Embed Size (px)
Citation preview

SAZA.CLB.18.03.0126
Sponsored by
• NMOSD-beyondAquaporin-4antibodies
• RevisedMcDonaldsCriteria2017
• ThespectrumandmanagementofAutoimmuneEncephalitis
Autoimmune Issue
Volume11No2-Issue362018
NeurologyNewsletter
SAZA.CLB.18.03.0126
Sponsored by
• Thepragmaticuseofcurrentlyavailableimmunomodulationinpatientswithmyastheniagravis
• Neurocognitivetesting• StephenHawking:Amindapart
• Stroke&HypertensionCongress2018-Reportback
Autoimmune Issue
Volume11No3-Issue372018
NeurologyNewsletter
SAZA.GVPA.18.07.0509(1)

Choose Control. Choose Life.
Valproate derivatives should never be prescribed to female children, female adolescents, pregnant women and women of childbearing potential for any indication other than epilepsy which is not effectively controlled by other available medicines with less risk of toxicity to an unborn child, or if these other medicines with less risk of toxicity to an unborn child are not tolerated. Such patients and/or their relatives should be fully informed of the risks to unborn children. Summary:• Children exposed in utero to valproate are at a high risk of serious developmental disorders (in up to 30 - 40 %) and/or congenital malformations (in approximately 10 % of cases).
• Valproate should not be prescribed to female children, female adolescents and pregnant women or women of childbearing potential with epilepsy unless other treatments with a lower risk of causing congenital abnormalities or developmental defects are ineffective or not tolerated.
• Valproate treatment must be started and supervised by a doctor experienced in managing epilepsy or bipolar disorder.
Sodium valproateValproic acid
Reference: 1. Lösher W. and Schmidt D. Modern antiepileptic drug development has failed to deliver: Ways out of the current dilemma. Epilepsia 2011;52(4):657-678For full prescribing information refer to the package insert(s) approved by the medicines regulatory authority.S3 Epilizine® CR 200/300/500 (Tablets). COMPOSITION: Each CR tablet contains 133,2/199,8/333,0 mg sodium valproate and 58,0/87,0/145,0 mg valproic acid equivalent to 200/300/500 mg sodium valproate respectively. REGISTRATION NUMBERS: A39/2.5/0038; A39/2.5/0039; A39/2.5/0040. NAME AND BUSINESS ADDRESS OF THE HOLDER OF THE CERTIFICATE OF REGISTRATION: Zentiva South Africa (Pty) Ltd, a Sanofi company. Reg. no.: 1931/002901/07. Sanofi House, 2 Bond Street, Grand Central Ext. 1 Midrand 1685. Tel: (011) 256 3700. Fax: (011) 256 3707. www.zentiva.com.SAZA.GVAVA.17.03.0183
Recommendations
• Carefully balance the benefits of valproate treatment against the risks of congenital malformations and developmental abnormalities. This assessment should be made when prescribing valproate for the first time, at routine treatment reviews, when a female child reaches puberty and when a woman plans a pregnancy or becomes pregnant.
• You must ensure that all female patients are fully informed of and understand:
- the risks associated with valproate during pregnancy;
- the need to use effective contraception;
- the need for regular review of treatment;
- the need to rapidly consult her prescribing physician if she is planning a pregnancy or becomes pregnant.
In Epilepsy a wide unsurpassed spectrum1
1162
9
11629 Epilizine advert.indd 1 2017/04/20 10:53 AM

Page 3 NEURON SA Volume 11 No 3 Issue 37 2018This newsletter is proudly sponsored by
Editorial - the autoimmune issue
Editor:DrShaheedGoraNeurologist, Health Systems Consultant, Netcare Milpark Hospital, Johannesburg
NeurosurgeryDrChristosProfyrisBBiomedSciHon(Monash),MA(Cantab),BM,BCh(Oxon),MRCS,FCNeurosurg(SA),MMedNeurosurg(WITS)Head of Department, Neurosurgery, Helen Joseph Hospital, Netcare Milpark Hospital
NeurologyDrShaheedGoraMBBCh(Wits)FCNeurol(SA)ENLS(NeuroCriticalCareSociety)Neurologist, Health Systems ConsultantNetcare Milpark Hospital, Johannesburg
NeurologyandSleepDrRakshaSitharamMBChB,FCNeurol(SA)NeurologistNetcare Waterfall City Hospital, Midrand
PublicHealthNeurologyDrStaceyRossouwMBChB(SU),FC(Neurol)SA,AHMP(YALE)Specialist Neurologist, Frere Hospital, East London
eHealthExpertMsAmeeraHamidBHScHonsFS,PDM,MBAeHealth Strategist and InnovatorOperations Manager, African Centre for eHealth Excellence (Acfee)Systems analyst, Health Information Systems Program South Africa (HISP-SA)
Neurology,vascularneurologyandmedicalinnovationDrNaeemBreyMBChB(UCT),FCNeurol(SA),DipHIVMan.(SA)Neurologist, Neurology Division, Tygerberg Hospital Lecturer, Faculty of Medicine and Health Sciences Stellenbosch University
NeuroPsychiatryDrFransKorbBSc(Hons)(UFS),MAClinicalPsychology(Wits),MBChB(UCT),MMedPsychiatry(Wits)Psychiatrist and psychologist in private practice, Blairgowrie, Johannesburg
EditorialBoard
Choose Control. Choose Life.
Valproate derivatives should never be prescribed to female children, female adolescents, pregnant women and women of childbearing potential for any indication other than epilepsy which is not effectively controlled by other available medicines with less risk of toxicity to an unborn child, or if these other medicines with less risk of toxicity to an unborn child are not tolerated. Such patients and/or their relatives should be fully informed of the risks to unborn children. Summary:• Children exposed in utero to valproate are at a high risk of serious developmental disorders (in up to 30 - 40 %) and/or congenital malformations (in approximately 10 % of cases).
• Valproate should not be prescribed to female children, female adolescents and pregnant women or women of childbearing potential with epilepsy unless other treatments with a lower risk of causing congenital abnormalities or developmental defects are ineffective or not tolerated.
• Valproate treatment must be started and supervised by a doctor experienced in managing epilepsy or bipolar disorder.
Sodium valproateValproic acid
Reference: 1. Lösher W. and Schmidt D. Modern antiepileptic drug development has failed to deliver: Ways out of the current dilemma. Epilepsia 2011;52(4):657-678For full prescribing information refer to the package insert(s) approved by the medicines regulatory authority.S3 Epilizine® CR 200/300/500 (Tablets). COMPOSITION: Each CR tablet contains 133,2/199,8/333,0 mg sodium valproate and 58,0/87,0/145,0 mg valproic acid equivalent to 200/300/500 mg sodium valproate respectively. REGISTRATION NUMBERS: A39/2.5/0038; A39/2.5/0039; A39/2.5/0040. NAME AND BUSINESS ADDRESS OF THE HOLDER OF THE CERTIFICATE OF REGISTRATION: Zentiva South Africa (Pty) Ltd, a Sanofi company. Reg. no.: 1931/002901/07. Sanofi House, 2 Bond Street, Grand Central Ext. 1 Midrand 1685. Tel: (011) 256 3700. Fax: (011) 256 3707. www.zentiva.com.SAZA.GVAVA.17.03.0183
Recommendations
• Carefully balance the benefits of valproate treatment against the risks of congenital malformations and developmental abnormalities. This assessment should be made when prescribing valproate for the first time, at routine treatment reviews, when a female child reaches puberty and when a woman plans a pregnancy or becomes pregnant.
• You must ensure that all female patients are fully informed of and understand:
- the risks associated with valproate during pregnancy;
- the need to use effective contraception;
- the need for regular review of treatment;
- the need to rapidly consult her prescribing physician if she is planning a pregnancy or becomes pregnant.
In Epilepsy a wide unsurpassed spectrum1
1162
9
11629 Epilizine advert.indd 1 2017/04/20 10:53 AM
“Although I can move and have to speak through a computer, in my mind I am free.”
- Stephen Hawking
recently read a review of the popular BMJ journal Practical Neurology that referred to it as “a journal for jobbing neurologists who plough through the tension headaches and funny turns week in and week out.” This struck home for me. Inasmuch as the nervous system encompasses the most complex physiology
and a fascinating array of pathologies that range from the quietly obscure to the downright bizarre, we are clinicians first. Patients may initially delight in our descriptions of autoimmunity or the current migraine hypothesis, but will quickly hit you with “great doc, now how do we fix it?”. In this issue we stay true to some of these day-to-day practicalities in diagnosis and management.
Wrapping up the autoimmune theme from the previous issue is a pragmatic approach to immunomodulation in patients with myasthaenia gravis. Dr Melody Asukile and Prof Jeanine Heckmann, who are both actively changing the academic landscape for the disease in the South African context, provide a complete management plan that can be replicated in the rooms. We learn that the goal of therapy is MMS or minimal manifestation status as well as how we are able to achieve this utilising currently available therapies. The timing and use of immunomodulatory therapy is beautifully proposed in algorithm that gets your patient as close to MMS as possible. Treating the most common autoimmune disorder of the neuromuscular junction, even the brittle myasthaenic, will feel a lot less daunting.
Switching to opposite end of the neuraxis, the higher functions and testing thereof are often relegated to a brief screen of memory or the MMSE. Dr Christine Albertyn reviews neurocognitive testing with a focus on practical, context specific tests in each cognitive domain. She tackles the classification of memory and the various cognitive domains in a refreshing style that can be used by all types of clinician from the generalist registrar to the memory
specialist. The correlation of each domain to its specific bedside test is particularly valuable in the elucidation and monitoring of the ever expanding dementia syndromes.
We lost a neurological icon in March 2018. Stephen Hawking, the unassuming quantum physics genius was initially criticised for his ambivalence about his disease and disability eventually brought ALS and as a result the complexity of degenerative neurology to the forefront of public awareness. Millennial instagrammers outdid each other’s ice bucket challenges. Romcom movie buffs celebrated Eddie Redmayne’s captivating performance and best actor Oscar in “The theory of everything”. Big Bang Theory ‘Sheldonesque’ armchair physicists quoted “A brief history of time” at dinner parties. All the while, ALS served as a unique backdrop to this incredible life. Dr Matthew Snyman does a fitting tribute to the man, his tenacity and, importantly, the practical and technological management of disability that allowed him to contribute to our knowledge far beyond black holes and the big bang theory.
To wrap up, Dr Pearl Thomas gives us some practical feedback from the recent stroke and hypertension congress in Stellenbosch. She provides some concise highlights regarding the pulse in modern day practice, the future of stroke from an interventionalist perspective. The “salt controversy” and lack of benefit from salt restriction is particularly fascinating.
Stephen Hawking felt free and lived an extraordinary life that lasted 76 years despite the most profound neurological disability. Sometimes a practical, tenacious approach is where we add most value in clinical practice. Practising neurology will always be most fun when unravelling the particularly challenging clinical localisation and understanding the pathogenesis behind a sign like Babinski’s, but for those days when yet another tension headache needs treating, I hope this issue adds some joy.
Till next time Shaheed

