Embed Size (px)
Citation preview
Pain Management with ChildrenIssue #45, November 2016
1
ChiPPS E-Journal Pediatric Palliative and Hospice Care
Issue #45; November, 2016
Issue Topic: Pain Management with Children
Welcome to the 45th issue of the ChiPPS E-Journal. This issue of our E-Journal offers a collection of articles that explore selected issues in managing pain with children. These articles offer suggestions for and examples of engaging in this important aspect of providing pediatric palliative/hospice care. We appreciate that a single issue on this subject will not do complete justice to this very broad subject area, but we hope that the articles in this issue will spur increased awareness and discussion of this subject. We are planning to follow this issue with one on symptom management with children. We welcome communications from anyone who has more to offer on these subjects.
This E-Journal is produced by ChiPPS (the Children’s Project on Palliative/Hospice Services), a program of the National Hospice and Palliative Care Organization and, in particular, by NHPCO’s E-Journal Work Group, chaired by Christy Torkildson. Archived issues of this publication are available at www.nhpco.org/pediatrics.
Comments about the activities of ChiPPS, its E-Journal Work Group, or this issue are welcomed. We also encourage readers to suggest topics, contributors, and specific ideas for future issues. Please contact Christy at [email protected].
Produced by the ChiPPS E-Journal Work Group
Donna Armstrong, MSW, CSW, Instructor, College of Social Work, University of Kentucky, Lexington, KY Charles A. Corr, PhD, Member, Board of Directors, Suncoast Hospice Institute, Pinellas County, FL; Senior
Editor Ann Fitzsimons, BS, MBA, Executive Director, here4U, Inc., Farmington Hills, MI Erin Gaab, PhD, Postdoctoral Scholar, University of California Merced, Health Sciences Research Institute,
Merced, CA Betsy Hawley, MA, Executive Director, Pediatric Palliative Care Coalition, Pittsburgh, PA Maureen Horgan, LICSW, ACHP-SW, Executive Director, Gentiva Hospice, Seattle, WA Melissa Hunt, PharmD, Pediatric Clinical Pharmacist, HospsiScript, an Optum Company, Montgomery, AL Nathan Ionascu, MD, Bioethics Consultant, Westchester End-of-Life Coalition, Westchester County, NY Randy Johnson, MDiv, Chaplain, Pikesville Hospital, Pikesville, KY Kelly Cronin Komatz, MD, MPH, FAAP, FAAHPM, Clinical Medical Director, Community PedsCare Program,
Medical Director, Pain and Palliative Care, Wolfson Children’s Hospital and Wolfson Center for the Medically Complex Child at University of Florida, Jacksonville, FL
Rachel Levi, PhD, Licensed Psychologist, Private Practice, Oakland, CA Suzanne Toce, MD, Retired Neonatologist, Gundersen Lutheran Health System, La Crosse, WI Rebecca Simonitsch, MS, MAEd, CT, CCLS, Advance Care Planning Coordinator, Cottage Health, Santa
Barbara, CA; UCSB Extension, Instructor Christy Torkildson, RN, PHN, MSN, PhD, Palliative Care Coordinator, UCSF Benioff Children's Hospital,
Oakland, CA; Chair
-###-

2
Issue #45: Pain Management with Children (Click on the “bookmark” tab on the left-hand side of the PDF document for links to the following articles.) I Often Wonder p. 4 Scott Newport Here is a new poem by our “resident poet” together with a photo of him and a caboose he built for an ill child. Pediatric Pain Assessment p. 5 Sheri G. Stewart, MSN, RN-BC, CHPPN Ms. Stewart provides a clear brief review for pediatric pain assessment and includes a list of tools and important points to remember during the assessment. Pediatric Pain Management Strategies p. 10 Melissa Hunt, PharmD Dr. Hunt reviews the components to be considered when initiating and administering pain medications in children, adolescents, and young adults. She not only provides a comprehensive table for the route, but pertinent information for the remaining three components clock, ladder, and child. Patient-Specific Opioid Selection Considerations in Children p. 14 Melissa Hunt, PharmD Dr. Hunt adds to her contribution for our readers by providing a comprehensive review for the selection of the correct opioid to be used for pain management in children of all ages and including non-opioid considerations. Virtual Reality as a Complementary Therapy to Ease Pain and Anxiety in Children p. 20 Simon Robertson, Anurag K. Agrawal, MD, Marsha Treadwell, PhD, Carolyn Hoppe, MD, & Anne Marsh. MD Dr. Marsh and her team, including Founder and CEO of kindVR, Simon Robertson, share with us their experience using Virtual Reality to assist in pain and anxiety management in children and adolescents. A new and exciting field. A Role for Palliative Care in the Pain of Childhood Sickle Cell Disease p. 23 Toluwalase (Lase) A. Ajayi, MD, & Kyle P. Edmonds, MD Drs Ajayi and Edmonds highlight the benefit of palliative care integrated into the care of patients with a chronic, congenital condition such as Sickle Cell Disease. Assessment and Management of Pain and Irritability in Children with Severe Neurologic Impairment (SNI): An Overview in in Children with Severe Neurologic Impairment p. 26 Lanna Olson, MD FRCPC Most palliative care programs have a population of children with severe neurologic impairment from multiple etiologies, known and unknown. Dr. Olson highlights the challenges in recognizing and treating pain in this unique population and explores some of the research that is currently being done in this field. Nonpharmacological Pain Management for Children p. 30 Kathy Davis, PhD, MSEd Dr. Davis provides a fine article on non-pharmacological management of pain in children as well as an excellent review of pain management and the stages of development. In addition to a comprehensive list of references, Dr. Davis includes two examples of Individualized Pain Management Programs.

3
Being With: Recognizing the Experience of Parents in the Face of Their Child’s Pain p. 43 Rachel B. Levi, PhD Dr. Levi, focuses on the parents and the impact of having a child who is ill and in pain, on their health and well-being. As she states, “…amidst a child’s serious illness a parent’s assumptive world and internal sense of security demand less attention and notice than the myriad of experiences and responsibilities endemic within the experience of parenting .... The ‘common’ nature of pain amongst the children cared for by palliative care providers does not minimize its impact. “ Reciprocal Relationships: Giving and Receiving Care with Children in Spiritual Pain p. 48 L. Dean Allen MDiv, PhD Dr. Allen provides a comprehensive review of spirituality and spirituality in children; reminding us of the impact of Spiritual Pain in children. Children who are dying or have died, their siblings, and children who have lost another family member as well as their caregivers can benefit from “viewing spirituality as having an indispensable communal element,” He ends with this beautiful thought, “…it is helpful to remind myself that (1) children of various ages have spiritual awareness and sensitivity and (2) children can both receive and give care.” Items of Interest p. 52 In each issue of our ChiPPS e-journal, we offer additional items of interest.
-###-
ADDITIONAL NOTES
ChiPPS is a program of the National Hospice and Palliative Care Organization. Learn more at www.nhpco.org/pediatrics.
Please note that the opinions expressed by the contributors to this issue are their own and do not necessarily reflect the views of the editors of this newsletter, ChiPPS and its E-Journal Work Group, or NHPCO. We invite readers with differing points of view to submit comments or suggestions for possible publication in a future issue.
Thank you for taking time to read this issue and for any feedback that you can offer us. Providing pediatric palliative and hospice care to children, adolescents, and their family members has made great strides in recent years, even though it is certainly not always easy and still faces many challenges and obstacles. We wish you all the best in your good work. If you are not on our mailing list and received this newsletter from a friend or some other source, please send an email message to [email protected] requesting to be added to our mailing list. If you are a member of NHPCO, you can go to the Communications Preferences tab in your individual member record online and “opt-in” for communications from ChiPPS. Member Services will be happy to help you adjust your communications preferences; contact them at 800-646-6460. Visit the ChiPPS Web page at www.nhpco.org/pediatrics for previous issues of this E-Journal, additional materials, and other resources of interest.
-###-
4
I OFTEN WONDER
By Scott Newport [email protected]
In my lonely place I share my morning tears With just myself For the children of satin lace Life’s tempest is always on the teeter for them each and every day In the midst of those long hospital stays- At home, my sleepless sheets Give me little peace When I see them again In either life or death I will never forget the floating, soapy bubbles bouncing off the vinyl bed rails or The squeaky smiles peeking past tangled hoses and sagging tubes on those magical days Even though the dusty, disease monster Still clings to cotton corners of every ICU room He never sleeps or even seems to care. Someday though, when grace reaches down for me, I hope to see them When they will guard and guide me to the faraway place “Lord, I wonder if they will ever come home,” I call out. A hope and prayer That will one day take this lonely place Away to another grassy hillside land across the deep, green divide Full of the flowing children of the satin lace Full of the flowing children of the satin lace
Scott Newport with a caboose that he built for a child.
-###-
5
PEDIATRIC PAIN ASSESSMENT
Sheri G. Stewart, MSN, RN-BC, CHPPN Director, Hands of Hope – Greenville, SC
[email protected] Pain The World Health Organization (2012) describes pain as a multidimensional phenomenon with sensory, physiological, cognitive, affective, behavioral, and spiritual components. Perhaps one of the most widely accepted definitions of pain is expressed in the definition that pain is whatever the experiencing person says it is, existing whenever he/she says it does (McCaffery & Pasero, 1999). While self-report of pain is the gold standard, this definition reveals the subjective nature of pain and the myriad of complexities when applying it to children (Manworren & Hynan, 2003). Children receiving hospice or palliative care services are often developmentally or cognitively unable to self-report their pain at some point in their disease trajectory because of their disease process or additional Chronic Complex Conditions (CCC). It is paramount to have the proper tools to ensure pain is adequately assessed in this vulnerable population. Scope of the Problem Each year in the United States, just over 45,000 infants, children, and adolescents die, with another 18,500 deaths among young adults aged 20 to 24 (Institute of Medicine, 2003). In 2001, it was estimated that on any given day 5,000 children with CCC were in the last 6 months of life. Data reveals only 5,000 of the 53,000 children who died that year received hospice services (National Hospice and Palliative Care Organization, 2001; Friebert & Williams, 2014). Evidence demonstrates that the use of developmentally- and cognitively-appropriate pain assessment tools is critical to advance pain assessment (Ramira, Instone, & Clark, 2016). A principal right for children dying is to ameliorate their pain and demands proper assessment (Kriechman, 2016). Adequate pain assessment and management can alleviate the interrelated symptoms of anxiety, distress, and suffering that accompany pain and precipitate the continuation of the vicious pain cycle (Berde, Charles, & Wolfe, 2003). Wolfe, Friebert, and Hilden (2002) revealed that parents perceptions of care for their child at the end of life related to seven symptoms experienced within the last month prior to their child’s death. Pain was the highest rated treated symptom and parents reported that 89% of children experienced “a lot” or a “great deal” of suffering which has been reported in additional studies (Drake, Frost. & Collins, 2003; Kuhlen et al., 2016; Wolfe, Friebert. & Hilden, 2002). Deleterious effects of unmanaged pain in children are well documented and further contribute to suffering for the child and their family (Oddson, Clancy, & McGrath, 2006; Olmstead, Scott, & Austin, 2010; Schechter, Berde, & Yaster, 2003; Simon, 2012; Snaman et al., 2016). Hospice nurses have a pivotal role in the assessment of pain utilizing their knowledge of developmentally-appropriate tools in conjunction with the multidimensional components of pain, which include affective, behavioral, cognitive, sensory, and physiological components, to alleviate pain and suffering (Wrede-Seaman, 2005). Thus knowledge of pediatric pain assessment and measurement tools is paramount to providing optimal care to this vulnerable population. Pediatric Pain Assessment Measurement There are a numerous pain assessment scales that have been developed and proven valid and reliable for the pediatric population. Scales vary on measurement by self-report of pain and observation of pain behaviors, and they address developmental appropriateness as well as cognitive impairments. Behavioral
6
assessment is useful for assessing pain in infants and preverbal children who do not yet possess the ability to communicate that they are in pain, or when mental clouding or confusion are a barrier to a child’s ability to communicate (Hockenberry & Wilson, 2014). It is crucial to discern the different applicable patient populations in order for proper assessment. Painful experiences are dynamic, with huge variation; therefore pain assessment tools must be versatile, repeatable, and accurate to accommodate such variation (Brand & Thorpe, 2016). The scales listed below are samples of the numerous scales available for use in the assessment of pediatric pain. Self-Report Pediatric Pain Tools
Wong-Baker FACES pain scale (Garra et al., 2010) o Intended for children 3 years and older o 53 available translations
Oucher [21, 22, 23] ( Beyer,1999; Beyer & Knott, 1998; Yeh, 2005)
o Intended for children 3 years and older o African American, Caucasian, and Hispanic versions
Numerical Rating Scale (NRS) (Baeyer, 2009)
o Verbal self-report of pain 0-10 for children ages 8 years and older
The Faces Pain Scale-Revised (Hicks et al., 2001) o Intended for children 4-16 years of age
Visual Analog scale (VAS) (von Baeyer, 2006)
o Intended for children 7 years of age and older o The child is asked to point to the area along the line that represents their pain
Pediatric Behavioral Observation Pain Tools
CRIES (C-Crying; R-Requires increased oxygen administration; I-Increased vital signs; E-Expression; S-Sleeplessness) (Breivik et al., 2008)
o Valid and reliable for the neonatal population - 32 weeks to 6 months o 10 point scale
Revised FLACC (Face, Legs, Activity, Cry, Consolability) (Malviya et al., 2006; Merkel, Voepel-
Lewis, & Malviya, 2002; Voepel-Lewis et al., 2002). o The FLACC score has been validated for measuring postoperative pain in children with
mild to severe cognitive impairment. o It has also been validated for the assessment of pain secondary to surgery, trauma,
cancer, or other painful diseases for all pre-verbal children (including infants).
PICIC (Pain Indicator for Communicatively Impaired Children) (Stallard, et al., 2002; Hockenberry & Wilson, 2014).
o Distinguishes between pain and non-pain in children with life-threatening illness who have communication challenges.
o The PICIC has six core pain cues: crying with or without tears; screaming, yelling, groaning, or moaning; screwed up or distressed looking face; body appearing stiff or tense; difficulty in comforting or consoling; and flinching or moving away if touched

7
Pain Assessment Mnemonic
Goals to achieve adequate assessment of pain should be patient- and family-focused. One tool that meets this goal is the QUESTT mnemonic developed for the provider to use with children. It is simple to recall and incorporates many crucial components of pediatric pain assessment (Armstrong-Dailey & Zarbock, 2001). QUESTT stands for:
Question the child
Use pain rating scales
Evaluate behavior and physiological changes
Secure Parents’ Involvement
Take the cause of pain into account
Take action and evaluate results
Questioning the child is essential in the pediatric pain assessment and every effort to involve the patient and family in the pain management plan should be made. Assessment should include location, quality, pattern, intensity, duration, alleviating factors, and aggravating factors. Assess and utilize developmentally-appropriate words that the child uses to describe pain such as “ouch,” “boo-boo,” or “hurt” (Armstrong-Dailey & Zarbock, 2001).
Use self-report or behavioral observation pain rating scales based on the child’s developmental and cognitive abilities. Evaluate behavior and physiological cues as children will often exhibit behavioral changes when experiencing pain. Caregivers can provide invaluable insight regarding past and current changes in behaviors related to pain. Physiologic response to pain can include increased blood pressure, sweating, decreased oxygen saturation rates, and pupillary constriction. It is important to note that absence of physiological symptoms does not represent absence of pain (Armstrong-Dailey & Zarbock, 2001; Berde, Charles, & Wolfe, 2003).
Parents should be included in pain assessment and management (Arora & Baidya, 2013). They can provide integral information on past experiences of pain including what was successful in alleviating pain and their child’s typical response to pain.
There are various types of pain and awareness of the disease process will aid in assessing the type of pain and determining the root of pain while also helping in the provision of appropriate interventions.
The intention of assessment is to treat and provide relief from pain. It is essential to formulate a plan with the multidisciplinary team which includes the patient and caregivers. Pediatric Hospice and Palliative Care is a philosophy and method to provide effective pain and symptom management, in addition to psychosocial care, spiritual care, and decision-making guidance (Friebert & Williams, 2014). The hospice and palliative care nurse must possess knowledge and skills necessary to assess pain and alleviate suffering that is intrinsic to children throughout their disease trajectory.
References
Armstrong-Dailey, A., & Zarbock, S. F. (2001). Hospice care for children. New York: Oxford University Press.
Arora, M. K., & Baidya, D. (2013). WHO guidelines on the pharmacological treatment of persisting pain in children with medical illness. The Indian Journal of Medical Research, 138(4), 570.
Baeyer, C. L. (2009). Numerical rating scale for self‐report of pain intensity in children and adolescents: Recent progress and further questions. European Journal of Pain, 13(10), 1005-1007.
Berde, C., Charles, & Wolfe, J. (2003). Pain, anxiety, distress, and suffering: Interrelated, but not interchangeable. The Journal of Pediatrics, 142(4), 361-363.
Beyer, J. E. (1989). The Oucher: A pain intensity scale for children. In E.M. Tornquist, M. T., Champagne, L. A. Copp, R. A. Wiese, & S. G. Funk (Eds.), Management of pain, fatigue and nausea (pp. 65-71). London: Macmillan Education.
8
Beyer, J. E., & Knott, C. B. (1998). Construct validity estimation for the African-American and Hispanic versions of the Oucher Scale. Journal of Pediatric Nursing, 13(1), 20-31.
Brand, K., & Thorpe, B. (2016). Pain assessment in children. Anaesthesia & Intensive Care Medicine, 17(6), 270-273.
Breivik, H., Borchgrevink, P.C., Allen, S. M., Rosseland, L. A., Romundstad, L., Hals, E. B., & Stubhaug, A. (2008). Assessment of pain. British Journal of Anaesthesia, 101(1), 17-24.
Committee on Approaching Death: Addressing Key End of Life Issues; Institute of Medicine. Dying in America: Improving quality and honoring individual preferences near the end of life. Washington (DC): National Academies Press; 2015 Mar 19. Appendix F, Pediatric End-of-Life and Palliative Care: Epidemiology and Health Service Use. Available from: https://www.ncbi.nlm.nih.gov/books/NBK285690/
Drake, R., Frost, J., & Collins, J. J. (2003). The symptoms of dying children. Journal of Pain and Symptom
Management, 26(1), 594-603. Friebert, S. & Williams, C. (2014). NHPCO Facts and Figures: Pediatric Palliative and Hospice Care in
America. Alexandria, VA: National Hospice and Palliative Care Organization. Garra, G., Singer, A. J., Taira, B. R., Chohan, J., Cardoz, H., Chisena, E., & Thode, H. C. (2010).
Validation of the Wong‐Baker FACES pain rating scale in pediatric emergency department patients. Academic Emergency Medicine, 17(1), 50-54.
Hicks, C. L., von Baeyer, C. L., Spafford, P. A., van Korlaar, I., & Goodenough, B. (2001). The Faces Pain Scale–Revised: Toward a common metric in pediatric pain measurement. Pain, 93(2), 173-183.
Hockenberry, M. J., & Wilson, D. (2014). Wong's nursing care of infants and children (10th ed.). St. Louis: Elsevier Health Sciences.
Kriechman, A. (2016). 8 The dying child. Depression in Children and Adolescents, 4, 97. Kuhlen, M., Hoell, J., Balzer, S., Borkhardt, A., & Janssen, G. (2016). Symptoms and management of
pediatric patients with incurable brain tumors in palliative home care. European Journal of Paediatric Neurology, 20(2), 261-269.
Manworren, R. C., & Hynan, L. S. (2003). Clinical validation of FLACC: Preverbal patient pain scale. Pediatric Nursing, 29(2), 140.
Malviya, S., Voepel-Lewis, T., Burke, C., Merkel, S., & Tait, A. R. (2006). The revised FLACC observational pain tool: Improved reliability and validity for pain assessment in children with cognitive impairment. Pediatric Anesthesia, 16(3), 258-265.
McCaffery, M., & Pasero, C. (1999). Pain. Clinical manual (2nd ed.). St Louis: Mosby. Merkel, S., Voepel-Lewis, T., & Malviya, S. (2002). Pain assessment in infants and young children: The
FLACC Scale: A behavioral tool to measure pain in young children. AJN The American Journal of Nursing, 102(10), 55-58.
National Hospice and Palliative Care Organization. (2001). ChiPPS White Paper: A call for change: recommendations to improve the care of children living with life-threatening conditions. 10US Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau. The National Survey
Oddson, B. E., Clancy, C. A., & McGrath, P. J. (2006). The role of pain in reduced quality of life and depressive symptomology in children with spina bifida. The Clinical Journal of Pain, 22(9), 784-789.
Olmstead, D. L., Scott, S. D., & Austin, W. J. (2010). Unresolved pain in children: A relational ethics perspective. Nursing Ethics, 17(6), 695-704.
Ramira, M.L.M., Instone, S., & Clark, M. J. (2016). Pediatric pain management: An evidence-based approach. Pediatric nursing, 42(1), 39.
Schechter, N. L., Berde, C. B., & Yaster, M. (Eds.). (2003). Pain in infants, children, and adolescents. Philadelphia: Lippincott Williams & Wilkins.
Simon, L. S. (2012). Relieving pain in America: A blueprint for transforming prevention, care, education, and research. Journal of Pain & Palliative Care Pharmacotherapy, 26(2), 197-198.
Snaman, J. M., Baker, J. N., Ehrentraut, J. H., & Anghelescu, D. L. (2016). Pediatric oncology: Managing pain at the end of life. Pediatric Drugs, 1-20.
Stallard, P., Williams, L., Velleman, R., Lenton, S., McGrath, P. J., & Taylor, G. (2002). The development and evaluation of the pain indicator for communicatively impaired children (PICIC). Pain, 98(1), 145-149.

9
Wrede-Seaman, L. (2005). Pediatric pain and symptom management algorithms for palliative care. Wolfe, J., Friebert, S., & Hilden, J. (2002). Caring for children with advanced cancer: Integrating palliative
care. Pediatric Clinics of North America, 49(5), 1043-1062. Voepel-Lewis, T., Merkel, S., Tait, A. R., Trzcinka, A., & Malviya, S. (2002). The reliability and validity of
the Face, Legs, Activity, Cry, Consolability observational tool as a measure of pain in children with cognitive impairment. Anesthesia & Analgesia, 95(5), 1224-1229.
Von Baeyer, C. L. (2006). Children’s self-reports of pain intensity: Scale selection, limitations and interpretation. Pain Research and Management, 11(3), 157-162.
Yeh, C. H. (2005). Development and validation of the Asian version of the Oucher: A pain intensity scale for children. The Journal of Pain, 6(8), 526-534.
-###-
10
PEDIATRIC PAIN MANAGEMENT STRATEGIES
Melissa Hunt, Pharm.D. Pediatric Clinical Pharmacist
Optum Hospice Pharmacy Services Dublin, OH
Pain is one of the most prevalent symptoms in children requiring palliative care. Adequate pain management requires a multidisciplinary approach, including non-pharmacologic interventions. Most children experiencing pain that receive palliative or hospice care require pharmacological management. There are four components often considered when initiating pharmacological pain medications:
1. By the route 2. By the clock 3. By the ladder 4. By the child
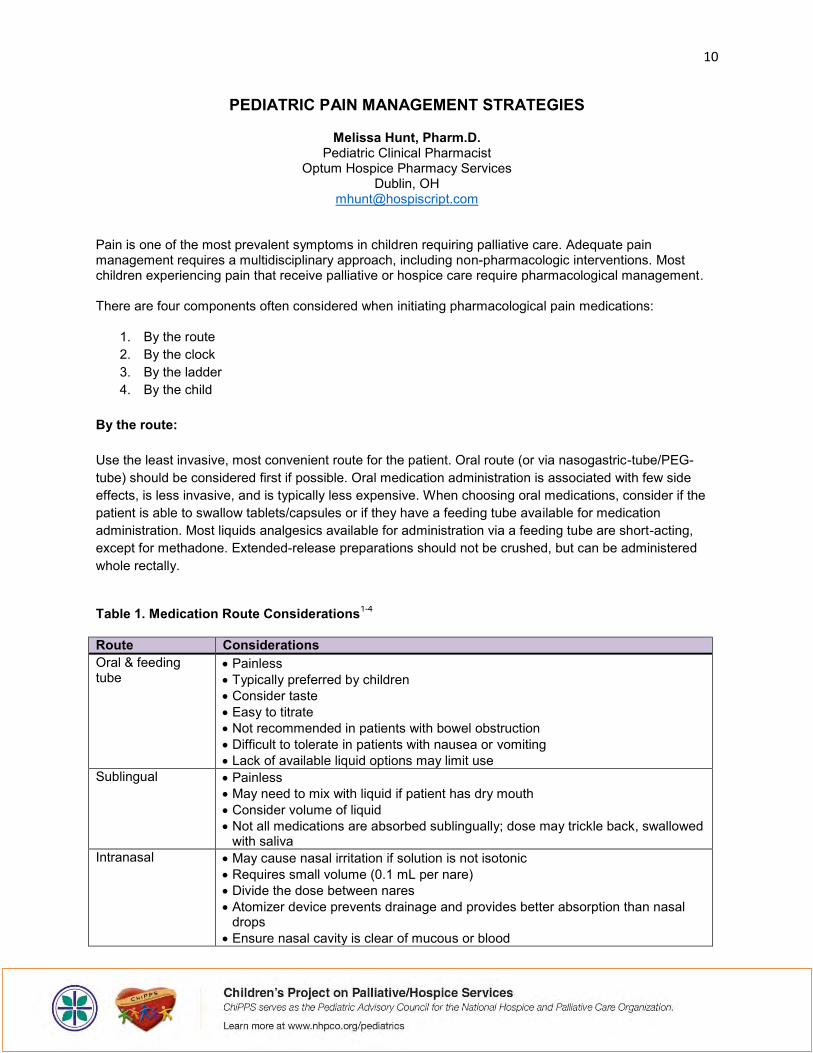
By the route: Use the least invasive, most convenient route for the patient. Oral route (or via nasogastric-tube/PEG-tube) should be considered first if possible. Oral medication administration is associated with few side effects, is less invasive, and is typically less expensive. When choosing oral medications, consider if the patient is able to swallow tablets/capsules or if they have a feeding tube available for medication administration. Most liquids analgesics available for administration via a feeding tube are short-acting, except for methadone. Extended-release preparations should not be crushed, but can be administered whole rectally.
Table 1. Medication Route Considerations1-4
Route Considerations Oral & feeding tube
Painless Typically preferred by children Consider taste Easy to titrate Not recommended in patients with bowel obstruction Difficult to tolerate in patients with nausea or vomiting Lack of available liquid options may limit use
Sublingual Painless May need to mix with liquid if patient has dry mouth Consider volume of liquid Not all medications are absorbed sublingually; dose may trickle back, swallowed
with saliva Intranasal May cause nasal irritation if solution is not isotonic
Requires small volume (0.1 mL per nare) Divide the dose between nares Atomizer device prevents drainage and provides better absorption than nasal
drops Ensure nasal cavity is clear of mucous or blood
11
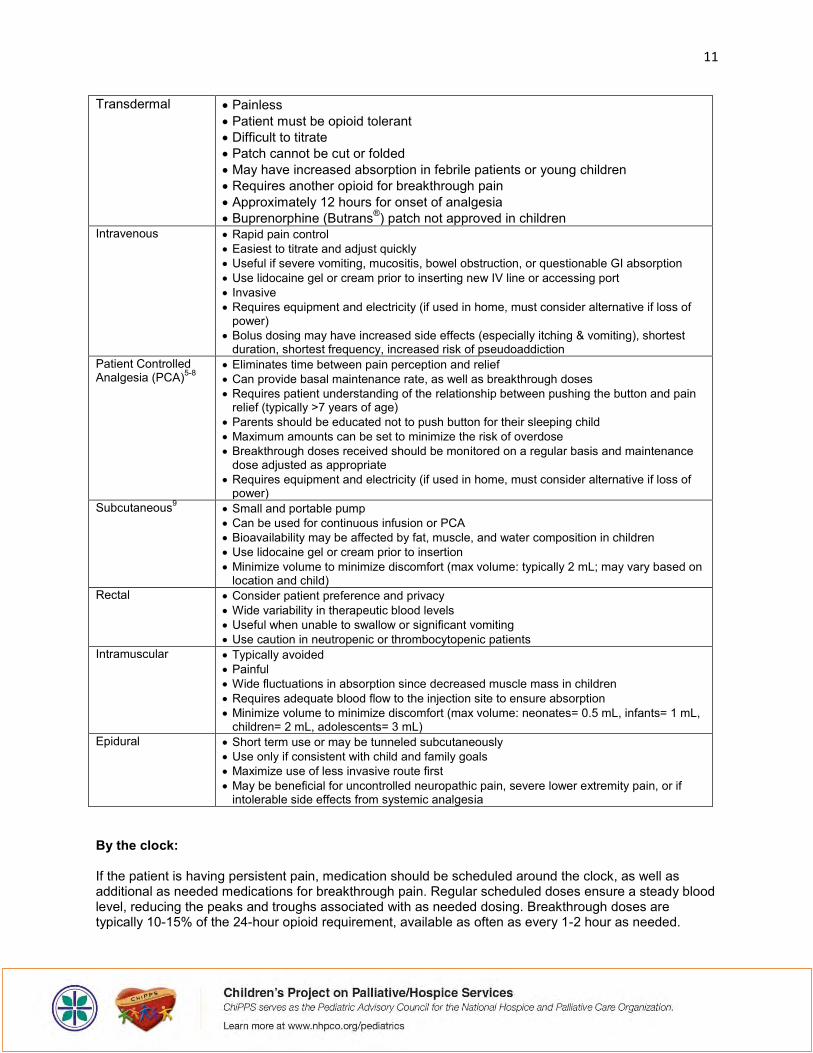
Transdermal Painless Patient must be opioid tolerant Difficult to titrate Patch cannot be cut or folded May have increased absorption in febrile patients or young children Requires another opioid for breakthrough pain Approximately 12 hours for onset of analgesia Buprenorphine (Butrans®) patch not approved in children
Intravenous Rapid pain control Easiest to titrate and adjust quickly Useful if severe vomiting, mucositis, bowel obstruction, or questionable GI absorption Use lidocaine gel or cream prior to inserting new IV line or accessing port Invasive Requires equipment and electricity (if used in home, must consider alternative if loss of
power) Bolus dosing may have increased side effects (especially itching & vomiting), shortest
duration, shortest frequency, increased risk of pseudoaddiction Patient Controlled Analgesia (PCA)5-8
Eliminates time between pain perception and relief Can provide basal maintenance rate, as well as breakthrough doses Requires patient understanding of the relationship between pushing the button and pain
relief (typically >7 years of age) Parents should be educated not to push button for their sleeping child Maximum amounts can be set to minimize the risk of overdose Breakthrough doses received should be monitored on a regular basis and maintenance
dose adjusted as appropriate Requires equipment and electricity (if used in home, must consider alternative if loss of
power) Subcutaneous9
Small and portable pump Can be used for continuous infusion or PCA Bioavailability may be affected by fat, muscle, and water composition in children Use lidocaine gel or cream prior to insertion Minimize volume to minimize discomfort (max volume: typically 2 mL; may vary based on
location and child) Rectal Consider patient preference and privacy
Wide variability in therapeutic blood levels Useful when unable to swallow or significant vomiting Use caution in neutropenic or thrombocytopenic patients
Intramuscular Typically avoided Painful Wide fluctuations in absorption since decreased muscle mass in children Requires adequate blood flow to the injection site to ensure absorption Minimize volume to minimize discomfort (max volume: neonates= 0.5 mL, infants= 1 mL,
children= 2 mL, adolescents= 3 mL) Epidural Short term use or may be tunneled subcutaneously
Use only if consistent with child and family goals Maximize use of less invasive route first May be beneficial for uncontrolled neuropathic pain, severe lower extremity pain, or if
intolerable side effects from systemic analgesia
By the clock: If the patient is having persistent pain, medication should be scheduled around the clock, as well as additional as needed medications for breakthrough pain. Regular scheduled doses ensure a steady blood level, reducing the peaks and troughs associated with as needed dosing. Breakthrough doses are typically 10-15% of the 24-hour opioid requirement, available as often as every 1-2 hour as needed.
12
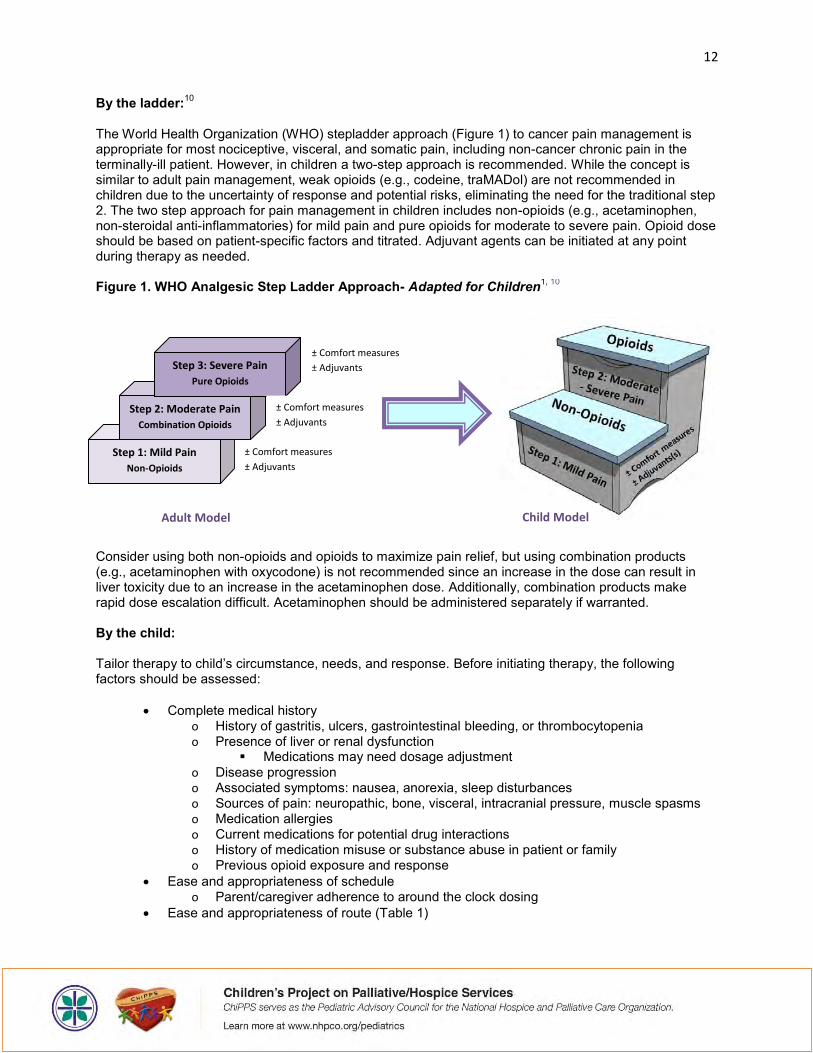
By the ladder:10 The World Health Organization (WHO) stepladder approach (Figure 1) to cancer pain management is appropriate for most nociceptive, visceral, and somatic pain, including non-cancer chronic pain in the terminally-ill patient. However, in children a two-step approach is recommended. While the concept is similar to adult pain management, weak opioids (e.g., codeine, traMADol) are not recommended in children due to the uncertainty of response and potential risks, eliminating the need for the traditional step 2. The two step approach for pain management in children includes non-opioids (e.g., acetaminophen, non-steroidal anti-inflammatories) for mild pain and pure opioids for moderate to severe pain. Opioid dose should be based on patient-specific factors and titrated. Adjuvant agents can be initiated at any point during therapy as needed. Figure 1. WHO Analgesic Step Ladder Approach- Adapted for Children1, 10
Consider using both non-opioids and opioids to maximize pain relief, but using combination products (e.g., acetaminophen with oxycodone) is not recommended since an increase in the dose can result in liver toxicity due to an increase in the acetaminophen dose. Additionally, combination products make rapid dose escalation difficult. Acetaminophen should be administered separately if warranted. By the child: Tailor therapy to child’s circumstance, needs, and response. Before initiating therapy, the following factors should be assessed:
Complete medical history o History of gastritis, ulcers, gastrointestinal bleeding, or thrombocytopenia o Presence of liver or renal dysfunction
Medications may need dosage adjustment o Disease progression o Associated symptoms: nausea, anorexia, sleep disturbances o Sources of pain: neuropathic, bone, visceral, intracranial pressure, muscle spasms o Medication allergies o Current medications for potential drug interactions o History of medication misuse or substance abuse in patient or family o Previous opioid exposure and response
Ease and appropriateness of schedule o Parent/caregiver adherence to around the clock dosing
Ease and appropriateness of route (Table 1)
Step 1: Mild Pain
Non-Opioids
Step 2: Moderate Pain
Combination Opioids
Step 3: Severe Pain
Pure Opioids
± Comfort measures
± Adjuvants
± Comfort measures
± Adjuvants
± Comfort measures
± Adjuvants
Child Model Adult Model
13
Summary: Family involvement in assessment, interventions, evaluation, and treatment plans is essential for success, remembering that care should be centered on the child and family. These four components offer a valuable starting point for initiating medications for pain management. Key References:
Hunt MO, Protus BM, Winters JP, Parker DC. Pediatric Palliative Care Consultant: Guidelines for Effective Management of Symptoms. Dublin, Ohio: HospiScript, a Catamaran Company; c2014.
Wrede-Seaman L. Pediatric Pain and Symptom Management Algorithms for Palliative Care. China: Intellicard, c2005. Pain, p. 86-146
Gregoire MC, Frager G. Ensuring pain relief for children at the end of life. Pain Res Manage 2006;11(3):163-71.
Zernikow B, Michel E, Craig F, et al. Pediatric Palliative Care: Use of opioids for the management of pain. Pediatr Drugs 2009;11(2):129-51.
Mackie AM, Coda BC, Hill HF. Adolescents use patient controlled analgesia effectively for relief from prolonged oropharyngeal mucositis pain. Pain 1991;46:265-269.
Collins JJ, Geake J, Grier HE, et al. Patient-controlled analgesia for mucositis pain in children: a three-period crossover study comparing morphine and hydromorphone. J Pediatr 1996;129(5):722-728.
Dunbar PJ, Buckley P, Gavrin JR, et al. Use of patient-controlled analgesia for pain control for children receiving bone marrow transplants. J Pain Symptom Manage 1995;10:604-611.
Berde CB, Lehn BM, Yee JD, et al. Patient controlled analgesia in children and adolescents: a randomized, prospective comparison with intramuscular morphine for postoperative analgesia. J Pediatr 1991;118:460-466.
Bruera E, Brenneis C, Michaud M, et al. Use of the subcutaneous route for the administration of narcotics in patients with cancer pain. Cancer 1988;62:407-411.
World Health Organization (WHO). Guidelines for analgesic drug therapy. In: Cancer pain relief and palliative care in children. Geneva: WHO/IASP; c1998.
-###-
14
PATIENT-SPECIFIC OPIOID SELECTION CONSIDERATIONS IN CHILDREN
Melissa Hunt, Pharm.D. Pediatric Clinical Pharmacist
Optum Hospice Pharmacy Services Dublin, OH
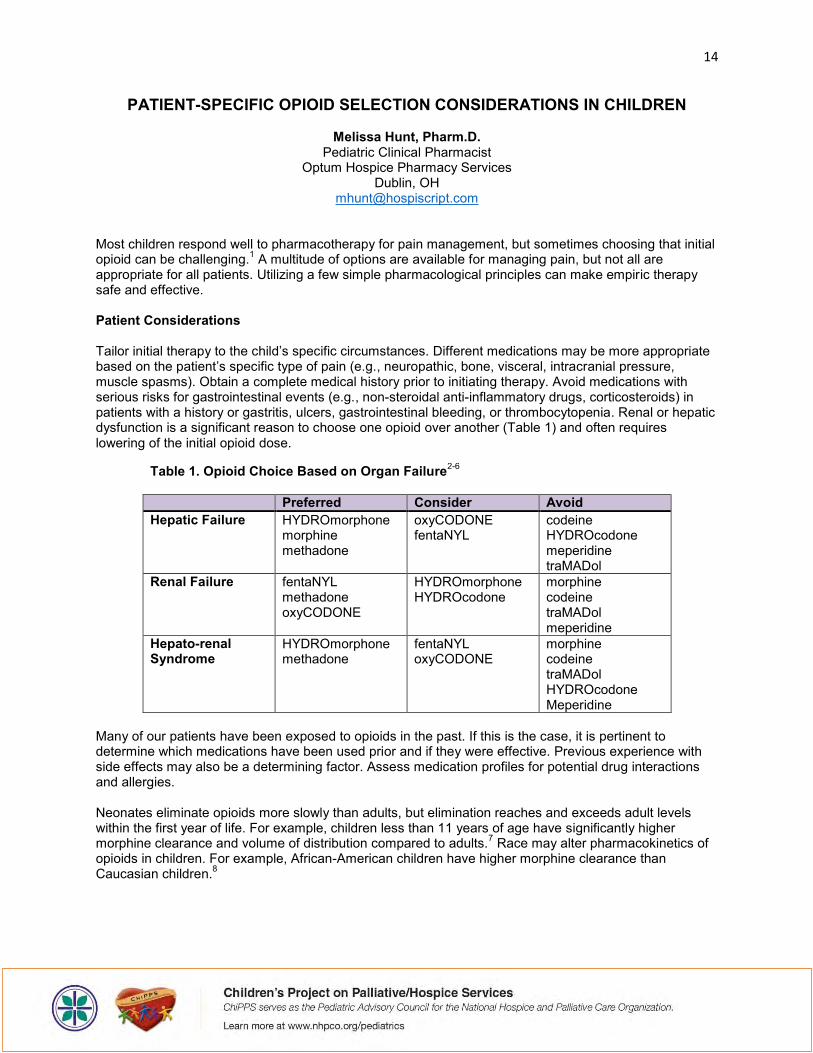
Most children respond well to pharmacotherapy for pain management, but sometimes choosing that initial opioid can be challenging.1 A multitude of options are available for managing pain, but not all are appropriate for all patients. Utilizing a few simple pharmacological principles can make empiric therapy safe and effective. Patient Considerations Tailor initial therapy to the child’s specific circumstances. Different medications may be more appropriate based on the patient’s specific type of pain (e.g., neuropathic, bone, visceral, intracranial pressure, muscle spasms). Obtain a complete medical history prior to initiating therapy. Avoid medications with serious risks for gastrointestinal events (e.g., non-steroidal anti-inflammatory drugs, corticosteroids) in patients with a history or gastritis, ulcers, gastrointestinal bleeding, or thrombocytopenia. Renal or hepatic dysfunction is a significant reason to choose one opioid over another (Table 1) and often requires lowering of the initial opioid dose.
Table 1. Opioid Choice Based on Organ Failure2-6
Preferred Consider Avoid Hepatic Failure HYDROmorphone
morphine methadone
oxyCODONE fentaNYL
codeine HYDROcodone meperidine traMADol
Renal Failure fentaNYL methadone oxyCODONE
HYDROmorphone HYDROcodone
morphine codeine traMADol meperidine
Hepato-renal Syndrome
HYDROmorphone methadone
fentaNYL oxyCODONE
morphine codeine traMADol HYDROcodone Meperidine
Many of our patients have been exposed to opioids in the past. If this is the case, it is pertinent to determine which medications have been used prior and if they were effective. Previous experience with side effects may also be a determining factor. Assess medication profiles for potential drug interactions and allergies. Neonates eliminate opioids more slowly than adults, but elimination reaches and exceeds adult levels within the first year of life. For example, children less than 11 years of age have significantly higher morphine clearance and volume of distribution compared to adults.7 Race may alter pharmacokinetics of opioids in children. For example, African-American children have higher morphine clearance than Caucasian children.8
15
Non-Opioid Considerations While acetaminophen (Tylenol®) is considered one of the best tolerated analgesics and is available over the counter (OTC), it has risk of hepatotoxicity, especially at higher doses (>75 mg/kg/day or >4,000 mg/day). Aspirin is typically avoided for pain management in children (<12 years of age) due to the risk of Reye’s syndrome (acute encephalopathy with liver damage). Ibuprofen (Motrin®) is another OTC analgesic that provides anti-inflammatory effects. However, infants less than six months of age are unable to adequately metabolize ibuprofen (hydroxylation via CYP2C9 and CYP2C8 enzymes in the liver). Avoid ibuprofen in infants less than six months of age. Ibuprofen has the least gastrointestinal side effects among the non-steroidal anti-inflammatory drugs (NSAIDs). Use NSAIDs with caution in patients with hepatic or renal impairment or history of gastrointestinal bleeding or ulcers. Opioid Considerations All opioids have black box warnings:6
Do not crush or chew extended or sustained release dosage forms. Long-acting opioids are indicated for the management of moderate to severe pain when
around the clock pain control is needed. Do not administer opioids with alcohol. Remain vigilant to signs of potential abuse, misuse, or diversion of opioids. Combined use of opioids with benzodiazepines or other drugs that depress the CNS may
result in serious adverse reactions, including slowed or difficult breathing.
Many pain medications have age restrictions associated with their use (Table 2). Avoid codeine and codeine-containing products in pediatric patients due to the highly variable pharmacokinetics and side effects, as well as lack of evidence and safety.9-11 Codeine is routinely converted to morphine by the CYP2D6 enzyme in the liver. People can have varying degrees of CYP2D6 activity. Poor metabolizers are deficient in CYP2D6 and have inadequate therapeutic response from codeine. On the other hand, people with higher than normal CYP2D6 activity, considered ultra-rapid metabolizers, may have supratherapeutic response and increased risk of adverse reactions.12 The FDA does not recommend the use of codeine in children, specifically following tonsillectomy and/or adenoidectomy, due to reports of respiratory depression and death.13 Similarly, hydrocodone must be metabolized by CYP2D6 to hydromorphone in order to provide most of its analgesic effect. Hydrocodone is also metabolized via CYP3A4 and other non-CYP pathways as well. Hydrocodone-containing products are not recommended in children <2 years of age and there is very limited dosing information in this population. Tablets and capsules are only approved for use in adults. Additionally, immediate-release hydrocodone is only available in combination with acetaminophen which may make rapid titration difficult and adds the hepatotoxicity risk. Extended-release hydrocodone products are not approved for use in children. Numerous sentinel events have occurred from high doses of hydromorphone being used in opioid-naïve patients. The IV formulation is available in multiple concentrations which may contribute to medication errors as well. Oral formulations of hydromorphone are only 1/5 as effective as IV formulations. Hydromorphone is metabolized via glucuronidation. Accumulation of the hydromorphone-3-glucuronide metabolite can contribute to neurotoxicity. Hydromorphine is not recommended in infants less than 6 months of age. Fentanyl is often considered in patients that are non-compliant with frequent medication administration or need a longer-acting agent. It is also a good choice for opioid rotation in situations of neurotoxicity or
16
dose-limiting side effects since it is structurally different. Fentanyl is not recommended in children less than two years of age, but the IV formulation is often used off-label in this population. Tolerance does develop quickly using the IV formulation. Avoid the transdermal patch in young children and opioid-naïve patients. The smallest dosage form available is 12.5 mcg/hr. At a minimum, the patient would have to be receiving 25 mg/day of oral morphine equivalents to consider transitioning to fentanyl transdermal patch. Transdermal fentanyl typically isn’t started in patients receiving less than 60 mg/day oral morphine equivalents. Infants generally have increased absorption of medication topically since their skin is thin and not a very effective barrier. Infants may also have decreased fat disposition making it difficult for a depo layer to form. Fentanyl is extremely lipid soluble and therefore penetrates the CNS quickly. The transmucosal fentanyl products are not recommended in children less than 18 years of age, this includes the buccal film, buccal tablet, and oral lozenge, which would all be choking hazards for a young child. Chest wall rigidity is a possible side effect of fentanyl. Methadone is commonly used in the hospice population due to its unique mechanism of action (mu receptor agonist, NMDA-receptor antagonist, and serotonin re-uptake inhibitor) making it beneficial for patients with neuropathic pain. Methadone is structurally different from other opioids and has a lower incidence of side effects, such as constipation; therefore, it is often chosen when patients have neurotoxicity from other agents. Methadone lacks active metabolites and is considered safe for use in renal failure and stable liver disease. Methadone has an extremely long half-life (longer than its duration of action), which may lead to accumulation and makes quick titration difficult, but also allows for less frequent dosing than other opioids. Methadone is available in numerous dosage forms that all maintain a long duration of action even when crushed. There are numerous conversion methods used when converting from other opioids to methadone; however there isn’t a standard conversion from methadone back to other opioids. With all of these complex features, methadone should be prescribed by practitioners with specific training or experience. Morphine is considered the gold standard for pain management and is typically first line in most patients. Although it does not have age restrictions associated with it, infants less than six months of age require much lower doses (0.08 mg/kg/dose) due to their decreased ability to metabolize morphine and decreased clearance. Infants are at increased risk of toxicity, such as respiratory depression, but morphine can be completely safe in this population as long as it is dosed appropriately. Morphine is metabolized by the liver and excreted by the kidneys; therefore morphine may not be the most appropriate agent in a patient with renal disease. Oxycodone is also metabolized by CYP2D6 and CYP3A4. Oxycodone has a slightly longer half-life than morphine, allowing for less frequent dosing. Oxycodone is often used in patients with renal dysfunction. Dosing information is not available for oxycodone in infants <6 months of age. Immediate release products are approved for use in adults; while extended release products are approved for use in children >11 years. Although tramadol is metabolized via CYP2D6 to the more potent O-desmethyltramadol, tramadol itself is a weak mu-receptor agonist with additional effect inhibiting norepinephrine/serotonin reuptake. Tramadol is not approved for use in children though and dosing is not available for children less than four years of age.14 One recent case report described a five-year-old girl who experienced respiratory depression after receiving a single dose of tramadol following a tonsillectomy/adenoidectomy.15 Tramadol is a weak opioid and would fall on step 2 of the World Health Organization (WHO) analgesic ladder that is not recommended in children. Avoid tramadol in patients with a history of seizures since it can decrease the seizure threshold.16-17
17
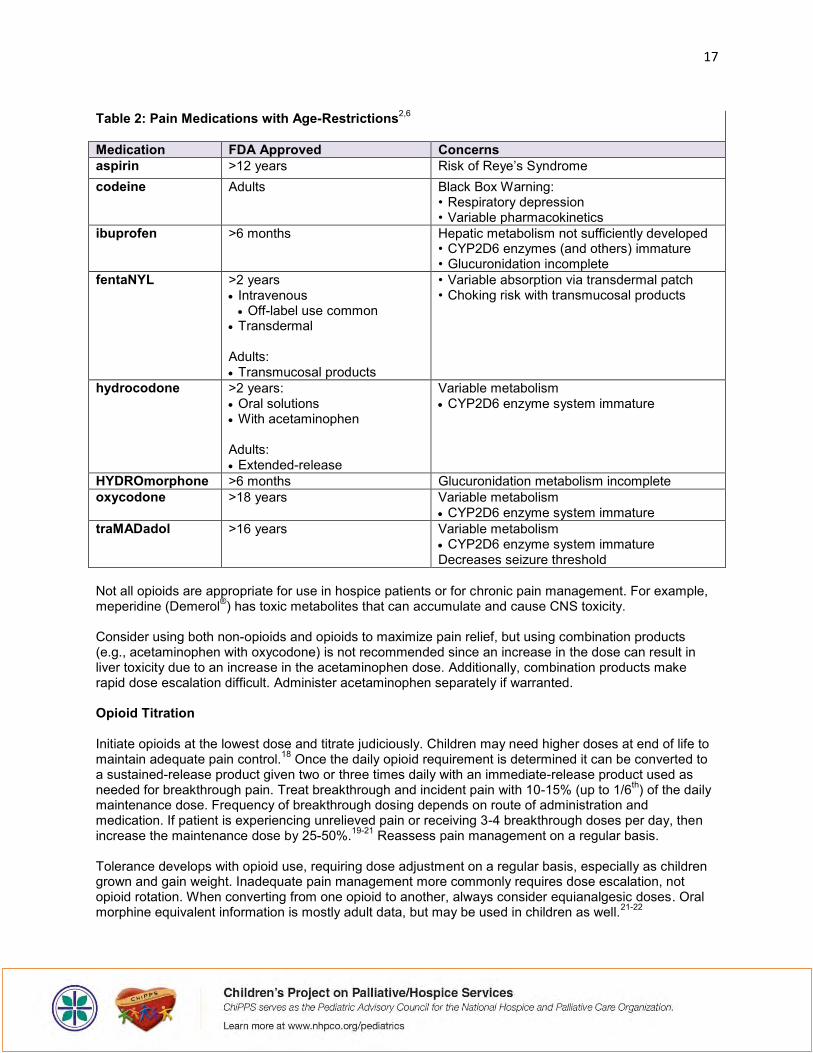
Table 2: Pain Medications with Age-Restrictions2,6
Medication FDA Approved Concerns aspirin >12 years Risk of Reye’s Syndrome codeine Adults Black Box Warning:
• Respiratory depression • Variable pharmacokinetics
ibuprofen >6 months Hepatic metabolism not sufficiently developed • CYP2D6 enzymes (and others) immature • Glucuronidation incomplete
fentaNYL >2 years Intravenous Off-label use common
Transdermal Adults: Transmucosal products
• Variable absorption via transdermal patch • Choking risk with transmucosal products
hydrocodone >2 years: Oral solutions With acetaminophen Adults: Extended-release
Variable metabolism CYP2D6 enzyme system immature
HYDROmorphone >6 months Glucuronidation metabolism incomplete oxycodone >18 years Variable metabolism
CYP2D6 enzyme system immature traMADadol >16 years Variable metabolism
CYP2D6 enzyme system immature Decreases seizure threshold
Not all opioids are appropriate for use in hospice patients or for chronic pain management. For example, meperidine (Demerol®) has toxic metabolites that can accumulate and cause CNS toxicity. Consider using both non-opioids and opioids to maximize pain relief, but using combination products (e.g., acetaminophen with oxycodone) is not recommended since an increase in the dose can result in liver toxicity due to an increase in the acetaminophen dose. Additionally, combination products make rapid dose escalation difficult. Administer acetaminophen separately if warranted. Opioid Titration Initiate opioids at the lowest dose and titrate judiciously. Children may need higher doses at end of life to maintain adequate pain control.18 Once the daily opioid requirement is determined it can be converted to a sustained-release product given two or three times daily with an immediate-release product used as needed for breakthrough pain. Treat breakthrough and incident pain with 10-15% (up to 1/6th) of the daily maintenance dose. Frequency of breakthrough dosing depends on route of administration and medication. If patient is experiencing unrelieved pain or receiving 3-4 breakthrough doses per day, then increase the maintenance dose by 25-50%.19-21 Reassess pain management on a regular basis. Tolerance develops with opioid use, requiring dose adjustment on a regular basis, especially as children grown and gain weight. Inadequate pain management more commonly requires dose escalation, not opioid rotation. When converting from one opioid to another, always consider equianalgesic doses. Oral morphine equivalent information is mostly adult data, but may be used in children as well.21-22

18
Potential Adverse Reactions In general, children are not more sensitive to the effects of opioids compared to adults. Infants less than 6 months of age are at increased risk of respiratory depression since they are unable to adequately metabolize and eliminate opioids therefore requiring lower initial doses (25-50% of typical pediatric opioid dosing). Monitor for potential side effects and initiate methods of prevention if possible. Common side effects of opioids include constipation, nausea and vomiting, itching, transient sedation, dry mouth, and sweats. Tolerance does not develop to the constipating effects of opioids. Initiate preventative bowel regimen when scheduled opioids are begun. Less common side effects include hallucinations, dysphoria, myoclonus, respiratory depression, and urinary retention.23-24 Counsel parents regarding potential side effects and the possibility of increased sleep initially once pain is controlled. Opioid-induced neurotoxicity is a possible side effect dependent on both the dose and duration of therapy. Neurotoxicity is possible with all opioids, but is seen most commonly with morphine or HYDROmorphone due to the accumulation of the morphine-3 glucuronide and HYDROmorphone-3 glucuronide metabolites. In cases of neurotoxicity, increasing the dose typically exacerbates the excitatory behaviors. After tapering the offending opioid, symptoms usually resolve over hours to days as the offending metabolite clears.19-20, 23 Treatment of neurotoxicity includes tapering the dose, rotating to a structurally different opioid, hydrating the patient if appropriate, and treating specific symptoms, such as delirium or myoclonus. Respiratory depression, although uncommon with proper dosing, may occur if a patient is opioid-naïve, in combination with other respiratory depressant drugs, or when overdose occurs. In the case of significant respiratory depression, naloxone (Narcan®) may be administered. Adjuvant Analgesics Add adjuvant agents at any point during therapy to treat concurrent symptoms that may exacerbate pain. Adjuvants can provide independent analgesic activity for specific types of pain. For example, anti-depressants (e.g., amitriptyline) and anticonvulsants (e.g., gabapentin) are often effective for neuropathic pain. Corticosteroids (e.g., dexamethasone) may provide benefit for patients with cerebral edema, bowel wall edema, hepatic distention, or significant inflammation. Anticholinergic agents (e.g., hyoscyamine) effectively treat colic, but can contribute to constipation. Palliative radiation is highly effective for treating pain due to localized bone lesions and may reduce the need for analgesics after a few days. Bisphosphonates are often considered for the treatment of bone pain, but are not FDA approved in children or recommended by the WHO. Response from bisphosphonates may not be seen for up to 12 weeks and they often lose their effectiveness over time. Conclusion Family involvement in assessment, interventions, evaluation, and treatment plans is essential for success. Encourage parents to ask question regarding medication use, pain control, fears, and concerns. Assess patient and family understanding of pain interventions and educate regarding pain management myths, especially regarding opioids. When pharmacologic interventions are warranted, consider patient-specific factors to ensure appropriate and safe opioid selection. Individualize analgesics according to the child’s pain and response to treatment, frequently reassessing and modifying as necessary. Key References:
1. Widdas D, McNamara K, Edwards F. A Core Care Pathway for Children with Life-limiting and Life-threatening Conditions, 3rd Ed [Internet]. Bristol: Together for Short Lives; February 2013 [cited 2016 September 1]. Available from: www.togetherforshortlives.org.uk.
2. Hunt MO, Protus BM, Winters JP, Parker DC. Pediatric Palliative Care Consultant: Guidelines for Effective Management of Symptoms. Dublin, Ohio: HospiScript, a Catamaran Company; c2014.
3. Delco F, Tchambaz L, Schlienger R, et al. Dose adjustment in patients with liver disease. Drug Safety 2005, 28(6):529-45.
19
4. Tegeder I, Lotsch J, Geisslinger G. Pharmacokinetics of opioids in liver disease. Clin Pharmacokinet 1999; 37(1):17-40.
5. Murtagh FEM, Chai MO, Edmonds PM, et al. The use of opioid analgesia in end stage renal disease patients managed without dialysis: recommendations for practice. Journal of Pain and Palliative Care Pharmacotherapy 2007;21(2):5-16.
6. Lexi-Comp Online, Pediatric & Neonatal Lexi-Drugs Online, Hudson, Ohio: Lexi-Comp, Inc; September 1, 2016.
7. Hunt AM, Joel S, Dick G, et al. Population pharmacokinetics of oral morphine and its glucuronides in children receiving morphine as immediate-release liquid or sustained-release tablets. J Pediar 1999;135(1):47-55.
8. Sadhasivam S, Krekels EH, Chidambaran V, et al. Morphine clearance in children: does race or genetics matter? J Opioid Manage 2012;8(4):217-26.
9. Magnani B, Evans R. Codeine intoxication in the neonate. Pediatrics 1999; 104: e75. 10. Voronov P, Przybylo HJ, Jaganathan N. Case report. Apnea in a child after oral codeine: a genetic variant –
an ultra-rapid metabolizer. Pediatr Anesth 2007; 17: 684–687. 11. Tobias JD, Green TP, Cote CJ, Section on Anesthesiology and Pain Medicine, Committee on Drugs.
Codeine: Time to Say “No”. Pediatrics 2016;138(4):e20162396. 12. Williams D, Patel A, Howard RF. Pharmacogenetics of codeine metabolism in an urban population of children
and its implication for analgesic reliability. Br J Anaesth 2002;89:839-845. 13. Food and Drug Administration (FDA). FDA Drug Safety Communication: Safety review update of codeine use
in children; new Boxed Warning and Contraindication on use after tonsillectomy and/or adenoidectomy. February 20, 2013. [Internet] http://www.fda.gov/Drugs/DrugSafety/ucm339112.htm. Accessed September 1, 2016.
14. Schnabel A, Reichl SU, Meyer-FrieBem C, et al. Tramadol for postoperative pain treatment in children. Cochrane Database Syst Rev 2015;(3):CD009574.
15. Orliaguet G, Hamza J, Couloigner V, et al. A case of respiratory depression in a child with ultrarapid CYP2D6 metabolism after tramadol. Pediatrics 2015;135(3):e753-5.
16. Bamigbade TA, Langford RM. The clinical use of tramadol hydrochloride. Pain Rev 1998;5: 155-82 17. Rose JB, Finkel JC, Arquedas-Mohs A, et al. Oral tramadol for the treatment of pain of 7-30 days' duration in
children. Anesth Analg 2003;96: 78-81. 18. Gregoire MC, Frager G. Ensuring pain relief for children at the end of life. Pain Res Manage 2006;11(3):163-
71. 19. Zernikow B, Michel E, Craig F, et al. Pediatric Palliative Care: Use of opioids for the management of pain.
Pediatr Drugs 2009;11(2):129-51. 20. Zernikow B, Smale H, Michel E, et al. Paediatric cancer pain management using the WHO analgesic ladder-
results of a prospective analysis from 2265 treatment days during the quality improvement study. European Journal of Pain 2006;10:587-95.
21. World Health Organization (WHO). Guidelines for analgesic drug therapy. In: Cancer pain relief and palliative care in children. Geneva: WHO/IASP; c1998. p.24-8.
22. Hain RDW, Miser A, Devins M, et al. Strong opioids in pediatric palliative medicine. Pediatr Drugs 2005;7(1):1-9.
23. Friedrichsdorf SJ, Kang TI. The management of pain in children with life-limiting illness. Pediatr Clin N Am 2007;54:645-72.
24. Berde CB, Nurko S. Opioid side effects: mechanism-based therapy. N Engl J Med 2008;358(22):2332-2343.
-###-

20
VIRTUAL REALITY AS A COMPLEMENTARY THERAPY TO EASE PAIN AND ANXIETY IN CHILDREN
Simon Robertson, Founder & CEO, kindVR1
Anurag K. Agrawal, MD, Associate Hematologist/Oncologist2 Marsha Treadwell, PhD, Clinical Scientist2
Carolyn Hoppe, MD, Associate Hematologist/Oncologist2 Anne Marsh, MD, Associate Hematologist/Oncologist2
1. kindVR 2. UCSF Benioff Children’s Hospital Oakland, CA
Children with chronic illness and terminal diagnoses are often living a reality far from one they or their families envisioned. The experiences that might characterize an idyllic childhood—from preschools, playgrounds, and play dates, to soccer fields, piano concerts, and college visits—are interrupted by debilitating symptoms, painful and anxiety-provoking procedures, medication side-effects, multiple visits to the medical establishment, and significant time in the hospital. Medical interventions alone are often insufficient to manage pediatric chronic pain as well as procedural pain and anxiety. To date, medical practice will often add medications which may increase side effects without positively impacting the underlying symptoms. Frequent pain and anxiety in the young child will often then lead to chronic pain syndromes later in life. The New York Times recently highlighted the benefit of non-opioid strategies for adult patients in a regional emergency department in New Jersey as well as the need to have a more integrated approach to managing chronic pediatric pain. [1,2]
Complementary therapies and cognitive behavioral interventions are potentially important ways to improve pain, anxiety, and quality of life in pediatric patients with chronic illness. Child life specialists and cognitive-behavioral interventions such as distraction are especially valuable in preparing the child and allowing for effective coping and adjustment. [3-5] A systematic review of children and adolescents undergoing needle-related procedures reported potential benefit for distraction, hypnosis, and combined cognitive behavioral interventions. [6] Additional reviews of hypnosis, distraction, imagery, music therapy, as well as relaxation and biofeedback techniques have shown benefit for procedural pain and distress in pediatric cancer patients. [7-11] Additionally, time in nature has been shown to be an important methodology to relieve stress and improve resilience. [12,13] Complementary therapies come with little risk and may provide pain relief and improvement in quality of life; therefore, resources for exploration of such modalities should be routinely provided to pediatric patients and their families.
Imagine being able to transport a child from a world with pain and anxiety into one where they can swim in the ocean with marine wildlife, fly in outer space, or walk and play in a park, all without leaving the comfort of their hospital bed? Virtual reality (VR) can do just that. VR is an immersive and interactive form of escapism. Using computer-generated technology, viewable through a light-weight, head-mounted display, VR transports users into an environment that allows them to escape their current surroundings. It engages multiple senses including sight, touch, and hearing. Some VR environments go so far as to integrate the sensory input of smell. While the entertainment and gaming industries are currently the largest market for VR applications, some developers are designing and exploring ways that VR can be used within the healthcare sector. A small body of literature exists on the use of VR for various pediatric health-related applications, including the use of VR to successfully distract children undergoing burn wound care, intravenous catheter placements, dental procedures, and for needle-related procedures in children with cancer. [14-18]
21
At UCSF Benioff Children’s Hospital Oakland, we are systematically exploring how VR can improve upon the many stressors experienced during hospitalization for our pediatric patients. Together with Simon Robertson, Founder and CEO of kindVR, a team of physicians and nurses from our Pediatric Hematology/Oncology department are studying ways to apply VR to achieve a common goal: minimize pain and suffering and thus improve quality of life.
Our first pilot study is exploring the use of VR as a complementary therapy to alter the perception of pain in hospitalized children with sickle cell disease (SCD). SCD is an inherited blood disorder with a wide-range of clinical manifestations, the most common of which are acute bouts of intense pain known as vaso-occlusive pain episodes (VOE). The pain of VOE is often intense enough to require hospitalization and intravenous opioid medications to attempt adequate analgesia. Opioid medications, while quite effective in reducing pain, have undesirable side effects such as pruritus, constipation, nausea and sedation that may create secondary problems necessitating additional medications to counteract these effects. Additionally, opioid therapy is often not effective when used alone for patients with chronic pain and underlying changes in neurosensory pathways which create problems such as hyperalgesia and allodynia. As a pilot, we enrolled 30 subjects with SCD ages 8 years and older and tested: 1) the usability and acceptability of VR technology for patients with SCD hospitalized with VOE pain; and 2) whether a VR immersive experience is effective in reducing pain scores. Subjects participated in a 15-minute VR experience using kindVR Aqua software. Participants completed the Adolescent Pediatric Pain Tool (APPT), a validated, multidimensional pain assessment tool that assesses pain location, intensity, and quality, pre- and post-VR experience. Patients completed two additional questionnaires including an assessment of possible adverse effects (simulator sickness) and how they perceived the VR experience. Our preliminary results show that the VR was positively received by all participants and led to a significant reduction in pain scores.
VR has multiple additional applications in the inpatient and outpatient setting which we are currently exploring including: 1) utilization of VR to decrease pain and anxiety associated with accessing an indwelling central venous catheter (i.e., a mediport) in children with cancer; 2) simulating the MRI suite prior to MRI imaging to assist with stress and anxiety related to this procedure; and 3) utilization of biofeedback and VR nature to improve the quality of life experience for patients with chronic pain as well as long-term hospitalized pediatric oncology patients. VR technology in the health care sector is a relatively novel complementary therapy with a potential for wide-ranging applicability that we are excited to explore further and are confident will have significant benefit for our patients.

22
References:
Hoffman J (2016, June 10) An E.R. Kicks the Habit of Opioids for Pain. The New York Times. Retrieved from http://www.nytimes.com/2016/06/14/health/pain-treatment-er-alternative-opioids.html
Peachman RR (2016, June 27) Why Aren’t We Managing Children’s Pain? The New York Times. Retrieved from http://well.blogs.nytimes.com/2016/06/27/when-its-not-just-a-boo-boo-the-push-to-treat-childrens-pain/?_r=
Hockenberry MJ, McCarthy K, Taylor O et al (2011) Managing painful procedures in children with cancer. J Pediatr Hematol Oncol 33:119-127
Hedén L, von Essen L, Ljungman G (2009) Randomized interventions for needle procedures in children with cancer. Eur J Cancer 18:358-363
Sadeghi T, Mohammadi N, Shamshiri M et al (2013) Effect of distraction on children’s pain during intravenous catheter insertion. J Spec Pediatr Nurs 18:109-114
Uman LS, Chambers CT, McGrath PJ, et al (2006) Psychological interventions for needle-related procedural pain and distreses in children and adolescents. Cochrane Syst Rev 4:CD005179
Landier W, Tse AM (2010) Use of complementary and alternative medical interventions for the management of procedure-related pain, anxiety, and distress in pediatric oncology: an integrative review. J Pediatr Nurs 25:566-579
Wild MR, Espie CA (2004) The efficacy of hypnosis in the reduction of procedural pain and distress in pediatric oncology: a systematic review. J Dev Behav Pediatr 25:207-213
Richardson J, Smith JE, McCall G et al (2006) Hypnosis for procedure-related pain and distress in pediatric cancer patients: a systematic review of effectiveness and methodology related to hypnosis interventions. J Pain Symptom Manage 31:70-84
Nguyen TN, Nilsson S, Hellström AL et al (2010) Music therapy to reduce pain and anxiety in children with cancer undergoing lumbar puncture: a randomized clinical trial. J Pediatr Oncol Nurs 27:146-155
Shockey DP, Menzies V, Glick DF et al (2013) Preprocedural distress in children with cancer: an intervention using biofeedback and relaxation. J Pediatr Oncol Nurs 30:129-138
Williams F (2015, December 8) This Is Your Brain on Nature. National Geograhic. Retrieved from http://ngm.nationalgeographic.com/2016/01/call-to-wild-text
Razani N, Meade K, Schudel C et al (2015) Healing through nature: a park-based health intervention for young people in Oakland, California. Children, Youth and Environments 25:147-159
Jeffs D, Dorman D, Brown S et al (2014) Effect of virtual reality on adolescent pain during burn wound care. J Burn Care Res 35:395-408
Schmitt YS, Hoffman HG, Blough DK et al (2011) A randomized, controlled trial of immersive virtual reality analgesia, during physical therapy for pediatric burns. Burns 37:61-68
Gold JI, Kim SH, Kant AJ et al (2006) Effectiveness of virtual reality for pediatric pain distraction during i.v. placement. Cyberpsychol Behav 9:207-212
Asl Aminabadi N, Erfanparast L, Sohrabi A et al (2012) The impact of virtual reality distraction on pain and anxiety during dental treatment in 4-6 year-old children: a randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospects 6:117-124
Nilsson S, Finnström B, Kokinsky E et al (2009) The use of Virtual Reality for needle-related procedural pain and distress in children and adolescents in a paediatric oncology unit. Eur J Oncol Nurs 13:102-109
-###-

23
A ROLE FOR PALLIATIVE CARE IN THE PAIN OF CHILDHOOD SICKLE CELL DISEASE
Toluwalase (Lase) A. Ajayi, MD
Rady Children’s Hospital, Department of Pediatrics San Diego, CA
Kyle P. Edmonds, MD Howell Palliative Care Service, Department of Medicine
UC San Diego Health Sciences San Diego CA
Introduction Sickle cell disease (SCD), a blood disease caused by a single nucleotide substitution, is the most common serious genetic disease in childhood. It affects nearly 1 in 2500 births and 100,000 individuals in the United States with 300,000 new cases globally each year (1). The characteristic feature of this disease is the vaso-occlusive painful crisis where pain results from sickled red blood cells disrupting blood flow in capillaries and other small blood vessels. As a result, 100,000 US children are at risk for acute pain every day. Although the ramifications of living with SCD go well beyond their painful episodes, this article will focus on the impact of pain on the developing child with SCD and how palliative care across all settings needs to be recognized as a viable resource for these children in management of their pain. Scope of Impact Children and adolescents with SCD perceive that the defining consequence of vaso-occulsive events are pain crises and the effect those crises have on their quality of life (2). Too many studies to cite have identified poor pain management in those with SCD. This is particularly devastating in the pediatric population, as we know that pain crises are the leading cause of hospitalization in children with SCD (3). Though the average length of stay for the child admitted for an SCD pain crisis is 4-5 days, these painful episodes generally last greater than 7 days (4) and early discharges lead to an increased risk for hospital readmission (5,6). One study in particular showed that approximately two-thirds of school-aged, hospitalized children have irregular school attendance and one-fourth of hospitalized patients had left school all together (7). This isolation from peer groups and social interactions leads to impaired psychosocial functioning, altered intra- and interpersonal relationships further reducing an already diminished quality of life (8). As these children grow to be adolescents, and their sense of isolation increases, they can present with anxiety, anger, depression, and feelings of disfranchisement (9). If not recognized and addressed, these emotions follow them into adulthood and become worse with age. We are then presented with the stereotyped person with SCD who has limited productivity in the adult workforce, a mistrust of the medical system and low expectations from his or her community. Medical providers are sensitized to people with SCD and expect this stereotype of a patient. A combination of endemic racial bias in the healthcare system, medical provider distrust of people with SCD, and general discomfort with opioid prescribing results in perceived discriminatory treatment during acute painful crises on the part the patient (10-13). These troublesome interactions with providers can reinforce mistrust of the medical system for those with SCD and a self-fulfilling prophesy can ensue. In fact, people with SCD report more communication deficits and worse quality of care in the US medical system than African Americans without SCD, who already report greater problems with medical discrimination than white patients (14).

24
It is not only children with SCD who endure these challenges as their family members also take this journey with them. Previous studies have demonstrated more stress, increased caregiving burden, and increased need for social support for caregivers of children with chronic illness (15-17). Further, the consequences of frequent hospitalizations is not limited to the child alone as caring for a child with SCD who has frequent and unpredictable pain crises results in missed work and increased financial stress on the part of the caregiver. Therefore, comprehensive care for these patients necessitates a multidimensional approach with a patient-centered and family-oriented focus. Palliative Care Involvement Chronic pain in the pediatric population outside of SCD requires an inclusive approach with a focus on medical and physiologic aspects and on the child’s physical functioning and emotional impairment (18). Intensive interdisciplinary pain treatment including at least three different coordinated disciplines is an emerging and rapidly accepted treatment of choice for these children with an end goal of improving function and reengagement in age-specific activities (19,20). When you add the complexities involved in living with a life-long disease such as SCD, it makes sense to incorporate a team that is knowledgeable about chronic illness and has expertise in pain control, as well as having staff available who are sensitive to the special needs of children with chronic illness. In this way, specialist palliative care teams can bring their unique expertise not only in symptom management and psychosocial-spiritual assessment, but also in team member self-awareness and monitoring for implicit bias (14,21). This is particularly important when specialist palliative care is able to provide continuity across healthcare settings, such as community-based programs that serve inpatients or stable inpatient teams that can see people across different admissions. Palliative teams can serve as a source of consistency and quality control and can have a role, ultimately, in assisting in the perilous transition of these children to the adult health system (21). Particularly, expert palliative care team members can bring skills in the appropriate and judicious use of opioids in the management of the acute and chronic pain of SCD. Pain Management Clinicians providing care for children and adolescents with SCD need not fear using opioids, but a plan must be put in place ahead of time. Pediatric patients with genotypes of SCD known to have increased risk of episodes of pain crisis should have a plan established with their outpatient provider that can be readily communicated with their local emergency departments and pediatric hospitals. Best practice includes having a written pain crisis action plan either on file in the Electronic Medical Record or carried as a sealed letter so that inpatient providers have the requisite background information (14). It is well known that rapid assessment and treatment of acute pain has been shown to decrease frequency of hospitalizations and duration of stay (22), but knowing what medications works best for each specific patient is critical. Moderate-to-severe pain crises require patient-controlled analgesia (PCA) with low or no basal and high bolus doses that can be readily started based on home medication dosing and knowledge of successful management of each child’s previous crises (23). Those children on home extended-release opioids should be continued on their home dose in the hospital. At discharge, any potential changes to home medication doses are preferably communicated to the patient’s primary outpatient provider so that they can be accomplished in the ambulatory setting. Additionally, the inpatient team should secure an appointment with that outpatient provider within 1-4 weeks and provide enough medication to last until that visit. These are important factors in ensuring adequate symptom control and preventing avoidable readmissions (14).
25
Conclusion Pain has a definite effect on the developing child with SCD and expert palliative care teams can play a pivotal role in ensuring adequate assessment and management of these sequelae. Palliative care teams begin to bridge some of the gaps in the lives of those with SCD by helping to ensure that these children’s symptoms are controlled, providing appropriate psychosocial-spiritual support, ensuring assistance for coping with acute and chronic illness, and beginning adequate planning for the future. When we partner with the multiple other teams engaged in the care of those with SCD, we provide an important service not only to these patients but to their families as well. Work Cited 1. Strouse J. Sickle cell disease. Handb Clin Neurol. 2016. 2. Sogutlu A, Levenson JL, McClish DK, Rosef SD, Smith WR. Somatic symptom burden in adults with sickle cell
disease predicts pain, depression, anxiety, health care utilization, and quality of life: The PiSCES project. Psychosomatics. 2011 May-Jun;52(3):272-9.
3. Brousseau DC, Owens PL, Mosso AL, Panepinto JA, Steiner CA. Acute care utilization and re-hospitalizations for sickle cell disease. JAMA. 2010;303(13):1288–1294.
4. Benz EJ. Disorders of hemoglobin. In: Fauci AS, Braunwald E, Kasper DL, et al. (Eds.), Harrison's Principles of Internal Medicine. New York, NY: McGraw Hill; 2008:635–642.
5. Sobota A, Graham DA, Neufeld EJ, Heeney MM. Thirty-day readmission rates following hospitalization for pediatric sickle cell crisis at freestanding children’s hospitals: risk factors and hospital variation. Pediatr Blood Cancer. 2012;58(1):61–65.
6. Frei-Jones MJ, Field JJ, DeBaun MR. Risk factors for hospital readmission within 30 days: A new quality measure for children with sickle cell disease. Pediatr Blood Cancer. 2009;52(4):481–485.
7. Salman ZA1, Hassan MK2. Hospitalization events among children and adolescents with sickle cell disease in Basra, Iraq. Anemia. 2015; 2015:195469.
8. Bakri MH, Ismail EA, Elsedfy GO, Amr MA, Ibrahim A. Behavioral impact of sickle cell disease in young children with repeated hospitalization. Saudi journal of anaesthesia. Oct 2014;8(4):504-509.
9. Gil KM, Carson JW, Porter LS, et al. Daily stress and mood and their association with pain, health-care use, and school activity in adolescents with sickle cell disease. J Pediatr Psychol. 2003; 28:363–373.
10. Haywood C, Jr., Bediako S, Lanzkron S, et al. An unequal burden: Poor patient-provider communication and sickle cell disease. Patient Education and counseling. Aug 2014;96(2):159-164.
11. Haywood C, Jr., Lanzkron S, Bediako S, et al. Perceived discrimination, patient trust, and adherence to medical recommendations among persons with sickle cell disease. Journal of General Internal Medicine. Dec 2014;29(12):1657-1662.
12. Waldrop RD, Mandry C. Health professional perceptions of opioid dependence among patients with pain. Am J Emerg Med. Sep 1995;13(5):529-531.
13. Maxwell K, Streetly A, Bevan D. Experiences of hospital care and treatment seeking for pain from sickle cell disease: A qualitative study. BMJ. 1999;318(7198):1585-1590.
14. Ajayi TA, Edmonds KP, Thornberry K, Atayee RA. Palliative care teams as advocates for adults with sickle cell disease. J Pall Med. 2016;19(2):195-201.
15. Lawoko S, Soares JJ. Quality of life among parents of children with congenital heart disease, parents of children with other diseases and parents of healthy children. Qual Life Res. 2003;12:655–666.
16. Sales E. Family burden and quality of life. Qual Life Res. 2003;12:33–41. 17. Helgeson VS. Social support and quality of life. Qual Life Res. 2003;12:25–31. 18. Hechler T, Kanstrup M, Holley AL, Simons LE, Wicksell R, Hirschfeld G, Zernikow B. Systematic review on
intensive interdisciplinary pain treatment of children with chronic pain. Pediatrics. 2015 Jul;136(1):115-27. 19. Odell S, Logan DE. Pediatric pain management: the multidisciplinary approach. J Pain Res. 2013;6:785–
790pmid:24250232 20. Hechler T, Ruhe AK, Schmidt P, et al. Inpatient-based intensive interdisciplinary pain treatment for highly
impaired children with severe chronic pain: Randomized controlled trial of efficacy and economic effects. Pain. 2014;155(1):118–128
21. Ajayi TA, Edmonds KP. Palliative care answers the challenges of transitioning serious illness of childhood to adult medicine. J Pall Med. 2014;17(4):469-71.
22. Brandow AM, Nimmer M, Simmons T, Charles Casper T, Cook LJ, Chumpitazi CE, Paul Scott J, Panepinto JA, Brousseau DC. Impact of emergency department care on outcomes of acute pain events in children with sickle cell disease. Am J Hematol. 2016 Aug 12.
23. Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. Management of sickle cell disease: Summary of the 2014 evidence-based report by expert panel members. JAMA. Sep 10 2014;312(10):1033-1048.
-###-

26
ASSESSMENT AND MANAGEMENT OF PAIN AND IRRITABILITY IN CHILDREN
WITH SEVERE NEUROLOGIC IMPAIRMENT (SNI): AN OVERVIEW
Lanna Olson, MD FRCPC
Palliative Care Fellow Canuck Place Children’s Hospice
Vancouver, British Columbia, Canada [email protected]
Case Vignette: 3-year-old Lisa has severe neurologic impairment (SNI) of unknown etiology. She is unable to communicate and has severe cognitive impairment. Lisa and her family live in a small rural community, with the busy local Family Physician being the primary point of medical contact. Lisa is followed intermittently by multiple sub-specialists at a tertiary care hospital over three hours away. You are seeing Lisa in the local General Pediatrics office for the first time. Her parents are concerned that she is “more irritable” and requested a referral. She has been grimacing, moaning, and crying out in an unpredictable pattern for the last month and a half, worsening significantly over the last week. No medical workup has been undertaken since the time of the referral, which was made 1 month ago. Her parents are hopeful that a Pediatrician will have “more time” to spend with Lisa. This article aims to highlight the challenges in recognizing and treating pain in children with SNI, suggests some basic considerations when evaluating pain and irritability in this unique population, and explores some of the research that is currently being done. Providing care for children with SNI can be daunting for the unfamiliar practitioner. In addition to medical care, families require guidance navigating the healthcare system and advocating for their children. Children with SNI now comprise 50% of the patients served by Pediatric Palliative Care teams in North America, emphasizing the need to educate the medical profession on this unique and growing patient population (1). The causes of SNI range from acquired hypoxic-ischemic encephalopathy to genetic neurodegenerative diseases, although for some children no etiology is ever identified. In addition, children with SNI are cognitively impaired and unable to communicate verbally. Despite the differences in their underlying conditions, children with SNI all share the same vulnerability and prognostic uncertainty. Sadly, most children with SNI live short lives, but with medical advances some now survive into early adulthood. Living longer creates more uncertainty given the limited data on “what to expect” as these children and teens progress along their disease trajectory. Studies have documented the large symptom burden affecting children with SNI. A multi-center randomized study, Charting the Territory, found that on average children had three symptoms of concern: pain, poor sleep, and feeding difficulties, with pain being the most common (1). Despite a symptom burden paralleling children with cancer, practitioners caring for children with SNI lack evidence-based symptom management guidelines (1). In 2011 the World Health Organization acknowledged the urgent need for quality research to help enhance our understanding of this population and provide better clinical care (2). Hunt and colleagues introduced three key forms of knowledge to enhance care for children with SNI and their families: “knowing the child, knowing the population and knowing the science” (3). Knowing the child stresses the importance of knowing the typical behaviors and mood of each child, in addition to their unique medical history and social circumstances. Knowing the population involves recognizing trends present in all children with SNI. These first two components will require significant commitment from health care practitioners on an individual and institutional level. Knowing the science includes knowing the diverse individual medical conditions, the potential medical complications and disease trajectory, and evidence-based treatments. Unfortunately, data on each of these components is sparse.

27
At first, physicians and nurses may feel uncomfortable caring for patients with complex care needs (1). Frustration may develop from external difficulties: coordinating multiple tests, following up results, and arranging treatments. Despite challenges, referring to pediatric subspecialists for the initial work-up and management of pain/irritability is not practical. Long wait-times will only lead to additional distress for the patient and his or her family, which negatively impacts quality of life and sense of burden on the parent. (4) This becomes even more relevant for rural and transitioning adolescent populations, when the family physician typically becomes the primary point of medical continuity.
When it comes to recognizing pain, existing data suggests that children with SNI experience more pain than healthy “unaffected” children (1). Pain, however, is inferred from pain-like behaviors which can vary greatly between children. Given the severe communication challenges affecting most children with SNI, interpretation of these behaviors is difficult (3). Research suggests that parents are able to recognize subtle changes in their children’s behavior from baseline, whereas clinicians tend to underreport symptoms (4). We are very reliant on parental report as it is the child's behavior, rather than verbal report, which has to be interpreted to determine if they have pain. The inherent difficulty in distinguishing which behaviors indicate pain have led to the development of pain assessment scales specifically geared toward children with disabilities. These tools can also be used to track response to therapeutic interventions (5). The Non-Communicating Children’s Pain Checklist-Revised can be used for children 3 to 18 years and administered by family members, care givers, and healthcare providers. It requires charting the child’s behaviors over a two-hour period, and if a cutoff score is exceeded, the child is likely to be in pain. An alternate version, The Non-Communicating Children’s Pain Checklist-Postoperative Version, can be used if pain is suspected after procedures or in the post-operative period. The Pediatric Pain Profile is another tool, which involves creating an individualized pain profile for the child. Although valid, this tool is not generalizable. It allows for long term tracking of symptoms and comparison to the child’s unique symptom baseline. Use of pain assessment tools, regardless of which is chosen, in addition to good communication with parents and caregivers, can help assess and monitor symptoms in children with SNI (5, 6).
Children with SNI have many potential sources of pain and therefore the differential for unexplained pain-like behaviors and irritability must remain broad. For instance, limited weight bearing and poor nutrition predisposes to pathological fractures, differences in muscle tone can affect gut motility and exacerbate constipation, and inadequate seating and splints may trigger pressure sores. Spasticity, gastro esophageal reflux, constipation, pathological fractures, dental problems, and iatrogenic pain have been cited as common causes of pain in children with cognitive impairment and limited communication (6). It is important to remember that everyday causes of pain (headache, teething, menstrual pain, etc.), which can affect all children regardless of cognitive ability, can also affect children with SNI and should not be overlooked. Existing literature suggests that when the source of pain is not identified, it may be due to a central-neuropathic pain, also known as neurological irritability (5). This type of central pain is thought to be related to primary activation of pain centers in the central nervous system without an external nociceptive trigger. As children with SNI age and functional abilities change, their ability to process and express pain may change. The exact relationship between functional status and expression of pain remains unclear (1). Charting the Territory found that children with G/J tubes, extensive mobility modifications, and lower levels of functioning experience higher symptom burden (1). This may be a result of more advanced disease or directly related to the presence of assistive devices and technology. Clearly, more research is required.
With this in mind, we are in need of a better approach to these patients to guide primary care practitioners. Siden et al. has attempted to bridge this gap in care, by creating a systematic protocol for evaluating and treating pain and irritability in children with SNI (7). The proposed pathway will be

28
evaluated through a proposed multi-center study, the first of its kind. The assessment begins with a full patient history, including a detailed pain history and physical exam. If information from the history and physical is suggestive of a particular pain source, directed testing for suspected causes should be done. If no obvious cause is identified, screening tests to assess for common medical complications will be done. Once again, if all screening tests are normal, the pain and irritability may be secondary to underlying central neurological irritability and treatment is initiated with the anti-convulsing gabapentin. Children with SNI are often prescribed multiple medications to manage their symptom burden despite limited evidence directing which medications should be used and which are effective (1). While the literature is generally limited, there is emerging evidence suggesting the use of gabapentin for undifferentiated pain in this population (8). A parallel pilot study evaluating medications to target pain/irritability when not resolved with the clinical pathway will also be undertaken to help guide future research. Secondary outcomes including quality of life, ease of implementation, and family feedback will also help with practical aspects of using an algorithm to assess children with SNI.
Additional research, both qualitative and quantitative, is needed to assist our understanding of the families and children we care for. Areas for future exploration include the impact of mental health conditions, including anxiety and depression, in children with SNI and their impact on behavior. In addition, the distinct conditions represented under the SNI umbrella deserve individual exploration, a point emphasized in one study demonstrating the differences in symptom expression between Batten’s Disease and Mucopolysaccharidoses (4). Symptoms have deep meaning for families, especially if they are deemed to represent disease progression (4). The care team should be mindful of this, and pay particular attention to parent coping around times of transition and changes in baseline functioning. In addition, parents of children with SNI experience more anxiety, depression, and feelings of burden when their child is experiencing pain and irritability. This emphasizes the need for a holistic bio-psycho-social approach when caring for children with SNI.
Return to our case: You perform a thorough history and physical. It is revealed that, for the last 3 weeks, Lisa has been holding her left leg in an abducted and externally rotated position. She seems to flinch and grimace when being transferred from wheelchair to bed. She hasn’t been sleeping well, moaning and whimpering throughout the night. Her parents have not trialled any medications, for fear that they may interact with her anti-convulsants or formula. Her mother notes and distinct change from baseline, “something is wrong”. Lisa is known to have osteopenia, but hasn't been on any supplemental vitamins or minerals. This, in addition to her reduced mobility and use of anticonvulsants, places her at high risk for pathological fracture and you suspect involvement of her left femur. She is sent for urgent X-ray which confirms your suspicion and you arrange for orthopedics to see her urgently. She is provided with morphine for pain control and settles. In consultation with the subspecialist and team nutritionist, Lisa’s diet is supplemented to optimize bone strength (or density). References: 1. Steele R, Siden H, Cadell S, et al. Charting the territory: symptoms and functional assessment in children with
progressive, non-curable conditions. Arch Dis Child. 2014;99(8):754-762. doi:10.1136/archdischild-2013-305246. 2. Milani B, Magrini N, Gray A, Wiffen P, Scholten W. WHO calls for targeted research on the pharmacological
treatment of persisting pain in children with medical illnesses. Evidence Based Child Health Cochrane Rev J. 2011;6(3):1017-1020.
3. Hunt A, Mastroyannopoulou K, Goldman A, Seers K. Not knowing-the problem of pain in children with severe neurological impairment. Int J Nurs Stud. 2003;40(2):171-183.
29
4. