Embed Size (px)
Citation preview

2019
Health Workforce Education and Training to Recognize and Support
Family Caregivers of Older Adults Symposium March 14-15, 2019: Summary Report
Sponsors: The symposium was funded by a Canadian Institutes of Health Research Planning and
Dissemination Grant and The Covenant Health Network of Excellence in Seniors Health and
Wellness.

1 | P a g e
NETWORK OF EXCELLENCE IN SENIORS’ HEALTH AND WELLNESS
The Network gives voice to seniors through active engagement and makes their priorities, its priorities. It
invests in pragmatic research projects through its Innovation Fund grants and strategic initiatives, and then
spreads the
knowledge gained
with targeted
communications to
expand uptake and
increase impact.
We partner with
seniors, families,
experts and staff to
design, evaluate,
and share ideas
that enable seniors
to live fully, as
active and
connected
members of their
communities.
Caregivers and Caring: A Strategic Focus of the Network
The Covenant Health Network of Excellence in Seniors’ Health and Wellness has engaged 400 multi-level
interdisciplinary stakeholders, including family caregivers, to discuss how to support for family caregivers of
seniors in the last five years. The first two meetings Supporting Family Caregivers of Seniors: Improving Care
and Caregiver Outcomes (2014) and Supporting Family Caregivers of Seniors within Acute and Continuing
Care Systems (2016) found stakeholders shining a light on two key health system issues: 1) the system is
complex, fragmented and challenging for caregivers to navigate and 2) health providers are ill-equipped and
under-resourced to provide support caregivers [1 2]. Stakeholders recommended earlier identification of
caregivers, education and skills training for health care providers and system changes aimed at providing
appropriate evidence-informed caregiver supports.
In 2017, stakeholders again highlighted the lack of orientation and education for health providers about
family caregivers and the lack of standardized processes for assessing caregivers’ stressors or needs at the
Fostering Resilience in Family Caregivers of Seniors in Care symposium [3 4]. They recommended
development of distinct education and training programs for health providers. Thus, the Healthcare
Workforce Training in Supporting Family Caregivers of Seniors in Care Symposium (2018) engaged 40 family
caregivers and stakeholders in a cross-sectoral dialogue about specific education and training topics that
would address caregiver needs [5]. Participants identified six issues as essential to health provider training

2 | P a g e
to support family caregivers: understanding the family caregiver role, caregiver-engaged patient-centered
care, effective engagement with family caregivers, caregiver coaching, challenging the status quo, and
fostering family caregivers’ resilience.
The results of these meetings [1 3-7], research evidence on the positive effects of training [8 9], as well as
recent calls for the development of Caregiver-Centered Care Competencies for the health workforce [10 11]
substantiated our goal to develop competencies for health providers and then competency-based resources
for training the health workforce to recognize and support family caregivers of seniors. In fact, American
caregiving scholar Schulz and colleagues (2018) came to a similar conclusion: “Educational and workforce
development reforms are needed to enhance the competencies of healthcare and long-term care service
providers to effectively engage caregivers” p. S36).
Our new objectives were twofold:
1. Develop Caregiver-Centered Care Competencies specific to health providers who interact with
family caregivers
2. Develop and evaluate the impacts of competency-based training resources for the health
workforce to recognize and support family caregivers of seniors.
PRE-SYMPOSIUM PREPARATION
There were two main stages in development of a Caregiver-Centered Care Competencies: identification of
potential competency domains and indicators and a four-phased Modified Delphi validation process. In the
absence of best practices or empirical evidence for the competency indicators for caregiver-centered care,
the first stage involved thematic analysis of stakeholder discussions at the Healthcare Workforce Training in
Supporting Family Caregivers of Seniors in Care Symposium[5] and concept mapping of our stakeholder
engagement meetings to identify the key competency domains for caregiver support. Competency domains
are the descriptive framework, the required elements and outcomes that define the knowledge, skills,
attitudes, values, and behaviors for caregiver-centered care practices [12 13]. Six competency domains
were identified: (1) Understanding and Recognizing the Caregiver Role, (2) Communicating with Family
Caregivers, (3) Partnering with Family Caregivers, (4) Fostering Resilience Among Caregivers, (5) Navigating
Health and Social Systems and Accessing Resources, and (6) Enhancing the Culture and Context of Care.
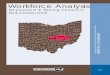
A literature review was used to identify potential competency indicators in each domain. Competency
indicators, also called functional or behavioral competencies, outline the specific knowledge, skills, and
abilities required by the health workforce to provide caregiver-centered care in the context of their role [12
13]. Figure 1 shows the competency framework development process.

