Embed Size (px)
Citation preview

1
Pittsburgh, PA
Gladwyn Leiman – UVMMC, VT
23rd Annual Seminar in Pathology
FLUIDS, Part 1
"Blue walls", Claudia Hansen, 2009
Introduction
o Challenging to everyone
o Almost any benign or malignant process may involve serous cavities
o Most cells round up in fluid, altering morphology considerably
o Classic stains used are Papanicolaou and Giemsa
o Immunocytochemistry has become a frequent standby on fluids & cell blocks
o All adjunctive tests can be performed on fluids
2
The Body Cavities
o Dynamic space
o 5-10L of fluid is filtered and reabsorbed each day
o Any significant accumulation is abnormal
o Maximum accumulation:
o 20L in peritoneal cavity
o 3L in each pleural cavity and
o 600cc in pericardial cavity
Neoplastic Exudates
Metastasis: – most frequent
– direct involvement or extension
Primary tumors: – Mesotheliomas
– Serous tumors
Advantages of fluid examination
o Easily accessible
o Repeated access for monitoring
o Provide useful clinical information: o Diagnosis, adjunctive tests
o Staging and prognosis
o Follow up and disease monitoring
o Frequent site of recurrence, metastasis
3
Fluid collection
o Thoracentesis
o Paracentesis
o Culdocentesis
o Peritoneal washing
o Pelvic washing
o During surgery
o During endoscopy
SEND THE FULL VOLUME 70 – 100ml lower limit
Cells in Benign Fluids
Mesothelial cells
Macrophages
Leukocytes
Normal mesothelial cells
o Single-layered, flat lining cells of serous membranes.
o 10-20 microns in diameter
o Appear singly or in small aggregates when naturally shed
o Appear in sheets if actively washed
o Round , regular nuclei with small nucleoli. May have grooves.

4
Normal mesothelial cells
• Basophilic, sharply demarcated cytoplasm
• Two-tone cytoplasm with brush borders.
• Perinuclear dense zone (due to organelles)
• Peripheral clear zone with lacy edge
• Intercellular “windows” between cells
• EM: regular, LONG microvilli on cell surface
Benign mesothelial cells (Pap)
5
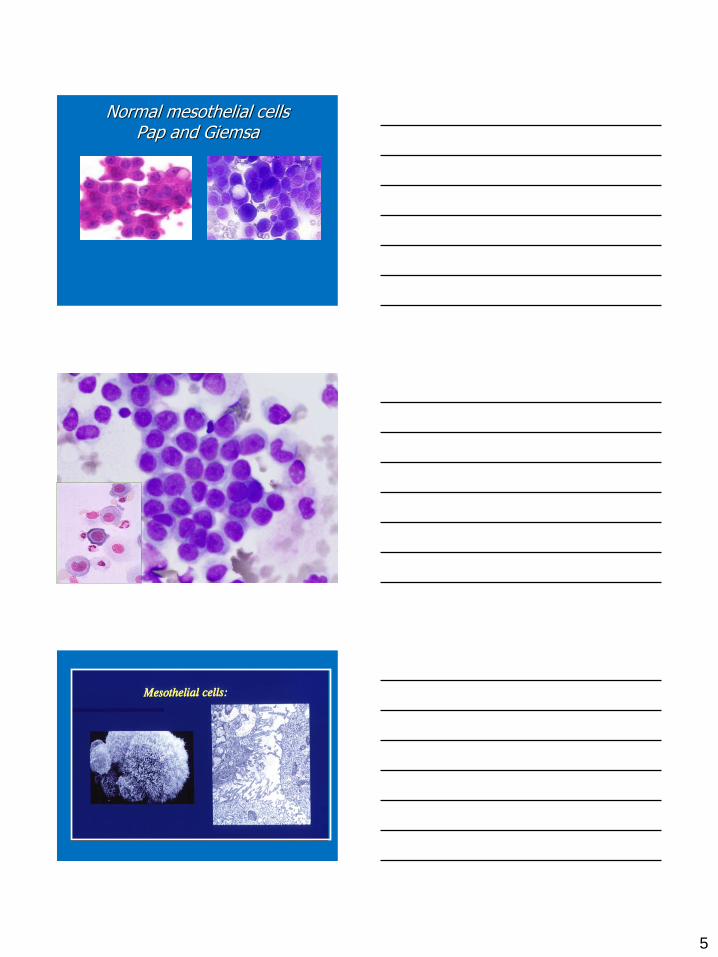
Normal mesothelial cells Pap and Giemsa

