Embed Size (px)
Citation preview
Page | 1
South East CCAC
Strategy Plan
2014-2017
RFS No.: SECCAC RFS 2-13-1
July 25, 2013
Scarborough Community Health Services Integration
Directional Plan
November 21, 2013
A facilitated integration process of the Central East Local Health Integration Network
Page | 2
BACKGROUND AND CONTEXT
The Central East Local Health Integration Network (LHIN) is one of the fastest growing geographic regions in the Province and covers an area that includes
Scarborough, Durham Region, Northumberland County, Peterborough City and County, City of Kawartha Lakes and Haliburton County. A mix of urban and
rural geography, the Central East LHIN is the sixth-largest LHIN in land area in Ontario (16,673 km2) and includes densely populated urban cities, suburban
towns, rural farm communities, cottage country villages and remote settlements. The neighbourhoods in the LHIN’s planning zones boast a rich diversity of
community values, ethnicity, language and socio-demographic characteristics.
With the second largest population in Ontario, the Central East LHIN is home to 1,572,500 people or 11.8% of the population of Ontario. The Central East LHIN
also has the fourth highest projected growth rate and it is expected that by 2021 the population will have increased by 17.0%, compared to a projected
increase of 13% for Ontario overall. The total population of Scarborough is 594,158 (2011 Census).
Reference Source – Provincial Common Environmental Scan, MOHLTC; HAB Profile Central East LHIN
The Central East LHIN’s Integrated Health Service (IHSP) for 2013-2016 provides the road map for Central East LHIN funded agencies including hospitals, long-
term care homes, community health centres, community mental health and addictions agencies, the Community Care Access Centre and community support
services to follow as they work together to create an integrated community-based health care system that can respond to changing demographics, financial
challenges, updated clinical practice and new technology.
With an overall theme of “Community First – Help Central East LHIN residents spend more time in their homes and their communities”, four strategic aims contained in the IHSP will guide the system over the next three years:
Reduce the demand for long-term care so that seniors spend 320,000 more days at home in their communities by 2016.
Continue to improve the vascular health of residents so they spend 25,000 more days at home in their communities by 2016.
Strengthen the system of supports for people with Mental Health and Addictions issues so they spend 15,000 more days at home in their communities by 2016.
Increase the number of palliative patients who die at home by choice and spend 12,000 more days in their communities by 2016.
Engagement with stakeholders and additional planning documents, available on the Central East LHIN website, validated the LHIN in the development of these
strategic aims.
Page | 3
To further support these “Community First” aims and to provide a seamless continuum of care, ease system navigation, build capacity and leverage existing
strengths within the Community Health Services sector, the Central East LHIN Board passed a motion in 2012 to support a Community Health Services (CHS)
Integration Strategy. This strategy directs Community Health Centres (CHCs) and Community Support Service agencies (CSSs) to design and implement a
cluster-based service delivery model for specified agencies by 2015 through integration of front-line services, back office functions, leadership and/or
governance to concurrently:
improve client access to high-quality services: Access to consistent and integrated basket of services will improve client and caregiver
experience and outcomes.
create readiness for future health system transformation: Create critical mass in governance, management, delivery and IT capacity to enable
future growth in community support services.
make the best use of the public’s investment: Create opportunities through efficiencies to re-invest in direct client services and reduce latent risk within the sector that jeopardizes quality and access to client service
In launching the strategy, the LHIN identified a number of Group 1 agencies that would be directed to participate in the facilitated integration process in each
of the clusters. Group 1 agencies included those single or multi-service health service providers (HSPs) who provided services within a clearly defined region
within the Central East LHIN (including LHIN services provided through municipalities.) The integration planning began with this group, and other specifically
identified agencies, based on the LHIN’s determination that integration would most likely achieve the greatest return on investment.
Agencies that were categorized as Group 2 (HSPs with broader affiliations – cross LHIN, provincial, national) and Group 3 (serving multiple LHIN clusters or a
specific client population) were to be included in later phases of the strategy although they could request to be included in the early timing. The Central East
Community Care Access Centre, which has a single governance structure for the Central East region, was not included in the CHS Integration Strategy.
