Embed Size (px)
Citation preview

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 45
3
3. Overall and disease-specific survival
of Hodgkin lymphoma survivors who
subsequently developed
gastrointestinal cancer
Submitted
Lisanne Rigter
Michael Schaapveld
Cécile Janus
Augustinus Krol
Richard van der Maazen
Judith Roesink
Josée Zijlstra
Gustaaf van Imhoff
Philip Poortmans
Max Beijert
Pieternella Lugtenburg
Otto Visser
Petur Snaebjornsson
Anna van Eggermond
Berthe Aleman
Flora van Leeuwen*
Monique van Leerdam*
* Both authors contributed equally

46 Chapter 3
Abstract
Background
Hodgkin lymphoma (HL) survivors have an increased risk of gastrointestinal (GI)
cancer. This study aims to evaluate whether survival of patients who survived HL
and developed GI cancer differs from survival of first primary GI cancer patients.
Patients and methods
Overall and cause-specific survival of GI cancer patients in a HL survivor cohort (GI-
HL, n=104, including esophageal, gastric, small intestinal and colorectal cancer) was
compared with survival of a first primary GI cancer patient cohort (GI-1, n=1025,
generated by case matching based on tumor site, gender, age and year of
diagnosis). Cox proportional hazards regression was used for survival analyses.
Multivariable analyses were adjusted for GI cancer stage, grade of differentiation,
surgery, radiotherapy, chemotherapy.
Results
GI-HL cancers were diagnosed at a median age of 54 years (interquartile range 45-
60). No differences in tumor stage or frequency of surgery were found. GI-HL
patients less often received radiotherapy (8% vs. 23% in GI-1 patients, P<0.001)
and chemotherapy (28% vs. 41%, P=0.01) for their GI tumor.
Compared with GI-1 patients, overall and disease-specific survival of GI-HL patients
was worse (univariable hazard ratio (HR) 1.30 (95% confidence interval (CI) 1.03-
1.65) P=0.03 and HR 1.29 (95% CI 1.00-1.67) P=0.049, respectively; multivariable
HR 1.33 (95% CI 1.05-1.68) P=0.02 and HR 1.33 (95% CI 1.03-1.72) P=0.03,
respectively). Mortality from other causes was non-significantly increased in GI-HL
patients compared with GI-1 patients (HR 1.44 (95% CI 0.81-2.56) P=0.22).
Conclusion
Long-term overall and disease-specific survival of GI cancer in HL survivors is worse
compared with first primary GI cancer patients. Differences in tumor stage, grade
of differentiation, treatment, or mortality from other causes could not explain this
worse survival. As such, this may be explained by a worse treatment response due
to HL-related comorbidities or due to a different pathogenesis of therapy-related
gastrointestinal cancer.

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 47
3
Background
Hodgkin lymphoma (HL) survivors are at increased risk of developing second
malignancies, which are a major cause for morbidity and mortality. 1-6 Compared
with the general population, the risk of developing gastrointestinal (GI) cancer is
approximately 5-fold higher in HL survivors. 1, 2, 4, 7-11 This risk remains elevated up
to 40 years after HL and is strongly related to HL treatment. 1 Both exposure to
radiotherapy and alkylating agents, such as procarbazine, have been associated
with the development of GI cancers. 1, 2, 7-9, 11-13
A few studies suggest a difference in clinical and histopathological characteristics
of GI cancer in HL survivors compared with first primary GI cancer. 14-16 To our
knowledge, only one previous study examined survival of GI cancer in HL survivors
and reported a worse overall survival in subgroups of HL survivors compared with
first primary GI cancer patients, i.e.; those diagnosed with TNM stage IIB-IV colon
cancer and a small group (n=8) of TNM stage I gastric cancer. 15 The same authors
found no differences in disease-specific survival.
The cause of the reported reduced overall survival of GI cancers in HL survivors
remained unknown. Less favorable survival might be due to differences in (HL
treatment-induced) carcinogenesis leading to differences in GI tumor
characteristics, or to adaptation of GI cancer treatment due to the previous
treatment for HL. Furthermore, increased risks of competing causes of death, such
as other malignancies or cardiovascular disease, might play a role. 5, 17, 18
In view of the reported worse overall survival of GI cancer in HL survivors and its
unknown etiology, we designed this study to evaluate overall and cause-specific
survival of GI cancer in HL survivors.
Patients and Methods
Study design This study compared overall and cause-specific survival of esophageal, gastric,
small intestinal and colorectal cancer in a HL survivor cohort (GI-HL) with survival of
a population-based cohort of first primary GI cancer patients (GI-1).

48 Chapter 3
Gastrointestinal cancer patients in a Hodgkin lymphoma survivor cohort (GI-HL) In a Dutch multicenter cohort of HL patients who survived at least 5 years after
primary treatment (n=2,996), 121 patients with carcinomas of the esophagus,
stomach, small intestine or colorectum were identified. Data on HL patients,
diagnosed in the period 1965-2000 and between 15 and 50 years of age at HL
diagnosis, were collected as previously described. 1, 5, 17 In short, data collection
comprised detailed HL treatment data and information on second cancers, using
medical records, by responses to questionnaires sent to general practitioners and
linkage with the Netherlands Cancer Registry (NCR, from 1989 onwards). 1
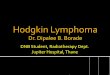
A total of 17/121 (13%) GI-HL patients were excluded, of whom 16 because they
were not confirmed by the NCR, most likely due to incomplete data registration as
HL was diagnosed before complete population-based cancer registration in the
Netherlands in 1989 (figure 1). In patients with more than one HL-GI cancer, only
the first (if metachronous) or highest TNM stage (if synchronous) was included in
the analyses.
First primary gastrointestinal cancer cohort (GI-1) For each GI-HL cancer, the NCR searched for 10 matched controls with a GI-1
cancer, based on the following criteria: gender, no prior diagnosis of invasive
tumors, tumor location (esophagus, stomach, small intestine or colorectum), year
of diagnosis (closest proximity, maximum of 5 years difference) and age at
diagnosis (closest proximity, maximum of 3 years difference). For three GI-HL
patients, it was not possible to obtain 10 matched GI-1 patients because of the
young age at diagnosis. Subsequently, data on GI cancer characteristics, treatment,
and follow up were collected for both GI-HL and GI-1 patients.
From Statistics Netherlands (CBS), we obtained information on the cause of death,
which was categorized into GI cancer of interest or other causes, including
unknown causes. As all data were processed and analyzed completely
anonymously, this study was exempt from review by the Institutional Review
Board.

