Embed Size (px)
Citation preview

155-OA-SGOFFHIXCERT (04/17) HMO Page 1
Section XXX
EmblemHealth Gold Open Access Schedule of Benefits
COST-SHARING
Medical Deductible Individual Family
Prescription DrugDeductible
Individual Family
Out-of-Pocket Limit Individual Family
Participating ProviderMember Responsibilityfor Cost-Sharing
$700$1,400
$100$200
$5,000$10,000
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
NoneNone
NoneNone
Non-Participating Providerservices are not Coveredexcept as required foremergency care.
OFFICE VISITS Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Primary Care Office Visits(or Home Visits)
3 visits covered in full,not subject to Deductible
After 3 visits, $10Copayment, not subjectto Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Specialist Office Visits(or Home Visits)
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 2
PREVENTIVE CARE Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Well Child Visits andImmunizations*
Adult Annual PhysicalExaminations*
Adult Immunizations*
Routine GynecologicalServices/Well WomanExams*
Mammograms,Screening andDiagnostic Imaging forthe Detection of BreastCancer
(14)[SterilizationProcedures for
Women*]
(15)[Vasectomy]
Bone Density Testing*
Screening for ProstateCancer Performed in a PCP
Office
Performed in aSpecialist Office
Covered in full
Covered in full
Covered in full
Covered in full
Covered in full
[Covered in full]
[See Surgical Services
Cost-Sharing]
Covered in full
$10 Copayment, notsubject to Deductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
[Non-Participating Providerservices are not Covered and
You pay the full cost]
[Non-Participating Providerservices are not Covered and
You pay the full cost]
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 3
PREVENTIVE CARE –Continued
All other preventiveservices required byUSPSTF and HRSA
*When preventiveservices are notprovided in accordancewith the comprehensiveguidelines supported byUSPSTF and HRSA
Participating ProviderMember Responsibilityfor Cost-Sharing
Covered in full
Use Cost-Sharing forappropriate service(Primary Care OfficeVisit; Specialist OfficeVisit; DiagnosticRadiology Services;Laboratory Proceduresand Diagnostic Testing)
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Limits
See benefit fordescription
EMERGENCY CARE Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Pre-Hospital EmergencyMedical Services(Ambulance Services)
$150 Copayment afterDeductible
$150 Copayment afterDeductible
See benefit fordescription
Non-Emergency AmbulanceServices
Preauthorizationrequired
$150 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Emergency Department
Copayment waived ifHospital admission
$150 Copayment afterDeductible
$150 Copayment afterDeductible
See benefit fordescription
Urgent Care Center $50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 4
PROFESSIONALSERVICES andOUTPATIENT CARE
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Acupuncture $20 Copayment, notsubject to Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Twelve (12)visits per PlanYear
Advanced Imaging Services
Performed in aSpecialist Office
Performed in aFreestandingRadiology Facility
Performed asOutpatient HospitalServices
$50 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Allergy Testing andTreatment
Performed in a PCPOffice
Performed in aSpecialist Office
$10 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Ambulatory Surgical CenterFacility Fee
Preauthorizationrequired
$150 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Anesthesia Services(all settings)
Covered in full Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Autologous Blood Banking
Preauthorizationrequired
10% Coinsurance afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
155-OA-SGOFFHIXCERT (04/17) HMO Page 5
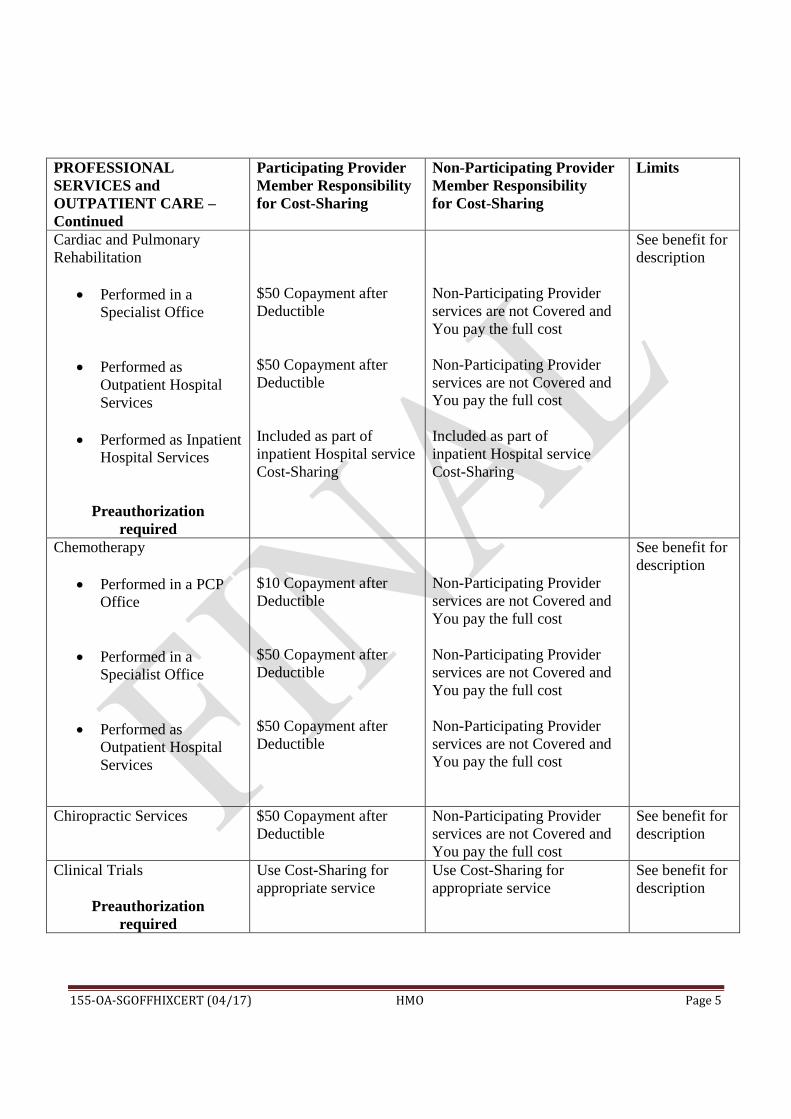
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Cardiac and PulmonaryRehabilitation
Performed in aSpecialist Office
Performed asOutpatient HospitalServices
Performed as InpatientHospital Services
Preauthorizationrequired
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Included as part ofinpatient Hospital serviceCost-Sharing
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Included as part ofinpatient Hospital serviceCost-Sharing
See benefit fordescription
Chemotherapy
Performed in a PCPOffice
Performed in aSpecialist Office
Performed asOutpatient HospitalServices
$10 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Chiropractic Services $50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Clinical Trials
Preauthorizationrequired
Use Cost-Sharing forappropriate service
Use Cost-Sharing forappropriate service
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 6
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Diagnostic Testing
Performed in a PCPOffice
Performed in aSpecialist Office
Performed asOutpatient HospitalServices
$10 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Dialysis
Performed in a PCPOffice
Performed in aSpecialist Office
Performed in aFreestanding Center
Performed asOutpatient HospitalServices
$10 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
$50 copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Dialysisperformed byNon-ParticipatingProviders islimited to ten(10) visits percalendar yearPreauthorization
required
Habilitation Services(Physical Therapy,Occupational Therapy orSpeech Therapy)
Preauthorizationrequired
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Ninety (90)visits percondition, perPlan Yearcombinedtherapies
Home Health Care
Preauthorizationrequired
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Forty (40) visitsper Plan Year

