Embed Size (px)
Citation preview

340 CHAPTER 16 Musculoskeletal and Connnective Tissue System
340
Musculoskeletal and Connective Tissue System
PHYSIOLOGY OF THE MUSCULOSKELETAL SYSTEM
Skeletal SystemA. Bonestructure. 1. Periosteum:densefibrousmembranecoveringthe bone;periostealvesselssupplybonetissue. 2. Epiphysis:awidenedareafoundattheendofalong bone. 3. Epiphysealplate(growthplate):acartilaginous areainchildren’sbonesthatprovidesforlongitu- dinalgrowthofthebone. 4. Redbonemarrow:primaryfunctionisproduction ofredbloodcells.B. Bonemaintenanceandhealing. 1. Regulatoryfactorsdeterminingboneformationand resorption. a. Weight-bearingstressstimulateslocalboneresorp- tionandformation;thereforeinstatesofimmobility whereweightbearingisprevented,calciumislost fromthebone. b. VitaminDpromotesabsorptionofcalciumfrom thegastrointestinal(GI)tractandacceleratesmo- bilizationofcalciumfromthebonetoincreaseor maintainserumcalciumlevels.C. Musculoskeletalchangesintheolderadult(Box16-1).
Connective Tissue: Joints and CartilageA. Joints. 1. Theactionofjointspermitsbonestochangeposi- tionandfacilitatebodymovement. 2. Synovialjointscontainsynovialfluid,whichlubri- catesthejointsandfacilitatesjointmobility. 3. Cartilageisrigidfibroustissuethatformsacapsule overtheendoftheboneandjoinstheendofeach bonetogether.B. Ligamentsandtendonsaretoughfibrousconnectivetis- suethatprovidesstabilitywhilecontinuingtopermit movement. 1. Tendonsattachmusclestothebone. 2. Ligamentsattachbonestojoints.
Skeletal Muscle A. Musclesareattachedtotendons,bones,andcon- nectivetissue. B. Lowermotorneuronscontroltheactivityofskeletal muscle.
C. Energyisconsumedwhenskeletalmusclescontractin responsetoastimulus.D. Musclecontraction. 1. Musclesaccomplishmovementonlybycontraction. a. Flexion:bendingatajoint. b. Extension:straighteningofajoint. c. Abduction:actionmovingawayfromthebody. d. Adduction:actionmovingtowardthebody.
NURSING PRIORITY: When caring for clients with orthopedic or musculoskeletal problems, it is essential to know the terms used for referring to movement of the joints.
2. Hypertrophy,orincreasedmusclemass,willoccur ifmuscleisexercisedrepeatedly. 3. Atrophy,ordecreasedmusclemass,willoccurwith muscledisuse.
System Data CollectionA. History. 1. Historyofmusculoskeletalinjuries,neuromuscular disabilities,inflammatoryandmetabolicconditions directlyorindirectlyaffectingthemusculoskeletal system. 2. Familialpredispositiontoorthopedicproblems.
✔
• Decreased bone density leads to more frequent fractures.
• Decrease in subcutaneous tissue results in less soft tissue over bony prominences.
• Degenerative changes in the spine alter posture and gait; disk compression causes a loss in height.
• Degenerative changes in cartilage and ligaments result in decreased joint movement as well as causing joint stiffness and pain.
• Decreased range of motion of extremities; older adult may need increased assistance with activities of daily living.
• Slowed movement and decreased muscle strength lead to decreased response time.
BOX 16-1 OLDER ADULT CARE FOCUSMusculoskeletal Changes
• The wider the base of support, the greater the stability. Position your feet wide apart. • The lower the center of gravity, the greater the stability. Flex the knees; let the strong muscles of the legs do the work. • Position yourself close to object and/or client. • Face the client; keep back, pelvis, and knees aligned; avoid twisting. • Balance activity between arms and legs. • Avoid bending to lift; this decreases strain on the back. • Encourage client to assist. • Pivoting, turning, rolling, and leverage require less work. • Person with heaviest load should coordinate team efforts. • Obtainassistancewithheavyordifficulttransfers or lifts. • Teach clients proper body mechanics.
TEST ALERT: Use good body mechanics when providing care – use assistive devises when possible
BOX 16-2 BODY MECHANICS
• Itismoredifficulttomaintainimmobilityinthese clients after fractures; therefore surgical intervention (e.g., ORIF) is frequently used for treatment.
• The older client heals more slowly, so use of the affected extremity and weight bearing are frequently delayed.
• Complications of immobility occur more frequently; mobilize hospitalized clients as early as possible.
• Do not rely on fever as the primary indication of infection; decreasing mental status is more common.
• Contractures are more common. Encourage use of assistive devices (canes and walkers).
BOX 16-3 OLDER ADULT CARE FOCUSMusculoskeletal Nursing Implications
• If pain lasts longer than 1 hour after exercise, need to change exercises that involve that joint.
• Plan activity and work schedule to conserve energy: do importanttasksfirst.
• Alternate activities; do not complete all heavy tasks at one time.
• Minimize stress on joints: sit rather than stand, avoid prolonged repetitive movements, move around frequently, avoid stairs or prolonged grasping.
• Use larger muscles rather than smaller ones: use shoulders or arms rather than hands to push open doors; pick up items without stooping or bending, use leg muscles; women can carry purses on their shoulders rather than in their hands.
• Painful,acutelyswolleninflamedjointsshouldnotbe exercised beyond basic ROM.
• Regularly exercise even when joints are slightly painful and stiff: swimming and bike riding maintain mobility without weight bearing.
BOX 16-4 OLDER ADULT CARE FOCUSProtecting Joints

CHAPTER 16 Musculoskeletal and Connnective Tissue System 341
3. Levelofnormalactivity. a. Occupation,exercise,recreation. b.Levelofnormalactivity,abilitytomaintainown ADLs. 4. Existenceofotherchronichealthproblems.B. Physicalassessment. 1. Initialinspectionforgrossdeformities,asymmetry, swelling,andedema. 2. Nutritionalstatus:appropriatenessofclient’sweight andbodyframe. 3. Joints a. Movement:activeandpassive;examineactive movementfirst;comparemovementandrangeof motiontooppositeside. b. Inflammationandtenderness:withorwithout movement. c. Presenceofjointdeformitiesordislocations. d. Palpatejointsforthepresenceofcrepitus. 4. Evaluateclient’sspinalalignment,posture,andgait. 5. Evaluateskeletalmuscle. a. Musclestrengthbilaterally. b. Coordinationofmovement. c. Presenceofatrophyorhypertrophy. d. Presenceofinvoluntarymusclemovement. 6. Assessperipheralpulsesandperipheralcirculation; capillaryrefillshouldnormallytakeabout2to3 seconds. 7. Assessforpresenceofandcharacteristicsofpain. a. Mostmusculoskeletalpainisrelievedbyrest. b. Identifyprecipitatingactivitiesand/orprecipitat- ingfactors. c. Typeofpainandlocation. 8. Assessforanyalterationofnormalsensationinex tremities. 9. Assessforuseofproperbodymechanics (Box16-2). 10. Assessforchangesinmusculoskeletalsystemre- latedtoaging(Box16-1). 11. Principlesofbodymechanicsforhealthcare personnel(Box16-2,Appendix3-1).
TEST ALERT: Orthopedic questions may be based on concepts of immobility, nursing assess-ment of an extremity, compromised circulation,
and/or general perioperative care. Pay close attention to the direction of the question.
DISORDERS OF THE MUSCULOSKELETAL SYSTEM
Developmental Dysplasia of the HipMalformations of the hip that occur as a result of
imperfectdevelopmentofthefemoralhead,theacetabulum,orboth.
✽
Data Collection (Newborn)A. Ortolanisign:Withtheinfantsupine,kneesflexed,and hipsfullyabducted,aclickisheardorfeltasthehipis abducted.B. Asymmetricalglutealandthighfolds.C. Shorteningofthelegontheaffectedside.D. Limitedhipabductiononaffectedside.
TreatmentA. Treatmentshouldbeinitiatedassoonasconditionis identified.B. Abductiondevices. 1.Pavlikharnessisafabricharnessthatmaintainsthe legsintheflexed,abductedpositionatthehip,it willholdtheaffectedhipinanabductionposi- tion,andpreventextensionandadduction.Itmaybe removedforbathingbuttheinfantwillwearitfull- timeuntilthehipisstable. 2. Hipspicacastmaybeusedwhenanadductioncon- tractureispresentC. Surgerymaybedoneifthecorrectionisnotfeasible withabductiondevices.
Nursing Interventionsv Goal:Toidentifyprobleminthenewbornbeforedis-charge.v Goal:Toassistparentstounderstandmechanismtomaintainreduction.A. Pavlikharness.
• Decreased bone density leads to more frequent fractures.
• Decrease in subcutaneous tissue results in less soft tissue over bony prominences.
• Degenerative changes in the spine alter posture and gait; disk compression causes a loss in height.
• Degenerative changes in cartilage and ligaments result in decreased joint movement as well as causing joint stiffness and pain.
• Decreased range of motion of extremities; older adult may need increased assistance with activities of daily living.
• Slowed movement and decreased muscle strength lead to decreased response time.
BOX 16-1 OLDER ADULT CARE FOCUSMusculoskeletal Changes
• The wider the base of support, the greater the stability. Position your feet wide apart. • The lower the center of gravity, the greater the stability. Flex the knees; let the strong muscles of the legs do the work. • Position yourself close to object and/or client. • Face the client; keep back, pelvis, and knees aligned; avoid twisting. • Balance activity between arms and legs. • Avoid bending to lift; this decreases strain on the back. • Encourage client to assist. • Pivoting, turning, rolling, and leverage require less work. • Person with heaviest load should coordinate team efforts. • Obtainassistancewithheavyordifficulttransfers or lifts. • Teach clients proper body mechanics.
BOX 16-2 BODY MECHANICS
• Itismoredifficulttomaintainimmobilityinthese clients after fractures; therefore surgical intervention (e.g., ORIF) is frequently used for treatment.
• The older client heals more slowly, so use of the affected extremity and weight bearing are frequently delayed.
• Complications of immobility occur more frequently; mobilize hospitalized clients as early as possible.
• Do not rely on fever as the primary indication of infection; decreasing mental status is more common.
• Contractures are more common. Encourage use of assistive devices (canes and walkers).
BOX 16-3 OLDER ADULT CARE FOCUSMusculoskeletal Nursing Implications
• If pain lasts longer than 1 hour after exercise, need to change exercises that involve that joint.
• Plan activity and work schedule to conserve energy: do importanttasksfirst.
• Alternate activities; do not complete all heavy tasks at one time.
• Minimize stress on joints: sit rather than stand, avoid prolonged repetitive movements, move around frequently, avoid stairs or prolonged grasping.
• Use larger muscles rather than smaller ones: use shoulders or arms rather than hands to push open doors; pick up items without stooping or bending, use leg muscles; women can carry purses on their shoulders rather than in their hands.
• Painful,acutelyswolleninflamedjointsshouldnotbe exercised beyond basic ROM.
• Regularly exercise even when joints are slightly painful and stiff: swimming and bike riding maintain mobility without weight bearing.
BOX 16-4 OLDER ADULT CARE FOCUSProtecting Joints
TEST ALERT: Use good body mechanics when providing care – use assistive devises when possible.