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 49
3
Statistical analyses Patient and tumor characteristics of GI-HL and GI-1 patients were compared using
Chi-square, Fishers’ exact or Mann-Whitney U tests. Overall survival and cause-
specific survival were presented using the Kaplan-Meier method. Cause-specific
survival was divided into disease-specific survival, related to the GI cancer of
interest, and survival related to other causes of death (using GI-cancer-related
death as a censoring event).
In 12 out of 104 GI-HL patients, the HL-GI tumor was not the first diagnosis of a
malignancy after HL. Since these other primary tumors or their treatment might
affect survival, these 12 patients and their matched controls were excluded from
further survival analyses (figure 1, supplementary table 1). Thus, 92/104 GI-HL
tumors and their 911 matched controls were included in Cox proportional hazards
regression models. As the grouping variable (GI-HL vs. GI-1) was the main
independent variable of interest, its effect on survival (e.g. HR) was primarily
evaluated in a univariable model. In addition, we evaluated the effect of patient-
related and tumor-related characteristics on the survival difference between GI-HL
and GI-1 patients, i.e. on the HR of this grouping variable. For this purpose, a
multivariable model with tumor characteristics, treatment characteristics and a
combination of tumor and treatment characteristics was created. We also assessed
disease-specific mortality while treating other causes of death as a competing risk.
Due to the relatively small number of patients in GI site-specific multivariable
models, the effect of tumor characteristics and treatment characteristics on the
survival difference between GI-HL and GI-1 patients was evaluated in models that
included the grouping variable and one other characteristic. In case of a >10%
change in the hazard ratio for the grouping variable (e.g. GI-HL vs. GI-1), a
characteristic was considered as an influencing factor on the survival difference
between groups. Analyses were performed using IBM SPSS Statistics 22 and STATA
version 14.

50 Chapter 3
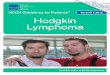
Figure 1. CONSORT diagram of gastrointestinal cancer in Hodgkin lymphoma survivors (GI-HL) and first primary gastrointestinal cancer patients (GI-1).
* The Netherlands Cancer Registry (NCR) attempted to register previous cancers for all patients with incident cancer since 1989; the history of previous cancers is known to be incomplete.

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 51
3
Results
General description and comparison of GI-HL and GI-1 patients GI-HL cancers were diagnosed at a median age of 54 years (interquartile range
(IQR) 45-60). The majority occurred in males (67%). Patients were diagnosed with
HL at a median age of 30 years (interquartile range (IQR) 22-41, supplementary
table 1). Median year of HL diagnosis was 1981 (range 1966-2000). In 53/104 (51%)
patients, HL had been treated with both radiotherapy and procarbazine-containing
chemotherapy and 43/104 (41%) patients had been treated for a HL recurrence.
Due to the matching procedure, GI-HL cancers were not different from GI-1
cancers with respect to gender and age at diagnosis (table 1). In addition, TNM
stage of both groups was comparable. GI-HL patients were less frequently treated
for their GI tumor with radiotherapy (8% vs. 23% in GI-1 patients, P<0.001) or
chemotherapy (29% vs. 41%, P=0.01). GI-HL tumors were treated more frequently
with surgery alone and less frequently with combined modality treatment that
included radiotherapy or chemotherapy compared with GI-1 tumors (P=0.005,
table 1).
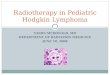
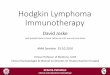
Gastrointestinal cancer: overall survival Median survival times of 104 GI-HL patients and 1,025 GI-1 patients were 2.4 years
and 2.5 years, respectively. Overall survival of GI-HL patients was worse than that
of GI-1 patients (hazard ratio (HR) 1.27, 95% confidence interval (CI) 1.01-1.58,
P=0.037). HL survivors in whom the GI-HL cancer was a third primary and their
matched controls were excluded for further survival analyses, leaving 92 GI-HL
patients who also had worse overall survival compared with 911 GI-1 patients (HR
1.30, 95% CI 1.03-1.65, P=0.028, supplementary table 1). After five years, overall
survival of GI-HL and GI-1 patients was 28% and 37%, respectively, after 10 years
18% and 30%, respectively, and after fifteen years 15% and 28%, respectively
(figure 2, table 2).
Several multivariable models were evaluated for the identification of contributive
(mediating) factors (e.g. tumor characteristics or treatment characteristics) to the
overall survival difference between GI-HL and GI-1 patients.

52 Chapter 3
Table 1. Characteristics of gastrointestinal cancer in Hodgkin lymphoma survivors and first primary gastrointestinal cancer patients.
Gastrointestinal cancers include two GI-HL small intestinal cancers and their matched GI-1 controls. Abbreviations: GI-HL, gastrointestinal cancer in Hodgkin lymphoma survivors; GI-1, first primary gastrointestinal cancer patients; RT, radiotherapy; CT, chemotherapy. * defined as neuroendocrine carcinomas, large cell carcinomas, undifferentiated carcinomas, anaplastic carcinomas or unspecified carcinomas.
GI cancer characteristic Gastrointestinal cancer
GI-HL (N=104)
GI-1 (N=1025)
n (%) n (%) P value Age Median (IQR) 54 (45-60) 54 (45-60) 0.82 Gender Male 70 (67) 698 (68) 0.87 Female 34 (33) 327 (32) Morphology category Adenocarcinoma 81 (78) 900 (88) <0.001 Squamous cell carcinoma 18 (17) 117 (11) Other carcinoma* 5 (5) 8 (1) TNM Stage I 12 (12) 124 (12) 0.79 II 24 (23) 202 (20) III 26 (25) 253 (25) IV 35 (34) 387 (38) Unknown 7 (7) 59 (6) Grade of differentiation Well / low grade 8 (8) 36 (4) 0.005 Moderate / intermediate 34 (33) 340 (33) Poor / high 22 (21) 338 (33) Undifferentiated / anaplastic 4 (4) 10 (1) Unknown 36 (35) 301 (29) Surgery No 37 (36) 396 (39) 0.54 Yes 67 (64) 629 (61) Radiotherapy No 96 (92) 785 (77) <0.001 Yes 8 (8) 240 (23) Chemotherapy No 75 (72) 608 (59) 0.01 Yes 29 (28) 417 (41) Treatment category No treatment 18 (17) 153 (15) 0.005 Surgery only 51 (49) 348 (34) Surgery & RT and/or CT 16 (15) 281 (27) RT and/or CT only 19 (18) 243 (24)

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 53
3
Figure 2. Overall survival of gastrointestinal cancer in Hodgkin lymphoma survivors (GI-HL, blue) compared with first primary gastrointestinal cancer patients (GI-1, green).
* first primary gastrointestinal cancer patients, green line, number of cases at risk. † gastrointes nal cancer in Hodgkin lymphoma survivors, blue line, number of cases at risk. In the first multivariable model, adjusted for tumor characteristics (TNM stage,
grade of differentiation, tumor location), the difference between GI-HL and GI-1
patients remained present (HR 1.33 (95% CI 1.05-1.68) P=0.02).
This difference also remained present after adjustment for treatment
characteristics (surgery, radiotherapy, chemotherapy) and after adjustment for
both tumor and treatment characteristics (HR 1.32 (95% CI 1.04-1.68) P=0.02 and
HR 1.33 (95% CI 1.05-1.68) P=0.02, respectively).

