Embed Size (px)
Citation preview
1
39th National Conference on Pediatric Health Care
©2018
March 19-22, 2018 CHICAGO
Developmental Delays and Behavioral Conditions in Young ChildrenSusan Van Cleve DNP, CPNP‐PC, PMHS, FAANP
Clinical Professor and PNP Director, University of Iowa College of Nursing, Iowa City, IA
PMHS, Pediatrics South, Pittsburgh, PA
©2018
Disclosures
• Consulting with Gene Foresight‐ no financial relationship
• Will be discussing off label use of medication
©2018
Learning Objectives
At the end of the session, the participant will be able to:
1. Describe signs and symptoms and developmental delays
2. Describe emotional and behavioral conditions in young children
3. Identify assessment process and screening tools that can be used to assist with diagnosis
4. Discuss treatment options for managing developmental delays and behavioral conditions in young children
©2018
Prevalence
• Estimates that 11‐20% of children 2‐5 year old children in US have a behavioral or emotional disorder
• 37‐39% of children will have an emotional or behavioral disorder by the age of 16
• Developmental and behavioral disorders now top 5 chronic conditions causing functional impairment in children
©2018
Risk for Behavioral and Emotional Conditions
• Economic disadvantage puts a child at risk due to increased exposure to environmental, familial, and psychosocial risks
• Recognition of greater risk for children who have Adverse Childhood Experiences including:
– emotional, physical and sexual abuse
– household challenges including mother treated violently, substance abuse in home, mental illness in home, parental separation or divorce, criminal in home
– physical or emotional neglect
©2018
The Effect of ACEs in Children
• ACEs in children include a range of experiences that can lead to trauma and toxic stress
• ACEs can impact children’s brain development and physical, social, mental, emotional, and behavioral health and well‐being
• There is growing evidence that it is the general experience of multiple ACEs, rather than the specific individual impact of any one experience, that matters

2
©2018
Effect of ACEs on Caregivers
• Found graded dose‐response relationship between ACEs and negative health and well‐being outcomes across the life course
• The higher the score the more likely to have adverse mental health and physical health outcomes in adulthood including alcoholism and alcohol abuse, COPD, depression, early initiation of smoking, early initiation of sexual activity, adolescent pregnancy, risk for sexual violence, poor academic achievement, suicide attempts, illicit drug use plus many more
©2018
Why is this important?
• Evidence supports that safe, stable, nurturing relationships have a significant protective effect on the intergenerational transmission of maltreatment, abuse, neglect
• Through early identification, we have an opportunity for early intervention and to provide trauma informed care to prevent the cycle of violence and promotion of health across the lifespan
• As part of every developmental and behavioral assessment and we must consider ACEs and the effect these experiences may be having on our patients
©2018
Young Children and Development
• Limitations using developmental screening, surveillance only model based on milestones
• Expand to understand the effect environment, social determinants have on infant and child mental health
• When considering developmental conditions, must also consider social and emotional health and child behavior
• Encourage NPs to be comprehensive when evaluating young children
©2018
Bright Futures, 4th Edition
• Bright Futures is a system of care designed to promote health and focus on child and family strengths and wellness
• Periodicity Schedule for well child care includes recommendations for screening, developmental assessment, assessment of social determinants of health, promoting strengths and protective factors‐ encourages this broader perspective in assessing and working with families
©2018
NP Role in Assessment for Developmental or Behavioral Conditions
• Comprehensive history including:
– Chief complaint
– Detailed health history (including parental and birth history)
–Medical conditions that could be causing delay or behavioral disorder (i.e. obstructive sleep apnea)
– Description of behavioral or developmental concerns; where and when behavior occurs, what works, what does not work
– Child’s temperament
©2018
Assessment
• Family medical and psychiatric history‐ ask about genetic or mental health conditions in addition to medical history
• Parenting style, parent child interactions, description of how parent views child
• Social history‐ home, child care, resources, neighborhood, social support. History of trauma, violence, addiction, abuse, criminal justice system involvement. Past and current involvement in protective services, other services
3
©2018
Assessment
• Comprehensive history for diet, elimination, sleep concerns‐level of functional impairment
• Evaluate for sensory impairment (hypersensitivity to light, sound, touch, smell, taste)
• Child’s strengths and weaknesses
• Child’s level of functioning home, community, school
©2018
Assessment
• Assess for child development include :
– Physical development (fine motor skills, gross motor skills)
– Cognitive development (intellectual abilities)
– Communication development (speech and language)
– Social or emotional development (social skills, emotional control, self regulation)
– Adaptive development (self‐care skills)
©2018
Physical Exam
• Complete physical exam
• Observe and interact with child‐observe child parent interactions
• Comprehensive neurological exam
–Disorders of tone, posture, persistence of primitive reflexes
–Abnormal DTR’s, asymmetries, gait abnormalities
– Tremors, soft neurological signs
–Performance of neurodevelopmental tasks‐ following directions, joint attention, attention span, language
©2018
Physical Exam
• Examine for dysmorphic features
• Facies‐ nose, philtrum, ears, lips
• Hands and feet‐ incurvature, webbing, palmar crease, clinodactyly, hyperextensibility or hypermobility of joints
• Growth parameters and body proportion‐head growth, trunk and limb size
• If find more than 2 dysmorphic features, consider genetic syndrome
©2018
American Academy of Pediatrics (AAP) Recommendations Developmental Screening
• Conduct developmental surveillance at every health supervision visit – Surveillance is flexible, longitudinal, continuous, and cumulative process ‐health care professionals identify children who may have developmental problems.
– There are 5 components of developmental surveillance: eliciting and attending to the parents' concerns about their child's development; documenting and maintaining a developmental history; making accurate observations of the child; identifying risk and protective factors; and maintaining an accurate record of documenting the process and findings.
©2018
AAP Recommendations Developmental Screening
• Conduct general developmental screening using evidence‐based tools at 9, 18, and 30 months, or whenever a concern is expressed
– Ages and Stages Questionnaire (ASQ‐3) $
– Parents Evaluation of Developmental Status (PEDS) $
4
©2018
AAP Recommendations Autism Specific Screening
• Autism‐specific screening is recommended at ages 18 and 24 months
–M‐CHAT‐R/F ‐16‐30 months‐ Free
– CSBS DP™ Infant‐Toddler Checklist‐ 6‐24 months‐Free
– Social Communication Questionnaire‐ 2 years and older $
©2018
AAP Recommendations Social‐Emotional Screening at Regular Intervals
• Social‐emo onal screening is recommended at regular intervals
– Achenbach System of Empirically Based Assessment 18‐60 months $
– Ages & Stages Questionnaire: Social‐Emotional (ASQ‐SE‐2) 3‐66 months $
– Brief Infant Toddler Social Emotional Assessment (BITSEA) 12‐36 months $
– Early Childhood Screening Assessment (ECSA) 18‐60 months‐ Free
– Pediatric Symptom Checklist (Baby & Preschool) 18‐60 months; Pediatric Symptom Checklist 4‐16 Years‐ Free
– Strengths and Difficulties Questionnaire 3‐16 Years‐ Free
©2018
AAP Recommenda ons Maternal Depression Screening
• Postpartum depression surveillance and screening at the 1‐, 2‐, 4‐, and 6‐month visits
– Edinburgh Postpartum Depression Scale (EPDS)‐ Free
– Patient Health Questionnaire‐2 (PHQ‐2); Patient Health Questionnaire‐9 (PHQ‐9)‐ Free
©2018
AAP Recommendations Social Determinants of Health Screening
• Surveillance for risk factors related to social determinants of health during all patient encounters. Ask family members questions about basic needs such as food, housing, and heat. –Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education Survey Instrument (WE CARE) Free
–Whole Child Assessment; Center for Youth Wellness ACE Questionnaire (CYW ACE‐Q) Free
• Assess Family Strengths– Integrate patient‐ and family‐centered care in practice, includes asking about and reinforcing family strengths.
©2018
Broad Screening Tools‐Young Children
• Strengths & Difficulties Questionnaire‐ 3‐16 years‐ screens for social‐emotional development and social determinants of health
• Survey of Wellbeing of Young Children screens for development, autism, social‐emotional development, maternal depression, social determinants of health‐ 1‐3 months, 4‐5 months, 6‐8 months, 9‐11 months, 12‐14 months, 15‐17 months, 18‐22 months, 23‐28 months, 29‐34 months, 35‐46 months, 47‐58 months, 59‐65 months
©2018
Screening Tools
• Tool should be highly validated, peer reviewed and nationally recognized
• Easy to use by parent and professionals
• Inexpensive
• Developmental and behavioral screening tools available at https://screeningtime.org/star‐center/#/screening‐tools
5
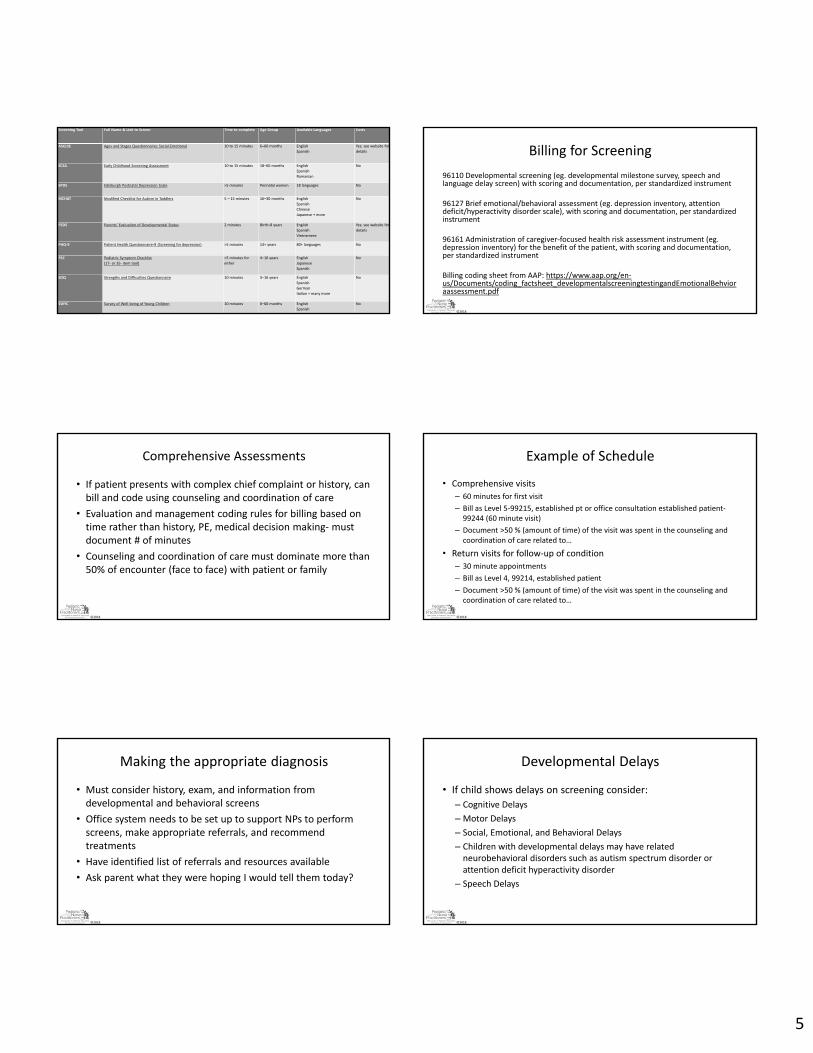
Screening Tool Full Name & Link to Screen Time to complete Age Group Available Languages Costs
ASQ:SE Ages and Stages Questionnaires Social‐Emotional 10 to 15 minutes 6–60 months English
Spanish
Yes; see website for
details
ECSA Early Childhood Screening Assessment 10 to 15 minutes 18–60 months English
Spanish
Romanian
No
EPDS Edinburgh Postnatal Depression Scale >5 minutes Perinatal women 18 languages No
MCHAT Modified Checklist for Autism in Toddlers 5 – 15 minutes 16–30 months English
Spanish
Chinese
Japanese + more
No
PEDS Parents’ Evaluation of Developmental Status 2 minutes Birth–8 years English
Spanish
Vietnamese
Yes; see website for
details
PHQ‐9 Patient Health Questionnaire‐9 (Screening for depression) >5 minutes 13+ years 80+ languages No
PSC Pediatric Symptom Checklist
(17‐ or 35‐ item tool)
>5 minutes for
either
4–16 years English
Japanese
Spanish
No
SDQ Strengths and Difficulties Questionnaire 10 minutes 3–16 years English
Spanish
German
Italian + many more
No
SWYC Survey of Well‐being of Young Children 10 minutes 0–60 months English
Spanish
No
©2018
Billing for Screening
96110 Developmental screening (eg. developmental milestone survey, speech and language delay screen) with scoring and documentation, per standardized instrument
96127 Brief emotional/behavioral assessment (eg. depression inventory, attention deficit/hyperactivity disorder scale), with scoring and documentation, per standardized instrument
96161 Administration of caregiver‐focused health risk assessment instrument (eg.depression inventory) for the benefit of the patient, with scoring and documentation, per standardized instrument
Billing coding sheet from AAP: https://www.aap.org/en‐us/Documents/coding_factsheet_developmentalscreeningtestingandEmotionalBehvioraassessment.pdf
©2018
Comprehensive Assessments
• If patient presents with complex chief complaint or history, can bill and code using counseling and coordination of care
• Evaluation and management coding rules for billing based on time rather than history, PE, medical decision making‐ must document # of minutes
• Counseling and coordination of care must dominate more than 50% of encounter (face to face) with patient or family
©2018
Example of Schedule
• Comprehensive visits
– 60 minutes for first visit
– Bill as Level 5‐99215, established pt or office consultation established patient‐99244 (60 minute visit)
– Document >50 % (amount of time) of the visit was spent in the counseling and coordination of care related to…
• Return visits for follow‐up of condition
– 30 minute appointments
– Bill as Level 4, 99214, established patient
– Document >50 % (amount of time) of the visit was spent in the counseling and coordination of care related to…
©2018
Making the appropriate diagnosis
• Must consider history, exam, and information from developmental and behavioral screens
• Office system needs to be set up to support NPs to perform screens, make appropriate referrals, and recommend treatments
• Have identified list of referrals and resources available
• Ask parent what they were hoping I would tell them today?
