Embed Size (px)
Citation preview
$172
329
SMFM Abstracts
VASCULAR ENDOTHELIAL GROWTH FACTOR EXPRESSION IN PLA- CENTAE FROM PREGNANCIES COMPLICATED BY PREECLAMPSIA M-~ O H ~, H-M RYU1, J-C SHIN 2, EJ POPEK3; ]Samsung Cheil Hospital & Women's Healthcare Center, Sungkyunkwan University, Depar tment of Obstetrics and Gynecology, Seoul; 2Catholic University, College of Medicine, Depar tment of Obstetrics and Gynecology, Seoul; 3Baylor College of Medicine, Depar tment of Pathology, Houston, TX
OBJECTIVE: The purpose of this study was to determine whether there is difference in vascular endothelial growth factor (VEGF) protein expression between placentae f rom preeclampsia patients and those f rom controls to clarify the source of increased systemic level of VEGF in preeclampsia.
STUDY DESIGN: Blood samples were collected f rom 12 preeclampsia patients and 10 normal p regnan t women shortly before delivery. Placentae were collected f rom preeclampsia pat ients (n = 10) a n d controls (n = 8) immediately after delivery. We have per formed western blot and competitive enzyme immunoassay using placental homogenates . We also measured the serum VEGF concentrat ion in both groups.
RESULTS: Two dist inct bands were ob ta ined on Western blots. The molecular weight of the weak bands appears to cor respond to that of the h u m a n recombinant VEGF 165 homodimers (42 kDa) and the other strong bands represent alternative post-translational modification of the VEGF 165. The relative intensities of the two bands demons t r a t ed no significant dif- ference between placentae f rom pre-eclampsia and those from control group. The median value of placenta tissue VEGF was 1.2 n g / m l (range 0.22-30.33 ng /ml ) in the preeclampsia group and 2.4 n g / m l (range 1.03-30.45 ng /ml ) in the control group, which showed no significant difference between the two groups. On the contrary, the serum VEGF levels were significantly higher in the preeclampsia g roup (median 18.2 ng /ml , range 4,6-101.6 n g / m l ) than the control group (median 4 .9ng/ml , range 2.3-9.1 ng /ml , P < .005).
CONCLUSION: This study suggests that placenta is not the origin of the increased circulating VEGF in preeclampsia and there may be other potential site of VEGF synthesis in preeclampsia.
331
December 2001 A m J Obstet Gyuecol
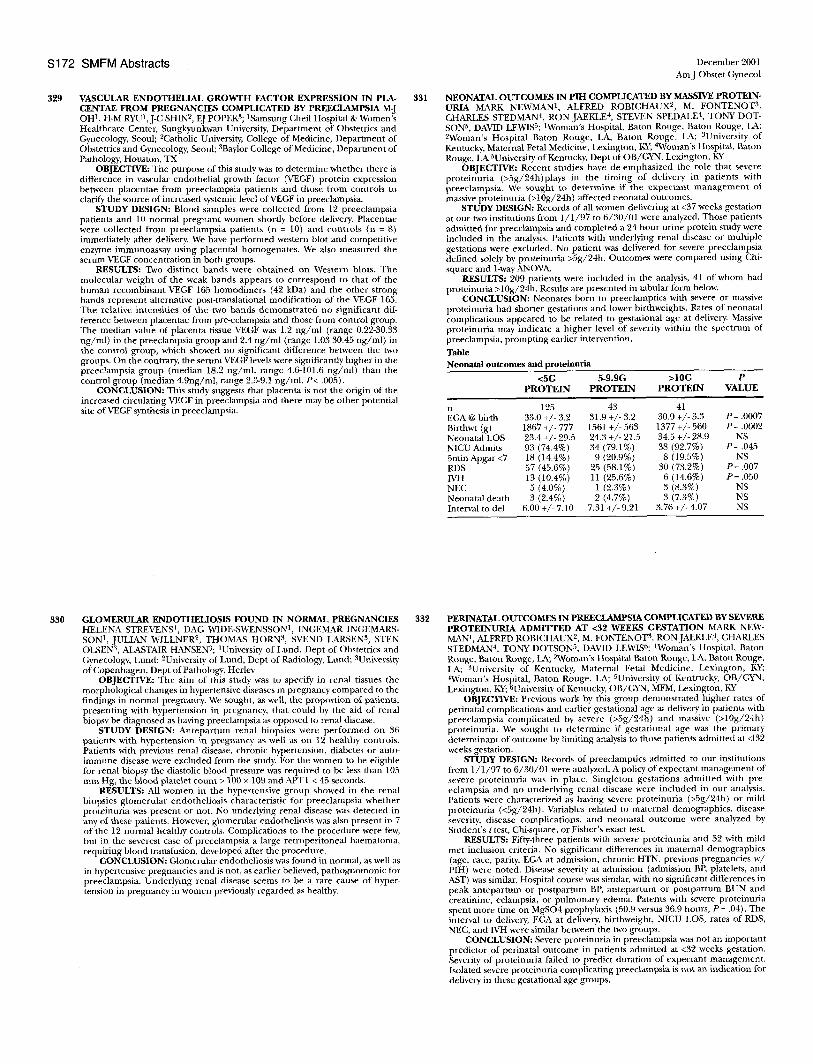
NEONATAL OUTCOMES IN PIH COMPLICATED BY MASSIVE PROTEIN° URIA MARK NEWMAN 1, ALFRED ROBICHAUX 2, M. FONTENOT 3, CHARLES STEDMAN 4, RON JAEKLE 4, STEVEN SPEDALE 4, TONY DOT- SON 5, DAVID LEWIS5; 1Woman's Hospital, Baton Rouge, Baton Rouge, LA; 2Woman's Hospital Baton Rouge, LA, Baton Rouge, LA; 3University of Kentucky, Maternal Fetal Medicine, Lexington, KY; 4Woman's Hospital, Baton Rouge, LA 5University of Kentucky, Dept of OB/GYN, Lexington, KY
OBJECTIVE: Recent studies have de-emphasized the role that severe pro te inur ia (>5g/24h)plays in the t iming of delivery in pat ients with preeclampsia . We sought to de te rmine if the expectant m a n a g e m e n t of massive proteinuria (>10g/24h) affected neonatal outcomes.
STUDY DESIGN: Records of all women delivering at <37 weeks gestation at our two institutions from 1 / 1 / 9 7 to 6 /30 /01 were analyzed. Those patients admitted for preeclampsia and completed a 24 h o u r urine protein study were included in the analysis. Patients with underlying renal disease or multiple gestations were excluded. No patient was delivered for severe preeclampsia defined solely by proteinuria >Sg/24h. Outcomes were compared using Chi- square and 1-way ANOVA.
RESULTS: 209 patients were included in the analysis, 41 of whom had proteinuria >10g/24h. Results are presented in tabular torm below.
CONCLUSION: Neonates bona to preeclamptics with severe or massive proteinuria had shorter gestations and lower birthweights. Rates of neonatal complications appeared to be related to gestational age at delivery. Massive pro te inur ia may indicate a h igher level of severity within the spect rum of preeclampsia, p rompt ing earlier intervention.
Table Neonatal outcomes and proteinuria
<5G 5-9.9G >10G P PROTEIN PROTEIN PROTEIN VALUE
n 125 43 41 EGA @ birth 33.0 +/- 3.2 31.9 +/- 3.2 30.9 +/- 3.3 P = .0007 Birthwt (g) 1867 +/- 777 1561 +/- 563 1377 +/- 560 P = .0002 Neonatal LOS 23.4 +/- 29.5 24.3 +/- 21.5 34.5 +/- 28.9 NS NICU Admits 93 (74.4%) 34 (79.1%) 38 (92.7%) P = .045 5rain Apgar <7 18 (14.4%) 9 (20.9%) 8 (19.5%) NS RDS 57 (45.6%) 25 (58.1%) 30 (73.2%) P = .007 IVH 13 (10.4%) 11 (25.6%) 6 (14.6%) P = .050 NEC 5 (4.0%) 1 (2.3%) 3 (8.3%) NS Neonatal death 3 (2.4%) 2 (4.7%) 3 (7.3%) NS Interval to del 6.00 +/- 7.10 7.31 +/- 9.21 3.76 +/- 4.07 NS
330 GLOMERULAR ENDOTHELIOSIS FOUND 1N NORMAL PREGNANCIES HELENA STREVENS 1, DAG WIDE-SWENSSON 1, INGEMAR INGEMARS- SON 1, JULIAN W1LLNER 2, THOMAS HORN 3, 8VEND LARSEN 3, STEN OLSEN 3, ALASTAIR HANSEN3; ]University of Lund, Dept of Obstetrics and Gynecology, Lund; 2University of Lund, Dept of Radiology, Lund; 3University of Copenhagen, Dept of Pathology, Herlev
OBJECTIVE: The aim of this study was to specify in renal tissues the morphological changes in hypertensive diseases in pregnancy compared to the findings in normal pregnancy. We sought, as well, the propor t ion of patients, present ing with hyper tension in pregnancy, that could by the aid of renal biopsy be diagnosed as having preeclampsia as opposed to renal disease.