155-OA-SGOFFHIXCERT (04/17) HMO Page 7
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Infertility Services
Preauthorizationrequired
Use Cost-Sharing forappropriate service(Office Visit; DiagnosticRadiology Services;Surgery; Laboratory andDiagnostic Procedures)
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Infusion Therapy
Performed in a PCPOffice
Performed in aSpecialist Office
Performed asOutpatient HospitalServices
Home InfusionTherapy
Preauthorizationrequired
$10 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Inpatient Medical Visits $0 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 8
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Interruption of Pregnancy
Medically NecessaryAbortions
(16)[Elective
Abortions]
Preauthorizationrequired
Covered in full
[$150 Copayment after
Deductible]
Non-Participating Providerservices are not Covered andYou pay the full cost
[Non-Participating Providerservices are not Covered and
You pay the full cost]
Unlimited
[One (1)procedure per
Plan Year]
Laboratory Procedures
Performed in a PCPOffice
Performed in aSpecialist Office
Performed in aFreestandingLaboratory Facility
Performed asOutpatient HospitalServices
$10 Copayment afterDeductible
$10 Copayment afterDeductible
$10 Copayment afterDeductible
$10 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 9
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Maternity and Newborn Care
Prenatal Care Prenatal Care
provided inaccordance with thecomprehensiveguidelinessupported byUSPSTF andHRSA
Prenatal Care that isnot provided inaccordance with thecomprehensiveguidelinessupported byUSPSTF andHRSA
Inpatient HospitalServices and BirthingCenter
Physician andMidwife Services forDelivery
Breastfeeding Support,Counseling andSupplies, includingBreast Pumps
Postnatal Care
Preauthorizationrequired for inpatientservices; breast pump
Covered in full
Use Cost-Sharing forappropriate service(Primary Care OfficeVisit; Specialist OfficeVisit; DiagnosticRadiology Services;Laboratory Proceduresand Diagnostic Testing)
$1,500 Copayment afterDeductible
$150 Copayment afterDeductible
Covered in full
Covered in full
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
One (1) homecare visit isCovered at noCost-Sharing ifmother isdischargedfrom Hospitalearly
Covered forduration ofbreast feeding

