Embed Size (px)
Citation preview
230413 Annual Report: Final 1
Infection Prevention & Control Annual Report 2012/2013
2010/2011
230413 Annual Report: Final 2
1 SUMMARY......................................................................................................................... 3
2. ACHIEVEMENTS AND INITIATIVES........................................................................3
3. UNPLANNED ACTIVITY...........................................................................................3
3.1 Outbreak management (Norovirus).......................................................... 3
3.3 Clostridium difficile investigations .......................................................... 3
3.4 Influenza ..................................................................................................... 3
3.5 MRSA “Hot Spots”..................................................................................... 4
3.6 Vancomycin Resistant Enterococci (VRE) in Critical care..................... 4
3.7 BLITZ Campaign ........................................................................................ 4
4. PLANNED ACTIVITY ................................................................................................4
4.1 Progress against the annual plan ............................................................ 4
4.2 Audit ........................................................................................................... 5
4.3 MRSA Screening........................................................................................ 5
4.4 Surveillance: Alert Organism ................................................................... 5
4.5 Hand hygiene ............................................................................................. 5
4.6 Surveillance: Surgical site infection (SSI) ............................................... 5
4.7 Clostridium difficile infection ................................................................... 6
4.8 Meticillin Sensitive Staphylococcus Aureus (MSSA) bacteraemia ....... 6
4.9 Meticillin Resistant Staphylococcus Aureus (MRSA) bacteraemia....... 6
4.10 MRSA other infection/colonisation .......................................................... 6
4.11 Escherichia coli (E.coli) bacteraemia....................................................... 6
4.12 Ward Commendation Scheme.................................................................. 7
4.13 Water safety ............................................................................................... 7
4.14 Data feedback ............................................................................................ 7
4.15 Link Person Group .................................................................................... 7
4.16 Education and Training............................................................................. 7
4.17 Saving Lives”............................................................................................. 8
4.18 Infection Control Intranet Site .................................................................. 8
4.19 St Giles Hospice (Whittington) ................................................................. 8
5. ISOLATION FACILITIES...........................................................................................8
6. STAFFING.................................................................................................................8
7. CARE QUALITY COMMISSION ...............................................................................9
8. MEETINGS AND REPORTS.....................................................................................9
9. INFECTION PREVENTION AND CONTROL POLICY .............................................9
10. INNOVATION ............................................................................................................9
11. KEY THEMES FOR THE YEAR 2013/14..................................................................9
APPENDIX 1: HAND HYGIENE DATA ................................................................. 10
APPENDIX 2: CLOSTRIDIUM DIFFICILE DATA...................................................11
APPENDIX 3: MRSA and MSSA DATA................................................................ 13
APPENDIX 4: EDUCATION DATA.........................................................................16
APPENDIX 5: USE OF SINGLE ROOMS...............................................................17
INFECTION CONTROL ANNUAL REPORT 2012-2013
230413 Annual Report: Final 3
1. SUMMARY
This report covers the period 1st April, 2012 to 31st March, 2013.
Performance in infection prevention and control over the past year has been excellent. The local target for Meticillin Resistant Staphylococcus aureus (MRSA) bacteraemia was met, with just one case in the year. Performance in relation to Clostridium difficile has noticeably improved with fourteen fewer cases and three less than the target set for the year. Meticillin Sensitive Staphylococcus aureus (MSSA) bacteraemia rates compare very favourably with similar sized Trusts in the West Midlands. MRSA screening compliance of 95% was achieved overall across the Trust. Influenza activity was negligible locally. Norovirus activity was significant during quarter three in keeping with regional and national rates.
2. ACHIEVEMENTS AND INITIATIVES 2.1 The following were key achievements and initiatives during the year:
2.1.1 Contribution to the continued development of the FY1 Doctors shadowing programme.
2.1.2 40% of policies standards and quick reference guides review and re-published 2.1.3 Julie Clarke successfully completed her Masters studies 2.1.4 MRSA bacteraemia target was met 2.1.5 No PII or Outbreaks of C.difficile for the whole year 2.2.6 C.difficile target was bettered 2.2.7 Development and provision of on line training for clinical updating 2.2.8 Contribution to the reduction of Catheter Associated Urinary Tract Infection
(CAUTI)
3. UNPLANNED ACTIVITY 3.1 Outbreak management (Norovirus)
3.1.1 The early incidence of Norovirus outbreaks resulted in a very significant challenge for the whole of quarter 3. This resulted in nineteen outbreaks or incidents where an outbreak was suspected but did not develop. The frequency and severity of outbreaks subsided during quarter 4. There were six instances where the outbreak definition was met but none of these developed into significant outbreaks.
3.1.2 End of year data shows that there were twenty eight instances where the
outbreak definition was met. Of these seven resulted in total ward closure as opposed to closure of bays within wards. Norovirus was confirmed in sixteen instances. A total of 222 patients and 55 members of staff were affected.
3.3 Clostridium difficile investigations
Periods of Increased Incidence (PII) occur when there are two cases of Trust acquired Clostridium difficile in a ward area within 28 days of each other. An outbreak is declared when two cases are of the same ribotype.
There were no instances of PII or outbreaks of C. difficile at the Queens Hospital site for the whole of the year. This is the first time that this has been achieved. There was one PII at Samuel Johnson Community Hospital in October 2012.
Further discussion about C.difficile is at paragraph 4.7
3.4 Influenza
Influenza activity in Trust this winter was insignificant. FFP3 respiratory mask fittings continued to be offered during the summer with no uptake. Vaccination uptake was poor There was no requirement this year to implement any contingency plans. Stocks of essential personal protective equipment are being maintained.
230413 Annual Report: Final 4
3.5 MRSA “Hot Spots” No “hot spot” investigations were required during this year. This indicates that numbers of patients colonised with MRSA in individual ward areas did not give rise to concern regarding transmission of the organism within the ward.
3.6 Vancomycin Resistant Enterococci (VRE) in Critical care
A significant investigation took place having identified a number of patients who were found to be colonised with VRE in Critical care. VRE was first isolated from two vascular catheter tips from different patients in Critical care on the same day (19th January 2013). A number of actions including screening of patients and the environment have been undertaken. Outbreak meetings were held appropriately with representatives from the Health Protection Agency and Commissioners. Weekly screening continues. Initial findings found colonisation in three other patients and in the environment. Since these were the same strain it is reasonable to conclude that in January there was transmission of the organism between patients either via healthcare workers, the environment or a combination of both.