©2018
Developmental Delays
• If child shows delays on screening consider:
– Cognitive Delays
–Motor Delays
– Social, Emotional, and Behavioral Delays
– Children with developmental delays may have related neurobehavioral disorders such as autism spectrum disorder or attention deficit hyperactivity disorder
– Speech Delays
6
©2018
Developmental delays
• May be due to underlying medical conditions:
– Cerebral palsy
– Fetal alcohol spectrum disorders
– Landau‐Kleffner syndrome
–Myopathies, including muscular dystrophies
– Genetic disorders, such as Down syndrome and Fragile X syndrome
©2018
Definition of Developmental Delay
• Child delayed in some area of development, can be one or more areas
• Part C of IDEA broadly defines the term “developmental delay” • Term varies from state to state• Each state describes evaluation and assessment procedures• Each state specifies level of delay in functioning (or other comparable criteria) that constitutes developmental delay
• What’s your state’s definition? Early Childhood Technical Assistance Center at: http://www.nectac.org/~pdfs/topics/earlyid/partc_elig_table.pdf
©2018
Treatment for Developmental Delay
• Determined by what area is delayed
• May require referral to specialist, genetics, or further evaluation
• Refer to Early Intervention
• Need to follow closely
©2018
Early Intervention (EI) for Developmental Delay
• Mainstay of treatment, but underlying conditions leading to developmental delay need to be treated
• Early intervention services may include:– Speech and Language Therapy
– Occupational Therapy
– Physical Therapy
– Behavior Therapies, such as those used to treat autism and behavioral issues
• If qualifies for EI, a service coordinator will serve as single point of contact with the early intervention system
©2018
Individualized Family Service Plan (IFSP) 0‐3 years
• IFSP is a written document that outlines early intervention services the child and family will receive – usually in home
• Includes: – Child’s physical, cognitive, communication, social/emotional, and adaptive development
levels and needs– Family information, including the resources, priorities – Major results or outcomes expected to be achieved for child and family– Specific services child will be receiving– When/where in the natural environment (e.g., home, community) services will be
provided– Number of days or sessions for each service and how long each session will last– Who will pay for the services
• 45 days to complete the evaluation
©2018
Individualized Education Plan (IEP) 3‐21 years
• Individuals with Disabilities Education Act (IDEA) requires that public schools create an IEP for every child receiving special education services
• These services must be provided by school district from 3‐5 years
• IEP should address child’s learning issues, include specific educational goals
• Is legally binding document
• Should include: – Child’s present level of performance, annual educational goals
– Special education supports and services school will provide
– Modifications and accommodations the school will provide
– How and when the school will measure child’s progress toward annual goals
7
©2018
If Positive Behavioral or Social Emotional Screen
• Consider most common conditions
– ADHD
– Oppositional Defiant Disorder
– Autism Spectrum Disorder
– Anxiety, separation anxiety
– Post Traumatic Stress Disorder
©2018
DSM‐V Definition of ADHD Persistent pattern of inattention and/or hyperactivity‐impulsivity that interferes with functioning or development
In addition to meeting diagnostic criteria, the following conditions must be met:
1. Several inattentive or hyperactive‐impulsive symptoms were present before age 12 years.
2. Several symptoms are present in two or more setting, (e.g., at home, school or work; with friends or relatives; in other activities).
3. There is clear evidence that the symptoms interfere with, or reduce the quality of social, school, or work functioning.
4. The symptoms do not happen only during the course of schizophrenia or another psychotic disorder. The symptoms are not better explained by another mental disorder
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013.
©2018
Inattention
Six or more symptoms of inattention for children up to age 16, or five or more for adolescents 17 and older and adults; symptoms of inattention have been present for at least 6 months, and they are inappropriate for developmental level:
• Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or with other activities.
• Often has trouble holding attention on tasks or play activities.
• Often does not seem to listen when spoken to directly.
• Often does not follow through on instructions and fails to finish schoolwork, chores,
or duties in the workplace (e.g., loses focus, side‐tracked).
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013.
©2018
Inattention
• Often has trouble organizing tasks and activities.
• Often avoids, dislikes, or is reluctant to do tasks that require mental effort over a long period of time (such as schoolwork or homework).
• Often loses things necessary for tasks and activities (e.g. school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
• Is often easily distracted
• Is often forgetful in daily activities.
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013
©2018
Hyperactivity and Impulsivity
Six or more symptoms of hyperactivity‐impulsivity for children up to age 16, or five or more for adolescents 17 and older and adults; symptoms of hyperactivity‐impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for the person’s developmental level:
• Often fidgets with or taps hands or feet, or squirms in seat.
• Often leaves seat in situations when remaining seated is expected.
• Often runs about or climbs in situations where it is not appropriate (adolescents or adults may be limited to feeling restless).
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013.
©2018
Hyperactivity and Impulsivity
• Often unable to play or take part in leisure activities quietly.
• Is often "on the go" acting as if "driven by a motor".
• Often talks excessively.
• Often blurts out an answer before a question has been completed.
• Often has trouble waiting his/her turn.
• Often interrupts or intrudes on others (e.g., butts into conversations or games)
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA., American Psychiatric Association, 2013
8
©2018
ADHD Practice Guidelines
• American Academy of Pediatrics developed evidence based practice guidelines in October, 2011. http://pediatrics.aappublications.org/content/early/2011/10/14/peds.2011‐2654
• The AAP worked with the National Initiative for Children's Healthcare Quality (NICHQ) to develop the ADHD Toolkit for use by primary care providers. Available for download at: http://www.nichq.org/childrens‐health/adhd/resources/adhd‐toolkit
• AACAP Work Group on Quality Issues. (2007). Practice parameter for the assessment and treatment of children and adolescents with Attention Deficit/Hyperactivity Disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 894‐921.
©2018
NICHQ Vanderbilt Assessment Scales
• Developed for initial evaluation and follow‐up of ADHD in preschool and school age children (ages 6‐12) – Parent Initial and Follow‐up Scales– Teacher Initial and Follow‐up Scales– Available at: http://www.nichq.org/childrens‐health/adhd/resources/vanderbilt‐assessment‐scales
• Screens for coexisting conditions (conduct disorder, oppositional‐defiant disorder, anxiety/depression)
• ADHD diagnoses:– Predominately inattentive subtype– Predominately hyperactive/impulsive subtype– ADHD combined inattention/hyperactivity
©2018
ADHD Treatment Preschoolers
AAP Recommendations:
• Preschool aged children (4‐5 years): parent or teacher administered behavioral intervention should be the first line of treatment; medication (methylphenidate) may be considered if first line treatments are not available or insufficient
©2018
Behavioral/Psychosocial Interventions in Home
• Schedule/routine– Morning routine often difficult‐ develop a clear written or visual schedule– Irritability in the late afternoon, early evening
• Consistent rules (clear, brief) and expectations• Reward positive behavior, ignore negative behavior• Use incentives to get work done• <18 months, avoid use of screen media other than video‐chatting. Parents
of children 18 to 24 months of age choose high‐quality programming, and watch it with their children. Ages 2 to 5 years, limit screen use to 1 hour per day of high‐quality programs and co‐view media.