3 | P a g e
Figure 1: Competency Development Process
THE MARCH 14-15 SYMPOSIUM: HEALTH WORKFORCE EDUCATION AND TRAINING TO RECOGNIZE AND SUPPORT FAMILY CAREGIVERS OF OLDER ADULTS
The objectives of the March 14-15, 2019 symposium were to:
1. Validate the competency indicators;
2. Identify education/training modalities;
3. Map strategies for implementation and dissemination;
4. Generate evaluation and research plans.

4 | P a g e
Fifty stakeholders including family caregivers, health care providers, health and community organization
leaders, policy influencers and makers, and academics from colleges and universities attended the meeting.
Invited experts presented on first-hand caregiving experiences, the need for caregiver- centered
competency-based education for the health workforce, effective models and modalities for education and
training, the barriers and facilitators to spreading and scaling effective innovations, and the potential for
research and evaluation. Stakeholders participated in four breakout sessions to validate the competency
indicators, identify potential education and training modalities, map strategies for implementation, and
generate evaluation and research plans. The groups of six to nine people were guided by expert facilitators
equipped with guiding questions on the topic at hand. The sessions were digitally recorded, transcribed
verbatim and qualitative content analysis was used to identify the key themes.
BREAKOUT SESSION 1: CONTENT VALIDATION OF CAREGIVER-CENTERED CARE COMPETENCIES DOMAIN AND INDICATORS
The caregiver-centered care competency
domains and competency indicators for
the Health Workforce were verified by
symposium participants.
The Caregiver-centered Care Comptency
Framework
Six competency domains highlight the
knowledge, skills, attitudes, and values
that shape caregiver-centered care
practice. While they are portrayed
individually, in practice the domains are
interdependent.
The six competency domains are:
A. Recognizing the Caregiver Role
B. Communicating with Family
Caregivers
C. Partnering with Family Caregivers
D. Fostering Resilience in Family
Caregivers
E. Navigating the Health and Social
Systems and Accessing Resources
F. Enhancing the Culture and Context of Care

5 | P a g e
Competency Domain A: Recognizing the Caregiver Role Competency Indicators
1. Demonstrates understanding of the value of family caregivers’ contributions to society and the
healthcare system.
2. Demonstrates knowledge of the consequences of caregiving on family caregivers.
3. Demonstrates awareness of, and identifies the family caregivers, their roles and responsibilities in
supporting the care recipient.
4. Understands the diversity among family caregivers (e.g., age, gender, culture, where they live, work).
Competency Domain B: Communicating with Family Caregivers Competency Indicators
1. Communicates in a manner that demonstrates respect, empathy, and compassion toward the family
caregiver.
2. Demonstrates ability to listen actively and respectfully to family caregivers.
3. Provides timely information to family caregivers in ways they will understand.
4. Supports coordinated care by providing consistent documentation and information amongst
providers and family caregivers.
Competency Domain C: Partnering with Family Caregivers. Competency Indicators
1. Understands the benefits of including family caregivers on the care team.
2. Establishes collaborative relationships with family caregivers.
3. Includes family caregiver’s knowledge of the care recipients in assessments and care planning.
4. Understands conflicts and works to de-escalate conflict.
Competency Domain D: Fostering Resilience in Family Caregivers Competency Indicators
1. Identifies and assesses family caregiver’s needs and goals on an ongoing basis.
2. Recognizes the dynamics of the caregiver- care recipient relationship.
3. Enhances family caregivers’ skills and abilities through education and support.
4. Promotes the health and wellbeing of family caregivers and encourages self-care.
Competency Domain E: Navigating the Health and Social Systems and Accessing Resources Competency Indicators
1. Works collaboratively with caregivers to access applicable supports in a timely manner.
2. Communicates with, and makes referrals to other providers, in accordance with family caregivers’
preferences.
3. Works with family caregivers to overcome barriers to access services and supports.