A total of seventeen patients have been identified as colonised with VRE. Fifteen of these have been identified by active screening rather than from clinical specimens. Of these eight appear to have become colonised extremely quickly (within three days) of admission to Critical care. No other markers of Healthcare Associated Infection have risen. There have been no significant changes in rates of MRSA, MSSA, E.coli or C.difficle within the unit. Hand hygiene compliance requires significant improvement but it would appear that the current deficit arises from visiting staff. In total sixty eight different patients have been screened. Prevalence rates appear to be in keeping with a number of studies of active VRE surveillance in critical care units.
3.7 BLITZ Campaign
BLITZ was born following an outbreak of C.difficile Ribotype 027 in September 2011 continued to be promoted during the whole of the year. The objective was to raise the bar ensuring that standards of practice improve and are sustained at the appropriate levels rightly expected by patients. Measurement of success was evidenced by improved assurance auditing scores, a reduction in healthcare acquired infection and no outbreaks.
4. PLANNED ACTIVITY 4.1 Progress against the annual plan
The following objectives from the rolling annual plan for 2012/2013 were delivered:
4.1.1 Maintain and improve delivery of routine infection prevention and control practice in accordance with part A of the annual plan.
4.1.2 Deliver new national reporting requirements for Meticillin Sensitive Staphylococcus Aureus (MSSA) bacteraemia and E.coli bacteraemia.
4.1.3 Work to embed the Ward Commendation Scheme in practice 4.1.4 Modify environmental audit tools to suit the local situation given the
unsuitability of available tools. 4.1.5 Contribution to reduction in catheter associated urinary tract infection 4.1.6 Contribute to improved compliance with the requirement to conduct MRSA
screening for all relevant patients. 4.1.7 Deliver a free service under a SLA for St Giles Hospice 4.1.8 40% of Policies, Standards and Quick Reference Guides reviewed and
revised. 4.1.9 Fulfilling all data requirements for centrally reported data and for
commissioners Formal audit and monitoring projects 4.1.10 Compliance with MRSA guidelines
230413 Annual Report: Final 5
4.1.11 Peripheral intravenous devices 4.1.12 MRSA acquisition in Trust 4.1.13 Compliance with hand hygiene in clinical practice 4.1.14 MRSA screening performance 4.1.15 Contract supervision – pressure relieving mattresses 4.1.16 Formal audit of endoscopy services using approved global rating scale
criteria
4.2 Audit Environmental auditing tools were modified from existing tools and the best aspects of the new tools leading to the ability to continue computer based entry and reporting. This ensures efficient use of time and concentration on the key areas of the hospital environment. Results are disseminated as part of the Ward Commendation Scheme. Hand hygiene auditing is now fully devolved to wards. Results are comparable to those that were obtained when performed solely by the infection prevention and control team. Results are disseminated as part of the Ward Commendation Scheme.
4.3 MRSA Screening Screening has been continued throughout the year with no changes in the categories of patients requiring this to be done. Contractually compliance should be 95% overall which includes relevant elective admissions and non-elective admissions. Analysis of the data at this trust shows that of the day case admissions 0.11% was found to be colonised with MRSA in the year 2011/12. This calls into question the value of carrying out these screens especially as the results are not known until after the patient has been discharged. The exclusion of this category of patient for screening going forward was not agreed by commissioners. Compliance with the screening standard has been challenging with performance on the Queens site ranging from 93.08% to 94.41%. When the Community Hospital performance is taken into account this improves to 95% - 96%.
4.4 Surveillance: Alert Organism This surveillance relates to organisms identified to the team via the HISS system as requiring immediate or urgent action on a daily basis. This includes action required within the Trust and those organisms causing conditions which require reporting to the Health Protection Agency (HPA). Clostridium difficile, MRSA bacteraemia and other infection/colonisation with MRSA will be considered below. National Surveillance was extended to include blood stream infection caused by Meticillin Sensitive Staphylococcus Aureus (MSSA) and Escherichia Coli (E.Coli).
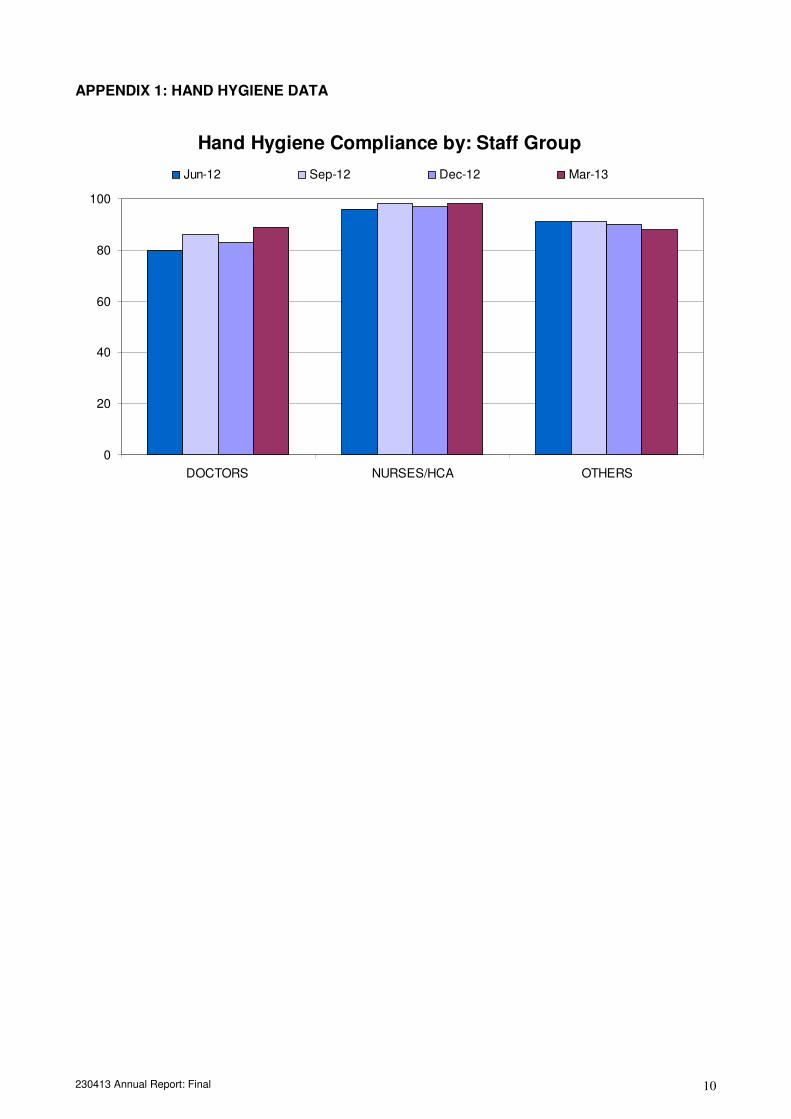
4.5 Hand hygiene
Hand hygiene audit has now been fully devolved to ward and department level. They are now conducted as part of the self assessment aspects of the Ward Commendation Scheme. Where there appears to be less than optimal performance assurance will be sought by confirmatory audit undertaken by the infection prevention and control team. Where there is evidence of transmission of pathogens between patients the frequency of hand hygiene audit is increased.