• Toddlers (1 to 3 years) & Pre‐schoolers (3 to 5 years)‐physically active every day for at least three hours, spread throughout the day
• Healthy eating and drinking, read books daily
©2018
ADHD Behavioral Interventions
• Parent training programs help parents:
Develop a positive relationship with their child
Teach them about how children develop
Help them manage negative behavior and increase positive behavior with positive discipline
• Parent training in effective child behavior management is essential
©2018
Parent Training for ADHD
• Recognizes that this disorder affects entire family, behavioral therapy involving all members of the household may restore balance
• Starts with parent understanding of ADHD as a neurophysiologic deficiency
• Evidence Based Programs include: New Forrest Therapy, Triple P, The Incredible Years Series, Parent Child Interactive Therapy (PCIT) https://childmind.org/article/choosing‐a‐parent‐training‐program/
9
©2018
FDA Approved Medications for ADHDMedication Indication FDA Approval and Age in
Years
Methylphenidate (stimulant) ADHD Yes > 6
Amphetamine (stimulant) ADHD Yes > 6 Can be used 3 on up
Guanfacine (alpha adrenergic agonist) Tenex, Intuniv
ADHD Yes > 6
Clonidine (alpha adrenergic agonist) Clonidine, Kapvay
ADHD Yes > 6
Atomoxetine (NRI) Strattera ADHD Yes > 6
©2018
Stimulants
• Common side effects: anorexia, weight loss or poor weight gain, delayed sleep onset, headache, stomachache, jitteriness or moodiness
• 15‐30% experience motor tics (may be transient)
• Basic principles in use of stimulants:
– Dosages are not weight dependent
– Start with low dose and titrate upward because of marked variability in response
– “Start low, go slow” particularly with younger children
©2018
Methylphenidate and Amphetamine
• Both approved for Rx of ADHD
• In general, dosing of amphetamines is one‐half of methylphenidate dosages
• No evidence of difference in advantages of different racemic mixtures (D‐verses DL‐)
• For preschool children, methylphenidate is recommended as the first line medication for ADHD after a 10 to 20 week trial of parent management training, parent child interactive therapy or both.
– PATS study used immediate release methylphenidate TID and found to be safe and effective in 3‐5 year olds
©2018
Immediate Release Methylphenidate Medications
• Methylphenidate
• Ritalin tablets‐ scored (5, 10 and 20 mg) Initial dose 5 mg BID
• Methylphenidate chewable (2.5, 5 and 10 mg tablets) Initial dose 5 mg BID
• Methylin solution (5 mg/5 ml or 10 mg/5ml) Initial dose 5 mg BID
• Focalin (dexmethylphenidate hydrochloride) tablets‐(2.5, 5 and 10 mg) Initial dose 2.5 mg BID
• Duration 3‐4 hours
©2018
Extended Release Methylphenidate Medications
• Methylphenidate ER capsules‐ 10, 20, 30, 40, 50 mg capsules‐ duration 8‐10 hours
• Concerta (Methylphenidate ER) capsules‐ noncrushable (18, 27, 36, 54, and 72 mg) Duration 9‐12 hrs
• Ritalin LA capsules‐ can be sprinkled (10, 20, 30 and 40, 60 mg) Duration 8 hrs
• Metadate ER tablets ( 10 and 20 mg) Duration 4‐8 hrs
• Metadate CD capsules (10, 20, 30, 40, 50, 60 mg) Duration 4‐8 hrs Can be sprinkled
• Focalin XR capsules (5, 10, 15, and 20, 25, 30, 35, 40 mg extended‐release) Duration‐ 6‐10 hours
©2018
Quillivant XR, Quillichew ER
• Methylphenidate hydrochloride for extended release oral suspension (after reconstitution with water): 25 mg per 5 mL (5 mg per mL)
• Quillichew 20, 30, 40 mg chewable tablets
• Recommended for patients 6 years and above, recommended starting dose is 20 mg given orally once daily in the morning
• Daily dosage above 60 mg is not recommended
• Shortage due to hurricane in Puerto Rico
10
©2018
Immediate Release Amphetamine
• Adderall tablets‐ scored (5, 7.5, 10, 12.5, 15, 20, and 30‐mg tablets)
• Approved 3‐5 year old, starting dose 2.5 mg QD
• Mixed salts of amphetamine (Dextroamphetamine/levoamphetamine)
• Duration‐ 4‐8 hours
©2018
Immediate Release Amphetamine • Zenzedi (d‐amphetamine sulfate)
– 3‐5 years 2.5 mg once daily
– 6‐17years 5‐40 mg BID
– Available in 2.5, 5, 7.5, 10, 15, 20 and 30 mg tablets
– 4‐8 hour effect
• ProCentra (d‐amphetamine sulfate)‐ liquid bubblegum flavor
– 3‐5 years 2.5 mg QD
– 6‐17 years 5‐40 mg BID
– 5 mg/5ml liquid
– <8 hour effect
©2018
Immediate Release Amphetamine
• Evekeo (amphetamine sulfate) Tablets: 5mg, 10mg, scored
• Not recommended for children under 3 years of age
• In children from 3 to 5 years of age, start with 2.5 mg daily; daily dosage may be raised in increments of 2.5 mg at weekly intervals until optimal response is obtained.
• In children 6 years of age or older, start with 5 mg once or twice daily
• Duration 4‐8 hours
©2018
Extended Release Amphetamines
• Adderall XR capsules‐can be sprinkled (5, 10, 15, 20, 25, and 30‐mg capsules)
–Mixed salts of amphetamine (Dextroamphetamine/levoamphetamine
– Duration‐ 8‐12 hours
• Dyanavel XR (Amphetamine extended release oral suspension 2.5 mg/ml)
– Duration‐ 8‐12 hours
©2018
Challenges in Medication Management ADHD
Titration‐ with children <6 years, may want to start with short acting BID until you get a sense of adequate response, then can change to long acting
Extended release may not last long enough‐ May wear off earlierMood changes‐ if extreme or “changes personality”, try new medication
Children with co‐morbidity have unique responses to meds‐ start low, go slow
Parents require frequent consultation and availability of provider for concerns when starting medication
©2018
Primary Care Management
• Patients treated with ADHD medication should have height and weight monitored (using growth charts), BP, pulse each visit
• Patients should be assessed periodically to determine if continued need for treatment or if symptoms have remitted‐ can use summers for regrowth or trial off medication
• Treatment should continue as long as symptoms remain present and cause impairment
• AAP recommends every 3‐6 month follow‐up once stable
11
©2018
Oppositional Defiant Disorder • 30‐40% of children with ADHD have ODD• Must exhibit 4 or more of the following symptoms:
– Often loses temper– Often argues with adults– Often actively defies or refuses to comply with adults' requests or rules– Often blames others for his or her misbehavior or mistakes– Is often touchy or easily annoyed by others– Is often angry and resentful– Is often spiteful and vindictive
• For children <5 years, the behavior should occur on most days for a period of at least 6 months, if > 5 years, the behavior should occur at least once per week for at least 6 months
©2018
Management of Explosive Behavior
• Understand that behavior is communication• The child is overwhelmed so is lashing out‐doesn’t have the skill to manage
feelings and express them in a more mature way. • May lack language, or impulse control, or problem‐solving abilities.• Advice to Parents:
– Stay calm. – Don’t give in. Don’t encourage child to continue behavior by agreeing to what child
wants to make it stop.– Praise appropriate behavior. When child has calmed down, give praise for pulling it
together. When child expresses feelings verbally, calmly, or tries to find a compromise on an area of disagreement, provide praise for those efforts.