54 Chapter 3
Gastrointestinal cancer: cause-specific survival Disease-specific survival was worse in GI-HL patients than in GI-1 patients (HR 1.29
(95% CI 1.00-1.67) P=0.049). Mortality from other causes appeared to be non-
significantly higher in GI-HL patients compared with GI-1 patients (HR 1.44 (95% CI
0.81-2.56) P=0.22). At five years after GI cancer diagnosis, cumulative disease-
specific mortality and cumulative mortality from other causes in GI-HL patients
were 66% and 7%, respectively, and in GI-1 patients 56% and 7%, respectively
(table 3). In a multivariable model adjusted for treatment characteristics, disease-
specific survival remained worse in GI-HL patients than in GI-1 patients (HR 1.33
(95% CI 1.03-1.72) P=0.03). After adjustment for both tumor characteristics and
treatment characteristics, this survival difference also remained present (HR 1.33
(95% CI 1.03-1.72) P=0.03).
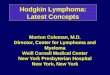
Esophageal cancer characteristics and survival GI-HL esophageal cancers were more frequently located in the upper esophagus
than GI-1 cancers (23% vs. 7%, P=0.01, figure 3). A lower frequency of
adenocarcinomas and a higher frequency of squamous cell and other carcinomas
(including neuroendocrine carcinomas, large cell carcinomas, undifferentiated
carcinomas, anaplastic carcinomas or unspecified carcinomas) was found in the GI-
HL group compared with the GI-1 group (P=0.005, supplementary table 2). No
differences in TNM stage or grade of differentiation were observed between both
groups. GI-HL esophageal cancers were treated less frequently with radiotherapy
(20% vs. 40% in GI-1, P=0.03) and chemotherapy (13% vs. 43%, P=0.001) or
treatments that included radiotherapy and/or chemotherapy (27% vs. 57%,
P=0.002). Overall survival was not significantly different in GI-HL esophageal cancer
patients compared with GI-1 patients (HR 1.20 (95% CI 0.79-1.85) P=0.41, figure 2,
table 2). Cumulative disease-specific mortality was high (79% in GI-HL and 74% in
GI-1 patients at 5 years) and did not differ between GI-HL and GI-1 patients (HR
1.17 (95% CI 0.75-1.84) P=0.49). When tumor and treatment characteristics were
added to the model, the survival difference between GI-HL and GI-1 patients
remained (not exceeding a 10% reduction in HR, supplementary table 3, 4).

Tabl
e 2.
Ove
rall
surv
ival
of g
astr
oint
estin
al c
ance
r in
Hod
gkin
lym
phom
a su
rviv
ors
com
pare
d w
ith fi
rst p
rimar
y ga
stro
inte
stin
al
canc
er p
atie
nts.
Abbr
evia
tions
: GI-H
L, g
astr
oint
estin
al c
ance
r in
Hod
gkin
lym
phom
a su
rviv
ors;
GI-1
, firs
t prim
ary
gast
roin
test
inal
can
cer p
atie
nts;
H
R, h
azar
d ra
tio; 9
5% C
I, 95
% c
onfid
ence
inte
rval
. *
Cox
prop
ortio
nal h
azar
ds re
gres
sion
mod
el a
djus
ted
for d
icho
tom
ized
var
iabl
es T
NM
sta
ge (I
/II v
s. II
I/IV)
, gra
de o
f di
ffere
ntia
tion
(wel
l/mod
erat
e vs
. poo
r/un
diffe
rent
iate
d) a
nd tu
mor
loca
tion
(eso
phag
us/s
tom
ach
vs. s
mal
l in
test
ine/
colo
rect
um).
†
Cox
prop
ortio
nal h
azar
ds re
gres
sion
mod
el a
djus
ted
for s
urge
ry, r
adio
ther
apy,
che
mot
hera
py.
‡ Co
x pr
opor
tiona
l haz
ards
regr
essio
n m
odel
adj
uste
d fo
r dic
hoto
miz
ed v
aria
bles
TN
M s
tage
, gra
de o
f diff
eren
tiatio
n su
rger
y,
radi
othe
rapy
, che
mot
hera
py.
$ Co
x pr
opor
tiona
l haz
ards
regr
essio
n m
odel
adj
uste
d fo
r tum
or su
bsite
: eso
phag
eal c
ance
r: u
pper
vs.
oth
er, g
astr
ic:
antr
um/p
ylor
us v
s. o
ther
, col
orec
tal c
ance
r: co
lon
vs. r
ectu
m.
Cha
ract
erist
ic
Gas
troi
ntes
tinal
can
cer
Esop
hage
al c
ance
r G
astr
ic c
ance
r Co
lore
ctal
can
cer
GI-H
L (n
=92)
%
(95%
CI)
GI-1
(n=9
11)
% (9
5% C
I) G
I-HL
(n=2
5)
% (9
5% C
I) G
I-1 (n
=243
) %
(95%
CI)
GI-H
L (n
=31)
%
(95%
CI)
GI-1
(n=3
08)
% (9
5% C
I) G
I-HL
(n=3
4)
% (9
5% C
I) G
I-1 (n
=340
) %
(95%
CI)
5-ye
ar s
urvi
val
28 (1
8-37
) 37
(34-
40)
12 (0
-25)
21
(16-
27)
13 (1
-26)
26
(21-
31)
50 (3
3-67
) 57
(52-
63)
10-y
ear s
urvi
val
18 (1
0-27
) 30
(27-
33)
6 (0
-16)
18
(13-
23)
7 (0
-16)
21
(17-
26)
37 (2
0-53
) 46
(40-
51)
15-y
ear s
urvi
val
15 (7
-23)
28
(25-
31)
6 (0
-16)
16
(12-
21)
7 (0
-16)
21
(16-
26)
27 (1
0-44
) 41
(36-
47)
G
I-HL
vs. G
I-1 (r
ef)
HR (9
5% C
I) P
valu
e HR
(95%
CI)
P va
lue
HR (9
5% C
I) P
valu
e HR
(95%
CI)
P va
lue
Uni
varia
ble
1.30
(1.0
3-1.
65)
0.03
1.
20 (0
.79-
1.85
) 0.
41
1.33
(0.9
1-1.
96)
0.15
1.
36 (0
.90-
2.06
) 0.
15
Mul
tivar
iabl
e, in
clud
ing
Tum
or c
hara
cter
istic
s* 1.
39 (1
.10-
1.76
) 0.
006
Trea
tmen
t cha
ract
erist
ics†
1.32
(1.0
4-1.
68)
0.02
Tu
mor
+ tr
eatm
ent‡
1.33
(1.0
5-1.
68)
0.02
Tu
mor
sub
site$
1.15
(0.7
4-1.
79)
0.54
1.
71 (1
.14-
2.55
) 0.
009
1.29
(0.8
5-1.
96)
0.24

56 Chapter 3
Figure 3. Subsite of gastrointestinal cancer in Hodgkin lymphoma survivors and first primary gastrointestinal cancer patients.
Both mid esophagus and stomach body contain overlapping or unspecified locations. Abbreviations: GI-HL, gastrointestinal cancer in Hodgkin lymphoma survivors; GI-1, first primary gastrointestinal cancer patients. * P=0.01 ** P<0.001 † including cecum, ascending, descending, sigmoid, overlapping, colon not otherwise specified (transverse colon includes the hepatic and splenic flexure).

