Embed Size (px)
Citation preview

Dent 355Dent 355Keratoses and Related Keratoses and Related
Disorders of Oral Mucosa IIDisorders of Oral Mucosa II
Dr. Rima Safadi Dr. Rima Safadi Modified from Dr. Huda Hammad Modified from Dr. Huda Hammad
lectureslecturesReference: Oral pathology book by Reference: Oral pathology book by
Soams and SouthamSoams and Southam

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
Wide range in histological appearances Wide range in histological appearances reflects reflects varying degrees varying degrees of:of:
keratosiskeratosis, , epithelial epithelial thicknessthickness, , epithelial epithelial dysplasiadysplasia,, chronic chronic inflammation inflammation in the lamina in the lamina
propria.propria.

It is important to remember that:It is important to remember that: Leukoplakia is a Leukoplakia is a clinical clinical
diagnosis diagnosis arrived at after arrived at after exclusion of other diseases and exclusion of other diseases and is is notnot based on any specific based on any specific histopathological features, i.e. histopathological features, i.e. the term leukoplakia has the term leukoplakia has no no histological connotation.histological connotation.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
Hyperkeratosis may be due to orthokeratosis, Hyperkeratosis may be due to orthokeratosis, parakeratosis, or both.parakeratosis, or both.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
Epithelium may be Epithelium may be hyperplastic or atrophic.hyperplastic or atrophic.
Areas of erythroplakia are Areas of erythroplakia are often associated with often associated with epithelial atrophy.epithelial atrophy.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
The junction The junction between normal between normal and abnormal and abnormal epithelium may be epithelium may be abrupt or there abrupt or there may be gradual may be gradual transition.transition.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
2 features are highly 2 features are highly suggestive of smoking as suggestive of smoking as an etiological factor:an etiological factor:
1. presence of chevron peaks 1. presence of chevron peaks in keratin.in keratin.
2. increased melanin 2. increased melanin production in basal production in basal keratinocytes and leakage keratinocytes and leakage of melanin into the of melanin into the underlying connective underlying connective tissue (melanin tissue (melanin incontinence).incontinence).

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
In some leukoplakias, keratosis and change in thickness are the In some leukoplakias, keratosis and change in thickness are the only abnormal features.only abnormal features.
Other cases show features of epithelial dysplasia.Other cases show features of epithelial dysplasia.
When dysplasia is present, not all dysplastic features are When dysplasia is present, not all dysplastic features are necessarily seen in any one case.necessarily seen in any one case.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
The degree of dysplasia is The degree of dysplasia is subjectively assessed subjectively assessed using terms using terms such as such as mild, moderate and mild, moderate and severe severe based on the based on the thicknessthickness of of epithelium involved.epithelium involved.
Mild (grade I) dysplasia Mild (grade I) dysplasia demonstrates proliferation of demonstrates proliferation of atypical or immature basal cells atypical or immature basal cells above the parabasal region but above the parabasal region but not extending beyond the lower not extending beyond the lower third of the epithelium. third of the epithelium.
Moderate (grade II) dysplasia Moderate (grade II) dysplasia demonstrates a similar demonstrates a similar proliferation into the proliferation into the middle one-middle one-third third of the epithelial cross-of the epithelial cross-section. section.
The term severe (grade III) The term severe (grade III) dysplasia is reserved for dysplasia is reserved for abnormal proliferation from abnormal proliferation from the basal layer into the upper the basal layer into the upper third of the epithelium.third of the epithelium.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
Although it is not possible to predict Although it is not possible to predict the presence and severity of the presence and severity of dysplasia from clinical appearance dysplasia from clinical appearance lesion, lesion,
erythroplakias and non-erythroplakias and non-homogeneous leukoplakias are homogeneous leukoplakias are more likely to be dysplastic (or even more likely to be dysplastic (or even malignant) than homogeneous malignant) than homogeneous leukoplakias.leukoplakias.
Several studies showed only about Several studies showed only about 10% of homogeneous leukoplakias10% of homogeneous leukoplakias to be dysplastic, as opposed to to be dysplastic, as opposed to 50% 50% or more of non-homogeneous typesor more of non-homogeneous types..
Speckled leukoplakias show a very Speckled leukoplakias show a very high incidence of dysplasia, which high incidence of dysplasia, which approaches 100%approaches 100% as speckling as speckling increases and as the clinical increases and as the clinical features more closely resemble features more closely resemble erythroplakia.erythroplakia.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial DysplasiaDysplasia
The individual The individual cellular changes cellular changes (cellular atypia) (cellular atypia) seen in dysplastic seen in dysplastic epithelium reflect epithelium reflect abnormalities in abnormalities in proliferationproliferation, , maturationmaturation, and , and differentiation of differentiation of epithelial cells. epithelial cells.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
1.1. Increased and abnormal mitoses.Increased and abnormal mitoses.2.2. Basal cell hyperplasia.Basal cell hyperplasia.3.3. Drop-shaped rete ridges.Drop-shaped rete ridges.4.4. Disturbed polarity of basal cells or loss of cellular orientation.Disturbed polarity of basal cells or loss of cellular orientation.5.5. Increase in nuclear/cytoplasmic ratio.Increase in nuclear/cytoplasmic ratio.6.6. Nuclear hyperchromatism.Nuclear hyperchromatism.7.7. Prominent and enlarged nucleoli.Prominent and enlarged nucleoli.8.8. Irregular epithelial stratification or disturbed maturation.Irregular epithelial stratification or disturbed maturation.9.9. Nuclear and cellular pleomorphism.Nuclear and cellular pleomorphism.10.10. Abnormal keratinization.Abnormal keratinization.11.11. Loss or reduction of intercellular adhesion.Loss or reduction of intercellular adhesion.First 7 features represents abnormal proliferation while last 4 First 7 features represents abnormal proliferation while last 4
represents abnormal maturation/differentiationrepresents abnormal maturation/differentiation