– Help child practice problem‐solving skills. When child is not upset help child try out communicating feelings and come up with solutions to conflicts before they escalate into aggressive outbursts.
©2018
Sensory Processing Disorder
• Sensory integration disorder, regulatory sensory processing disorder, sensory processing dysfunction, or sensory processing dysfunction
• Neurological disorder that involves impairment in processing data from the different senses (vision, auditory, touch, olfaction, and taste), the vestibular system (movement), and proprioception (body awareness)
• Refer to sensory trained OT for evaluation
• Not evidence based
©2018
Autism Spectrum Disorder DSM V Diagnostic Criteria
A. Persistent deficits in social communication and social interaction across multiple contexts as manifested by the following, currently or by history:
1. Deficits in social‐emotional reciprocity, ranging from abnormal social approach and failure of normal back‐and‐forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
American Psychiatric Association, 2013
©2018
Autism Spectrum Disorder DSM V Diagnostic Criteria
2. Deficits in nonverbal communicative behaviors used for social interaction, ranging from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and the use of gestures; to a total lack of facial expressions and nonverbal communication.
American Psychiatric Association, 2013
©2018
Autism Spectrum Disorder DSM V Diagnostic Criteria
3. Deficits in developing, maintaining and understanding relationships, ranging from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or making friends; to absence of interest in peers.
American Psychiatric Association, 2013

12
©2018
Autism Spectrum Disorder DSM V Diagnostic Criteria
B. Restricted , repetitive patterns of behaviors, interests or activities as manifested by at least two of the following, currently or by history:
1. Stereotyped or repetitive motor movements, use of objects, or speech
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior
3. Highly restricted, fixated interests that are abnormal in intensity or focus.
4. Hyper or hypo reactivity to sensory input or unusual interest in sensory aspects of the environment
American Psychiatric Association, 2013
©2018
Autism Spectrum Disorder DSM V Diagnostic Criteria
C. Symptoms must be present in the early developmental period but may not become fully manifest until the social demands exceed limited capabilities, or may be masked by learned strategies later in life.
D. Symptoms cause clinical significant impairment in social, occupational or other important areas of current functioning
American Psychiatric Association, 2013
©2018
Autism Spectrum Disorder DSM V Diagnostic Criteria
E. These disturbances are not better explained by intellectual disability or global developmental delay.
Specify current severity for A and B
Severity in Level 1, 2 or 3
– Level 1‐ requiring support
– Level 2‐ requiring substantial support
– Level 3‐ Requiring very substantial support
American Psychiatric Association, 2013
©2018
Presentation <2 years
• No babbling by 9 months• Does not respond to name by 12 months • Does not point at objects to show interest or gestures (point at an airplane
flying over) by 12‐14 months• No single word – 16 months• Does not play "pretend" games (pretend to "feed" a doll) by 18 months • Avoids eye contact and prefers to be alone • Gets upset by minor changes in routine• Self‐stimulatory behaviors‐flaps hands, rocks body, or spins self in circles • Any loss of language or social skills at any time• Child with a sibling with ASD
©2018
Unusual Interests and Behaviors
Repetitive motions are actions repeated over and over again. These types of activities are known as self‐stimulation or "stimming."
Thrive on routine
They might "lose control" and have a "melt down" or tantrum if in a strange place.
May develop routines that might seem unusual or unnecessary. Not being allowed to do these types of routines might cause severe frustration and tantrums.
©2018
Positive Screening
• If screening significant ASD symptomatology, a thorough diagnostic evaluation should be performed to determine the presence of ASD
• Clinicians should coordinate an appropriate multi‐disciplinary assessment of children with ASD
• All children with ASD should have a medical assessment, including a physical examination, a hearing screen, a Wood’s lamp examination for signs of Tuberous Sclerosis, and genetic testing (G‐banded karyotype, Fragile X or chromosomal microarray)
• The yield of genetic testing in the presence of clinical suspicion is currently in the range of 1/3 or more of cases
Volkmar et al, 2014

13
©2018
Referral for Diagnostic Evaluation
• Refer to Developmental Pediatricians, Child Neurologists, Child Psychologists or Psychiatrists, NPs‐Pediatric Mental Health Specialists
• Should also refer for hearing and vision evaluation
• While waiting for evaluation, refer to Early Intervention (0‐3 years)
• If >3 years, refer to local school district for evaluation
• May also benefit from speech therapy, OT, PT, behavioral therapy
• In some states, children with ASD qualify for Medical Assistance
©2018
Treatment‐ Focus on Behavior and Communication
• Applied behavior analysis (ABA)
– Is widely accepted
–Used in schools and treatment clinics
– Encourages positive behaviors and discourages negativebehaviors in order to improve a variety of skills
–Child’s progress is tracked and measured
–Resources for parents: Autism Speaks‐Applied BehaviorAnalysis: A Parent's Guide available in Resources
©2018
ABA uses ABC for Behavior Management
• A: Antecedent‐the environment, the events or the behavior that precedes the Behavior of Interest, or Target Behavior. Also known as the "Setting Event," the antecedent is anything that might contribute to the behavior.
• B: Behavior‐what the child does. This is sometimes referred to as "the behavior of interest" or "target behavior. It is the behavior that you are focusing on, that is either pivotal (leads to other undesirable behavior, or contributes to other undesirable behaviors) a problem behavior that creates danger for the child or others, or a distracting behavior, that removes the child
• C: Consequence‐outcome. It is the outcome that is reinforcing for the child, so it reinforces the maladaptive behavior.? Does the parent give the child a preferred item or food, in order to stop the behavior? Obviously, the behavior had the desired effect.
©2018
Primary Care Provider Role
• See every 6 months to one year for well child care/case management
• Monitor growth, diet, elimination and sleep concerns
• Refer for treatments‐ behavioral intervention, speech, OT, other therapies as needed
• Review progress in school and advocate for support and specialized educational program (IEP)
• Evaluate for co‐morbid conditions
• May order genetic testing
©2018
Anxiety
• Most common psychiatric illness in children and adolescents, affecting 8% to 10% of the population
• Strong familial tendency believed to be related to a combination of genetic predisposition and environmental factors
• Age of onset as early as preschool years, but impairment may not be present until school age
• Girls have twice the likelihood of developing anxiety disorders as boys
©2018
Anxiety
• A physiologic response necessary for all human beings to survive.
• Fears‐ emotional response to a given stimuli or situation that is identified as threatening or scary. Fears are normal part of development
• Worries are the cognitive or thinking manifestations of fear and anxiety
• Anxiety disorders‐ diagnosed when fears, worries, or anxiety occur outside the range of normal developmental responses or are extreme and cause significant distress or impairment in functioning (school, home, social settings)
14
©2018
DSM‐5 Anxiety Disorders
1. Anxiety Disorders (separation anxiety disorder, selective mutism, specific phobia, social phobia, panic disorder, agoraphobia, and generalized anxiety disorder).
2. Obsessive‐Compulsive Disorders (obsessive‐compulsive disorder, body dysmorphic disorder, hoarding disorder, trichotillomania, and excoriation disorder).