155-OA-SGOFFHIXCERT (04/17) HMO Page 10
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Outpatient Hospital SurgeryFacility Charge
Preauthorizationrequired
$150 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Preadmission Testing
Preauthorizationrequired
$0 Copayment, not subjectto Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Prescription DrugsAdministered in Office
Performed in a PCPOffice
Performed in aSpecialist Office
Included as part of thePCP office visit Cost-Sharing
Included as part of theSpecialist office visitCost-Sharing
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Diagnostic RadiologyServices
Performed in a PCPOffice
Performed in aSpecialist Office
Preauthorizationrequired
Performed in aFreestandingRadiology Facility
Preauthorizationrequired
Performed asOutpatient HospitalServices
Preauthorizationrequired
$10 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 11
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Therapeutic RadiologyServices
Performed in aSpecialist Office
Performed in aFreestandingRadiology Facility
Performed asOutpatient HospitalServices
$50 Copayment afterDeductible
$50 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Rehabilitation Services(Physical Therapy,Occupational Therapy orSpeech Therapy)
Preauthorizationrequired
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Ninety (90)visits percondition, perPlan Yearcombinedtherapies.Speech andphysicaltherapy areonly Coveredfollowing aHospital stayor surgery.
Second Opinions on theDiagnosis of Cancer, Surgeryand Other
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Second opinions on diagnosisof cancer are Covered atparticipating Cost-Sharing fornon-participating Specialistwhen a Referral is obtained.
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 12
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Surgical Services(including Oral Surgery;Reconstructive BreastSurgery; Other Reconstructiveand Corrective Surgery; andTransplants)
Inpatient HospitalSurgery
Outpatient HospitalSurgery
Surgery Performed atan AmbulatorySurgical Center
Office Surgery Performed in a
PCP Office
Performed in aSpecialist Office
Preauthorizationrequired
$150 Copayment afterDeductible
$150 Copayment afterDeductible
$150 Copayment afterDeductible
$10 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Alltransplantsmust beperformed atdesignatedFacilities