342 CHAPTER 16 Musculoskeletal and Connnective Tissue System
1. Putanundershirtontheinfantandplacethebrace ontheoutsideoftheshirt;alwaysplacethebrace strapsontheoutsideofthediaper. 2. Checktheskinundertheharnessforirritationor pressureareas. 3. Donotapplyoilsorlotionsundertheharness. 4. Evaluateperipheralcirculationandmaintainclean- liness.B. Teachparentscastcareifhipspicacastisapplied.
TEST ALERT: Apply or remove immobilizing equipment.
v Goal:Tofacilitatedevelopmentalprogressandadaptnurturingactivitiestomeetneedsofinfantandparents.A. Provideappropriatestimuliandactivityfordevelop- mentallevel.B. Encourageparentstoholdandcuddlechild.C. Maintainnormalhomeroutine.
Herniated Intervertebral DiskThe intervertebral disk forms a cushion between
thevertebralbodiesofthespinalcolumn.Asstressonaninjuredordegenerateddiskoccurs,thecartilagematerialof the disk (nucleus pulposa) herniates inward towardthespinalcolumn,causingcompressionortensiononthespinalnerveroot.
Data CollectionA. Theproblemmostcommonlyoccursinthelumbosacral area.B. Maybecausedbyaninjuryorstresstothelowerback.C. Clinicalmanifestations. 1. Lowbackpainradiatingdownonebuttockandthe posteriorthigh(sciaticapain). 2. Coughing,straining,sneezing,bending,twisting, andliftingaggravatethepain. 3. Lyingsupineandraisingtheleginanextendedpo- sitionwillprecipitatethepain.D. Diagnostics:Appendix16-1
TreatmentA. Medical. 1. Analgesics,musclerelaxants,antiinflammatory medications. 2. Weightreductionifappropriate. 3. Cooltherapy(ice)maybeusedforthefirst24to48 hoursafteraninjury,andthenmoistheatisapplied. 4. Physicaltherapy. 5. Bedrestwithgoodbodyalignmentwhenpainis acute,thenactivitymodificationusinggoodbody mechanics.
✽
B. Surgical. 1. Laminectomy:removaloftheherniatedportionof thedisk. 2. Microlaminectomy(diskectomy):removalofthe herniateddiskwiththeuseofamicroscopeto minimizetheincision.Thereislesstraumainthe diskarea,improvedhemostasis,minimalnerveroot involvement,andquickerrecoveryusingthis procedure.
Nursing Interventionsv Goal:Torelievepainviaconservativemeasuresandpreventrecurrenceofproblem.A. Decreasemusclespasmswithbedrestandmedications.B. Beginambulationslowlyandavoidhavingclientbend, stoop,twist,sit,orlift.C. Instructtheclientregardingtheprinciplesofproper bodymechanics(Box16-2)andanyprescribedmobility limitations.D. Theclientwillneedafirmmattress;clientshouldnot sleeporlieintheproneposition.E. Encouragecorrectposture;avoidprolongedstanding.F. Sitinstraight-backedchairs.v Goal:Toprepareclientforlaminectomy.A. Followgeneralpreoperativenursinginterventions.B. Haveclientpracticelogrollingpreoperatively.C. Haveamaleclientpracticevoidingfromsupine position.D. Explaintoclientthatpostoperativepainisverysimilar topreoperativepain,duetotemporaryinflammation andedemaoftheareaaroundthespinalcord.E. Evaluatebowelandbladderfunction.F. Recordspecificcharacteristicsofpaintoincludeina databasesothatpreoperativepaincanlaterbecom- paredwithpostoperativepain.G. Establishabaselineneurologicassessmentforpostop- erativereference.v Goal:Tomaintainspinalalignmentpostoperativelaminectomy.A. Keepthebedinaflatposition.B. Logrollclientwhenturning.C. Keeppillowsbetweenthelegswhenpositionedonthe side;donotplacepillowundertheknees.D. Elasticstockingsorpneumaticcompressiondevices maybeusedtoincreasevenousreturn.E. Encouragegoodpulmonaryhygiene(e.g.,increasefluid intake;performcoughing,deepbreathing,andspirom- etryexercises).F. Theclientwithmicrodisksurgerywillhavefewerlimi- tationsonmobility.Generally,theclientmayassumea positionofcomfort.v Goal:Tomaintainhomeostasisandassessforcompli-cationspostoperativelaminectomy.

CHAPTER 16 Musculoskeletal and Connnective Tissue System 343
NURSING PRIORITY: A hematoma at the incisional area may cause swelling and pressure resulting in neuro-logical deficits in the lower extremities.
A. Evaluateincisionareaforpossibleleakageofspinalfluidandbleeding.
NURSING PRIORITY: Notify RN or surgeon if clear fluid is leaking from incision.
B. Evaluatecharacteristicsofpain,administeranalgesics.C. Performneurovascularchecksonextremities. 1. Evaluatesensationofextremities. 2. Evaluateabilitytomovefeetandtoes. 3. Evaluatevascularstatusoflegsandfeet.D. Assessforurinaryretentionandlossofsphinctercon- trol.Need to notify RN or physician immediately; it may be an indication of cord compression.Normal bladderfunctionusuallyreturnsin24-48hours.E. Ambulateassoonasindicated(frequentlyonfirstpost- operativedayifnofusionwasdone).Clientwhohasa microdisklaminectonywillhavefewerlimitationson movement.F. Iffusionwasperformed,oftenneedtoapplyaback braceorbodybracebeforeambulation.G. Theclientwiththemicrolaminectomygenerallyexperi- enceslesspain,isfrequentlyoutofbedthedayof surgery,andhasfewercomplications.
NURSING PRIORITY: The laminectomy client frequently has difficulty voiding after surgery. Palpate the suprapubic area to make sure the bladder is not full.
ScoliosisAdolescentidiopathicscoliosisisalateralcurvature
ofthespine.Withouttreatment,itwillseverelyaffecttheshapeofthethoraciccavityandimpairventilation.
Data CollectionA. Mostfrequentlyidentifiedatbeginningofgrowthspurt; morecommoninfemales..B. Visiblecurvatureofthespinalcolumn;headandhips arenotinalignment.C. Whenclientbendsforwardfromthewaist,thereis visibledifferenceintheleveloftheshoulders.Theribs andshoulderaremoreprominentononeside.D. Waistlineisuneven,onehipismoreprominent.F. Defectisprogressiveifnottreated.
✔
✔
✔
✽
TreatmentA. Braceifspinalcurvatureprogresses,Cotrel’straction usedforearlycorrection;Milwaukeebraceusedfor highthoraciccurvatures.B. Surgery:spinalfusionandplacementofarodorinstru- menttomaintainalignmentofthefusedsegment. Therodmaybeleftinplacepermanentlyunlessit becomesdisplacedorcausesdiscomfort.
Nursing Interventionsv Goal:Toidentifydefectsearlyandpromoteeffectiveconservativetherapy.A. Promotehealthprogramsinschoolstoidentifycondi- tion.B. Assistclientandparentstoproperlyusebraces. 1. Ensurebraceisproperlyfittedanddoesnotinadver- tentlyrubbonyprominences. 2. MayputlightT-shirtunderbraceforcomfort. 3. Initiallythebraceisworn20to23hoursperday. 4 Braceisregularlyadjustedtopromotecorrection. 5. Ifprogressisgood,childisweanedfromthebrace duringthedaytimeandwearsitonlyatnight. 6. Supplementalexercisesmaybeprescribed.v Goal:Tomaintainspinalalignmentpostoperativecor-rection(seeprecedingpostoperativelaminectomygoal).v Goal:Tomaintainhomeostasisandassessforcompli-cationspostoperativecorrection(seeprecedingpostoperativelaminectomygoal).
FracturesA disruption or break in the continuity of a bone;
generallyoccursfromatraumaticinjury.A. Pathologicalfracturesoccursecondarytoadisease process.B. Classificationoffractures. 1. Type. a. Comminuted:fracturewithmultiplebonefrag- ments;morecommoninadults. b. Greenstick:anincompletefracturewithbending andsplinteringofthebone;morecommonin children. c. Complete:fracturelineextendsthroughtheen- tirebone;theperiosteumisdisruptedonboth sidesofthebone. d.Impacted:completefracturewithbonefrag- mentsbeingdrivenintoeachother. 2. Classifiedaccordingtolocationonthebone:proxi- mal,middle,ordistal. 3. Simple,closedfracture:doesnotproduceabreakin theskin. 4. Complex,open,orcompound:fractureinvolvesan openwoundthroughwhichthebonehasprotruded.
✽