Data are shown at appendix 1.
4.6 Surveillance: Surgical site infection (SSI)
Mandatory surveillance in orthopaedics of total knee and hip replacements was completed at the end of quarter four of 2012/13 as planned. Results are not yet available. The next cycle of audit will commence on 1st January 2014.
230413 Annual Report: Final 6
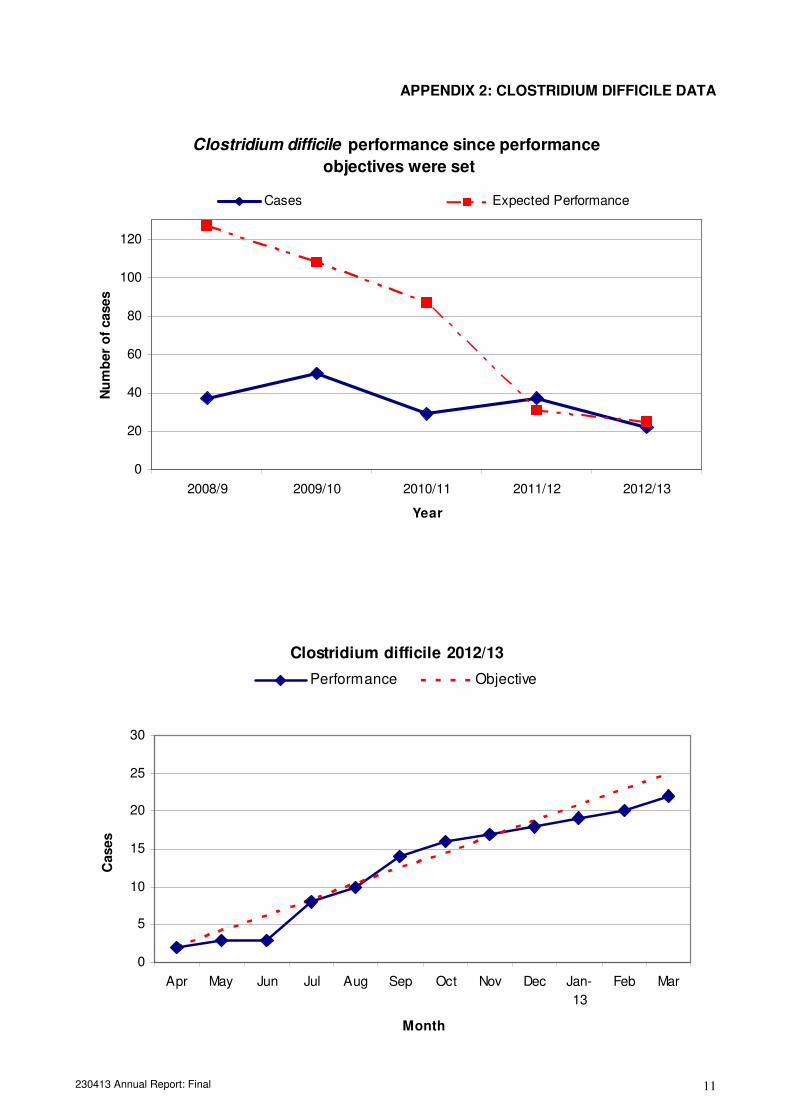
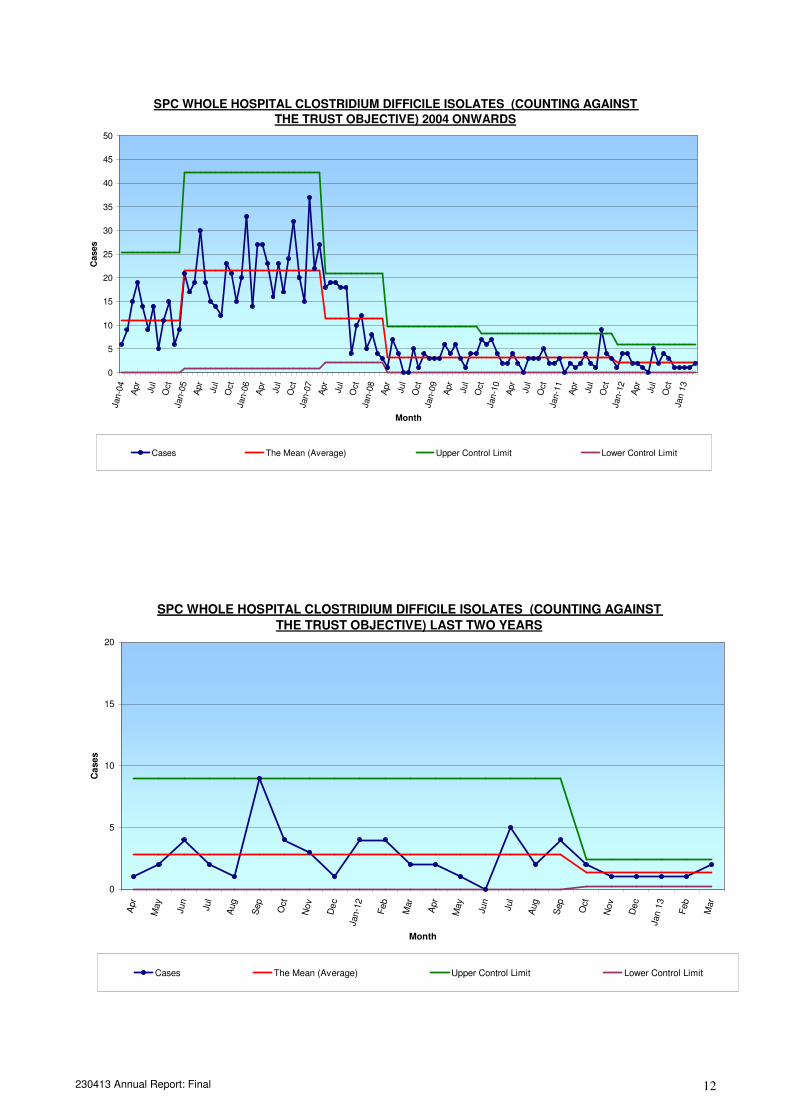
4.7 Clostridium difficile infection
Once again this was a challenging year in meeting the target set by the DH. Despite the fact that there were no PII or outbreaks there was concern at the mid year point that the Trust would overshoot the target by a significant number of cases. At that time contact was made with three similar sized Trusts who were performing better in this regard. The purpose of this was to learn from the best performers, assess Trust practice against what others were doing and apply those which may have a positive benefit for patients here. There was a move to disposable wash bowls, the consideration of a new antibiotic for certain cases and the active assessment and isolation of “carriers”. The end of year outcome was that the position was recovered and the target bettered by three cases Data are at appendix 2
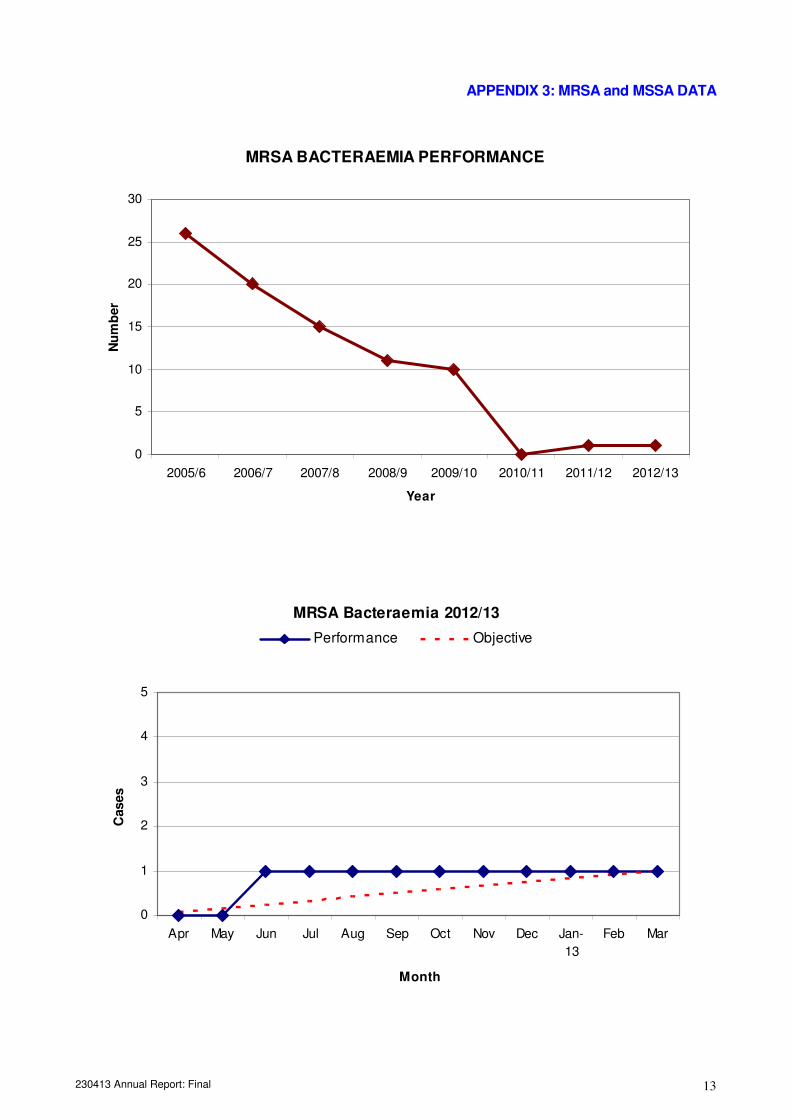