155-OA-SGOFFHIXCERT (04/17) HMO Page 13
PROFESSIONALSERVICES andOUTPATIENT CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Telemedicine Program Provided by a
TelemedicinePhysician
Provided by aDietitian/Nutritionist
$0 Copayment, notsubject to Deductible
$0 Copayment, notsubject to Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
ADDITIONAL SERVICES,EQUIPMENT andDEVICES
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
ABA Treatment for AutismSpectrum Disorder
Preauthorizationrequired
$10 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Assistive CommunicationDevices for Autism SpectrumDisorder
Preauthorizationrequired
10% Coinsurance afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Diabetic Equipment, Suppliesand Self-ManagementEducation
Diabetic Equipment,Supplies and Insulin(30-day supply)
Diabetic Education
Preauthorizationrequired
$10 Copayment afterDeductible
$10 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Durable Medical Equipmentand Braces
Preauthorizationrequired
10% Coinsurance afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 14
ADDITIONAL SERVICES,EQUIPMENT andDEVICES – Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
External Hearing Aids
Preauthorizationrequired
10% Coinsurance afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Singlepurchase onceevery three (3)years
Cochlear Implants
Preauthorizationrequired
10% Coinsurance afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
One (1) per earper timeCovered
Hospice Care
Inpatient
Outpatient
Preauthorizationrequired
$1,500 Copayment afterDeductible
$50 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Two hundredten (210) daysper Plan Year
Five (5) visitsfor familybereavementcounseling
Medical Supplies
Preauthorizationrequired
10% Coinsurance afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Prosthetic Devices
External
Internal
Preauthorizationrequired
10% Coinsurance afterDeductible
Included as part ofinpatient Hospital Cost-Sharing
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
One (1)prostheticdevice, perlimb, perlifetime withcoverage forrepairs andreplacements
Unlimited;See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 15
INPATIENT SERVICESand FACILITIES
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Inpatient Hospital for aContinuous Confinement(including an Inpatient Stayfor Mastectomy Care, Cardiacand PulmonaryRehabilitation, and End ofLife Care)
Preauthorization required.However, Preauthorization
is not required foremergency admissions.
$1,500 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Observation Stay $150 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Skilled Nursing Facility(including Cardiac andPulmonary Rehabilitation)
Preauthorizationrequired
$1,500 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Three hundredsixty-five(365) days perPlan Year
Inpatient Habilitation Services(Physical, Speech andOccupational Therapy)
Preauthorizationrequired
$1,500 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Sixty (60) daysper Plan Yearcombinedtherapies
Inpatient RehabilitationServices(Physical, Speech andOccupational Therapy)
Preauthorizationrequired
$1,500 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Sixty (60) daysper Plan Yearcombinedtherapies
Speech andphysicaltherapy areonly Coveredfollowing aHospital stayor surgery

155-OA-SGOFFHIXCERT (04/17) HMO Page 16
MENTAL HEALTH andSUBSTANCE USEDISORDER SERVICES
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Inpatient Mental Health Careincluding ResidentialTreatment (for a continuousconfinement when in aHospital)Preauthorization required.However, Preauthorization
is not required foremergency admissions.
$1,500 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Outpatient Mental HealthCare(including PartialHospitalization and IntensiveOutpatient Program Services)
$10 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Inpatient Substance UseServices including ResidentialTreatment(for a continuous confinementwhen in a Hospital)Preauthorization required.However, Preauthorization
is not required foremergency admissions or for
Participating OASAS-certified Facilities.
$1,500 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Outpatient Substance UseServices(including PartialHospitalization, IntensiveOutpatient Program Services,and Medication AssistedTreatment)
$10 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Unlimited; Upto twenty (20)visits per PlanYear may beused for familycounseling
PRESCRIPTION DRUGS
*Certain Prescription Drugs arenot subject to Cost-Sharingwhen provided in accordancewith the comprehensiveguidelines supported by HRSAor if the item or service has an“A” or “B” rating from theUSPSTF and obtained at aparticipating pharmacy.
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits

155-OA-SGOFFHIXCERT (04/17) HMO Page 17
PRESCRIPTION DRUGS –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Retail Pharmacy30-day supplyTier 1
Tier 2
Tier 3
If You have an EmergencyCondition, Preauthorization isnot required for a five (5) dayemergency supply of aCovered Prescription Drugused to treat a substance usedisorder, including aPrescription Drug to manageopioid withdrawal and/orstabilization and for opioidoverdose reversal.
$10 Copayment, notsubject to Deductible
$30 Copayment afterDeductible
$70 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Mail Order PharmacyUp to a 90-day supplyTier 1
Tier 2
Tier 3
$25 Copayment, notsubject to Deductible
$75 Copayment afterDeductible
$175 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription
Enteral FormulasTier 1
Tier 2
Tier 3
$10 Copayment, notsubject to Deductible
$30 Copayment afterDeductible
$70 Copayment afterDeductible
Non-Participating Providerservices are not Covered andYou pay the full cost
See benefit fordescription