Tabl
e 3.
Cau
se-s
peci
fic c
umul
ativ
e m
orta
lity
from
gas
troi
ntes
tinal
can
cer i
n H
odgk
in ly
mph
oma
surv
ivor
s an
d fir
st p
rimar
y ga
stro
inte
stin
al c
ance
r pat
ient
s.
Cum
ulat
ive
mor
talit
y w
as c
alcu
late
d us
ing
com
petin
g ris
k an
alys
es. A
bbre
viat
ions
: GI-H
L, g
astr
oint
estin
al c
ance
r in
Hod
gkin
lym
phom
a su
rviv
ors;
GI-1
, firs
t pr
imar
y ga
stro
inte
stin
al c
ance
r pat
ient
s; H
R, h
azar
d ra
tio; 9
5% C
I, 95
% c
onfid
ence
inte
rval
. *
Cox
prop
ortio
nal h
azar
ds re
gres
sion
mod
el a
djus
ted
for s
urge
ry, r
adio
ther
apy,
che
mot
hera
py.
† Co
x pr
opor
tiona
l haz
ards
regr
essio
n m
odel
adj
uste
d fo
r dic
hoto
miz
ed v
aria
bles
TN
M s
tage
, gra
de o
f diff
eren
tiatio
n, su
rger
y, ra
diot
hera
py, c
hem
othe
rapy
. ‡
Cox
prop
ortio
nal h
azar
ds re
gres
sion
mod
el a
djus
ted
for t
umor
subs
ite: e
soph
agea
l can
cer:
uppe
r vs.
oth
er, g
astr
ic: a
ntru
m/p
ylor
us v
s. o
ther
, col
orec
tal
canc
er: c
olon
vs.
rect
um.
Cum
ulat
ive
mor
talit
y
G
astr
oint
estin
al c
ance
r Es
opha
geal
can
cer
Gas
tric
can
cer
Colo
rect
al c
ance
r G
I-HL
(n=9
2)
% (9
5% C
I) G
I-1 (n
=911
) %
(95%
CI)
GI-H
L (n
=25)
%
(95%
CI)
GI-1
(n=2
43)
% (9
5% C
I) G
I-HL
(n=3
1)
% (9
5% C
I) G
I-1 (n
=308
) %
(95%
CI)
GI-H
L (n
=34)
%
(95%
CI)
GI-1
(n=3
40)
% (9
5% C
I) 5-
year
mor
talit
y G
I can
cer
Oth
er c
ause
s of
dea
th
66 (5
5-75
) 7
(3-1
3)
56 (5
3-59
) 7
(6-9
) 79
(57-
91)
8 (1
-23)
74
(68-
79)
5 (3
-8)
81 (6
2-91
) 6
(1-1
9)
65 (5
9-70
) 9
(6-1
3)
44 (2
7-60
) 6
(1-1
7)
35 (3
0-41
) 7
(5-1
0)
10-y
ear
mor
talit
y G
I can
cer
Oth
er c
ause
s of
dea
th
72 (6
2-80
) 9
(4-1
7)
61 (5
7-64
) 10
(8-1
2)
85 (6
2-95
) 8
(1-2
3)
76 (7
0-81
) 7
(4-1
0)
87 (6
9-95
) 6
(1-1
9)
69 (6
3-74
) 10
(9-1
4)
50 (3
3-66
) 13
(4-2
7)
42 (3
7-48
) 12
(9-1
6)
15-y
ear
mor
talit
y G
I can
cer
Oth
er c
ause
s of
dea
th
72 (6
2-80
) 13
(7-2
2)
61 (5
8-65
) 11
(9-1
3)
85 (6
2-95
) 8
(1-2
3)
76 (7
0-81
) 8
(5-1
2)
87 (6
9-95
) 6
(1-1
9)
69 (6
3-74
) 10
(9-1
4)
50 (3
3-66
) 22
(9-4
0)
45 (3
9-50
) 14
(10-
18)
Di
seas
e-sp
ecifi
c
GI-H
L vs
. GI-1
(ref
) HR
* (9
5% C
I) P
valu
e HR
* (9
5% C
I) P
valu
e HR
* (9
5% C
I) P
valu
e HR
† (95%
CI)
P va
lue
Uni
varia
ble
1.29
(1.0
0-1.
67)
0.04
9 1.
17 (0
.75-
1.84
) 0.
49
1.43
(0.9
5-2.
13)
0.08
1.
27 (0
.77-
2.10
) 0.
35
Mul
tivar
iabl
e, in
clud
ing
Trea
tmen
t cha
ract
erist
ics*
1.33
(1.0
3-1.
72)
0.03
Tu
mor
+ tr
eatm
ent†
1.33
(1.0
3-1.
72)
0.03
Tu
mor
sub
site‡
1.11
(0.7
0-1.
76)
0.67
1.
80 (1
.19-
2.74
) 0.
006
1.11
(0.6
6-1.
86)
0.70
O
ther
cau
ses o
f dea
th
Uni
varia
ble
1.44
(0.8
1-2.
56)
0.22
1.
60 (0
.36-
7.06
) 0.
53
1.02
(0.3
1-3.
34)
0.97
1.
61 (0
.76-
3.38
) 0.
21