6 | P a g e
Competency Domain F: Enhancing the Culture and Context of Care Competency Indicators
1. Recognizes that care and caregiving are affected by societal views (e.g., ageism, stigma,
discrimination).
2. Models caregiver-centered care.
3. Engages in self-reflection to improve interactions with, and support of, family caregivers.
BREAKOUT SESSION 2: IDENTIFY EDUCATION AND TRAINING MODALITIES
The competencies set out what the health workforce need to know, so the overarching question is for this
conversation circle was: “How should caregiver-centered care education be delivered?”
1. Who are the learners?
• Everyone in the health workforce who interacts with family caregivers needs to have some level
caregiver-centered care education. This included people in diverse:
o settings such as primary care, emergency and acute care, homecare, supportive housing and
long-term care; and,
o roles/ levels of influence like policy makers/ organization leaders; regulated and unregulated
health providers, and janitors, receptionists, and ward clerks in health workforce roles.
o points in their career such as undergraduates, graduates, and those needing caregiver-
centered care competency refreshers.
“I think anybody that intersects at all with a family or resident or patient, need some level
of understanding of the philosophy and what we're trying to do, the environment we're
trying to create.”
2. How do we want them to learn? What is the best way to teach competencies?
• The competency domains, competency indicators, and level of learning will need be tailored to
learner’s role. Groups all recommended there were core competencies that everyone should be
exposed to and then a curriculum tailored for specific roles.
“Exactly. There's a core, some basic principles that are common to everybody, and then
there need to be some that are specific, almost like a slice of the pie that's relative to the
policy decision makers, physicians, nurses, case managers.”
“You might want your unregulated workforce to have a level of awareness but then your
regulated workforce to be educated to a greater skill level or knowledge level, and then
the policy makers might need an awareness but something else as well.”
• The example one group used to illustrate education should be tailored to particular roles was policy
makers. They suggested policymakers would benefit from training about two domains: Competency

7 | P a g e
Domain A: Recognizing the Caregiver Role and leading change guidance of Competency Domain F:
Enhancing the Culture and Context of Care whereas homecare case managers need the practical
skills
• Professional societies, accreditation bodies, academics in educational institutions, and employers
such as Alberta Health Services and Covenant Health should support education and training
development. Five of the six groups thought champions played critical roles in leading change.
“Many people here are already committed. So at least for Alberta, you've got a group of
people at that level who are probably champions already. In other provinces, we don't
have that yet, at least not here in this setting.”
• Stakeholders suggested the best delivery modalities would be combination of online and face-to-
face. Several people suggested webinars were a good interactive format especially for engaging
rural and remote learners.
“For our staff, best education that happens is a combination of doing a module on the
computer where the information is provided, but then there's hand some hands-on
learning that happens with the care that needs to be provided. That seems to be the most
effective way to help people to shift how they're doing things. But then for sustainability, it
has to be part of the essential education for home care, for our health care aides and even
our nurses. Otherwise you could teach it in post secondary, but if it's not sustained in the
places where they go to work, it's not going to hold.”
“Some of these competencies and domains lend themselves to different modalities.
Absolutely. Just infrastructure wise, you'd want to build online and face-to-face at the
same time.”
3. Who is best equipped to deliver the learning? What skills and attributes do they need?
• Participants asserted that the facilitator should be a caregiver-centered care champion, an
enthusiastic train the trainer, who would model change in education and as a leader in the field.
“So yeah, a champion is essentially a train the trainer. They would also be another way of
really getting that momentum in there and some buy-in.”
“And I like the champion model that we heard about. I think that would help with moving
things faster through the system. We need those champions as people that will buy-in and
really move something forward.”
• Caregivers should be involved as co-facilitators, or their stories/ experiences should be included in
video vignettes, case studies, or role plays.