155-OA-SGOFFHIXCERT (04/17) HMO Page 18
WELLNESS BENEFITS Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Gym Reimbursement Up to $200 per six (6)month period; up to anadditional $100 per six(6) month period forSpouse;not subject to Deductible
Up to $200 per six (6) monthperiod; up to anadditional $100 per six (6)month period for Spouse;not subject to Deductible
Up to $200 persix (6) monthperiod; up toan additional$100 per six(6) monthperiod forSpouse
VISION CARE Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Pediatric Vision Care
Exams
Lenses and Frames
Contact Lenses
$10 Copayment, notsubject to Deductible
10% Coinsurance, notsubject to Deductible
10% Coinsurance, notsubject to Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost One (1) exam
per twelve (12)month period;One (1)prescribedlenses andframes pertwelve (12)month period
Adult Vision Care
Exams
Lenses and Frames
Contact Lenses
$10 Copayment, notsubject to Deductible
10% Coinsurance, notsubject to Deductible
10% Coinsurance, notsubject to Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost One (1) exam
per twelve (12)month period;One (1)prescribedlenses andframes pertwelve (12)month period

155-OA-SGOFFHIXCERT (04/17) HMO Page 19
DENTAL CARE Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Pediatric Dental Care
Emergency DentalCare
Preventive DentalCare
Routine Dental Care
Major Dental Care(Endodontics,Periodontics,Prosthodontics andOral Surgery)
Orthodontics
Major Dental Careand OrthodonticsrequirePreauthorization
$10 Copayment, notsubject to deductible
$0 Copayment, notsubject to Deductible
$10 Copayment, notsubject to Deductible
$50 Copayment, notsubject to Deductible
$50 Copayment, notsubject to Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
One (1) dentalexam andcleaning persix (6) monthperiod
Full mouth x-rays orpanoramic x-rays at thirty-six (36) monthintervals andbitewing x-rays at six (6)monthintervals

155-OA-SGOFFHIXCERT (04/17) HMO Page 20
DENTAL CARE –Continued
Participating ProviderMember Responsibilityfor Cost-Sharing
Non-Participating ProviderMember Responsibilityfor Cost-Sharing
Limits
Adult Dental Care
Emergency DentalCare
Preventive DentalCare
Routine Dental Care
$10 Copayment, notsubject to Deductible
$0 Copayment, notsubject to Deductible
$10 Copayment, notsubject to Deductible
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
Non-Participating Providerservices are not Covered andYou pay the full cost
One (1) dentalexam andcleaning persix (6) monthperiod
Full mouth x-rays orpanoramic x-rays at thirty-six (36) monthintervals andbitewing x-rays at six (6)monthintervals
All in-network Preauthorization requests are the responsibility of Your Participating Provider. You will notbe penalized for a Participating Provider’s failure to obtain a required Preauthorization. However, ifservices are not Covered under the Certificate, You will be responsible for the full cost of the services.