344 CHAPTER 16 Musculoskeletal and Connnective Tissue System
Data CollectionA. Clinicalmanifestations. 1. Edema,swellingofsofttissuearoundtheinjured site. 2. Pain:immediateandoftensevere. 3. Abnormalpositioningofextremity;deformity. 4. Lossofnormalfunctionduetodisruptionofbone integrity. 5. Falsemovement;movementoccursatthefracture site. 6. Crepitation:palpableoraudiblecrunchingasthe endsofthebonesrubtogether. 7. Discolorationoftheskinaroundtheaffectedarea. 8. Sensationmaybeimpairedifthereisnervedamage.B. Diagnostics-Clinicalmanifestationsandhistory. (Appendix16-1).
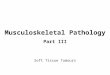
TreatmentA. Immediateimmobilizationofsuspectedfracturearea.B. Fracturereduction. 1. Closedreduction:nonsurgical,manualrealignment ofthebones;injuredextremityisusuallyplacedina castforcontinuedimmobilizationuntilhealing occurs. 2. Openreductionandinternalfixation(ORIF):surgi- calcorrectiontomaintainbonealignmentwithsteel platesandscrews. 3. Externalfixation:applicationofarigidexternal deviceconsistingofpinsplacedthroughthebone andheldinplacebyametalframe(Figure16-1). a.Maybeusedtotreatopencomplicatedfractures. b. Requiresmeticulouscareofpininsertionsiteto preventinfection. c. ProvidesearlymobilityfortheclientC. Traction(Figure16-2). 1. Purposes. a. Immobilizationoffracturesuntilsurgicalcor- rectionisperformed;immobilizationoralign- mentoffractureuntiledemaisdecreased enoughtopermitcasting. b. Decrease,prevent,orcorrectdeformitiesassoci- atedwithmusclediseasesandboneinjury. c. Decreaseorpreventmusclespasms. 2. Types. a. Skeletal:wireormetalpinisinsertedintoor throughtheboneandasystemofweightsand pulleysareusedtomaintainanexternalforce ofpulltotheboneforimmobilizationoffracture site(e.g.,Crutchfieldtongs). b. Skin:forceofpullisapplieddirectlytotheskin andindirectlytotheboneatthefracturesiteto maintainfracturereduction.D. Castapplicationtomaintainimmobilityofaffectedarea aboveandbelowtheinjuredarea.
ComplicationsA. Infection 1. Osteomylitis:infectioninthebone a.Mostoftenhasasuddenonset. b.Tendernessandpainatthesite. c.Morecommoninolderadultswithopenwounds thathavecausedabreakintheperiosteum. 2. Infectionatsiteofwoundorincision,mayprogress toosteomyelitis. a. Infectionmayoccurunderthecast,aroundpin sitesorintheincision. b.Unpleasantodor. c. Purulentdrainage,eitherthroughthecast,orat incisionorpinsites. d. Elevatedbodytemperature. e. Increasedwarmthoncastoverinjuredarea.B. Compartmentsyndrome. 1. Causedbyinternalpressurewithinoraroundthe compartmentsoftissuelinedbyfascia;thefascia doesnotexpandinresponsetoanincreaseinthe contentsofthecompartment(Figure16-3). 2. Anyincreaseinthesizeofthecompartmentdue tobleedingorswellingwillputpressureonthe structures(nervesandvessels)withinthatcompart- ment. 3. Maybecausedbyexternalpressurefromacastor dressingthatistootight. 4. Eitherexternalorinternalpressuremaycauseper- manentdamageifnotrelievedassoonaspossible– itispossibleforpermanentdamagetooccurwithin hours.
FIGURE 16-1 External fixation. (From deWit, S. Medical surgical nursing: concepts and practices, St Louis, 2009, Saunders/Elsevier.)

CHAPTER 16 Musculoskeletal and Connnective Tissue System 345
5. Anearlysignofcompartmentsyndromeispares- thesia;weakpulseorpulselessnessisalatesign. Clientsmaycomplainofathrobbing,severepain unrelievedbyanalgesics. 6. Evidenceofdecreasedcirculationdistaltothein- volvedarea. a.Decreasedqualityofpulsesdistaltotheinjury. b.Painandedema. c. Pale,cool,duskyextremity. d. Decreasedcapillaryrefilltime. 7. Evidenceofpressureonanerve. a. Decreasedsensationtotouch. b. Paresthesia,tingling. c. Impairedmotion. 8. Treatmentisdirectedtowardimmediatereleaseof pressure.Iftheclienthasacast,thecastmaybe “bivalved.”Thecastissplitinhalf,andthehalves aresecuredaroundtheextremitybyawrapsuchas anelasticbandage. 9. Volkmann’scontracture:atypeofcompartment syndromethatoccurswhenpressureisexerted ontheradialorulnarnervesatthewrist,causinga flexioncontractionofthehand.Mostcommonly occurswithfracturestotheelbowandforearm. Theflexioncontractionmaybepermanent.C. Venousstasisandthrombusformationrelatedtoimmo- bility(seeChapter11).D. Fatembolism. 1. Oftenassociatedwithfracturesoflongbones;pri- marilyoccursinadults.
2. Clinicalmanifestationsmostoftenoccurwithin thefirst48hoursofinjury. 3. Fatglobulemovesthroughthevenoussystemtothe lungs. a.Changeinmentalstatus b.Respiratorydistress–tachypnea,tachycardia, petechiaeoveruppertorso. c. Anxietyanddecreasingpulseoximetry.
FIGURE 16-2 Examples of common types of traction (From deWit, S. Medical surgical nursing: concepts and practices, St Louis, 2009, Saunders/Elsevier).
FIGURE 16-3 Compartment syndrome. (From Monahan: Phipp’s W. Medical-surgical nursing: Health and illness perspectives, ed 8, St Louis, 2007, Mosby.)

346 CHAPTER 16 Musculoskeletal and Connnective Tissue System
Nursing Interventionsv Goal:Toprovideimmobilityandemergencycarebe-foretransportingvictim.A. Evaluatecirculationdistaltoinjury.B. Splintandimmobilizeextremitybeforetransfer.C. Iftractionisinitiatedforimmobilization,donotrelease ituntilfurtherevaluationandtreatmentisavailable.v Goal:Toidentifycomplicationsearly,performfre-quentperipheralnerveandvascularassessmentdistaltotheareaofinjury(beforetreatmentandongoingafterimmobili-zationofinjury).A. FivePsofneurocirculatoryassessment(Figure16-4): 1. Pain. a. Location. b. Increasingordecreasing,throbbing,responseto analgesics. c. Precipitatingfactors.
NURSING PRIORITY: Immediately report pain that is unrelieved by analgesics
2. PresenceofperipheralPulses. 3. Pallorofskin. a. Skinpaleandcooltotouch. b. Nailbeds:normalcapillaryrefilloccurswithin 3seconds. 4. Paresthesia(nervecompression). a. Decreasedsensation. b. Numbness,tingling. 5. Paralysis(nervecompression).
B. Evaluateforpresenceofcompartmentalsyndrome– ifanysymptomsarepresent,obtainassistance immediately.
NURSING PRIORITY: It is important for the nurse to be aware of the symptoms of compartment syndrome, identify it early and report it immediately.
C. Fatemboli. a. Monitorclientforchangesinmentalstatus–change inlevelofconsciousness,confusion,disorientation, andlethargy. b. Assessrespiratorystatus,ifhypoxicplaceclientin semitohighFowler’sposition,beginoxygenand staywithclient. c. Anemergentcrisis,staywithclientandrequest assistanceimmediately.
TEST ALERT: Identify client at increased risk for compromised circulation; implement mea-
sures to prevent neurovascular complications; recog-nize client at increase risk for complications.
✔
✔
D. Monitorforpresenceofinfection.v Goal:Tomaintainimmobilizationviatraction(seeFigure16-2).A. Assumethattractioniscontinuousunlessdesignated otherwise.B. Carefullyassesspressurepointsforskinbreakdown, especiallyundertheclient.C. Donotchangeorremovetractionweightsonaclient withcontinuoustraction.D. Thetractionropesandweightsshouldhangfreefrom anyobstructions.E. Tractionappliedinonedirectionrequiresanequal countertractiontobeeffective;client’sweightisthe countertraction. 1. Donotlettheclient’sfeettouchtheendofthebed; itwillcausethecountertractiontobelost. 2. Donotallowthetractionweightstorestonany thingattheendofthebed;thisnegatesthepullof thetraction.F. Carefullyassessthepinsitesforevidenceofinfection inclientswithskeletaltraction,orwithexternalfixa- tion.G. Positiontheclientinthecenterofthebedwiththetrac- tionpullinastraightline.
TEST ALERT: Maintain client traction devices; implement measures to promote venous return.
v Goal:Tomaintainimmobilizationviacast.A. Allowplastercasttodryadequatelybeforehandlingor movingtheclient. 1. Donotcoverthecastwithablanket. 2. Encouragecasttodrybyusingfansandmaintain- ingadequatecirculation. 3. Syntheticcastsdryinabout20minutes;castwill feelwarmduringthedryingprocess. 4. Plastercaststakeseveralhourstodrycompletely; thecastwillalsofeelwarmduringdrying. 5. Avoidhandlingawetcasttopreventindentions, whichmaycausepressureareasinsidethecast.
FIGURE 16- 4 5 P’s of neurovascular assessment (From Zerwekh J. Claborn J. Memory notebook of nursing, Vol 2, 3rd ed, Ingram, Texas, 2007, Nursing Education Consultants).

CHAPTER 16 Musculoskeletal and Connnective Tissue System 347
6. Repositionclientevery2hourstofacilitatethedry ingofallcastsurfaces. 7. “Petaling”acastisdonetocovertherough, crumblingedgesofaplastercast.Smallstripsof waterproofadhesiveareusedtocoverthecase edges.B. Continuetoassessforcompartmentsyndrome.C. Bodyjacketcastandhipspicacast. 1. Evaluateforabdominaldiscomfortduetocastcom- pressionofmesentericarteryagainstduodenum. 2. Reliefofgastricdistention:maybenecessaryto relievegastricdistentionbyanasogastrictubeand gastricsuction. 3. Evaluateforpressureareasoveriliaccrest.D. Donotallowcasttobecomeexcessivelydamportoget wet.E. Elevatecastedextremity,especiallyduringthefirst24 hoursafterapplication.F. Applyicepacksdirectlyovertheareaofinjuryduring thefirst24hours,beingcarefulnottoallowthecastto becomewet.
NURSING PRIORITY: Do not apply any type of heat to a cast to enhance drying.
G. Assessforevidenceofinfection.v Goal:Toprovidecaretoaclientwithanexternalfixa-tiondevice.A. Assessforneurovascularcomplications.B. Inspectexposedskinandpininsertionsitesforsignsof infection.C. Donotuseframetopullorliftclient.D. Framewillberemovedwhenfracturehashealed.v Goal:Topreventcomplicationsofimmobility(seeChapter3).
Home CareA. Clientshouldnot: 1. Bearweightonthecastuntilinstructedtodoso. 2. Allowtheplastercasttogetwet;discussalterna- tivesforbathing. 3. Insertanythingunderorinthecast. 4.Removeanyofthepaddingunderthecast.B. Clientshouldreportanysymptomsassociatedwithswellingorincreasedpain.
NURSING PRIORITY: Check for complications caused by cast, traction, external fi xation device or other immobilizing equipment.
✔
✔
Specifi c FracturesA. Colles’fracture. 1. Fractureofthedistalradius. 2. Primarycomplicationiscompartmentalsyndrome.B. Fracturedpelvis. 1. Frequentlyoccursinolderadultsandisassociated withfalls. 2. Maycauseseriousintraabdominalandurinarytract injury. 3. Bedrestisprescribedfortreatmentofstablefrac- tures. 4. CombinationofexternalfixationandORIFmaybe usedtotreatcomplexfractures. 5. Turnclientonlyonspecificorders.C. Fracturedhip. 1. Commoninwomenover60yearsofage,increased riskinclientswithosteoporosis. 2. Clinicalmanifestations. a. Externalrotationandadductionoftheaffected extremity. b. Shorteningofthelengthoftheaffected extremity. c. Severepainandtenderness. 3. Treatment. a. Initially,Buck’sorRussell’stractionwithsand bagsandtrochanterrolltoimmobilizefracture, decreasemusclespasms,andcontrolexternal rotation(seeFigure16-2). b. Surgicalrepairwhenclient’sconditionallows (permitsearliermobilityandprevents complicationsofimmobility). 4. Nursinginterventionspostoperatively(Box16-3). a. Circulatoryandneurologicalchecksdistalto areaofinjury/surgery. b. Positiontopreventflexion,adduction,andinter- nalrotation,whichmaycausedislocationofthe prosthesis.
• Decreased bone density leads to more frequent fractures.
• Decrease in subcutaneous tissue results in less soft tissue over bony prominences.
• Degenerative changes in the spine alter posture and gait; disk compression causes a loss in height.
• Degenerative changes in cartilage and ligaments result in decreased joint movement as well as causing joint stiffness and pain.
• Decreased range of motion of extremities; older adult may need increased assistance with activities of daily living.
• Slowed movement and decreased muscle strength lead to decreased response time.
BOX 16-1 OLDER ADULT CARE FOCUSMusculoskeletal Changes
• The wider the base of support, the greater the stability. Position your feet wide apart. • The lower the center of gravity, the greater the stability. Flex the knees; let the strong muscles of the legs do the work. • Position yourself close to object and/or client. • Face the client; keep back, pelvis, and knees aligned; avoid twisting. • Balance activity between arms and legs. • Avoid bending to lift; this decreases strain on the back. • Encourage client to assist. • Pivoting, turning, rolling, and leverage require less work. • Person with heaviest load should coordinate team efforts. • Obtainassistancewithheavyordifficulttransfers or lifts. • Teach clients proper body mechanics.
TEST ALERT: Use good body mechanics when providing care – use assistive devises when possible
BOX 16-2 BODY MECHANICS
• Itismoredifficulttomaintainimmobilityinthese clients after fractures; therefore surgical intervention (e.g., ORIF) is frequently used for treatment.
• The older client heals more slowly, so use of the affected extremity and weight bearing are frequently delayed.
• Complications of immobility occur more frequently; mobilize hospitalized clients as early as possible.
• Do not rely on fever as the primary indication of infection; decreasing mental status is more common.
• Contractures are more common. Encourage use of assistive devices (canes and walkers).
BOX 16-3 OLDER ADULT CARE FOCUSMusculoskeletal Nursing Implications
• If pain lasts longer than 1 hour after exercise, need to change exercises that involve that joint.
• Plan activity and work schedule to conserve energy: do importanttasksfirst.
• Alternate activities; do not complete all heavy tasks at one time.
• Minimize stress on joints: sit rather than stand, avoid prolonged repetitive movements, move around frequently, avoid stairs or prolonged grasping.
• Use larger muscles rather than smaller ones: use shoulders or arms rather than hands to push open doors; pick up items without stooping or bending, use leg muscles; women can carry purses on their shoulders rather than in their hands.
• Painful,acutelyswolleninflamedjointsshouldnotbe exercised beyond basic ROM.
• Regularly exercise even when joints are slightly painful and stiff: swimming and bike riding maintain mobility without weight bearing.
BOX 16-4 OLDER ADULT CARE FOCUSProtecting Joints

348 CHAPTER 16 Musculoskeletal and Connnective Tissue System
(1) Donotadducttheaffectedlegpasttheneutral (midline)position. (2) Maintaintheaffectedleginanabductedposi- tion;initiallywithanA-framepilloworby keepingpillowsbetweentheknees. (3) Itisimportanttopreventinternalorexternal rotationand/orabductionoftheoperativehip bytheuseofsandbags,pillows,ortrocanter rollsateachthigh. (4) Avoidgreaterthan90-degreeflexionofthe operativehip,whenoutofbedpositionclient inachairthatprovidessupport,butnotsitting ata90-degreeangleofflexion. (5) Donotallowlegstocrossatthekneesorthe feet.
NURSING PRIORITY: Check with the RN regarding the positioning for clients with fractured hip; positioning for these clients is critical.
c. Evaluatebloodloss. (1) Checkundertheclientforhemorrhage. (2) Measurethediameterofthethightoevaluate thepresenceofinternalbleeding. d. Clientisfrequentlymobilizedonfirstorsecond postoperativedaytopreventcomplicationsof immobility. e. Theclientispronetocomplicationsofimmobility; usethigh-highanti-embolismstockingsorpneu- maticcompressiondevicesonlegs;encouragefoot flexion;low-doseheparinmaybeusedprophy- lactically.D. Ribfractures. 1. Usuallyhealin3to6weekswithnoresidual impairment. 2. Painfulrespirationscauseclient’stobreathmore shallowandrefrainfromcoughing,thisincreased problemsofatelectasis. 3. Chesttapingorstrappingisnotusuallydone becauseitpreventsthoracicexcursionanddeep breathing. 4. Multipleribfracturesmayprecipitatethedevelop mentofapneumothoraxoratensionpneumothorax (seeChapter10).E. Mandiblefracture. 1. Wiringofjaws(intermaxillaryfixation)iscommon treatment. 2. Postoperativeproblems:airwayobstructionand aspirationofvomitus. 3. Wirecuttersatbedsideincaseofemergency a.Suctionclientvianasopharyngealandororal methodsifvomitingoccurs. b.Cutthewiresonlyaslastresortinanemergency (cardiacorrespiratoryarrest).
✔
c.Wirecuttersshouldremainwiththeclientatall times. 4. Oralhygieneisveryimportant–usenormalsaline rinsesaftereatingandasoftcatheterorwaterpik foramorethoroughoralcleansing. 5. Tracheostomysetatbedside. 6. Establishsystemforcommunication-apad/pencil orpictureboardtocommunicatepost-op. 7. Dischargeteaching:oralhygiene,techniquesfor handlingsecretions,diet(problemswithconsti- pationduetolowfiberindiet),alwayskeepwire cutterswiththem.
Hip ReplacementA. Hipreplacementsurgerymaybeperformedtocorrect apathologicalfractureorastreatmentforadisease processsuchasrheumatoidarthritis.B. Preoperativecare. 1. Encourageclienttopracticeusingeithercrutchesor awalker,whicheverisanticipatedtobeusedpost operatively(seeAppendix16-4). 2. Encourageclienttopracticemovingfromthebedto thechairinthesamemannerclientwillperform thistransferpostoperatively. 3. ClientshoulddiscontinueuseofNSAID’sandor aspirinaboutaweekpriortosurgery.
Nursing ImplicationsA. Postoperativecare(seeChapter2). 1. Positionclienttopreventcomplications. a.Supinewithheadslightlyelevated,maintain abductionofaffectedleg,donotusekneegatch onbed. b. Donotallowtheclient’shiptoflexgreaterthan 90degrees;thereforedonotelevatethebed greaterthan60degrees. c. Maintainabductionandpreventexternalrotation ofextremity. d. Whensitting,keepclient’skneesbelowlevelof hip. e. Legsshouldnotbecrossed,eitheratthekneeor theankle. 2. Clientmaybeoutofbedtostandatthebedsideon thefirstpostoperativeday. 3. Encouragepostoperativeexercisestomaintain muscletoneandpreventDVT. 4. Performneurovascularassessmentwithvitalsign checks. 5. Monitorwounddrainage;frequentlythisclientwill haveaportablewoundsuctiondevice. 6. Preventcomplicationsofimmobility a.Carefullymonitorskinforareasofpressure. b.Keepclient’sheelsoffthebedtopreventskin breakdown.

