. Since the
publication of thefirst International Diabetes Federation
DiabetesAtlas in 2000 successive editions have
providedconsistent evidence of the continuing growth inrates of
diabetes incidence and prevalence world-wide. This 6th edition
brings new evidence of thesame kind, and carries a bitter but
unavoidablemessage: despite the array of tools at our disposalto
tackle the disease – effective drug therapies,advanced technology,
ever-improving educationand preventive strategies – the battle to
protect
people from diabetes and its disabling, life-threat-ening
complications is being lost.
Executive summary
56 M37 M
138 M24 M
72 M35 M
20 M
Number of people with diabetes by IDF Region, 2013
MIDDLE EAST ANDNORTH AFRICA MENA
SOUTH AND CENTRALAMERICA SACA
WESTERN PACIFIC WP
NORTH AMERICA ANDCARIBBEAN NAC
EUROPE EUR
AFRICA AFR
SOUTHEASTASIA SEA
WORLD
382 Mpeople living
with
diabetes
46%undiagnosed
-
8/20/2019 2013 IDF.pdf
12/160
12 I IDF Diabetes Atlas I Sixth edition
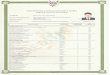
WORLD
382 M
Type 1 diabetes
Normal situation
gestational diabetes
Type 2 diabetes
of the long-term damage being caused by theirdisease.
Gestational diabetes, which appearsduring pregnancy, can lead to
serious health risksto the mother and her infant and increase the
riskfor developing type 2 diabetes later in life.
All types of diabetes require close collabora-tion between those
affected and their healthcare
providers in order to prevent a range of costly,dangerous
complications, which can provokedamage to the eyes, kidneys, feet
and heart, and,left untreated, result in early death.
What is diabetes? The three main types of diabetes – type 1
diabetes,type 2 diabetes and gestational diabetes –occurwhen the
body cannot produce enough of thehormone insulin or cannot use
insulin effectively.Insulin acts as a key that lets the body’s
cells takein glucose and use it as energy.
People with type 1 diabetes, the result of an auto-
immune process with very sudden onset, needinsulin therapy to
survive. Type 2 diabetes, on theother hand, can go unnoticed and
undiagnosed foryears. In such cases, those affected are unaware
Diabetes is a huge
and growing problem,
and the costs to society
are high and escalating.
AFR ↗109.1%
WP ↗46%
SACA ↗59.8%
SEA ↗70.6%
MENA ↗96.2%
EUR ↗22.4%
2013 2035
NAC ↗37.3%
WORLD
592 Mpeople living
with diabetes
in 2035
increase:
↗55%
i n c r e a s e
CELLS
G L U C
O S E
CELLS
CELLS
BLOOD
BLOOD
G L U C
O S E
G L U C
O S E
PANCREAS
PANCREAS
PANCREAS
I N S U
L I N
I N S U
L I N
INSULIN
CELLS
CELLS
CELLS
-
8/20/2019 2013 IDF.pdf
13/160
IDF Diabetes Atlas I Sixth edition I 13
→
E X E C U T I V E
S U M M A R Y
Top 10 countries / territories of number
of people with diabetes (20-79 years), 2013
China
India
USA
Brazil
RussianFederation
Mexico
Indonesia
Germany
Egypt
Japan
Millions
0 10 20 30 40 50 60 10070 80 90
98.4
65.1
24.4
11.9
10.9
8.7
8.5
7.6
7.5
7.2
The Global Burden The majority of the 382 million people
with diabetesare aged between 40 and 59, and 80% of them live
in low- and middle-income countries. All types ofdiabetes are on
the increase, type 2 diabetes inparticular: the number of people
with diabetes willincrease by 55% by 2035.
An additional 21 million cases of high blood glucosein pregnancy
are estimated to contribute to theglobal burden of diabetes. That
is equivalent to17% of live births to women in 2013 that had
someform of high blood glucose in pregnancy.
In human as well as financial terms, the burdenof diabetes is
enormous, provoking 5.1 million
deaths and taking up some USD 548 billion dollarsin health
spending (11% of the total spent world-wide) in 2013.
Top 10 countries/territories for prevalence* (%) of diabetes
(20-79 years), 2013
MIDDLE EAST ANDNORTH AFRICA
WESTERNPACIFIC
23%
23%
23%
24%
24%26%
29%
35%35%
37%
* comparative prevalence
VANUATU
COOK ISLANDS
MARSHALLISLANDS
FEDERATED STATESOF MICRONESIA
NAURU
SAUDI ARABIA QATAR
KUWAIT
KIRIBATI
TOKELAU
More than 21 million
live births were affected
by diabetes during
pregnancy in 2013.
-
8/20/2019 2013 IDF.pdf
14/160
14 I IDF Diabetes Atlas I Sixth edition
Diabetes caused
5.1 million deaths
in 2013. Every six
seconds a person dies
from diabetes.
Regional overviews Different regions are being affected to
widelydiffering degrees. With more than 138 millionpeople affected,
the Western Pacific has morepeople with diabetes than any other
region. At theother end of the regional diabetes ranking,
Africa’sdiabetes population is currently the smallestamong the
regions. However, this is set to double
by 2035, and, ominously for Africa’s capacity todevelop, more
than three-quarters of deaths fromdiabetes in 2013 occurred in
people under 60 – thatis to say, in their prime productive
years.
The outlook is similarly worrying in South andCentral America,
where the diabetes populationis projected to increase by 60% by
2035. Rapiddevelopment has driven a fast-growing epidemic
ofdiabetes in South-East Asia, accounting for close to
one-fifth of all cases worldwide. Similarly, wealthand
development in the Middle East and NorthAfrica has led to high
proportions of diabetes whereone in ten adults in the region have
the disease.
A look at health spending on diabetes by regionreveals huge
disparities in responses to the
epidemic. Two regions spent more on diabetesthan the rest of the
regions put together: NorthAmerica and Caribbean, with an estimated
USD 263billion – equal to nearly half the world’s healthexpenditure
on diabetes; and Europe with USD 147billion. Despite their growing
diabetes populations,spending in South-East Asia and Africa
accountedfor less than 1% of all global health expenditureon the
disease.
56 M37 M
138 M24 M
72 M35 M
20 M54%
62%
36%
48%
27%
24%
49%
c a s e s
u n d i a g n o s e d
Number of people with diabetes (20-79 years), 2013 Proportion of
cases of d iabetes (20-79 years)that are undiagnosed, 2013
Global health expenditure due to diabetes
(20-79 years)
$$$
2013
2035
548billionUSD
627billionUSD
-
8/20/2019 2013 IDF.pdf
15/160
IDF Diabetes Atlas I Sixth edition I 15
→
E X E C U T I V E
S U M M A R Y
IDF
REGION
2013
MILLIONS
2035
MILLIONS
INCREASE
%
Africa 19.8 41.4 109%
Middle East and North Africa 34.6 67.9 96%
South-East Asia 72.1 123 71%
South and Central America 24.1 38.5 60%
Western Pacific 138.2 201.8 46%
North America and Caribbean 36.7 50.4 37%
Europe 56.3 68.9 22%
World 381.8 591.9 55%
147 B
14 B
263 B
26 B
88 B76%
28%
50%
38%
44%
55%
44%
m o r t a l i t y < 6 0
e x p e n d i t u r e s
IDF Regions and global projections of the number of people with
diabetes (20-79 years),
2013 and 2035
MIDDLE EAST AND
NORTH AFRICA MENA
SOUTH AND CENTRAL
AMERICA SACA
WESTERN PACIFIC WP
NORTH AMERICA AND
CARIBBEAN NAC
EUROPE EUR
AFRICA AFR
SOUTHEAST
ASIA SEA
Health expenditure (USD) due to diabetes (20-79 years),
2013Proportion of deaths due to diabetes in peopleunder 60 years of
age, 2013
4 B
6 B
-
8/20/2019 2013 IDF.pdf
16/160
16 I IDF Diabetes Atlas I Sixth edition
Global issuesin diabetesDespite the predominantly urban impact
of theepidemic, type 2 diabetes is fast becoming a majorhealth
concern in rural communities in low- andmiddle-income
countries.
No countries are escaping the diabetes epidemic,and in states
and territories worldwide it is thepoor and disadvantaged who are
suffering most.Indigenous communities are among those espe-cially
vulnerable to diabetes.