Group Health Incorporated (GHI), HIP Health Plan of New York (HIP), HIP Insurance Company of New York and EmblemHealth Services Company, LLC are EmblemHealth companies. EmblemHealth Services Company, LLC provides administrative services to the EmblemHealth companies. 10-9127 6/18
ATTENTION: Language assistance services, free of charge, are available to you. Call 1-877-411-3625 (TTY/TDD: 711). Español (Spanish) ATENCIÓN: Usted tiene a su disposición, gratis, servicios de ayuda para idiomas. Llame al 1-877-411-3625 (TTY/TDD: 711).
中文 (Traditional Chinese) 注意:我們免費提供相關的語言協助服務。請致電 1-877-411-3625 (TTY/TDD: 711)。
Pусский (Russian) ВНИМАНИЕ! Вам доступны бесплатные услуги переводчика. Звоните по тел. 1-877-411-3625 (служба текстового телефона TTY/TDD: 711).
Kreyòl Ayisyen (Haitian Creole) ATANSYON: Gen sèvis èd nan lang gratis ki disponib pou ou. Rele nimewo 1-877-411-3625 (TTY/TDD: 711).
한국어 (Korean) 주의: 귀하에게 언어 지원 서비스가 무료로 제공됩니다. 1-877-411-3625(TTY/TDD: 711)번으로 전화하십시오.
Italiano (Italian) ATTENZIONE: sono disponibili servizi gratuiti di assistenza linguistica. Chiami il numero 1-877-411-3625 (TTY/TDD: 711).
(Yiddish) אידיש 1-877-411-3625 רופט. זיינען דא צו באקומען פאר אייך, אהן קיין פרייז, שפראך הילף סערוויסעס: אכטונג
(TTY/TDD: 711).
বাাংলা (Bengali) মন োন োগ দি : ভোষো সহোয়তো পদিনষবোগুদি আপ োি জ য দব োমূনিয উপিব্ধ আনে। 1-877-411-3625(TTY/TDD: 711) ম্বনি ফ ো করু ।
Polski (Polish) UWAGA: dostępna jest bezpłatna pomoc językowa. Prosimy zadzwonić pod numer 1-877-411-3625 (TTY/TDD: 711).
(Arabic) العربية . (TTY/TDD: 711)أو 3625-411-877-1 الرقمعلى اتصل ،رجى الانتباه: تتوفر لك خدمات المساعدة اللغوية مجانا ي
Français (French) ATTENTION : une assistance d’interprétation gratuite est à votre disposition. Veuillez composer le 1-877-411-3625 (TTY/TDD : 711).

(Urdu)اردو بان لیے کے آپ دیں: وجہ یں۔ کال پر (TTY/TDD: 711) 1-877- 411-3625 ہیں۔ دستیاب مفت ،خدمات کی اعانت متعلق سے ز کر
Tagalog (Tagalog) NANANAWAGAN NG PANSIN: Mayroon kang magagamit na mga serbisyo para sa tulong sa wika nang walang bayad. Tawagan ang 1-877-411-3625 (TTY/TDD: 711).
Ελληνικά (Greek) ΠΡΟΣΟΧΗ: Διατίθενται για σας υπηρεσίες γλωσσικής βοήθειας, δωρεάν. Καλέστε το 1-877-411-3625 (για άτομα με προβλήματα ακοής (TTY/TDD): 711).
Shqip (Albanian) VINI RE: Shërbime ndihmore për gjuhën, falas, janë në dispozicionin tuaj. Telefononi në 1-877-411-3625 (TTY/TDD: 711).
NOTICE OF NONDISCRIMINATION POLICY EmblemHealth complies with Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. EmblemHealth does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
EmblemHealth: Provides free aids and services to people with disabilities to
help
– Qualified sign language interpreters
– Written information in other formats (large print, audio, accessible electronic formats, other formats)
Provides free language services to people whose first language is not English, such as: – Qualified interpreters
– Information written in other languages
If you need these services, please call member services at 1-877-411-3625 (TTY/TDD: 711).
If you believe that EmblemHealth has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with EmblemHealth Grievance and Appeals Department, PO Box 2844, New York, NY 10116, or call member services at 1-877-411-3625. (Dial 711 for TTY/TDD services.) You can file a grievance in person, by mail or by phone. If you need help filing a grievance, EmblemHealth’s Grievance and Appeals Department is available to help you. You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office of Civil Rights electronically through the Office of Civil Rights Complaint Portal, available at ocrportal.hhs.gov/ocr/portal/lobby.jsf or by mail or phone at U.S. Department of Health and Human Services, 200 Independence Avenue SW, Room 509F, HHH Building, Washington, DC 20201; 1-800-368-1019, (dial 1-800-537-7697 for TTY services). Complaint forms are available at hhs.gov/ocr/office/file/index.html.





