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
1. Increased and abnormal mitoses.1. Increased and abnormal mitoses.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
2. Basal cell hyperplasia.2. Basal cell hyperplasia.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
3. Drop-shaped rete ridges.3. Drop-shaped rete ridges.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
4. Disturbed polarity of basal cells or loss of 4. Disturbed polarity of basal cells or loss of cellular orientation.cellular orientation.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
5. Increase in nuclear/ cytoplasmic ratio.5. Increase in nuclear/ cytoplasmic ratio.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
6. Nuclear hyperchromatism.6. Nuclear hyperchromatism.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia7. Prominent and enlarged nucleoli.7. Prominent and enlarged nucleoli.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia8. Irregular epithelial stratification or 8. Irregular epithelial stratification or
disturbed maturation.disturbed maturation.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
9. Nuclear and cellular pleomorphism.9. Nuclear and cellular pleomorphism.

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
10. Abnormal keratinization (dyskeratosis).10. Abnormal keratinization (dyskeratosis).

Leukoplakia: Pathology, Epithelial Leukoplakia: Pathology, Epithelial Dysplasia- Features of Epithelial Dysplasia- Features of Epithelial
DysplasiaDysplasia
11. Loss or reduction of intercellular 11. Loss or reduction of intercellular adhesion.adhesion.

Epithelial DysplasiaEpithelial Dysplasia
Cellular atypia of minor degree may Cellular atypia of minor degree may be seen in reaction to inflammation be seen in reaction to inflammation in conditions such as lichen planus in conditions such as lichen planus and candidosis (reactive cellular and candidosis (reactive cellular atypia)atypia)

Leukoplakia: PrognosisLeukoplakia: Prognosis
Unpredictable tendency to undergo malignant Unpredictable tendency to undergo malignant transformation.transformation.
Marked variation in reported rates from different countries.Marked variation in reported rates from different countries.
Differences in diagnostic criteria and etiological factors.Differences in diagnostic criteria and etiological factors.
Transformation times vary from one to several years.Transformation times vary from one to several years.
Combining results from several studies, a rate of ~14% Combining results from several studies, a rate of ~14% over a period of up to 20 years has been reported.over a period of up to 20 years has been reported.