All nations – rich andpoor – are suffering
the impact of the
diabetes epidemic.
Indigenous peoples are
especially vulnerable
to diabetes.
of people with diabeteslive in low- and middle-
income countries
80%
age (years)
p r e v a l e n c e
Prevalence (%) of diabetes (20-79 years) by income group and
age
20
10
0
%
LOWERMIDDLEINCOME
UPPERMIDDLEINCOME LOWINCOMEHIGHINCOME
-
8/20/2019 2013 IDF.pdf
17/160
IDF Diabetes Atlas I Sixth edition I 17
→
E X E C U T I V E
S U M M A R Y
Resourcesand solutionsThe International Diabetes Federation
(IDF) isan umbrella organisation of over 200 nationaldiabetes
associations in more than 160 countries.It represents the interests
of the growing numberof people with diabetes and those at risk.
TheFederation has been leading the global diabetescommunity since
1950. IDF’s mission is to promotediabetes care, prevention and a
cure worldwide.
IDF is committed to promoting best practice in
diabetes through guidelines, position statements,and tools for
health professionals to improve thelives of people with
diabetes.
Linking local to global IDF plays a pivotal role in efforts
to reduce expo-nentially the global impact of diabetes,
catalysinggrass roots activism, influencing global health
anddevelopment policy, and driving the global agendaon diabetes. In
calling for a specific health target
14/11WORLD
DIABETESDAY
26/12WORLD
DIABETESCONGRESS
2013 2014
November NovemberSeptember
14/11
WORLDDIABETES
DAY
09/2015MILLENNIUM
DEVELOPMENTGOALS
SUMMIT
09/2014UN HIGH
LEVEL REVIEWOF THE POLITICAL
DECLARATIONON NCDs
2015
SeptemberDecember October
There are solutions
for managing and curbing
the diabetes epidemic.
Diabetes is more than a
health issue and requires
concerted policy action
across many sectors.
IDF isthe legitimate
voice of people with
diabetes
in the post-2015 development framework, theFederation is heading
a campaign for an all-of-society approach to diabetes prevention,
care andsupport.
As a leading supporter of people and organisa-tions working in
diabetes education and care,IDF produces educational resources
designedto improve the expertise of diabetes educatorsand other
healthcare professionals. IDF publica-tions are used widely around
the world, and theFederation’s programmes, campaigns and
eventsprovide a global awareness-raising platform forpeople with
diabetes and those at risk.
-
8/20/2019 2013 IDF.pdf
18/160
18 I IDF Diabetes Atlas I Sixth edition
© I st o c k ph ot o. c om
© I st o c k ph ot o. c om
-
8/20/2019 2013 IDF.pdf
19/160
IDF Diabetes Atlas I Sixth edition I 19
1What isdiabetes?
c h a p t e r 1
W H A T I S D I A B E T E S ?
-
8/20/2019 2013 IDF.pdf
20/160
20 I IDF Diabetes Atlas I Sixth edition
People with type 2diabetes can remain
UNDIAGNOSED for many years, unaware of
the LONGTERM DAMAGE
being caused by the disease
main types
of diabetes:
type 1 diabetes
type 2 diabetes
gestational
diabetes3
P e o p l e w i t h t y p e 1 d i a b e t e s w i l l d i e w i t h o u t i n s u l i n
There are
382 M peopleliving with
diabetes
46%undiagnosed
-
8/20/2019 2013 IDF.pdf
21/160
IDF Diabetes Atlas I Sixth edition I 21
c h a p t e r 1
W H A T I S D I A B E T E S ?
Effective managementof diabetes requiresa partnership
between
the person with diabetesand health professionals
People with diabetes
have an increased risk of
developing a number of
serious health problems
Poorly manageddiabetes leadsto serious
COMPLICATIONS and early death
-
8/20/2019 2013 IDF.pdf
22/160
22 I IDF Diabetes Atlas I Sixth edition
What is
diabetes?Diabetes is a chronic disease that occurs when thebody
cannot produce enough insulin or cannot useinsulin
effectively.1 Insulin is a hormone producedin the pancreas
that allows glucose from food toenter the body’s cells where it is
converted intoenergy needed by muscles and tissues to function.A
person with diabetes does not absorb glucose
properly, and glucose remains circulating in theblood (a
condition known as hyperglycaemia)damaging body tissues over time.
This damagecan lead to disabling and life-threatening
healthcomplications.
There are three main types of diabetes:
• type 1 diabetes
• type 2 diabetes
• gestational diabetes
Type 1 diabetesType 1 diabetes is caused by an autoimmune
reac-tion, where the body’s defence system attacks
theinsulin-producing beta cells in the pancreas. As aresult, the
body can no longer produce the insulin itneeds. Why this occurs is
not fully understood. Thedisease can affect people of any age, but
usuallyoccurs in children or young adults. People with this
form of diabetes need insulin every day in order tocontrol the
levels of glucose in their blood. Withoutinsulin, a person with
type 1 diabetes will die.
Type 1 diabetes often develops suddenly and canproduce symptoms
such as:
• abnormal thirst and a dry mouth
• frequent urination
• lack of energy, extreme tiredness
• constant hunger
• sudden weight loss
• slow-healing wounds
• recurrent infections
• blurred vision
People with type 1 diabetes can lead a normal,
healthy life through a combination of daily insulintherapy,
close monitoring, a healthy diet, andregular physical exercise.
The number of people who develop type 1 diabetesis increasing.
The reasons for this are still unclearbut may be due to changes in
environmental riskfactors, early events in the womb, diet early in
life,or viral infections.
-
8/20/2019 2013 IDF.pdf
23/160
IDF Diabetes Atlas I Sixth edition I 23
c h a p t e r 1
W H A T I S D I A B E T E S ?
Type 2 diabetesType 2 diabetes is the most common type
ofdiabetes. It usually occurs in adults, but is increas-ingly seen
in children and adolescents. In type 2diabetes, the body is able to
produce insulin but
either this is not sufficient or the body is unable torespond to
its effects (also known as insulin resist-ance), leading to a
build-up of glucose in the blood.
Many people with type 2 diabetes remain unawareof their illness
for a long time because symptomsmay take years to appear or be
recognised, duringwhich time the body is being damaged by
excessblood glucose. They are often diagnosed only
whencomplications of diabetes have already developed(see below,
Diabetes complications).
Although the reasons for developing type 2 diabetesare still not
known, there are several importantrisk factors. These include:
• obesity
• poor diet
• physical inactivity
• advancing age
• family history of diabetes
• ethnicity
• high blood glucose during pregnancy
affecting the unborn child
In contrast to people with type 1 diabetes, themajority of those
with type 2 diabetes usually donot require daily doses of insulin
to survive. Manypeople are able to manage their condition througha
healthy diet and increased physical activity ororal medication.
However, if they are unable toregulate their blood glucose levels,
they may beprescribed insulin.
The number of people with type 2 diabetes isgrowing rapidly
worldwide. This rise is associated
with economic development, ageing populations,increasing
urbanisation, dietary changes, reducedphysical activity, and
changes in other lifestylepatterns.2
Gestational diabetesWomen who develop a resistance to insulin
andsubsequent high blood glucose during preg-nancy are said to have
gestational diabetes (alsoreferred to as gestational diabetes
mellitus or
GDM). Gestational diabetes tends to occur aroundthe
24th week of pregnancy. The condition arisesbecause the action
of insulin is blocked, probablyby hormones produced by the
placenta.
As gestational diabetes normally develops later inpregnancy, the
unborn baby is already well-formedbut still growing. The immediate
risk to the babyis therefore not as severe as for those whosemother
had type 1 diabetes or type 2 diabetesbefore pregnancy (a condition
known as diabetes inpregnancy). Nonetheless, uncontrolled
gestationaldiabetes can have serious consequences for both
the mother and her baby.Poorly managed blood glucose during
pregnancycan lead to a significantly larger than averagebaby (a
condition known as fetal macrosomia),which makes a normal birth
difficult and risky.The newborn will be at risk for shoulder injury
andbreathing problems. In many cases, a caesareansection is
necessary, putting the mother’s health atrisk, particularly in
low-resource settings, whereaccess to good healthcare is limited.