6
Reactive mesothelial cells
• Cellular, with 3D clusters, mimic epithelial cells
• Nuclear enlargement, binucleation and multinucleation, can appear atypical
• Can have hyperchromasia with mostly regular nuclear membranes
• Cytoplasmic vacuolization resemble signet-ring cells (never mucin positive).
• Often with inflammatory background.
Reactive mesothelial cells
Reactive mesothelial cells

7
Reactive mesothelial cells (MGG)
Other cells
Histiocytes - ubiquitous (likely transformed mesos) – Similar in size to mesothelials
– Lightly stained cytoplasm
– Irregular nuclei with low N/C ratio
Some kidney-bean shaped,
Multinucleated
– Phagocytized debris
– Foamy cytoplasm
– Cytoplasmic vacuolation
(MGG)
Other Cells
Lymphocytes:
– Chronic and chylous effusions, TB, (CLL/SLL)
Neutrophils: Infection, infarction, rupture
Eosinophils: designated eosinophilic if >10%
– Trauma
– Hypersensitivity/allergy
– ~ 5% associated with malignancy.
– Hydatid disease
8
Congestive Heart Failure
Most common cause of benign effusion
Pleural, pericardial effusion and ascites
Usually transudates except when associated with inflammation
Rarely blood-stained
CYTOLOGY:
Reactive mesos and lymphs if chronic
Cirrhosis
o Usually transudates:
o Low protein synthesis
o Portal hypertension
o CYTOLOGY:
o Reactive mesothelial cells
o Atypical mesothelial cells:
o papillary clusters
o acini, rosettes
o Signet ring forms
Acute inflammatory processes
o Composed of purulent exudate
o Bacterial pneumonia
o Lung abscess
o Pleurisy, pericarditis, peritonitis
o CYTOLOGY: Neutrophils ++
Few mesothelials
9
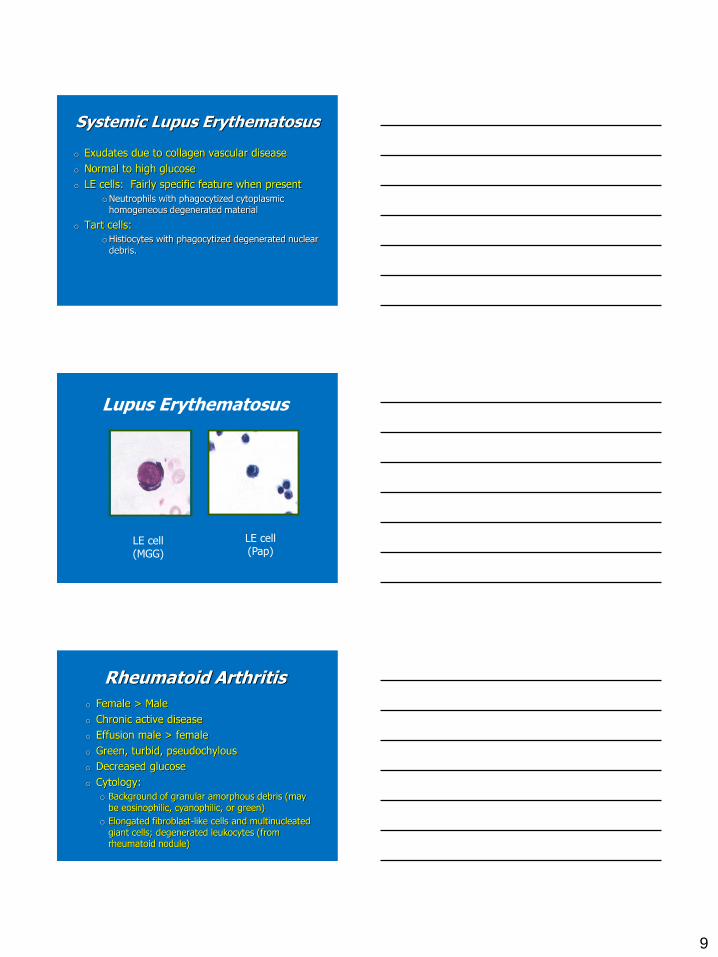
Systemic Lupus Erythematosus
o Exudates due to collagen vascular disease
o Normal to high glucose
o LE cells: Fairly specific feature when present
oNeutrophils with phagocytized cytoplasmic homogeneous degenerated material
o Tart cells:
oHistiocytes with phagocytized degenerated nuclear debris.
Lupus Erythematosus
LE cell (Pap)
LE cell (MGG)
Rheumatoid Arthritis
o Female > Male
o Chronic active disease
o Effusion male > female
o Green, turbid, pseudochylous
o Decreased glucose
o Cytology:
o Background of granular amorphous debris (may be eosinophilic, cyanophilic, or green)
o Elongated fibroblast-like cells and multinucleated giant cells; degenerated leukocytes (from rheumatoid nodule)

