Embed Size (px)
Citation preview
2016 GPRO Readiness2016 GPRO RANDOM SAMPLE REPORTING
January 17, 2017 to March 17, 2017
112/2/2016
GPRO Readiness AgendaWhat Quality Measures?
Projected Reporting Timeline
EIDM Access (GPRO WI)
2016 QM Import Chart
Data Imports
Patient Assignment
GPRO 2016 – How to Use Interface?
QM Performance Scoring
QM Total Score
Email Distribution
QM Priority Matrix
Single File
Spec File
212/2/2016

What Quality Measures?2016 GPRO RANDOM SAMPLE REPORTING
312/2/2016

18 GPRO Quality Measures
1. ACO-13 (CARE-2) Falls: Screening for Future Fall Risk
2. ACO-39 (CARE-3) Documentation of Current Medications in the Medical Record
3. ACO-14 (PREV-7) Preventive Care and Screening: Influenza Immunization
4. ACO-15 (PREV-8) Pneumonia Vaccination Status for Older Adults
5. ACO-16 (PREV-9) Preventive Care and Screening: Body Mass Index Screening and Follow-up
6. ACO-17 (PREV-10) Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
7. ACO-18 (PREV-12) Preventive Care and Screening: Clinical Depression and Follow-up Plan
8. ACO-19 (PREV-6) Colorectal Cancer Screening
9. ACO-20 (PREV-5) Breast Cancer Screening
412/2/2016
18 GPRO Quality Measures
10. ACO-21 (PREV-11) Preventive Care and Screening; Screening for High Blood Pressure and Follow-up Documented
11. ACO-42 (PREV-13) Statin Therapy for the Prevention and Treatment of Cardiovascular Disease
12. ACO-40 (MH-1) Depression Remission at 12 Months
13. ACO-27 (DM-2) Diabetes: Hemoglobin A1c Poor Control
14. ACO-41 (DM-7) Diabetes: Eye Exam
15. ACO-28 (HTN-2) Controlling High Blood Pressure
16. ACO-30 (IVD-2) Ischemic Vascular Disease: Use of Aspirin of Another Antithrombotic
17. ACO-31 (HF-6) Heart Failure: Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction
18. ACO-33 (CAD-7) Coronary Artery Disease: Angiotensin Receptor Blocker Therapy – Diabetes or Left Ventricular Systolic Dysfunction (LVEF < 40%)
512/2/2016
GPRO Web Interface: Measure Changes from PY2015 to PY2016
6
ACO-16 (PREV-9) – BMI Screening and Follow-up Plan
– Medical and patient reason exceptions are now denominator
exclusions (i.e., these patients are now removed from the
denominator up front)
ACO-19 (PREV-6) – Colorectal Cancer Screening
– Documentation of both the results of the colorectal cancer
screening and the date of the screening are required.
– FIT-DNA screening (e.g., ColoGuard) will be considered numerator
compliant
– CT Colonography (i.e., virtual colonoscopy) screening will also be
considered numerator compliant.
GPRO Web Interface: Measure Changes from PY2015 to PY2016
7
ACO-20 (PREV-5) – Breast Cancer Screening
– 3D mammogram will not be considered numerator compliant. If the beneficiary receives a 3D mammography, submit a ticket for an “Other CMS approved reason.”
ACO-21 (PREV-11) – Screening for High Blood Pressure and Follow-up Documented
– Patient reason exception is now allowed with respect to the follow-up plan.
ACO-31 & 33 (HF-6 and CAD-7) – Beta Blocker Therapy for LVSD and ACE Inhibitor or ARB Therapy: Diabetes and LVSD
– List of synonyms for “moderate” and “severe” with respect to LVSD no longer applicable.
– Measure only allows the words “moderate” or “severe” to describe LVSD.
GPRO Web Interface: New Measure in PY2016
8
ACO-42 (PREV-13) Statin Therapy for the Prevention and Treatment
of Cardiovascular Disease

Projected Timeline2016 GPRO RANDOM SAMPLE REPORTING
912/2/2016
10
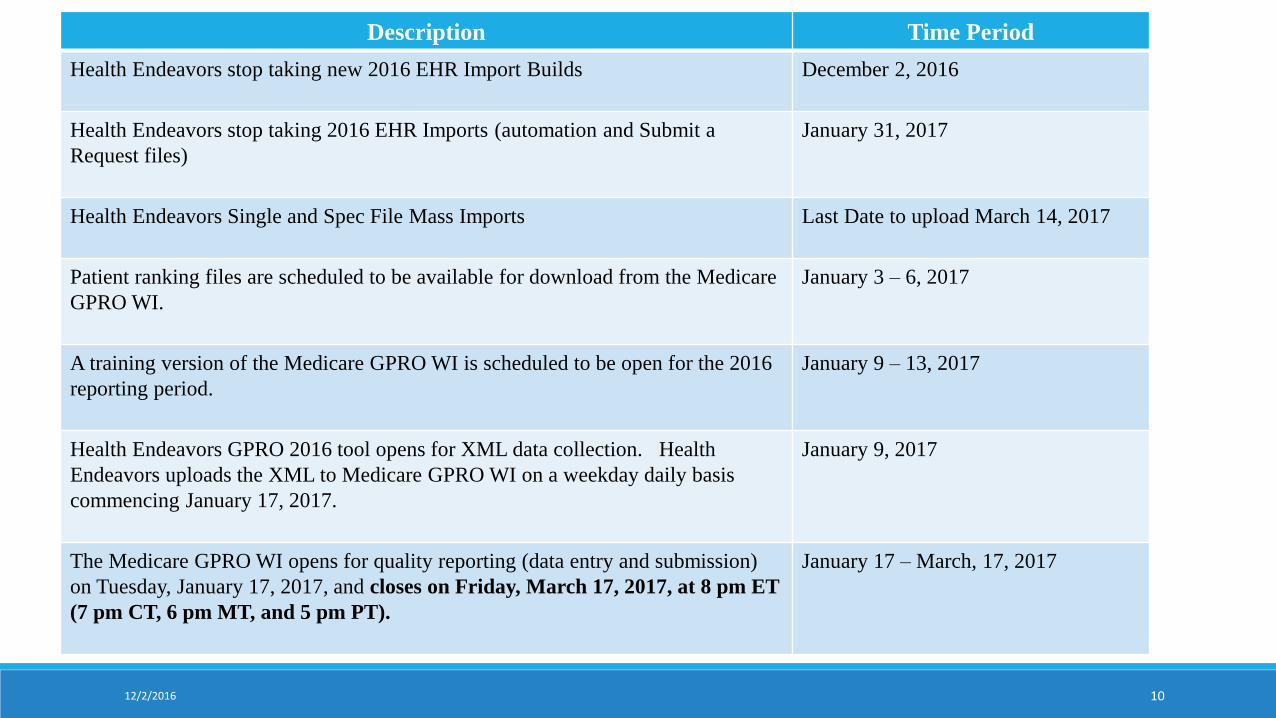
Description Time Period
Health Endeavors stop taking new 2016 EHR Import Builds December 2, 2016
Health Endeavors stop taking 2016 EHR Imports (automation and Submit a
Request files)
January 31, 2017
Health Endeavors Single and Spec File Mass Imports Last Date to upload March 14, 2017
Patient ranking files are scheduled to be available for download from the Medicare
GPRO WI.
January 3 – 6, 2017
A training version of the Medicare GPRO WI is scheduled to be open for the 2016
reporting period.
January 9 – 13, 2017
Health Endeavors GPRO 2016 tool opens for XML data collection. Health
Endeavors uploads the XML to Medicare GPRO WI on a weekday daily basis
commencing January 17, 2017.
January 9, 2017
The Medicare GPRO WI opens for quality reporting (data entry and submission)
on Tuesday, January 17, 2017, and closes on Friday, March 17, 2017, at 8 pm ET
(7 pm CT, 6 pm MT, and 5 pm PT).
January 17 – March, 17, 2017
12/2/2016
GPRO Web Interface Reporting Requirements
11
The 18 GPRO Web Interface measures are associated with 8
disease modules or patient care measures.
The 18 disease module or patient care measures in the GPRO Web
Interface are pre-filled with 17 beneficiary samples for each ACO.
For each beneficiary sample, the ACO is required to consecutively
confirm and complete 248 beneficiaries, or 100% of their sampled
beneficiaries if < 248 are available.
GPRO Web Interface Sampling: Selecting the Sample
12
Each measure will have its own beneficiary sample. In other words,
each ACO will have 16 samples of 616 beneficiaries, and one sample
of 750 beneficiaries (for the statin therapy measure).
The beneficiary’s place in the sample (e.g., 1, 2, 3, etc.) is referred to
as the beneficiary’s rank.
Each ACO is required to confirm and complete data entry on 248
consecutive beneficiaries for each measure.
2016 GPRO Web Interface Sampling Methodology:
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS/downloads/2016_WebInterface_Sampling-.pdf
GPRO Web Interface Reporting
13
Prior to the opening of the GPRO Web Interface submission period,
ACOs will be able to access their Patient Ranking file which includes:
– The ACO’s beneficiary samples for each module/measure,
– Each beneficiary’s rank order number in each module/measure,
– The TIN or CCN at which the patient received the most care, and
– 3 NPIs from whom the beneficiary received the most care.
This file will be provided both as a download from the GPRO Web
Interface, and as an Excel file.
GPRO Web Interface Sampling: FAQs
14
Q: Why are there so many beneficiaries in each sample (an
oversample) if we only need to report on 248?
– A: CMS provides an oversample for each measure in case medical record
data indicate some beneficiaries are not appropriate for the sample. An
oversample allows those beneficiaries to be skipped and replaced with
another sampled beneficiary, so the 248 beneficiary requirement can still
be reached.
Q: What if my ACO doesn’t have enough beneficiaries for a
complete sample of 616, or 750?
– A: Some ACOs may not have 616 (or 750) eligible beneficiaries for some
measures. In those cases CMS provides all the eligible beneficiaries that
are available. Similarly, if you do not have 248 beneficiaries to report on,
you must report on all the eligible beneficiaries that are available to your
ACO.
GPRO Web Interface Sampling: FAQs
15
Q: Will my ACO really have 10,606 beneficiaries in its sample
(616 beneficiaries for 16 measures, plus 750 beneficiaries for the
statin therapy measure)?
– A: No. In order to minimize the resource burden on practices, CMS
samples in a way that maximizes beneficiary overlap between each
measure’s sample. This means a single beneficiary may be sampled for
multiple measures. To the extent possible, for a single beneficiary that is
sampled into more than one measure, CMS assigns a similar rank to the
beneficiary in each of those measures.
GPRO Web Interface: Skip Reasons
16
A beneficiary is removed from all measures and performance
calculations if these skip reasons are chosen:
– Not Qualified for Sample
– Medical Record Not Found
GPRO Web Interface: Skip Reasons
17
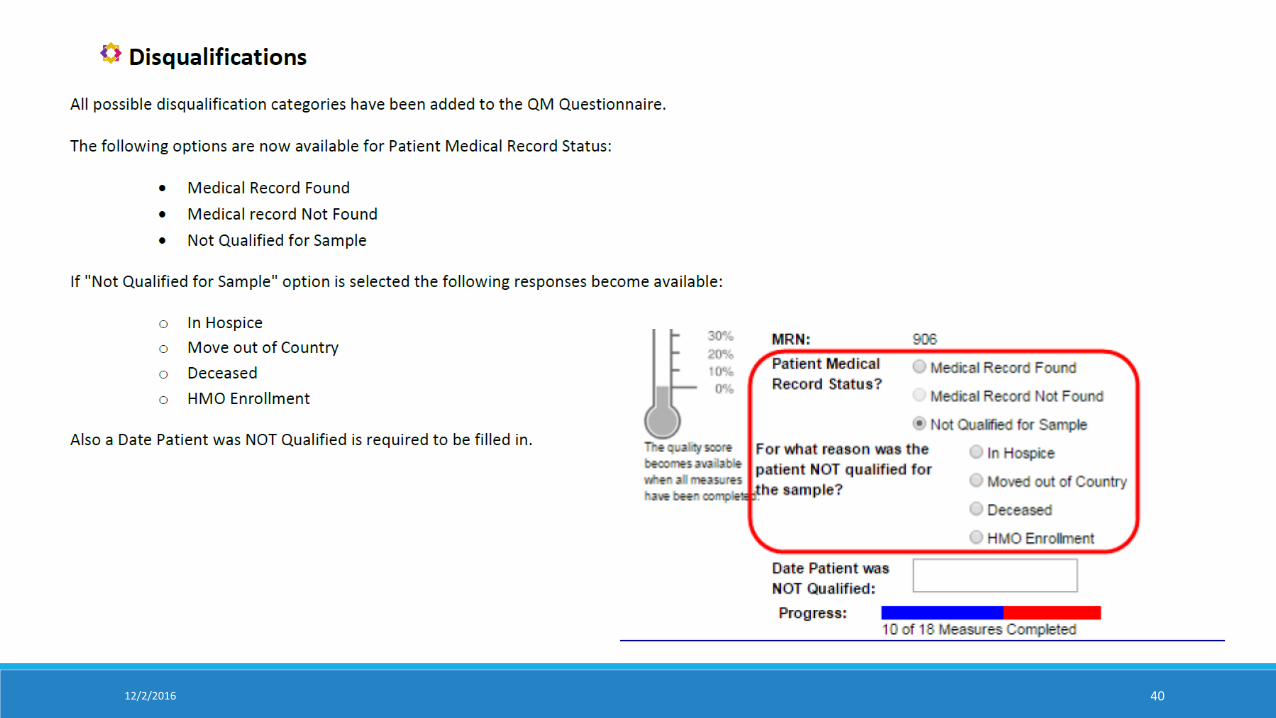
Not Qualified for Sample
– Beneficiary was in hospice during the performance year
– Beneficiary moved out of the country during the performance year
– Beneficiary died during the performance year
– Beneficiary was enrolled in an HMO during the performance year
GPRO Web Interface: Skip Reasons, cont’d
18
Medical Record Not Found (MRNF)
– It is expected that the ACO make every effort to locate/obtain
access to the medical record and that the providers within the ACO
share the necessary records/data for the purposes of coordinating
care and reporting quality measure information
– Elevated rates of selecting MRNF is a factor considered for
inclusion in the Quality Measures Validation Audit
GPRO Web Interface: Skip Reasons, cont’d
19
A beneficiary is removed from a specific measure (Skip):
Diagnosis could not be confirmed
Denominator inclusion criteria are not met (age, gender)
Denominator exclusion criteria are met
Other CMS approved reason requested
– Must obtain CMS approval before selecting Other CMS approved
reason
– Email the QualityNet Help Desk ([email protected]) to work
with CMS for approval
Include the beneficiary rank, measure, and reason for request
Maintain the approved Help Desk ticket number for entry in the GPRO
Web Interface
EIDM Web Interface Role2016 GPRO RANDOM SAMPLE REPORTING
2012/2/2016
EIDM Web Interface RoleInformation needed by Health Endeavors:◦ Security Official Name◦ Security Official Email◦ Security Official Phone
Confirm with Jeffrey Snowden at [email protected] all Web Interface Submitter roles have been processed by December 16, 2016 or the reason for failure to process. If not processed Health Endeavors will not be able to submit on your behalf.
Web Interface Submitter Roles – Mandatory Setup*
Caroline Wise*Jeffrey Snowden*Vidal IseghohimenKris Gates
2112/2/2016
22
NEW Enterprise Identity Management (EIDM) for ACOs User’s Tip ACOs in the Shared Savings Program reporting quality measures for performance year 2016 must have
the necessary Enterprise Identity Management (EIDM) accounts and roles to access the CMS Group
Practice Reporting Option Web Interface (GPRO WI).