3. Trauma and Stressor‐Related Disorders (reactive attachment disorder, disinhibited social engagement disorder, PTSD, acute stress disorder, and adjustment disorder).
©2018
Generalized Anxiety Disorder
• Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance).
• The child finds it difficult to control the worry.
©2018
Generalized Anxiety Disorder
• For children, the anxiety and worry are associated with one (or more) of the following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months):– Restlessness or feeling keyed up or on edge
– Being easily fatigued
– Difficulty concentrating or mind going blank
– Irritability
– Muscle tension
– Sleep disturbance (difficulty falling or staying asleep, or restlessness, unsatisfying sleep)
©2018
Separation Anxiety
• Onset from preschool until 18 years of age• Duration at least 4 weeks• Developmentally inappropriate worry related to separation
from home or to whom one is attached
©2018
Separation Anxiety
• Three of the following are present:
– Distress with separation or anticipated separation
–Worry of harm to caretakers, worry of untoward event causing separation, physical complaints with separation
– Anticipated separation, repeated nightmares of separation
• School refusal type of separation anxiety‐ described as a persistent pattern of not wanting to go to school, avoidance of school, or high distress associated with going to school
©2018
Social Phobia
• Anxiety disorder involving discomfort around social interaction, and concern about being embarrassed and judged by others
• This discomfort will be experienced as fear and anxiety, and may be accompanied by autonomic arousal, including diaphoresis, apnea, tremors, tachycardia, and nausea
• Essential feature is anxiety caused by exposure to a feared social situation, duration of at least 6 months
15
©2018
Social Phobia
• Ranges from discomfort that can be circumvented and adapted to, to a virtually disabling fear with infiltration into multiple areas of life
• The discomfort can generalize to routine activities such as eating in front of others, or using a public bathroom
• Children social phobia desire social contacts, want to participate in social situations, but their anxiety can become unbearable
©2018
Selective Mutism
• Selective Mutism is a childhood disorder typified by an inability to speak in certain circumstances
• A consistent failure to speak in certain social situations where there is a natural expectation of speaking
• Researchers believe the behavior is a form of social phobia
©2018
Obsessive‐Compulsive Disorder (OCD)
• Condition in which an individual experiences intrusive thoughts, images, or impulses that creates a high degree of emotional distress
• The person feels a need to perform some type of ritual (either overt or covert in nature)
• The ritual serves two functions: (1) to reduce the intensity of the anxiety, disgust, etc. and (2) to prevent or lessen the likelihood of acting on the thought/image. This is referred to as “thought‐action fusion” (TAF)
©2018
Behaviors Related to Posttraumatic Stress Disorder in Preschool Children
• One of the following related to traumatic events:– persistent avoidance of activities, places, or physical reminders– people, conversations, or interpersonal situations that arouse recollections– diminished interest or participation in significant activities such as play– socially withdrawn behavior– persistent reduction in expression of positive emotions
• Two or more of the following:– irritable, angry, or aggressive behavior, including extreme temper tantrums– hypervigilance– exaggerated startle response– problems with concentration– difficulty falling or staying asleep or restless sleep
©2018
Cognitive Behavioral Therapy: Evidence Based Psychotherapy
• The Child/Adolescent Anxiety Multimodal Study (CAMS) found that high quality cognitive behavioral therapy (CBT), given with or without medication, can effectively treat anxiety disorders, OCD, PTSD in children
• Can be very effective in 2/3 of children, may be used in as young as 2‐3 years old
• Short‐term therapy, with anywhere from 8‐16 sessions
©2018
Cognitive Behavioral Therapy (CBT)
• Therapists teach children that thoughts cause feelings and moods which can influence behavior.
• Child learns to identify harmful thought patterns and replace this thinking with thoughts that result in more appropriate feelings and behaviors.
• Primary goal of CBT to change maladaptive learning and thought patterns
• Core component is cognitive restructuring of anxious cognitions
• Requires the child to first explicitly recognize their “self‐talk” and then to understand the links between self‐talk and their symptoms
16
©2018
CBT with Preschool Children
• Parent Role: co‐therapist, can provide incentives for practicing skills, can practice with child
• Some of the techniques used with young children include:– children’s symptoms are given a name and put in a story form, involves cognitive tasks of self‐reflection, autobiographical recall, and causal reasoning.
– fears are placed in a bigger context of other feelings and other situations.– children are taught self‐control with relaxation tools with the message that these carry a change in locus of control.
– children are asked to imagine themselves in future situations that may trigger anxiety. This is a cognitive task of perspective taking and causal reasoning.
©2018
The time is now
• NPs have the training, the skill, and the passion for caring for children with behavioral conditions.
• These children and their families need your help and expertise!
• Good luck!
Questions?
Additional Resources
©2018
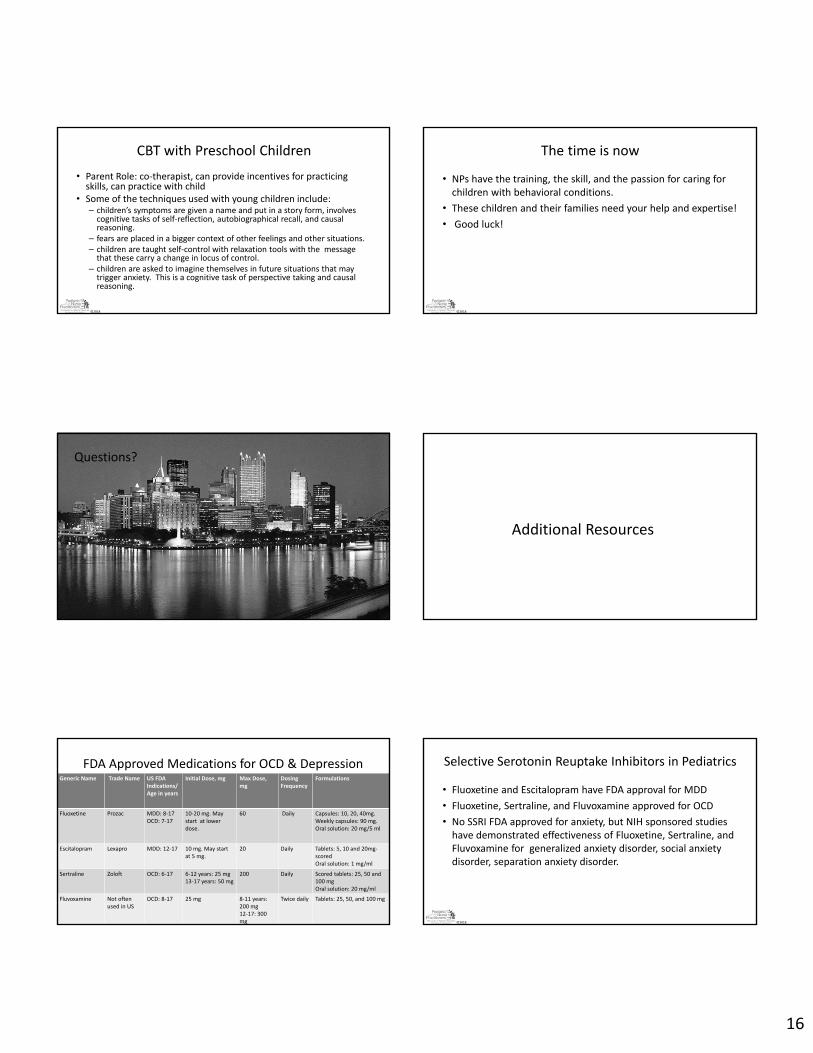
FDA Approved Medications for OCD & DepressionGeneric Name Trade Name US FDA
Indications/Age in years
Initial Dose, mg Max Dose, mg
Dosing Frequency
Formulations
Fluoxetine Prozac MDD: 8‐17OCD: 7‐17
10‐20 mg. May start at lower dose.