10
Rheumatoid Pleurisy
Multinucleated giant cells Fibrinoid debris
Tuberculosis
o Pseudochylous
o When TB doesn’t directly involve pleura:
o Lymphocytosis - mostly T cells
o Plasma cells
o Rare Langerhans’ cells
o Decreased/absent mesothelial cells
TB pleurisy

11
Pulmonary infarction
Highly atypical mesothelial cells can be present
Eosinophils, neutrophils, siderophages and lymphocytes
Can be blood-stained
Radiation changes
Radiation pleuritis and pericarditis
Immediate or delayed - months/years
Differential is recurrent malignancy
Mesothelial changes:
– Nuclear enlargement with hyperchromasia
– Cytoplasmic and intranuclear vacuolation and blebs
– Multinucleation
Radiation changes

12
Miscellaneous cells
Hepatocytes
– May be seen in right-sided pleural effusion
Ciliated bronchial cells
- trauma, broncho-pulmonary fistula
Squamous cells - dermoid cyst
Megakaryocytes/hematopoiesis in EMH
Detached ciliary tufts
Normal, physiologic phenomenon. Anucleated fragments of ciliated columnar epithelial cells from the fallopian tube
Seen in peritoneal fluids
Do not confuse with organism

13
Peritoneal Washings
Obtained intraoperatively during laparotomy for gynecologic surgery
Mesothelium characterized by large, flat, monolayer sheets of cells fitting together in orderly mosaic pattern
Nuclei are round, oval, regular, grooved (sometimes kidney-bean and convoluted)
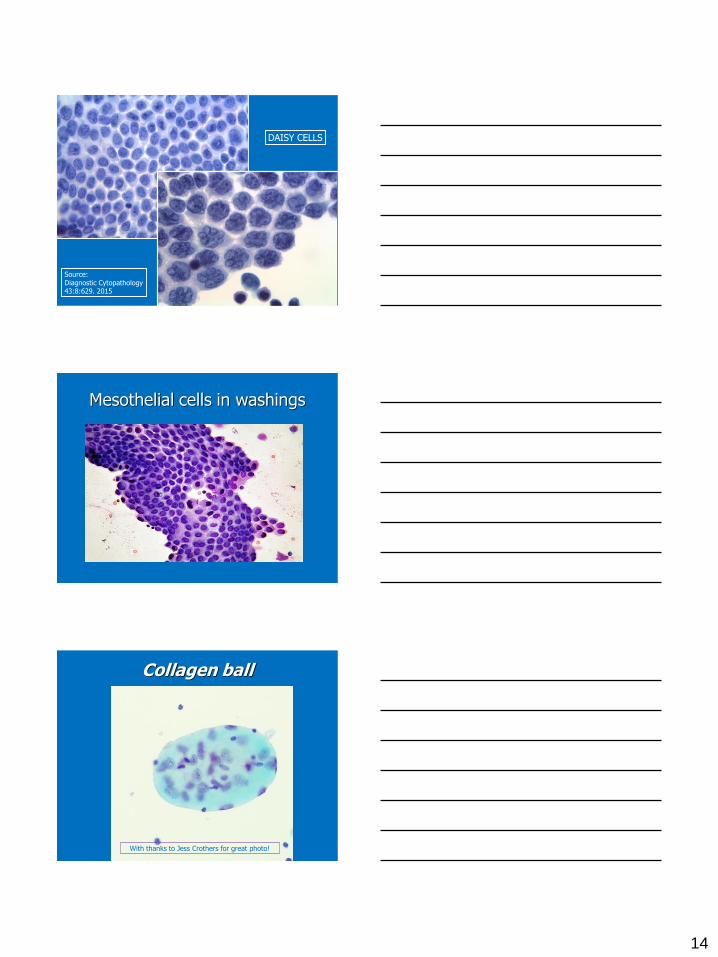
Mesothelial cells in washings
Mesothelial cells in washing specimen
14
Source: Diagnostic Cytopathology 43:8:629. 2015
DAISY CELLS
Mesothelial cells in washings
Collagen ball
With thanks to Jess Crothers for great photo!
15
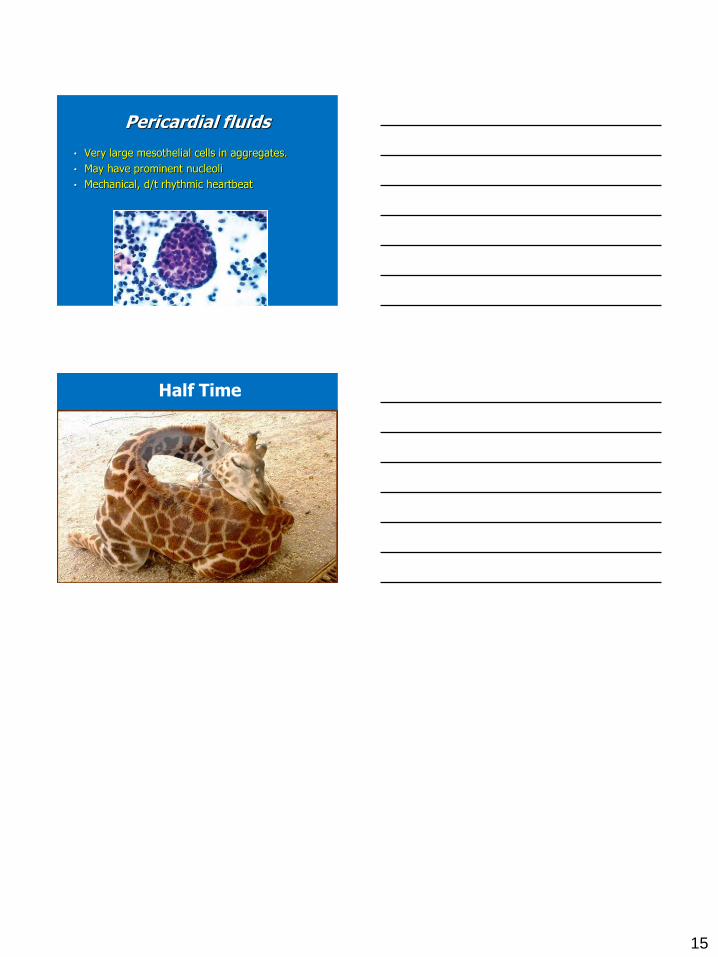
Pericardial fluids
• Very large mesothelial cells in aggregates.
• May have prominent nucleoli
• Mechanical, d/t rhythmic heartbeat
Half Time





























![USTA TrafficAnalysisBriefing V7 0 20150530 FINAL[1] · PDF file1."Executive"Summary" ... In2014thethreemajorGulfcarriers" –"Emirates,"Qatar"Airways"and"Etihad" Airways"–"carried"some"4.3"million"passengers"intoandout"of"the](https://img.pdfslide.net/doc/110x75/5aa125967f8b9a46238b5bf2/usta-trafficanalysisbriefing-v7-0-20150530-final1-in2014thethreemajorgulfcarriers.jpg)