58 Chapter 3
Gastric cancer characteristics and survival GI-HL gastric cancers were more frequently located in the antrum or pylorus (41%
vs. 20% in GI-1) and less frequently in the cardia or fundus (18% vs. 31% in GI-1,
P=0.01, figure 3). Treatment with surgery alone was more frequent in HL-GI
patients than in GI-1 patients (59% vs. 37%, P=0.02), and treatment that included
at least radiotherapy or chemotherapy was less frequently given (24% vs. 43%,
P=0.04, supplementary table 2).
There was a trend towards worse overall and disease-specific survival in GI-HL
gastric cancer patients compared with GI-1 patients (HR 1.33 (95% CI 0.91-1.96)
P=0.15 and HR 1.43 (95% CI 0.95-2.13) P=0.08, respectively, figure 2, table 2 and
3). In multivariable models that included TNM stage, tumor subsite (cardia/body vs.
antrum/pylorus) or surgery, the overall and disease-specific survival difference
between GI-HL gastric cancer patients and GI-1 patients substantially increased
(defined as a >10% change in HR of the grouping variable GI-HL vs. GI-1 patients;
disease-specific survival adjusted for subsite, HR 1.80 (95% CI 1.19-2.74) P=0.006;
adjusted for stage, HR 1.66 (95% CI 1.11-2.49) P=0.01; adjusted for surgery, HR
2.00 (95% CI 1.33-3.01) P=0.001, supplementary table 3, 4). None of the evaluated
characteristics decreased the survival difference, so none of these characteristics
could explain the observed difference in survival.
Colorectal cancer characteristics and survival GI-HL colorectal cancers were more frequently located in the transverse colon and
less frequently in the rectum compared with GI-1 colorectal cancers (34% and 11%
vs. 9% and 32%, respectively, P<0.001, figure 3). It is likely that (partly) due to this
difference in rectal cancer frequency, a difference in treatment with radiotherapy
was present between GI-HL and GI-1 patients (5% vs. 26%, P=0.004, supplementary
table 2). No further differences in TNM stage, surgery or chemotherapy were
present between groups.
Overall and disease-specific survival were not significantly different when
comparing GI-HL patients with GI-1 patients (HR 1.36 (95% CI 0.90-2.06) P=0.15
and HR 1.27 (95% CI 0.77-2.10) P=0.35, respectively). In a multivariable model,

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 59
3
tumor location was the only characteristic that decreased any possible difference
in survival. After adjustment for location either in colon or rectum, disease-specific
survival differences between GI-HL patients and GI-1 patients became substantially
smaller (HR 1.11 (0.66-1.86) P=0.70, supplementary table 3, 4).
Discussion
Our study is the first to demonstrate both a worse overall survival and disease-
specific survival of GI-HL patients compared with survival of GI-1 patients. The
survival difference was small and appeared largest for gastric cancer patients and
smallest for colorectal cancer patients. Although some differences in GI tumor
characteristics and treatment were present between GI-HL patients and GI-1
patients, none of these characteristics offered sufficient explanation for the
survival differences. Although mortality from other causes was not significantly
higher in GI-HL patients, a higher rate of morbidity may have influenced the
efficacy of GI-HL treatment. In addition to HL-related comorbidities, a different
pathogenesis of therapy-related gastrointestinal cancer may also affect the efficacy
of GI-HL treatment, resulting in worse survival.
A difference in carcinogenesis has been suggested only for therapy-related
colorectal cancer diagnosed in HL survivors, as these tumors are more frequently
microsatellite instable. 16 This high frequency of microsatellite instability is not
caused by promoter hypermethylation of the mismatch repair gene MLH1, which is
common in the general population, but by somatic mutations in mismatch repair
genes. In therapy-related esophageal cancer compared with sporadic cancer, no
difference in frequency of microsatellite instability or loss of heterozygosity was
found. 14 To our knowledge, no data are available for therapy-related gastric cancer
and therapy-related small bowel cancer.
A second important finding of our study is that GI-HL patients were treated
differently compared with GI-1 patients. GI-HL patients were more frequently
treated with surgery alone, and combined modality treatments were less
frequently given. Probably due to prior HL treatment, radiotherapy and
chemotherapy are given less frequently for GI-HL patients, either as a result of

60 Chapter 3
dosage limitations or comorbidity. 17, 18 Additionally, the differences in treatment
may partially result from the distribution of GI cancer subsites in GI-HL patients, as
these were less frequently located in the rectum. Previous studies also reported
that therapy-related GI cancers are more frequently located within irradiation
fields. 12, 15, 19 Surprisingly, the observed treatment differences did not explain the
worse survival. The limited treatment regimens for GI cancer in HL survivors may
therefore perform better than expected. Unfortunately, we did not have detailed
data on GI cancer treatment regimens (e.g. sequences of treatment, type of
chemotherapy).
The only previous, comparable study performed used a similar study design but
had somewhat different results. 15 They found a worse overall survival for HL
survivors with TNM stage I gastric cancer (N=8) and with TNM stage IIB-IV
colorectal cancer (N=70) compared with a significantly older population cohort
with these GI cancers. This study did not show a difference in overall survival for
other stage subgroups or in disease-specific survival. In addition, our methods of
patient selection differed from Youn et al. As GI-HL cancer is diagnosed at a
relatively young age, we deliberately generated our population-based comparison
cohort with primary GI cancers by matching on age at diagnosis, and additionally
on year of diagnosis and gender. We excluded GI-HL patients with a second
malignancy between HL and GI-HL from survival analyses to increase comparability
with the GI-1 population. This selection method may have caused a decrease in
mortality from other causes in the GI-HL population, resulting in a more
comparable mortality from non-GI-cancer-related causes for GI-HL patients and GI-
1 patients. In a study on breast cancer survival in HL survivors, in which patients
with another second malignancy diagnosed between HL and breast cancer were
not excluded, mortality from other causes was indeed higher in HL survivors with
breast cancer than in first primary breast cancer patients. 20 In our study, the
likelihood of detecting a difference in mortality from other causes was small, as
mortality from GI cancer was high and the number of patients was relatively low. 21
The selection procedure of the population-based controls is one of the strengths of
this study. Also, this is the first study with sufficient and long-term follow-up data

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 61
3
to demonstrate a worse overall and disease-specific survival in patients who
survived HL and developed GI cancer, and to provide data that excluded several
possible etiologic factors.
The survival differences were, however, not large and the power was insufficient to
confirm differences in survival between GI-HL and GI-1 patients for GI cancer
subsites, or for specific HL treatment exposure subgroups (as the majority received
combination treatments for HL, which limits statistical power). An additional
limitation was the absence of information on other factors associated with GI
cancer risk, such as family history and obesity.
As HL survivors have an increased incidence of GI malignancies, and a slightly
worse survival, treating physicians should focus on GI cancer awareness and
prevention. Personalized surveillance programs should be developed for this
purpose. Our research group is currently performing a multicenter cohort study on
a first surveillance colonoscopy in HL survivors. (Dutch Trial Registry NTR4961)
Additionally, further research is necessary to evaluate therapy-related GI
carcinogenesis, as differences compared with sporadic carcinogenesis may have
consequences for the clinical approach, such as surveillance technique and
interval.
In current clinical practice, decision-making about curative HL treatment involves
the balance of disease control and the risk of long-term side effects. Due to the
increased gastrointestinal cancer risk associated with radiotherapy and
procarbazine, and the associated increased mortality from gastrointestinal cancer,
the indication for the BEACOPP regimen should involve careful consideration and
radiation fields should be limited. 22
In conclusion, overall and disease-specific survival of GI cancer patients is slightly
worse in HL survivors compared with first primary GI cancer patients. This
difference is most clear in gastric cancer patients. Differences in tumor stage,
grade of differentiation, treatment, or mortality from other causes could not
explain the worse survival of GI cancer in HL survivors. As such, this may be
explained by a worse treatment response due to HL-related comorbidities or due
to a different pathogenesis of therapy-related gastrointestinal cancer.