The process was initiated in the Durham Cluster in April 2012 and is being rolled out across all three clusters with an anticipated completion date of March
2015.
Adjustments to CHS Integration Strategy phasing in the Scarborough and Northeast Clusters were required to support the alignment with provincial priorities
including Health Links and the Small Rural and Northern Hospital Transformation fund implementation in the Northumberland, City of Kawartha Lakes and
Haliburton communities.
The current phase of the CHS Integration Strategy in Scarborough involves the following five organizations that are single or multi-service health service
providers that provide services within Scarborough: TAIBU Community Health Centre, Scarborough Centre for Healthy Communities, St. Paul's L'Amoreaux
Centre, TransCare Community Support Services, and the Centre for Immigrant and Community Services.
Page | 4
These organizations formed the Scarborough Integration Planning Team in the fall of 2013, and have reviewed and approved a Terms of Reference to guide
their activities. The Board of Governors of each of the Health Service Providers (HSP) involved in the Scarborough CHS Integration Planning Team have also
signed off on a set of Guiding Principles that establish a set of foundational principles to guide discussions and actions. The Guiding Principles articulates the
Legislative due diligence required of all HSPs and the LHIN.
At the Central East LHIN, integration is achieved through the application of the Local Health System Integration Act. Examples of previous integrations in the
Central East LHIN can be found at http://www.centraleastlhin.on.ca/Page.aspx?id=96&ekmensel=e2f22c9a_72_206_96_3
Legislative Due Diligence
Under legislation (LHSIA), the LHIN, the Minister of Health and Long-Term Care and health service providers themselves can integrate in several ways.
1. Coordinate services and interactions between different persons and entities
2. Partner with another person or entity in providing services or in operating
3. Transfer, merge or amalgamate services, operations, persons or entities
4. Start or cease providing services
5. Cease to operate or dissolve or wind up the operations of a person or entity
It is important to note that the LHIN does not have the authority to integrate by “Ceasing to operate or to dissolve or wind up the operations of a person or
entity” (#5). This authority is reserved for the Minister of Health and Long-Term Care and/or voluntarily by the persons/entities involved. In other words, aside
from the Minister, only HSPs can decide to dissolve their own corporate entity.
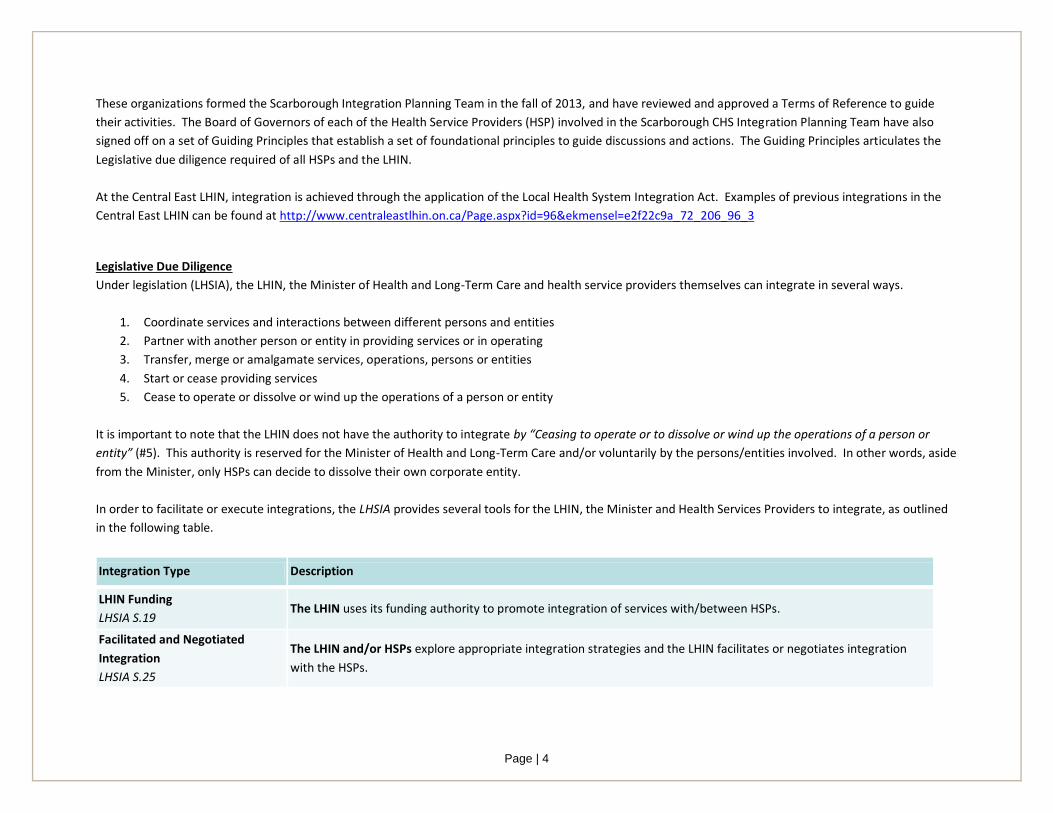
In order to facilitate or execute integrations, the LHSIA provides several tools for the LHIN, the Minister and Health Services Providers to integrate, as outlined
in the following table.
