Embed Size (px)
Citation preview

Clinical Monthly
209th Edition

2
The Clinical Monthly Team
Sam Barr News of the Month
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: Back pain, health and wellbeing
Chloe Whitman
Clinical differential of the Month
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: shoulders, sports and paediatrics.
Abi Peck Editor
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: Hands and spinal pathology, netball rehab
Ryan Crowther Podcast of the Month
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: Injury prevention and return to activity/sport. Tendons.
Lee Platt Journal of the Month
Qualified: MSc (Hons) Physiotherapy
Clinical Interests: all areas in MSK
3
News of the Month
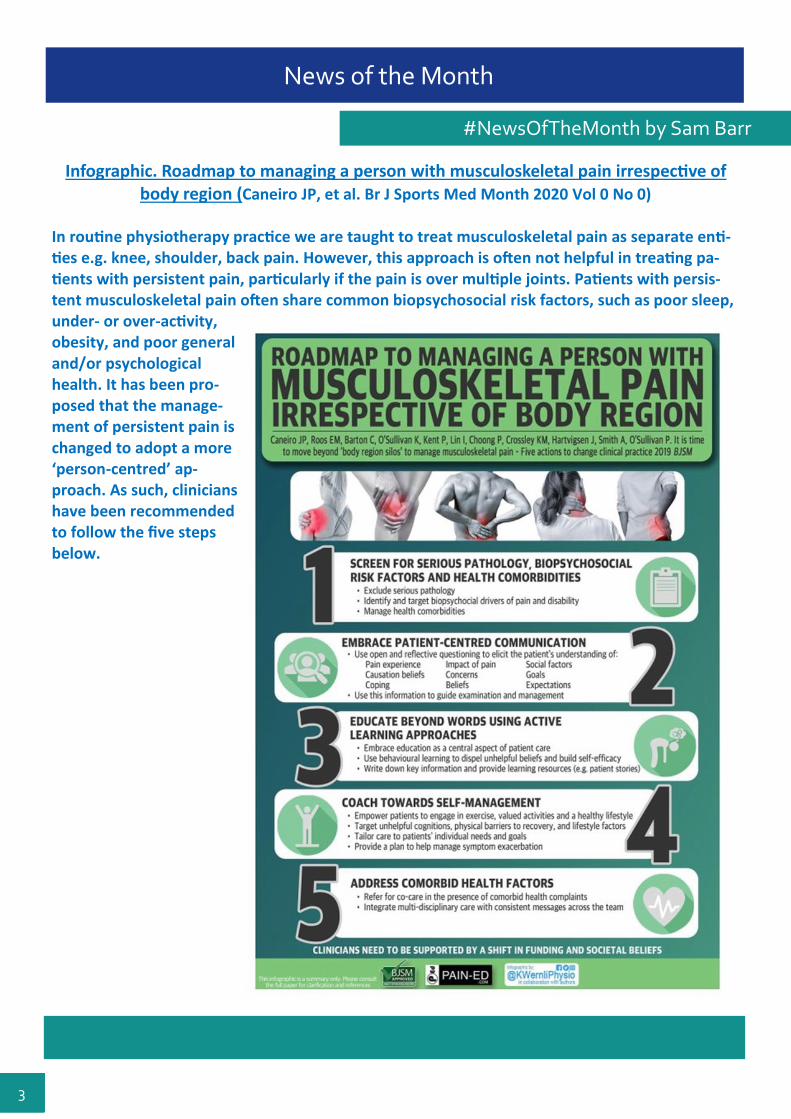
Infographic. Roadmap to managing a person with musculoskeletal pain irrespective of body region (Caneiro JP, et al. Br J Sports Med Month 2020 Vol 0 No 0)
In routine physiotherapy practice we are taught to treat musculoskeletal pain as separate enti-ties e.g. knee, shoulder, back pain. However, this approach is often not helpful in treating pa-tients with persistent pain, particularly if the pain is over multiple joints. Patients with persis-tent musculoskeletal pain often share common biopsychosocial risk factors, such as poor sleep, under- or over-activity, obesity, and poor general and/or psychological health. It has been pro-posed that the manage-ment of persistent pain is changed to adopt a more ‘person-centred’ ap-proach. As such, clinicians have been recommended to follow the five steps below.
#NewsOfTheMonth by Sam Barr
4
News of the Month
Is there a place for intra-articular corticosteroid injections in the treatment of knee osteoarthritis? Orchard, J. BMJ 2020; 368:l6923 Intra-articular corticosteroid injections are widely pre-scribed for the treatment of mild to moderate osteoar-thritis in the hope of delaying the need for joint re-placement. Current research with low quality evidence suggests that intra-articular corticosteroid injections may provide short term relief along with an improve-ment in physical function for up to six weeks. Patients with more severe disease are likely to experience greater improvements. Guidelines on the treatment of osteoarthritis have typically supported the use of these injections but does the short-term improvement in pain outweigh the long-term safety or harms? Risks of intra-articular corticosteroid injections A 2015 Cochrane review of corticosteroid injections for knee osteoarthritis did not find any evidence of harm in the short term (<6 months) but did not assess long-term harms. A trial in 2017 reported a small (-0.1mm) reduction in the thickness of knee cartilage following a cortico-steroid injection. Both cartilage depth and quality are radiological indicators of disease progression – it is not known whether this would manifest clinically. Recent cohort studies found worsening pain, stiffness, and function with progression to receiving a total knee replacement two years post corticosteroid injection. It is thought repeat intra-articular injections pose the greatest risk of disease progression, but the joint may still deteriorate with a single injection. There is an increased risk of infection after knee surgery in patients who had received a corticosteroid in-jection in the same knee within three months before surgery. It is therefore suggested that intra-articular corticosteroid injections possibly offer a small, short-term im-provement in knee osteoarthritis symptoms. However, this may result in disease progression in the long-term. Clinicians and patients need to be able to weigh up the risks and benefits and to consider whether the short-term or long-term outcome is more important. Corticosteroid injections may be beneficial for frail elderly patients who are unsuitable for joint replacement. However, for younger patients where the long-term outcome is more important corticosteroids are not recommended – unless short-term im-provement is desired for a particular event e.g. travelling, wedding etc. What patients need to know: Osteoarthritis is a lifelong condition and pain and stiffness can fluctuate, Moderate exercise is the most appropriate treatment for mild to moderate symptoms, Cortisone injections may give a small degree of symptom relief in the short term (<6 weeks), but symp-toms are likely to return as studies do not indicate long-term improvements, There are new studies highlighting possible cartilage deterioration and worsening of symptoms with re-peated injections.
#NewsOfTheMonth by Sam Barr