For womenliving in outlying rural areas there is a
life-threat-ening risk from prolonged obstructed labour. There
also exists the risk of preeclampsia, a conditionwhere sudden
high blood pressure threatens thehealth (and in some cases the
life) of the motherand her baby.
Gestational diabetes in mothers normally disap-pears after
birth. However, women who havehad gestational diabetes are at a
higher risk ofdeveloping gestational diabetes in
subsequentpregnancies and of developing type 2 diabetes laterin
life. Babies born to mothers with gestationaldiabetes also have a
higher lifetime risk of obesityand developing type 2 diabetes.
Women with gestational diabetes or diabetesin pregnancy need to
monitor and control theirblood glucose levels to minimise risks to
the baby.Normally, this can be done by taking up a healthydiet and
moderate exercise, but in some casesinsulin or oral medication may
be needed as well.
-
8/20/2019 2013 IDF.pdf
24/160
24 I IDF Diabetes Atlas I Sixth edition
Impaired glucosetolerance andimpaired fastingglucosePeople whose
blood glucose levels are high but notas high as those in people
with diabetes are saidto have impaired glucose tolerance
(commonlyreferred to as IGT) or impaired fasting glucose(IFG). IGT
is defined as high blood glucose levelsafter eating; whereas IFG is
defined as high bloodglucose after a period of fasting. The term
‘predia-betes’ is also used to describe people with theseconditions
– a ‘grey area’ between normal glucoselevels and diabetes.
People with IGT are at high risk of developing type 2diabetes.
Unsurprisingly, IGT shares many charac-teristics with type 2
diabetes and is associated withobesity, advancing age and the
inability of the bodyto use the insulin it produces. Not everyone
withIGT goes on to develop type 2 diabetes: a large bankof evidence
supports the effectiveness of lifestyleinterventions – healthy diet
and physical exercise– to prevent the progression to diabetes.3
DiabetescomplicationsPeople with diabetes are at risk of
developing anumber of disabling and life-threatening
healthproblems. Consistently high blood glucose levelscan lead to
serious diseases affecting the heartand blood vessels, eyes,
kidneys, and nerves.People with diabetes are also at increased risk
ofdeveloping infections. In almost all high-incomecountries,
diabetes is a leading cause of cardio-vascular disease, blindness,
kidney failure, andlower-limb amputation. As the prevalence oftype
2 diabetes grows in low- and middle-incomecountries, so too does
the impact of these costly
– in both human and economic terms – compli-cations. Maintaining
blood glucose levels, bloodpressure and cholesterol close to normal
canhelp delay or prevent diabetes complications.People with
diabetes need regular monitoring forcomplications.
Cardiovascular diseaseCardiovascular disease is the most
commoncause of death and disability among peoplewith diabetes. The
cardiovascular diseases thataccompany diabetes include angina,
myocardial
infarction (heart attack), stroke, peripheral arterydisease, and
congestive heart failure. In peoplewith diabetes, high blood
pressure, high choles-terol, high blood glucose and other risk
factorscontribute to the increased risk of
cardiovascularcomplications.
Kidney diseaseKidney disease (nephropathy) is far more commonin
people with diabetes than in people withoutdiabetes; and diabetes
is one of the leading causesof chronic kidney disease. The disease
is caused bydamage to small blood vessels, which can causethe
kidneys to be less efficient, or to fail altogether.Maintaining
near-normal levels of blood glucoseand blood pressure can greatly
reduce the risk ofnephropathy.
Eye diseaseMany people with diabetes develop some form ofeye
disease (retinopathy), which can damage visionor provoke blindness.
Persistently high levels ofblood glucose, together with high blood
pressure
and high cholesterol, are the main causes of retino-pathy. The
network of blood vessels that supplythe retina can become blocked
and damaged inretinopathy, leading to permanent loss of
vision.Retinopathy can be managed through regular eyechecks and by
keeping blood glucose levels closeto normal.
Nerve damageWhen blood glucose and blood pressure are
exces-sively high, diabetes can provoke damage to nerves
throughout the body (neuropathy). This damagecan lead to
problems with digestion and urination,erectile dysfunction and a
number of other func-tions. The most commonly affected areas are
theextremities, particularly the feet. Nerve damage inthese areas
is called peripheral neuropathy, andcan lead to pain, tingling, and
loss of feeling. Lossof feeling is particularly dangerous because
it canallow injuries to go unnoticed, leading to seriousinfections
and ulceration, diabetic foot disease,and major amputations.
-
8/20/2019 2013 IDF.pdf
25/160
IDF Diabetes Atlas I Sixth edition I 25
c h a p t e r 1
W H A T I S D I A B E T E S ?
Figure 1.1 The major diabetes complications
Eyes (retinopathy)
Oral health
Heart and coronary circulation
(coronary heart disease)
Brain and cerebral circulation
(cerebrovascular disease)
Kidney
(nephropathy)
Lower limbs
(peripheral vascular disease)
Peripheral nervous system
(neuropathy)
Diabetic foot
(ulceration and amputation)
-
8/20/2019 2013 IDF.pdf
26/160
26 I IDF Diabetes Atlas I Sixth edition
Other complications
Oral healthDiabetes can pose a threat to oral health.
Forexample, there is an increased risk of inflamma-
tion of the gums (gingivitis) in people with poorglucose
control. Gingivitis in turn is a major causeof tooth loss and may
also increase the risk ofcardiovascular disease.
Sleep apnoeaRecent research demonstrates the likelihood of
arelationship between type 2 diabetes and obstruc-tive sleep
apnoea. Estimates suggest that up to40% of people with sleep apnoea
have diabetes,although the incidence of new diabetes in peoplewith
sleep apnoea is not known.5 In people withtype 2 diabetes,
sleep apnoea may have effects ontheir ability to control blood
glucose.
Diabetic footPeople with diabetes may develop a number
ofdifferent foot problems as a result of damage tonerves and blood
vessels. These problems caneasily lead to infection and ulceration,
which
increase a person’s risk of amputation. Peoplewith diabetes face
a risk of amputation that maybe more than 25 times greater than
that in peoplewithout diabetes.4 However, with good
manage-ment, a large proportion of amputations can beprevented.
Even when a person undergoes ampu-tation, the remaining leg – and
the person’s life– can be saved by good follow-up care from a
multi-disciplinary foot team.4 People with diabetes
mustexamine their feet regularly.
Pregnancy complicationsWomen with any type of diabetes during
preg-nancy risk a number of complications if they donot carefully
monitor and manage their condition.Women with diabetes require
detailed planningand close monitoring before and during pregnancyto
minimise complications. High blood glucoseduring pregnancy can lead
to fetal abnormalitiesand cause it to gain excess size and weight,
andoverproduce insulin. These can lead to problemsat delivery,
injuries to the child and mother, anda sudden drop in blood glucose
(hypoglycaemia)in the child after birth. Children who are
exposed
for a long time to high blood glucose in the wombare at higher
risk of developing type 2 diabeteslater in life.
-
8/20/2019 2013 IDF.pdf
27/160
IDF Diabetes Atlas I Sixth edition I 27
c h a p t e r 1
W H A T I S D I A B E T E S ?
Box 1.1 InsulinInsulin is a hormone that is produced in
thepancreas. Insulin allows glucose to enter thebody’s cells, where
it is converted into energy.
People with type 1 diabetes cannot survivewithout daily insulin
doses. Some people withtype 2 diabetes or gestational diabetes
alsoneed doses of insulin together with othermedication.
In Canada in 1921, scientist Frederick Bantingand medical
student Charles Best isolated asubstance from the pancreas of dogs,
whichthey named isletin – and which is now known asinsulin. In a
series of experiments, they found
that a pancreatectomised dog could be keptalive with injections
of isletin. The followingyear, after much laboratory work to
purify
insulin extracted from a fetal calf, a 14-year-old boy called
Leonard Thompson became thefirst person with diabetes to receive an
insulininjection, and his condition improved signifi-cantly. Prior
to the discovery of insulin, peoplewith diabetes were put on a
starvation diet andhad no hope of survival.
News of the success with insulin spread veryquickly, and demand
for the drug skyrocketedworldwide. Since then, huge advances
havebeen made in research and development.However, nearly a century
since its discovery,people with type 1 diabetes in many parts of
theworld cannot access insulin – either because
they cannot afford to pay for it or because it isnot readily
available – and die soon after devel-oping diabetes.
Figure 1.2 Insulin production and action
LiverGlycogen Glucose
Glucagon
InsulinStimulates glucoseuptake from blood
Promotesglucagonrelease
Promotesinsulinrelease
Stimulatesformation
of glycogen
Stimulatesbreakdownof glycogen
Tissue Cells(muscle, brain, fat, etc.)
Pancreas
Highbloodglucose
Raisesbloodglucose
Lowbloodglucose
Lowersbloodglucose
-
8/20/2019 2013 IDF.pdf
28/160
28 I IDF Diabetes Atlas I Sixth edition
© I st o c k ph ot o. c om
-
8/20/2019 2013 IDF.pdf
29/160
IDF Diabetes Atlas I Sixth edition I 29
The globalburden
2 c h a p t e r 2
T H E G L O B A L B U R D E N
-
8/20/2019 2013 IDF.pdf
30/160
30 I IDF Diabetes Atlas I Sixth edition
175 million people
with diabetes are
undiagnosed
382 million peoplehave diabetes
By 2035 this will riseto 592 MILLION
The numberof people withtype 2 diabetesis increasingin every
country
The greatestnumber of people
with diabetes arebetween 40 and59 years of age
-
8/20/2019 2013 IDF.pdf
31/160
IDF Diabetes Atlas I Sixth edition I 31
c h a p t e r 2
T H E
G L O B A L
B U R D E N
Diabetes caused at leastUSD 548 billion dollarsin health
expenditure in2013 – 11% of total healthspending on adults
of people with diabeteslive in low- and middle-income
countries
80%
More than
79,000 children developed type 1diabetes in 2013
More than
21 million live births were affectedby diabetes
duringpregnancy in 2013
Diabetes caused 5.1 million
deaths in 2013
Every six seconds a persondies from diabetes
-
8/20/2019 2013 IDF.pdf
32/160
32 I IDF Diabetes Atlas I Sixth edition
The global
burdenIn addition to diabetes, impaired glucose tolerance(IGT),
in which blood glucose levels are higher thannormal but not as high
as in diabetes, is also amajor public health problem. People with
IGT havea high risk of developing diabetes as well as anincreased
risk of cardiovascular disease.
Prevalence and projectionsIn this edition of the IDF Diabetes
Atlas, theprevalence of diabetes and IGT are estimated forthe years
2013 and 2035. Data are provided for219 countries and territories,
grouped into theseven IDF Regions: Africa (AFR), Europe
(EUR),Middle East and North Africa (MENA), NorthAmerica and
Caribbean (NAC), South and CentralAmerica (SACA), South-East Asia
(SEA), and theWestern Pacific (WP).
Full details of the methods used to generate the
prevalence estimates for diabetes in adults and theproportion
undiagnosed, including how the datasources were evaluated and
processed, can befound in the journal Diabetes Research and
ClinicalPractice and on the IDF Diabetes
Atlas website:www.idf.org/diabetesatlas.
Diabetes andimpaired glucosetoleranceDiabetes is one of the most
common non-commu-nicable diseases (NCDs). It is the fourth or
fifthleading cause of death in most high-income coun-
tries and there is substantial evidence that it isepidemic in
many economically developing andnewly industrialised countries.
Diabetes is undoubtedly one of the most chal-lenging health
problems of the 21st century.
The number of studies describing the possiblecauses and
distribution of diabetes over the last20 years has been
extraordinary. These studiescontinue to confirm that it is the low-
and middle-income countries that face the greatest burdenof
diabetes. However, many governments and
public health planners remain largely unaware ofthe current
magnitude of and future potential forincreases in diabetes and its
serious complications.
Population-based diabetes studies consistentlyshow that a
substantial proportion of those foundto have diabetes had not been
previously diag-nosed. Many people remain undiagnosed
largelybecause there are few symptoms during the earlyyears of type
2 diabetes, or those symptoms maynot be recognised as being related
to diabetes.
-
8/20/2019 2013 IDF.pdf
33/160
IDF Diabetes Atlas I Sixth edition I 33
c h a p t e r 2
T H E
G L O B A L
B U R D E N
ComplicationsComplications due to diabetes (Chapter 1) are
amajor cause of disability, reduced quality of life,and death.
Diabetes complications can affectvarious parts of the body,
manifesting in different
ways in different people.There are no internationally agreed
standards fordiagnosing and assessing diabetes complications.Due to
the variety of methods of these studies, itis difficult to make
comparisons between differentpopulations. However, it is clear that
diabetes
complications are very common, with at leastone present in a
large proportion of people withdiabetes (50% or more in some
studies) at the timeof diagnosis.
In this edition of the IDF Diabetes Atlas , estimatesof
complications were not included due to the lackof available
comparable data. International stand-ards for measuring
complications are essentialto provide accurate estimates of this
major causeof disability.
AT A GLANCE 2013 2035
Total world population (billions) 7.2 8.7
Adult population (20-79 years, billions) 4.6 5.9
DIABETES AND IGT (20-79 YEARS)
Diabetes
Global prevalence (%) 8.3 10.1
Comparative prevalence (%) 8.3 8.8
Number of people with diabetes (millions) 382 592
IGT
Global prevalence (%) 6.9 8.0
Comparative prevalence (%) 6.9 7.3
Number of people with IGT (millions) 316 471
Table 2.1 Top 10 countries/territories for prevalence* (%)
of diabetes (20-79 years), 2013 and 2035
COUNTRY/
TERRITORY
2013
(%)
COUNTRY/
TERRITORY
2035
(%)
Tokelau 37.5 Tokelau 37.9
Federated States of Micronesia 35.0 Federated States of
Micronesia 35.1
Marshall Islands 34.9 Marshall Islands 35.0
Kiribati 28.8 Kiribati 28.9
Cook Islands 25.7 Cook Islands 25.7Vanuatu 24.0 Saudi Arabia
24.5
Saudi Arabia 24.0 Vanuatu 24.2
Nauru 23.3 Nauru 23.3
Kuwait 23.1 Kuwait 23.2
Qatar 22.9 Qatar 22.8
*comparative prevalence
-
8/20/2019 2013 IDF.pdf
34/160
34 I IDF Diabetes Atlas I Sixth edition
2.1 DiabetesDiabetes can be found in every country.
Withouteffective prevention and management programmes,the burden
will continue to increase worldwide.1
Type 2 diabetes accounts for 85% to 95% of alldiabetes in
high-income countries and may accountfor an even higher percentage
in low- and middle-income countries.1 Type 2 diabetes is a
common
condition and a serious global health problem.In most countries
diabetes has increased along-side rapid cultural and social
changes: ageingpopulations, increasing urbanisation,
dietarychanges, reduced physical activity and
unhealthybehaviours.1
Type 1 diabetes, although less common than type 2diabetes, is
increasing each year in both rich andpoor countries. In most
high-income countries, themajority of diabetes in children and
adolescentsis type 1 diabetes.
Gestational diabetes is common and, like obesityand type 2
diabetes, is increasing throughout theworld.2 The risk of
developing type 2 diabetes ishigh in women who have had gestational
diabetes.The reported prevalence of gestational diabetesvaries
widely among different populations aroundthe world. Much of the
variability is due to differ-ences in diagnostic criteria and study
populations.
PrevalenceSome 382 million people worldwide, or 8.3% ofadults,
are estimated to have diabetes. About80% live in low- and
middle-income countries. Ifthese trends continue, by 2035, some 592
millionpeople, or one adult in 10, will have diabetes. Thisequates
to approximately three new cases every10 seconds, or almost 10
million per year. The
largest increases will take place in the regionswhere developing
economies are predominant.
Age distributionAlmost half of all adults with diabetes are
betweenthe ages of 40 and 59 years. More than 80% of the184 million
people with diabetes in this age grouplive in low- and
middle-income countries.
This age group will continue to comprise the greatestnumber of
people with diabetes in the coming years.By 2035, it is expected
that the number will increase
to 264 million. Again, more than 86% will be livingin low- and
middle-income countries.