60 Daily Capsules: 10, 20, 40mg. Weekly capsules: 90 mg. Oral solution: 20 mg/5 ml
Escitalopram Lexapro MDD: 12‐17 10 mg. May start at 5 mg.
20 Daily Tablets: 5, 10 and 20mg‐scoredOral solution: 1 mg/ml
Sertraline Zoloft OCD: 6‐17 6‐12 years: 25 mg 13‐17 years: 50 mg
200 Daily Scored tablets: 25, 50 and 100 mgOral solution: 20 mg/ml
Fluvoxamine Not often used in US
OCD: 8‐17 25 mg 8‐11 years: 200 mg12‐17: 300 mg
Twice daily Tablets: 25, 50, and 100 mg
©2018
Selective Serotonin Reuptake Inhibitors in Pediatrics
• Fluoxetine and Escitalopram have FDA approval for MDD
• Fluoxetine, Sertraline, and Fluvoxamine approved for OCD
• No SSRI FDA approved for anxiety, but NIH sponsored studies have demonstrated effectiveness of Fluoxetine, Sertraline, and Fluvoxamine for generalized anxiety disorder, social anxiety disorder, separation anxiety disorder.
17
©2018
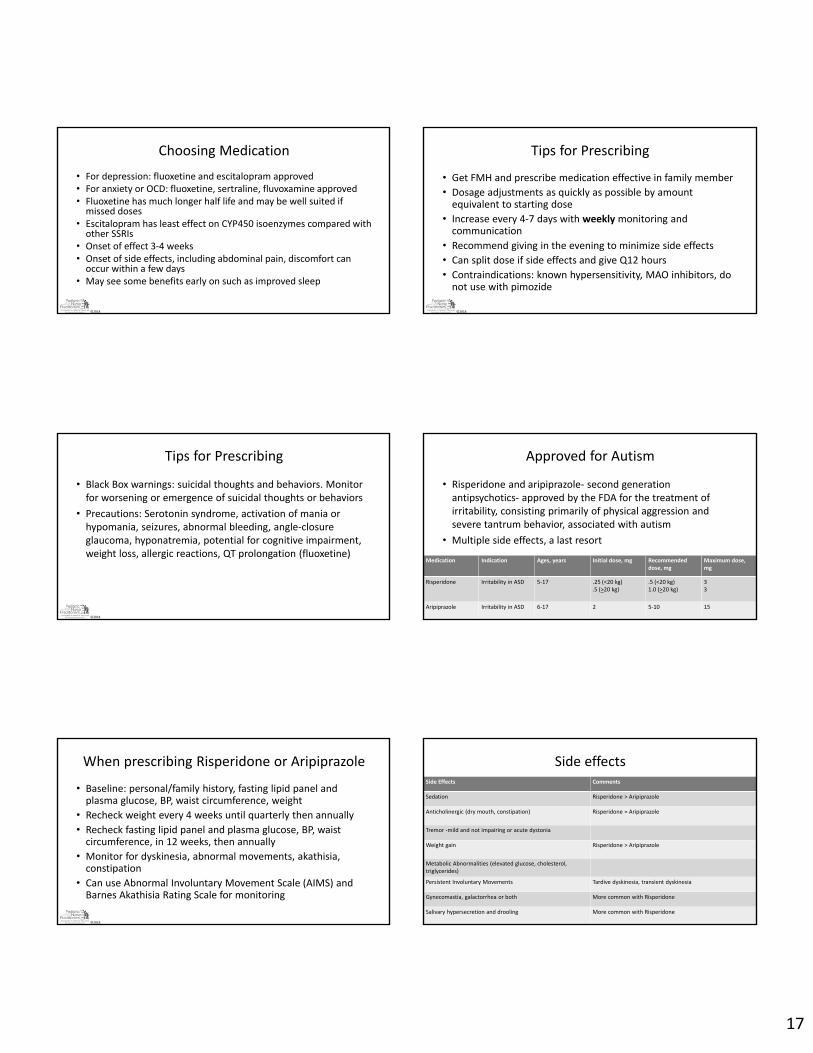
Choosing Medication
• For depression: fluoxetine and escitalopram approved• For anxiety or OCD: fluoxetine, sertraline, fluvoxamine approved• Fluoxetine has much longer half life and may be well suited if missed doses
• Escitalopram has least effect on CYP450 isoenzymes compared with other SSRIs
• Onset of effect 3‐4 weeks• Onset of side effects, including abdominal pain, discomfort can occur within a few days
• May see some benefits early on such as improved sleep
©2018
Tips for Prescribing
• Get FMH and prescribe medication effective in family member
• Dosage adjustments as quickly as possible by amount equivalent to starting dose
• Increase every 4‐7 days with weeklymonitoring and communication
• Recommend giving in the evening to minimize side effects
• Can split dose if side effects and give Q12 hours
• Contraindications: known hypersensitivity, MAO inhibitors, do not use with pimozide
©2018
Tips for Prescribing
• Black Box warnings: suicidal thoughts and behaviors. Monitor for worsening or emergence of suicidal thoughts or behaviors
• Precautions: Serotonin syndrome, activation of mania or hypomania, seizures, abnormal bleeding, angle‐closure glaucoma, hyponatremia, potential for cognitive impairment, weight loss, allergic reactions, QT prolongation (fluoxetine)
©2018
Approved for Autism
• Risperidone and aripiprazole‐ second generation antipsychotics‐ approved by the FDA for the treatment of irritability, consisting primarily of physical aggression and severe tantrum behavior, associated with autism
• Multiple side effects, a last resort
Medication Indication Ages, years Initial dose, mg Recommended dose, mg
Maximum dose, mg
Risperidone Irritability in ASD 5‐17 .25 (<20 kg).5 (>20 kg)
.5 (<20 kg)1.0 (>20 kg)
33
Aripiprazole Irritability in ASD 6‐17 2 5‐10 15
©2018
When prescribing Risperidone or Aripiprazole
• Baseline: personal/family history, fasting lipid panel and plasma glucose, BP, waist circumference, weight
• Recheck weight every 4 weeks until quarterly then annually
• Recheck fasting lipid panel and plasma glucose, BP, waist circumference, in 12 weeks, then annually
• Monitor for dyskinesia, abnormal movements, akathisia, constipation
• Can use Abnormal Involuntary Movement Scale (AIMS) and Barnes Akathisia Rating Scale for monitoring
©2018
Side effectsSide Effects Comments
Sedation Risperidone > Aripiprazole
Anticholinergic (dry mouth, constipation) Risperidone = Aripiprazole
Tremor ‐mild and not impairing or acute dystonia
Weight gain Risperidone > Aripiprazole
Metabolic Abnormalities (elevated glucose, cholesterol, triglycerides)
Persistent Involuntary Movements Tardive dyskinesia, transient dyskinesia
Gynecomastia, galactorrhea or both More common with Risperidone
Salivary hypersecretion and drooling More common with Risperidone

18
©2018
Time Outs
• Time outs for nonviolent misbehavior can work well with younger children
• Avoid triggers. Most kids who have frequent meltdowns do it at very predictable times, like homework time, bedtime, or when it’s time to stop playing, whether it’s Legos or the Xbox. The trigger is usually being asked to do something they don’t like, or to stop doing something they do like. Time warnings (“we’re going in 10 minutes”), breaking tasks down into one‐step directions and preparing child for situations can help avoid meltdowns.
