Embed Size (px)
Citation preview

University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 107
University J Dent Scie 2015; No. 1, Vol. 3
ABSTRACT : Crouzon syndrome is a rare craniofacial dysostosis with autosomal dominant mode of inheritance with variable phenotypic expression .It is characterized by early closure of cranial sutures leading to range of problems like calvarial deformities, midface hypoplasia and exopthalmus. Early diagnosis is critical in these cases to avoid complications like hearing and vision problems.There are 50% chances of transmission when one of the parents is affected. We hereby report a familial case of a 9yr old girl and mother along with pedigree analysis of the trait
1 2 3Lavina Taneja, Vishal Arya , Puneeta Vohra1,3Reader, Department of Oral Medicine and
2Radiology, Professor, Department of Pedodontics and Preventive Dentistry,Faculty of Dental Sciences, SGT University,Gurgaon.
INTRODUCTION : Louiss Edouard Octave Crouzon , a
French neurosurgeon ,in 1912 first published a case of a
mother and son with abnormal facial features. The
eponymous syndrome was described by him as a classic triad
of calvarial deformities,facial anomalies and exopthalmus.
[1] Crouzon syndrome or craniofacial dysostosis is one of a
rare syndrome occurring 1 in every 25,000 live
births.[2]There is 50% risk of transmission if one of the
parents has the disease. [3]There is autosomal dominant mode
of inheritance is about 67% of cases others with autosomal
recessive and spontaneous mutation have also been
described.[ 4]
The phenotypic expression of the abnormality varies between
the affected members of same family. The order and rate of
fusion is determining factor.The present case report
highlights a familial case of a 9 year old female patient and
mother along with pedigree analysis of trait running in
maternal family.
Case report
A 9 yr old female patient reported to the department with the
chief complaint of deposits on teeth since 6 months. This was
her first dental visit. Medical history revealed recurrent eye
infection and hearing problem. General examination revealed
short stature and hand and feet were normal.She was of
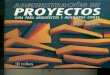
normal intelligence On extraoral examination examination
patient had straight profile,frontal bossing,flat
forehead,depressed nasal br idge,hypertelor ism,
exopthalamous , short upper lip,low placed ears(figure 1).
Figure 1: Frontal view of child showing hypertelorism,
proptosis, flat forehead,short upper lip
On intraoral examination there was edentulous space wrt 12
and 22, stains and calculus, ,high arched palate( figure 2) and
crowding of lower anteriors. Maxillary arch was v shaped
FAMILIAL CASE OF CROUZON SYNDROME : CASE REPORTAND REVIEW OF LITERATURE
Journal of Dental Sciences
University
Keywords : Crouzon syndrome,Familial,Pedigree
Source of support : NILConflict of interest : NIL
Case Report

with posterior crossbite on right side (figure 3).Patient was
accompanied by her mother who also showed typical
facies.Mother had flat forehead, proptosis, hypertelorism
(figure 4) and gave history of severe headache specially in
summer season. There was no history of consangious
marriage. Father was normal and couple's elder son also had
no such features. Patient's maternal family had history of
similar facies as depicted in pedigree analysis. (Figure 5)
Pedigree showing the trait depicted as dark in maternal
family of patient.
Figure 2-Intraoral oicture showing high arched palate.
Figure 3 Intraoral picture showing missing 12 and 22,
crossbite on right side and anterior open bite.
Figure 4:Mothers frontal view showing flat forehead,
proptosis and hypertelorism. Pedigree analysis
Figure 5 : Pedigree analysis
Patient was advised OPG (figure 6), lateral cephalogram
(figure 7)., PA cephalogram (figure 8). The skull typically
showed copper beaten appearance and small sinuses were
observed. Mothers OPG (figure 9) and Lateral cephalogram
were taken and skull showed copper beaten appearance
(figure 10).
Figure 6: OPG of the child
Fig.7:Lateral Ceph of child showing copper beaten appearance
Fig. 8:PA Skull of child showing copper beaten appearance
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 108
University J Dent Scie 2015; No. 1, Vol. 3