STUDY DESIGN: Antepa r tum renal biopsies were p e r f o r m e d on 36 patients with hypertension in p regnancy as well as on 12 healthy controls. Patients with previous renal disease, chronic hypertension, diabetes or auto- immune disease were excluded f rom the study. For the women m be eligible for renal biopsy the diastolic blood pressure was required to be less than 105 m m Hg, the Mood platelet count > 100 x 109 and APTT < 45 seconds.
RESULTS: All women in the hypertensive g r o u p showed in the renal biopsies g lomeru la r endotheliosis characterist ic for preeclampsia whether proteinuria was present or not. No underlying renal disease was detected in any of these patients. However, glomerular endotheliosis was also present in 7 of the 12 normal healthy controls. Complications to the procedure were few, but in the severest case of preeclampsia a large retroperi toneal haematoma, requir ing blood transfusion, developed after the procedure.
CONCLUSION: Glomerular endotheliosis was found in normal, as well as in hypertensive pregnancies and is not, as earlier believed, pa thognomouic for preeclampsia. Under lying renal disease seems to be a rare cause of hyper- tension in pregnancy in women previously regarded as healthy.
332 pERINATAL OUTCOMES IN PREECLAMPSIA COMPLICATED BY SEVERE PROTEINURIA ADMITTED AT <32 WEEKS GESTATION MARK NEW- MAN 1 , ALFRED ROBICHAUX 2, M. FONTENOT 3, RON JAEKLE 4, CHARLES STEDMAN 4, TONY DOTSON 5, DAVID LEWISt; tWoman's Hospital, Baton Rouge, Baton Rouge, LA; ~ o m a n ' s Hospital Baton Rouge, LA, Baton Rouge, LA; 3University of Kentucky, Maternal Fetal Medicine, Lexington, KY; ~Woman's Hospital, Baton Rouge, LA; 5University of Kentrucky, OB/GYN, Lexington, KY; 6University of Kentucky, OB/GYN, MFM, Lexington, KY
OBJECTIVE: Previous work by this group demonstra ted h igher rates of perinatal complications and earlier gestational age at delivery in patients with preeclampsia compl ica ted by severe (>5g/24h) and massive (>10g/24b) prote inur ia . We sought to de te rmine if gestat ional age was the pr imary determinant of ontcmne by limiting analysis to those patients admit ted at <132 weeks gestation.
STUDY DESIGN: Records of preectamptics admitted to our institutions from 1 / 1 / 9 7 to 6 /30 /01 were analyzed. A policy of expectant management of severe p ro te inur ia was in place. Singleton gestations admit ted with pre- eclampsia and no under ly ing renal disease were inc luded in our analysis. Patients were characterized as having severe proteinuria (>Sg/24h) or mild proteinuria (<5g/24h). Variables related to materual demographics, disease severity, disease complicat ions, and neonata l ou tconm were analyzed by Student 's t test, Cbi-square, or Fisher's exact test.
RESULTS: Fifty-three patients with severe proteinuria and 52 with mild met inclusion criteria. No significant differences in maternal demographics (age, race, parity, EGA at admission, chronic HTN, previous pregnancies w / PIH) were noted. Disease severity at admission (admission BP, platelets, and AST) was similar. Hospital course was similax, with no significant differences in peak an t epa r tum or pos tpa r tum BP, an t epa r tum or pos tpa r tum BUN a n d creatinine, eclampsia, or pu lmonary edema. Patents with severe proteinuria spent nmre time on MgSO4 prophylaxis (50.9 versus 36.9 hours, P = .04). The interval to delivery, EGA at delivery, birthweight, NICU LOS, rates of RDS, NEC, and IVH were similar between the two groups.
CONCLUSION: Severe proteinuria in preeclampsia was not an important predictor of perinatal outcome in patients admit ted at <32 weeks gestation. Severity of proteinuria failed to predict durat ion of expectant management . Isolated severe proteinuria complicating preeclampsia is not an indication for delivery in these gestational age groups.



























![BMJ Openhave explored the postterm effect on maternal mental health.[26-30] Blom et al. interestingly reported that certain perinatal complications such as preeclampsia, hospitalization,](https://img.pdfslide.net/doc/110x75/5e7040f2caf7426e376accb9/bmj-open-have-explored-the-postterm-effect-on-maternal-mental-health26-30-blom.jpg)