Leukoplakia: PrognosisLeukoplakia: Prognosis
Potential for malignant Potential for malignant transformation is greater transformation is greater in high risk sites (ventral in high risk sites (ventral tongue, FOM, lingual tongue, FOM, lingual aspect of lower alveolar aspect of lower alveolar mucosa).mucosa).
Lesions in these areas are Lesions in these areas are designated as designated as sublingual sublingual keratosis keratosis to draw to draw attention to these sites.attention to these sites. 25% showed invasive SCC in 25% showed invasive SCC in
some studiessome studies

Leukoplakia: PrognosisLeukoplakia: Prognosis
Dysplastic lesions carry an increased risk of Dysplastic lesions carry an increased risk of malignant transformation (<10%->30%).malignant transformation (<10%->30%).
The more severe the dysplastic features, the The more severe the dysplastic features, the greater the risk, but no clear correlation.greater the risk, but no clear correlation.
The majority of dysplastic lesions remain The majority of dysplastic lesions remain unchanged during observation period.unchanged during observation period.
A proportion of these will improve or regress.A proportion of these will improve or regress.

Leukoplakia: PrognosisLeukoplakia: Prognosis
Speckled and other non-Speckled and other non-homogeneous types have homogeneous types have an increased rate of an increased rate of malignamalignant transformation.nt transformation.
ErythroplakiaErythroplakia alone or as alone or as part of speckled part of speckled leukoplakia shows invasive leukoplakia shows invasive carcinoma or carcinoma or carcinoma icarcinoma in n situ on ~situ on ~ 50% o 50% of initial f initial biopsies, and most of the biopsies, and most of the remaining show severe remaining show severe dysplasia.dysplasia.

Leukoplakia: PrognosisLeukoplakia: Prognosis
Candidal Candidal leukoplakia has a leukoplakia has a high high incidence of incidence of dysplasia or dysplasia or malignant malignant transformation transformation (~30%).(~30%).

Epithelial dysplasia Epithelial dysplasia
Dysplastic leukoplakia-Dysplastic leukoplakia- higher rate to higher rate to progress than non neoplastic (10-30%)progress than non neoplastic (10-30%)
More severe dysplasiaMore severe dysplasia higher risk higher risk Majority of dysplasia remain unchangedMajority of dysplasia remain unchanged
May progress or improveMay progress or improve No clear corelation between histology and No clear corelation between histology and
clinical:clinical: Sublingual keratosis even with mild dysplasia is Sublingual keratosis even with mild dysplasia is
high riskhigh risk

Leukoplakia: PrognosisLeukoplakia: Prognosis
Malignant transformation likely to be due to Malignant transformation likely to be due to progressive accumulation of genetic changes progressive accumulation of genetic changes over time.over time.
Recent studies show that leukoplakias with Recent studies show that leukoplakias with abnormal DNA content of epithelial cells are abnormal DNA content of epithelial cells are more likely to undergo malignant transformation.more likely to undergo malignant transformation.
This may become an important prognostic This may become an important prognostic indicator in the future.indicator in the future.

Leukoplakia PrognosisLeukoplakia Prognosis
DNA content is related to number of chromosomes:DNA content is related to number of chromosomes: Malignant cells have abonormal number of chromosomes Malignant cells have abonormal number of chromosomes
(deletions replications etc..)(deletions replications etc..) Variation in number of chromosomes: aneuoploidyVariation in number of chromosomes: aneuoploidy Duplication of chromosomes: tetraploidyDuplication of chromosomes: tetraploidy Normal cells with 2 copies: diploidyNormal cells with 2 copies: diploidy
Leukoplakia:Leukoplakia: DiploidDiploid low risk low risk AneuploidAneuploid high risk high risk TetraploidTetraploidintermediate riskintermediate risk

Leukoplakia: PrognosisLeukoplakia: Prognosis
At present, risk assessment is based At present, risk assessment is based on:on:
1.1. SizeSize2.2. SiteSite3.3. Clinical appearanceClinical appearance4.4. Degree of epithelial dysplasia.Degree of epithelial dysplasia.