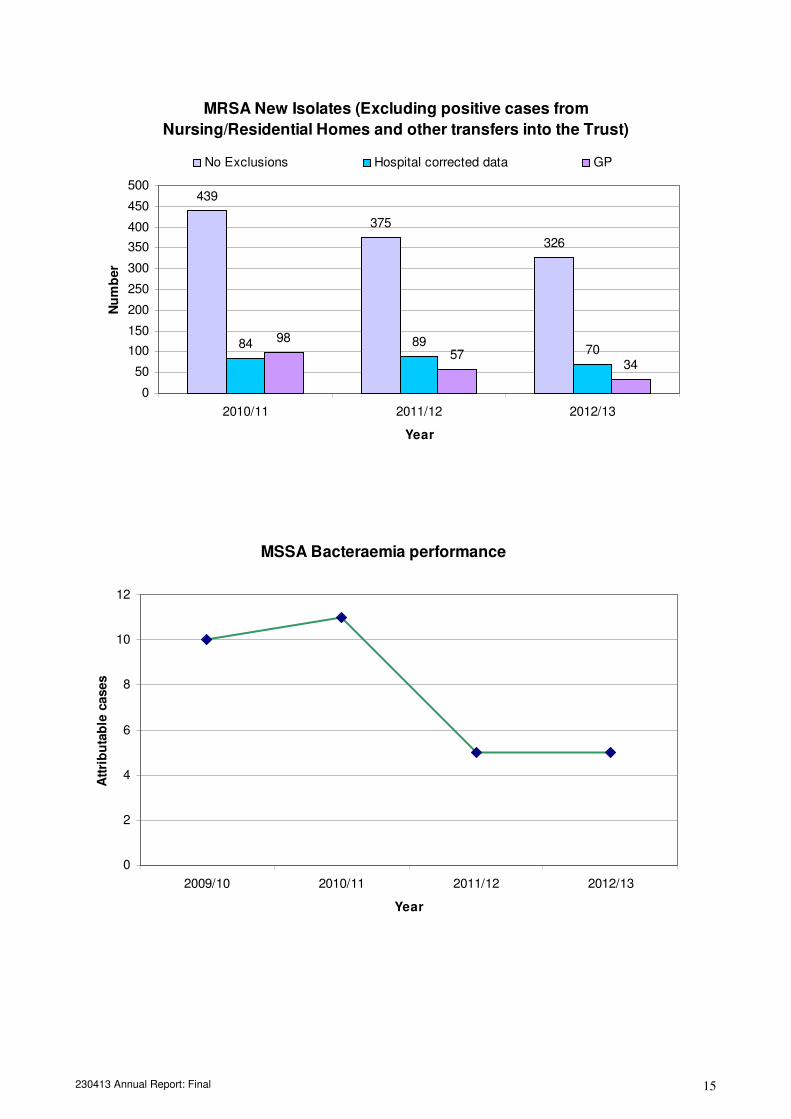
4.8 Meticillin Sensitive Staphylococcus Aureus (MSSA) bacteraemia The requirement to nationally report all instances of MSSA bacteraemia continued throughout the year. Criteria for attribution of Trust apportioned cases are the same as those set for MRSA bacteraemia. Trust performance this year continues to be very encouraging with just five cases during the whole year. This data compares very favourably to other similar sized providers. Once again no specific target has been set for the coming year. Root cause analysis will be continue to be carried out when cases occur so that learning can be applied to practice thus reducing the risk of harm to patients.
Data are presented at appendix 3
4.9 Meticillin Resistant Staphylococcus Aureus (MRSA) bacteraemia The national target set for the Trust was that there should be an aspiration of zero cases in the year. The Trust was at that time one of twenty five Trusts in the UK which had been commended by the Department of Health (DH) for having gone more than one year between cases. No actual target was set by the DH and our commissioners set a local target of no more than one case. The Trust had one case during the year and thus the locally set target was met. Five other cases not counting against the Trust trajectory were