Embed Size (px)
Citation preview

2 reports follow, first by Ciaran Malone ( Belfast), second by Samir Dawoud (Leeds)
Ciaran Malone (Northern Ireland Cancer Centre, Belfast
From the 19th
to the 23rd
of April
descended on the Palexpo in Geneva, Switzerland for the 2
being recognised as a global financial centre
easy reach of CERN was a unique
ESTRO forum hosted several meetings reflecting the different interdisciplinary aspects of
radiation oncology. The Clinical & Translational
the Physics Biennial meeting, the
Evaluation and Eradication of Normal Tissue effects of radiotherapy)
different disciplines together to
experience.
The scientific experts of the five meetings
including symposia, presidential and joint sessions, teaching lectures and debates spread
over the main auditorium and
physicists, biologists, radiat
international meeting, it was hard not to be overwhelmed with the sheer volume of
interesting talks held in parallel sessions, making it impossible to attend
most of my time within the physics sessions which covered modern and rapidly changing
topics such as dose verification of advanced radiotherapy, small field challenges, image
guided and adaptive radiotherapy, proton dosimetry, the flatt
Figure 1. One of the ten congress rooms that hosted topics throughout the five days.
Intrafraction motion managemen
My current work focuses mainly on
such, I was particularly interested in
radiotherapy to learn more about new concepts and practices in the use
alternatives that are available.
guided radiotherapy and intrafraction motion management
2nd
ESTRO Forum 2013
19-23 April 2103
Geneva, Switzerland 2 reports follow, first by Ciaran Malone ( Belfast), second by Samir Dawoud (Leeds)
Northern Ireland Cancer Centre, Belfast): of April approximately 3,700 delegates from
on the Palexpo in Geneva, Switzerland for the 2nd
ESTRO Forum 2013. Geneva,
being recognised as a global financial centre, a worldwide centre for diplomacy
unique location for such a large and international event.
several meetings reflecting the different interdisciplinary aspects of
Clinical & Translational meeting, the GEC-ESTRO
meeting, the RTT meeting, and the PREVENT (Prediction, Recognition,
aluation and Eradication of Normal Tissue effects of radiotherapy) meeting
disciplines together to facilitate interesting exchanges of knowledge and
The scientific experts of the five meetings compiled an impressive scientific programme
including symposia, presidential and joint sessions, teaching lectures and debates spread
the main auditorium and 10 rooms (figure 1), dedicated to clinicians, med
physicists, biologists, radiation technologists and nurses. As it was my first major
was hard not to be overwhelmed with the sheer volume of
in parallel sessions, making it impossible to attend
thin the physics sessions which covered modern and rapidly changing
topics such as dose verification of advanced radiotherapy, small field challenges, image
guided and adaptive radiotherapy, proton dosimetry, the flattening filter free modality and
intrafraction motion management. Due to
the volume of talks held concurrently
the five days it is impossible to cover
everything and even harder to fit it all into
one article. Thus, I selected
that related to my work
particularly interesting
selection offers a taste of the topics
covered in the ESTRO 2nd
Figure 1. One of the ten congress rooms that hosted topics throughout the five days.
Intrafraction motion management
mainly on intrafraction motion management, specifically 4DCT
was particularly interested in talks related to intrafraction motion and image guided
to learn more about new concepts and practices in the use
alternatives that are available. Over the course of the conference it was clear that
guided radiotherapy and intrafraction motion management are rapidly developing area
2 reports follow, first by Ciaran Malone ( Belfast), second by Samir Dawoud (Leeds)
from over 80 countries
ESTRO Forum 2013. Geneva,
worldwide centre for diplomacy and within
uch a large and international event. The 2nd
several meetings reflecting the different interdisciplinary aspects of
ESTRO-ISIORT meeting,
ENT (Prediction, Recognition,
meeting brought the
interesting exchanges of knowledge and
scientific programme
including symposia, presidential and joint sessions, teaching lectures and debates spread
dedicated to clinicians, medical
as my first major
was hard not to be overwhelmed with the sheer volume of
in parallel sessions, making it impossible to attend everything! I spent
thin the physics sessions which covered modern and rapidly changing
topics such as dose verification of advanced radiotherapy, small field challenges, image
ening filter free modality and
intrafraction motion management. Due to
held concurrently over
the five days it is impossible to cover
and even harder to fit it all into
selected a few talks
o my work or that I found
and hopefully this
offers a taste of the topics nd
Forum.
