Embed Size (px)
Citation preview

©2013 MFMER | 3311226-1
Division of GASTROENTEROLOGY& HEPATOLOGY
Use and Misuse of CT and MR Imaging in IBD
David H. Bruining, MDMayo Clinic, Rochester, MN

©2013 MFMER | 3311226-2
Disclosures
Consulting
• Bracco
• Avantis
Research Support
• Janssen Biotech
• Given
• Genentech

©2013 MFMER | 3311226-3
Discussion Points
What is known/standard of care
• Benefits of Imaging
• CTE and MRE performance
Appropriation / inappropriate applications
• How are we doing?
• New developments
©2013 MFMER | 3311226-4
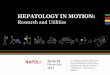
Symptoms Aren’t Enough
Jones et al: Clin Gastroenterol Hepatol, 2008
Correlation coefficients (bolded) were significant; P<0.05; n=164CDAI; Crohn’s disease activity index: SES-CD; simple endoscopic core for Crohn's disease
IL-6 Calprotectin Lactoferrin CDAI SES-CD
Hs-CRP 0.65 0.47 0.52 0.16 0.46
IL-6 0.45 0.55 0.15 0.43
Calprotectin 0.76 0.23 0.45
Lactoferrin 0.19 0.48
CDAI 0.15
©2013 MFMER | 3311226-5
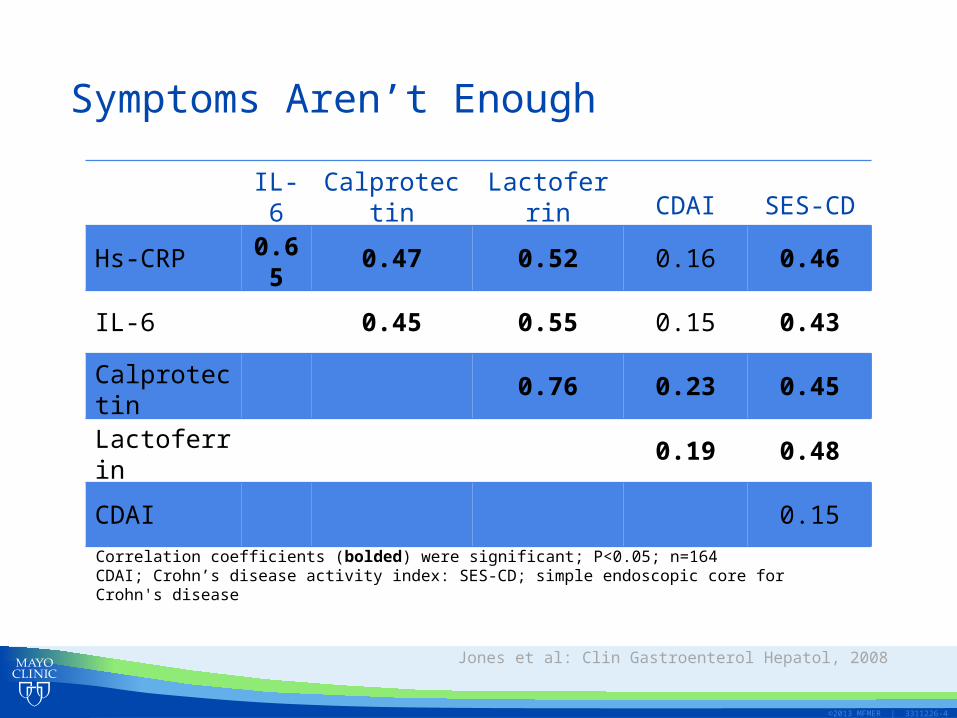
CT and MR EnterographySimilar Performance to CTE for Identifying Active Disease
Siddiki et al: Am J Roentgenol, 2009
CTE MRE

©2013 MFMER | 3311226-6
CT and MR Enterography
Advantages – CTE
• Less interobserver variability
• Higher image quality
• Shorter image acquisition times
• Cost
• Access
• Bone assessments
Advantages – MRE
• No radiation
• Multiple phases
• Detection of fibrosis
• MRI superior for perianal disease
• Pregnancy
• Renal insufficiency

©2013 MFMER | 3311226-7
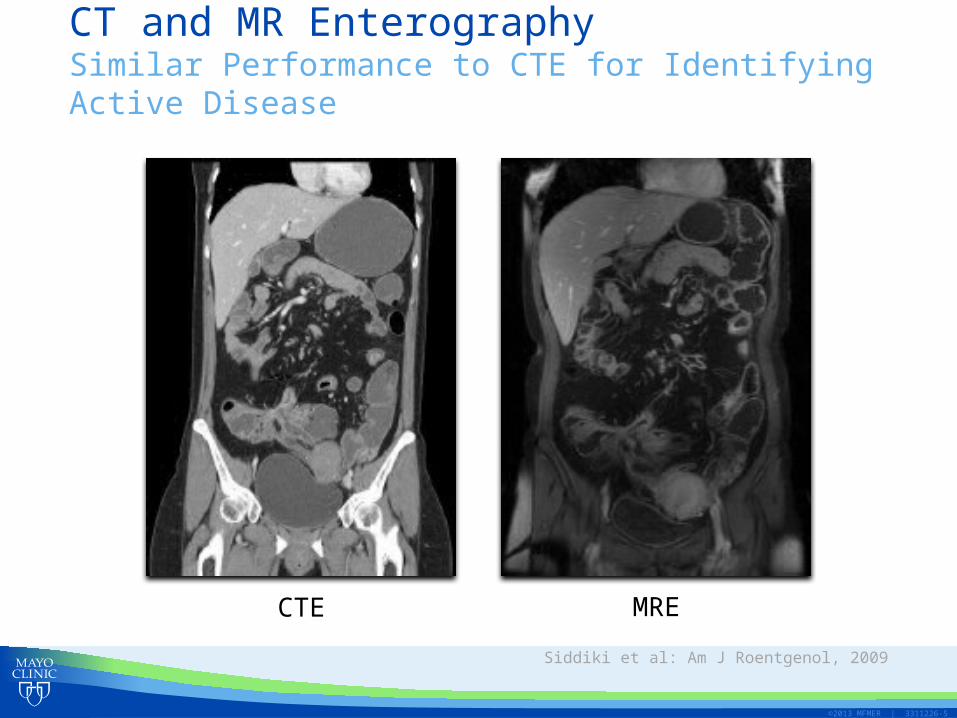
Appropriate UseRight Test for the Right Patient
©2013 MFMER | 3311226-8

©2013 MFMER | 3311226-9
Use of CT and MR Enterography in Crohn’s Disease
Suspected Crohn’s disease
• Establish disease
• Determine optimal strategy for endoscopic confirmation (BAE)
• Define extent and severity
• Exclude alternate etiologies
• Penetrating and stricturing complications
• Extra-intestinal disease manifestation
Established Crohn’s disease
• Response to treatment
• Surgical planning
• Exclude alternate etiologies
• Penetrating and stricturing complications
• Extraintestinal disease manifestation
• Bone health interrogations

©2013 MFMER | 3311226-10
Lesion Remodeling on CTE
*Infliximab initiated in 2004 after examination
6/7/2004* 9/26/2005 6/18/2007

©2013 MFMER | 3311226-11
CTE Generated Finite Element ModelBone Strength
Weber et al: DDW, 2013
Densitydistribution
Regions of failure

©2013 MFMER | 3311226-12
When and How to Image
Suspected disease• Establish diagnosis• Exclude alternate or additional
etiologies for patient symptoms
Established disease• Disease activity• Disease extent• Disease severity• Evaluate for penetrating disease• Surgical planning• Assess response to therapy
MRE• Age <35 years• Serial examinations• Renal disease• Pregnancy• Stricture• Perianal disease
CTE
Postoperative• SBFT (complex)
Occult stricture• Enteroclysis
Other• VCE and ultrasound

©2013 MFMER | 3311226-13
Misuse of CT and MR Enterography
Wrong test
• Multiple CTEs in young patient (MRE)
• MRE in elderly (CTE)
• CTE or MRE for dysplasia (colonoscopy)
• MRE for inpatient with sepsis/SIRS, tremor, obese, diabetics (CTE)
• CTE in patient with renal insufficiency or pregnancy (MRE)
Wrong patient
• Chronic abdominal pain with multiple negative CT or MR examinations
©2013 MFMER | 3311226-14
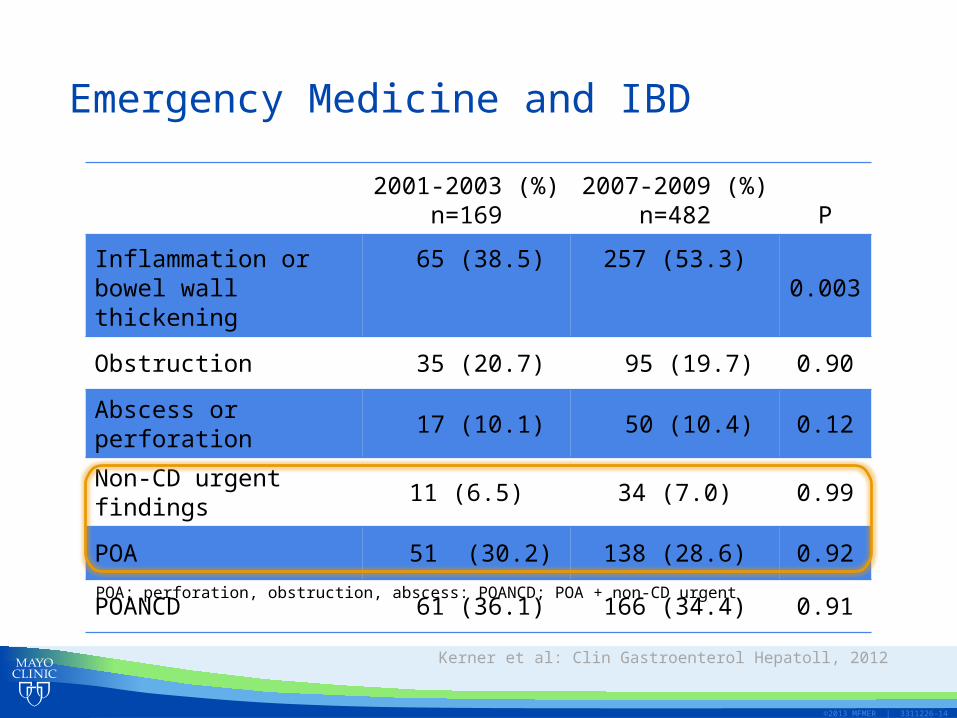
Emergency Medicine and IBD
Kerner et al: Clin Gastroenterol Hepatoll, 2012
2001-2003 (%)n=169
2007-2009 (%)n=482 P
Inflammation or bowel wall thickening
65 (38.5) 257 (53.3) 0.003
Obstruction 35 (20.7) 95 (19.7) 0.90
Abscess or perforation 17 (10.1) 50 (10.4) 0.12
Non-CD urgent findings 11 (6.5) 34 (7.0) 0.99
POA 51 (30.2) 138 (28.6) 0.92
POANCD 61 (36.1) 166 (34.4) 0.91
POA; perforation, obstruction, abscess: POANCD; POA + non-CD urgent

©2013 MFMER | 3311226-15
Can We Do Better?
• Several models in development for ED triage
• APON Risk Score• APON: Abscess, perforation, obstruction, new or
worsening non-CD urgent findings• Final model variables: History of obstruction, history
of intra-abdominal abscess, current hematochezia and WBC >12,000/µL
• Score subtracts 1 for hematochezia and adds 1 point for others
• APON risk score -1 is associated with low risk
Kerner et al: Inflamm Bowel Dis, 2013

©2013 MFMER | 3311226-16
Summary
• Cross-sectional imaging • Objective measure of disease activity• Detects penetrating disease and extraintestinal
manifestations• Alters management plans
• Appropriate use• Applications continue to expand• Key is to match right patient with right exam

©2013 MFMER | 3311226-17
Future Research
• Fine-tuned predictive models – acute presentations• Widely available ED tool• Simple
• Role of ultrasound
• Standardized imaging algorithms, guidelines and reporting lexicon