referred for investigation to the relevant Primary Care Trust (PCT). There is now a new national “zero tolerance” approach to MRSA blood stream infections. New post infection review actions within a strictly limited time frame are required in the event of a case. Our aim will be to achieve zero cases in the coming year.
Data are given within Appendix 3.
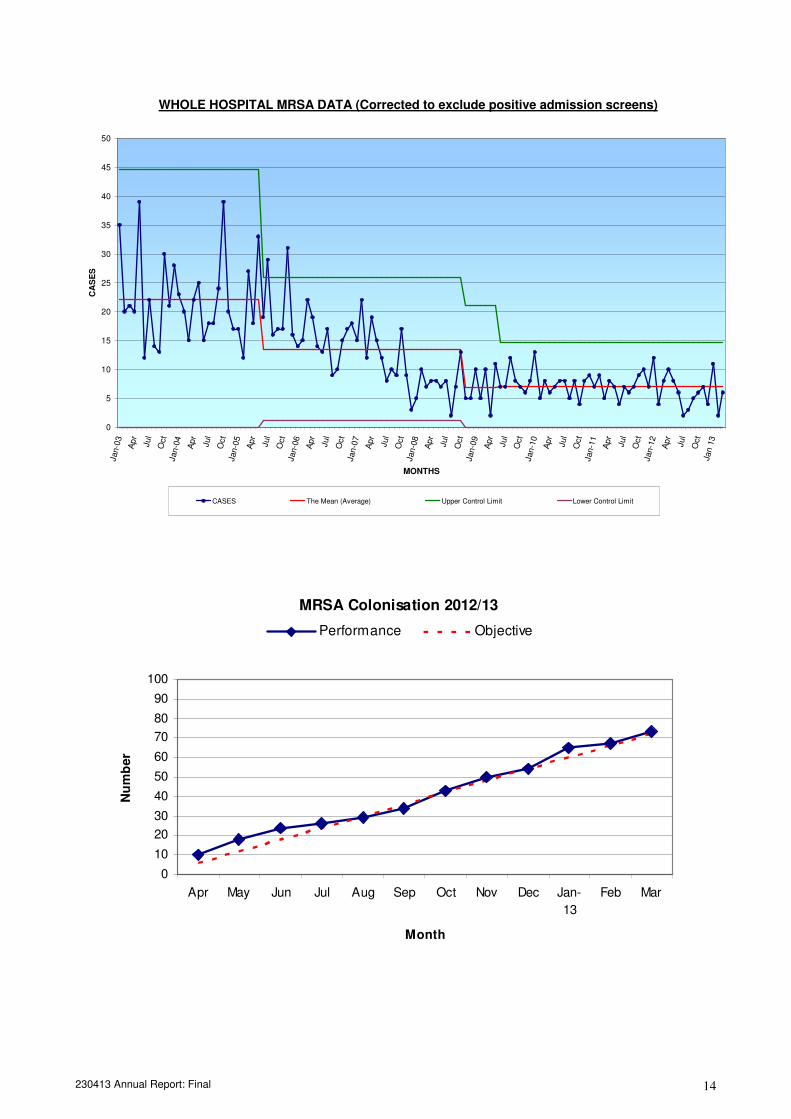
4.10 MRSA other infection/colonisation
Data are presented in appendix 3 and includes all new isolates of MRSA whether colonised or infected and whether originating from the Trust or from elsewhere. The number of MRSA colonisation has fallen this year as has the number of Trust acquired MRSA colonisation. The Trust should continually strive to significantly reduce this number. The risks of cross infection are mitigated by the Patient Group Directive (PGD) for prescribing decolonisation/suppression treatment.
4.11 Escherichia coli (E.coli) bacteraemia E.coli infections are very common and are often linked with urinary tract infections and patients who have indwelling urinary catheters. One hundred and twenty six cases were reported to the Health protection Agency during the year. All except twenty of these occurred in patients who were admitted with the infection and were not acquired within the Trust.