The 2016 Quality Reporting Guide: EIDM Account and Role Set-up guidance document is available on the
SSP ACO Portal under the Announcement, 2016 Quality Measurement and Reporting Guides.
This guide provides instructions for setting up your EIDM account and checking your EIDM roles.
If you need assistance with your EIDM account please contact the QualityNet helpdesk at
12/2/2016
2312/2/2016
2412/2/2016
2512/2/2016
QM 2016 Import Chart2016 GPRO RANDOM SAMPLE REPORTING
2612/2/2016
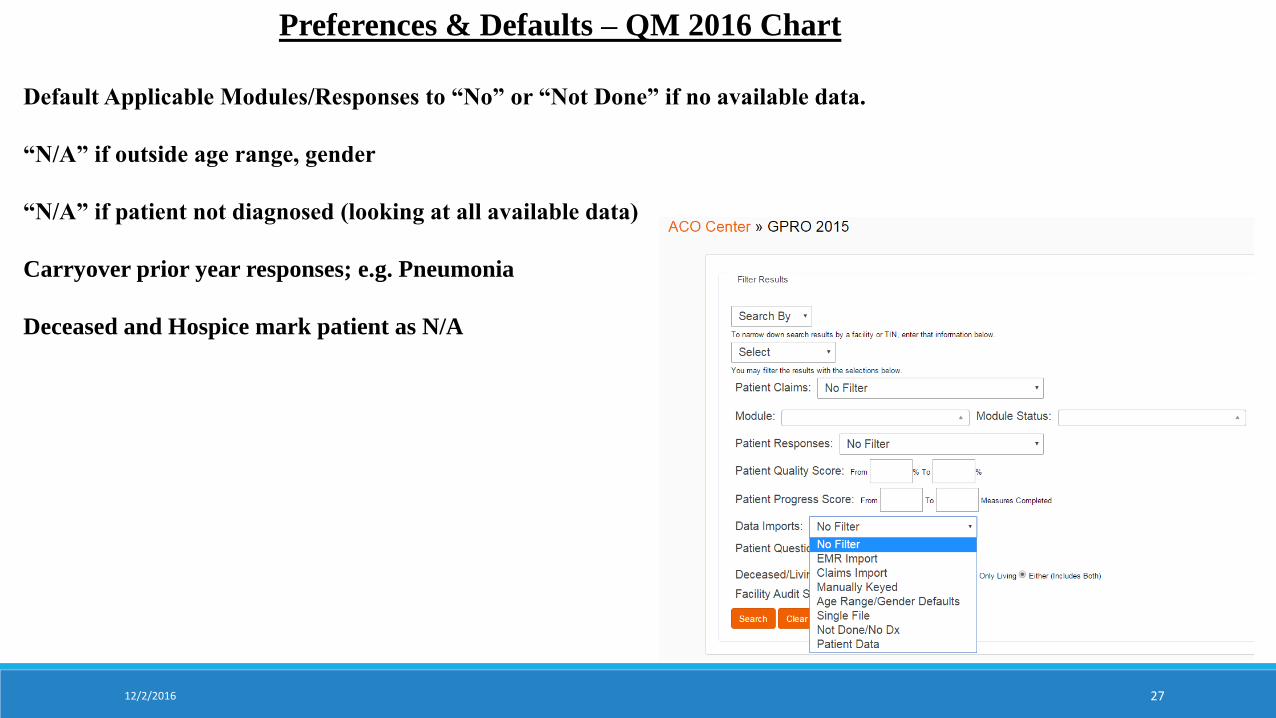
Preferences & Defaults – QM 2016 Chart
Default Applicable Modules/Responses to “No” or “Not Done” if no available data.
“N/A” if outside age range, gender
“N/A” if patient not diagnosed (looking at all available data)
Carryover prior year responses; e.g. Pneumonia
Deceased and Hospice mark patient as N/A
12/2/2016 27
28
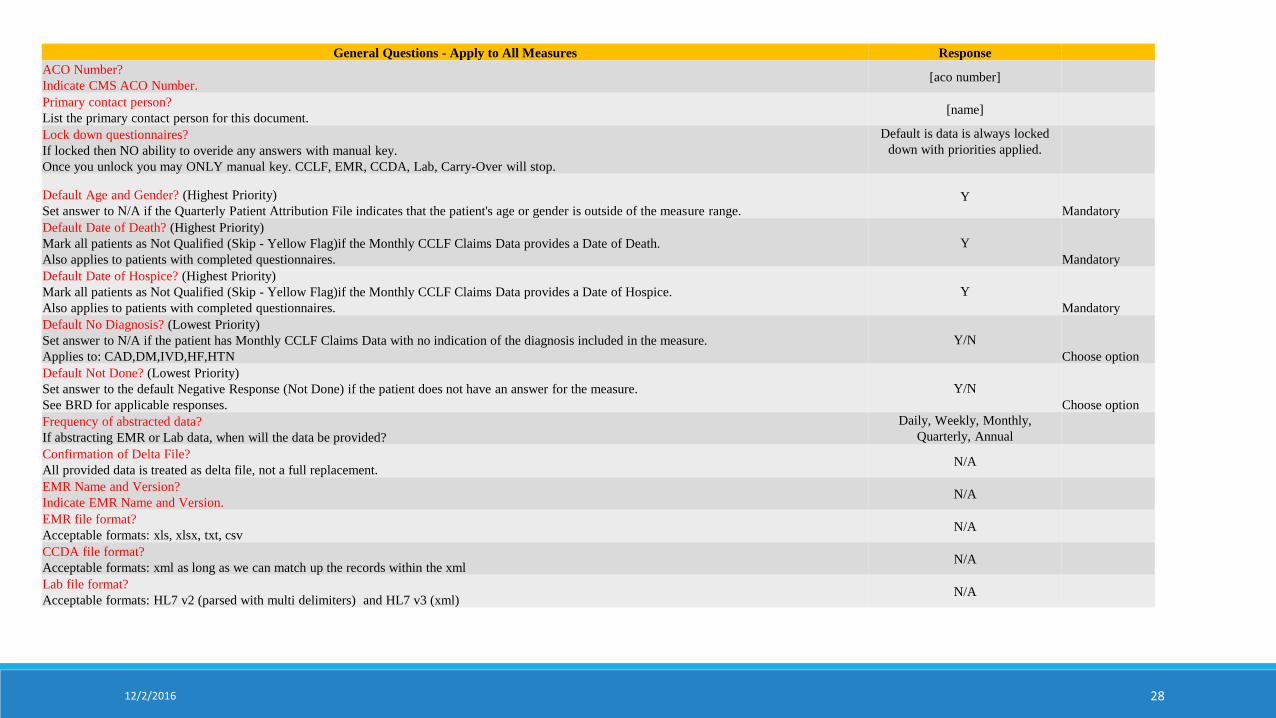
General Questions - Apply to All Measures Response
ACO Number?
Indicate CMS ACO Number.[aco number]
Primary contact person?
List the primary contact person for this document.[name]
Lock down questionnaires?
If locked then NO ability to overide any answers with manual key.
Once you unlock you may ONLY manual key. CCLF, EMR, CCDA, Lab, Carry-Over will stop.
Default is data is always locked
down with priorities applied.
Default Age and Gender? (Highest Priority)
Set answer to N/A if the Quarterly Patient Attribution File indicates that the patient's age or gender is outside of the measure range.Y
Mandatory
Default Date of Death? (Highest Priority)
Mark all patients as Not Qualified (Skip - Yellow Flag)if the Monthly CCLF Claims Data provides a Date of Death.
Also applies to patients with completed questionnaires.
Y
Mandatory
Default Date of Hospice? (Highest Priority)
Mark all patients as Not Qualified (Skip - Yellow Flag)if the Monthly CCLF Claims Data provides a Date of Hospice.
Also applies to patients with completed questionnaires.
Y
Mandatory
Default No Diagnosis? (Lowest Priority)
Set answer to N/A if the patient has Monthly CCLF Claims Data with no indication of the diagnosis included in the measure.
Applies to: CAD,DM,IVD,HF,HTN
Y/N
Choose option
Default Not Done? (Lowest Priority)
Set answer to the default Negative Response (Not Done) if the patient does not have an answer for the measure.
See BRD for applicable responses.
Y/N
Choose option
Frequency of abstracted data?
If abstracting EMR or Lab data, when will the data be provided?
Daily, Weekly, Monthly,
Quarterly, Annual
Confirmation of Delta File?
All provided data is treated as delta file, not a full replacement.N/A
EMR Name and Version?
Indicate EMR Name and Version.N/A
EMR file format?
Acceptable formats: xls, xlsx, txt, csvN/A
CCDA file format?
Acceptable formats: xml as long as we can match up the records within the xmlN/A
Lab file format?
Acceptable formats: HL7 v2 (parsed with multi delimiters) and HL7 v3 (xml)N/A
12/2/2016
Data Imports2016 GPRO RANDOM SAMPLE REPORTING
2912/2/2016
Data Imports – QM 2016 Chart ReviewCCLF (claims) Monthly Imports
EHR Builds (Custom or EMR BRD)
◦xls, xlsx, txt, csv
◦XML
◦CCDA
Health Endeavors Single File Upload Tool
Health Endeavors Spec File Upload Tool
Manual Key
3012/2/2016
31
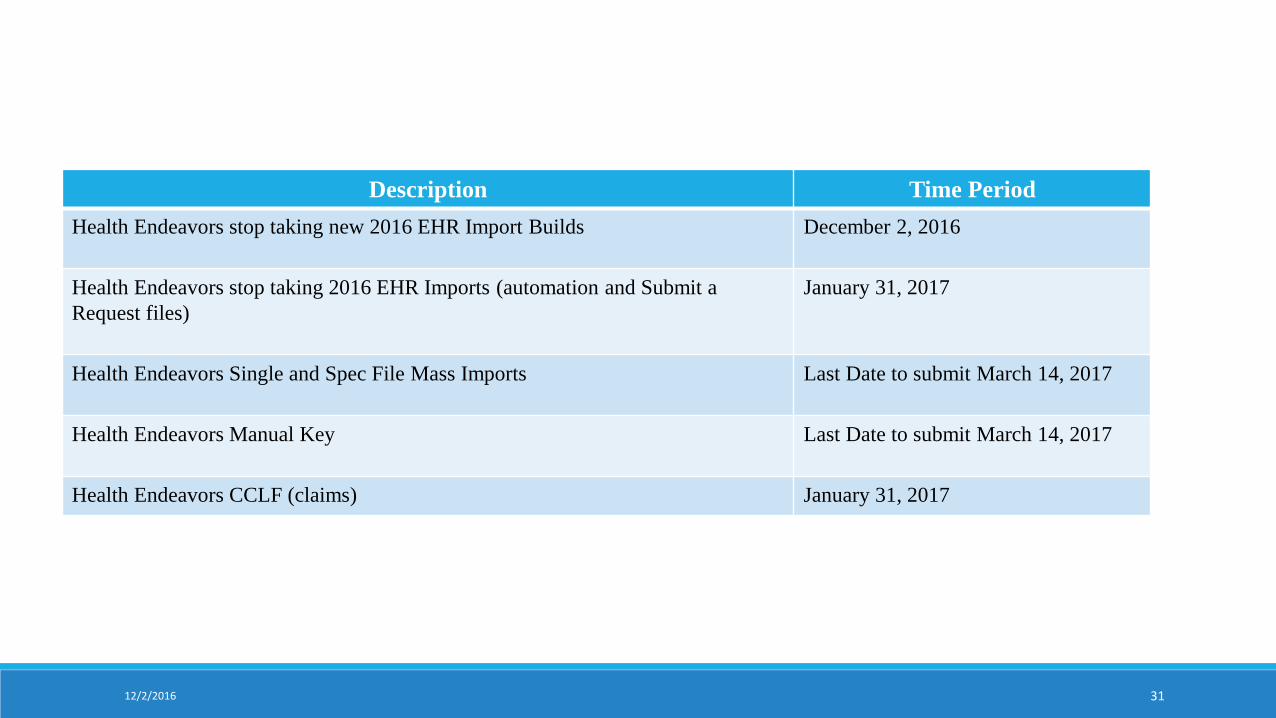
Description Time Period
Health Endeavors stop taking new 2016 EHR Import Builds December 2, 2016
Health Endeavors stop taking 2016 EHR Imports (automation and Submit a
Request files)
January 31, 2017
Health Endeavors Single and Spec File Mass Imports Last Date to submit March 14, 2017
Health Endeavors Manual Key Last Date to submit March 14, 2017
Health Endeavors CCLF (claims) January 31, 2017
12/2/2016
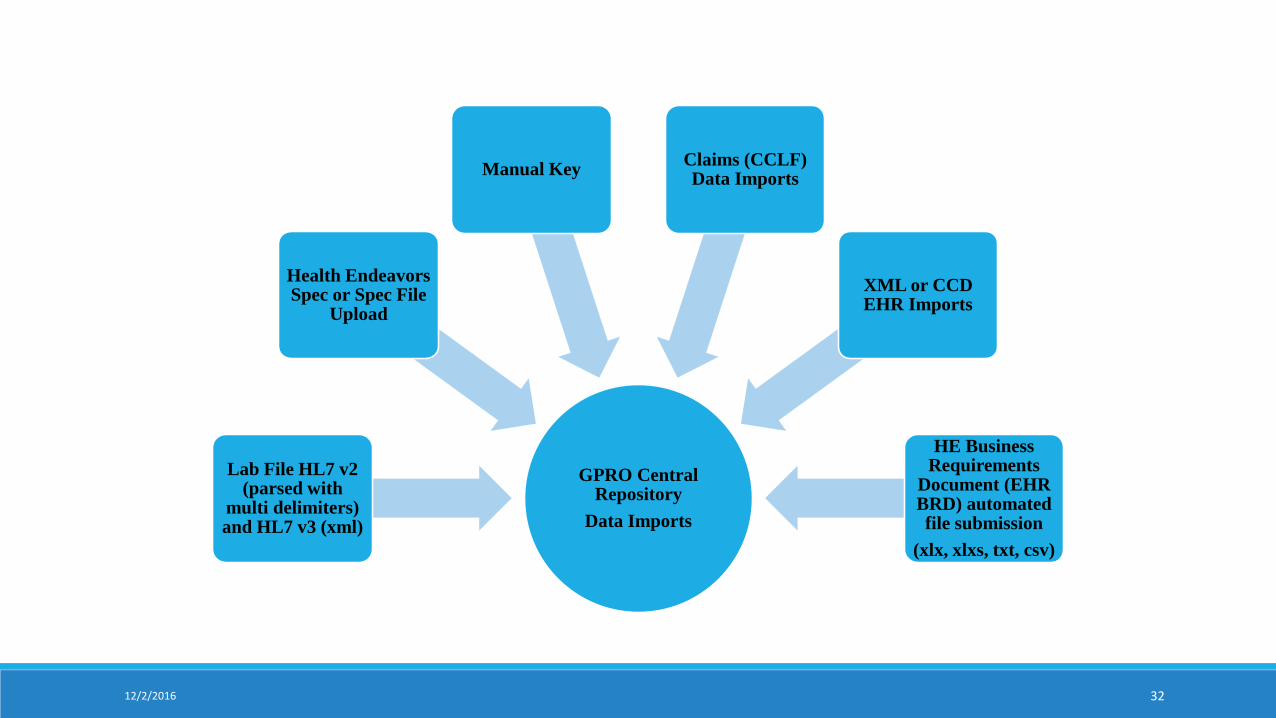
GPRO Central Repository
Data Imports
Lab File HL7 v2 (parsed with
multi delimiters) and HL7 v3 (xml)
Health Endeavors Spec or Spec File
Upload
Manual KeyClaims (CCLF) Data Imports
XML or CCD EHR Imports
HE Business Requirements
Document (EHR BRD) automated file submission
(xlx, xlxs, txt, csv)
12/2/2016 32
Patient Assignment2016 GPRO RANDOM SAMPLE REPORTING
3312/2/2016
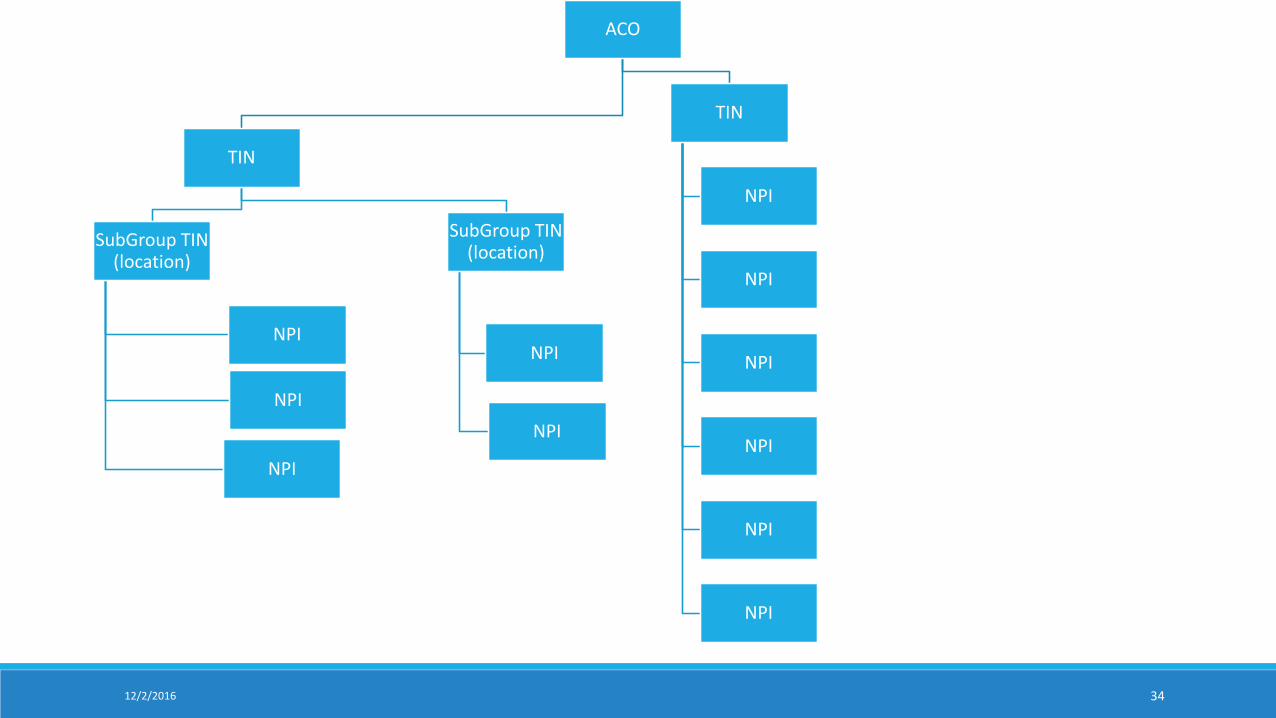
ACO
TIN
SubGroup TIN (location)
NPI
NPI
NPI
SubGroup TIN (location)
NPI
NPI
TIN
NPI
NPI
NPI
NPI
NPI
NPI
12/2/2016 34
Patient Assignment AlgorithmPrimary Care Provider TINs – Priority #1
Specialist TINs –Assign to Specialist TIN or Assign to PCP – Priority #2
Associate the NPIs under the selected TIN (from above)
NPI with the greater number of visits in last 12 months
◦ Using Part B attribution code visits
12/2/2016 35
GPRO 2016 Interface2016 GPRO RANDOM SAMPLE REPORTING
3612/2/2016
Tips & PitfallsReview your QM 2016 Import Chart
Have a Plan of Action for excessive measure Skips.