8 | P a g e
“Well, or you do it as a dyad model where you have the caregivers and the educators that
actually have content and have been trained on how to involve caregivers’ stories, but it is
best if you do it together.”
• The facilitator/ educator must be an excellent educator. Participants regarded the facilitator as
critical to ensuring the curriculum gets adapted to the learner’s context and roles, and then can
engage the students in program delivery.
• Participants thought that while Alberta Health Services Essential Education or Covenant Health’s
CLIC online modules could be useful to reach many people, having a course facilitator would
improve learning outcomes.
4. What education and training formats might be useful in your setting?
• There was general agreement that program duration and module length needed to be customized
to the learners’ roles and work context. Participants believed there needed to be adequate time to
cover the competency domains that learners needed. They expected that regulated health providers
working directly with caregivers would need greater duration, perhaps ½ day or a full day. Programs
for unregulated workforce, such as health care aides in homecare and continuing care could be
offered in shorter bites of 5 to 30 minutes.
• Participants brought up a variety of formats including combination of theoretical and experiential, virtual reality, storytelling, case-based learning simulation, reflection, feedback, assignments and readings. Videos, simulation, role play, and case-based learning were thought to produce the best learning outcomes, but several participants also noted these could be more expensive to implement.
5. In your experience, what are the facilitators and barriers to education and training?
Participants identified the same number of facilitators and barriers to caregiver-centered care education.
• Facilitators included: people wanting to do a good job/ being committed to supporting case managers, monitoring and policy modeled after reducing antipsychotics, building caregiver-centered care into workplace processes; employer buy-in, accreditation/certification, including Caregiver-Centered Care Competencies into professional competencies, evaluation to showcasing the benefits of training on staff turnover, staff satisfaction and the quality of care,
“You know, our licensing body for nurses, in Alberta, determines competencies, right?
Those competencies there are in undergraduate programs. Family-centered care is a main
component, and then under there and then on the aging is about health caregivers. So,
there's pieces there, and it's embedded in the program. If you develop good resources for
faculty to use in their courses, they will use them.”
• Time and money were the barriers mentioned most frequently, followed by already jam-packed undergraduate curricula, policy and attitudes that focus on serving patients not caregivers, the difficulty of training the health workforce to navigate the complex siloed health system, too much

9 | P a g e
being expected of the health system, unions, and undergraduates lack of interest in older people.
Speaker 2: “You're asking me to backfill and I am already short-staffed.”
Speaker 1: “And you're not giving me the money for training or staffing.”
BREAKOUT SESSION 3: MAP STRATEGIES FOR IMPLEMENTATION AND DISSEMINATION
This breakout session was geared to mapping the strategies for implementing and disseminating training
resources for the health workforce. The overarching question was: “How do we begin to educate the health
workforce?”
1. What are the most important steps we need to take to implement and disseminate these resources?
Stakeholders in all six groups agreed that a primary step was getting “buy-in” for caregiver- centered
care from individuals, leadership, and organizations. There were two main themes to getting buy-in: 1)
Making the case/ Seeing the need; 2) Ensuring that the educational product is high-quality and meets
needs of individuals and organizations.
Some stakeholders suggested just building the education and then “they will come” but the majority
indicated that a better pathway was getting buy-in from one or two key organizations to develop and
refine a high-quality educational product.
Making the case. Participants advised getting commitment at multiple levels: governmental policy,
health system, universities and college programs that educate health providers, professional regulatory
colleges, health and community organization leadership, and caregivers.
It comes from the bottom, percolates up, and comes from the top. So, you have to work at
all these levels. It seems you have got some policy and momentum going. Those are the
guys you start marketing to.
• Policies --work to get caregiver-centered care into government and organization policies such as the
rights-based approach taken in Scotland, an Alberta caregiver strategy/ framework, and/or
standards of care. One group recommended advocating for a Strategic Clinical Network for
Caregivers.
• College and university engagement—academics suggested that although curriculums are “jam-
packed”, there are opportunities to introduce caregiver-centered care.
Speaker 1: So, the competencies are really important. But then, if the educational
institutions don't pick up the competencies and the health system doesn't pick up the
competencies, how impactful will they be? So is that a step of work that needs to be done
as well.

10 | P a g e
Speaker 2: I think that's where you, you continue to use the collaborative model that
you're already using where the post secondary institutions and the instructors at those
institutions are part of building the educational resources and the competencies. You
know, it makes it a lot easier for them if there are good educational resources.
• In-service training—community and health system leaders said they were committed to education
and could see direct benefits of education for the organization, staff, clients, and caregivers. They
wanted education to change attitudes and practices. Therefore, they recommended education for
the whole organization and utilizing champions within the organization as facilitators.
We need to change attitudes. If you have online modules, that's fairly easy to make
available to people, but we know that they don't necessarily take much away from that. So
if we have online resources, but we actually train a facilitator in each of the organizations
to walk through people using those modules, that's different, because if they have
discussions, so if it's online modules together with a facilitator discussion thing and then a
place where they can set goals together as a group and move forward with those goals
and then evaluate how they're doing, that's more likely to change attitudes.
• Involving caregivers—All groups recommended caregiver engagement.
I do think there is power in talking to the public and to giving caregivers, like having the
caregiver, because right now with person centered care, or whatever term we use, patient-
centered care, we're having caregivers and patients on all kinds of decision-making
boards. They're in the strategic clinical networks. They're supposed to be everywhere. And
there's a collective voice and it's in the public so they know what to pick up and bring
forward, I think we are listening to patients and families and caregivers now. That's part of
who we are to be.
Ensure the educational product is “high-quality”. There was general agreement that design of the
education was critical to buy-in. Evaluation of participant satisfaction and changes in attitudes and practices
were put forth as key elements of high-quality education. Participants recommended modeling education
on successful programs.
I think about successful trainings and the trainings that have been really successful, like
ASIST comes to might, right? Just a completely well adopted training that people
consistently evaluate very well. They take those skills and they use them in practice. We
can look at those examples, and I'm sure there's others that aren't coming to my mind.
2. What factors will make it easy to implement and disseminate these resources?
The facilitators were: partnerships and collaboration, leadership commitment to education, champions
within the organization, and education that is easy to deliver within the organization context and evaluates
well.