Gender distributionThere is little gender difference in the
globalnumbers of people with diabetes for 2013 or2035. There are
about 14 million more menthan women with diabetes (198 million men
vs184 million women). However, this difference isexpected to
increase to 15 million (303 million menvs 288 million women) by
2035.
Table 2.2 Top 10 countries/territories for number of
people with diabetes (20-79 years),
2013 and 2035
COUNTRY/
TERRITORY
2013
MILLIONS
COUNTRY/
TERRITORY
2035
MILLIONS
China 98.4 China 142.7
India 65.1 India 109.0
United States of America 24.4 United States of America 29.7
Brazil 11.9 Brazil 19.2
Russian Federation 10.9 Mexico 15.7
Mexico 8.7 Indonesia 14.1
Indonesia 8.5 Egypt 13.1
Germany 7.6 Pakistan 12.8
Egypt 7.5 Turkey 11.8
Japan 7.2 Russian Federation 11.2
-
8/20/2019 2013 IDF.pdf
35/160
IDF Diabetes Atlas I Sixth edition I 35
c h a p t e r 2
T H E
G L O B A L
B U R D E N
countries, the number of people with diabetes inurban areas is
181 million, while 122 million livein rural areas. By 2035, the
difference is expectedto widen, with 347 million people living in
urbanareas and 145 million in rural areas.
Urban/rural distributionThere are more people with diabetes
living inurban (246 million) than in rural (136 million)areas
although the numbers for rural areasare on the increase. In low-
and middle-income
Figure 2.1 Prevalence* (%) of diabetes (20-79 years)
by IDF Region, 2013 and 2035
12
10
8
6
4
2
0
AFR EUR MENA NAC SACA SEA WP
%
2013
2035 *comparative prevalence
Figure 2.2 Prevalence (%) of people with diabetes by
age
and sex, 2013
20
15
10
5
0
20 25 30 35 40 45 50 55 60 65 70 75
age (years)
%
Female
Male
-
8/20/2019 2013 IDF.pdf
36/160
36 I IDF Diabetes Atlas I Sixth edition
M a p 2 . 1
P r e v a l e n c e * ( % ) o f d i a b e t e s i n a d u l t s ( 2 0 - 7 9 y e a r s ) , 2 0 1
3
< 4
4 - 5
5 - 7
7 - 9
9 - 1 2
> 1 2
* c o m p a r a t i v e p r e v a l e n c e
-
8/20/2019 2013 IDF.pdf
37/160
IDF Diabetes Atlas I Sixth edition I 37
c h a p t e r 2
T H E
G L O B A L
B U R D E N
M a p 2 . 2
N u m b e r o f p e o p l e w i t h
d i a b e t e s ( 2 0 - 7 9 y e a r s ) , 2 0 1 3
< 1 0 0 , 0 0 0
1 0 0 , 0 0 0 - 5 0 0 , 0 0 0
5 0 0 , 0 0 0 - 1 , 0 0 0 , 0 0 0
1 , 0 0 0 , 0 0 0 - 1 0 , 0 0 0 , 0 0 0
1 0 , 0 0 0 , 0 0 0 - 2 0 , 0 0 0 , 0 0 0
> 2 0 , 0
0 0 , 0 0 0
-
8/20/2019 2013 IDF.pdf
38/160
38 I IDF Diabetes Atlas I Sixth edition
CostsThe costs associated with diabetes includeincreased use of
health services, productivityloss and disability, which can be a
considerableburden to the individual, families and society.
When
people have long-standing undiagnosed diabetes,the potential
benefits of early diagnosis and treat-ment are lost. Furthermore,
the costs related toundiagnosed diabetes are considerable. One
studyfrom the USA found that undiagnosed diabeteswas responsible
for an additional USD 18 billionin healthcare costs in one
year.5
Identifying peoplewith diabetesOpportunistic identification of
people with risk
factors for undiagnosed type 2 diabetes is feasibleand
cost-effective.6 Risk scores and ‘tick tests’listing risk
factors have been developed in manycountries based on
epidemiological surveys ofthe local populations, and are widely
available.While undiagnosed diabetes is a substantialproblem,
population-wide screening for diabetesis not appropriate. Countries
must first develophealth systems that can meet the needs ofpeople
living with the disease. Priority shouldbe given to providing good
care and treatment topeople already identified with diabetes.
Targeted
screening for those at high risk of undiagnoseddiabetes may be
considered once a working systemfor care is in place.
Estimating undiagnoseddiabetesPopulation-based studies provide
the basis for esti-mating undiagnosed diabetes. A sample of
peopleliving in a particular area is tested for diabetes,which
identifies both known and previously undi-agnosed cases. The IDF
Diabetes Atlas estimates
undiagnosed diabetes using representative popu-lation-based
studies reporting the proportion ofpreviously undiagnosed cases.
The findings fromthese studies are then combined by Region
andincome group to generate an estimate that is laterapplied to the
prevalence estimates. Full detailsof the methods and results are
available in thepublished paper at www.idf.org/diabetesatlas.
2.2 UndiagnoseddiabetesIDF estimates that as many as 175 million
peopleworldwide, or close to half of all people withdiabetes, are
unaware of their disease. Most ofthese cases are type 2 diabetes.
The earlier aperson is diagnosed and management of diabetesbegins,
the better the chances of preventingharmful and costly
complications. The need todiagnose and provide appropriate care to
peoplewith diabetes is therefore urgent.
Disparities by regionNo country has diagnosed every person that
hasdiabetes. In sub-Saharan Africa, where resourcesare often
lacking and governments may not
prioritise screening for diabetes, the proportionof people with
diabetes who are undiagnosed isas high as 90% in some
countries.1 Even in high-income countries, about one-third of
people withdiabetes have not been diagnosed. The South-EastAsia
Region (35.1 million) and the Western PacificRegion (74.7 million)
together account for over 60%of all people with undiagnosed
diabetes. Globally,84% of all people who are undiagnosed live in
low-and middle-income countries.
ComplicationsA person with type 2 diabetes can live for
severalyears without showing any symptoms. But duringthat time high
blood glucose is silently damagingthe body and diabetes
complications may bedeveloping. The complications associated
withdiabetes are so varied that even when symptomsdo exist,
diabetes may not be recognised as thecause unless accurate and
appropriate testing iscarried out. Those who are undiagnosed will
not betaking steps to manage their blood glucose levelsor
lifestyle. Studies have found that many peoplewith undiagnosed
diabetes already have compli-
cations, such as chronic kidney disease and heartfailure,
retinopathy and neuropathy.2-4
-
8/20/2019 2013 IDF.pdf
39/160
IDF Diabetes Atlas I Sixth edition I 39
c h a p t e r 2
T H E
G L O B A L
B U R D E N
Map 2.3 Prevalence* (%) of undiagnosed diabetes (20-79
years), 2013
*comparative prevalence
< 1
1-2.5
2.5-3
3-4.5
4.5-6
> 6
Table 2.3 Undiagnosed diabetes (20-79 years) by IDF Region
and income group, 2013
IDF
REGION
PROPORTION
UNDIAGNOSED %
CASES
MILLIONS
Africa 12.4Low-income countries 75.1Middle-income countries
46.0
Europe 20.1Low-income countries 29.3Middle-income countries
35.1High-income countries 36.6
Middle East and North Africa 16.8Low-income countries
50.0Middle-income countries 50.0High-income countries 40.7
North America and Caribbean 9.9Low-income countries
29.4Middle-income countries 25.0High-income countries 27.7
South and Central America 5.8Middle-income countries 24.1
South-East Asia 35.1Low-income countries 43.6Middle-income
countries 49.1
Western Pacific 74.7Low-income countries 63.0Middle-income
countries 54.1High-income countries 49.4
-
8/20/2019 2013 IDF.pdf
40/160
40 I IDF Diabetes Atlas I Sixth edition
Figure 2.3 Number of people with IGT by age
(20-79 years), 2013 and 20352.3 Impaired
glucosetoleranceImpaired glucose tolerance (IGT), along
withimpaired fasting glucose (IFG), is recognised as
being a stage preceding diabetes when bloodglucose levels are
higher than normal. Thus,people with IGT are at high risk of
developingtype 2 diabetes, although all people with IGT donot
always go on to develop the disease. In morethan one-third of
people with IGT, blood glucoselevels will return to normal over a
period of severalyears.1
Data on IGT are included in this report becauseIGT greatly
increases the risk of developing type 2diabetes1 and it is
linked with the development ofcardiovascular disease.2,3 In
addition, some of the
best evidence on the prevention of type 2 diabetescomes from
studies involving people with IGT.