CHAPTER 16 Musculoskeletal and Connnective Tissue System 349
c.Clientisusuallyoutofbedonfirstorsecond postoperativeday. d.Antiembolismstockingsand/orsequentialcom- pressionpumpsonlowerextremitytoprevent venousstasis. e.Low-molecular-weightheparin(seeAppendix 11-3)maybegiventopreventthrombophlebitis anddeepveinthrombosis.
NURSING PRIORITY: After surgery, do not allow the repaired hip to flex greater than 90 degrees; avoid adduction and internal rotation of extremity. Flexion and adduction will dislocate the hip prosthesis (use raised toilet seats, reclining wheelchairs).
7. Observeforsignsofpossiblehipdislocation. a. Increasedhippain. b. Shorteningofaffectedleg. c.Externallegrotation. d.Ifthesesymptomsareobserved,contacttheRN immediately. 8.Painmanagement. a.Paincontrolisfrequentlydifficultsecondaryto age,respiratorystatus,andneedtomobilize client. b.Evaluatepainusingapainscale. c. Epiduralorintraspinalanalgesia,oraPCAmay beused;clientfrequentlyonoralpain medicationonthe2ndor3rdpostoperativeday. d.Utilizenon-pharmacologicmethodsforpainre- lief(seeChapter3). 9. Closelyobservetheincisionalareaforevidenceof infection;feverisnotacommonsignofinfection intheolderadult,assessforchangeinorientation statusandconfusion.
Total Knee ReplacementA. Thissurgeryisoftenperformedtotreatjointcomplica- tionsofarthritis.B. Postoperativecare 1. Clientusuallyreturnsfromsurgerywithacompres- siondressing;monitorneurovascularstatusof extremitydistaltotheoperativesite. 2. Applycoldpackstoincisionsitetodecreaseedema andbleeding. 3. Clientmayhaveaportablewoundsuctiondeviceto removedrainagefromwound. 4. Acontinuouspassivemotion(CPM)devicemaybe used;itpromoteshealingbyincreasingcirculation andmovementofjoint. a.Checksettingsforscheduleofdesignatedhours andflexion. b.Makesurejointispositionedcorrectlyon equipment.
✔
c.Assessclient’stoleranceofmotion. d.Turnmachineoffformealsinbed. e.Providepaddingtopreventpressurepoints. 5. Whenclientisoutofbedinachair,theknee- immobilizingdevicemaybeapplied;elevatethe extremity. 6. Clienthasweight-bearinglimitationspostopera tively;weightbearinggraduallyincreaseswith healing. 7. Painmanagement a.Providecomfort;promoteincreasedactivityand jointmobility. b.Seepaincontrolfortotalhipreplacement,may alsouseperipheralnerveblocks. c.Evaluatepainusingapainscale. 8. Maintainkneeinaneutralposition,donotallow externalorinternalrotation. 9. Assessfordevelopmentofanemia,infection,and DVT. 10. Clientisfrequentlyambulatoryatdischargewith useofassistivedevices.(Appendix16-4)
OsteoporosisAmetabolicbonediseasethatinvolvesanimbalance
betweennewboneformationandboneresorption.A. Primaryosteoporosisismostcommontype;occurs mostofteninwomenaftermenopause.B. Bonelossoccurspredominantlyinthevertebralbodies ofthespineandthefemoralneckinthehip.Asbone massdeclines,thebonebecomesbrittleandweak.
OLDER ADULT PRIORITY: Aging is the major risk factor; protect older adult clients from falls.
Data CollectionA. Clinicalmanifestations(Figure16-5). 1. Maybeasymptomaticuntilx-raysdemonstrate skeletalweakening.Bonelossinexcessof25% occursbeforeosteoporosiscanbeidentifiedon standardx-rays. 2. Spinaldeformityand“dowager’shump.” a. Maybediagnosedafterafractureoravertebral compressionfracture. b. Graduallossofheight. c. Increaseinspinalcurvature(kyphosis). 3. Vertebralfracturesmayoccurspontaneouslyorasa resultofminimaltrauma. 4. Chroniclowthoracicandmidlinebackpain. 5. Heightlossmayprecipitatethoracicproblems,such asadecreaseinabdominalvolumeandexercise tolerance. 6. Hipfracturesandvertebralcompressionare frequentcomplications.
✽
✔

350 CHAPTER 16 Musculoskeletal and Connnective Tissue System
B. Diagnostics. 1. Serumlabvaluesofcalcium,phosphorus,andalka linephosphataseareusuallynormal. 2. Computedtomographytoevaluateboneloss. 3. Bonescantoidentifybonedensity.
TreatmentA. Dietary:increasedintakeofprotein,calcium,and vitaminD.B. Calciumsupplements,andmedicationstoincreasebone density(seeAppendix16-2).C. VitaminDsupplementstoenhanceutilizationofcal- cium.E. Exercise:activitiesthatplacemoderatestressonbones byworkingthemagainstgravity.Weight-bearingexer- ciseisbelievedtodecreasethedevelopmentof osteoporosisandpossiblyincreasenewboneformation. 1. Swimmingandyogamaynotbeasbeneficialbe- causeoflackofstressonbonemass. 2. Walkingfor30minutes3-5timesaweekismost effectiveexercise,alongwithliftingweights.F. Compressionfracturesofthevertebraeusuallyheal withoutsurgicalintervention.
ComplicationsBonefracturesoccurringinthevertebralbodies,distalradius,orthehip.
Nursing Interventionsv Goal:Todecreasepainandpromoteactivitiestodi-minishtheprogressofthedisease.A. Encouragepainreliefmeasures. 1. Bedrestinitiallywithafirmmattress. 2. NarcoticanalgesicsinitiallyfollowedbyNSAIDs.B. Assessbowelandbladderfunction;clientwillbeprone toconstipationandparalyticileusifvertebraeare involved.
C. Encourageregular,dailyweight-bearingexercise; encourageoutdoorexercisesbecausesunlightincreases utilizationofvitaminD.D. Discourageuseofcaffeine,alcohol,andcigarettes.
Home CareA. Decreasefallsandinjurybymaintainingasafehome environment;useassistivedevices.B. Understandneedtocontinuemedications,evenifthey donotmaketheclientfeelbetter.Importantforclientto understandthatthecalciumsupplementsareto preventfurtherdamage.C. Donotexerciseifpainoccurs.D. Avoidheavylifting,stooping,andbending.Reviewand demonstrategoodbodymechanicswiththeclient(Box 16-2).
OsteomyelitisAn infection of the bone, bone marrow, and sur-
roundingtissue.ThemostcommoncausativeorganismisStaphylococcus.
Data CollectionA. Tenderness,swelling,andwarmthinaffectedarea.B. Drainagefrominfectedsiteorwound.C. Fever,chills.D. Constantpaininaffectedarea–getsworsewith activity.E. Maybeachronicprocesswithpersistentproblems andexacerbations.
DiagnosticsA. Woundand/orbloodcultures.
TreatmentA. Preventionisprimarygoal.B. Intensiveintravenous(IV)antibiotics.C. Immobilizationofaffectedarea.D. Surgicaldebridementmaybenecessary.
Nursing Interventionsv Goal:Todecreasepain,promotecomfort,anddecreasespreadofinfection.A. Maintaincorrectbodyalignment. 1. Moveaffectedextremitygentlyandwithsupport. 2. Preventcontracturesbyencouragingjointmobility, especiallyofaffectedextremity. 3. Applywarm,moistsoakstoincreasecirculation andhealing.B. Ifthereisanopenwound,maintainwoundcontactpre- cautions(seeChapter5).C. Clientisusuallydischargedwithantibioticsandshould maintainclosefollow-upcare.
✽
FIGURE 16-5 Progression of osteoporosis. (From Black JM, Hawks JH: Medical-surgical nursing: Clinical management for positive outcomes, ed 7, Philadelphia, 2005, Saunders.)

CHAPTER 16 Musculoskeletal and Connnective Tissue System 351
D. Conditionmaybecomechronicwithreoccurrenceafter primaryinfection.
TEST ALERT: Monitor client’ wounds for infec-tion; identify signs and symptoms of infection.
Malignant Bone TumorsA. Themostcommonprimarybonecancerisosteogenic sarcoma;itadvancesveryrapidlywithmetastasistothe lungsviatheblood(seeChapter2).Bonesmaybea primarysiteorametastaticcancersite. 1. Mostcommonlyaffectsthelongbones,especially thedistalendofthefemur. 2. Primarymalignancymostoftenoccursinmales10 to25yearsold.B. Metastaticbonecanceroccurswhenthereisamalig- nancyinanotherpartofthebodythathasmetastasized tothebone(e.g.,breastandprostatecancer).
Data CollectionA. Clinicalmanifestations:generallynonspecific. 1. Localizedpainandswelling. 2. Tender,palpablebonymass.C. Diagnostics.(SeeAppendix16-1)
TreatmentA. Primarysite:extensiveresectionofareaaroundtumor; amputationmaybenecessary.B. Metastaticsite:identifyandtreatprimarysiteifpos- sible.C. Chemotherapyandradiationmaybeused.(Chapter2)
Nursing Interventionsv Goal:Tomaintainhomeostasisandpreventcomplica-tionsaftersurgery.A. Anextensivepressuredressingwithwounddrains/ suctionmaybepresent.B. ROMisusuallybegunimmediately;continuouspassive motionmaybeusedimmediatelyoronfirstpostopera- tivedayforbothupperandlowerextremitysurgery.C. Muscletoningisimportantbeforeweightbearing.D. Frequentneurovascularassessmentisnecessarybe- causeofresectionofnervesandvesselsinarea; extremitymayalsobecastedorsplintedforsupport.v Goal:Topreventcomplicationsandpromotemobilityafteramputation(seeAppendix16-3).v Goal:Toassisttheclient/childandfamilytocopewiththediagnosisandbuildbasisforrehabilitation.v Goal:Toassisttheclientandfamilytocopewiththediagnosisandbuildabasisforrehabilitation.A. Providehonest,straightforwardinformationtoclient andfamilyregardingthesituation.B. Allowopportunityforclientandfamilytoexpress concernsandfears.
C. Anticipatesenseoflossofcontrolandangerover changesinbody.D. Encouragenormalgrowthanddevelopmentalactivities asappropriate;allowclienttobeasindependentas possible.v Goal:Toassisttheclientandfamilytocopewiththesideeffectsofchemotherapyandradiation(seeChapter2).
Rheumatoid ArthritisAsystemicautoimmunediseasethataffectsallareas
of the body. It produces a chronic inflammatory process involvingconnectivetissue,especiallysynovialjoints.
A. Exacerbationsandremissionsoccur.Conditiontends tobeprogressivewitheachexacerbation.Seldomdoes theclientreturntothepreviousleveloffunctioning beforetheexacerbation.B. Earlydiagnosismaypreventordelaypermanentdam- age.C. Mayoccurinchildrenasjuvenilerheumatoidarthritis.
Data CollectionA. Clinicalmanifestations. 1. Gradualonset. 2. Stiffnessandpainworseinthemorning;generally decreaseduringthedaywithmoderateactivity. 3. Jointinvolvementisbilateralandsymmetrical,most frequentlyinvolvesthehandsandfeet. a. Warm,tender,red,painfuljoints. b. Decreaseinrangeofmotion. c. Decreaseinstrength. 4. Subcutaneousnodulesonthefingers. 5. Systemiceffects. a. Lowfever. b. Malaiseandweakness. c. Anorexiaandweightloss. d. Depression. e. Easilyfatigued. 6. Chronicdeformitiesdevelopmostofteninthe handsandfeet. 7. Exacerbationofsymptomsmaybeassociatedwith physicaloremotionalstress.B. Diagnostics(Appendix16-1).
TreatmentA. Nonsteroidalantiinflammatorydrugs(NSAIDs).B. Corticosteroids.C. Disease-modifyingantirheumaticdrugs(DMARDs) (seeAppendix16-2).D. Heatand/orcoldapplications.E. Physicalandrehabilitativetherapy.F. Surgery:jointreplacements.
Nursing Interventionsv Goal:Torelievepainandpreservejointmobilityandmusclestrength.
✽