Integration Type Description
LHIN Funding
LHSIA S.19 The LHIN uses its funding authority to promote integration of services with/between HSPs.
Facilitated and Negotiated
Integration
LHSIA S.25
The LHIN and/or HSPs explore appropriate integration strategies and the LHIN facilitates or negotiates integration
with the HSPs.
Page | 5
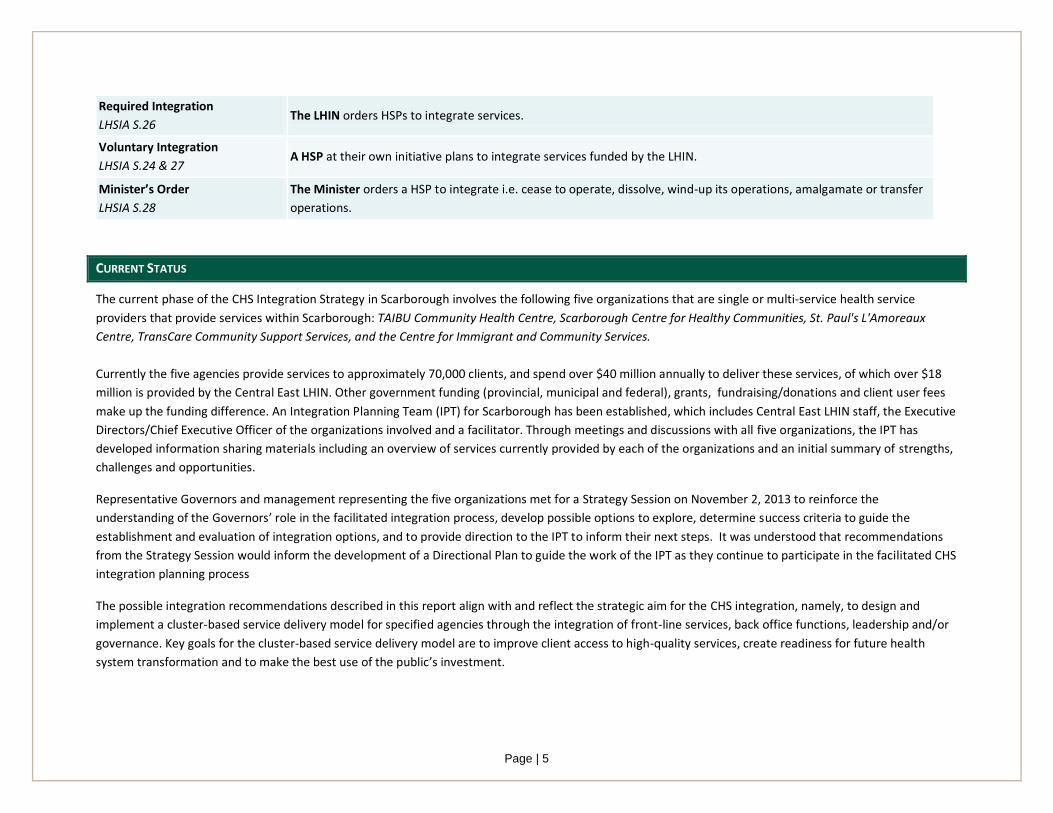
Required Integration
LHSIA S.26 The LHIN orders HSPs to integrate services.