5
Differentials of the Month
Hip Differentials by Chloe Whitman
Last months
Clinical case
Subjective: A 30 year old female who is a keen runner attends clinic with one week sudden onset of anterior hip/groin pain. Patient reports clicking and pseudo locking. Dull aching anterior hip/groin especially when walking/twisting/changing direction or sitting for a prolonged period of time.
The working diagnosis of last issues ‘differential diagnosis’ case study is an FAI. Patho-aetiology FAI is subcategorised into two primary bony causes: CAM and pincer. CAM refers to extra bone growth on the neck of the femur, this bone growth isn’t a problem in itself how-ever, becomes painful when one tries to move the hip to end ranges. Movements into flexion, adduction and internal rotation can lead to catching of the femoral head on the acetabulum and impinge the struc-tures in-between. This type of FAI seems to be most common in younger active men. Pincer is related to an increase in depth of the acetabulum. It is commonly described as a deep aching sen-sation and is often with no history of trauma. It usually occurs after activities that have involved extremes of movement, for instance dancers or athletes who play ball sports with lots of twisting or pivoting. There may also be a clicking, locking or feeling of instability which could be attributed to a labral tear, as around 73% of patients with FAI also had concurrent labral tears (Brukner et al, 2015).
Management options: Researchers are still researching to ascertain the best course of treatment for those with FAI. To date, hip arthroscopy has commonly been utilized but early reports tended to be limited to cohort-level, typically showed only short-term benefits and were usually authored by surgeons, thus introducing the possibility of population bias. "there is currently no high-level evidence to support the choice of a definitive treatment for FAI syndrome" therefore all options should be considered for each patient and an approach should be selected based on a shared decision-making process” (Reiman and Thorborg, 2015). Casertelli et al (2016) suggest that improving neuromuscular function of the hip should be a goal of con-servative protocols for FAI syndrome due to weakness of deep hip musculature and an expected subse-quent reduction in dynamic stability of the hip joint. These authors recommend including hip-specific and functional lower limb strengthening, core stability and postural balance exercises. To improve dynamic sta-bility of the hip, there should be a focus on strengthening the deep hip external rotators, abductors and flexors in the transverse, frontal and sagittal planes. In a randomized controlled trial, Mansell et al (2018) compared patient outcomes for surgical intervention versus physiotherapy (working mainly on manual techniques, motor control and mobility exercises). At the two year follow-up, there was no statistically significant difference in outcomes found between the surgical and non-surgical groups and on average, subjects in both groups reported no improvement in their condi-tion.
References: Brukner, P., Khan, K., Clarsen, B., Cook, J., Cools, A., Crossley, K., Hutchinson, M., McCrory, P., Bahr, R. and Brukner, P. (2015). Brukner & Khan's clinical sports medicine. 4th ed. McGraw-Hill Education Ltd. Casartelli, N., Maffiuletti, N., Bizzini, M., Kelly, B., Naal, F. and Leunig, M. (2016). The management of symptomatic femoroacetabular impingement: what is the rationale for non-surgical treat-ment?. British Journal of Sports Medicine, 50(9), pp.511-512. Griffin, D., Dickenson, E., O'Donnell, J., Agricola, R., Awan, T., Beck, M., Clohisy, J., Dijkstra, H., Falvey, E., Gimpel, M., Hinman, R., Hölmich, P., Kassarjian, A., Martin, H., Martin, R., Mather, R., Philippon, M., Reiman, M., Takla, A., Thorborg, K., Walker, S., Weir, A. and Bennell, K. (2016). The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an interna-tional consensus statement. British Journal of Sports Medicine, 50(19), pp.1169-1176. Mansell, N., Rhon, D., Meyer, J., Slevin, J. and Marchant, B. (2018). Arthroscopic Surgery or Physical Therapy for Patients With Femoroacetabular Impingement Syndrome: A Randomized Con-trolled Trial With 2-Year Follow-up. The American Journal of Sports Medicine, 46(6), pp.1306-1314. Reiman, M. and Thorborg, K. (2015). Femoroacetabular impingement surgery: are we moving too fast and too far beyond the evidence?. British Journal of Sports Medicine, 49(12), pp.782-784.