352 CHAPTER 16 Musculoskeletal and Connnective Tissue System
A. Usewarm,moistcompressestorelievepainandstiff- nessofmusclespasmsassociatedwithchronicstiff- ness.B. Ifacuteinflammationispresent,coldcompressesmay providerelief.C. Acutelyinflamedjointsmaybeimmobilizedinadevice thatmaintainsafunctionalposition.D. Positionclienttomaintaincorrectbodyalignmentand preventcontractures,especiallyflexioncontractures.E. Performrangeofmotion(ROM)exercisestomaintain jointmobilityandtodecreasepain.F. Antiinflammatorymedicationsshouldbetakenwith mealsorfoodtodecreasegastricupset.G. Ifclientistakingcorticosteroids,medicalidentification shouldbeworn.
NURSING PRIORITY: Nursing care of the client with arthritis is directed toward decreasing pain and maintaining joint function.
v Goal:Toassistclienttounderstandimplicationsofthediseaseprocessandmeasurestopreventjointdeformity,relievepain,andreduceinflammation.(Box16-4).A. Encourageregularlyscheduledrestperiodstorelieve fatigueandpain;amountofrestvarieswiththein- dividualandthediseaseprocess.B. Protectsmalljoints. 1. Maintainjointalignment;avoidpositionsthatpre- cipitatejointcontraction(e.g.,donotusepillow undertheknees;encourageactivitiesthatinvolve pressingdownthefingers). 2. Changepositionfrequently;maintaingoodbody alignment. 3. Uselargemusclegroupsinsteadofsmallerones; avoidrepetitivemovementsinsmalljoints. 4. Modifyhomeroutinetodecreaseoravoidstresson joints:modifydressingactivitiesandotheractivi- tiesofdailyliving(ADLs)asneeded.C. Ifjointbecomespainfulduringexercise,andthepain persistsfor2hoursaftertheexercise,theactivity shouldbeevaluated.D. Discusswithclientimportanceofidentifyingfalsead- vertisingregardingclaimsofcureandreliefofchronic pain.E. EncourageclienttobeindependentinADLsaslongas possible–focusonwhatclientcando.
OsteoarthritisA progressive degenerative joint disease that
primarilyaffectsthesynovialjointsofweight-bearinglongbones. It is nonsystemic and noninfl ammatory.
A. Frequentlyinvolvesjointthathaveexcessiveuse –kneesinathletes,feetingymnastanddancers.B. Hipsandkneesarecommondiseasesites.
✔
✽
Data CollectionA. Clinicalmanifestations. 1. Jointsinvolved. a. Primarilyinvolvesweight-bearingjoints. b. Maybeunilateralandinvolveasinglejoint. c. Jointsofhandsmaybeinvolved. 2. Pain,swellingandtenderness,stiffnessofthejoint. 3. Painoccursonmotionandwithweight-bearing activity. 4. Painincreasesinseveritywithactivity–painbe comesworseasdayprogresses.B. Diagnostics–(Appendix16-1).
TreatmentA. NSAIDsmaybeeffectiveinpainrelief.B. Methotrexatetodecreaseswellingandpain.C. Activitybalancedwithadequaterest.D. Jointinjectionwithcorticosteriods.E. Physicaltherapyandexercise.F. Surgicalinterventionwithjointreplacement.
Nursing Interventionsv Goal:Torelievepain,preventfurtherstressonthejoint,andmaintainfunction.A. Maintainfunctionaljointalignment;desiredposition maynotbepositionofcomfort.B. PlanADLstopreventstressoninvolvedjointsandpro- videadequaterestperiods.C. Usewarmcompressesandhotshowerstoreducestiff- nessandpain.D. Coldcompressesmaybeusedifthejointisacutelyin- flamed.
• Decreased bone density leads to more frequent fractures.
• Decrease in subcutaneous tissue results in less soft tissue over bony prominences.
• Degenerative changes in the spine alter posture and gait; disk compression causes a loss in height.
• Degenerative changes in cartilage and ligaments result in decreased joint movement as well as causing joint stiffness and pain.
• Decreased range of motion of extremities; older adult may need increased assistance with activities of daily living.
• Slowed movement and decreased muscle strength lead to decreased response time.
BOX 16-1 OLDER ADULT CARE FOCUSMusculoskeletal Changes
• The wider the base of support, the greater the stability. Position your feet wide apart. • The lower the center of gravity, the greater the stability. Flex the knees; let the strong muscles of the legs do the work. • Position yourself close to object and/or client. • Face the client; keep back, pelvis, and knees aligned; avoid twisting. • Balance activity between arms and legs. • Avoid bending to lift; this decreases strain on the back. • Encourage client to assist. • Pivoting, turning, rolling, and leverage require less work. • Person with heaviest load should coordinate team efforts. • Obtainassistancewithheavyordifficulttransfers or lifts. • Teach clients proper body mechanics.
TEST ALERT: Use good body mechanics when providing care – use assistive devises when possible
BOX 16-2 BODY MECHANICS
• Itismoredifficulttomaintainimmobilityinthese clients after fractures; therefore surgical intervention (e.g., ORIF) is frequently used for treatment.
• The older client heals more slowly, so use of the affected extremity and weight bearing are frequently delayed.
• Complications of immobility occur more frequently; mobilize hospitalized clients as early as possible.
• Do not rely on fever as the primary indication of infection; decreasing mental status is more common.
• Contractures are more common. Encourage use of assistive devices (canes and walkers).
BOX 16-3 OLDER ADULT CARE FOCUSMusculoskeletal Nursing Implications
• If pain lasts longer than 1 hour after exercise, need to change exercises that involve that joint.
• Plan activity and work schedule to conserve energy: do importanttasksfirst.
• Alternate activities; do not complete all heavy tasks at one time.
• Minimize stress on joints: sit rather than stand, avoid prolonged repetitive movements, move around frequently, avoid stairs or prolonged grasping.
• Use larger muscles rather than smaller ones: use shoulders or arms rather than hands to push open doors; pick up items without stooping or bending, use leg muscles; women can carry purses on their shoulders rather than in their hands.
• Painful,acutelyswolleninflamedjointsshouldnotbe exercised beyond basic ROM.
• Regularly exercise even when joints are slightly painful and stiff: swimming and bike riding maintain mobility without weight bearing.
BOX 16-4 OLDER ADULT CARE FOCUSProtecting Joints

CHAPTER 16 Musculoskeletal and Connnective Tissue System 353
E. Acutelyinflamedjointmaybeimmobilizedwitha splintorbrace.F. Maintainregularexerciseprogram,decreaseactivityin affectedjoints.v Goal:Toassistclienttounderstandmeasurestomain-tainhealth.(Box16-4)A. Identifyactivitiesrequiringincreasedstressonin- volvedjoints.B. Encourageregularexerciseprogramtopreservemuscle strengthandjointmobility,protectaffectedjoints (activitiesthatdonotcausejointstress,suchasswim- ming).C. EncourageindependenceinADLs.v Goal:Tomaintainpsychologicalequilibriumandpro-motepositiveself-esteem(seeprecedingrheumatoidarthritisgoal).
TEST ALERT: maintain correct body align-ment; monitor client response to interventions
to prevent complications; implement measures to main-tain range of motion.
GoutAnarthriticconditionresultingfromadefectinthe
metabolismofuricacid(hyperuricemia).
Data CollectionA. Clinicalmanifestations. 1. Characterizedbyremissionsandexacerbationsof acutejointpain.
✽
2. Onsetisgenerallyrapid. 3. Intensepainandinflammationofoneormoresmall joints,especiallythejointinthelargetoe. 4. Presenceoftophioruricacidcrystalsonthebigtoe ortheouterear.B. Diagnostics:persistenthighserumuricacidlevels.
TreatmentA. Antigoutmedications(seeAppendix16-2).B. Decreasedietaryintakeofpurine(seeChapter3).C. Avoidaspirin,alcohol,anddiuretics,astheymay precipitateanattack.
Nursing Interventionsv Goal:Topreventacuteattack,promotecomfort,andmaintainjointmobility.A. Medicationsshouldbetakenearlyintheattacktode- creasetheseverity.B. Protectaffectedjoint. 1. Immobilizethejoint. 2. Elevatethejoint. 3. Noweight-bearingactivityonthejoint.C. Coldpacksmaydecreasepain.D. Provideclientwithinformationregardingalow-purine diet.E. Encouragehighfluidintaketoincreaseexcretionof uricacidandtopreventthedevelopmentofuricacid kidneystones.F. Frequentlyrequirespainmedication.
Study Questions: Musculoskeletal System
1. Whatnursingobservationswouldcausethenursethe mostconcernforaclientwhois3dayspostoperative forabelow-the-kneeamputation? 1 Warmthattheendofthestump. 2 Serosanguineousdrainageonthedressing. 3 Brightredbloodonthedressing. 4 Bilateralfemoralpulsesof80beatsperminute.2. Aclientisadmittedwithafracturedhip.Beforesur- gerytheclientisplacedinBuck’straction.Whatisan importantnursinginterventionforthisclient? 1 Removethetractionbootevery4hourstocheck circulation. 2 Checkthepinsitesforinfectionandcleanthem threetimesaday. 3 Checkforadequatecirculationatthefracturesite. 4 Makesuretheclient’sfeetarenottouchingtheend ofthebed.3. Thenurseischeckingaclientforcapillaryrefill.What isthenormaltimeforthenailbedtoreturntoitspink color? 1 1minute. 2 2to3seconds.
3 10seconds. 4 15seconds.4. Theclienttellsthenursethatheisfeelingpaininthe areawherehisleghasbeenremoved.Whatisthebest nursingresponse? 1 Becausetherewasseverepaininthatareaprevi- ously,thisisasubconsciouspain. 2 Thepainisreferredfromanotherareathatis injured. 3 Theinjurednerveendingsdonotaccuratelyreflect theareaofthepain. 4 Thisispainthatisactuallyoccurringatthestump.5. Aclientisbeingtreatedwithalonglegcastforhisleg fracture.Whatareimportantnursingmeasureswhile thecastisstillwet? 1 Thefingertipsshouldbeusedwhenhandlingthe cast. 2 Supportthecastonapillowwithaplasticcover. 3 Applyaheatlampandafantoacceleratethedrying time. 4 Donotrepositiontheclientuntilthecastisdry.