Voluntary Integration
LHSIA S.24 & 27 A HSP at their own initiative plans to integrate services funded by the LHIN.
Minister’s Order
LHSIA S.28
The Minister orders a HSP to integrate i.e. cease to operate, dissolve, wind-up its operations, amalgamate or transfer
operations.
CURRENT STATUS
The current phase of the CHS Integration Strategy in Scarborough involves the following five organizations that are single or multi-service health service
providers that provide services within Scarborough: TAIBU Community Health Centre, Scarborough Centre for Healthy Communities, St. Paul's L'Amoreaux
Centre, TransCare Community Support Services, and the Centre for Immigrant and Community Services.
Currently the five agencies provide services to approximately 70,000 clients, and spend over $40 million annually to deliver these services, of which over $18
million is provided by the Central East LHIN. Other government funding (provincial, municipal and federal), grants, fundraising/donations and client user fees
make up the funding difference. An Integration Planning Team (IPT) for Scarborough has been established, which includes Central East LHIN staff, the Executive
Directors/Chief Executive Officer of the organizations involved and a facilitator. Through meetings and discussions with all five organizations, the IPT has
developed information sharing materials including an overview of services currently provided by each of the organizations and an initial summary of strengths,
challenges and opportunities.
Representative Governors and management representing the five organizations met for a Strategy Session on November 2, 2013 to reinforce the
understanding of the Governors’ role in the facilitated integration process, develop possible options to explore, determine success criteria to guide the
establishment and evaluation of integration options, and to provide direction to the IPT to inform their next steps. It was understood that recommendations
from the Strategy Session would inform the development of a Directional Plan to guide the work of the IPT as they continue to participate in the facilitated CHS
integration planning process
The possible integration recommendations described in this report align with and reflect the strategic aim for the CHS integration, namely, to design and
implement a cluster-based service delivery model for specified agencies through the integration of front-line services, back office functions, leadership and/or
governance. Key goals for the cluster-based service delivery model are to improve client access to high-quality services, create readiness for future health
system transformation and to make the best use of the public’s investment.
Page | 6
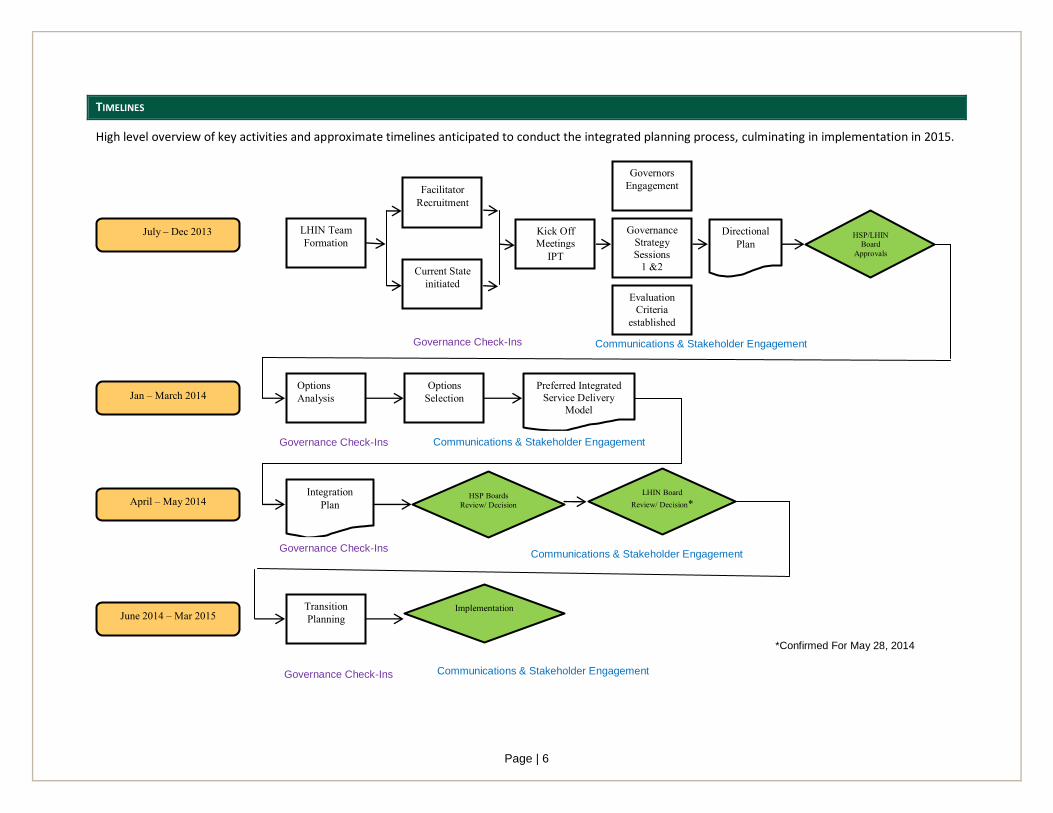