Do not get stuck on 1 record. In the first 10 days complete as many records as possible.
You can always return to a record.
Do not spend a lot of time on requested dates in the questions if not legible as CMS allows us to default to December 31, 2016 if date is illegible.
Do not overwrite data unless you are certain of the data is correct and more recent than the data entered.
Click Submit Data to CMS daily.
Be done in 6 weeks (NOT 8 weeks)
To obtain Shared Savings = GET DONE
3712/2/2016
RanksRandom Sample Rank File received in January, 2017
◦ NOTE – Has been sent to MFT portal for past 4 years
Patients Ranked 1 to 616 in each Module◦ May have less than 616 if not enough patients to fill the module
Required to complete 1 to 248 consecutively
249 to 616 the oversample [Patient or Module Skips]
Focus on completion of 1 to 248 (Lowest to Highest Rank)◦ Generally ACOs urge working 350 and below to account for skips in the first 2 weeks.
3812/2/2016
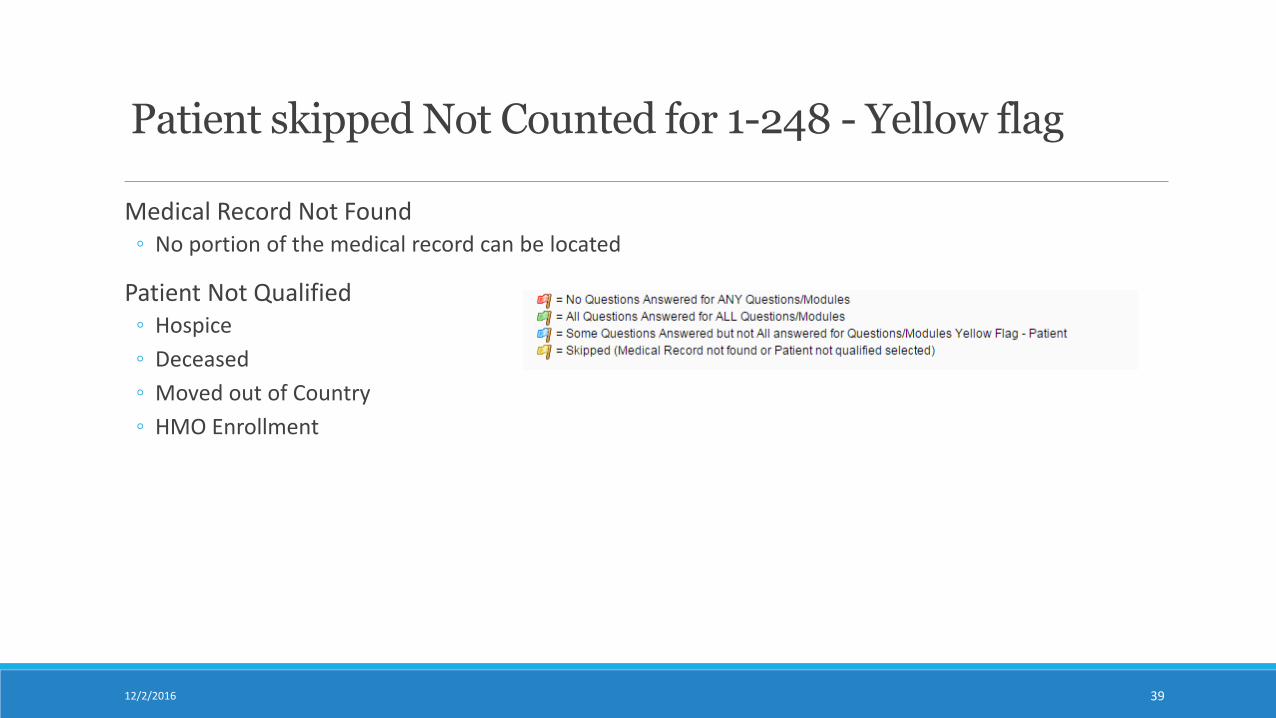
Patient skipped Not Counted for 1-248 - Yellow flag
Medical Record Not Found◦ No portion of the medical record can be located
Patient Not Qualified◦ Hospice
◦ Deceased
◦ Moved out of Country
◦ HMO Enrollment
3912/2/2016
12/2/2016 40
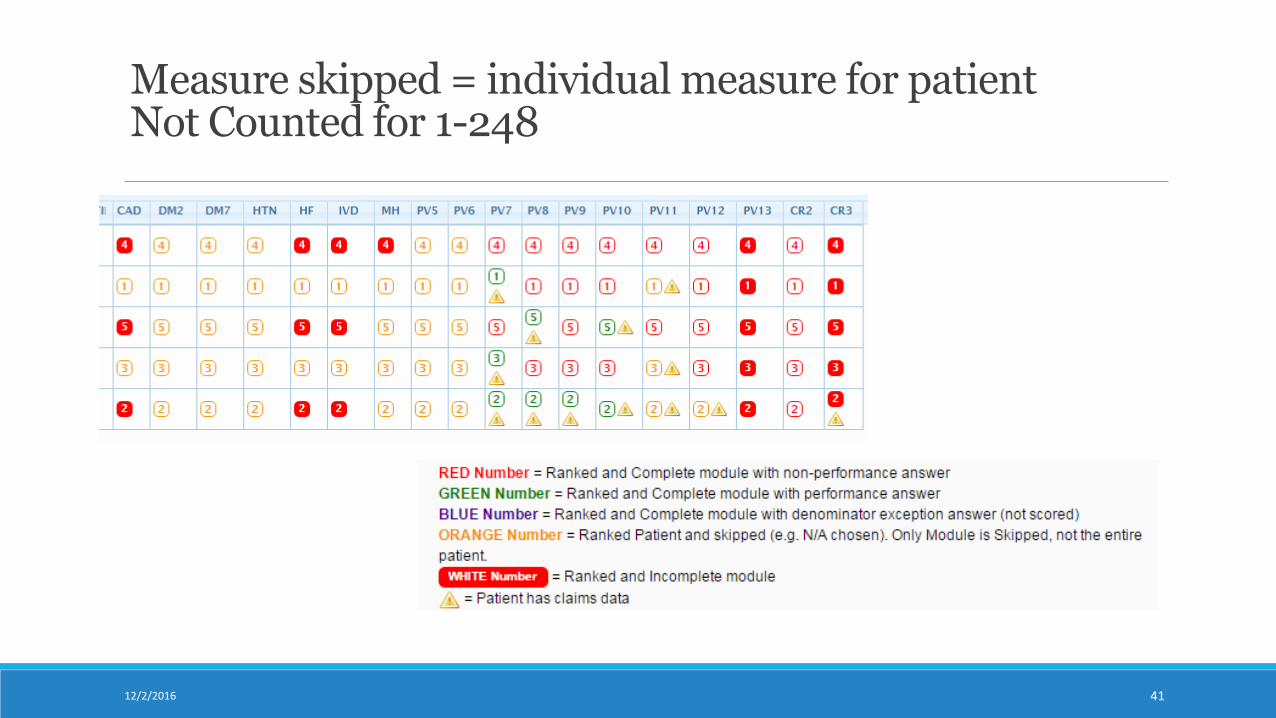
Measure skipped = individual measure for patient Not Counted for 1-248
4112/2/2016
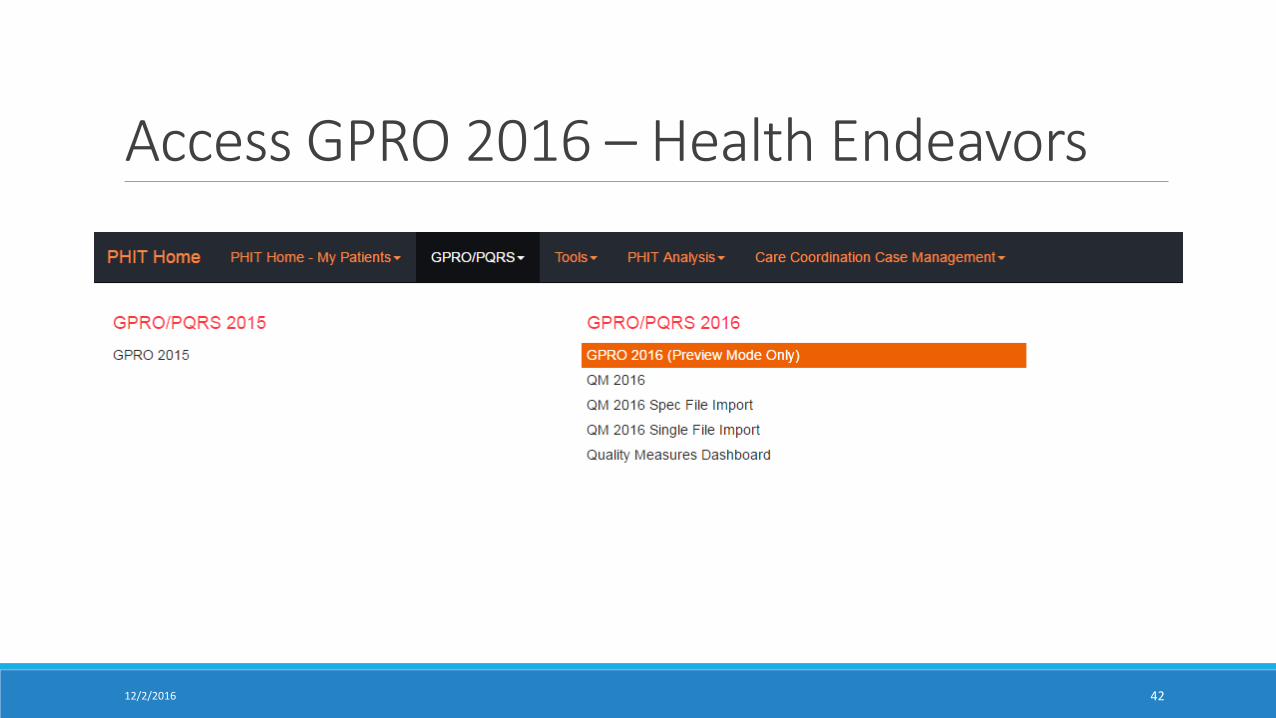
Access GPRO 2016 – Health Endeavors
4212/2/2016
4312/2/2016
4412/2/2016
12/2/2016 45
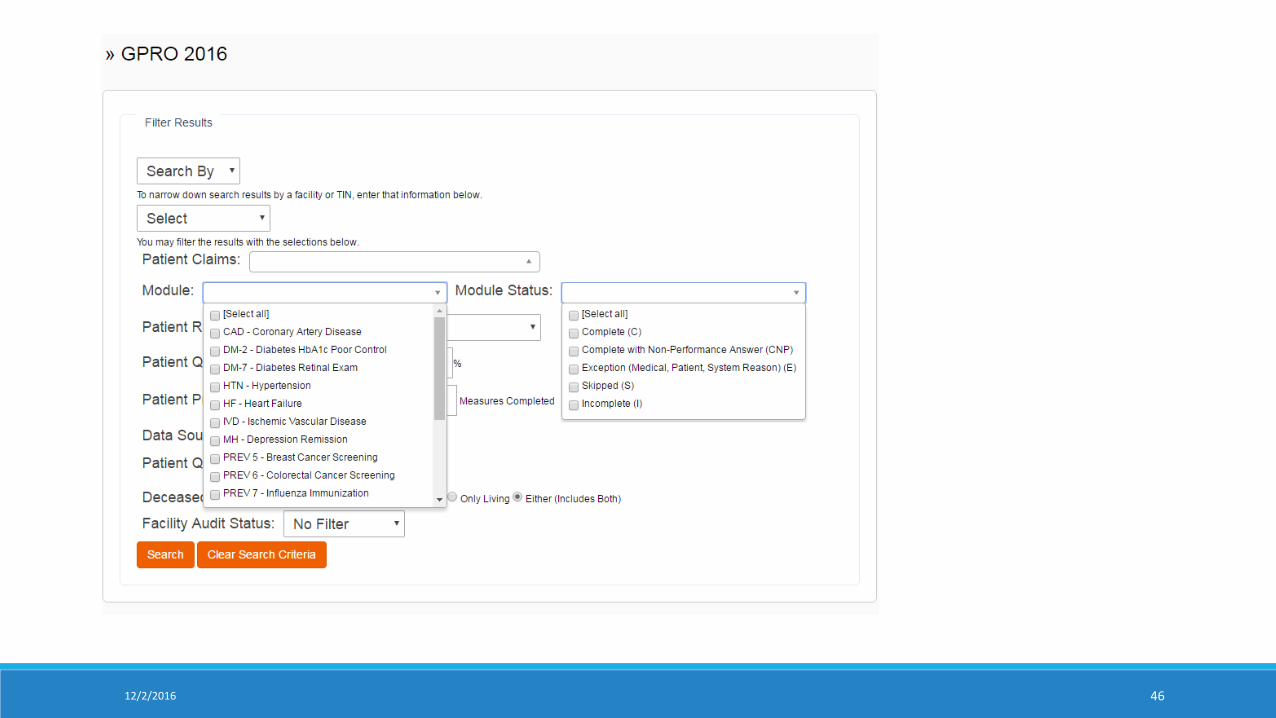
12/2/2016 46
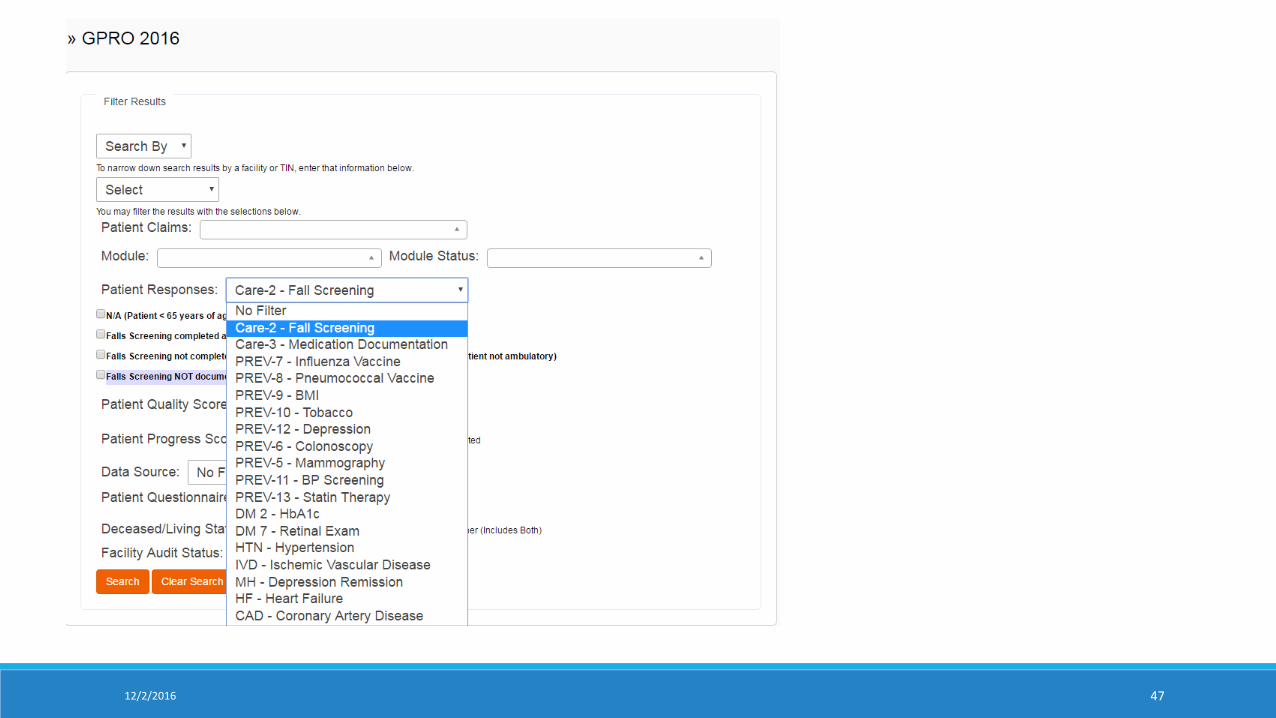
12/2/2016 47
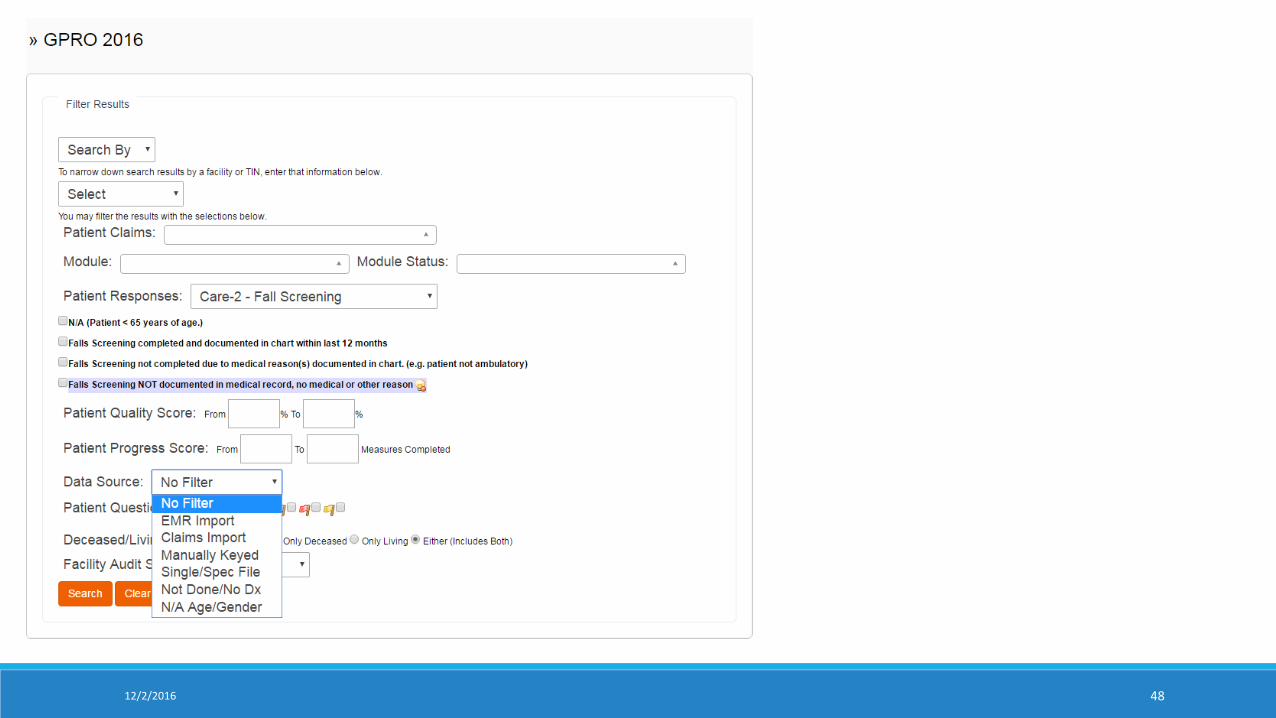
12/2/2016 48
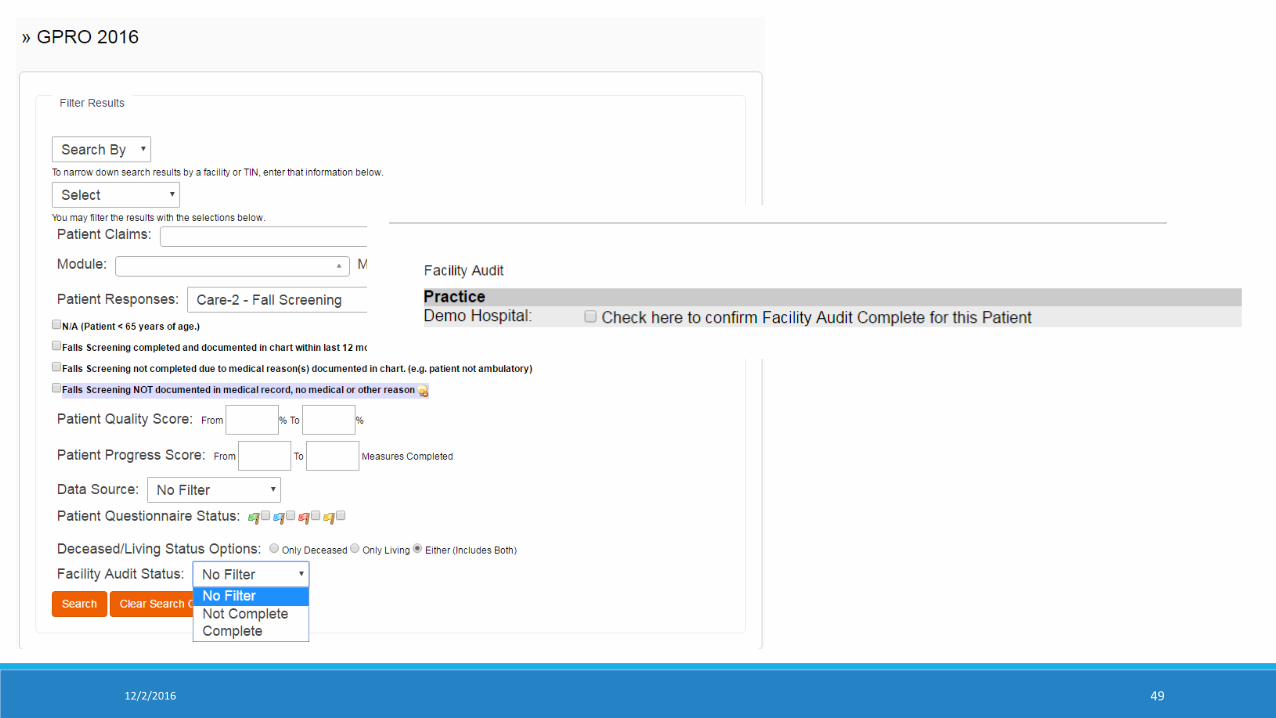
12/2/2016 49
12/2/2016 50
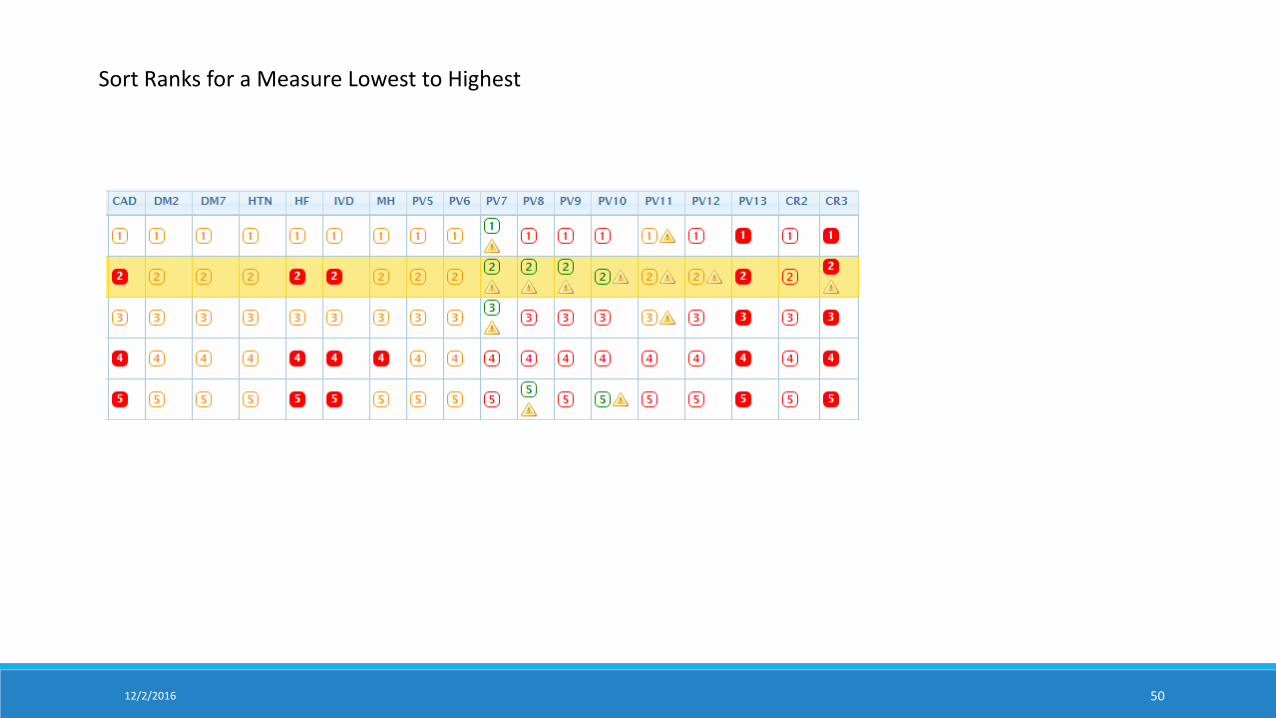
Sort Ranks for a Measure Lowest to Highest
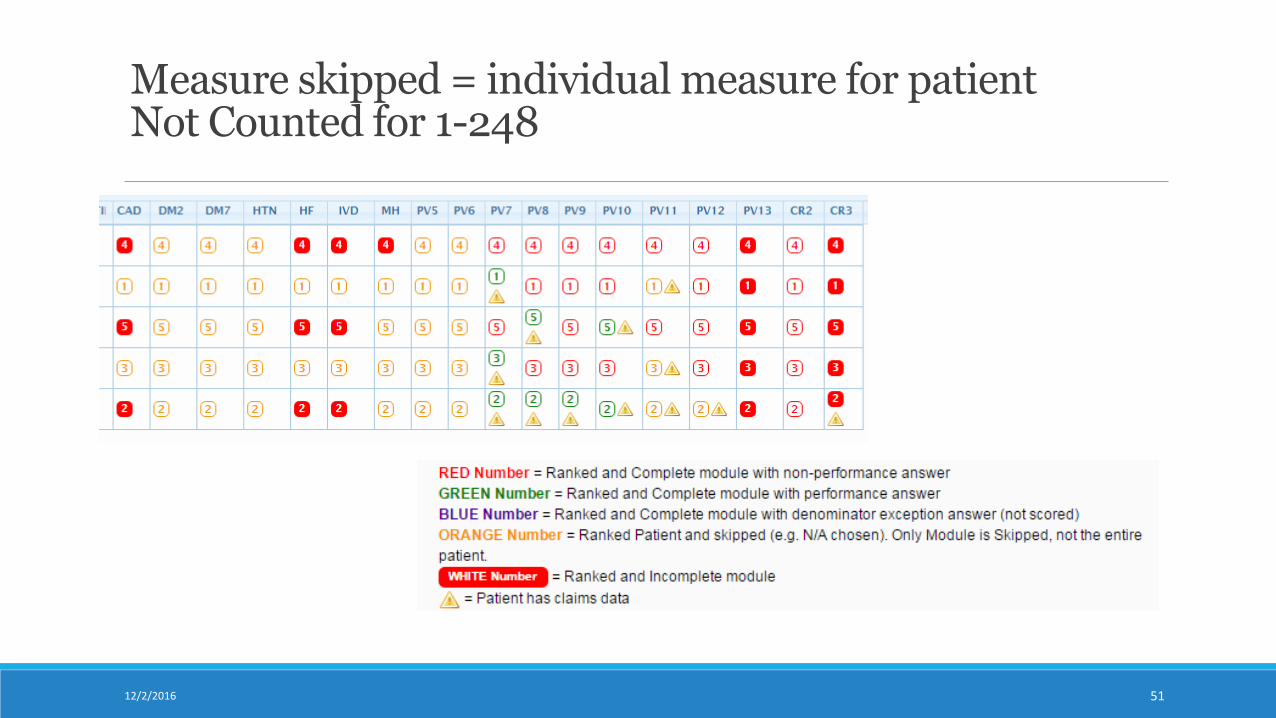
Measure skipped = individual measure for patient Not Counted for 1-248
5112/2/2016
12/2/2016 52