354 CHAPTER 16 Musculoskeletal and Connnective Tissue System
6. Aclienthasacomminutedfractureoftherighttibia andfibula.Anexternalfixationdevicehasbeenap- pliedtothelegforfractureimmobilization.Thisclient isatincreasedriskforwhatpostoperativecomplication? 1 Osteomyelitis. 2 Poorbonerealignment. 3 Hipflexioncontraction. 4 Venousstasisandpulmonaryemboli.7. Anolderadultclienthadafracturedhiprepaired.The clientreturnstotheunitwithawounddrainagesystem thatisconnectedtolowsuction.Overthenext4hours, theclienthas75mLofbrightredbloodydrainage. Whatisthebestnursingaction? 1 Notifythephysicianoftheabnormalamountof bleedinginthecontainer. 2 Emptythedrainagecontainer,recordtheamount, andcontinuetoobserve. 3 Applypressureattheincisionalareaandevaluate forincreaseindrainage. 4 Checktheoperativerecordfortheplacementofthe drain.8. Thenurseischeckingachildinalefthipspicacast andsuspectsaninfection.Whatfindingswouldvalidate thenurse’sconclusion? 1 Increasedcomplaintsofpainandahotspotfound overtheincisionarea. 2 Complaintsofitchinganddiscomfortinsidethecast. 3 Duskycoloredtoeswithweakpedalpulses. 4 Tinglingofthelegwitha3-secondcapillaryrefill.9. Aclienthasacompoundfractureofhisleftfemur.He hasrequiredanincreasedamountofpainmedication, butwithouttherapeuticresults.Whatcomplication shouldthenurseassessforinthisclient? 1 Infection. 2 Compartmentsyndrome. 3 Deepveinthrombosis. 4 Musclecramping.10. Aclientcomplainsthattheplastercastonhislegisrub- binghisskinraw.Whatisthebestnursingaction? 1 Callthephysiciantohavethecastcutback. 2 Applyaloeveralotiontotheirritatedarea. 3 Petaltheedgesofthecast. 4 Increasetheclient’spainmedication.11. Thenurseiscaringforaclientwhoisexperiencingan exacerbationofherrheumatoidarthritis.Herhandsand fingersarepainful,swollen,andinflamed.Whatis animportantnursingmeasureforthisclient? 1 Assistwithactiverange-of-motionexercisesinthe affectedextremity. 2 Placeclient’shandsinapositionofcomfortand applycoldpacks. 3 Applywarmpackstoincreasecirculationtothearea. 4 Explaintheimportanceoftherapeuticjointexer- cisestoincreasemobility.12. AnadolescentisplacedinBuck’stractionfortempo- raryreductionofafemoralfracture.Theclientis scheduledforanopenreductionandinternalfixation
ofthefracture.Beforesurgery,whatwouldbean importantnursingintervention? 1 Evaluatethequalityofthepulsesproximaltothe temporarycast. 2 Checktheclient’sfeettomakesuretheyarenot touchingtheendofthebed. 3 Evaluateundertheclientforskinbreakdown. 4 Checkthepinsitesforinflammationandpurulent drainage.13. Thenurseiscaringforaclientintheimmediatepost- operativeperiodfollowingalumbarlaminectomy. Whatnursingobservationswouldcausethenursethe mostconcern? 1 Complaintsofpainwhenmovingeitherleg. 2 Painradiatingdownthehipandthigh. 3 Bilaterallydelayedcapillaryrefillonthelower extremities. 4 Complaintsofnumbnessandtinglingintheclient’s rightfoot.14. Whatisthenursingmanagementforaclientinbal- ancedsuspensiontraction? 1 Positionclientwithhisfeetagainsttheendofthe bedtopreventfootdrop. 2 Removetheweightstoallowtheclienttoreposition himself. 3 Adjusttheweightsevery8hourstoimprovequality ofcirculation. 4 Checktheweightstomakesuretheyarehanging freelyinplace.15. Aclientislearningtousecrutches.Whatisimportant forthenursetoteachtheclient? 1 Whengoingupstairs,advancetheaffectedlegfirst. 2 Theaxillarybaronthecrutchesshouldbefirmlyin theaxillaryareaforfullweightbearing. 3 Alwayskeeparmsandelbowsstraightwhen walking. 4 Theaxillarybaronthecrutchesshouldbetwo fingerswidthbelowtheaxillaryarea.16. Awomanisgoingtobetakingalendronate(Fosamax) fortreatmentofherosteoporosis.Thenurseisdis- cussingwiththewomanhowsheshouldtakethemedi- cation.Whatisveryimportanttoincludeinthisdiscus- sion? 1 Themedicationmustbetakenonanemptystom- ach,andnofoodmustbeeatenforatleast30 minutesafterthemedicationistaken. 2 Themedicationshouldbetakenwithaminimal amountofwater,andtheclientshouldliedown aftertakingit. 3 Theclientshouldtakethemedicationeverynightat bedtime,andsheshouldnotsuddenlystoptakingit. 4 Orthostatichypotensionmaybeapotentialside affect,sosheshouldstandupslowlyandmakesure shehasherbalance.
Answers and rationales to these questions are in the section at the end of the book titled Chapter Study Questions: An-swers and Rationales.

CHAPTER 16 Musculoskeletal and Connnective Tissue System 355
Appendix 16-1 DIAGNOSTIC STUDIES
Serum Diagnostics
Rheumatoid factor (RF):Usedtodeterminepresenceofautoantibodies(rheumatoidfactor)foundinclientswithconnectivetissuedisease;ifantibodyispresent,itissuggestiveofrheumatoidarthritis;thehighertheantibodytiter,thegreaterthedegreeofinflammation.Antinuclear antibody (ANA): Identifiesthepresenceofantibodiesthatdestroythenucleusofbodytissuecells(i.e.,thoseseeninconnectivetissuediseases);apositivetestresultisassociatedwithsystemiclupuserythematosus.Creatine kinase (CK):Elevatedlevelsfoundinmusculardystrophyandtraumaticskeletalmuscleinjury.
Invasive Diagnostics
Arthroscopy: Involvestheuseofanarthroscopeinsertedintoajointforvisualizationofthejointstructure;procedureisusuallyconductedintheoperatingroomandperformedwitheitherlocalorgeneralanesthesia;frequentlyusedtodiagnosestructuralabnormalitiesoftheknee.
Nursing Implications1. Performpreoperativenursinginterventions,appropriateforthelevelofanesthesiatobeused.2. Afterprocedure,woundiscoveredwithasteriledressing.3. Acompressionbandagemaybeappliedfor24hoursafterthetest.4. Teachclientsymptomsofvascularcompromise,mobilityrestrictions,anddressingchangeprocedure.5. Weightbearingmaybelimited,walkingispermitted;however,excessiveexerciseshouldbeavoidedforafewdays.6. Teachtheclientsignsofinfection(increasedtemperature,localinflammation,anddrainageatsite).Arthrocentesis:Incisionofajointcapsuletoobtainsamplesofsynovialfluid;localanesthesia,andasepticpreparationisdonebeforefluidaspiration.Synovialfluidisexaminedforinfectionandbleedingintothejointandtoconfirmspecifictypesofarthritis.
Nursing Implications1. Explainproceduretoclient.2. Maybedoneatbedsideorinanexaminationroom.3. Compressiondressingisusuallyapplied,andjointisrestedforseveralhoursaftertest.4. Observedressingforleakageofbloodorfluid.5. Assessthepuncturesiteforevidenceofinfection.Myelogram and CT scan:Usedtodeterminestatusofvertebraldisk.SeeAppendix15-1.Bone biopsy: Maybeperformedinclient’sroomorinatreatmentroom.Localanesthesiaisusedandalongneedleisinsertedintothebone,orasmallincisionismadetoobtainbonetissue.
Nursing Implications1. Planforanalgesictobeadministeredbeforeprocedure.2. Ifanincisionwasmade,maintainapressuredressingoverthesite.3. Extremityiselevatedtodecreaseedemaandmaybeimmobilizedforabout12to24hours.4. Assessthepuncturesiteorincisionforevidenceofinfection.Electromyelogram (EMG):Evaluatestheelectricpotentialofthemusclewithmusclecontraction.Smallneedlesareinsertedintothemuscleandrecordingofelectricalactivityisperformed.
Nursing Implications1.Explaintoclientthatthereisdiscomfortwithprocedure.2.Nostimulants(caffeine)orsedatives24hoursbeforetheprocedure.
Noninvasive DiagnosticsX-ray films: Themostcommondiagnosticproceduretodeterminemusculoskeletalproblems.1. Identifymusculoskeletalproblems.2. Determineprogressofdiseaseorcondition.3. Evaluateeffectivenessoftreatment.Bone scan:Radioisotopesmaybeinjectedintravenously,andboneisscannedtodeterminewheretheisotopesare“takenup.”Maybeusedtodeterminepresenceofmalignancies,arthritis,andosteoporosis.Nospecialprecautionsbeforeoraftertest;needtoencouragefluidintaketoincreaseexcretionofdye.Computerized axial tomography (CAT scan): SeeAppendix15-1.Magnetic resonance imaging (MRI): SeeAppendix15-1.