Dermatological Causes of White Dermatological Causes of White PatchesPatches
Lichen PlanusLichen Planus
Lupus ErythematosusLupus Erythematosus

Lichen PlanusLichen Planus
Name provided by Name provided by Erasmus Wilson in 1869.Erasmus Wilson in 1869.
He probably thought the He probably thought the skin lesions looked like skin lesions looked like lichens growing on rocks.lichens growing on rocks.
Lichens are primitive Lichens are primitive plants composed of plants composed of symbiotic algae and fungi.symbiotic algae and fungi.

Lichen PlanusLichen Planus Relatively common disease (0.5-2% population).Relatively common disease (0.5-2% population).
Worldwide distribution.Worldwide distribution.
Involves skin and mucous membranes.Involves skin and mucous membranes.
Peaks between ages 30-50.Peaks between ages 30-50.
60% females.60% females.
Oral lesions detected in ~50% of patients with initial skin lesions.Oral lesions detected in ~50% of patients with initial skin lesions.
Skin lesions in 10-50% of patients with initial oral lesions.Skin lesions in 10-50% of patients with initial oral lesions.
Oral lesions may occur before, at the same time as, or after skin lesions.Oral lesions may occur before, at the same time as, or after skin lesions.

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Skin lesions:Skin lesions: Violaceous, itchy papules, Violaceous, itchy papules,
may have white streaks on may have white streaks on surface (Wickham’s striae).surface (Wickham’s striae).
Variable patterns for Variable patterns for papules: discrete, linear, papules: discrete, linear, annular, bullous, or annular, bullous, or widespread rash.widespread rash.

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Skin Lesions:Skin Lesions:

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Skin Lesions:Skin Lesions:
Predilection to flexor Predilection to flexor surface of wrist.surface of wrist.
10% with nail involvement 10% with nail involvement in the form of vertical in the form of vertical ridges.ridges.
Lesions develop slowly and Lesions develop slowly and 85% resolve within 18 85% resolve within 18 months, sometimes with months, sometimes with recurrence.recurrence.

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Oral Lesions:Oral Lesions:
In contrast to skin lesions, oral lesions pursue a much more chronic course, In contrast to skin lesions, oral lesions pursue a much more chronic course, sometimes extending over many years.sometimes extending over many years.
Mostly affect buccal mucosa, may also affect tongue, gingiva, palate, and lips.Mostly affect buccal mucosa, may also affect tongue, gingiva, palate, and lips.
Bilateral and wide spectrum of presentations, alone or in combination.Bilateral and wide spectrum of presentations, alone or in combination.

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Oral Lesions:Oral Lesions:
Non-erosive typeNon-erosive type::
- reticular or annular, - reticular or annular, papular, plaque-papular, plaque-like.like.
- usually - usually asymptomatic.asymptomatic.

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Oral Lesions:Oral Lesions:
Erosive/atrophic types:Erosive/atrophic types:
- red glazed appearance with - red glazed appearance with areas of superficial ulceration areas of superficial ulceration which may take several weeks which may take several weeks to heal.to heal.
- occasionally, ulcers are preceded - occasionally, ulcers are preceded by by bullae (bullous type).bullae (bullous type).
- often associated with typical - often associated with typical areas of non-erosive lichen areas of non-erosive lichen planus.planus.
- pain and discomfort may be - pain and discomfort may be severe.severe.

Lichen Planus: Clinical FeaturesLichen Planus: Clinical Features
Oral Lesions:Oral Lesions:
Lichen planus involving the Lichen planus involving the gingiva often presents as a gingiva often presents as a desquamative gingivitis.desquamative gingivitis.
More typical areas can More typical areas can usually be seen elsewhere usually be seen elsewhere on the oral mucosa.on the oral mucosa.