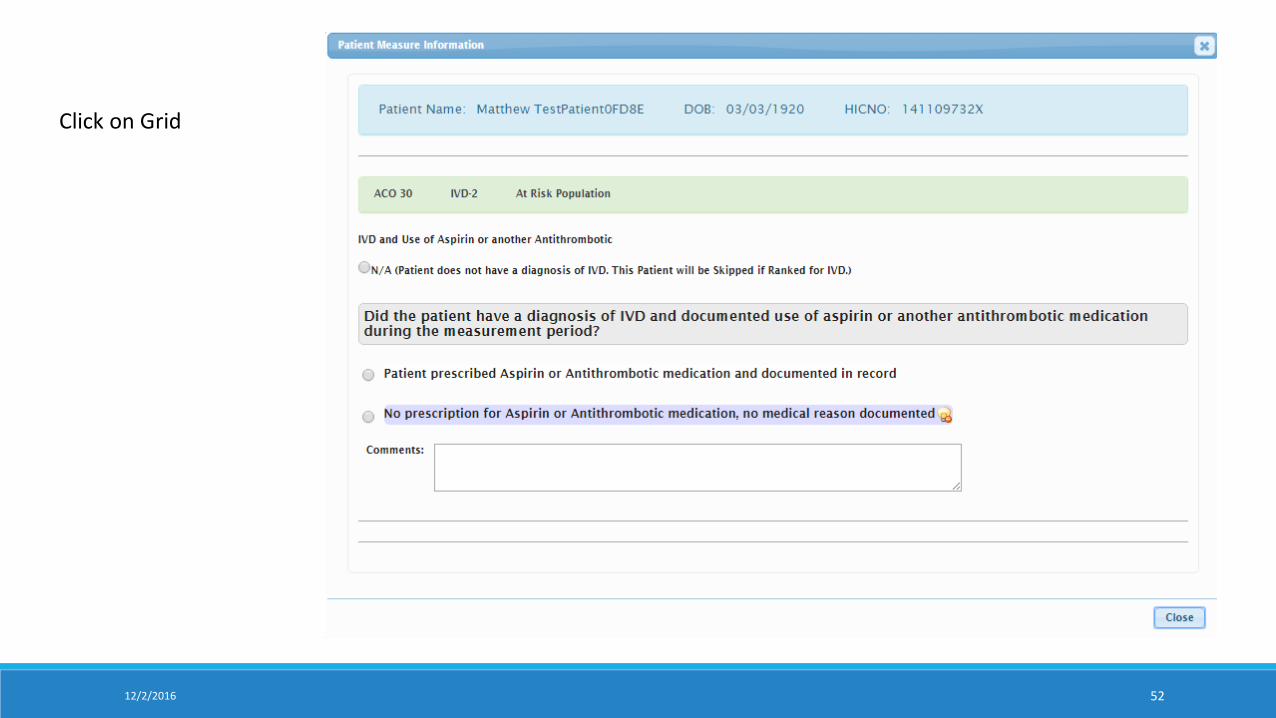
Click on Grid
12/2/2016 53
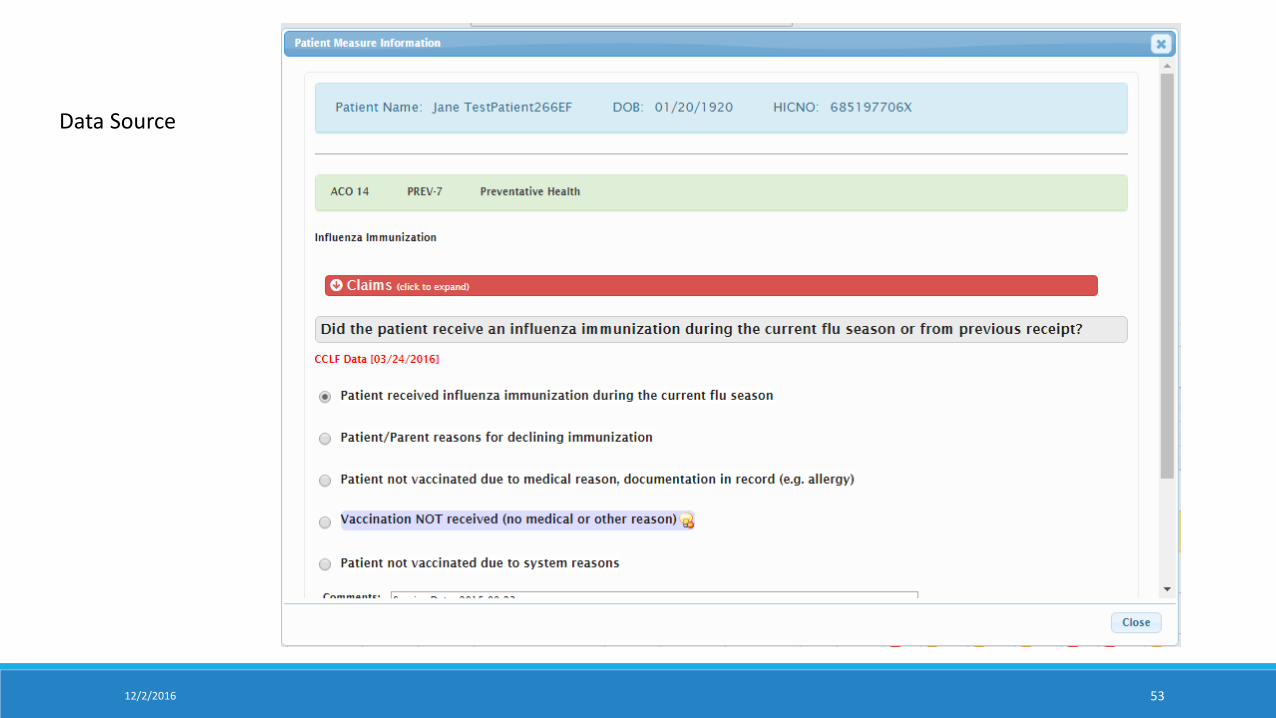
Data Source
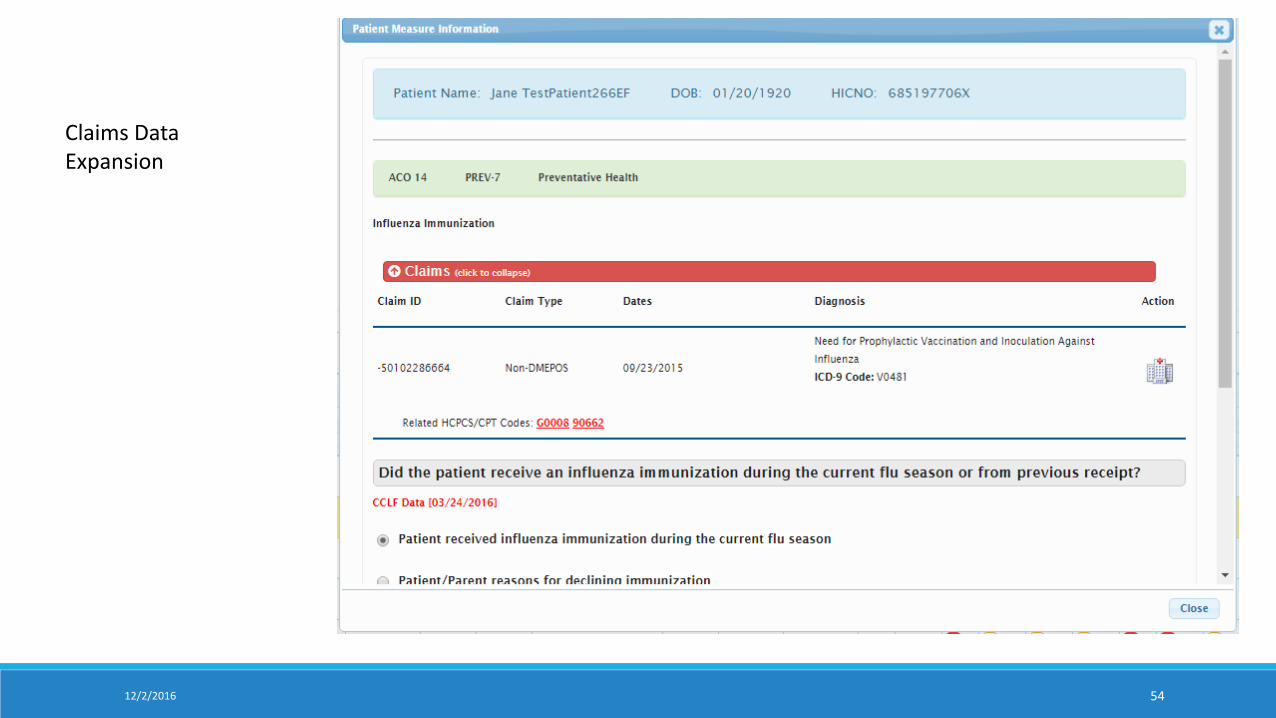
12/2/2016 54
Claims Data Expansion
5512/2/2016
5612/2/2016
GPRO Performance Scoring2016 GPRO RANDOM SAMPLE REPORTING
5712/2/2016
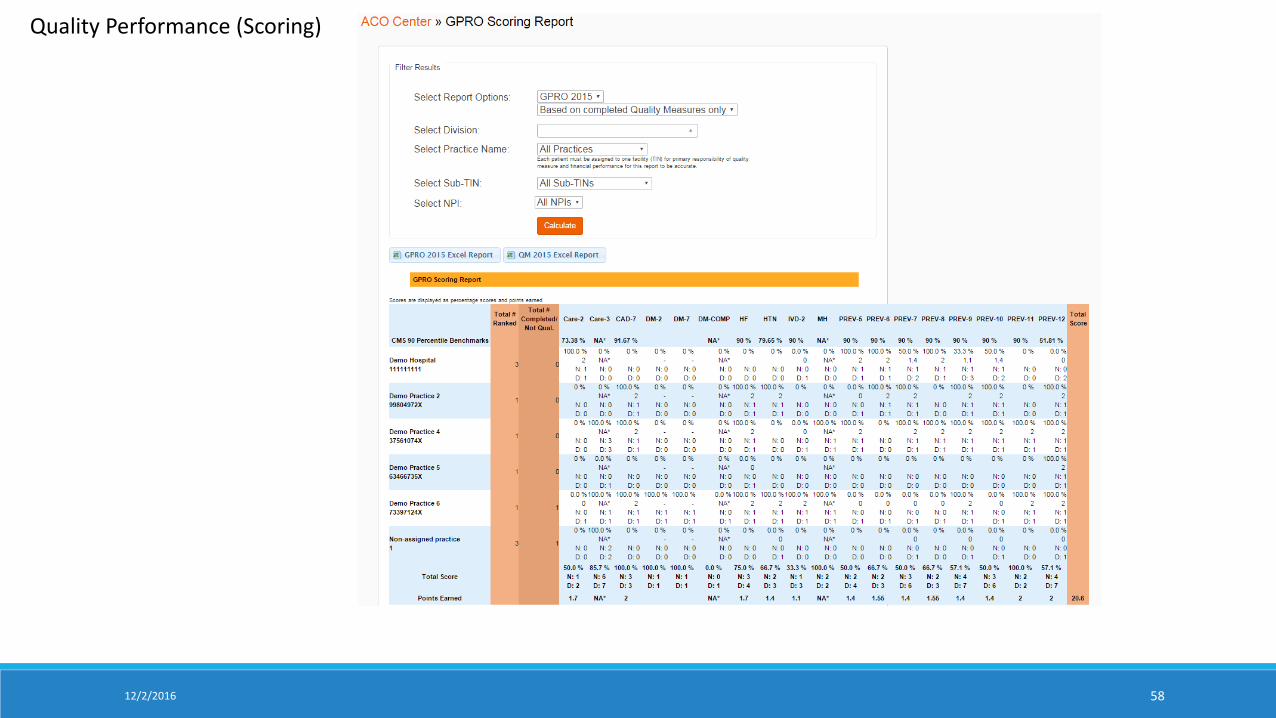
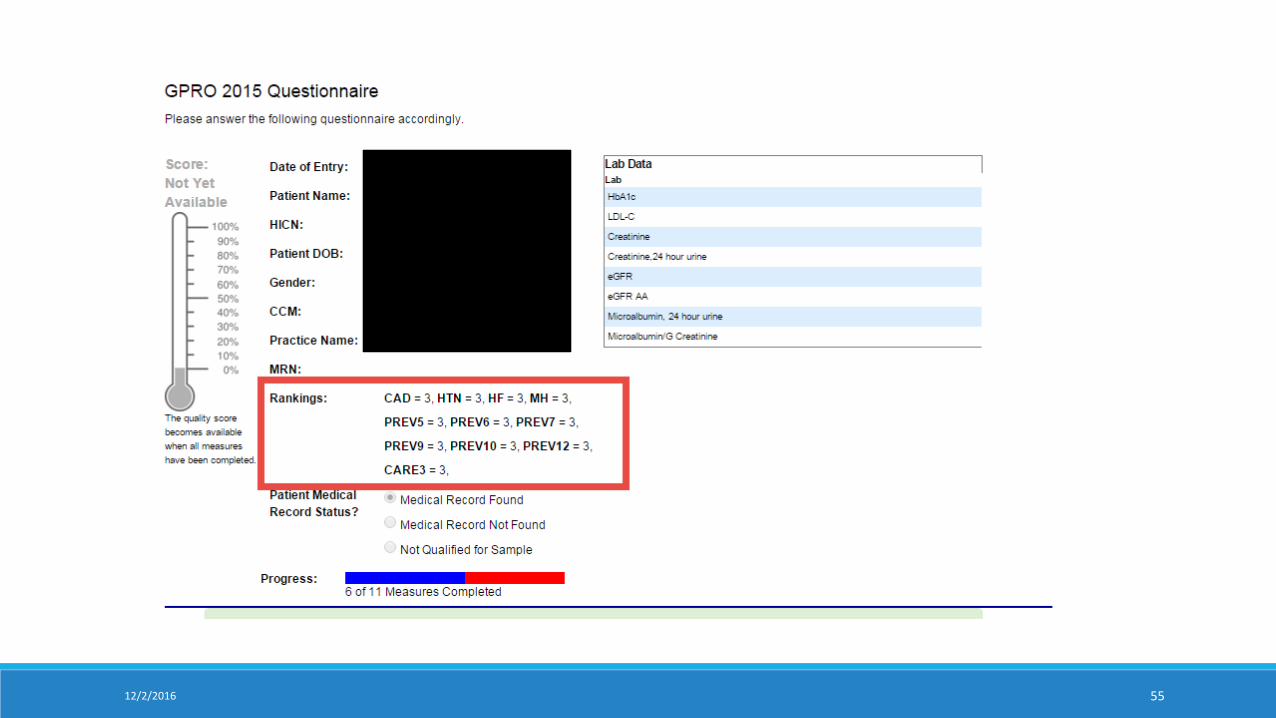
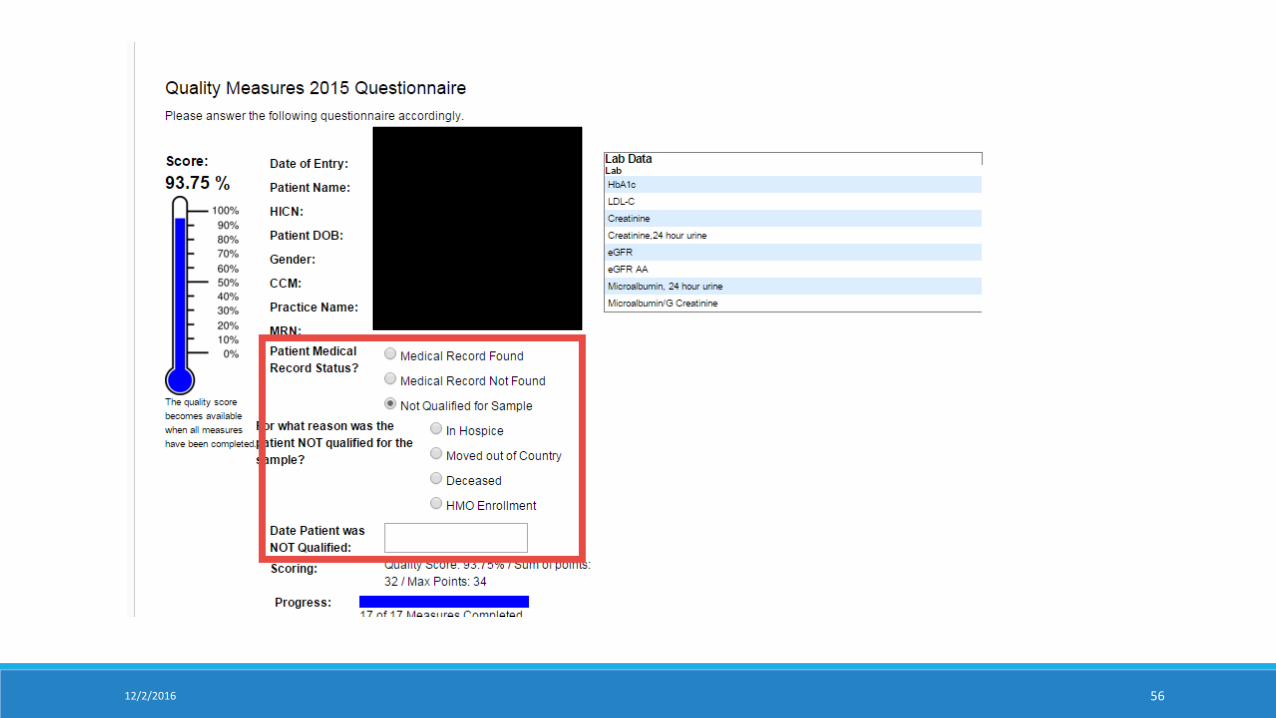
58
Quality Performance (Scoring)
12/2/2016

Total Quality Score2016 GPRO RANDOM SAMPLE REPORTING
5912/2/2016
Single and Spec File Mass Imports 2016 GPRO RANDOM SAMPLE REPORTING
6012/2/2016
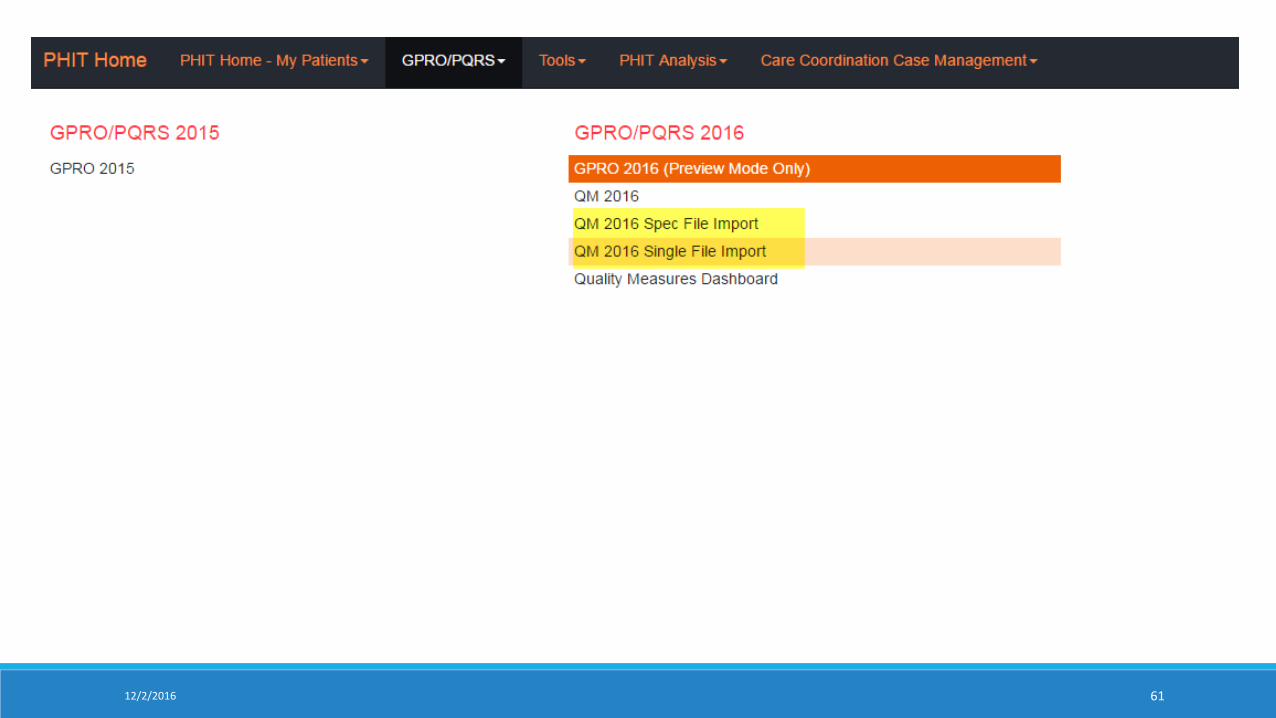
12/2/2016 61
Single File Upload Tool
12/2/2016
Only positive questionnaire responses can be uploaded with the Tool.
Select the module and related question you would like to complete.
Upload the properly formatted file that contains the patient HIC Numbers or Patient First Name, Last Name and DOB.