11 | P a g e
• Stakeholders credited development of caregiver-centered care for the health workforce to the
relationships developed through partnerships and collaboration. They recommended ongoing
collaboration.
• Commitment from organization leaders that facilitated a whole organization approach to change
ensures that learners are supported to put education into practice.
• Champions, staff at all levels who are passionate about the innovation, lead the spread process.
Stakeholders saw education as the pathway to develop multiple organizational champions within
the organization. They thought champion’s ownership and energy helped to facilitate innovation
spread, scale, and sustainability.
• Participants wanted education that would fit or be adapted to their local context. They wanted
education to be effective at changing attitudes and the culture of care around caregivers.
I think we've got to be innovative. We've got to do something that makes the difference. If
we have somebody for 15 minutes, we've got to make 14 of those minutes really make a
difference? We should get really innovative and try to make people understand in their
soul that caregivers are vital somehow.
3. What factors will make it challenging to implement and disseminate these resources?
Barriers included: the breadth of the challenge, silos and fragmentation, the difficulty evaluating/
demonstrating economic impacts, and funding.
• Educating all the people who interact with caregivers is a huge challenge. Participants talked about
starting with providers with the most influence as the way to overcome this challenge.
• Homecare, primary care, and undergraduate education were promising target populations. The
Care of the Elderly Physicians and the pilot caregiver support project in Edmonton Home Living
were used as examples of strengths. Every group also warned not to overlook training for the
community workforce.
• Participants were concerned that silos and fragmentation within the health system, between the
health and community systems, and competition between organizations would impede spread and
scale. They talked about the difficulty for health providers to navigate the health system as well as
the problems sharing caregiver’s information with community organizations. Two participants
though competition between organizations could prevent collaboration.
Well, there are so many organizations that deal with caregivers. In terms of caregiver
groups in mental health and addictions there’s a major bucket but they are all represented
by different organizations with different pieces of the pie. It's like we have caregivers and
mood disorders, eating disorders, schizophrenia society, all of which have major voice and
then there's also substance abuse and there's some real kind of like infighting between
them and different kind of philosophical orientations.

12 | P a g e
• Participants warned of the difficulty evaluating education, particularly demonstrating practice
changes or the economic impacts of education.
• All six groups spoke about finding adequate funding for developing and implementing education as a
barrier.
BREAKOUT SESSION 4: GENERATE EVALUATION AND RESEARCH PLANS
This breakout session considered evaluation and research of the impacts of health workforce education and
training. The overarching question was: “How do we evaluate the impacts of health workforce education?”
Our systematic review of the components of effective health workforce education revealed that lack of an evaluation framework was a significant weakness in educational interventions. Education intervention planners were not systematically considering the impacts of education at various levels.
At the symposium, we provided participants with the Kirkpatrick Barr four level framework for evaluating health workforce education programs to facilitate conversations for measuring educational impacts
1. What impacts should we expect from a health workforce trained to provide caregiver-centered care?
Two themes ran through discussions in all six groups: 1) changing attitudes about care and caregiving and 2)
demonstrating relational behaviors. Participants acknowledged that increased knowledge and skills were
important impacts but thought that changing attitudes should be the key outcome of education.
Attitude of management types has been more of a problem than the support. I understand
it's their job to do what the policies are that's their job, but if the underlying attitude
doesn't change it doesn’t matter if they know the policy or passed the test.
I think from a healthcare provider perspective, as an RN, I think that attitude change is,
"I'm not just responsible for the patient, I'm responsible for the patient and the caregiver,
to ensure that I'm considering their perspectives, their needs, as well." And I think an