62 Chapter 3
Acknowledgements
We would like to acknowledge the Netherlands Cancer Registry and Statistics
Netherlands (CBS) for the collaboration. In addition, we thank Mette van
Ramshorst and Lotte Elshof for their assistance with Cox proportional hazards
regression models and competing risk models.

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 63
3
References 1. Schaapveld M, Aleman BM, van Eggermond AM, et al. Second Cancer Risk
Up to 40 Years after Treatment for Hodgkin's Lymphoma. N Engl J Med
2015;373:2499-511.
2. Hodgson DC, Gilbert ES, Dores GM, et al. Long-term solid cancer risk
among 5-year survivors of Hodgkin's lymphoma. J Clin Oncol 2007;25:1489-
97.
3. Swerdlow AJ, Higgins CD, Smith P, et al. Second cancer risk after
chemotherapy for Hodgkin's lymphoma: a collaborative British cohort
study. J Clin Oncol 2011;29:4096-104.
4. Ng AK, Bernardo MV, Weller E, et al. Second malignancy after Hodgkin
disease treated with radiation therapy with or without chemotherapy:
long-term risks and risk factors. Blood 2002;100:1989-96.
5. Aleman BM, van den Belt-Dusebout AW, Klokman WJ, et al. Long-term
cause-specific mortality of patients treated for Hodgkin's disease. J Clin
Oncol 2003;21:3431-9.
6. Ng AK, Bernardo MP, Weller E, et al. Long-term survival and competing
causes of death in patients with early-stage Hodgkin's disease treated at
age 50 or younger. J Clin Oncol 2002;20:2101-8.
7. Nottage K, McFarlane J, Krasin MJ, et al. Secondary colorectal carcinoma
after childhood cancer. J Clin Oncol 2012;30:2552-8.
8. Morton LM, Dores GM, Curtis RE, et al. Stomach cancer risk after
treatment for hodgkin lymphoma. J Clin Oncol 2013;31:3369-77.
9. Henderson TO, Oeffinger KC, Whitton J, et al. Secondary gastrointestinal
cancer in childhood cancer survivors: a cohort study. Ann Intern Med
2012;156:757-66, W-260.
10. Dores GM, Metayer C, Curtis RE, et al. Second malignant neoplasms among
long-term survivors of Hodgkin's disease: a population-based evaluation
over 25 years. J Clin Oncol 2002;20:3484-94.

64 Chapter 3
11. Tukenova M, Diallo I, Anderson H, et al. Second malignant neoplasms in
digestive organs after childhood cancer: a cohort-nested case-control
study. Int J Radiat Oncol Biol Phys 2012;82:e383-90.
12. van den Belt-Dusebout AW, Aleman BM, Besseling G, et al. Roles of
radiation dose and chemotherapy in the etiology of stomach cancer as a
second malignancy. Int J Radiat Oncol Biol Phys 2009;75:1420-9.
13. Morton LM, Gilbert ES, Stovall M, et al. Risk of esophageal cancer following
radiotherapy for Hodgkin lymphoma. Haematologica 2014;99:e193-6.
14. Boldrin E, Rumiato E, Fassan M, et al. Genetic features of metachronous
esophageal cancer developed in Hodgkin's lymphoma or breast cancer
long-term survivors: an exploratory study. PLoS One 2015;10:e0117070.
15. Youn P, Li H, Milano MT, et al. Long-term survival among Hodgkin's
lymphoma patients with gastrointestinal cancer: a population-based study.
Ann Oncol 2013;24:202-8.
16. Rigter LS, Snaebjornsson P, Rosenberg EH, et al. Double somatic mutations
in mismatch repair genes are frequent in colorectal cancer after Hodgkin’s
lymphoma treatment. Gut 2016; Published Online First DOI 10.1136/gutjnl-
2016-312608.
17. van Eggermond AM, Schaapveld M, Lugtenburg PJ, et al. Risk of multiple
primary malignancies following treatment of Hodgkin lymphoma. Blood
2014;124:319-27.
18. Bhakta N, Liu Q, Yeo F, et al. Cumulative burden of cardiovascular
morbidity in paediatric, adolescent, and young adult survivors of Hodgkin's
lymphoma: an analysis from the St Jude Lifetime Cohort Study. Lancet
Oncol 2016;17:1325-34.
19. Hauptmann M, Fossa SD, Stovall M, et al. Increased stomach cancer risk
following radiotherapy for testicular cancer. Br J Cancer 2015;112:44-51.
20. Milano MT, Li H, Gail MH, et al. Long-term survival among patients with
Hodgkin's lymphoma who developed breast cancer: a population-based
study. J Clin Oncol 2010;28:5088-96.

Survival of gastrointestinal cancer in Hodgkin lymphoma survivors 65
3
21. Bhuller KS, Zhang Y, Li D, et al. Late mortality, secondary malignancy and
hospitalisation in teenage and young adult survivors of Hodgkin lymphoma:
report of the Childhood/Adolescent/Young Adult Cancer Survivors
Research Program and the BC Cancer Agency Centre for Lymphoid Cancer.
Br J Haematol 2016;172:757-68.
22. Jiang Y, Chen Y, Huang R, et al. Comparison of the efficiency of ABVD
versus BEACOPP for Hodgkin lymphoma treatment: a meta-analysis. Int J
Hematol 2016;104:413-9.

66 Chapter 3
Supplements Supplementary table 1. Hodgkin lymphoma patient characteristics.
HL characteristic GI-HL n (N=104)*
Esophagus n (N=30)
Gastric n (N=34)
CRC n (N=38)
Age of HL diagnosis
Median (interquartile range) 30 (22-41) 31 (25-39) 26 (21-36) 30 (22-45) Treatment period 1966-1979 1980-1989 1990-2000
44 33 27
11 12
7
11 11 12
22
9 7
HL radiotherapy (RT)
No RT 6 3 1 2
Mantle field only 31 14 6 10
Mantle field + infradiaphragmatic RT 51 12 24 15
Infradiaphragmatic RT only 11 0 1 9
Yes, field unknown 5 1 2 2
HL chemotherapy (CT)
No CT 43 13 17 13
CT, no procarbazine 12 4 1 7
Procarbazine-containing CT 41 10 15 14
Yes, type of CT unknown 8 3 1 4
HL recurrence 43 13 16 14 Second non-gastrointestinal cancer diagnoses in HL survivors †
Oropharynx 3 2 0 1
Lung 1 1 0 0
Breast 4 1 2 1
Lymphoma (NOS) 2 1 1 0
Cervix 1 0 0 1
Connective/soft tissue (NOS) 1 0 0 1
Abbreviations: HL, Hodgkin lymphoma; RT, radiotherapy; CT, chemotherapy; NOS, not otherwise specified. * including two HL patients with a small intestinal cancer. † GI-HL is the third cancer, excluded from extensive survival analyses.