Page 4NEURON SA Volume 11 No 3 Issue 37 2018
yasthenia gravis (MG) is an antibody mediated disease which most commonly targets the acetylcholine receptor (AChR), and rarely muscle-specific kinase (MuSK).1 MG treatment focuses on symptomatic and immune-
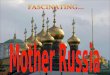
modulatory treatment. Due to its heterogeneous nature, there is currently no internationally accepted standard treatment regimen. Choice of treatment depends on disease severity and individual patient characteristics. The goal of therapy is to obtain minimal manifestation status (MMS) or better (asymptomatic off therapy).2 Figure 1 shows a proposed treatment algorithm.
SymptomatictreatmentAcetylcholinesterase (AChE) inhibitors prevent the breakdown of acetylcholine at the neuromuscular junction. Pyridostigmine bromide (Mestinon®) is the initial treatment used in MG and for some may be all that is required. Doses of 60mg every 4-8 hours are commonly used. Side effects include nausea, salivation, diarrhoea, abdominal and muscle cramps and fasciculation, which improve on reduced doses. They should be used cautiously in patients with severe bulbar dysfunction. MuSK-MG patients may respond poorly to AChE inhibitors.3
ImmunetherapiesMost MG patients will require immune therapy in addition to symptomatic therapy.
AcuteimmunetherapyAcute immune therapies induce rapid, albeit short-lived clinical improvement, which is useful in patients with severe MG symptoms.
PlasmaExchange (PLEX) removes and temporarily reduces the circulating pathogenic antibodies resulting in clinical improvement within days. Rebound clinical worsening will occur in 4-8 weeks if concomitant immunosuppressive treatment is not used.3 A total of 3-5 exchanges performed on alternate days typically comprise one course. PLEX may be more effective than intravenous immune globulin (IVIG) in MuSK-MG.4 Its use is limited by high cost and need for specialist services. Complications include thrombosis, infection, nausea and vomiting, bleeding tendencies, electrolyte imbalances and hypotension.
Intravenous immunoglobulin (IVIG) has multiple effects on the immune system including competition with antibodies and inhibition of pro-inflammatory processes.5 It has similar use and efficacy as PLEX but is easier to administer. The standard dosing regimen is 400mg/kg/day infusions for 5 days. In younger patients without co-morbid cardiac or renal disease, 1g/kg/day for 2 days can be administered safely. Clinical improvement may be noted within 5-14 days of treatment. Adverse effects include infusion-rate related headaches, chills, myalgia and chest discomfort. More serious rare complications include acute tubular necrosis, aseptic meningitis, deep vein thrombosis and pulmonary embolism. Anaphylactic reactions in patients with IgA deficiency are extremely rare.
MaintenanceimmunetherapyMaintenance therapies are used to sustain clinical improvement.
Corticosteroids (prednisone) are considered first line immune therapy in MG, particularly because they are cheap, rapidly acting and reliable.3 They result in immune-modulation by multiple effects on the immune system.
Corticosteroids are recommended in patients who remain symptomatic after initiating AChE inhibitors. Prednisone is most commonly initiated at a dose of 15-20mg daily and increased by 5mg every 2-7 days to a dose of 60 – 80mg or less if limited by side effects or if the symptoms resolve. Initiating prednisone at high doses has a small but real risk of aggravating weakness and is thus only recommended if the patient already requires ventilator support. Improvement is usually observed within 2 – 4 weeks, but may take longer. Treatment response varies substantially among individuals with some suggesting up to 30% of patients responding poorly.3
The ultimate goal is to use the lowest effective dose in order to limit the multiple steroid-related complications. Bone protection with calcium and vitamin D (+/- bisphosphonates) is required in most patients. Gastric ulcer prophylaxis is required in patients with a previous history of peptic ulcer disease or new symptoms of gastric irritation. Additionally, monitor for cataract, glaucoma, hyperglycaemia, hypokalaemia, and emotional and psychiatric effects.
Azathioprine (AZA) inhibits nucleic acid synthesis hence disrupting T-cell and B-cell proliferation. It is considered a first line steroid-sparing agent with evidence from two randomised controlled trials (RCTs).6,7 Improvement on azathioprine can take 9-15 months at a total daily dose of 2-3 mg/kg.1 Thus, one should be cautious in interpreting limited improvement in less than one year of use as lack of efficacy. Full blood count can be used to monitor efficacy and titrate treatment as a reduction in total white cell count (WCC) sometimes correlates with clinical effect. Important adverse effects are hepatotoxicity and leukopenia, warranting regular WCC and liver transaminase testing.3 Doses must be reduced if the WCC falls below 3x106 cells/L and stopped for levels below 1x106 cells/L. Liver transaminase levels must not increase by greater than two-times the upper limit of normal. Nausea can be remedied by twice daily dosing after meals.
Methotrexate(MTX) is an anti-metabolite thought to provide its immunosuppressive effect by inhibiting lymphocyte proliferation. A single blind study of 24 newly-diagnosed MG cases found that methotrexate was equivalent to azathioprine as a steroid-sparing agent, and showed efficacy after 9 months.8 However, a RCT in chronic MG patients refractory to steroids, did not show steroid-sparing activity within 1 year.9 It is commonly used due to its low cost, few side effects and ease of administration (weekly dosing). A starting dose of 10-12.5mg weekly can be escalated quickly to a dose of 15-25mg weekly (typically 17.5mg weekly), used in conjunction with folate 5-10mg weekly. Although uncommon, hepatotoxicity
The pragmatic use of currently available immu-nomodulation in patients with myasthenia gravisDrMelodyTAsukile,ProfJeannineMHeckmannDivision of Neurology, Department of Medicine, Groote Schuur Hospital and the University of Cape Town, Cape Town