Figure 1. One of the ten congress rooms that hosted topics throughout the five days.
specifically 4DCT. As
related to intrafraction motion and image guided
to learn more about new concepts and practices in the use of 4DCT and any
t was clear that image
rapidly developing areas of

radiotherapy. For example, I selected three of the talks
interesting:
A “Novel 4DCT technique for breathing motion modelling”
Center for Radiation Oncology, USA)
free images and the ability to generate
Coming from a 4DCT background
irregular breathing artifacts in 4DCT
and deformable registration to determine
breathing phase. All the images are
image geometry and averaged.
deformed to a user specified breathing phase.
this promising technique which
clinical 4DCT protocols.
Currently, in the Northern Ireland Cancer Centre we use 4DC
patients with lung cancer and
Hospital in Dublin I was curious to learn m
ways. A presentation by N.C.M.G. Van der Voort Van
Cancer Centre, Netherlands)
choosing an internal surrogate marker that is moving sy
Her results show that a 4DCT scan is necessary to select markers moving
the tumour and that if the markers
as assessed by 4DCT, the standard deviation of the tracking errors were reduced.
The main sessions and award talks took place in the enormous
arena (figure 2). Aidan J. Cole
Ireland Cancer Centre, Belfast)
received an award for his interesting
work on the “Radiobiological implications
of respiratory motion in the treatment of
lung cancer” presented his engaging
work in the auditorium. The talk mainly
focused on the radiobiological response
to tissue cells in motion as, to date,
vitro studies examining such responses
have only been carried out exclu
under static conditions.
Figure 2. The main auditorium which hosted the opening ceremony,
topics, presidential symposium and award lectures.
, I selected three of the talks in these areas
for breathing motion modelling” presented by
Center for Radiation Oncology, USA) demonstrated a technique that can
free images and the ability to generate low-noise images at arbitrary breathing phases.
Coming from a 4DCT background I was very curious to see how it was possible t
artifacts in 4DCT images. This was achieved using multiple
to determine the tissue motion as a function of the measured
ll the images are then co-registered and are deformed to single reference
image geometry and averaged. This motion model allows the aggregate image
r specified breathing phase. I’m looking forward to learning more about
which helps solve some of the issues and pitfalls
Currently, in the Northern Ireland Cancer Centre we use 4DCT for planning treatments for
patients with lung cancer and having previously worked on a 4DCT project in St.
was curious to learn more about how 4DCT could be utilized
N.C.M.G. Van der Voort Van Zyp (Erasmus MC
Cancer Centre, Netherlands) showed how 4DCT can provide valuable information when
choosing an internal surrogate marker that is moving synchronous to the tumour motion.
Her results show that a 4DCT scan is necessary to select markers moving
markers were excluded based on their non-synchronous motion
the standard deviation of the tracking errors were reduced.
sessions and award talks took place in the enormous auditorium in
Cole (Northern
Ireland Cancer Centre, Belfast), who
received an award for his interesting
“Radiobiological implications
of respiratory motion in the treatment of
presented his engaging
. The talk mainly
focused on the radiobiological response
to tissue cells in motion as, to date, in
uch responses
have only been carried out exclusively
Figure 2. The main auditorium which hosted the opening ceremony, Clinical practice
topics, presidential symposium and award lectures.
hese areas that I found quite
presented by Daniel Low (UCLA
can produce artifact
noise images at arbitrary breathing phases.
s to see how it was possible to eliminate
multiple helical scans
the tissue motion as a function of the measured
and are deformed to single reference
aggregate image to be
m looking forward to learning more about
and pitfalls in using current
planning treatments for
previously worked on a 4DCT project in St. Luke’s
ore about how 4DCT could be utilized in other
Erasmus MC-Daniel den Hoed
provide valuable information when
nchronous to the tumour motion.