You will provided a review of actions to be taken prior to any updates being committed.
The process is limited to 1000 records per upload.
62
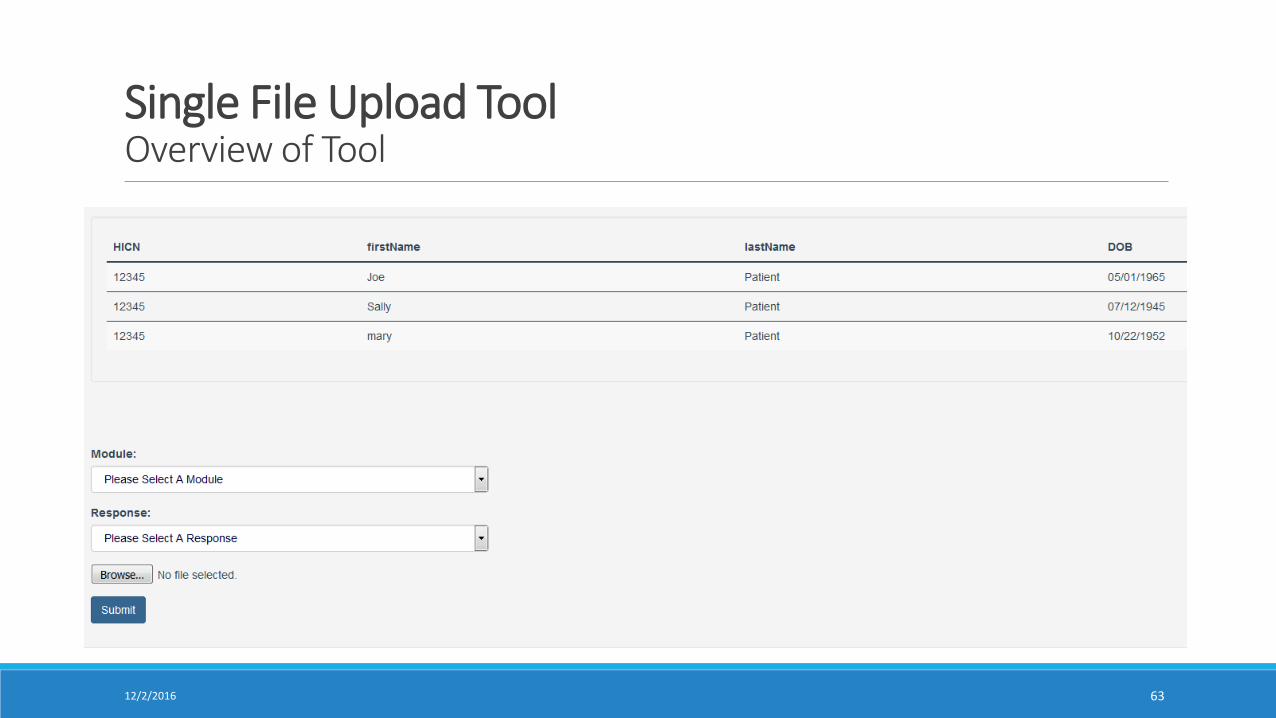
Single File Upload ToolOverview of Tool
12/2/2016 63
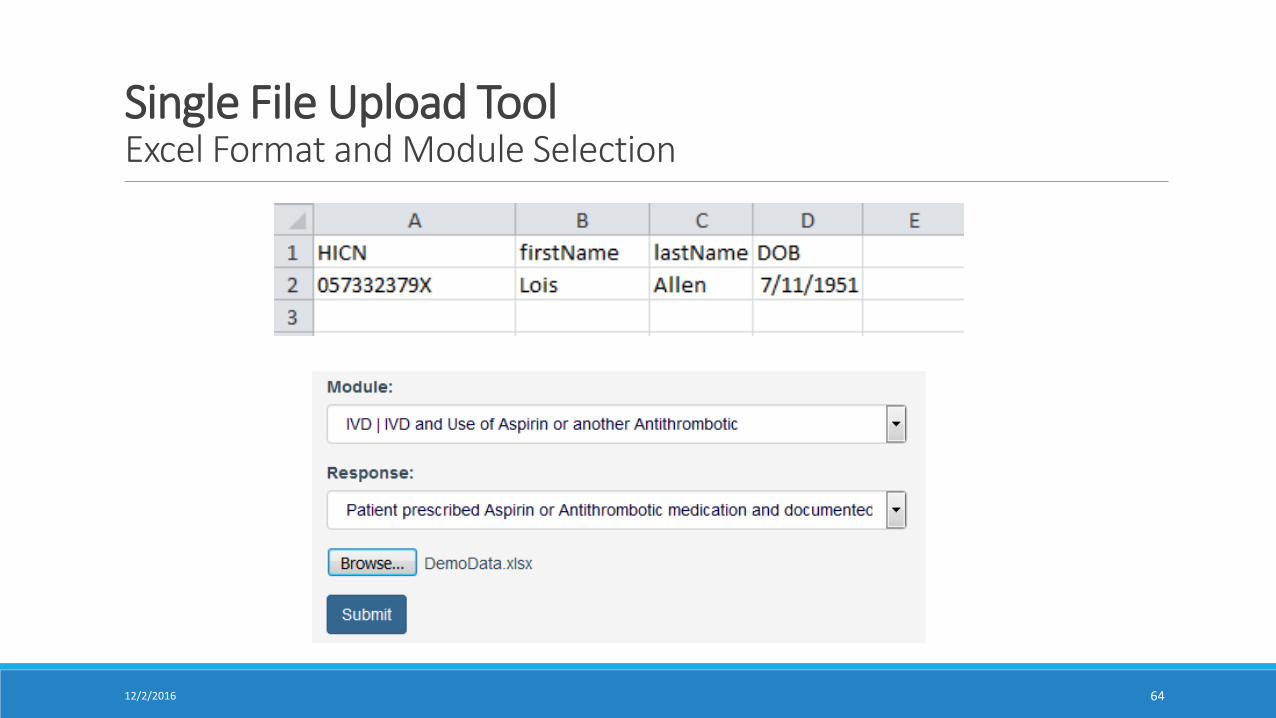
Single File Upload ToolExcel Format and Module Selection
12/2/2016 64
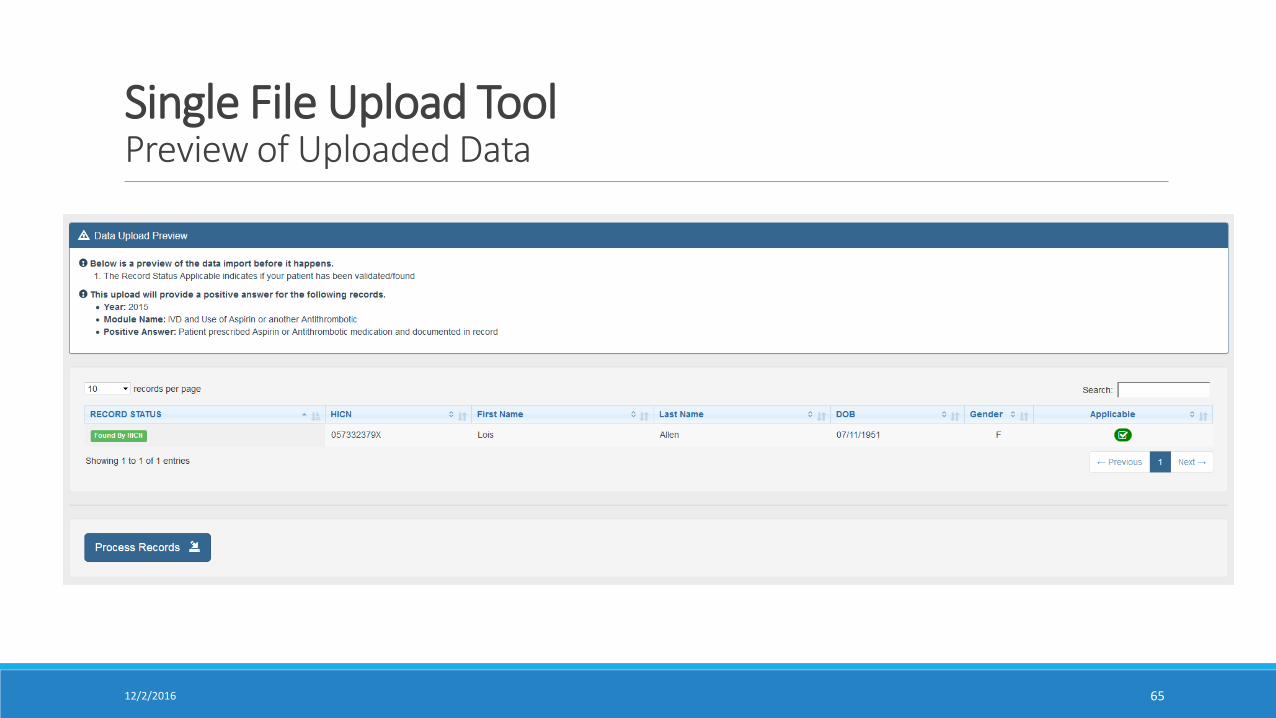
Single File Upload ToolPreview of Uploaded Data
12/2/2016 65
Spec File Import ToolOverview of the Tool
12/2/2016
All questionnaire responses can be imported using the tool.
Select the module and from the sidebar.
Upload the properly formatted file that contains the patient HIC Numbers or Patient First Name, Last Name and DOB. Each measure contains a template to be used for the data.
An answer legend will be provided for each measure to detail the responses.
You will provided a review of actions to be taken prior to any updates being committed.
The process is limited to 1000 records per upload.
66
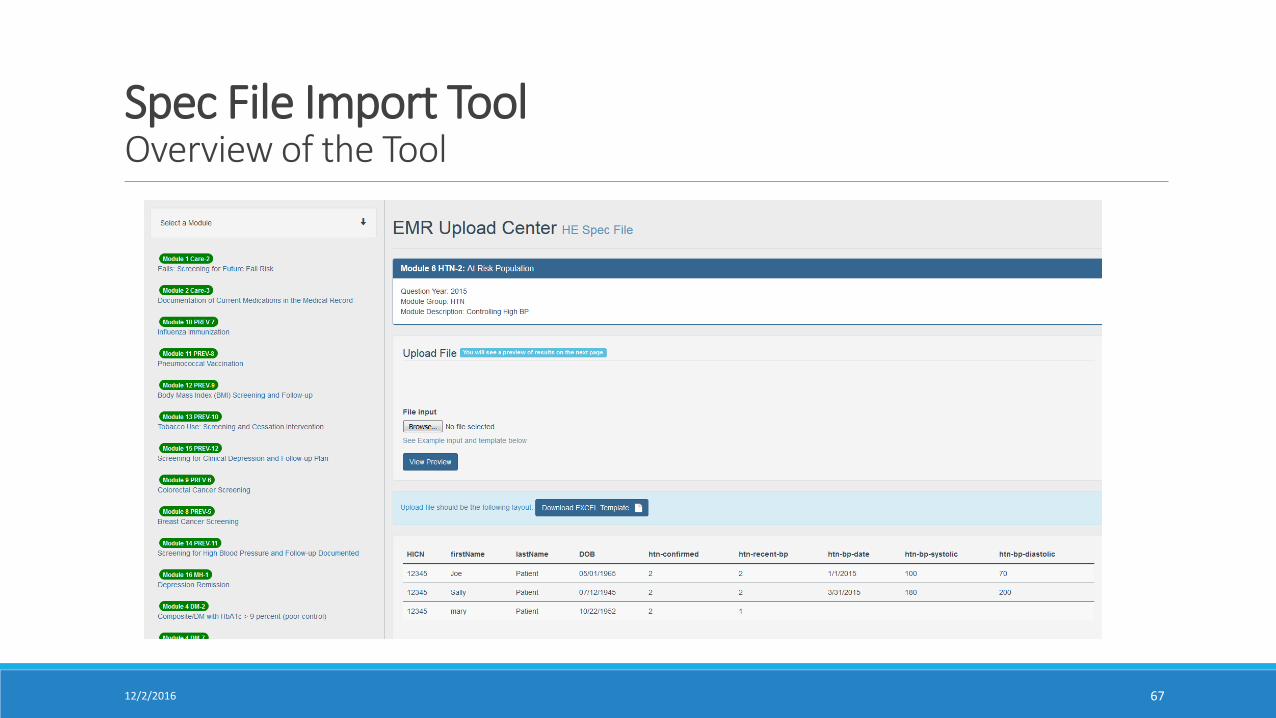
Spec File Import ToolOverview of the Tool
12/2/2016 67
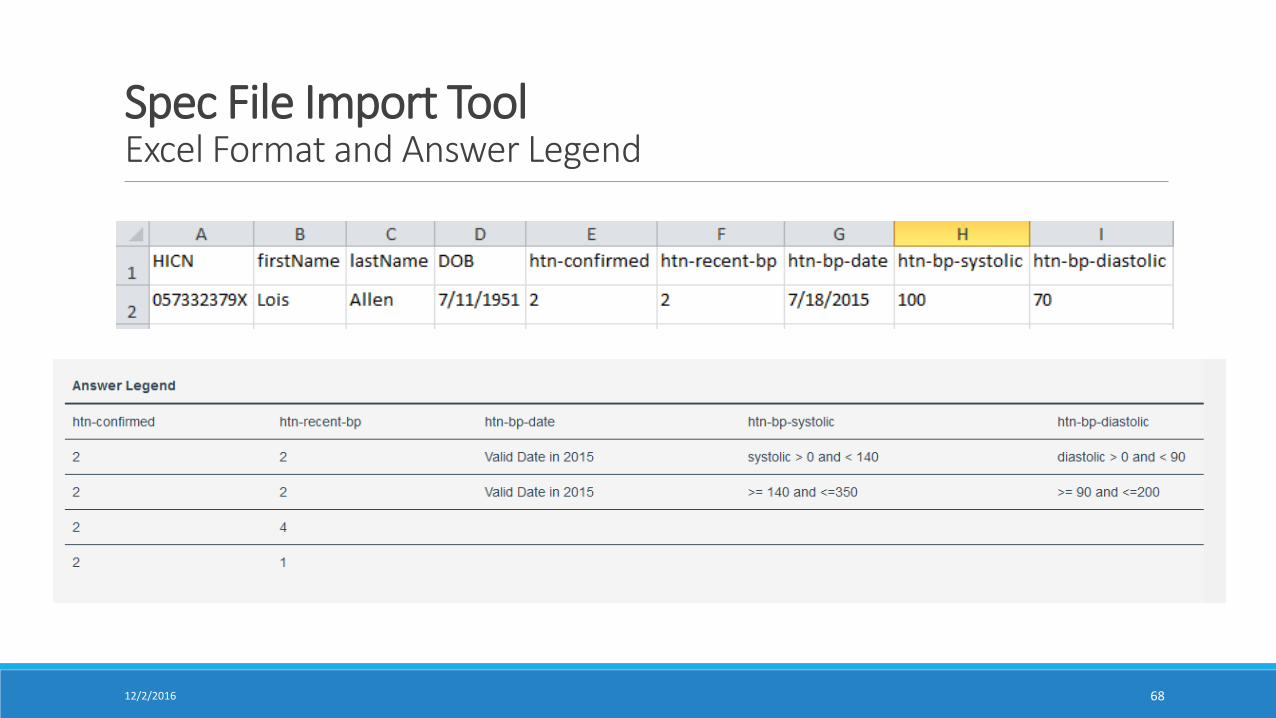
Spec File Import ToolExcel Format and Answer Legend
12/2/2016 68
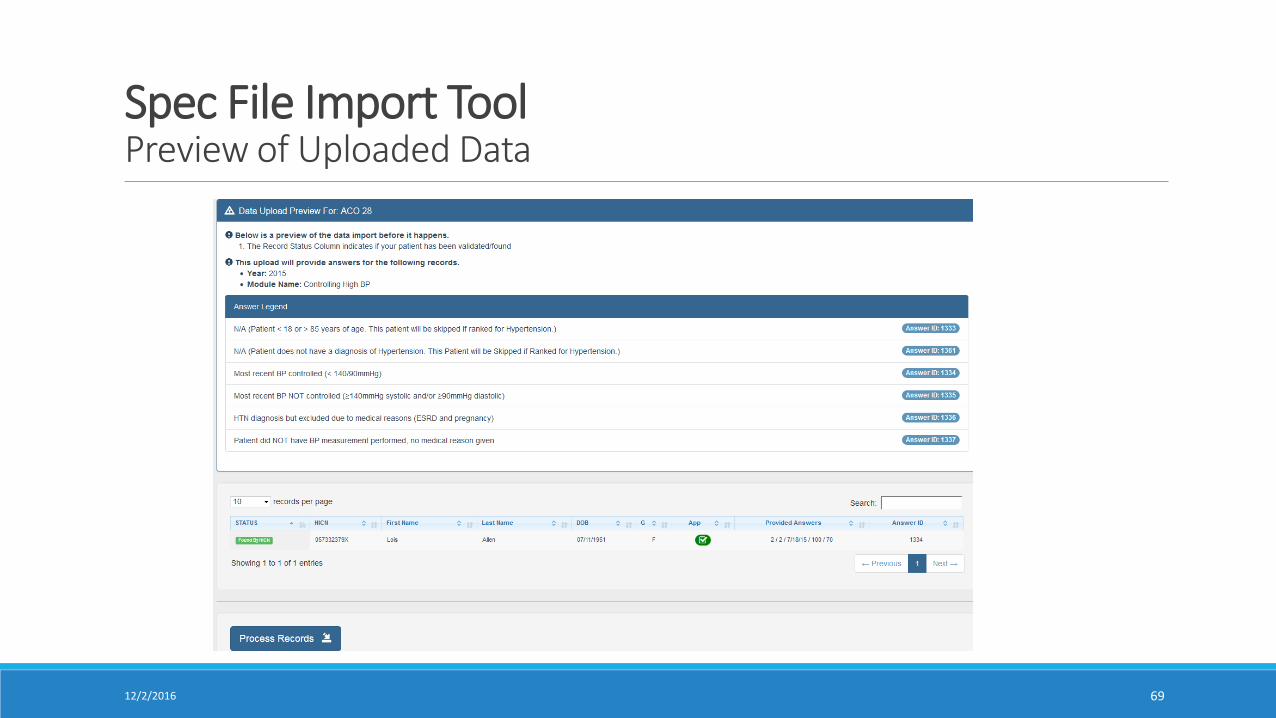
Spec File Import ToolPreview of Uploaded Data
12/2/2016 69
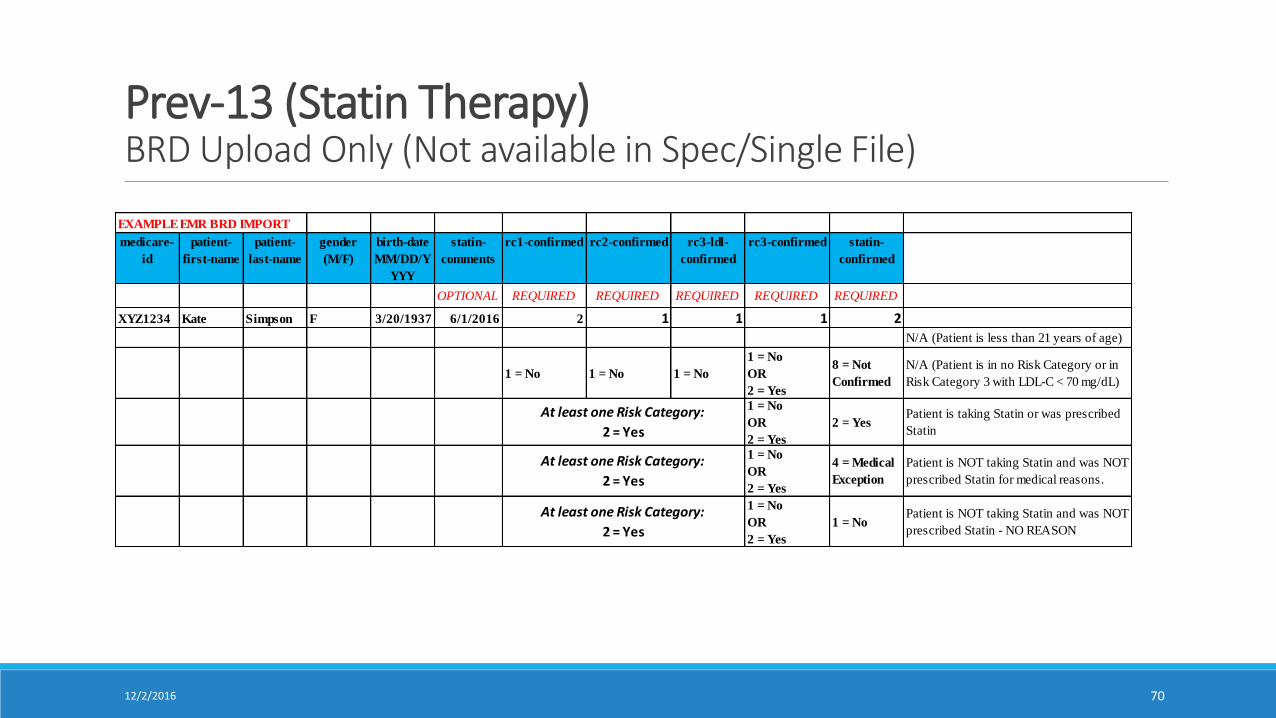
Prev-13 (Statin Therapy)BRD Upload Only (Not available in Spec/Single File)
12/2/2016 70
EXAMPLE EMR BRD IMPORT
medicare-
id
patient-
first-name
patient-
last-name
gender
(M/F)
birth-date
MM/DD/Y
YYY
statin-
comments
rc1-confirmed rc2-confirmed rc3-ldl-
confirmed
rc3-confirmed statin-
confirmed
OPTIONAL REQUIRED REQUIRED REQUIRED REQUIRED REQUIRED
XYZ1234 Kate Simpson F 3/20/1937 6/1/2016 2 1 1 1 2
N/A (Patient is less than 21 years of age)
1 = No 1 = No 1 = No
1 = No
OR
2 = Yes
8 = Not
Confirmed
N/A (Patient is in no Risk Category or in
Risk Category 3 with LDL-C < 70 mg/dL)
1 = No
OR
2 = Yes
2 = YesPatient is taking Statin or was prescribed
Statin
1 = No
OR
2 = Yes
4 = Medical
Exception
Patient is NOT taking Statin and was NOT
prescribed Statin for medical reasons.
1 = No
OR
2 = Yes
1 = NoPatient is NOT taking Statin and was NOT
prescribed Statin - NO REASON
At least one Risk Category:
2 = Yes
At least one Risk Category:
2 = Yes
At least one Risk Category:
2 = Yes
Discussion Topics2016 GPRO RANDOM SAMPLE REPORTING
7112/2/2016
Health Endeavors Review Session [Jan 2017]Checklist - Topics of Discussion
Do you need to update your QM Chart?
Is your ACO ready to enable the “Save” on GPRO 2016 for manual key?
What is your EMR import schedule between now and January 15th?◦ EMR data imports must be remitted to Health Endeavors no later than January 31, 2017.
Confirm - QM Scoring Report Enabled for GPRO 2016.
One more set of claims data in January, 2016.
Patient Assignment – we use algorithm or custom file
Claims data and documentation internal discussion.
Click Submit Data to CMS daily.
7212/2/2016
Audit Changes2016 GPRO RANDOM SAMPLE REPORTING
7312/2/2016
GPRO Web Interface: Quality Measures Validation Audit – ACO, Measure,
and Beneficiary Selection
74
Shared Savings Program ACOs may be selected for audit
– In 2016, 10% of the SSP ACOs will be selected for audit
– Selection will be random or based on data anomalies
– Anomalies include such things as unusually high skip rates due to Medical
Record Not Found
Audit Measure and Beneficiary Selection
– CMS will audit about 200 records per ACO, across 4 to 5 measures
– All records will be reviewed by CMS
Pioneer and Next Generation Model ACOs – Information on the
2016 QMV Audit will be provided in the Pioneer Briefing and the Next
Generation ACO Newsletter
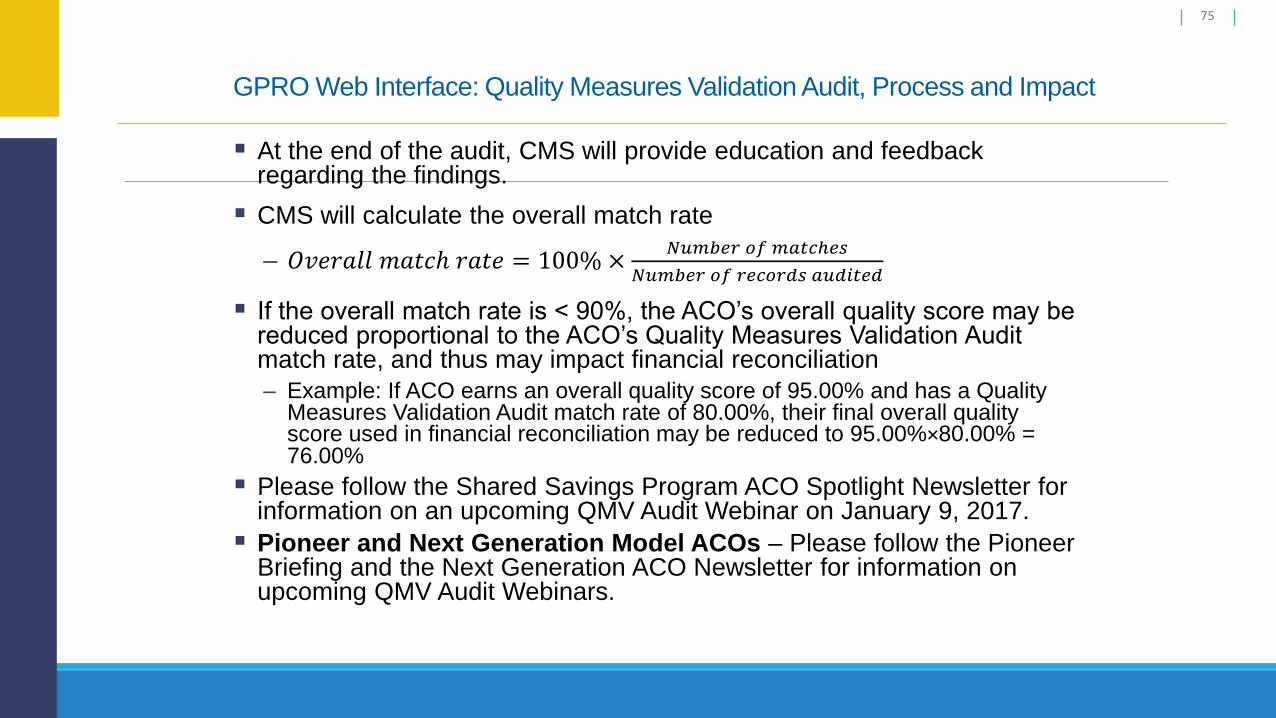
GPRO Web Interface: Quality Measures Validation Audit, Process and Impact
75
At the end of the audit, CMS will provide education and feedback regarding the findings.