Page 5 NEURON SA Volume 11 No 3 Issue 37 2018
and anaemia are serious side effects that should be monitored. It has significant teratogenicity and should be avoided in childbearing women.
Cyclosporine (CsA) is a calcineurin inhibitor and thus specifically inhibits T-cell activation. It has shown efficacy within 3-6 months. The recommended initiating dose is 4-6mg/kg/day in two divided doses, However, the effect may be sustained at lower doses.10 Compared to the other steroid-sparing agents, CsA shows quicker onset of action but may more frequently cause adverse effects. Nephrotoxicity and hypertension are the main adverse reactions and thus trough levels and creatinine levels must be monitored. Other side effects include hirsutism, anaemia, gum hyperplasia, headache and tremor.
Mycophenolate mofetil(MMF) selectively inhibits the proliferation of T and B-lymphocytes. Efficacy as a steroid-sparing agent in generalised MG has been suggested in small studies despite two failed RCTs over a 9 month period.11,12 MMF is given at a standard dose of 1g twice daily, which may be increased to 3g per day if no improvement within 9 months.3 Leukopenia is an important adverse effect that warrants WCC monitor-ing. Others include terato-genicity, carcinogenicity and severe infections, including progressive multifocal leu-koencephalopathy (PML). MMF has the advantage of being a “liver-friendly” drug.
Cyclophosphamide (CP) in-terferes with DNA structure, and is likely cytotoxic to lym-phocytes. Its particularly ef-fective in B-cell mediated diseases such as MG. Both oral and intravenous cyclophosphamide has been used in treatment-resistant MG although the side effect profile is reported to be more favourable with IV pulses.10 One RCT showed that pulsed doses of IV cyclophosphamide (500mg/m2) monthly for 6 months and then 2-monthly for 6 months was effective in previously treatment-refractory MG cases.13 Several re-ports, including our own experience, have found that a short
course of monthly pulses of cyclophosphamide (typically 750-1000mg IVI) either as rescue therapy or additional induc-tion therapy in severe refractory MG patients, can be highly effective and long lasting. Important adverse effects include diarrhoea, nausea, vomiting, alopecia and haemorrhagic cys-titis (monitor by checking urine one week post-infusion). It also has carcinogenic and teratogenic potential and may in-duce infertility.
Improves
Good response
Exacerbation
Good response
Moderate exacerbation
Loss of treatment effect
Severe exacerbation
Poor response
No
Yes
MG diagnosis confirmed
Patient stable?
Start pyridostigmine
Myasthenic crisis - Severe bulbar
dysfunction - Respiratory crisis
PLEX or IVIG + steroids
Start prednisone
Optimise and maintain at lowest
effective dose
Add steroid-sparing
agent
1st line: AZA, MTX, MMF.
2nd line: CsA, RTX*...
Rescue: PLEX, IVIG, CP
Poor response Adverse effects
Consider thymectomy if AChR ab +ve,
Age<65
Optimise dose and monitor
Optimise and maintain at lowest
effective dose
Switch if adequate time has elapsed
or intolerable side effects
Poor response Good response
MMS/ Remission
Positive
Negative
C
M
Y
CM
MY
CY
CMY
K
MG flowchart_14May2018.pdf 1 2018/09/04 10:22:28 AM
Figure1:Proposedalgorithmforthetreatmentofmyastheniagravis.AChRab(acetylcholinereceptorantibody),AZA(azathioprine),MTX(methotrexate),CsA(cyclosporine),MMF(mycophenolatemofetil),RTX (rituximab), CP (cyclophosphamide), PLEX (plasma exchange), IVIG (IV immunoglobulin), MMS(minimalmanifestationstatus).Aftermyastheniccrisis,patientshouldbeinitiatedonasteroid-sparingagentincombinationwithprednisone.*Rituximab2ndlineforMuSK-MG