TIMELINES
High level overview of key activities and approximate timelines anticipated to conduct the integrated planning process, culminating in implementation in 2015.
Facilitator
Recruitment
Communications & Stakeholder Engagement
Evaluation
Criteria
established
Governors
Engagement
Current State
initiated
LHIN Team
Formation Kick Off
Meetings
IPT
Governance
Strategy
Sessions 1 &2
July – Dec 2013 Directional Plan
Transition
Planning June 2014 – Mar 2015 Implementation
Communications & Stakeholder Engagement
Options
Analysis Options
Selection Jan – March 2014 Preferred Integrated
Service Delivery
Model
Communications & Stakeholder Engagement Governance Check-Ins
April – May 2014 HSP Boards
Review/ Decision LHIN Board
Review/ Decision* Integration
Plan
Communications & Stakeholder Engagement Governance Check-Ins
Governance Check-Ins
Governance Check-Ins
HSP/LHIN Board
Approvals
*Confirmed For May 28, 2014
Page | 7
SUMMARY OF GOVERNORS STRATEGY SESSIONS DISCUSSION
Representative Governors and management from the five Phase 1 Scarborough organizations participated in a facilitated Strategy Session in Scarborough (November 2, 2013). The five organizations were St. Paul’s L’Amoreaux Centre, TransCare Community Support Services, TAIBU Community Health Centre, Scarborough Centre for Healthy Communities, and the Centre for Immigrant and Community Services. The objectives for the session were as follows:
Build commitment of Governors to pursue integration;
Reinforce understanding Governors’ role in setting collaborative strategic possibilities for the CHS Integration;
Review current state of services and integration opportunities;
Develop strategic possibilities as options to explore;
Determine success criteria to guide the establishment and evaluation of integration models; and
Provide direction to the IPT to support their work on the Scarborough CHS initiative.
In advance of the Strategy Session, the attendees were provided with relevant background materials prepared by the Scarborough IPT, including a Community
Health Services Summary Matrix, Current State Programs Matrix, Current State Community Health Services Bubble Diagram, Insights into the Five
Organizations, and a summary of Strengths, Challenges, Trends and Issues.
The Strategy Session began with an overview of the following: objectives for the session, role of governors, and the integration goals and planning process. A
current state summary of integration opportunities and concerns, as extracted from the background materials, was presented, and tied back to the integration
goals of improving client access to high-quality services, creating readiness for future health system transformation and making the best use of the public’s
investment.