6
Differentials of the Month
Hip Differentials by Chloe Whitman
Clinical case
55 year old women with a 4 weeks history of lateral hip pain with an insidious onset. Reports pain can radiate to the knee. Worse with walking with pain on instant weight bearing and sitting for pro-longed periods of time.
Differential diagnosis
1) Hip flexor tendinopathy
2) Gluteal tendinopathy
3) Stress fracture
Last months differential diagnosis has been revealed as FAI. This months differential diagnosis is detailed below, lets see how well you can do!

7
Podcast of the Month
PhysioEdge podcast 096 - Thoracic outlet syndrome with Jo Gibson
What is thoracic outlet syndrome (TOS)?
Compression of one part of the neurovascular bundle within the tho-racic outlet, either the brachial plexus, subclavian vein or subclavian artery.
Split into three types:
Neurogenic type – most common (80%). Involves compression of the brachial plexus in the scalene triangle (floor between the first rib and the anterior and middle scalene muscles), or in the retropectal space behind pec minor. Up to 75% of people with neurogenic type will have compression at both areas. 6% will also have a venous component to symptoms.
Incidence – 1 per 10000 people per year. As prevalent as Crohns disease or ovarian cancer.
More prevalent in women (71%), and associated with hypermobility spectrum patients (24%).
Mean symptom duration prior to diagnosis is 5 years, on average seeing 6 doctors.
Venous type – compression of the subclavian vein, generally at the junction of first rib and clavicle.
Arterial type – (least common) generally caused by damage of the subclavian artery, normal-ly due to abnormal bony damage.
Consensus document from US college of vascular surgeons requires 3 out of 4 criteria for diagno-sis:
1) Hand and arm symptoms consistent with nerve compression. Worse with overhead activity or arms dangling. Can be referred into arm, head, face, upper back, shoulder girdle, axilla, chest. May well have had previous surgeries for peripheral neuropathies without success.
2) Pain and tenderness (with potentially associated reproduction of patients symptoms) on palpation of scalene triangle or pectoralis minor insertion. Localised tenderness in one of the two areas is sufficient.
3) Absence of another diagnosis, e.g. peripheral nerve entrapment (tests Tinels and Phalens), or cervical nerve root compression, (myotomal or dermatomal presentation, with findings on cervical spine, palpation, Spurlings test, and/or imaging. Cervicobrachial symptoms ques-tionnaire can help to differentiate between cervical cause or TOS.
4) Positive response to a scalene block or injection. Not available to all.
Common features: Heaviness in the arm, radiating paraesthesia and numbness, changes in colour, loss of hand dexterity, muscle atrophy, dilated veins in hands.
Consider patients reporting onset following a history of trauma or repetitive overhead use that could demonstrate compromise of the thoracic outlet via scalene hypertrophy, or trauma causing fibrous bands/scarring.
# Podcasts by Ryan