©2018
Tantrums/Time Out
• Response depends on severity. Ignore as often as possible, since even negative attention can be encouraging.
• If child gets physical, ignoring not recommended‐can result in harm
• Put child in a safe environment that does not give access to parent or any other potential rewards.
• For young children can place in a time out chair. If child will not stay in the chair, take to backup area where child can calm down without anyone else in the room. Should not have toys or games in the area that might make it rewarding.
• Child should stay in that room for one minute and must be calm before allowed out. Then child should come back to the chair for time out. This gives the child an immediate and consistent consequence for aggression, removes all access to reinforcement in environment.
©2018
ODD Treatment
• Parent training. Therapist helps parents be more consistent, more positive with child
• Parent‐child interaction therapy (PCIT). Therapist coaches parents while they interact with child, guides parents through strategies that reinforce child's positive behavior
• Individual and family therapy. Therapist helps child learn to manage anger and express feelings in a healthier way. Helps parent‐child communication.
• Cognitive problem‐solving training. Therapy aimed at helping child identify and change thought patterns that lead to behavior problems.
• Social skills training. Therapy that helps child be more flexible and learn how to interact more positively and effectively with peers.
©2018
Coding Options
• F98.9 Unspecified behavioral and emotional disorders with onset usually occurring in childhood and adolescence
• F63.81 Intermittent explosive disorder
Helpful Resources for Parents and Providers Caring for Children with MH Disorders
CHADD (Children and Adults with Attention/Hyperactivity Deficit Disorder) http://www.chadd.orgo A resource for both parents and providers that includes: Home of the National Resource Center for ADHD, ADHD toolkit, information on training
opportunities, medications and natural treatment options and publishes a magazine ‘Attention’. Must pay to be a member for full access to their website. ADDitude Magazine (https://www.additudemag.com)
o Wide range of information for both providers and parents. Quarterly magazine available online and in print. Restricts access with charge both for magazine and membership.
American Academy of Pediatrics (AAP) Healthy Children https://www.healthychildren.org/English/health‐issues/conditions/adhd/Pages/Understanding‐ADHD.aspx
o Wide range of information on variety of physical and emotional topics related to ADHD. No cost to access website. Not very interactive. American Academy of Child and Adolescent Psychiatry (AACAP) ADHD Resource Center
http://www.aacap.org/aacap/Families_and_Youth/Resource_Centers/ADHD_Resource_Center/Home.aspxo Wide range of information on ADHD and other co‐morbid psychiatric conditions along with treatment options. Free information for both parents and
providers. Website not very interactive. Child Mind Institute https://childmind.org/about‐us/
o Provides information on symptoms and treatment of mental health disorders. Excellent parenting suggestions and guides. Section for educators. Includes a symptom checker for parents.
National Alliance on Mental Illness (NAMI) https://www.nami.orgo Provides information on disorders and treatment. Superior information for family members and caregivers. Has LGBTQ section.
National Institute on Mental Illness (NIMH) https://www.nimh.nih.gov/health/topics/attention‐deficit‐hyperactivity‐disorder‐adhd/index.shtmlo Extensive information on symptoms and treatment options. All evidence based information. Technical information and probably more useful to
provider than parents.
Resources Autism
• PCP support‐ First Signs http://www.firstsigns.org/
• Parent support‐ Autism Speaks https://www.autismspeaks.org/
• Child Mind Institute: http://www.childmind.org/en/health/disorder‐guide/autism‐spectrum‐disorder
• Autism and Medication: A Guide for Families of Children with Autism Safe and Careful Use‐ available as PDF at https://www.autismspeaks.org/news/news‐item/autism‐speaks‐launches‐autism‐and‐medication‐tool‐kit.
19
©2018
Resources for Children with ADHD
•CHADD (Children and Adults with Attention/Hyperactivity Deficit Disorder) http://www.chadd.orgA resource for both parents and providers that includes: Home of the National Resource Center for ADHD, ADHD toolkit, information on training opportunities, medications and natural treatment options and publishes a magazine ‘Attention’. Must pay to be a member for full access to their website.
•ADDitude Magazine (https://www.additudemag.com)Wide range of information for both providers and parents. Quarterly magazine available online and in print. Restricts access with charge both for magazine and membership.
•American Academy of Pediatrics (AAP) Healthy Children https://www.healthychildren.org/English/health-issues/conditions/adhd/Pages/Understanding-ADHD.aspx
Wide range of information on variety of physical and emotional topics related to ADHD. No cost to access website. • American Academy of Child and Adolescent Psychiatry (AACAP) ADHD Resource Center
http://www.aacap.org/aacap/Families_and_Youth/Resource_Centers/ADHD_Resource_Center/Home.aspxWide range of information on ADHD and other co-morbid psychiatric conditions along with treatment options. Free information for both parents and providers. Website not very interactive.
•Child Mind Institute https://childmind.org/about-us/Provides information on symptoms and treatment of mental health disorders. Excellent parenting suggestions and guides. Section for educators. Includes a symptom checker for parents.
©2018
Other Resources
• American Academy of Pediatrics guidelines, recommendations
• Bright Futures, 4th Edition
• Zero to Three, DC:0‐5 Diagnostic Classification of Mental Health & Developmental Disabilities of Infancy and Childhood
• NICHQ Report on Promoting Young Children’s (0‐3) Socioemotional Development in Primary Care
• Infant Mental Health literature‐ promotes enhancing the social and emotional competence of young children
©2018
Building Resilience in Children
• Sesame Street Toolkit: https://www.sesamestreet.org/sites/default/files/media_folders/Images/Resilience_Edguide_Probsolve.pdf
• How to Foster Resilience in Kids: https://childmind.org/article/foster‐resilience‐kids/
• Building Resilience in Children (AAP): https://www.healthychildren.org/English/healthy‐living/emotional‐wellness/Building‐Resilience/Pages/Building‐Resilience‐in‐Children.aspx
©2018
Mindfulness Apps
• Breathe, Think, Do with Sesame
– Sections for both parents and children, this app teaches young kids how to calm down and solve everyday challenges. Children enjoy the interactive “play time” with a Sesame Street monster, and educational tools are identified for parents to help manage their child’s anxieties or anger issues.
• Calm
– Practices meditation, with a focus on relaxation and sleep. “Sleep Stories” function tells tales to help users fall asleep easier. There’s also a special section for “Calm Kids.”
•
©2018
Mindfulness Apps
• Daniel Tiger’s Grr‐ific Feelings
– PBS’s Daniel Tiger teaches children how to calm down when angry, celebrate proud moments, and relax with music