CMS will calculate the overall match rate
– 𝑂𝑣𝑒𝑟𝑎𝑙𝑙 𝑚𝑎𝑡𝑐ℎ 𝑟𝑎𝑡𝑒 = 100% ×𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑚𝑎𝑡𝑐ℎ𝑒𝑠
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑟𝑒𝑐𝑜𝑟𝑑𝑠 𝑎𝑢𝑑𝑖𝑡𝑒𝑑
If the overall match rate is < 90%, the ACO’s overall quality score may be reduced proportional to the ACO’s Quality Measures Validation Audit match rate, and thus may impact financial reconciliation
– Example: If ACO earns an overall quality score of 95.00% and has a Quality Measures Validation Audit match rate of 80.00%, their final overall quality score used in financial reconciliation may be reduced to 95.00%×80.00% = 76.00%
Please follow the Shared Savings Program ACO Spotlight Newsletter for information on an upcoming QMV Audit Webinar on January 9, 2017.
Pioneer and Next Generation Model ACOs – Please follow the Pioneer Briefing and the Next Generation ACO Newsletter for information on upcoming QMV Audit Webinars.
12/2/2016 76
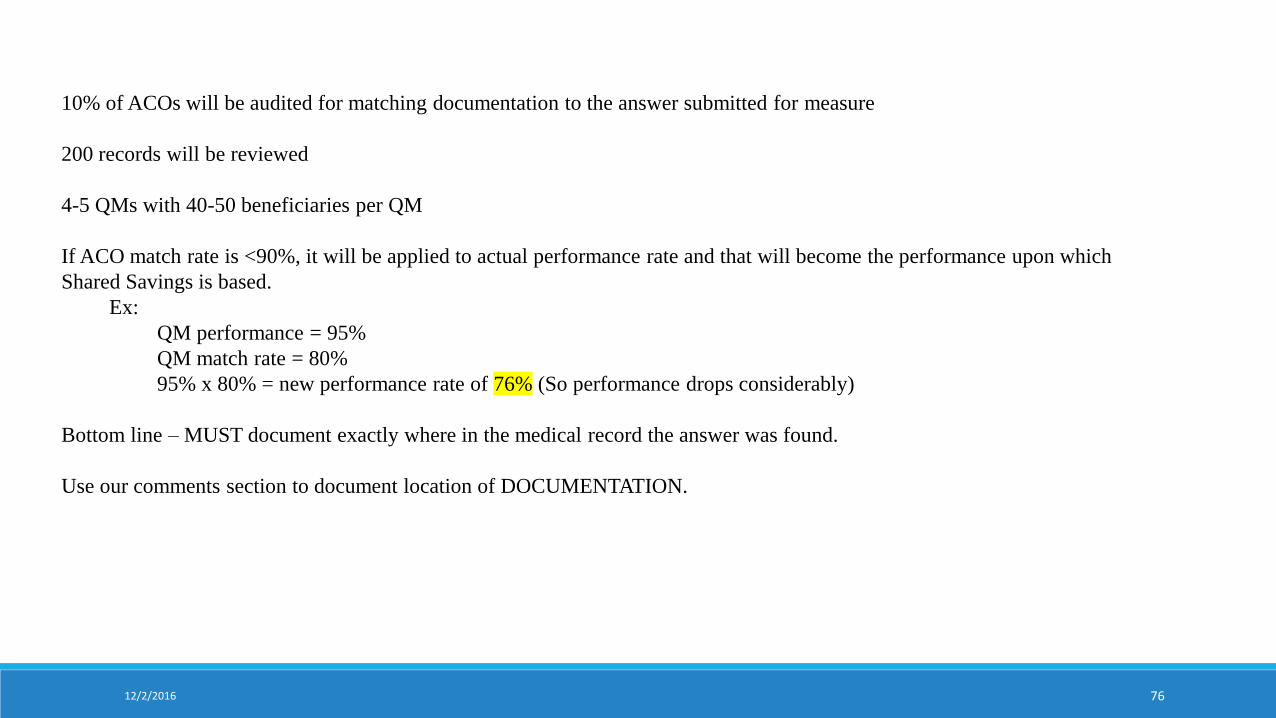
10% of ACOs will be audited for matching documentation to the answer submitted for measure
200 records will be reviewed
4-5 QMs with 40-50 beneficiaries per QM
If ACO match rate is <90%, it will be applied to actual performance rate and that will become the performance upon which
Shared Savings is based.
Ex:
QM performance = 95%
QM match rate = 80%
95% x 80% = new performance rate of 76% (So performance drops considerably)
Bottom line – MUST document exactly where in the medical record the answer was found.
Use our comments section to document location of DOCUMENTATION.
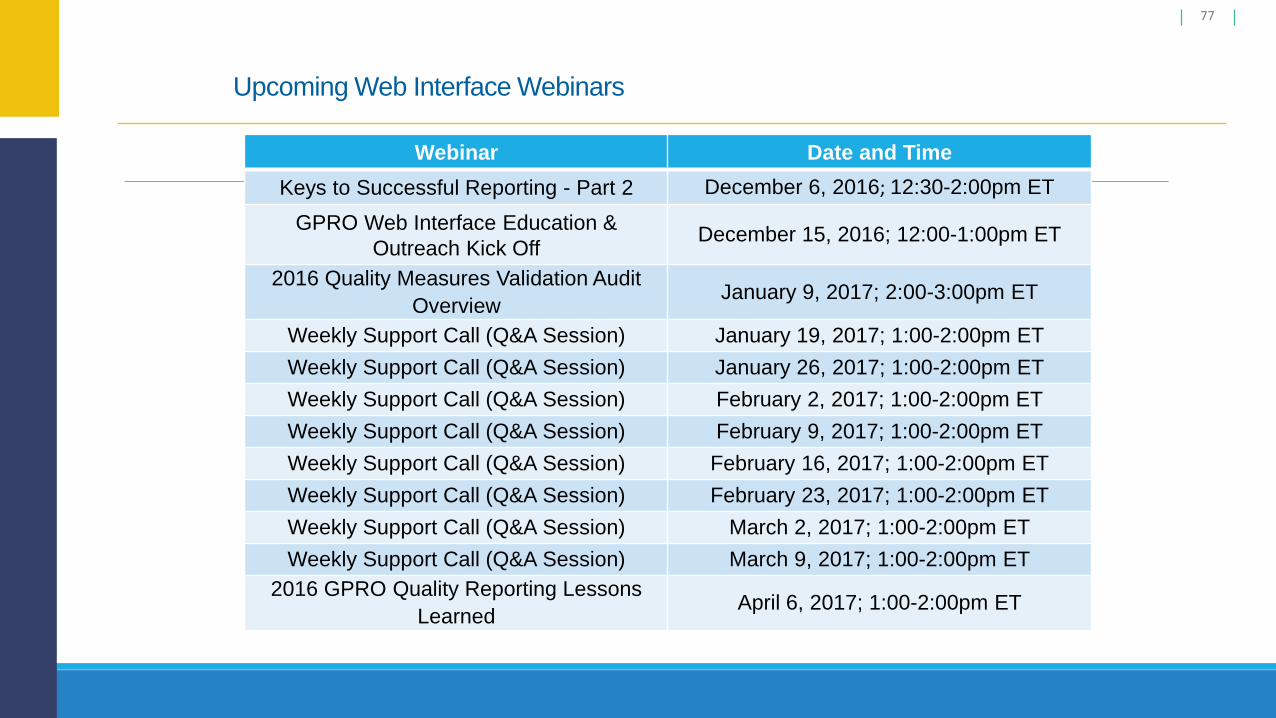
Upcoming Web Interface Webinars
77
Webinar Date and Time
Keys to Successful Reporting - Part 2 December 6, 2016; 12:30-2:00pm ET
GPRO Web Interface Education &
Outreach Kick Off December 15, 2016; 12:00-1:00pm ET
2016 Quality Measures Validation Audit
OverviewJanuary 9, 2017; 2:00-3:00pm ET
Weekly Support Call (Q&A Session) January 19, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) January 26, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) February 2, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) February 9, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) February 16, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) February 23, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) March 2, 2017; 1:00-2:00pm ET
Weekly Support Call (Q&A Session) March 9, 2017; 1:00-2:00pm ET
2016 GPRO Quality Reporting Lessons
LearnedApril 6, 2017; 1:00-2:00pm ET
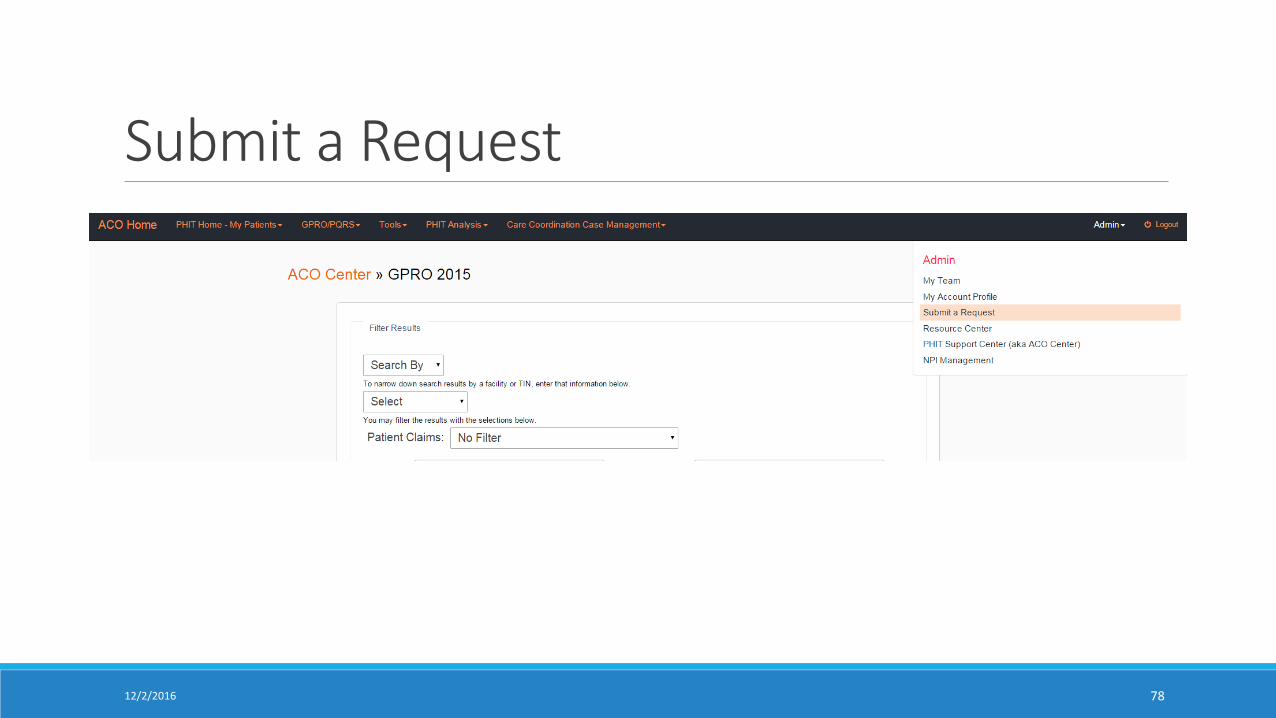
Submit a Request
7812/2/2016
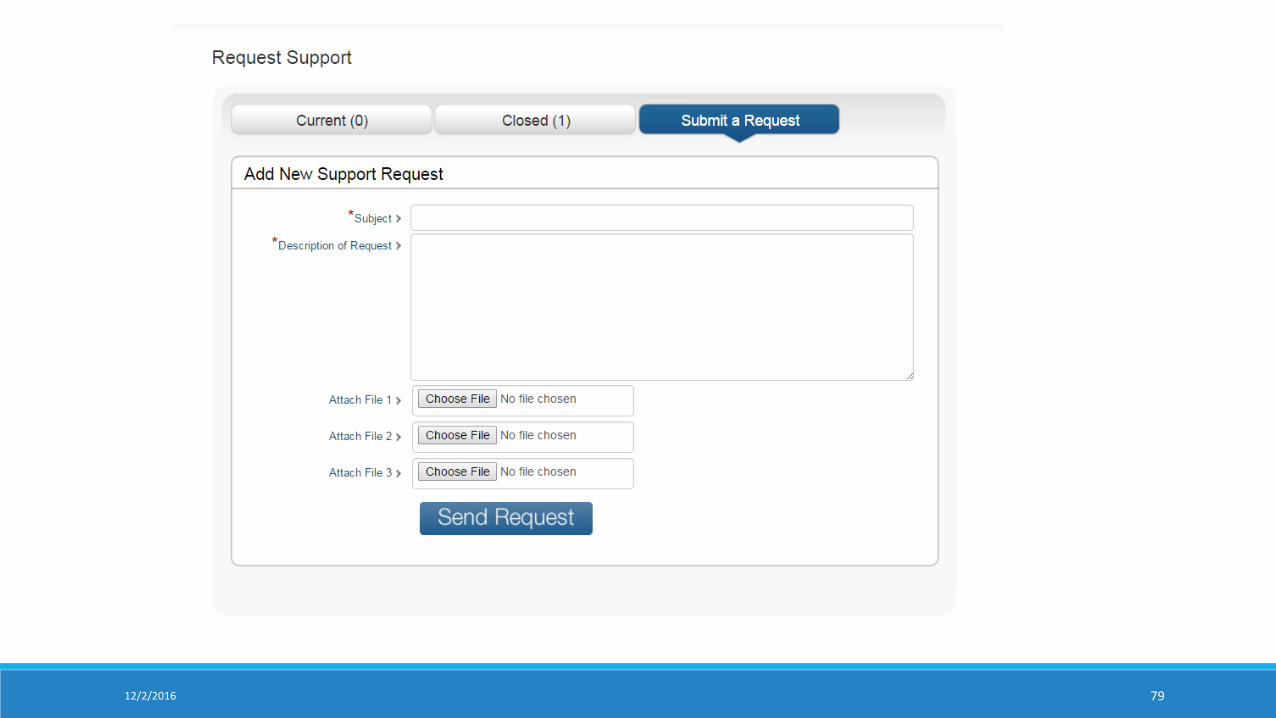
7912/2/2016