The approach for the Session was explained and the participants formed groups that consisted of representatives from all five Phase 1 Scarborough
organizations (where possible) and which were a mix of governors and management. The groups were asked to brainstorm potential options for integration
while considering how the option adds value for the client, to consider how the proposed option is different from – or similar to - the current state, and to
describe whether the nature of the proposed integration is best described as integration related to governance, service delivery or back office. Each group
reported back to the whole group, and from this report back five options emerged. The options included:
Improved sharing of current and best practices
Client service intake/referral process
Client services integration
Back office integration
Reducing the number of LHIN-funded organizations
Page | 8
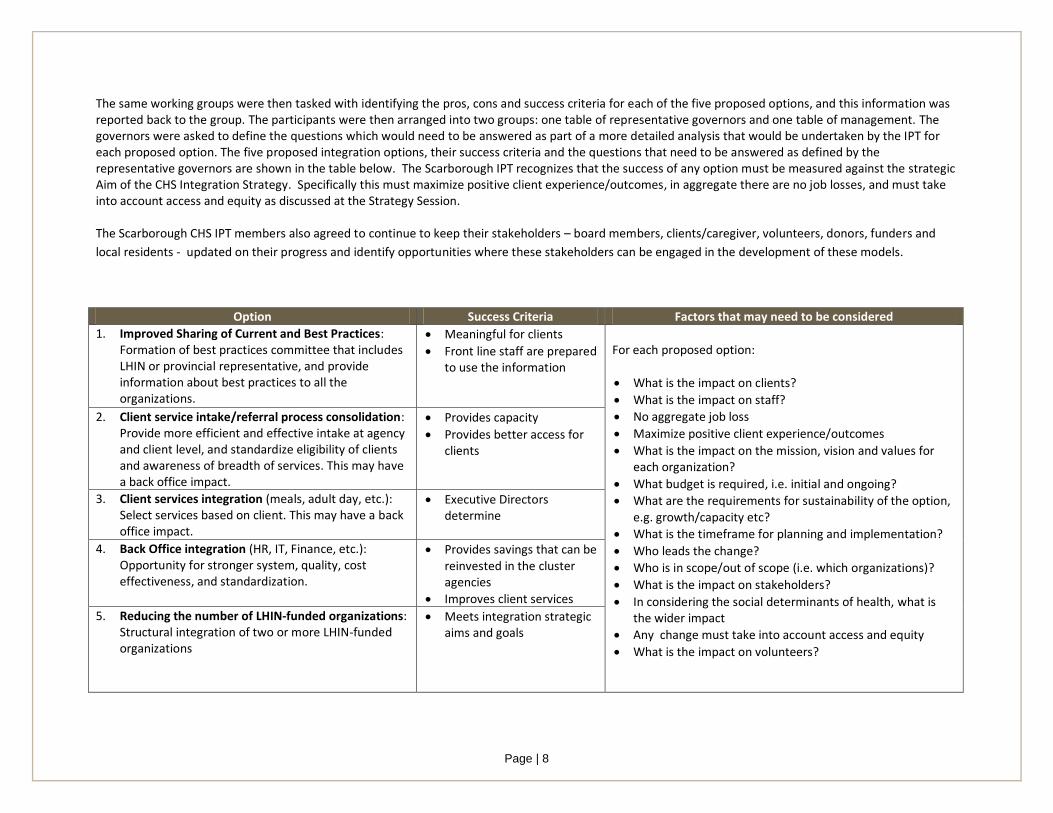
The same working groups were then tasked with identifying the pros, cons and success criteria for each of the five proposed options, and this information was reported back to the group. The participants were then arranged into two groups: one table of representative governors and one table of management. The governors were asked to define the questions which would need to be answered as part of a more detailed analysis that would be undertaken by the IPT for each proposed option. The five proposed integration options, their success criteria and the questions that need to be answered as defined by the representative governors are shown in the table below. The Scarborough IPT recognizes that the success of any option must be measured against the strategic Aim of the CHS Integration Strategy. Specifically this must maximize positive client experience/outcomes, in aggregate there are no job losses, and must take into account access and equity as discussed at the Strategy Session. The Scarborough CHS IPT members also agreed to continue to keep their stakeholders – board members, clients/caregiver, volunteers, donors, funders and
local residents - updated on their progress and identify opportunities where these stakeholders can be engaged in the development of these models.