Her results show that a 4DCT scan is necessary to select markers moving synchronously to
synchronous motion
the standard deviation of the tracking errors were reduced.
auditorium in the Palexpo
Clinical practice - state of the art

Advances in radiotherapy delivery techniques to improve dose delivery and account for
respiratory motion have been introduced without full concomitant understanding of the
underlying radiobiological response. Thus, the context of the study was to determine
whether tumour motion can impact on cancer cell survival when exposed to clinically
relevant radiotherapy treatments. Results: In his talk, Aidan described a novel in vitro set up
to investigate lung cancer cell survival with respiratory motion. The study found that the
presence of respiratory motion in uniform irradiation did not differ from static conditions
for cell survival. However, when shielding was applied there was significantly higher cell
survival in-field and out-of-field with respiratory motion compared to a static set-up. The
out of field cell kill is mainly due to the “bystander” effect. With the addition of motion this
affect appears to reduce, increasing the fraction of surviving cells out of field. The setup
used is shown in Figure 3 and the results may indicate reduced efficacy of radiotherapy in
regions of inadequate tumour coverage where respiratory motion is present.
Figure 3. Experimental setup from "Radiobiological implications of respiratory motion in the
treatment of lung cancer" Dr. Aidan Cole. Picture shows the experiemental setup for in-field and out-
of-field irradiated areas.
Re-thinking margins
After previously attending a stimulating talk by Marcel van Herk (The Netherlands Cancer
Institute, The Netherlands), I decided to attend his talk on “Re-thinking margins in the daily
IGRT context” and it did not disappoint. Marcel talked about where we should be going with
our margins and how we should be leaving the hard work to the planning system. Marcel
started with a nice overview of the past and methods of selecting margins starting with the
publication of ICRU 50, the differentiation of systematic and random errors and the trade-
off between potentially overdosing with large margins and under dosing with smaller
margins. Marcel then followed with a compelling argument to forget about conventional
margins as we know them for IMRT planning and to implement a probabilistic planning
approach. Marcel proposed that margins should be generated by incorporating the
knowledge about residual uncertainty distributions directly into IMRT planning. Thus, robust
dose distributions can be sculpted that take into account the actual shape of the dose
distribution and location of the organs at risk when generating a ‘margin’.
Dose verification for advanced radiotherapy
Mark Podesta (Maastro, The Netherlands) presented an interesting piece on “Time
dependent pre-treatment verification of VMAT using flattened or flattening filter free
beams”. Pre-treatment verification of VMAT deliveries are difficult, as with dynamic
treatments the field shape, dose-rate and gantry are all varying with time. For static
treatments, misalignments and dose discrepancies are visible using standard tolerances e.g.
3%/3mm. However these deviations can be missed with dynamic treatments as deviations
during the delivery can average out and so are hidden in integrated Portal Dose Images
(PDIs). Mark Podesta and his team added the time dimension into the tolerances e.g.
3%/3mm/3sec to account for the variations the static integrated model would miss. In his
talk Mark described a general calibration method for EPIDs to measure both flattened and
FFF beams in a time dependent manner. Deviations from predicted doses were observed
that are typically hidden in integrated PDIs. They found that typically the first and last
control points deviate most but typically contain relatively low dose compared to the rest of
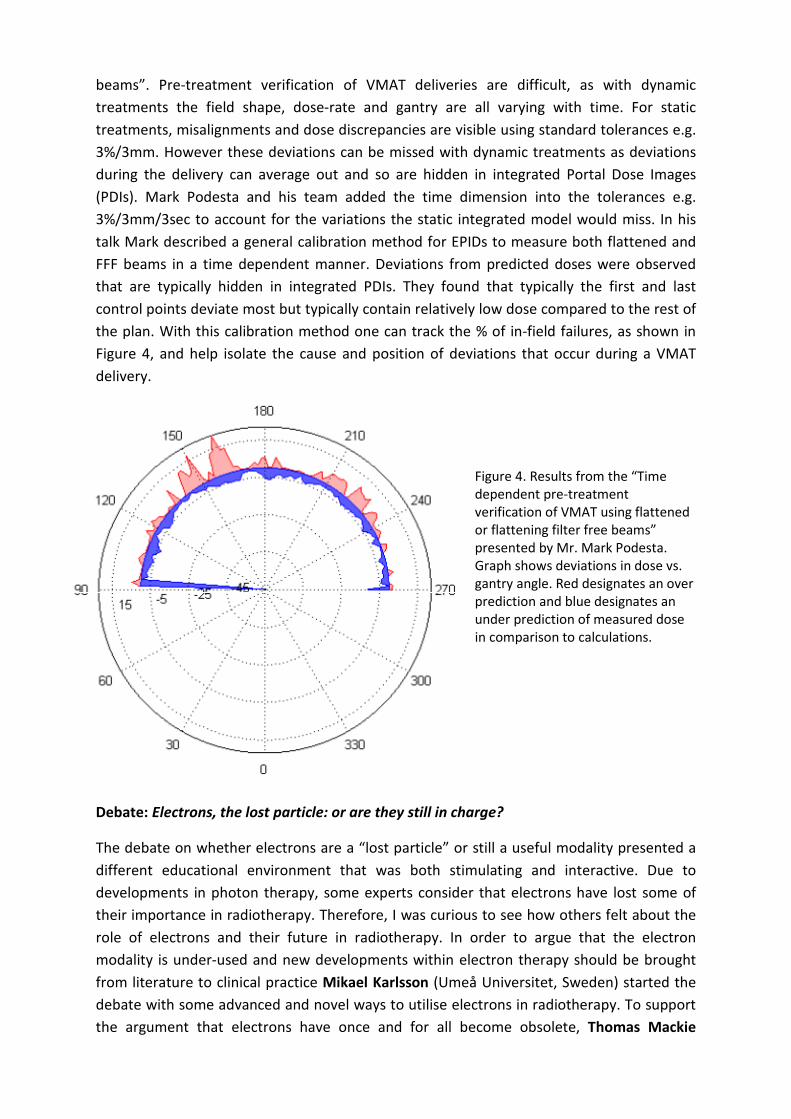
the plan. With this calibration method one can track the % of in-field failures, as shown in
Figure 4, and help isolate the cause and position of deviations that occur during a VMAT
delivery.
Figure 4. Results from the “Time
dependent pre-treatment
verification of VMAT using flattened
or flattening filter free beams”
presented by Mr. Mark Podesta.
Graph shows deviations in dose vs.
gantry angle. Red designates an over
prediction and blue designates an
under prediction of measured dose
in comparison to calculations.
Debate: Electrons, the lost particle: or are they still in charge?
The debate on whether electrons are a “lost particle” or still a useful modality presented a
different educational environment that was both stimulating and interactive. Due to
developments in photon therapy, some experts consider that electrons have lost some of
their importance in radiotherapy. Therefore, I was curious to see how others felt about the
role of electrons and their future in radiotherapy. In order to argue that the electron
modality is under-used and new developments within electron therapy should be brought
from literature to clinical practice Mikael Karlsson (Umeå Universitet, Sweden) started the
debate with some advanced and novel ways to utilise electrons in radiotherapy. To support
the argument that electrons have once and for all become obsolete, Thomas Mackie

(University of Wisconsin School of Medicine and Public Health) followed with some hard
facts about electrons diminishing role in radiotherapy making the debate both educational
and one that would split the room almost 50/50.
Mikael Karlsson began the debate by showing many examples of how electrons can be used
to form complex dose distributions and the need for a planning system that can optimize
electrons and photons together. For example, using multiple electron energies to produce
an energy modulated electron wedge as shown in Figure 5. One of Mikael’s main points was
that there is an underutilisation of both photons and electrons together, where “a mixed
electron/photon planning technique (E + IMRT) can decrease the normal tissue integral dose
compared to a photon only IMRT plan.” The first few clinical examples shown by Mikael
showed an impressive array of techniques using electrons alone and both electrons and
photons together in a beneficial way. The last area Mikael discussed was methods to modify
the treatment unit to produce much better electron dose distribution that would be more
comparable to photon dose distributions. E.g. Scanning beam or scattering foils at the target
position to reduce penumbra, Helium in the head to reduce air scatter and double focused
MLCs. What I took away from Mikael’s talk was that if the amount of research that was
undertaken in photon radiotherapy was also undertaken to improve electron radiotherapy
then electrons might be far more effective than they are currently.
Figure 5. Slides from Prof. Mikael Karlsson’s talk on the uses of electrons in radiotherapy. Examples
of how electrons can be used to produce complex and useful dose distributions. Right: Examples of
mixing photon and electron fields. Left: Mixing electron fields of different energies to produce a
wedged dose distribution.
Thomas Mackie’s talk followed to show how electrons before IMRT were used for about 5%
of all radiotherapy treatments. However, with the advent of IMRT, electron treatments have
been overshadowed by photon treatments that are easier to plan, more homogeneous and
have smaller dosimetric uncertainties. The talk described the fundamental physical flaws
with using electrons e.g. how electrons as a particle scatter easily and thus leads to a
blurring of the beam penumbra compared to photons, the bremsstrahlung tail and how the

higher electron energies are never used. T. Mackie then continued by showing examples of
how photon treatments could offer similar or even better dose distributions for sites
historically treated with electrons. e.g. To use tomotherapy or multiple tangential fields to
mould the dose distribution around the patients surface rather than using electrons.
The debate ended with strong points from both parties and no unanimous verdict was
reached. However, the debate was quite informative and promoted a lively debate on the
future role of electrons in radiotherapy. Whether we will invest in the software and
technology to optimize and utilize electrons as we currently do with photons, or simply
replace electrons with advanced photon techniques will be an interesting future to be a part
of.
Flattening Filter Free Linacs
The symposium on Flattening Filter Free linacs opened with a talk by Dietmar Georg
(Medical University of Vienna) highlighting the dosimetric challenges present when using
FFF linacs. His talk covered many aspects of FFF beam dosimetry including small field
dosimetry, radiobiology, radiation protection and pre-treatment dose verification. Dietmar’s
talk offered a great starting point for anyone not familiar with the properties of FFF beams
and their potential effects. This presentation was followed with a talk by Antonella Fogliata
(Oncology Institute of Southern Switzerland) who presented a review of the current status
of treatment planning and dose calculations for FFF beams. With a good introduction to the
characteristics of FFF beams the presentation progressed to show many interesting
examples of stereotactic and IMRT plan comparisons through recent published data
between flattened and un-flattened beams. Dr.Fogliata showed that FFF beams, used with
current treatment planning systems, are beneficial not only for stereotactic treatments but
for most other sites due to their high dose per fraction, high dose rate and lower out of field
dose to organs at risk. Following on from this, Alan Hounsell (Northern Ireland Cancer
Centre, Belfast) provided a comprehensive review of the current literature on the
radiobiological implications of FFF beams. The talk introduced some of the radiobiological
concepts used and then addressed three questions in relation to using FFF beams: Does a
change in instantaneous dose rate impact cell survival? Does the reduction in overall
treatment time impact on cell survival and does the reduction in fraction time impact on cell
survival with FFF treatment beams? Prof. Alan Hounsell showed from recent literature that
almost all recent studies, across a wide range of cell lines, agree that changes to the
instantaneous dose rate or pulse repetition frequency for FFF beams are unlikely to alter cell
response, with further careful investigation needed for doses over 10Gy. Finally, Robin
Garcia (Institut Sainte Catherine, France) ended the symposium with a talk highlighting how
care should be taken with FFF beams and that due to the differences between flattened and
un-flattened beams geometric and dosimetric tolerances need to be re-defined. During the
talk, Robin showed several examples, using delta4 phantom measurements and gamma
analysis, the effect of errors in the position, energy and angle of the treatment field,
suggesting that tolerances used for FFF beam QA must be extracted from what we would
consider as clinically acceptable effects.

Conclusions
The 2nd
ESTRO forum in Geneva was an informative and thoroughly enjoyable event and I
am very grateful to IPEM for facilitating my trip to the Forum. The wide variety of
presentation topics meant you were never left short of something to see. When the time
allowed the exhibition showcased a vast sea of new technology and software (a playground
for most radiotherapy physicists) and a place to network with people from radiotherapy and
oncology professions around the world. Due to the proximity of CERN, the biggest particle
accelerator in the world, it allowed for delegates to visit and learn about the linear
accelerators bigger brother, the Large Hadron Collider (LHC). Some pictures of CERN are
shown in Figure 6. For a physicist, this was an opportunity not to be missed!
Figure 6. Images from CERN. Top left: The ATLAS detector building. Top Right: Inside the visitor
centre. Bottom: Model showing the inside of the ATLAS detector.
In summary, the conference was an incredible opportunity which allowed me to present and
share my work in the form of an E-poster and to bring home a wealth of information, ideas
and contacts. It certainly inspired me to work towards attending another conference in the
future.

Samir Dawoud (St James Institute of Oncology - Leeds Teaching Hospitals NHS Trust):
It’s three days before the European Society for Radiotherapy and Oncology (ESTRO) 2013
conference and my colleague is furious. ‘Lunch will be available for purchase and is not
included with your conference fee,’ he exclaims, ‘what do we pay our fees for?’. We laugh
and get back to trip planning but underneath the joke lies a pertinent point; in a climate of
tight budgets and cost cutting more delegates than ever will be asking ‘can I justify the
expense to attend?’. This year, the annual 2nd
ESTRO Forum took place just outside the
beautiful city of Geneva, Switzerland, in the monolithic Palexpo centre (fig 1), which stands
just next to the airport and in the shadow of the Jura mountains (fig 2). The conference aims
to bring together the multi-disciplinary strands of radiotherapy into a single event and foster
interdisciplinary exchange. For the device manufacturers, it’s an opportunity to convince the
community that their latest kit is the last word in patient treatment, which no department
should be without. It’s an exciting prospect but it’s not a cheap one, as the conference fee
(sans lunch) attests to. So how can we qualify ‘value for money’ in relation to such
conferences?
Fig 1 The Palexpo conference venue exterior Fig 2 View of Geneva and Alps from UN
building
I’m a Part 2 radiotherapy physics trainee, so my primary aim is to present my work. ESTRO is
my first opportunity to present research that I have done to the scientific community
allowing me to further develop communication skills essential for a successful career as a
clinical scientist. As an early-career medical physicist, I’m also keen to start building a
bibliography of my own publications and ESTRO seems like the ideal place to start. I will also
be able to broaden my knowledge of radiotherapy practices through the multi-disciplinary
themes offered at the conference. At least, my bursary and study leave applications are
filled with statements like these as I plead my case for why my attendance at ESTRO is ‘value
for money’. In the weeks before the conference I was excited to receive notice of my
successful abstract submission and a little intrigued to read that I would be presenting an E-
poster. An e-poster is simply that; an electronic copy of a poster presented at a conference.
At first glance, the concept sounds quite appealing; one could imagine a dynamic poster,
with animated or video figures designed to clarify key concepts in eye-catching and
informative ways on large screens for delegates to browse at their leisure in a dedicated e-
Hub (I made up the idea of an e-Hub in my head because I’m optimistic and maybe a little

naïve). From the conference organisers’ point of view
the e-poster is an excellent idea; you can accept
more abstracts without the need to hire larger,
costlier exhibition space. I busy myself with my
poster preparations and travel arrangements and
before long I depart Manchester Airport for Geneva.
In order to off-set the cost of travel in and around
Geneva (my hotel is located on the French side of the
border, necessitating an international commute each
day to the conference) I arrange a bike-hire for the
duration of my stay. This turns out to be the best
decision I could have made; I have a swift and
picturesque ride to the conference each morning and
I have the ideal tool to explore bike-friendly Geneva
during my free time (fig 3). At the end of my visit, I’m
so attached to my trusty bike that the walk back to
my hotel feels completely alien and outrageously
time consuming (a distance of about 1 mile).
Fig 3 Me and my conference bike
At my first visit to the conference I am greeted by the cavernous exhibition space, which is
dominated by Elekta’s colossal
show-room-style stand (fig 4).
Centre stage is their latest linac;
the Versa HD. Elekta are making
quite a song and dance over the
Versa HD (figuratively of course,
as opposed to Accuray’s literal
approach; deploying ribbon-
twirling gymnasts on day one to
draw attention to their
CyberKnife and Tomotherapy
systems). Fig 4 The conference exhibition space
Away from the exhibition, the lecture sessions run in parallel with 6 streams dedicated to
various topics each day. I spend most of my time in the ‘blue’ stream, which is dedicated to
topics in physics including dosimetry, delivery, imaging and adaptive techniques. It was the
adaptive radiotherapy techniques that interested me most, not because of any personal
specialisation (as a pre-registration trainee I am hardly in a position to be considered an
authority on any subject) but because of the advances that technology has allowed in the
field. Personally, the most memorable example of this came from Tom Depuydt of
Universitair Ziekenhuis (UZ) Brussel, who summarised work using Brainlab’s Vero linac to

deliver dynamic tumour tracking as part of SBRT plans. The Vero is an intriguing machine (fig
5); with the outward appearance of a large-bore CT scanner it is in fact a compact linac
mounted on a ring-style gantry. At either side of the treatment head there are two kV-
imaging tubes, which project orthogonally to each other and 45° either side of the
treatment beam axis. This allows the system to deliver stereo fluoroscopy as well as cone-
beam CT capability. But the Vero’s truly unique feature lies in the directability of the
treatment beam; the accelerator is mounted on a gimbal, which allows the treatment beam
to be steered about a solid angle projected from the treatment head. This allows the
treatment beam to track
targets as they move about
within the field of view
defined by the limits of
movement of the gimbal
system.
Fig 5 Model of the Vero linac
from the Brainlab stand
Meanwhile, Depuydt’s presentation outlined the research and commissioning work
undertaken at UZ Brussel, including quantification of uncertainties associated with dynamic
tumour tracking, correlation of external patient markers to internal fiducial markers and the
OAR dose savings achievable using the technique, which are impressive.
But despite the advanced technology and the meticulous preparation used to achieve such
specialised treatments, a question sprang to mind that I just couldn’t resolve; is it worth it?
This is not to say that current methods of SBRT treatments cannot be improved upon but
the workload associated with the dynamic tumour tracking method seemed considerable.