Regezi

Lichen Planus: PathologyLichen Planus: Pathology
Histopathologic Features:Histopathologic Features:
Ortho- or parakeratosis.Ortho- or parakeratosis.
Epithelial atrophy or Epithelial atrophy or acanthosis (sawtooth acanthosis (sawtooth pattern of rete ridges).pattern of rete ridges).
Dense, well-defined band Dense, well-defined band of subepithelial of subepithelial mononuclear infiltrate, mononuclear infiltrate, mainly T-cells.mainly T-cells.


Lichen Planus: PathologyLichen Planus: Pathology
Histopathologic Features:Histopathologic Features:


Lichen Planus: PathologyLichen Planus: Pathology
Histopathologic Features:Histopathologic Features:
Liquefactive Liquefactive degeneration of basal degeneration of basal cell layer associated cell layer associated with edema and with edema and lymphocytic infiltration.lymphocytic infiltration.
Civatte bodies: hyaline Civatte bodies: hyaline shrunken bodies shrunken bodies representing apoptotic representing apoptotic cells.cells.

Lichen Planus: PathologyLichen Planus: Pathology
Histopathologic Histopathologic Features:Features:
Basal cell Basal cell degeneration may degeneration may result in subepithelial result in subepithelial bullae formation and bullae formation and ulceration.ulceration.


Lichen Planus: PathologyLichen Planus: Pathology
Almost all cases run a benign Almost all cases run a benign course.course.
Malignant transformation has Malignant transformation has been described in a very been described in a very small proportion (0.5%-2.5% small proportion (0.5%-2.5% over 5 years).over 5 years).
Some studies suggest that Some studies suggest that atrophic/erosive forms are atrophic/erosive forms are more likely for such more likely for such transformation.transformation.
Other studies found it more Other studies found it more likely with plaque lesions.likely with plaque lesions.

Lichen Planus: Etiology & Lichen Planus: Etiology & PathogenesisPathogenesis
Not fully understood.Not fully understood.
Widely accepted that Widely accepted that cell-mediated immune responses cell-mediated immune responses to to an external antigen, or internal antigenic changes in an external antigen, or internal antigenic changes in epithelial cells, are involved.epithelial cells, are involved.
Response resembles type IV hypersensitivity.Response resembles type IV hypersensitivity.
Cytotoxic lymphocytes damage basal epithelium.Cytotoxic lymphocytes damage basal epithelium.
In most cases the precipitating factors are unknown.In most cases the precipitating factors are unknown. May be hypersensitivity to drugs and dental materialsMay be hypersensitivity to drugs and dental materials Association with systemic conditions: Hep CAssociation with systemic conditions: Hep C Graft versus host reaction presents with LP like lesions Graft versus host reaction presents with LP like lesions

Lichen Planus: Etiology & Lichen Planus: Etiology & PathogenesisPathogenesis
In some patients, lesions In some patients, lesions are triggered by are triggered by hypersensitivity to drugs or hypersensitivity to drugs or dental materials.dental materials.
In such cases the condition In such cases the condition resolves upon withdrawal resolves upon withdrawal of the offending agent.of the offending agent.
Such lesions are referred Such lesions are referred to as to as “lichenoid reactions“lichenoid reactions” ” to distinguish them from to distinguish them from idiopathic lichen planus.idiopathic lichen planus.
Lichenoid reaction to dental amalgamLichenoid reaction to dental amalgam

External antigen challenge and/or modified antigenic structure of epithelial cellsExternal antigen challenge and/or modified antigenic structure of epithelial cells
Antigen challengeAntigen challenge
Langerhans cells KeratinocytesLangerhans cells KeratinocytesExpression of ICAM-1Expression of ICAM-1
Expression of class II MHC Cytokine releaseExpression of class II MHC Cytokine release
Antigen presentation LymphocyteAntigen presentation Lymphocyteto CD4 cells infiltrationto CD4 cells infiltration
Activation of CD8 Damage to basal cellsActivation of CD8 Damage to basal cellscytotoxic cellscytotoxic cells
Lichen Planus: Lichen Planus: PathogenesisPathogenesis