13 | P a g e
attitude change, like you speak about the transition, and the yearly meeting, and instead
of saying in my head, "Oh, this is the fifth interdisciplinary conference I've got today," this
is the one for that family. This is the one time this year that they're meeting with
everybody.”
One provider wanted competency-based health workforce education to achieve an attitudinal cultural
change:
Speaker 4: We train our professionals to see cure, technology, emergency and all that kind
of stuff as something exciting, and actually, giving care properly is a highly skilled thing to
do. And I don't think we value it enough in our society. So, I would like our professionals to
value care as much as they do cure.
The second theme was health providers behaviors, the demonstration of changes in knowledge, skills and
attitudes would have positive impacts for family caregivers, care-recipients, health providers, and on the
quality of care. One stakeholder referred to this as “demonstrable relationality”.
There is demonstrable relationality. There are personalized care plans that are evident for
both the care recipient and the carer. There is an openness and more responsive two-way
communication and there is a communication plan that is fluid. There is flexibility within
the system to be responsive to caregiver needs. The quality of care remains as good as it is
and has an added enhancement of a relational dimension. The satisfaction in the
workplace and the satisfaction by both carers and recipients is increased. People feel that
they are validated and have a sense of place. The carer feels like they have a sense of
place on the team, and that isn't even questioned any longer.

14 | P a g e
The potential impacts are included in the figure below:
HOW WOULD WE MEASURE THE IMPACTS OF HEALTH WORKFORCE EDUCATION?
Participants recommended that we focus on measuring changes with mixed methods to capture the complexity. Academics were asked if there were ways to measure changes in attitudes and behaviors. Several scales were recommended, and one academic suggested that one research project could be developing and validating a caregiver-centered care education scale.
Four groups recommended looking to successful training programs currently in use for formats and even modules aligned with the competencies e.g., Applied Suicide Intervention Skills Training [ASIST] https://edmonton.cmha.ca/programs-services/applied-suicide-intervention-training-asist/, interdisciplinary training or communication modules. One participant mentioned that Dr. Claire Surr had talked about best practices in dementia education in Calgary and recommended that the research team look at her “'What

15 | P a g e
works' in dementia education and training?” resources: https://www.leedsbeckett.ac.uk/school-of-health-and-community-studies/what-works/.
Stakeholders wanted caregivers to continue to be included as integral partners in design research and
evaluation:
I guess what I'm getting at is that caregivers should continue be a big part of the decision-
making as to which competencies are important, reviewing the education, and approving
the resources or not. The research on education. I think caregivers should have a big say in
that as well.

16 | P a g e
ACKNOWLEDGEMENTS
The Network is grateful to everyone who invested their time, knowledge, and expertise to the symposium.
Our Speakers
Sean Chilton Linda Chow-Turner Brenda Bell Dr. Ann-Margriet Pot
Dr. Rhoda MacRae Dr. Jenny Ploeg Dr. Paul Williams
The Research Team
Jasneet Parmar, MBBS, MCFP(CAC) MSc. Medical Director, Covenant Health – Network of Excellence in Seniors' Health and Wellness, Edmonton Medical Lead, Home Living and Transitions, Alberta Health Services – Edmonton Zone Continuing Care Associate Professor, Department of Family Medicine, University of Alberta Suzette Brémault-Phillips, PhD Associate Professor, Occupational Therapy, University of Alberta Consultant, Spiritual and Mental Fitness and Resilience, Canadian Armed Forces, Edmonton Wendy Duggleby, PhD, RN Professor and Associate Dean of Research, Nursing Research Chair in Aging and Quality of Life, Director of Innovations in Seniors' Care Research Unit, Faculty of Nursing, University of Alberta Jayna Holroyd-Leduc, MD, FRCPC Professor and Section of Geriatric Medicine, Department of Medicine, Cumming School of Medicine, University of Calgary Brenda Strafford Foundation Chair in Geriatric Medicine, University of Calgary Medical Director, Specialized Geriatric Services, Calgary Zone, Alberta Health Services Anne Margriet Pot, PhD Senior Health Adviser, Ageing and Life-Course, World Health Organization (WHO) Professor, Clinical Geropsychology, Department of Clinical Psychology, VU University, Amsterdam