230413 Annual Report: Final 7
4.12 Ward Commendation Scheme
There has been no significant change to the three core elements to the scheme which are; monthly self assessment, quality assurance and outcome measures. Data is fed back to wards on a monthly basis. Areas which give rise to concern are followed up.
4.13 Water safety
Management and control of Legionella has always been a fundamental part of water safety. Similar controls now apply to Pseudomonas aeruginosa an organism which is particularly harmful to those who are most vulnerable. These patients are those being those cared for in critical care and the neonatal unit. A water safety group has been established and meets quarterly to monitor water testing results and to review actions taken where results give rise for concern. Immediate actions are taken in between meetings should results of routine testing require them. In addition microbiological results are monitored to ensure that these high risk patients have not been affected.
4.14 Data feedback
Data regarding rates of MRSA and Clostridium difficile are analysed monthly and disseminated across the Trust to the Board and to wards via the appropriate reporting structures. Weekly and monthly reports are also produced for Commissioners.
4.15 Link Person Group The link person group continued to be well attended with meetings also held for staff at the Community Hospitals. These meetings give staff the opportunity to raise issues for discussion and share best practice with their colleagues, alongside the provision of further education. Topics included in meetings were: 4.15.1 Performance data feedback
4.15.2 Root Cause Analysis feedback
4.15.3 Aseptic non-touch technique
4.15.4 Pseudomonas Aeruginosa
4.15.5 Changes to Clostridium Difficile testing
4.15.6 Norovirus Outbreak Management
4.15.7 Pertussis
4.15.8 Vancomycin Resistant Enterococci
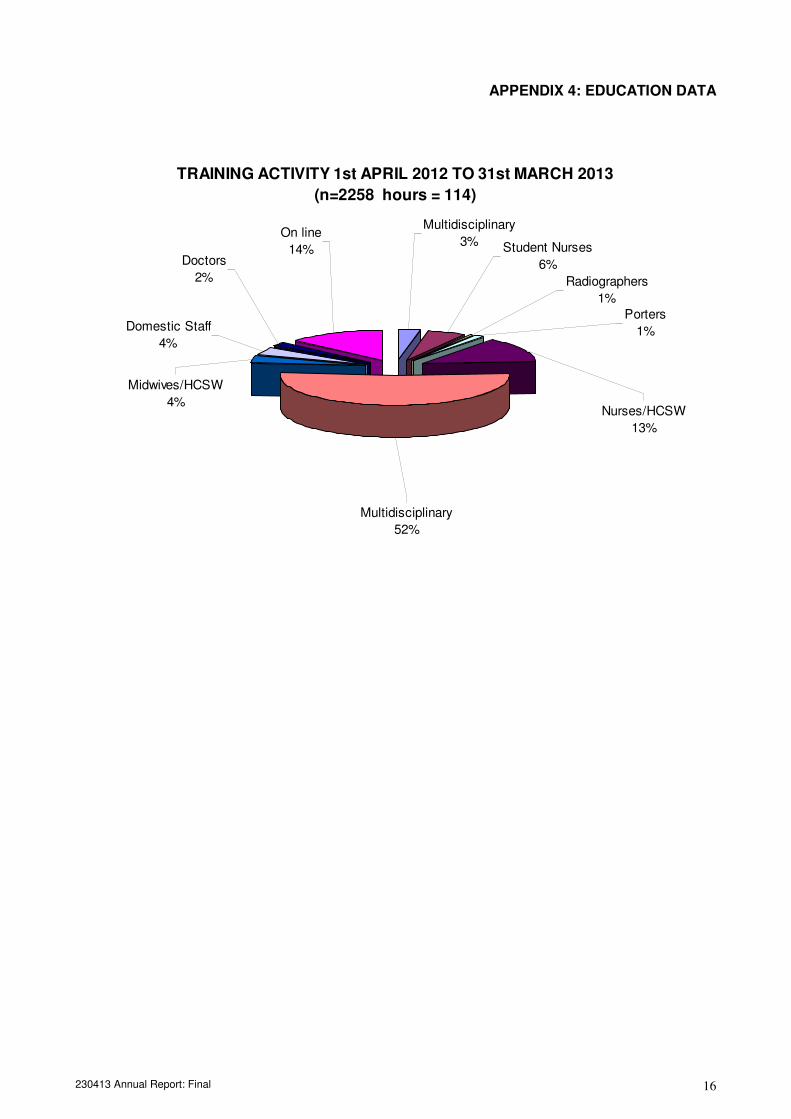
4.16 Education and Training There were 114 hours of infection control education delivered to approximately 1950 Trust staff and volunteers during the year by face to face method of delivery. This year saw the development of an on line version of the IC2 mandatory update session for clinical staff. This was available from September 2012 and 383 staff attempted update by this means of which 308 completed.
There were several core and bespoke presentations as listed below: 4.16.1 IC1 Induction 4.16.2 IC2 Mandatory annual update for staff with clinical contact with patients 4.16.3 IC3 Mandatory annual update for staff (Domestic Services, Porters) 4.16.4 IC4 Mandatory 3 yearly update for staff with no clinical contact with patients 4.16.5 First year (Pre ward) student nurses 4.16.6 Developments in infection prevention and control for second year student
nurses 4.16.7 NVQ level 2 and 3 4.16.7 Volunteers 4.16.8 St Giles Hospice mandatory annual updates for clinical staff 4.16.9 Work experience induction sessions
230413 Annual Report: Final 8
The foundation work for the on line session for 2013/14 has been completed and has been “live” from 1st April 2013. Data presenting numbers attending and staff group analysis are in appendix 4
4.17 Saving Lives”
The High Impact Interventions (HII) forms an integral part of the Ward Commendation Scheme. There is an expectation that practice in relation to all relevant interventions will be assessed on a monthly basis with feedback via the ward commendation scheme.
4.18 Infection Control Intranet Site The site has been maintained throughout the year and is the prime vehicle for data feedback, publishing standards, quick reference guides and highlighting new issues. On a daily basis an infection state is published. This highlights those areas where there are patients with infections, and what those infections are to all staff. In addition there are daily reports regarding any ongoing outbreaks of Norovirus in the Trust.