8
Podcast of the Month
What tests should be used to assess for thoracic outlet syndrome?
Important to perform a good neurological exam, including muscle strength (identification of wasting), reflexes, and sensation (pin prick and thermal detection).
Tests of good value from the reporting guidelines; Elevated arm east test (rues test) is 90% sensitive. Both arms in surrender position 90 shoulder abduction and 90 elbow flexion, then open and close the hands for up to 3 minutes. A reproduction of symptoms, or changes of limb colour is a positive test. Ensure arm is in correct position, slight extension. Mean time to onset 1 minute 40 seconds.
Upper limb tension test, with bilateral upper limb abduction and elbow extension. Extend wrists bilaterally, tilt the head to each direction with symptom reproduction being a positive test. Positive in 80% of patients. A neg-ative result doesn’t rule out TOS especially in patients with persistent pain where upper limb tension tests may become less sensitive over time.
Investigations including MRI, MRneurography, nerve conduction studies, dopplers may all come back normal.
Research by Anina Schmid shows nerve degeneration due to compression may only affect the small fibres within the nerve. These small fibres aren’t typically picked up on nerve conduction studies so they can give a false negative. Clinical tests we can use to look at small fibre degeneration include pin prick (light touch), and thermal (cold and warm) from the quantitative sensory testing protocol. Cold and warm testing using coin of room temp vs from 30 minutes in your pocket, comparing the affected area to another area on the arm is a sensitive way of testing thermal detection. If thermal detection is normal it is unlikely there is any small fibre degeneration. Normal pin-prick doesn’t rule out having small fibre degeneration. Both being negative gives best reliability.
Nerve blocks under US guidance in scalene triangle and retropectal regions are suggested to be positive in 80%.
Who in this patient group should be referred on for surgical opinion?
Recommended that all patients with thoracic outlet syndrome should have physio as first line treatment. How-ever those with nerve function compromise, whether small fibre or gross neurological change should be con-sidered for an early referral to a surgeon. Typically refer to a vascular surgeon or those with a special interest that perform high volumes of surgery for TOS.
Botox injections into scalene muscles may be considered.
In the acute phase of symptoms treatment will largely be activity modification and posture advice, and strengthening the upper quadrant. Some papers indicate that targeting the upper fibres of trapezius can be of benefit, such as the Newcastle region. It’s hypothesised to cause posterior tilt of the scapula and open up the supraclavicular region. Any strategies to improve neck and shoulder strength, including those to ensure func-tion of the rotator cuff and scapula muscles, can open up the area and have an unloading effect.
# Podcasts by Ryan
Next Month - The physio matters podcast – Session 65 – Cauda equine syndrome with Chris Mercer.
What is cauda equina syndrome (CES)?
What are the questions we should be asking?
How can we effectively manage patients with low back pain with respect to CES?

9
Journal of the Month
#Journal club by Lee Platt
Is running associated with a lower risk of all-cause cardiovascular and cancer mor-tality, and is the more the better? A systematic review and meta-analysis Pedisic et al (2019) CASP for Systematic Review Section A: Are the results of the review valid? 1) Did the review address a clearly focused ques-
tion? No rather than a specific question, the au-thors were assessing the association between running (and the dosage of running) with the risk of all-cause, cardiovascular and cancer mor-tality (assessed as three separate cohorts).
2) Did the authors look for the right type of pa-pers? Yes.
3) Do you think all the important, relevant studies were included? Mostly, howev-er only prospective cohort studies were included to assess the long term asso-ciation between running and mortality.
4) Did the review’s authors do enough to assess quality of the included studies? Yes, and in doing so, one study was considered ‘fair quality’ whilst the remain-ing studies were all considered to be ‘good quality’.
5) If the results of the review have been combined, was it reasonable to do so? Yes – when analyses for single cohorts were combined the longest follow up was used. The overall results were combined to assess the association be-tween running participation and all-cause, cancer and cardiovascular mortality separately, as well as the comparison of the running dosage and overall risk of mortality.
Section B: What are the results? 6) What are the overall results of the review? Running participation was found to be associated with 27%, 30% and 23% reduced risk of all-cause, cardiovascular and cancer mortality, respectively. There was no significant dosage of running found to be most beneficial to mortality, and greater amounts of running were not found to have any significant benefit either. 7) How precise are the results? There is variation between studies of the confi-dence intervals for each cohort.

10
Journal of the Month
#Journal club by Lee Platt
Section C: Will the results help locally? 8) Can the results be applied to the local population? Yes, especially with running being one of the most popular forms of physical activity. According to the authors, significant reductions in mortality risk can be gained from any dose of running, even if just once a week, or 50 minutes per week. 9) Were all important outcomes considered? Many of the papers did not consider other forms of physical activity that may also have contributed to overall lower mortality risk, especially as runners may also engage in other forms of exercise and fitness. Individuals with a history of cardiovascular and/or cancer were not included in a number of studies. Running distance was assessed in only one cohort study and therefore its impact on effective dosage is unknown. Self-reported running participation was used in all of the studies and therefore may have had variable reliability. 10) Are the benefits worth the harms and costs? There were no reported harms or
costs.
Next month: Efficacy of early controlled motion of the ankle compared with immobilisa-tion in non-operative treatment of patients with an acute Achilles ten-don rupture: an assessor-blinded, randomised controlled trial Barfod et al., 2019 Journal of sports medicine. CASP tool—RCT

11
‘Leading the way towards healthier, happier lives’
Find us on social media
www.ahpsuffolk.co.uk
#Journal club by Lee Platt