Page 6NEURON SA Volume 11 No 3 Issue 37 2018
Tacrolimus is a calcineurin inhibitor that modulates T-cell activity. It is commonly used in Japan.14 One study in MG failed to show benefit. The recommended dose is 0.035mg/kg twice daily with a target trough level 6-9 ng/ml.3 The important adverse effect is nephrotoxicity and may exacerbate diabetes and hypertension. Other side effects include gastrointestinal discomfort, diarrhoea, tremor and paraesthesia.
Rituximab is a monoclonal antibody that targets CD-20 expressing B cells. It is used in treatment-resistant MG. Its efficacy in a RCT suggests it should be considered earlier in MuSK MG patients showing poor response to steroids and other immunosuppressants.1 Typical dosing consists of cycles administered every 6 months if clinically required. The dose of 375mg/m2 of body surface given once a week for 4 weeks was based on the “lymphoma-protocol”. There are increasing reports of efficacy with lower doses e.g. 500mg IVI repeated after 2 weeks as a single cycle, and even a single 600 - 1000mg dose showing clinical and immunological efficacy lasting for 6 months or longer.15 Pre-treatment with acetaminophen, diphenhydramine and corticosteroids is used to reduce infusion reactions. Severe infections, including PML, pneumocystis pneumonia and reactivation of latent Hepatitis B infection may occur.
Eculizumab is a monoclonal antibody directed against the C5 component of complement. It has recently been found to be effective for treatment-resistant AChR antibody-positive MG patients in a phase 3 trial.16 It is currently not available in South Africa, and at a cost of approximately $400,000 per year is among the most expensive drugs in use.
Immunetreatmentinspecificgroups
MGandPregnancyMG is common in women of childbearing age. The clinical course of MG in pregnancy is highly variable among individuals with equal probabilities of worsening, improving or staying the same. Mestinon and prednisone are safe. Despite lack of robust supporting evidence, PLEX and IVIG are considered safe. Azathioprine, cyclosporine and tacrolimus are also considered safe based on decades of experience in various autoimmune diseases. Methotrexate and MMF have significant teratogenic potential and are contraindicated in pregnancy.17
PaediatricMGTreatment considerations of MG patients under the age of 18 are more difficult and as in adults must be individualised. Corticosteroids are associated with growth retardation and osteoporosis in later life. Azathioprine and methotrexate have been used safely in younger children when steroid-sparing agents are required.
ConclusionMG is a treatable condition and if the patient does not respond to therapy it is important to consider the possibility of an alternative diagnosis and referral to a MG specialist.
References1. Gilhus NE, Verschuuren JJ. Myasthenia gravis: Subgroup
classification and therapeutic strategies. Lancet Neurol. 2015;14(10):1023–36.
2. Sanders DB, Wolfe GI, Benatar M, Evoli A, Gilhus NE, Illa I, et al. International consensus guidance for management of myasthenia gravis: Executive summary. Neurology. 2016;87(4):419–25.
3. Kaminski HJ. Treatment of Myasthenia Gravis. Myasthenia Gravis and Related Disorders. Cham: Springer International Publishing; 2018 p. 169–87.
4. Guptill JT, Sanders DB, Evoli A. Anti-musk antibody myasthenia gravis: Clinical findings and response to treatment in two large cohorts. Muscle Nerve. 2011 Jul;44(1):36–40.
5. Peter JG, Heckmann JM, Novitzky N. Recommendations for the use of immunoglobulin therapy for immunomodulation and antibody replacement. South African Med J. 2014;104(11):796.
6. Palace J, Newsom-Davis J, Lecky B. A randomized double-blind trial of prednisolone alone or with azathioprine in myasthenia gravis. Neurology. 1998 Jun 1;50(6):1778–83.
7. Heckmann J, LeePan E, Eastman R. High-dose immunosuppressive therapy in generalised myasthenia gravis - a 2-year follow-up study. South African Med J. 2001;(91):765–70.
8. Heckmann JM, Rawoot A, Bateman K, Renison R, Badri M. A single-blinded trial of methotrexate versus azathioprine as steroid-sparing agents in generalized myasthenia gravis. BMC Neurol. 2011 Dec 5;11(1):97.
9. Pasnoor M, He J, Herbelin L, Burns TM, Nations S, Bril V, et al. A randomized controlled trial of methotrexate for patients with generalized myasthenia gravis. Neurology. 2016 Jul 5;87(1):57–64.
10. Meriggioli MN, Sanders DB. Autoimmune myasthenia gravis: emerging clinical and biological heterogeneity. Lancet Neurol. 2009;8(5):475–90.
11. Muscle Study Group TMS. A trial of mycophenolate mofetil with prednisone as initial immunotherapy in myasthenia gravis. Neurology. 2008 Aug 5;71(6):394–9.
12. Sanders DB, Hart IK, Mantegazza R, Shukla SS, Siddiqi ZA, De Baets MH V, et al. An international, phase III, randomized trial of mycophenolate mofetil in myasthenia gravis. Neurology. 2008 Aug 5;71(6):400–6.
13. Gustavo De Feo L, Schottlender J, Martelli NA, Molfino NA. Use of intravenous pulsed cyclophosphamide in severe, generalized myasthenia gravis. Muscle Nerve. 2002 Jul 1;26(1):31–6.
14. Murai H. Japanese clinical guidelines for myasthenia gravis: Putting into practice. Clin Exp Neuroimmunol. 2015 Feb 1;6(1):21–31.
1. The goal of MG treatment is to render the patient free of symptoms
2. MG treatment frequently requires a combination of symptomatic and immune- modulatory therapies
3. Treatment must be individualised to the patient e.g. if the patient is potentially childbearing.
4. Immune-modulatory drugs are safe but do require regular monitoring
5. Consider referral to a specialist centre if the patient is not responding to treatment
TAKEHOME MESSAGE
References15-17availableonrequest.

Page 7 NEURON SA Volume 11 No 3 Issue 37 2018
he aim of this review is to give some structure to neurocognitive testing, while acknowledging the limitations of neuropsychological screening tests, particularly those developed in first world coun-tries. A flexible, patient-centred approach, with an
emphasis on the quality of performance rather than a test score, is reiterated.
History As with most neurological patients, there is great return on investing in a good history. In patients with cognitive complaints, the collateral history is particularly relevant to highlight cognitive and behavioural features. When taking the history, questioning can be constructed around domain abilities:• Attention and concentration: Ability to read newspaper,
follow a TV progamme• Memory: Recent activities and experiences (family news,
sporting events), as well as more remote events such as wedding day.
• Language: Word errors, halting speech, understanding, reading and writing.
• Numericalskills: Working with money, paying bills. • Executive function: Ability to plan, organise, solve
problems, be flexible. • Visuospatialfunctionandneglect:Route finding, landmark
recognition, dressing, visual hallucinations. • Personality and social conduct: Mood, motivation/apa-
thy, anxiety, eating habits, delusions, hallucinations, rituals, obsessive-compulsive behaviour.
• Activitiesofdailyliving: Basic activities such as dressing, feeding, and hygiene, but also instrumental activities such as the use of a cellphone, microwave, and managing medication.
NeurocognitiveexaminationAn approach suggested by behavioural neurologist, John Hodges, is to assess distributed functions before localised functions.1 Distributed functions are those systems or networks that are usually not affected by single discreet lesions, but rather imply extensive or bilateral involvement, or toxic/metabolic causes (such as delirium). The widely distributed functions include attention and concentration, memory, and executive function. In contrast, localised functions are typically lateralised to either dominant or non-dominant hemispheres and have domain-specific functions. For the dominant hemisphere, these include language, praxis and calculation. For the non-dominant hemisphere, functions include spatially directed attention, visuo-perceptive skills, constructional ability, prosody of language, and emotional processing. The biggest advantage of assessing the distributed functions first is that it identifies, early on, the patient with
Neurocognitive testing
DrChristineAlbertynConsultant Neurologist, Division of Neurology, Faculty of Medicine and Health Sciences, Tygerberg Hospital and Stellenbosch University, Cape Town
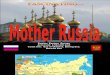
Figure1:Classificationoflong-termmemoryanditsanatomicalsubstrate
significant inattention and poor concentration, which is a major confound of performance in subsequent domains.
Orientationandattention/concentrationThis distributed function consists of bottom-up (ascending reticular activating system) and top-down (multimodal association areas in the prefrontal and parietal lobes with right bias) components. The elements of attention include arousal, vigilance, divided attention, and selective attention. Because routine tests of attention also rely on working memory, it is included here. Working memory (also called short-term memory in neuropsychological literature) is part of our larger attentional system, and relates to the ability to hold on to bits of new information for brief periods of time; typically a few seconds; in order to complete a task.2 Examples include repeating a phone number in one’s head until you can write it down, or mentally following a route.
Testing of attention and concentration include:• Orientation to time and place (also dependent on episodic
memory) • Days of week or months of the year forward and in reverse• Digit span forward (range 6 ± 1) and backward (range 5 ± 1)• Serial subtraction of 7s from 70 or 3s from 20
MemoryMemory can be divided into short- and long-term memory, and as mentioned before, short-term (working) memory is largely under control of the dorsolateral prefrontal cortex (DLPFC) and works independently of, but in parallel with, longer-term memory .1
Long-term memory can be further subdivided as shown in Figure1.