4.19 St Giles Hospice (Whittington) The IPCT has delivered the service level required in accordance with the Service Level Agreement. This involves delivery infection prevention and control update, seven sessions annually and general infection prevention and control advice as required.
5. ISOLATION FACILITIES
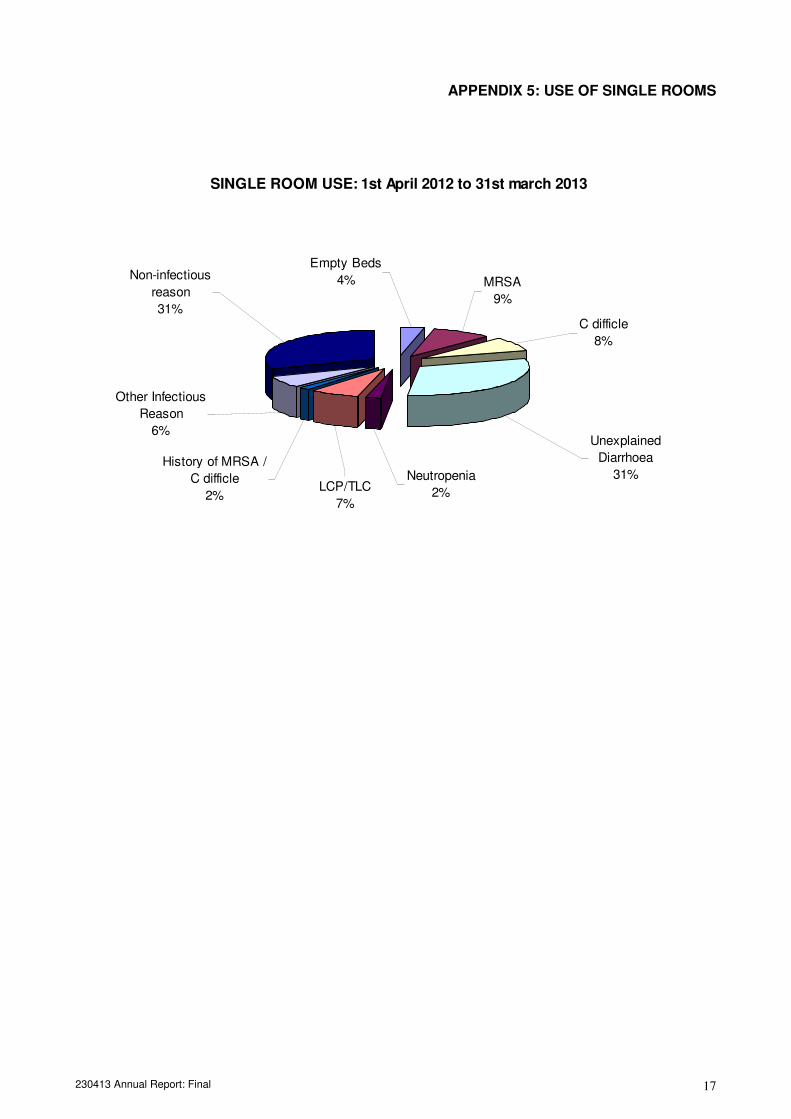
Ideally all patients with MRSA colonisation/infection should be cared for in single rooms. Patients with Clostridium difficile infection should be cared for in a single room for the duration of their admission. In addition those patients who are found to be carriers of C.difficile are managed through isolation similar to patients with active toxin producing infection, and are given treatment if symptomatic. Weekly isolation deficit audit has been maintained throughout the year and findings are as follows:
• MRSA deficits: 242
• Clostridium difficile deficits: 2
• VRE deficits 11 Isolation management tools have been provided to ensure that the appropriate patient is cared for in the appropriate environment. Instances where there have been deficits in isolating patients with C.difficile and VRE colonisation occurred in Critical care where there are no single room facilities. The number of deficit instances for MRSA patients has fallen but will continue at high levels due to admission screening. The prompt operation of the prescribing set for MRSA decolonisation/suppression treatment is a crucial activity in preventing potential cross infection between patients. Despite that fact that MRSA patients are being cared for in open wards there is no evidence of significant transmission of the organism between patients. Data is presented at appendix 5 on the utilisation of single rooms.
6. STAFFING The department is undergoing significant change. One member of staff has just started maternity leave and a seconded member of staff is expected in post shortly to cover this period. The administrative team co-ordinator post is currently vacant with help being provided from the Corporate Nursing Team during each weekday morning. One team
230413 Annual Report: Final 9
member successfully completed her masters’ degree studies in Infection Prevention and Control. The other infection Prevention and Control Nurse has now successfully completed her first year of study towards a masters degree.
7. CARE QUALITY COMMISSION The Care Quality Commission undertook four unannounced visits to the Trust during the year. The second visit in June 2012 confirmed that “there was evidence available to confirm suitable practices were in place regarding infection control and its management”. Thus it was confirmed that the Trust was compliant with Outcome 8 of the essential standards of quality and safety.
8. MEETINGS AND REPORTS The IPCT is represented at numerous committees and groups both within the Trust and the whole health economy. The Infection Prevention Board met quarterly throughout the year receiving reports and papers from the IPCT and directorates. The Board reports to the Board of Directors via the Governance Risk and Assurance Committee to which quarterly reports are submitted.
9. INFECTION PREVENTION AND CONTROL POLICY The infection prevention and control policy has been amended to reflect the changes to the delivery of infection control services within the Trust. Infection Control Standards and quick Reference Guides have been developed to replace what were known as guidelines. This activity is now forty percent complete. Further revisions will be brought before the Infection Prevention Board for ratification as authorised by Policy.
10. INNOVATION There is an opportunity for the Trust to be involved as one of three pilot sites in the UK in cutting edge technology relating to remote audit of hand hygiene compliance. Initial steps have been taken and a response is now awaited from the company involved so that the project can proceed.
11. KEY THEMES FOR THE YEAR 2013/14 The actions listed below are key themes extracted from the annual plan for healthcare associated infections which was tabled at the Infection Prevention Board on 25th April 2013.
11.1 Actions to meet the challenge of meeting the C.difficile target 11.2 Identify evaluate trial and implement new disinfectant wipes Trust wide 11.3 Maintain and improve delivery of routine infection prevention and control practice. 11.4 Contribute to the implementation of EU Directive 2010/32/EU (Prevention of sharps
injuries in the healthcare sector) 11.5 Co-ordinate local reporting for new Health Protection England surveillance systems. 11.6 Continue to work to embed the “HOUDINI” principles in relation to catheter
associated urinary tract infection 11.7 Contribute to improved compliance with the requirement to conduct MRSA
screening for all relevant patients. 11.8 Complete the re-categorisation revision and publication of Policies, Procedures and
Quick Reference Guides 11.9 Technological advances in hand hygiene compliance monitoring
230413 Annual Report: Final 10
APPENDIX 1: HAND HYGIENE DATA
Hand Hygiene Compliance by: Staff Group
0
20
40
60
80
100
DOCTORS NURSES/HCA OTHERS
Jun-12 Sep-12 Dec-12 Mar-13
230413 Annual Report: Final 11
APPENDIX 2: CLOSTRIDIUM DIFFICILE DATA
Clostridium difficile performance since performance
objectives were set
0
20
40
60
80
100
120
2008/9 2009/10 2010/11 2011/12 2012/13
Year
Nu
mb
er
of
cases
Cases Expected Performance
Clostridium difficile 2012/13
0
5
10
15
20
25
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan-
13
Feb Mar
Month
Cases
Performance Objective
230413 Annual Report: Final 12
SPC WHOLE HOSPITAL CLOSTRIDIUM DIFFICILE ISOLATES (COUNTING AGAINST
THE TRUST OBJECTIVE) 2004 ONWARDS
0
5
10
15
20
25
30
35
40
45
50
Jan-0
4
Apr
Jul
Oct
Jan-0
5
Apr
Jul
Oct
Jan-0
6
Apr
Jul
Oct
Jan-0
7
Apr
Jul
Oct
Jan-0
8
Apr
Jul
Oct
Jan-0
9
Apr
Jul
Oct
Jan-1
0
Apr
Jul
Oct
Jan-1
1
Apr
Jul
Oct
Jan-1
2
Apr
Jul
Oct
Jan
13
Month
Cases
Cases The Mean (Average) Upper Control Limit Lower Control Limit
SPC WHOLE HOSPITAL CLOSTRIDIUM DIFFICILE ISOLATES (COUNTING AGAINST
THE TRUST OBJECTIVE) LAST TWO YEARS
0
5
10
15
20
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
De
c
Jan
-12
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
De
c
Jan
13
Feb
Mar
Month
Ca
se
s
Cases The Mean (Average) Upper Control Limit Lower Control Limit
230413 Annual Report: Final 13
APPENDIX 3: MRSA and MSSA DATA
MRSA BACTERAEMIA PERFORMANCE
0
5
10
15
20
25
30
2005/6 2006/7 2007/8 2008/9 2009/10 2010/11 2011/12 2012/13
Year
Nu
mb
er
MRSA Bacteraemia 2012/13
0
1
2
3
4
5
Apr May Jun Jul Aug Sep Oct Nov Dec Jan-
13
Feb Mar
Month
Cases
Performance Objective
230413 Annual Report: Final 14
WHOLE HOSPITAL MRSA DATA (Corrected to exclude positive admission screens)
0
5
10
15
20
25
30
35
40
45
50
Jan-0
3
Apr
Jul
Oct
Jan-0
4
Apr
Jul
Oct
Jan-0
5
Apr
Jul
Oct
Jan-0
6
Apr
Jul
Oct
Jan-0
7
Apr
Jul
Oct
Jan-0
8
Apr
Jul
Oct
Jan-0
9
Apr
Jul
Oct
Jan-1
0
Apr
Jul
Oct
Jan-1
1
Apr
Jul
Oct
Jan-1
2
Apr
Jul
Oct
Jan 1
3
MONTHS
CA
SE
S
CASES The Mean (Average) Upper Control Limit Lower Control Limit
MRSA Colonisation 2012/13
0
10
20
30
40
50
60
70
80
90
100
Apr May Jun Jul Aug Sep Oct Nov Dec Jan-
13
Feb Mar
Month
Nu
mb
er
Performance Objective
230413 Annual Report: Final 15
MRSA New Isolates (Excluding positive cases from
Nursing/Residential Homes and other transfers into the Trust)
439
375
326
84 8970
98
5734
0
50
100
150
200
250
300
350
400
450
500
2010/11 2011/12 2012/13
Year
Nu
mb
er
No Exclusions Hospital corrected data GP
MSSA Bacteraemia performance
0
2
4
6
8
10
12
2009/10 2010/11 2011/12 2012/13
Year
Att
rib
uta
ble
cases
230413 Annual Report: Final 16
APPENDIX 4: EDUCATION DATA
TRAINING ACTIVITY 1st APRIL 2012 TO 31st MARCH 2013
(n=2258 hours = 114)
On line
14%
Radiographers
1%
Student Nurses
6%
Porters
1%
Nurses/HCSW
13%
Multidisciplinary
3%
Doctors
2%
Domestic Staff
4%
Midwives/HCSW
4%
Multidisciplinary
52%
230413 Annual Report: Final 17
APPENDIX 5: USE OF SINGLE ROOMS
SINGLE ROOM USE: 1st April 2012 to 31st march 2013
Non-infectious
reason
31%
Empty Beds
4% MRSA
9%
C difficle
8%
Unexplained
Diarrhoea
31%Neutropenia
2%LCP/TLC
7%
Other Infectious
Reason
6%
History of MRSA /
C difficle
2%














![ECH zarzadzanie jakoscia 250413.ppt [tryb zgodności]ekspercibolonscy.org.pl/ekspercibolonscy.org.pl/sites/e... · 2016-09-20 · WARUNKIEM EFEKTYWNEGO FUNKCJONOWANIA WEWNĘTRZNEGO](https://img.pdfslide.net/doc/110x75/5c75e5e409d3f25d028b7583/ech-zarzadzanie-jakoscia-tryb-zgodnosciekspercibolonscyorgplekspercibolonscyorgplsitese.jpg)