PrevalenceSome 316 million people worldwide, or 6.9% ofadults,
are estimated to have IGT. The vast majority(70%) of these people
live in low- and middle-income countries. By 2035, the number of
peoplewith IGT is projected to increase to 471 million, or8.0% of
the adult population.
Age distributionThe majority of adults with IGT are under the
ageof 50 (153 million) and, if left untreated, are athigh risk of
progressing to type 2 diabetes laterin life. This age group will
continue to have thehighest number of people with IGT in 2035,
risingto 198 million, as shown in Figure 2.3. It is impor-tant to
note that nearly one-third of all those whocurrently have IGT are
in the 20 to 39 year agegroup, and are therefore likely to spend
many yearsat high risk – if indeed they do not go on to
developdiabetes.
The prevalence of IGT is generally similar to thatof diabetes,
but somewhat higher in the Africa andEurope Regions and lower in
the South-East AsiaRegion.
Figure 2.4 Prevalence (%) of IGT (20-79 years)
by age and sex, 2013
200
180
160
140
120
100
80
60
40
20
0
m i l l i o n s
20-39 40-59 60-79
age (years)
16
14
12
10
8
6
4
2
0
20 25 30 35 40 45 50 55 60 65 70 75
age (years)
%
Female
Male
2013
2035
-
8/20/2019 2013 IDF.pdf
41/160
IDF Diabetes Atlas I Sixth edition I 41
c h a p t e r 2
T H E
G L O B A L
B U R D E N
Table 2.4 Top 10 countries/territories for prevalence* (%)
of IGT (20-79 years), 2013 and 2035
COUNTRY/
TERRITORY
2013
(%)
COUNTRY/
TERRITORY
2035
(%)
Kuwait 17.9 Poland 19.3
Qatar 17.1 Kuwait 18.1
United Arab Emirates 16.6 Qatar 17.4
Poland 16.5 United Arab Emirates 17.0
Bahrain 16.3 Bahrain 16.7
Malaysia 15.2 Malaysia 15.3
Hong Kong SAR 13.3 Hong Kong SAR 13.2
Nicaragua 12.9 Anguilla 13.0
Japan 12.6 Guadeloupe 13.0
Singapore 12.4 Macau SAR 12.9
*comparative prevalence
Map 2.4 Prevalence* (%) of impaired glucose tolerance
(20-79 years), 2013
< 6
6-8
8-10
10-12
12-14
> 14*comparative prevalence
-
8/20/2019 2013 IDF.pdf
42/160
42 I IDF Diabetes Atlas I Sixth edition
is less common. Also, several European studieshave suggested
that, in relative terms, increasesare greatest among younger
children.
There is also evidence that similar trends exist inmany other
parts of the world, but in sub-Saharan
Africa incidence data are limited or non-existent.Special
efforts must be made to collect more data,especially in those
countries where diagnoses maybe missed.
Some 79,100 children under 15 years are estimatedto develop type
1 diabetes annually worldwide. Ofthe estimated 497,100 children
living with type 1diabetes, 26% live in the Europe Region, where
themost reliable and up-to-date estimates of inci-dence are
available, and 22% in the North Americaand Caribbean Region.
Type 2 diabetes inyoung peopleThere is evidence that type 2
diabetes in childrenand adolescents is increasing in some
countries.However, reliable data are sparse.4 As with type
1diabetes, many children with type 2 diabetes riskdeveloping
complications in early adulthood, whichwould place a significant
burden on the familyand society. With increasing levels of obesity
andphysical inactivity among young people in manycountries, type 2
diabetes in childhood has the
potential to become a global public health issueleading to
serious health outcomes. More informa-tion about this aspect of the
diabetes epidemic isurgently needed.
2.4 Diabetesin young peopleType 1 diabetes is one of the most
common endo-crine and metabolic conditions in childhood.The number
of children developing this form ofdiabetes every year is
increasing rapidly, espe-cially among the youngest children. In a
growingnumber of countries, type 2 diabetes is also beingdiagnosed
in children.
The challengesIn type 1 diabetes, insulin therapy is
life-savingand lifelong. A person with type 1 diabetes needsto
follow a structured self-management plan,including insulin use and
blood glucose moni-toring, physical activity, and a healthy diet.
In
many countries, especially in low-income families,access to
self-care tools, including self-manage-ment education, as well as
to insulin, is limited.This leads to severe disability and early
death inchildren with diabetes.
Many children and adolescents may find it difficultto cope
emotionally with their disease. Diabetescan result in
discrimination and may limit socialrelationships. It may also have
an impact on achild’s academic performance. The costs of treat-ment
and monitoring equipment, combined withthe daily needs of a child
with diabetes, may place
a serious financial and emotional burden on thewhole family.
Incidence and prevalenceThree major collaborative projects, the
DiabetesMondiale study (DIAMOND),1 the Europe andDiabetes
study (EURODIAB),2 and the SEARCH forDiabetes in Youth
study3 have been instrumentalin monitoring trends in incidence
(the number ofpeople developing a disease in a year). This hasbeen
done by setting up population-based regional
or national registries using standardised defini-tions, data
collection forms, and methods forvalidation.
The incidence of type 1 diabetes among children isincreasing in
many countries, particularly in chil-dren under the age of 15
years. There are strongindications of geographic differences in
trendsbut the overall annual increase is estimated tobe around
3%.1,2 Evidence shows that incidenceis increasing more steeply
in some Central andEastern European countries, where the
disease
-
8/20/2019 2013 IDF.pdf
43/160
IDF Diabetes Atlas I Sixth edition I 43
c h a p t e r 2
T H E
G L O B A L
B U R D E N
AT A GLANCE 2013
Total child population (0-14 years, billions) 1.9
TYPE 1 DIABETES IN CHILDREN (0-14 YEARS)
Number of children with type 1 diabetes (thousands) 497.1
Number of children per year (thousands) 79.1
Annual increase in incidence (%)1,2 3
Figure 2.5 Estimated number of children (0-14 years)
with
type 1 diabetes by IDF Region, 2013
120
100
80
60
40
20
0
AFR EUR MENA NAC SACA SEA WP
t h o u s a n d s
Map 2.5 New cases of type 1 diabetes (0-14 years per
100,000 children per year), 2013
< 1.5
1.5-5
5-8.5
8.5-14
14-24
> 24
No data
-
8/20/2019 2013 IDF.pdf
44/160
44 I IDF Diabetes Atlas I Sixth edition
PrevalenceIDF estimates that 21.4 million or 16.8% of livebirths
to women in 2013 had some form of hyper-glycaemia in pregnancy. An
estimated 16% of thosecases were due to diabetes in pregnancy and
would
require careful monitoring during the pregnancyand follow-up
post-partum.
There are some regional differences in the preva-lence (%) of
hyperglycaemia in pregnancy, with theSouth-East Asia Region having
the highest preva-lence at 25.0% compared to 10.4% in the
NorthAmerica and Caribbean Region. A staggering91.6% of cases of
hyperglycaemia in pregnancywere in low- and middle-income
countries, whereaccess to maternal care is often limited.
The prevalence of hyperglycaemia in pregnancyincreases rapidly
with age and is highest in womenover the age of 45 (47.7%),
although there arefewer pregnancies in that age group. This
explainswhy just 23% of global cases of hyperglycaemia inpregnancy
occurred in women over the age of 35,even though the risk of
developing the conditionis higher in these women.
Estimating prevalenceThere is great diversity in the methods and
criteriaused for identifying women with hyperglycaemia inpregnancy,
which increases the difficulty of making
comparisons between studies and generatingestimates on
prevalence.2 However, the recentpublication of a guideline
from the World HealthOrganization on diagnosing hyperglycaemia
inpregnancy will contribute to a standard approachto estimating
prevalence.3
Data on hyperglycaemia in pregnancy from studieswere available
for 34 countries across all IDFRegions. Although each of the
Regions was repre-sented, the majority of the studies were
carriedout in high-income countries. More informationis available
on the methods used to generate the
estimates at www.idf.org/diabetesatlas.