Option Success Criteria Factors that may need to be considered
1. Improved Sharing of Current and Best Practices: Formation of best practices committee that includes LHIN or provincial representative, and provide information about best practices to all the organizations.
Meaningful for clients
Front line staff are prepared to use the information
For each proposed option:
What is the impact on clients?
What is the impact on staff?
No aggregate job loss
Maximize positive client experience/outcomes
What is the impact on the mission, vision and values for each organization?
What budget is required, i.e. initial and ongoing?
What are the requirements for sustainability of the option, e.g. growth/capacity etc?
What is the timeframe for planning and implementation?
Who leads the change?
Who is in scope/out of scope (i.e. which organizations)?
What is the impact on stakeholders?
In considering the social determinants of health, what is the wider impact
Any change must take into account access and equity
What is the impact on volunteers?
2. Client service intake/referral process consolidation: Provide more efficient and effective intake at agency and client level, and standardize eligibility of clients and awareness of breadth of services. This may have a back office impact.
Provides capacity
Provides better access for clients
3. Client services integration (meals, adult day, etc.): Select services based on client. This may have a back office impact.
Executive Directors determine
4. Back Office integration (HR, IT, Finance, etc.): Opportunity for stronger system, quality, cost effectiveness, and standardization.
Provides savings that can be reinvested in the cluster agencies
Improves client services
5. Reducing the number of LHIN-funded organizations: Structural integration of two or more LHIN-funded organizations
Meets integration strategic aims and goals
Page | 9
The participants’ reported that the session was a valuable and important first step in building mutual relationships and an understanding of the services
delivered by each the organizations. There was also a perspective that while there is support for collaboration amongst this group of agencies, there are other
stakeholders who should join the discussion.
In general, it was a difficult exercise with participant uncertainty regarding the expectations and outcomes for the sessions; despite this, the working groups
made good progress in discussion of the five proposed options. There was a sense of hesitation amongst the governors regarding the fifth option (reducing the
number of LHIN-funded organizations), from a feasibility perspective in terms of timing. There was also uncertainty as to whether reducing the number of
organizations will actually meet the three goals/outcomes for integration: to improve client access to high-quality services, to create readiness for future
health system transformation and to make the best use of the public’s investment. There was a higher level of comfort for the first four options described
above (improved sharing of current and best practices, client service intake/referral process consolidation, client services integration and back office
integration), with the view that these approaches could allow the organizations time to get to know each other, and to work towards greater definition of what
an integrated entity or more integrated service delivery would look like.
There was also interest in working collaboratively to explore opportunities for client service improvements, which when established would also create
efficiencies for the agencies. An example is establishing a common client intake process across the organizations, i.e., service integration without structural
integration of the agencies.
In addition, there is a desire to continue to build on the momentum that has been created through providing opportunities for further discussions with this
group, including learning about previous Central East LHIN integrations and related best practices in order to support the governors to make strategic decisions
on integration of CHS for the Phase 1 Scarborough organizations.
Based on the outcome of the Strategy Sessions, recommended next steps are to conduct analysis on the above five options. The analysis should include
consideration of the success criteria and answer the questions posed for each option. This analysis will generate the information required to have a more
fulsome and detailed discussion on what is possible in Scarborough now and in the future.
Page | 10
SUMMARY
Desired Outcome for CHS Integration
The strategic aim of the Central East LHIN for the Community Health Services (CHS) integration strategy is to design and implement a cluster-based service
delivery model for specified agencies by 2015 through integration of front-line services, back office functions, leadership and/or governance, that concurrently:
• improves client access to high-quality services,
• creates readiness for future health system transformation
• makes the best use of the public’s investment Given the CHS strategic aim, and based on direction received from representative governors from the five Phase 1 Scarborough organizations, five potential options are proposed for further consideration and analysis. The Scarborough IPT will continue to develop evaluation criteria in addition to the success criteria factors suggested at the facilitated strategy session.
The five potential options proposed for further review and analysis by the Scarborough IPT are:
1. Improved Sharing of Current and Best Practices
2. Client service intake/referral process consolidation
3. Client services integration
4. Back Office integration
5. Reducing the number of LHIN-funded organizations