17
The CIHR Planning Grant Team
Brenda Bell BEd. Family Caregiver Carleen Brenneis, MHSA, RN Dennis Cleaver, MHSA Laura Krefting, PhD, Family Caregiver Bonnie Dobbs, PhD Vivian Ewa, MBBS, CCFP(COE), MMedEd, FCFP, FRCP(Edin) Konrad Fassbender, PhD Laura Forsyth Paulette Gelinas, Family Caregiver Carmen Grabusic, MA Anwar Haq, PhD, MBA, MPP Arlene Huhn
Wonita Janzen, PhD Rhoda MacRae, PhD Jennifer Mah, MN Karen McDonald, MBA Anita Murphy, CMA Jenny Ploeg, PhD, RN Cheryl Pollard, PhD, RN, RPN Kara Schick-Makaroff, PhD, RN Sandy Sereda, BFA Valerie Smith, MD, FCFP, DipCOE Peter George Tian, MD, MPH Jeanne Weis, MN, RN Beth Wilkey, MN, RN

18
References
1. Charles L, Brémault-Phillips S, Parmar J, Johnson M, Sacrey LA. Understanding How to Support Family Caregivers of Seniors with Complex Needs. Canadian Geriatrics Journal 2017;20(2):75-84 doi: 10.5770/cgj.20.252. 2. Parmar J, Jette N, Brémault-Phillips S, Holroyd-Leduc J. Supporting people who care for older family members. CMAJ 2014;186(7):487-88 doi: 10.1503/cmaj.131831 3. Parmar J, Torti J, Bremault-Phillips S, Charles L, Chan K, Tian PGJ. Supporting Family Caregivers of Seniors Within Acute and Continuing Care Systems. Canadian Geriatrics Journal 2018;21(4):292-96 doi: 10.5770/cgj.21.317. 4. Parmar J, Torti JM, Babiuk J-A, Bremault-Philips S, Charles L, Anderson S. Fostering reslience in family caregivers of seniors in care Journal of Gerontological Nursing Submitted 5. Fisher Rl, Brémault-Phillips S, Parmar J, et al. Healthcare workforce training to effectively support family caregivers of seniors Canadian Geriatrics Journal Submitted 6. Holroyd-Leduc JM, McMillan J, Jette N, et al. Stakeholder Meeting: Integrated Knowledge Translation Approach to Address the Caregiver Support Gap. Canadian Journal on Aging-Revue Canadienne Du Vieillissement 2017;36(1):108-19 doi: 10.1017/s0714980816000660 7. Parmar J, Charles L, Chan K, et al. Supporting family caregivers of seniors within acute and continuing care systems. 2016. http://seniorsnetworkcovenant.ca/wpcontent/uploads/2017/09/Supporting-Family-Caregivers-of-Seniors-within-Acute-and-Continuing-Care-Systems-Conversation-Circle-Summary-Report-2016-Dr.-Jasneet-Parmar.pdf. 8. McMillan SS, Kendall E, Sav A, et al. Patient-centered approaches to health care: A systematic review of randomized controlled trials. Medical Care Research and Review 2013;70(6):567-96 doi: 10.1177/1077558713496318 9. Brookman C, Jakob L, Decicco J, Bender D. Client-centred care in the canadian home and community sector : A review of key concepts. 2011. https://www.saintelizabeth.com/getmedia/4aba6e8e-0303-4b9c-9117-a8c22a43f8bd/Client-Centred-Care-in-the-Canadian-Home-and-Community-Sector.pdf.aspx. 10. Badovinac LM, Nicolaysen L, Harvath TA. Are we ready for the CARE Act?: Family caregiving education for health care providers. Journal of Gerontological Nursing 2019;45(3):7-11 doi: 10.3928/00989134-20190211-02 11. Schulz R, Beach SR, Friedman EM, Martsolf GR, Rodakowski J, Everette James A. Changing Structures and Processes to Support Family Caregivers of Seriously Ill Patients. Journal of Palliative Medicine 2018;21(S2):S36-S42 doi: 10.1089/jpm.2017.0437 12. Mitchell T. Guide for writing functional competencies. Baltimore, MD: University of Baltimore, 2005:31. 13. Fisher C, Cusack G, Cox K, Feigenbaum K, Wallen GR. Developing Competency to Sustain Evidence-Based Practice. The Journal of nursing administration 2016;46(11):581-85 doi: 10.1097/nna.0000000000000408