2.5 Hyperglycaemiain pregnancyHigh blood glucose, or
hyperglycaemia, is one ofthe most common health problems of
pregnancy.1 Hyperglycaemia in pregnancy can be a result
ofeither previously existing diabetes in a pregnantwoman, or the
development of insulin resistancelater in the pregnancy in a
condition known asgestational diabetes. Unlike diabetes in
pregnancy,gestational diabetes resolves once the pregnancyends.
Hyperglycaemia in pregnancy is categorised(see Box 6.1) as either
diabetes in pregnancy orgestational diabetes, depending on blood
glucosevalues obtained during screening.
Risks and complications
Any unmanaged hyperglycaemia in pregnancycan result in birth
complications that can affectboth mother and child including:
increased riskof preeclampsia, obstructed labour due to
fetalmacrosomia and hypoglycaemia at birth forthe infant.
As the prevalence of both obesity and diabetes inwomen of
childbearing age continue to rise in allregions, so will the
prevalence of hyperglycaemiain pregnancy. In addition, women who
developgestational diabetes have an increased lifetimerisk of
developing type 2 diabetes.2 Babies born to
mothers who have hyperglycaemia in pregnancyare also at an
increased risk of developing type 2diabetes later in life.
-
8/20/2019 2013 IDF.pdf
45/160
IDF Diabetes Atlas I Sixth edition I 45
c h a p t e r 2
T H E
G L O B A L
B U R D E N
AT A GLANCE 2013
Total live births (20-49 years, millions) 127.1
HYPERGLYCAEMIA IN PREGNANCY IN WOMEN (20-49 YEARS)
Global prevalence (%) 16.9
Comparative prevalence (%) 14.8
Number of live births with hyperglycaemia in pregnancy
(millions) 21.4
Proportion of cases that may be due to diabetes in pregnancy (%)
16.0
Table 2.5 Hyperglycaemia in pregnancy (20-49 years) by IDF
Region, 2013
IDFREGION
Cases in live births MILLIONS
Prevalence* %
Proportion of cases that may bedue to diabetes in pregnancy
%
AFR 4.6 14.4 19.6EUR 1.7 12.6 10.9
MENA 3.4 17.5 17.7
NAC 0.9 10.4 24.9
SACA 0.9 11.4 17.3
SEA 6.3 25.0 9.5
WP 3.7 11.9 14.1
*comparative prevalence
Map 2.6 Data sources providing information on prevalence
of hyperglycaemia in pregnancy, 2013
1-3
3-5
5-7
7-9
9-15
> 15
No data
-
8/20/2019 2013 IDF.pdf
46/160
46 I IDF Diabetes Atlas I Sixth edition
TrendsThe number of deaths attributable to diabetes in2013
showed an 11% increase over estimates for2011.1,2 This
increase was largely due to rises inthe number of deaths due to the
disease in the
Africa, Western Pacific, and Middle East and NorthAfrica
Regions. This can be explained in part by arise in diabetes
prevalence in some highly popu-lated countries in each Region.
While there hasbeen a documented decline in mortality from someNCDs
in some countries,3 no such decline has beenreported for
diabetes.
Accuracy of mortality dataThe mortality estimates should be
interpreted withcaution. However, they are probably more
realisticthan estimates based on routine sources of
healthstatistics, which consistently underestimate theburden of
mortality from diabetes largely becausediabetes is often omitted
from death certificatesas the cause of death. A substantial
proportionof these deaths are potentially avoidable throughpublic
health action directed at population-basedprevention of diabetes
and its complications andimprovements in care for all people with
diabetes.4
2.6 MortalityDiabetes and its complications are major causesof
early death in most countries. Cardiovasculardisease (see Chapter
1) is one of the leadingcauses of death among people with diabetes.
It can
account for 50% or more of deaths due to diabetesin some
populations. Estimating the number ofdeaths due to diabetes is
challenging because onthe one hand, more than a third of countries
donot have any data on diabetes-related mortality;and on the other,
because existing routine healthstatistics underestimate the number
of deaths dueto diabetes. To provide a more realistic estimate
ofmortality, the IDF Diabetes Atlas uses a
modellingapproach to estimate the number of deaths thatcan be
attributed to diabetes.1
Burden of mortalityApproximately 5.1 million people aged between
20and 79 years died from diabetes in 2013, accountingfor 8.4% of
global all-cause mortality amongpeople in this age group. This
estimated numberof deaths is similar in magnitude to the
combineddeaths from several infectious diseases that aremajor
public health priorities,* and is equivalentto one death every
six seconds. Close to half (48%)of deaths due to diabetes are in
people under theage of 60. The highest number of deaths due
todiabetes occurred in countries with the largest
numbers of people with the disease: China, India,USA, and the
Russian Federation.
Gender distributionThere is very little difference between men
andwomen in the total number of deaths due todiabetes. However,
there are important differencesin the distribution of these
deaths.
In all but the Middle East and North Africa, andWestern Pacific
Regions, diabetes accounts fora higher proportion of deaths in
women than in
men, representing up to a quarter of all deathsin middle-aged
women. This disparity is likely tobe due to higher rates of
mortality in men fromother causes.
* In 2009 there were 1.8 million deaths from
HIV/AIDS,5 781,000 from malaria6 and 1.3 million from
tuberculosis.7
-
8/20/2019 2013 IDF.pdf
47/160
IDF Diabetes Atlas I Sixth edition I 47
c h a p t e r 2
T H E
G L O B A L
B U R D E N
Map 2.7 Deaths attributable to diabetes (20-79 years),
2013
Figure 2.6 Deaths attributable to diabetes as a percentage
of
all deaths (20-79 years) by IDF Region, 2013
15
10
5
0
AFR EUR MENA NAC SACA SEA WP
%
< 100
100-1,500
1,500-8,000
8,000-40,000
40,000-100,000
> 100,000
No data
-
8/20/2019 2013 IDF.pdf
48/160
48 I IDF Diabetes Atlas I Sixth edition
Disparities inhealth spendingThere is a large disparity in
health spending ondiabetes between regions and countries. Only20%
of global health expenditure on diabetes wasmade in low- and
middle-income countries, where80% of people with diabetes live. On
average, theestimated health spending due to diabetes wasUSD 5,621
(ID 5,305) per person with diabetesin high-income countries,
compared to USD 356(ID 545) in low- and middle-income
countries.
The USA spent USD 239 billion of its health dollarson diabetes,
or 36% of global health expenditure.Meanwhile, China, the country
with the most peopleliving with diabetes, spent just USD 38
billion,less than 7% of the global total. The combinedspending of
the top three countries, the USA,Germany and China, was equivalent
to more thanhalf of all global health expenditure on diabetesin
2013. Norway spent an average of USD 10,368on diabetes healthcare
per person with diabetes,while countries such as Somalia and
Eritrea spentless than USD 30.
Economic burdenCompared with those living in high-income
coun-tries, people living in low- and middle-incomecountries pay a
larger share of health expendi-
ture because they lack access to health insuranceand publicly
available medical services. In LatinAmerica, for instance, families
pay between 40%and 60% of medical expenses from their
ownpockets.1 In some of the poorest countries, peoplewith
diabetes and their families bear almost thetotal cost of medical
care.
Implementing inexpensive, easy-to-use interven-tions can reduce
the huge economic burden ofdiabetes. Many of these interventions
are cost-effective and/or cost saving, even in
developingcountries.2 Nonetheless, these interventions are
not widely used.
2.7 HealthexpenditureDiabetes imposes a large economic burden on
indi-viduals and families, national health systems, andcountries.
Health spending on diabetes accountedfor 10.8% of total health
expenditure worldwide in2013. About 90% of the countries covered in
thisreport dedicated between 5% and 18% of their totalhealth
expenditure to diabetes. Health expenditureincludes medical
spending on diabetes by healthsystems, as well as by people living
with diabetesand their families.
Global health expenditureGlobal health spending to treat
diabetes and managecomplications totalled at least USD 548 billion
in
2013. By 2035, this number is projected to exceedUSD 627
billion. Expressed in International Dollars(ID), which correct for
differences in purchasingpower, global health spending on diabetes
wasestimated to be at least ID 581 billion in 2013 andID 678
billion in 2035. An estimated average ofUSD 1,437 (ID 1,522) per
person with diabeteswas spent globally on treating and managing
thedisease in 2013.