Supp
lem
enta
ry ta
ble
2. C
hara
cter
istic
s of
gas
troi
ntes
tinal
can
cer s
ubsit
es in
Hod
gkin
lym
phom
a su
rviv
ors
and
first
prim
ary
gast
roin
test
inal
can
cer p
atie
nts.
Abbr
evia
tions
: GI-H
L, g
astr
oint
estin
al c
ance
r in
Hod
gkin
lym
phom
a su
rviv
ors;
GI-1
, firs
t prim
ary
gast
roin
test
inal
can
cer p
atie
nts;
RT,
radi
othe
rapy
; CT,
ch
emot
hera
py.
* de
fined
as
neur
oend
ocrin
e ca
rcin
omas
, lar
ge c
ell c
arci
nom
as, u
ndiff
eren
tiate
d ca
rcin
omas
, ana
plas
tic c
arci
nom
as o
r uns
peci
fied
carc
inom
as.
GI c
ance
r cha
ract
erist
ic
Esop
hage
al c
ance
r G
astr
ic c
ance
r Co
lore
ctal
can
cer
G
I-HL
(N
=30)
G
I-1
(N=2
87)
GI-H
L
(N=3
4)
GI-1
(N
=338
) G
I-HL
(N
=38)
G
I-1
(N=3
80)
n
(%)
n (%
) P
valu
e n
(%)
n (%
) P
valu
e n
(%)
n (%
) P
valu
e Ag
e M
edia
n (IQ
R)
54 (4
5-59
) 54
(46-
59)
0.67
46
(36-
55)
47 (3
6-54
) 0.
98
56 (4
9-61
) 56
(49-
61)
1.00
G
ende
r
Mal
e 18
(6
0)
180
(63)
0.
77
22
(65)
21
8 (6
4)
1.00
29
(7
6)
290
(76)
1.
00
Fem
ale
12
(40)
10
7 (3
7)
12
(3
5)
120
(36)
9 (2
4)
90
(24)
Mor
phol
ogy
cate
gory
Aden
ocar
cino
ma
10
(33)
16
7 (5
8)
0.00
5 32
(9
4)
335
(99)
0.
07
38
(100
) 37
8 (1
00)
0.65
Sq
uam
ous
cell
carc
inom
a 17
(5
7)
115
(40)
1 (3
) 2
(1)
-
- -
-
Oth
er c
arci
nom
a*
3 (1
0)
5 (2
)
1 (3
) 1
(<1)
0 (0
) 2
(<1)
TNM
Sta
ge
I/I
I 6
(20)
61
(2
1)
0.23
13
(3
8)
99
(29)
0.
52
16
(42)
16
3 (4
3)
0.11
III
/IV
20
(67)
19
5 (6
8)
19
(5
6)
218
(64)
21
(55)
21
1 (5
6)
U
nkno
wn
4 (1
3)
31
(11)
2 (6
) 21
(6
)
1 (3
) 6
(2)
G
rade
of d
iffer
entia
tion
W
ell /
low
gra
de
0 (0
) 10
(4
) 0.
21
1 (3
) 4
(1)
0.02
7
(18)
21
(6
) 0.
04
Mod
erat
e / i
nter
med
iate
10
(3
3)
78
(27)
6 (1
8)
53
(16)
18
(47)
20
4 (5
4)
Po
or /
high
6
(20)
10
4 (3
6)
11
(3
2)
171
(51)
5 (1
3)
55
(14)
Und
iffer
entia
ted
/ ana
plas
tic
1 (3
) 4
(1)
3
(9)
5 (1
)
0 (0
) 1
(<1)
Unk
now
n 13
(4
3)
91
(32)
13
(38)
10
5 (3
1)
8
(21)
99
(2
6)
Tr
eatm
ent c
ateg
ory
N
o tr
eatm
ent
10
(33)
65
(2
3)
0.01
5 6
(18)
69
(2
0)
0.05
4 2
(5)
16
(4)
0.39
Su
rger
y on
ly
12
(40)
59
(2
1)
20
(5
9)
125
(37)
18
(47)
15
4 (4
1)
Su
rger
y &
RT
and/
or C
T 2
(7)
49
(17)
1 (3
) 51
(1
5)
13
(3
4)
177
(47)
RT a
nd/o
r CT
only
6
(20)
11
4 (4
0)
7
(21)
93
(2
8)
5
(13)
33
(9
)

Supp
lem
enta
ry ta
ble
3. Im
pact
of p
atie
nt a
nd tu
mor
cha
ract
erist
ics
on o
vera
ll su
rviv
al d
iffer
ence
of g
astr
oint
estin
al c
ance
r in
Hod
gkin
lym
phom
a su
rviv
ors
(GI-H
L) a
nd fi
rst p
rimar
y ga
stro
inte
stin
al c
ance
r pat
ient
s (G
I-1).
Impa
ct o
f oth
er fa
ctor
s on
HR
for G
I-HL
vs. G
I-1 (r
ef),
indi
cate
d in
bol
d in
cas
e of
a >
10%
cha
nge.
Ab
brev
iatio
ns: G
I-HL,
gas
troi
ntes
tinal
can
cer i
n H
odgk
in ly
mph
oma
surv
ivor
s; G
I-1, f
irst p
rimar
y ga
stro
inte
stin
al c
ance
r pat
ient
s; H
R, h
azar
d ra
tio; 9
5% C
I, 95
% c
onfid
ence
inte
rval
; AC,
ade
noca
rcin
oma;
SCC
, squ
amou
s ce
ll ca
rcin
oma.
*
Wel
l-mod
erat
e vs
. poo
r-un
diffe
rent
iate
d.
† G
astr
oint
esna
l can
cer:
esop
hagu
s/ga
stric
vs.
sm
all b
owel
/col
orec
tum
, eso
phag
eal c
ance
r: up
per v
s. o
ther
, gas
tric
: ant
rum
/pyl
orus
vs.
oth
er, c
olor
ecta
l ca
ncer
: col
on v
s. re
ctum
.
Cha
ract
erist
ic
Gas
troi
ntes
tinal
can
cer
HR fo
r GI-H
L vs
. GI-1
(ref
) HR
95%
CI
P
valu
e
Esop
hage
al c
ance
r HR
for
GI-H
L vs
. GI-1
(ref
) H
R
95
% C
I
P va
lue
Gas
tric
can
cer
HR f
or G
I-HL
vs. G
I-1 (r
ef)
HR
9
5% C
I
P va
lue
Colo
rect
al c
ance
r HR
for
GI-H
L vs
. GI-1
(ref
) H
R
95%
CI
P
valu
e U
niva
riabl
e 1.
30
1.03
-1.6
5 0.
03
1.20
0.
79-1
.85
0.41
1.
33
0.91
-1.9
6 0.
15
1.36
0.
90-2
.06
0.15
Ad
ded
char
acte
ristic
Ye
ar o
f inc
iden
ce
1.30
1.
03-1
.64
0.03
1.
20
0.78
-1.8
5 0.
41
1.35
0.
92-1
.98
0.13
1.
34
0.88
-2.0
3 0.
17
Age
at d
iagn
osis
1.30
1.
03-1
.64
0.03
1.
18
0.77
-1.8
3 0.
45
1.37
0.
93-2
.01
0.12
1.
35
0.89
-2.0
4 0.
16
Gen
der m
ale
vs. f
emal
e 1.
30
1.03
-1.6
4 0.
03
1.21
0.
78-1
.86
0.40
1.
34
0.91
-1.9
7 0.
14
1.36
0.
90-2
.06
0.15
St
age
I/II
vs. I
II/IV
1.
38
1.09
-1.7
4 0.
008
1.14
0.
74-1
.75
0.57
1.
54
1.05
-2.2
8 0.
03
1.44
0.
95-2
.18
0.09
G
rade
of d
iffer
entia
tion*
1.
32
1.04
-1.6
7 0.
02
1.20
0.
78-1
.85
0.42
1.
34
0.91
-1.9
6 0.
14
1.47
0.
97-2
.24
0.07
Su
rger
y no
vs.
yes
1.
51
1.19
-1.9
1 0.
001
1.43
0.
93-2
.21
0.11
1.
86
1.26
-2.7
5 0.
002
1.35
0.
89-2
.05
0.16
RT
no
vs. y
es
1.24
0.
98-1
.58
0.07
1.
14
0.74
-1.7
7 0.
55
1.34
0.
91-1
.97
0.14
1.
23
0.81
-1.8
8 0.
33
CT n
o vs
. yes
1.
32
1.04
-1.6
7 0.
02
1.08
0.
70-1
.69
0.72
1.
40
0.95
-2.0
7 0.
09
1.38
0.
91-2
.09
0.13
Tu
mor
(sub
)site
† 1.
32
1.04
-1.6
7 0.
02
1.15
0.
74-1
.79
0.54
1.
71
1.14
-2.5
5 0.
009
1.29
0.
85-1
.96
0.24
M
orph
olog
y AC
vs.
SCC
1.11
0.
72-1
.73
0.63