356 CHAPTER 16 Musculoskeletal and Connnective Tissue System
Appendix 16-2 MEDICATIONS
Medications Side Effects Nursing Implications
AnTiGouTAGenTS:Decreasetheplasmauricacidlevelseitherbyinhibitingthesynthesisofuricacidorincreasingtheexcretionofuricacid.
Colchicine:PO
Allopurinol(Zyloprim):PO
Probenecid(Benemid):PO
Nausea,vomiting,diarrheaToxiceffects:bonemarrowdepression
Rash,GIdistress,fever,headache
GIdisturbances,headache,skinrash,fever
1. Takemedicationatearliestindicationofimpendinggoutattack.2. Takemedicationwithfood.3. Encouragehighfluidintaketopromoteuricacidexcretion.4. Inacuteattack,administer1tableteveryhouruntilsymptomssubside,untilGIproblemsoccur,oruntilatotalof8mghasbeentaken.
1. Administerwithfoodtodecreasegastricupset.2. Discontinuemedicationifrashoccurs.3. Usewithcautioninclientswithrenalinsufficiency.4. Maybeusedtodecreaseserumuricacidlevelsinclientsreceivingchemotherapy.
1. Uratetophidepositsshoulddecreaseinsizewiththerapy.2. Givewithfood.
SkeleTAlMuScleRelAxAnTS:Relaxskeletalmusclebydepressingsynapticpathwaysinthespinalcord.
Methocarbamol(Robaxin):PO,IM,IV
Cyclobenzaprine(Flexeril):POCarisoprodol(Soma)
Baclofen(lioresal):PO
Dantrolene(Dantrium):PO,IV
Drowsiness,dizziness,GIupset,rash,blurredvision
Drowsiness,dizziness,headache,GIupset,orthostatichypotension.
Drowsiness,weakness,fatigue,confu-sion
Hepatotoxicity,muscleweakness,drowsiness
1. Usedtotreatmusclespasms.2. Cautionclientstoavoidactivitiesthatrequirementalalertnessforsafety(driving,usingpowertools,etc.).3. AdviseclienttoavoidCNSdepressants(e.g.,alcohol,opioids,antihistamines).4. AdministerwithmealstodecreaseGIdistress.
1. Teachclientssymptomstoreportanyyellowingskinoreyes,itmayindicateaproblemwithliverfunction.2. Actsdirectlytorelaxskeletalmuscle.
cAlciuMMeDicATionS:Hormonesthatenhancebonedensitybypreventingthereabsorptionofcalciuminboneandkidneys.
Calcitonin-salmon(calcimar,Miacalcin):subQ,IM,nasalspray
Bisphosphonates—alendronate(Fosamax),ibandronate,(Boniva):PO,nasalspray
GIupset,localinflammationatinjec-tionsite,flushing
Esophagitis,GIflushing,rash,musculoskeletalpain,fever,chills,jawpain
1. Monitorlevelsofserumcalcium.2. Treatmentofestablishedpostmenopausalosteoporosis.
1. Haveclientswallowtabletwhole;itshouldnotbechewed.2. Takeinmorningonanemptystomachwithlargeglassofwater(6to8oz)andwaitatleast30minutesbeforeeatingorlyingdown.3. EncourageclienttotakesupplementalvitaminD.4. Usedforpreventionandtreatmentofpostmenopausalosteoporosis.
coRTicoSTeRoiDS:SeeAppendix5-7.
Continued

CHAPTER 16 Musculoskeletal and Connnective Tissue System 357
Appendix 16-2 MEDICATIONS—cont’d.
Medications Side Effects Nursing Implications
DiSeASe-MoDiFyinGAnTiRheuMATicDRuGS(DMARDs):Antimetabolite,antirheumatic,andantimalarialdrugsthatactto decreaseinflammation.
(Rheumatrex)
Hydroxychloroquine(Plaquenil)
Leflunomide(Arava)
Toxic effects:hepatotoxicity,bonemarrowdepressionNausea,vomiting,stomatitis
Toxic effects:retinopathy,skeletalmusclemyopathyorneuropathyHeadache,anorexia,dizziness
Toxic effects:hepatotoxicity,diarrhea,teratogenesis
1. Cautionwomenofchildbearingagetoavoidpregnancy.2. MonitorCBCregularly.3. Avoidalcoholduringtherapy.4. Administerwithfood.
1. Recommendeyeexamsevery3months.2. Notrecommendedforchildren.3. Therapeuticeffectmaynotbeevidentfor3to6months.
1.Notrecommendedforwomenwhomaybecomepregnant.2.Mayslowtheprogressionofjointdamagecausedbyrheumatoidarthritisandimprovesphysicalfunction.
BioloGicAlTheRAPy:AgentsthatbindTNFtodecreaseinflammatoryandimmuneresponses;usedincasesofseverearthritis.
Etanercept(enbrel):subQ
Infliximab(Remicade):IVAdalimumab(humira):subQ
Increasedriskforinfections,injectionsitereactions,heartfailure,headache,nausea,dizziness
Increasedriskforopportunisticinfections,abdominalpain,nausea/vomiting,headache,rash,injectionsitereactions
1. Usecautiouslyinclientswithheartdisease.2. Rotateinjectionsitesatleast1inchapart.3. Adviseclientsthatinjectionsitereactiongenerallydecreaseswithcontinuedtherapy.4. Donotadministertoclientswithchronicorlocalizedinfections.5.Haveclientreportsignsofinfection,bruising,orbleeding.
1. Avoidinclientswithheartdisease.2. Assessclientsforinfections;administerTBskintestandchestx-raybeforestartingmedication.3. Rotateinjectionsitesatleast1inchapart.4. PerformperiodicCBCstomonitorforblooddyscrasias.
nonSTeRoiDAlAnTiinFlAMMAToRyMeDicATionS(nSAiDS):SeeAppendix5-8.
CBC,Completebloodcount;CHF,congestiveheartfailure;CNS,centralnervoussystem;GI,gastrointestinal;IV,intravenous;PO,bymouth(orally);subQ,subcutaneous;TNF,tumornecrosisfactor.

358 CHAPTER 16 Musculoskeletal and Connnective Tissue System
Appendix 16-3 AMPUTATIONS
Removalofallorpartofanextremity.Theprecipitatingproblemdeterminesiftheamputationisanelectiveoranemergencyprocedure.
POSTOPERATIVE CAREResidual limb wound care1. Theresiduallimbmaybeelevatedforapproximately24hours;afterthattime,keepthejointimmediatelyabovethelimbinanextended position.Flexioncontracturehinderstheuseofaprosthesis.2. Discussthephenomenonofphantomlimbpain;itdoesnothelpforthenursetopointouttotheclientthattheextremityisgone.3. Administeranalgesics;assisttheclienttodifferentiatebetweenincisionalpaininresiduallimbandphantomlimbpain;phantomlimb painisveryrealtotheclient.4. Theresiduallimbmaybeelevatedforashorttimepostoperativelytodecreaseedema;theskinflapshould bepinkandtheareashouldbewarmwithminimumdrainage.5. Arigidcompressiondressing(plastermoldedoverthewounddressing)maybeappliedtopreventinjuryandtodecreaseswelling. Controllingtheedemawillenhancehealingandpromotecomfort.6. Iftheclientisnotfittedwitharigidcompressiondressing,theresiduallimbwillbeshapedwithacompressionbandage.7. Compressionwrappingwithelasticbandageshouldbeappliedinadistaltoproximaldirection.Toprotectcirculationafigure8wrapping shouldbeusedwithdecreasingpressurewhilewrappingfromthedistaltotheproximalarea.8. Forclientwithabovetheknee(AKA),orbelowthekneeamputations(BKA),encouragerangeofmotionexercises,especiallytotheknee andthehip.Discourageprolongedtimeinsemi-Fowler’spositionintheclientwithabove-the-kneeamputation;thispositionencourages flexioncontractionatthehip.9. ForclientswithaAKA,encouragerestinginapronepositionfor30minutesevery3-4hours.
Residual limb care after wound has healed1. Continuallyassessforskinbreakdown;visuallyinspecttheresiduallimbdaily.2. Theresiduallimbshouldbewashed,carefullyrinsed,anddrieddaily.Soapandmoisturecontributetoskinbreakdown.3. Donotapplyanythingtotheresiduallimb(alcoholincreasesskindrynessandskincracking;lotionskeepskinsoftandhinder prostheticuse).4. Clientshouldputtheprosthesisonwhenhe/shegetsupanditshouldbewornallday.Theresiduallimbtendstobecomeedematousifthe prosthesisisnotapplied.Themoretheclientwearstheprosthesis;thelessedemawilloccur.
TEST ALERT: Provide support to client with changes in body image. Maintain correct body alignment of cli-ent. Monitor client mobility, gait, and strength.
NURSING PRIORITY: Be familiar with the nursing management of a client with an amputated extremity, especially regarding positioning to prevent contractures

CHAPTER 16 Musculoskeletal and Connnective Tissue System 359
Appendix 16-4 ASSISTIVE DEVICES FOR IMMOBILITY
CrutchesMeasuring a Client (Figure 16-5)
• Measurementmaybetakenwithclientsupine,orstanding.
• Supine-measurethedistancefromtheclient’saxillatoapoint6inches
lateraltotheheel.
• Standing–measurethedistancefromtheclient’saxillatoapoint4
-6inchestothesideand4-6inchesinfrontofthefoot.
• Adjusthandbarssothatclient’selbowsareflexedapproximately30
degrees.
• Ifclientwasmeasuredwhilesupine,assistclienttostandwithcrutches.
Checkthedistancebetweenclient’saxillaandarmpieces.You
shouldbeabletoputtwoofyourfingersbetweenclient’saxillaandthe
crutchbar.
Three-Point Alternate Crutch Gait• Mostcommongaitforclientswithmusculoskeletalinjuries.
• Theclientmustbeabletobearthetotalbodyweightononefoot;the
affectedfootorlegiseitherpartiallyortotallynon-weight-bearing.
• Inthisgaitbothcrutchesaremovedforwardtogetherwiththeaffectedleg
whiletheweightisbeingbornebytheclient’shandsonthecrutches.The
unaffectedlegisthenadvancedforward.
Crutch Walking• upstairs:Unaffectedlegmovesupfirst,followedbythecrutchesandthe
affectedleg.
• Downstairs:Whilebearingweightonunaffectedleg,crutchesaremoved
tolowerstairandclienttransfersweighttocrutchesandmovesaffectedleg
first,bodyweightistransferredtothecrutches,andtheunaffectedlegis
moveddown.
Canes• Thecaneisusedonthesideoppositetheaffectedlegandtheelbowshouldbeflexednomorethan30°.
• Thecaneandtheaffectedlegmovetogether.
• Thetopofthecaneshouldbeparalleltothegreatertrochanterofthefemur.
Walkers• Liftthewalkerandplaceitapproximately12-18inchesinfront;makesureall4feetofwalkerarerestingonthefloor.Whilerestingon
walker,stepforwardwithweakerlegfirst,takealternatingsmallstepstowardwalker.
• Gainbalancebeforemovingwalkerforwardagain;balanceprovidesstabilityandequalweightbearing.
TEST ALERT: Assess client’s use of assistive devices; evaluate correct use; assist client to ambulate with an assistive device.
FIGURE 16-6 Crutch measurement (From Harkreader H, Hogan MA: Fundamentals of nursing: Caring and clinical judgment, ed 2, Philadelphia, 2004, Saunders).













![Dynamic skin deformation simulation using musculoskeletal ......Dynamic skin deformation simulation using musculoskeletal model and soft tissue dynamics 3 method [15–17] or the finite](https://img.pdfslide.net/doc/110x75/600f1e2fc3ebee442d49627d/dynamic-skin-deformation-simulation-using-musculoskeletal-dynamic-skin-deformation.jpg)