Health spending due to diabetes is not evenlydistributed across
age groups. The estimates showthat 76% of global health expenditure
on diabetes
in 2013 was for people between the ages of 50 and79 years.
-
8/20/2019 2013 IDF.pdf
49/160
IDF Diabetes Atlas I Sixth edition I 49
c h a p t e r 2
T H E
G L O B A L
B U R D E N
*see Glossary
Map 2.8 Mean diabetes-related health expenditure per
person with diabetes (20-79 years)
(USD), R=2*, 2013
Figure 2.7 Health expenditure due to diabetes by age
(USD, R=2), 2013
< 50
50-500
500-1,500
1,500-3,000
3,000-6,500
> 6,500
No data
160
140
120
100
80
60
40
20
0
20-29 30-39 40-49 50-59 60-69 70-79
b i l l i o n s
age (years)
-
8/20/2019 2013 IDF.pdf
50/160
50 I IDF Diabetes Atlas I Sixth edition
© I st o c k ph ot o. c om
-
8/20/2019 2013 IDF.pdf
51/160
IDF Diabetes Atlas I Sixth edition I 51
3Regionaloverviews
c h a p t e r 3
R E G I O N A L O V E R V I E W S
-
8/20/2019 2013 IDF.pdf
52/160
52 I IDF Diabetes Atlas I Sixth edition
More was spent onhealthcare for diabetes
in the North America andCaribbean than in anyother region
In the Middle East
and North Africa,
1 in 10 adults
has diabetes
/10
In South-East Asia,half of people withdiabetes are
undiagnosed
$
$
$
-
8/20/2019 2013 IDF.pdf
53/160
IDF Diabetes Atlas I Sixth edition I 53
c h a p t e r 3
R E G I O N A L O V E R V I E W S
Europe has the highestprevalence of CHILDRENwith type 1
diabetes
In the Western Pacific,
138 million adults have diabetes– the largest
number
of any region
In Africa, 76%of deaths due todiabetes were in
people underthe age of 60
↗60%In South and CentralAmerica, the number
of people with diabetes
will increase by 60%
by 2035
-
8/20/2019 2013 IDF.pdf
54/160
54 I IDF Diabetes Atlas I Sixth edition
3 Regionaloverviews
lation compared with the other Regions althoughthis is projected
to more than double by 2035. Interms of the prevalence of adults
with diabetes,the Middle East and North Africa Region has
thehighest, at 10.9%. MENA is followed closely bythe 9.6% rate
found in the North America andCaribbean Region while 8.2% of adults
in the
South and Central America Region have diabetes(Table 3.0).
The picture is similar for IGT. The Western PacificRegion is
estimated to have the greatest numberof people with IGT and
consequently at greatlyincreased risk for developing type 2
diabetes, withsome 110 million; although the North Americaand
Caribbean Region has the highest compara-tive prevalence, with
12.1% of the adult populationaffected. Worldwide, the prevalence
(%) of IGT islower than that of diabetes but there is a high
riskthat, if not treated early, these people will progress
to diabetes.
Deaths due to diabetesMortality attributable to diabetes ranges
from8.6% of all deaths in adults aged between 20and 79 in the
Africa Region to almost 15.8% inthe Western Pacific Region. Almost
half of alldeaths due to diabetes occurred in people underthe age
of 60. Diabetes is a major cause of deathworldwide; investment in
reducing this burden is justified and necessary.
A global perspectiveThe majority of people with diabetes live in
theeconomically less-developed regions of the world.Even in Africa,
the Region with the lowest preva-lence, it is estimated that around
522,600 peopledied due to diabetes in 2013. The disparities inthe
world’s response to the epidemic are huge:
although 80% of people with diabetes live in low-and
middle-income countries, only 20% of globalhealth expenditure on
the disease was made inthose countries.
A global perspective of the epidemic is essentialto understand
the true dimensions of the diabetesburden and its consequences.
This chapterpresents an overview of each of the seven IDFRegions:
Africa (AFR), Europe (EUR), the MiddleEast and North Africa (MENA),
North Americaand Caribbean (NAC), South and Central America(SACA),
South-East Asia (SEA), and the Western
Pacific (WP). Each Region is highly diverse insocioeconomic and
geographical terms and indiabetes prevalence, related deaths, and
healthexpenditure.
Prevalence of diabetes andimpaired glucose toleranceA staggering
138 million people are living withdiabetes in the Western Pacific,
more than inany other IDF Region. With 19.8 million peopleaffected,
Africa has the smallest diabetes popu-
-
8/20/2019 2013 IDF.pdf
55/160
IDF Diabetes Atlas I Sixth edition I 55
c h a p t e r 3
R E G I O N A L O V E R V I E W S
160
140
120
100
80
60
40
20
0
200 400 600 800 1,000 1,200 1,400 1,600 1,800
N u m b e r o f p e o p l e w i t h d
i a b e t e s ( m i l l i o n s )
Population (millions)
Pacific Region spent only USD 88 billion, despitehaving the
largest number of people with diabetes.The South and Central
America, and Middle Eastand North Africa Regions each dedicated
to
diabetes less than 5% of global diabetes healthexpenditure,
while the South-East Asia and AfricaRegions spent less than 1%.
Health expenditureThe disparities between the Regions can be
seenclearly in healthcare spending on diabetes. TheNorth America
and Caribbean Region spentan estimated USD 263 billion – 48% of
global
health expenditure on diabetes. Europe spentUSD 147 billion. The
spending of each of theseRegions on diabetes healthcare was greater
thanthat of the other Regions combined. The Western
Table 3.0 Regional estimates for diabetes (20-79 years),
2013 and 2035
Figure 3.0 Number of people with diabetes by population
(20-79 years) by IDF Region, 2013
2013 2035 Increasein the
number ofpeople with
diabetes%
IDFREGION
PopulationMILLIONS
Number ofpeople with
diabetesMILLIONS
Comparativediabetes
prevalence%
PopulationMILLIONS
Number ofpeople with
diabetesMILLIONS
Comparativediabetes
prevalence%
AFR 407.9 19.8 5.7 775.5 41.5 6.0 109.6
EUR 658.7 56.3 6.8 668.7 68.9 7.1 22.4
MENA 374.5 34.6 10.9 583.7 67.9 11.3 96.2
NAC 334.9 36.8 9.6 404.5 50.4 9.9 37.3
SACA 300.5 24.1 8.2 394.2 38.5 8.2 59.8
SEA 883.2 72.1 8.7 1,216.9 123.0 9.4 70.6
WP 1,613.2 138.2 8.1 1,818.2 201.8 8.4 46.0
World 4,572.9 381.8 8.3 5,861.8 591.9 8.8 55.0
AFRSACA
MENA
EUR
NAC
Bubble size indicates the projected
increase in the number of people
with diabetes from 2013 to 2035WP
SEA
-
8/20/2019 2013 IDF.pdf
56/160
56 I IDF Diabetes Atlas I Sixth edition
MortalityAlthough only 8.6% of all deaths in the AfricaRegion
can be attributed to diabetes, in 2013 astaggering 76.4% of those
deaths occurred inpeople under the age of 60. Furthermore,
there
were more than 50% more deaths from diabetes inwomen compared to
men. This is in part becausemen are more likely to die from other
causes, suchas armed conflict, and because in many caseswomen have
poor access to healthcare.
Health expenditureAccording to estimates for the Africa Region,
atleast USD 4 billion was spent on diabetes health-care in 2013,
and this spending is expected toincrease around 58% by 2035. In the
same period,the prevalence of diabetes is projected to
almostdouble. With its health expenditure on diabetesthe lowest of
any of the IDF Regions, a two-foldincrease in diabetes prevalence
without a corre-sponding increase in spending will almost
certainlyhave a very negative impact on rates of complica-tions and
death for people with diabetes in Africa.
Data sourcesThe number of data sources examining theprevalence
of diabetes in adults in the Regionhas increased substantially in
recent years. For
this edition of the IDF Diabetes Atlas , 69 sourcesfrom 29
countries were considered, and a totalof 21 sources from 19
countries were selected.How