Lichen Planus: PathogenesisLichen Planus: Pathogenesis Lichen planus has been associated with some Lichen planus has been associated with some systemic systemic
diseases.diseases.
In many of these, a In many of these, a cause-and-effect relationship has not cause-and-effect relationship has not been established.been established.
The systemic condition may merely The systemic condition may merely exacerbateexacerbate a pre- a pre-existing lesion.existing lesion.
Strong evidence of association of chronic liver disease Strong evidence of association of chronic liver disease associated with associated with hepatitis C virus infection.hepatitis C virus infection.
Oral and cutaneous lesions resembling lichen planus Oral and cutaneous lesions resembling lichen planus occur occur in graft vs. host diseasein graft vs. host disease Transplanted T cells Transplanted T cells react to antigens on host epithelial cells.react to antigens on host epithelial cells.

GVHGVH

Lupus ErythematosusLupus Erythematosus
Two main forms:Two main forms:
1.1. Chronic discoid LE: localized.Chronic discoid LE: localized.
2.2. Systemic LE: disseminated.Systemic LE: disseminated. A variety of autoantibodies are present in A variety of autoantibodies are present in
SLE, e.g. antinuclear antibodies (ANAs).SLE, e.g. antinuclear antibodies (ANAs).
Females > males.Females > males.

Lupus Erythematosus: Clinical Lupus Erythematosus: Clinical FeaturesFeatures
Chronic Discoid Lupus Chronic Discoid Lupus Erythematosus (DLE):Erythematosus (DLE):
Lesions often restricted to Lesions often restricted to skin and usually occur on skin and usually occur on the face.the face.
Scaly red patches which heal Scaly red patches which heal with scarring.with scarring.
Sometimes facial lesions in Sometimes facial lesions in both forms both forms have a have a symmetric distribution symmetric distribution (butterfly rash).(butterfly rash).


Lupus Erythematosus: Clinical Lupus Erythematosus: Clinical FeaturesFeatures
Chronic Discoid Lupus Erythematosus Chronic Discoid Lupus Erythematosus (DLE): (DLE):
Oral lesions in up to 50% of cases.Oral lesions in up to 50% of cases.
Buccal mucosa most frequently Buccal mucosa most frequently affected.affected.
Considerable variation in oral Considerable variation in oral lesions.lesions.
Most common is a discoid area of Most common is a discoid area of erythema or ulceration erythema or ulceration surrounded surrounded by white keratotis border by white keratotis border sometimes with sometimes with radiating striaeradiating striae..
Main D/D lichen planus.Main D/D lichen planus.


Lupus Erythematosus: Clinical Lupus Erythematosus: Clinical FeaturesFeatures
Systemic Lupus Erythematosus Systemic Lupus Erythematosus (SLE): (SLE):
Disseminated disease almost Disseminated disease almost involving every organ.involving every organ.
Skin rashes: maculopapular, Skin rashes: maculopapular, photosensitive especially on photosensitive especially on face (butterfly rash).face (butterfly rash).
Oral lesions variable.Oral lesions variable.
May be fatal.May be fatal.

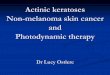
Lupus erythematosus Lupus erythematosus histopathologyhistopathology
Deep perivascular Lymphocytic infiltrate

Lupus Erythematosus: Histopathologic Lupus Erythematosus: Histopathologic FeaturesFeatures
Subepithelial and Subepithelial and deep perivascular deep perivascular lymphocytic infiltrates.lymphocytic infiltrates.
Liquefactive Liquefactive degenerartion of basal degenerartion of basal cells.cells.

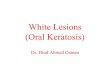
Lupus erythematosusLupus erythematosus
Immunofluorescence studies show Immunofluorescence studies show abundant deposits of IgG and abundant deposits of IgG and complement-complement- Lupus Band Lupus Band

Revision slidesRevision slides



White Sponge nevusWhite Sponge nevus


LeukoplakiaLeukoplakia


Submucous fibrosisSubmucous fibrosis(epithelial atrophy)(epithelial atrophy)


SCCSCC

Plummer Vinson syndromePlummer Vinson syndrome(epithelial atrophy)(epithelial atrophy)