Figure 9: OPG of Mother
Figure 10 : Lateral Ceph of Mother showing copper beaten
appearance.
Based on the above findings and investigation patient was
diagnosed as a familial case of crouzon syndrome. Mother
was also informed about her status and genetic transmission
and counseled about complication and correlation with
ophthalmic and hearing problem. Mother was also informed
about her own status. Patient was refered for routine scaling
and cleaning, and ophthalmologist and ENT opinion and oral
surgery and orthodontic advice.
DISCUSSION : Mutation of fibroblast growth factor
2(FGFR2) gene located on chromosome 10q25- 26 is related
to Crouzon syndrome.About 25 mutations have been
identified to its pathogenesis. 5There is 50%of risk of
transmission when one of the parents has a disease without
dependence on individual's sex. 3
FGFR mutation results in secretion of cytokines in
autocrinous and paracrinous manner that leads to
modification of matrix. These changes in genesis in the
osteogenic process lead to the pathosis. 6
There is no racial or sexual predilection for this syndrome but
sagittal and metopic suture fusion displays male
predominance whereas coronal suture involvement shows
slight female predilection. 7
Fibrous sutures in the skull and face are abnormal i.e they fuse
early resulting In distorted bone growth leading to
craniofacial abnormalities i.e. craniostenosis. 8 There is
premature closure of cranial suture most commonly coronal
and saggital suture .Once the suture is fused growth
perpendicular to that suture becomes restricted and starts
parallel to the suture and the fused bone act as a single bony
structure.Compensatory growth of open sutures occur to
allow brain growth. [9]
During infancy, the coronal and saggital suture and
occasionally lambdoidal suture fuse early and this is
completed by second or third year. The condition is usually
detected in the first year of life .However congenital
premature forms may also exist in which fusion starts in utero
life and is evident at birth.
Premature fusion of cranial base leads to shallow orbits
leading to ocular proptosis are seen in 100% of patients
.Other ocular abnormalities like hypertelorism,strabismus
and reduced vision acquity are also seen.Hypertelorism
occurs due to decrease in growth of sphenozygomatic and
sphenotemporal suture.[10]
Approximately one third of these patients suffer from hearing
loss due to middle ear deformities and upper airway
obstruction due to midface hypoplasia and narrow
epipharynx. [11]
Diminished mental function is present in about 12% of
patient's. Headache and apprehension because of intracranial
pressure and progressive hydrocephaly is seen in 30%cases.
[9]. The clinical features of Crouzon Syndromeare tabulated
in table 1.
Radiographic examination play a crucial role in the diagnosis.
The earliest sign are sclerosis and overlapping edges
representing suture synostosis. Normally radiolucent sutures
on the skull view are not detected or show sclerotic changes.
Digital impression of inner surface of cranial vault which
appear as multiple radiolucency. 2Typical name given to this
appearance of calvarium on skull radiograph are beaten
metal/copper beaten/hammered silver appearance. It
represents internal remodeling of calvaria due to increase in
intracranial pressure as a result of premature cranial suture
fusion.
Spine radiograph may reveal fusion at C2-C3 or C5-C6 level
and at times butterfly vertebrae and fusion of posterior body
and element. 4These changes are seen in 18% of patients. 4CT
Scan reveals fused sutures along with indentation on inner
table of skull, hydrocephalus, midface hypoplasia, shallow
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 109
University J Dent Scie 2015; No. 1, Vol. 3

orbits and small paranasal sinuses .MRI is used to view corpus
callosum occasional agenesis and optical atrophy.
Table -1 showing clinical features f Crouzon Syndrome
DIFFERENTIAL DIAGNOSIS : 100 syndromes with
craniostenosis have been described.The most common and
well known among these are Crouzon and Apert syndrome.
Table - 2 showing differential diagnosis of Crouzon
Syndrome
CONCLUSION : Dental professionals can play a pivotal
role in early recognition and diagnosis of these condition and
through counseling to the affected families regarding genetic
transmission.Early intervention by multidisciplinary
approach thus can prevent complications like effect on
blindness,hearing loss and mental and psychological growth.
ACKNOWLEDGEMENT : I would like to acknowledge
Dr. Akshika Sharma for the support and help in preparation of
this manuscript.
REFERENCES
1. Crouzon o.dysostoses craniofaciale hereditaire:bull soc
med hosp paris 1912;33:545-555
2. CohenMM, craniosynostosis and syndrome with
craniosynostosis:incidence,genetics,penetrance,variabil
ity and new syndrome updating.birth defects orig artic
ser1979;15:13-63
3 . P h a r o h W . O r a l r a d i o l o g y P r i n c i p l e s a n d
interpretation.5th edition Mosby:Elsevier;2005 pg640-
641
3. Carinci F,Pezzetti F,Locci P,et al.Apert and crouzon
syndromes:clinical findings,genes and Extracellular
matrix.J craniofac surg.2005,3(16):361-6
4. Gorlin RJ ,Cohen MN Jr,Hennekam R.Syndromes of
Head and Neck.4th ed.2001 pg 658-9
5. Reardon W,Winter RM,Rutland P,et al.Mutations in the
fibroblast growth factor receptor 2 gene cause crouzon
syndrome.Nature Genet.1994,8:98-103.
8. C Scully,J Landon,J Evans.Marathon of eponyms:3
crouzon syndrome.oral Diseases 2009,15:367-8
9 . E r n e s t L . B o w l i n g , F e r n a n d o D , C r o u z o n
syndrome,Burstein optometry.2006,77:217-222
10. Singer SL,Walpole I ,Brogan WF,Goldblat t
J.Dentofacial features of a family with crouzon
syndrome-case report.Aust Dent J 1997;42:11-7
11. Da silva DL,Palheta Neto FX,Carneiro SG et al.crouzon
s y n d r o m e : l i t e r a t u r e r e v i e w . I n t l A r c h
otorhinolaryngol,Sao Paulo 2008;12:436-41
CORRESPONDING AUTHORS:
Dr. Lavina Taneja
A 150 Second floor, Lok vihar, Pitampura,
New delhi 110034
E mail : [email protected]
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 110
University J Dent Scie 2015; No. 1, Vol. 3