Supp
lem
enta
ry ta
ble
4. Im
pact
of p
atie
nt a
nd tu
mor
cha
ract
erist
ics
on d
iseas
e-sp
ecifi
c su
rviv
al d
iffer
ence
of g
astr
oint
estin
al c
ance
r in
Hod
gkin
lym
phom
a su
rviv
ors
(GI-H
L) a
nd fi
rst p
rimar
y ga
stro
inte
stin
al c
ance
r pat
ient
s (G
I-1).
Char
acte
ristic
Gas
troi
ntes
tinal
can
cer
HR fo
r GI-H
L vs
. GI-1
(ref
) HR
95%
CI
P v
alue
Esop
hage
al c
ance
r HR
for G
I-HL
vs. G
I-1 (r
ef)
HR
95
% C
I
P va
lue
Gas
tric
can
cer
HR fo
r GI-H
L vs
. GI-1
(ref
) HR
95%
CI
P
valu
e
Colo
rect
al c
ance
r HR
for G
I-HL
vs. G
I-1 (r
ef)
HR
95
% C
I
P va
lue
Uni
varia
ble
1.29
1.
00-1
.67
0.04
9 1.
17
0.7
5-1.
84
0.49
1.
43
0.95
-2.1
3 0.
08
1.27
0.
77-2
.10
0.35
Ad
ded
char
acte
ristic
Ye
ar o
f inc
iden
ce
1.29
1.
00-1
.67
0.04
8 1.
17
0.7
5-1.
84
0.49
1.
44
0.97
-2.1
6 0.
07
1.26
0.
76-2
.09
0.36
Ag
e at
dia
gnos
is 1.
29
1.00
-1.6
7 0.
049
1.16
0
.74-
1.82
0.
53
1.46
0.
97-2
.18
0.07
1.
27
0.77
-2.0
9 0.
36
Gen
der m
ale
vs. f
emal
e 1.
29
1.00
-1.6
6 0.
053
1.17
0
.75-
1.85
0.
49
1.43
0.
96-2
.14
0.08
1.
27
0.77
-2.1
0 0.
36
Stag
e I/
II vs
. III/
IV
1.37
1.
06-1
.77
0.02
1.
10
0.7
0-1.
74
0.67
1.
66
1.11
-2.4
9 0.
01
1.38
0.
83-2
.28
0.21
G
rade
of d
iffer
entia
tion*
1.
31
1.01
-1.6
9 0.
04
1.17
0
.75-
1.84
0.
49
1.43
0.
96-2
.14
0.08
1.
36
0.82
-2.2
5 0.
24
Surg
ery
no v
s. y
es
1.52
1.
17-1
.96
0.00
1 1.
41
0.9
0-2.
22
0.14
2.
00
1.33
-3.0
1 0.
001
1.24
0.
75-2
.06
0.39
RT
no
vs.
yes
1.
24
0.96
-1.6
0 0.
11
1.13
0
.72-
1.79
0.
60
1.43
0.
95-2
.13
0.09
1.
13
0.68
-1.8
7 0.
64
CT n
o vs
. yes
1.
32
1.02
-1.7
1 0.
03
1.06
0
.67-
1.69
0.
80
1.52
1.
01-2
.28
0.04
5 1.
31
0.79
-2.1
6 0.
30
Tum
or (s
ub)s
ite†
1.30
1.
01-1
.68
0.04
1.
11
0.70
-1.7
6 0.
67
1.80
1.
19-2
.74
0.00
6 1.
11
0.66
-1.8
6 0.
70
Impa
ct o
f oth
er fa
ctor
s on
HR
for G
I-HL
vs. G
I-1 (r
ef),
indi
cate
d in
bol
d in
cas
e of
a >
10%
cha
nge.
Ab
brev
iatio
ns: G
I-HL,
gas
troi
ntes
tinal
can
cer i
n H
odgk
in ly
mph
oma
surv
ivor
s; G
I-1, f
irst p
rimar
y ga
stro
inte
stin
al c
ance
r pat
ient
s; H
R, h
azar
d ra
tio; 9
5% C
I, 95
% c
onfid
ence
inte
rval
. *
Wel
l-mod
erat
e vs
. poo
r-un
diffe
rent
iate
d.
† G
astr
oint
esna
l can
cer:
esop
hagu
s/ga
stric
vs.
sm
all b
owel
/col
orec
tum
, eso
phag
eal c
ance
r: up
per v
s. o
ther
, gas
tric
: ant
rum
/pyl
orus
vs.
oth
er, c
olor
ecta
l ca
ncer
: col
on v
s. re
ctum
.