Page 8NEURON SA Volume 11 No 3 Issue 37 2018
Although the most common complaint in cognitive disorder clinics is forgetfulness,3 it is not specific for an amnestic disorder. An amnestic disorder is one where memory and learning are affected disproportionately to other cognitive functions,4 and where working memory and implicit memory are preserved. A distinction is made between anterograde amnesia (impaired acquisition of new information) and retrograde amnesia (the recall of past events). There is a temporal gradient of memory loss, also known as Ribot’s law, which states that recent memories are more vulnerable to decay than more remote memories.5 Memory is executed by the extended limbic system (Papez circuit), with crucial structures including the medial temporal lobes (particularly the hippocampus), diencephalon (mamillary bodies and antero-dorsomedial thalami), and basal forebrain nuclei.
Three main types of amnestic syndromes are recognised: Hip-pocampal, diencephalic (including the basal forebrain), and frontal lobe types. Hippocampal amnesia is characterised by anterograde amnesia with limited retrograde amnesia. These patients perform poorly on tests of word list or story recall and do not typically ben-efit from cues or prompts. In other words, both recall and recognition memory is impaired. Causes include herpes simplex virus encephalitis, limbic encephalitis, or anoxia leading to hippocampal damage. In Alzheimer’s disease, the mechanism of memory loss is more complex, and al-though there is always anterograde amne-sia, retrograde extension does also occur.
Diencephalic (including basal forebrain circuitry) amnesia is characterised by both anterograde and more extensive retrograde amnesia. In this syndrome, the temporal order of events is also deranged (achronogenesis) and patients mistake when they learnt various things. A more florid form of these “false memories” manifest when patients relate the occur-rence of things that did not happen to them, i.e. confabulate. Diencephalic am-nesia is best exemplified by medial tha-lamic and mammillary body involvement in Korsakoff’s syndrome. Other causes include anterior communicating artery aneurysm rupture and third ventricle tu-mours.
Patients with frontal lobe pathology (DLPFC in particular) frequently complain of forgetfulness. Although not part of the Papez circuit, the prefrontal lobes play a part in encoding new information, and also in retrieving these details. The analogy of the prefrontal lobe as the conductor of the memory orchestra has been used: all the members of the orchestra may be present, but without the conductor there is chaos.1 This disorganised encoding and retrieval process helps one understand why these patients perform poorly on spontaneous recall of stories or word lists, but benefit from prompts, cues, or recognition-based memory tests.
Table1:Executivefunctionsubdomainsandexamplesoftesting
Executivefunctionsubdomain
Tests
Initiationandgenerativity• Letter fluency (F,A,S for English; S,B,K for Afrikaans,
not validated for isiXhosa) • Category fluency (animals, fruit & veg)
Abstraction• Similarities (arm and leg, apple and orange)• Proverb interpretation
Problemsolving• “18 books problem”1 or “chickens and dog
problem”2
Responseinhibition• Draw alternating sequences (squares and
triangles) or loops• Go-no-go test3
Setshifting• Trail making test B • Oral alternation test4
• Stroop test
Motorsequencing• Luria three-step test5 or alternating hand
movement6
1”Therewereeighteenbooksontwoshelves,buttheywerenotequallydivided:Therewere twiceasmanybookson theoneshelfason theother.Howmanybookswerethereoneachshelf?”2”Youhavetwochickensandonedog.Howmanylegsaretherealtogether?”3”TaponcewhenItaponce,donottapifItaptwice”4Alternatebetweenlettersofalphabetandnumbersverbally(i.e.1A,2B,3C,etc.)5Fist,edge,palmsequence6Outstretchedarms:Alternatebetweenonehandwithextendedfingersandtheotherwithclenchedfist
Practicalpointstorememberwhentestingfrontallobefunctions
• Executivefunctioningisparticularlysensitivetoconfoundssuchaspain,lackofsleep,medicationeffects,andmooddisorders
• Thequalityoftheperformance(impulsivity,perseveration,impersistence,inappropriateness)isoftenmoreimportantthantheactualtestscore
• Collateralhistoryiscrucialtoidentifybehaviouralchanges• Evenmildimpairmentofexecutivefunctioningontestingcanhavesignificantconsequencesforfunctioningindailylife.
Anterograde verbal episodic memory can be tested by recall of five (culturally familiar) words; with the use of prompts or cues if incorrect; or by recall of a story (South African versions include the Township fire story or the Knysna flood story). Anterograde visual memory can be tested by recall of shapes or the Rey-Osterrieth Complex Figure. When we ask a patient to remember a story or word list in the clinic, we are therefore testing anterograde, verbal, explicit, long-term memory! Retrograde memory is assessed by enquiring about autobiographical memories (wedding day, schooling) and famous events (sporting events, national elections, etc.)
FrontallobecognitivefunctionsThe diverse abilities of the frontal lobes can be dichotomised as follows:• Executiveabilities: How to plan, organise, and successfully
execute actions that are adaptive, goal-directed and future-oriented6
• Behavioural modulation: Inhibitory control, emotion and social cognition.

Page 9 NEURON SA Volume 11 No 3 Issue 37 2018
The frontal-subcortical circuitry as it relates to behaviour, as described by Cummings,7 identifies three circuits with connectivity to the prefrontal cortex: • DLPFC: Plays a role in executive cognitive functions and
pathology leads to a dysexecutive clinical syndrome • Orbital frontal: Responsible for behavioural responses to
limbic and emotional information and pathology leads to disinhibition and impulsivity
• Mesial frontal (anteriorcingulategyrus): Supports drive, initiation and motivation; when this region is affected it leads to apathy (in severe cases an akinetic-mute state)
In individual patients, these syndromes are rarely as neatly defined, and bedside tests of frontal lobe function are quite crude. Furthermore, it is not easy to isolate each frontal lobe subdomain, as one test often taps into multiple abilities simultaneously. Frontal lobe executive functions and its tests are shown in Table1.
An interesting and expanding field is social cognition and emotion processing, which encompasses abilities such as empathy, perceiving the emotional state of others, theory of mind (the ability to put oneself in another’s shoes), and grasping the nuances of social interaction. Unfortunately tests of these abilities often lack ecological validity, meaning that it does not accurately correlate with behaviour in the real world.
LanguageA detailed discussion of the assessment of aphasia is beyond the scope of this article, but the building blocks needed to classify the aphasic syndromes are: fluency, comprehension, repetition, and naming. Reading and writing should also be tested.
FluencyFluency reliably localises the deficit as either posterior (fluent) or anterior (non-fluent) to the Sylvian fissure. The terms expressive or receptive aphasia may be misleading as all aphasic patients have difficulty with language expression to some extent. To make a judgement about fluency, listen to the patient’s spontaneous speech during conversation or let them to tell you about work or family; and ask them to describe a picture.
Non-fluent speech is halting, laborious, and agrammatic (or at its most severe, telegraphic). Sentences lack proper syntax and prepositions, and are filled with nouns and function words. Patients are frustrated by their word-finding difficulty and commonly have associated articulation difficulty.
Fluent speech, in contrast, is produced at a normal rate with normal phrase length and syntax, but with phonemic (i.e. calling a pencil a fencil) and more frequently semantic (i.e. orange for apple) paraphasic errors. The speech may be empty of content and patients often seem unaware of the errors they are making.
ComprehensionThis is best assessed in a graded manner by starting with simple commands, which are then increased in complexity. To test single word comprehension, ask the patient to point to objects in the room (or especially laid out on the table). For sentence comprehension, one can start by asking the patient to put the pen on top of the paper. Sentences with more demanding syntax can then be used: “Pick up the cell phone, after putting the pen on the paper”. One could also ask: ‘‘If the lion ate the tiger, who remained?’’.
RepetitionAsk the patient to repeat increasingly complex sentences. An example frequently used is “The orchestra played and the audience applauded”, but the sentence should be adapted to the patient’s culture and language. If repetition is impaired, the perisylvian language areas (Broca’s area and the insula anteriorly, and Wernicke’s area posteriorly, together with the arcuate fasciculus connecting these regions) are affected. If repetition is preserved compared with spontaneous speech, the lesion is located cortically or subcortically outside these primary language areas, and is termed a transcortical aphasia (which can then further be divided into motor and sensory subtypes).
NamingThe ability to name objects is universally impaired in aphasic patients, albeit to different degrees, and therefore does not distinguish between the aphasia subtypes. It is, however, a useful measure of overall severity. Start by testing naming of high-frequency objects such as a door and hand, followed by low-frequency objects such as a hinge and knuckle. Using a magazine with pictures for naming can be useful.
PraxisThis can be tested when apraxia is suspected from the history or neurological examination. One can ask the patient to do the following:• Imitate meaningful gestures (such as a hitch-hiking sign or
salute)• Perform meaningful gestures to command• Imitate meaningless gestures (such as non-symbolic hand
positions)• Demonstrate the use of imagined objects (comb your hair,
brush your teeth, carve a loaf of bread). Patients often use a body part as the tool, such as a finger for a toothbrush, and this finding in isolation is not necessarily pathologic.
• Perform orobuccal movements (blow out a candle, stick out your tongue, lick your lips).
NeglectNeglect can be subdivided into:• Personal neglect, where there is denial of the deficit (anosa-
gnosia) or an unconcern about the deficit (anosodiaphoria)• Sensory neglect: for visual, auditory or tactile modalities, is
present when the patient appears to ignore stimuli on the affected side (typically the left) and sensory extinction is found to bilateral simultaneous stimulation
• Extrapersonal neglect is demonstrated on copies of sym-metrical drawings, line bisection tests, and clock drawing tasks, where the left side of the drawing is ignored, distort-ed or minimised
DressingandconstructionalapraxiaVisuospatial difficulty may manifest as difficulty with dressing and construction. Confusingly, they are termed apraxias, but are best considered visuospatial deficits, rather than motor impairments. One can ask a patient to put on a shirt that has been turned inside-out. For constructional ability, copying of 2D (intersecting hexagons) and 3D (wire cube) shapes are easy bedside tests. A more stringent task would be a copy of the Rey-Osterrieth Complex Figure.
VisuoperceptualabilitiesandtheagnosiasDeficits in object and face recognition may be missed from the history, because the patients themselves find it difficult to describe their impairment, and may complain of

Page 10NEURON SA Volume 11 No 3 Issue 37 2018
“blurry vision” or “forgetting names of people”. If a patient is unable to recognise an object despite intact vision and language, visual agnosia should be suspected. Two types are described:
ApperceptivevisualagnosiaThere is a breakdown at the stage of perceptual analysis and the patient cannot identify a visually presented object. These patients struggle to copy a drawing. However, they are able to name objects to description, or by touch, indicating a preserved underlying semantic representation of the object. As an example, a patient cannot identify a banana when shown it, and cannot copy a drawing of it, but can tell you what a banana is and will identify it by touch and smell. This phenomenon is the result of widespread, bilateral occipitotemporal pathology.
AssociativevisualagnosiaIn this setting, the perceptual stages of object recognition are intact, but patients cannot make sense of the visual information. The deficit reflects a disruption of stored semantic knowledge, and involves all modalities accessing this information. These patients can therefore copy a drawing of a banana, despite not recognising it. Touching or smelling the banana will not aid identification. The lesion is usually in the anterior left temporal lobe.
ProsopagnosiaThis is the inability to recognise familiar faces, and people are identified through other clues, such as gait, voice or hairstyle. Patients retain semantic knowledge associated with a particular person and can describe attributes of a given face (i.e. “Tell me what Paul’s face looks like”). The lesion is usually in the occipitotemporal lesion and may be an acquired or developmental finding.
ScreeningtestsThe most commonly used cognitive screening test is Folstein’s Mini-mental state examination (MMSE), which became subject to copyright in 2001.8 Its usefulness lies in decades of experience in both developed and developing countries, and by giving clinicians a common language when describing mild, moderate or severe dementia. The major limitations of the MMSE are its weighting on orientation and memory; while being insensitive to language impairment; and does not assess executive functions.9 It is confounded by language, levels of literacy, and culture,10 and in smaller studies in South Africa has been found to have moderate accuracy only.11
A systematic review and meta-analysis of the diagnostic performance of cognitive tests for the detection of dementia12
found that the most commonly used test was the MMSE, with other frequently employed tests including the Mini-Cog test (a five-minute test consisting of a word recall and clock drawing task), the Addenbrooke’s Cognitive Assessment-Revised (ACE-R), and the Montreal Cognitive Assessment (MoCA). The Mini-Cog test and the ACE-R are the best alternative screening tests for dementia, while the MoCA is the best alternative for mild cognitive impairment. All three these tests have comparable diagnostic performance against the MMSE, are freely available, and easy to perform. Unfortunately, these tests have not been validated on any large scale in South Africa.
A study of the utility of the MoCA to screen for HIV-associated neurocognitive disorder (HAND) in South Africa highlighted the challenges of using the MoCA.13 In healthy controls, significant floor effects (majority of participants obtaining low scores) were observed on cube drawing, rhinoceros naming, serial 7s, and one
abstraction item. Additionally, for Xhosa-speaking participants, the letter (F) fluency task was substituted with a category (animals) fluency task, while the sentence repetition task was dropped as it was deemed too complex. These findings are an indication that the normative data from the North-American MoCA samples is inappropriate for our population and may lead to misclassification of healthy individuals as impaired.
Therefore, one should remain cognisant of the potential pitfalls of screening tests that are not adapted to local culture, education and language, and for which good local normative data is not available. Large-scale efforts to adapt, validate and norm internationally validated tests should be strongly encouraged.
ConclusionA good history from the patient and informant, together with a directed neurological examination, allow one to generate a hypothesis regarding the patient’s most likely cognitive deficit/syndrome. The hypothesis can then be tested at the bedside in a qualitative, flexible, manner and can be a rewarding process for both clinician and patient.
References1. Hodges JR. Cognitive assessment for clinicians. Third ed.
Oxford, United Kingdom: Oxford University Press; 2018 2018.
2. Baddeley A. The episodic buffer: a new component of working memory? Trends Cogn Sci. 2000;4(11):417-23.
3. Kipps C, Hodges J. Cognitive assessment for clinicians. J Neurol Neurosurg Psychiatry. 2005;76(Suppl 1):i22-30.
4. Kopelman MD. Disorders of memory. Brain. 2002;125(Pt 10):2152-90.
5. Piolino P. Autobiographical memory in aging. Psychol Neuropsychiatr Vieil. 2005;1(1):25-35.
6. Suchy Y. Executive Functioning: Overview, assessment, and research Issues for non-neuropsychologists. Ann Behav Med.2009(37):106-16.
7. Cummings JL. Frontal-subcortical circuits and human behavior. Arch Neurol. 1993;50(8):873-80.
8. Newman JC. Copyright and Bedside Cognitive Testing: Why We Need Alternatives to the Mini-Mental State Examination. JAMA internal medicine. 2015;175(9):1459-60.
9. Devenney E, Hodges JR. The Mini-Mental State Examination: pitfalls and limitations. Pract Neurol. 2016;17(1):79-80.
10. Scazufca M, Almeida OP, Vallada HP, Tasse WA, Menezes PR. Limitations of the Mini-Mental State Examination for screening dementia in a community with low socioeconomic status: results from the Sao Paulo Ageing & Health Study. Eur Arch Psychiatry Clin Neurosci. 2008;259(1):8-15.
11. Ramlall S, Chipps J, Bhigjee AI, Pillay BJ. The sensitivity and specificity of subjective memory complaints and the subjective memory rating scale, deterioration cognitive observee, mini-mental state examination, six-item screener and clock drawing test in dementia screening. Dement Geriatr Cogn Disord. 2013;36(1-2):119-35.
12. Tsoi KK, Chan JY, Hirai HW, Wong SY, Kwok TC. Cognitive Tests to Detect Dementia: A Systematic Review and Meta-analysis. JAMA internal medicine. 2015;175(9):1450-8.
13. Robbins RN, Joska JA, Thomas KG, Stein DJ, Linda T, Mellins CA, et al. Exploring the utility of the Montreal Cognitive Assessment to detect HIV-associated neurocognitive disorder: the challenge and need for culturally valid screening tests in South Africa. Clin Neuropsychol. 2013;27(3):437-54.

Page 11 NEURON SA Volume 11 No 3 Issue 37 2018
“The doctorwho diagnosedmewithALS,ormotorneurondisease,toldmethat it would kill me in two or threeyears.”
-StephenHawking
ur knowledge on black holes, time and cosmology would never be where it is today without the great mind of Stephen Hawking. But his gift of scientific knowledge and understanding are eclipsed by his tenacity, resilience and positivity, demonstrating
to mankind exactly what can be overcome and conquered with the human mind and spirit alone.
Stephen Hawking was diagnosed with early onset motor neuron disease (amyotrophic lateral sclerosis/ALS) shortly after his 21st birthday. At the time, he was completing his final year of his doctorate at Oxford, and noticed an increase in clumsiness, difficulties with sport and mildly slurred speech. Although far outliving the limits set in his first diagnosis, Hawking experienced relentless, ongoing, debilitating deterioration, and within 7 years, had lost the ability to write.
As would become a theme in Hawking’s battle with ALS, he developed an incredible technique to overcome the difficulty of not being able to write. He started seeing and depicting complex mathematical equations in terms of geometry instead. As he had always maintained: the prospect of an early death urged him onward through numerous intellectual breakthroughs.
Hawking’s tenacity and habit for overcoming the problems his disability presented, was not all based on a positive outlook and great motivation. As are all things in real life, there was a darker side.
Hawking became incredibly depressed after his diagnosis, and initially had difficulty accepting his declining health, as evidence by his stubbornness to use a wheelchair when it became a necessity. It must be said, that once he was in the wheelchair, he became known as a fiercely reckless and aggressive driver, propagating his pre-disability reputation of being a daredevil.
Hawking also came into much criticism over his ambivalence to be being an ambassador for his disease and disability, often trying, instead, to distance himself from both.
This was, however, temporary, with Stephen Hawking becoming taking up the mantle in later years, as a celebrated
Stephen Hawking: A mind apart
DrMatthewSnymanMBBCh,BSc(Hons)Elixir Ideas (Owner)
StephenHawkingbeingpresentedbyhisdaughterLucyHawkingatthelecturehegaveforNASA’s50thanniversary.

Page 12NEURON SA Volume 11 No 3 Issue 37 2018
champion for ALS and disabled rights in general. Hawking even volunteered himself for the ‘ice-bucket challenge’, which had become a social media phenomenon. As made clear by his treating physicians, having a bucket of ice water dumped over your head is probably a bad idea if you currently have pneumonia, so luckily he let his children do the challenge on his behalf.
Stephen Hawking’s ability to overcome the limitations of his illness was also made possible by advancements in science and technology, often with the advice and ideas of physicist himself.
At the time of his death, his wheelchair and speech interpretation technology were a far cry from their humble beginnings, where he would raise his eyebrows to choose letter on a spelling card.
Hawking first encountered the technology is its recognisable form in 1986, as a computer program called ‘Equalizer’, which the creator had designed for his mother-in-law, who also suffered from ALS.
Once a small, wheel-chair based computer was developed to house the program, Stephen would use his hand to input language, which was then translated to computer-generated speech (albeit in an American accent). Hawking would continue to use this method for the majority of his life. It is also of interest that Hawking started to identify so strongly with this voice that he refused to change it or update it to more advanced versions once they became available
The hand-controlled text input had to be changed in 2005 when Hawking lost the use of his hand, amazingly, to be controlled by the movement of his cheek muscles.
With further deterioration of his muscle-control, and at the risk of developing locked-in syndrome, Hawking collaborated with software giant Intel to modify the software to receive inputs directly from Hawking’s brain waves and combinations of fine facial expressions. This, together with Swiftkey, a piece of software most of us use for typing text messages, enabled Hawking to communicate successfully until his death in March 2018.
Another interesting component to Steven Hawking’s story is the one of his disease state and his unique presentation. The initial prognosis was obviously blatantly incorrect, with his life expectation, initially estimated at 2-3 years, the physicist only passed away at the age of 76, 53 years later than expected.
There have been many theories as to the factor contributing to his slower-than-normal decline:
The fact that Hawking contracted the disease so early is thought to have contributed to the slow progression seen in his case. In patients first diagnosed over 50 years of age, we see a much more rapid decline, and the average age of diagnosis is 55. The ALS association says that the average life expectancy of an ALS sufferer is 14 months from the time of diagnosis, although this can vary enormously. 50 percent of patients make it past 3 years, 20 percent make it past 5 years and less than five percent make it past 20. Why an earlier onset improves progression is still not understood.
This further emphasises the uniqueness of Hawking’s presentation, having survived 45 years with the disease with
a nearly unheard of stabilization of progression. As Prof Nigel Leigh, professor of clinical neurology at King’s College in London told the BMJ: “I am not aware of anyone else who has survived with [ALS] this long”. The exceptional case of Stephen Hawking has been used as an example of the vastly different ways that ALS can affect its victims.
Prof Leo McCluckey, associate professor of neurology and medical director of the ALS Centre at the University of Pennsylvania, commented on the possible reason behind the slow progression of the disease in Hawking’s case: When asked whether he would attribute his longevity being due to the biology of Hawking’s particular form of ALS or rather any excellent care he has received, McCluckey stated that Hawking’s longevity could be a combination of both, although the fact that his diaphragm and oesophagus had remained unaffected, it was most likely due, solely, to the biology of his disease, illustrating once again the myriad ways the disease can manifest.
Science, medicine and cosmology aside, Stephen Hawking is a role model for anyone struggling with a disability, or any setback for that matter. He is a shining example of what is possible when someone has the right tenacity, motivation and stubbornness not to give in. And in Hawking’s case, a naughty sense of humour didn’t hurt either.
"I have noticed that even people who claim everything is predetermined and that we can do nothing to change it, look before they cross the road."Stephen Hawking
References:1. McCoy T. How Stephen Hawking, diagnosed with ALS decades
ago, is still alive [Internet]. Washington Post. 2015 [cited 15 July 2018]. Available from: https://www.washingtonpost.com/news/morning-mix/wp/2015/02/24/how-stephen-hawking-survived-longer-than-possibly-any-other-als-patient/?noredirect=on&utm_term=.e496bd8d8eb5
2. Dobson R. An exceptional man. BMJ [Internet]. 2002 [cited 15 July 2018];324(7352):1478-1478. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1123440/
3. CHENG M. Stephen Hawking at 70: How has he survived so long? [Internet]. msnbc.com. 2012 [cited 14 July 2018]. Available from: http://www.nbcnews.com/id/45886738/ns/health-aging/t/stephen-hawking-how-has-he-survived-so-long/#.W1A5ptUza72
4. Harmon K. How Has Stephen Hawking Lived Past 70 with ALS? [Internet]. Scientific American. 2018 [cited 15 July 2018]. Available from: https://www.scientificamerican.com/article/stephen-hawking-als/
5. Rossman S. USA Today [Internet]. Usatoday.com. 2018 [cited 14 July 2018]. Available from: https://www.usatoday.com/story/news/nation-now/2018/03/14/how-did-stephen-hawking-live-so-long-als/423313002/
6. Ducharme J. http://time.com [Internet]. Time. 2018 [cited 14 July 2018]. Available from: http://time.com/5199001/stephen-hawking-als/
7. Ferguson K. Stephen hawking. New York: St. Martin’s Press; 2014.8. Medeiros J, Hempel J, Tiku N, Lapowsky I, Finley K. How Intel
Gave Stephen Hawking a Voice [Internet]. WIRED. 2018 [cited 14 July 2018]. Available from: https://www.wired.com/2015/01/intel-gave-stephen-hawking-voice/
9. White M, Gribbin J. Stephen Hawking. London: National Academies Press;.
10. Ferguson K. Stephen hawking. New York: St. Martin’s Press; 2014.11. Larsen K. Stephen Hawking. Westport, Conn.: Greenwood Press;
2005.

Page 13 NEURON SA Volume 11 No 3 Issue 37 2018
Stroke & Hypertension Congress 2018 - Reportback
DrPearlThomasSpecialist Neurologist, Melomed Tokai Private Hospital, Tokai, Cape Town
he Stellenbosch mountains provided a serene backdrop to the 3rd Biennial Congress of the South-ern African Hypertension Society and the South Af-rican Stroke Society, which was held from 3-5 Au-gust 2018 at the Protea Hotel. The content of the
meeting was, however, far from placid.
Arguably, the highlight of the meeting was the exposition of a new biomarker for cardiovascular risk assessment which can be measured in the office using a specialised device, and the celebration of the tenacity and triumphs of the champions of emergent stroke care in our resource limited environment.
International speakers included Professor Atte Meretoja(Finland), ProfessorJanStaessen (Leuven, Belgium) and DrRayTownsend (USA).
ProfessorMeretoja dubs himself a “frontline neurologist” and has successfully implemented highly successful acute stroke services in both Helsinki and Melbourne.
Professor Staessen is a career researcher and giant in the field hypertension and cardiovascular disease.
ProfessorTownsend is a nephrologist who conducts research into the role of arterial stiffness in outcomes such as death and kidney failure progression, especially among patients with chronic kidney disease.
ThepulseinmoderndaypracticeThe bedside palpation of the pulse is a practice as old as allopathic medicine. Fast forward a few millennia - the pulse is still as important, but a finger will no longer suffice. ProfNorton journeyed us through the indices of aortic stiffness (notably, aortic pulse wave velocity) and the reflected waves observed in the arteriolar system. While arterial stiffness and its measure, pulse wave velocity, is a well-recognised marker
of cardiovascular morbidity independent of the effect of hypertension, of interest is new research that suggests backward reflected wave pressures are independently and strongly correlated with cardiovascular risk biomarkers such as left ventricular mass. This is an exciting frontier in cardiovascular research as alterations in the backward reflected wave pressures can be observed in the young adult, decades before the onset of aortic stiffness.
Furthermore, adequately treat-ed hypertension does not alter aortic stiffness or backward wave dynamics – suggesting
these may be therapeutic targets for the future. For now, these markers can be measured and employed as risk assessment tools with the use non-invasive, office-based equipment that require minimal training for operation.
OfficeBPversus homeBPmonitoring: Pros andConsHypertension remains the leading risk factor for cardiovascu-lar morbidity across all ethnicities and ages. ProfStaessen un-packed the complexity of the accurate diagnosis of hyperten-sion. Although ambulatory blood pressure recording remains the gold standard for the diagnosis of hypertension, it is quite clear that automated home blood pressure measurement is superior to office blood pressure measurement to classify pa-tients as hypertensive or not. For patients with target organ disease and normal office blood pressure readings, further in-vestigation with automated home-based and/or ambulatory blood pressure recording is warranted, to detect cases of noc-turnal and masked hypertension.
PhysiologicaltreatmentofresistanthypertensioninAfricaOn day 2, ProfRaynerpointed out the issues with adopting the SPRINT trial’s blood pressure targets in South Africa. As cardiovascular mortality risk doubles with each 20/10 mmHg increment in systolic/diastolic blood pressure, the additional benefit of lowering blood pressure below 140/90 is small and may be quickly offset by adverse effects such as dizziness and syncope. South Africa, like the rest of the African continent, has a large population of undetected hypertensives as well as suboptimal control in known hypertensives compared to the US or European countries. From a public health perspective, in our setting resources are best vested in achieving existing targets. He summarised this poignantly by stating that, “we must walk before we can sprint”. In his talk on “Physiological treatment of resistant hypertension in South Africa”, he makes

Page 14NEURON SA Volume 11 No 3 Issue 37 2018
Production Editor: Ann Lake Publications - Ann Lake, Helen Gonçalves Design: Jane Gouveia Sponsors: SanofiEnquiries: Ann Lake Publications, PO Box 265, Gallo Manor, 2052 Fax: 086 671 9397 Email: [email protected]
DisclaimerThe content contained in this publication contains medical or health sciences information and is intended for professional use within the medical field. No suggested test or procedure should be carried out unless, in the reader’s judgement, its risk is justified. Because of rapid advances in the medical sciences, we recommend that the independent verification of diagnoses and drug dosages should be made. Discussions views, and recommendations as to medical procedures, products, choice of drugs, and drug dosages are the views of the authors. The views expressed by the editor or authors in this newsletter do not necessarily reflect those of the sponsors or publishers. The sponsors, publishers and editor will not be liable for any damages or injuries of any kind arising from the use or misuse of information provided in this publication and do not support the use of products for off label indications.
a cogent case for why treatment refractory hypertension in Africa is probably best treated with Amiloride rather than Spironolactone. To date, however, Amiloride is not registered as a single-agent drug in South Africa and he bemoaned the deafness of bureaucratic ears.
Thesaltcontroversy:Howlowshouldwego?On the final day, Prof Staessen presented data generated across a career spanning his lifetime to show that restricting daily salt intake to <1.5g even in high risk populations does not lead to risk reduction and may even lead to harm, by virtue of the activation of the RAAS and lipid alterations. He urged listeners to heed his words with not just a pinch of salt, but up to 6 grams of it.
ThedaysofstrokenihilismarenumberedOver the course all three days, several speakers including ProfFerozaMotara, DrStaceyRossouw, ProfAlanBryer, ProfMeretoja and DrWillemStassen spoke about the structural organisations and service adaptions required to miminise door-to-needle time for intravenous thrombolysis in the management of acute stroke.
DrMarkAbelson, a specialist cardiologist in private practice in the Western Cape, shared his journey as a pioneering interventionist during the early days of mechanical thrombectomy for acute stroke.
ProfMeretoja offered his perspective on the arrangement of a comprehensive acute stroke service, including the “mother ship” model whereby the thrombectomy service is limited to key nodes in a network of hospitals that have open referral pathways to the thrombectomy service. Using this model, emergent computed tomography (CT) imaging of the brain and CT angiography of the carotid and cerebral vessels can be done as a combined investigation at the first instance when an acute stroke is identified in the frontline service, and patients can then be rapidly selected and transferred for mechanical thrombectomy if they have proximal vessel occlusions.
It was a stimulating meeting that evoked excitement for what the future of stroke and hypertension holds.

S4 AUBAGIO® 14mg (Film-coated Tablet). Each film-coated tablet contains 14 mg of teriflunomide. Reg.No.: 47/32.16/0859

JANSSEN PHARMACEUTICA (PTY) LTD, (Reg. No. 1980/011122/07), Building 6, Country Club Estate, 21 Woodlands Drive, Woodmead, 2191. www.janssen.co.za. Medical Info Line: 0860 11 11 17. PHZA/NEUC/0817/0001
Together we cover your family
S6 NEUCON® 18 mg, 27 mg, 36 mg, 54 mg extended-release tablets containing 18 mg, 27 mg, 36 mg, 54 mg of methylphenidate hydrochloride respectively. Reg. Nos.: 46/1.2/0380; 46/1.2/0381;46/1.2/0382; 46/1.2/0383. For full prescribing information, refer to the latest package insert (April 2017).
References: 1. Coghill D, Seth S. Osmotic, controlled-release methylphenidate for the treatment of ADHD. Expert Opinion Pharmacotherapy 2006;7(15):2119-2138. 2. Data on file.
The only clone OROS® engineered for full patient benefits 1 Affordable 2 Effective 1
New !