For example, each such treatment requires implantation of fiducial markers, adding a level
of surgical risk to the patient. Planning time was also quoted as 1 week with the
requirement for generating a dynamically tracked and an ITV-based plan. Furthermore,
despite the Vero’s impressive mechanical versatility it is limited in terms of the types of
treatment it can deliver. It is a single energy machine (6MV) and despite a capable 0.5cm
leaf width projected at isocentre it can only manage a maximum field size of 15x15cm.
Back at the Elekta stand, there is much interest in the Versa HD. Yet despite faster leaf
speeds and flattening filter free modes the Versa HD is essentially the same linac we are
used to underneath newer, sleeker covers. Ironically, this is probably the machine’s greatest
advantage over fancier specialised systems like the Vero; it is able to deliver a wide variety
of treatment types from straight-forward breast parallel opposed pairs through complicated
VMAT plans (where faster leaf speeds should make the most impact) to highly conformal,
high-dose SBRT treatments. It is easy to see how such a machine will fit easily into a busy
radiotherapy centre’s existing workflow rather than commissioning the new techniques and

treatment types necessary to get the most out of a newer-design device for a smaller sub-
set of treatments.
If there is one thing I will take away from ESTRO as a mere Part 2 trainee (aside from the
pens, notepads, lanyards, brochures and breath-mints courtesy of Varian) it is the
realisation that the UK is perhaps not the frontier in terms of technological innovation. And
yet, that is not specifically a bad thing; the NHS has a huge and varied radiotherapy
workload that must be met with a limited budget and in such conditions, the most advanced
solution may not always be the best. I find this to be something of a theme at ESTRO this
year, which culminates with a final day debate entitled the house believes that technology is
the obsession but not the answer, which I am frustrated to miss due to travel arrangements.
With my knowledge/appreciation of radiotherapy suitably expanded and my certificate of
attendance secured (which I assume I need to wave about in frantic rain-dance like ritual to
attain some of those mysterious CPD points), what of my primary aim; to get my first poster
out to the radiotherapy community? After all, this was my personal aim of attending ESTRO,
a chance to practice being a working scientist with things to talk about and results to
disseminate! As self-important as it might sound, presenting my own work is a principal
benefit I’m personally expecting as a delegate in exchange for that lunch-less registration
fee.
Unfortunately, I’m in for some disappointment. After traversing the labyrinth of physical
poster displays I happen upon a row of desktop computers with little screen marked ‘e-
poster viewing stations’ (not quite my e-Hub vision of the future). Searching poster abstracts
returns lists of results but posters are displayed in low resolution and each section is
readable only as pop-out clickable fields. Transition animations between screens slow things
down a bit making review of several posters just that bit more time consuming. Individually,
these are small gripes but they make the e-poster experience a little too frustrating
compared with simply looking at and reading a physical counterpart. Worse still, it appears
that the idea of disseminating results is altogether hampered by ESTRO’s e-poster system.
For each e-poster, delegates have the option of e-mailing themselves or a colleague for
further reference. Following Tim Depuydt’s tumour tracking with Vero presentation I hit the
e-poster station to review some of the works he referenced. I identify six of interest and
click the ‘e-mail poster’ option for each one. Two months after the conference, I’m still
waiting for those e-mails. Something tells me they aren’t coming.
So was ESTRO 2013 ‘value for money’ for a Part 2 trainee like me? Certainly I didn’t feel I
achieved my aims of adequately presenting my work though the e-poster system. In that
respect I would think twice about attending a conference to present work in this format in
the future and that may be of concern to conference organisers. After all, when convincing
delegates to part with their registration fee cash they will need to consider all aspects that
delegates perceive as being of value and balance this against the savings they think they will
make by further limiting the amount of physical poster space. However, as an opportunity
to see the latest developments in radiotherapy technology and to learn about research

undertaken both within the UK and from around the world, ESTRO exceeds all of my
expectations. I am so interested in talking to exhibition stand representatives about their
new devices or fellow delegates eagerly standing next to their physical posters that I hardly
notice that I have missed that lunch I was supposed to buy for myself.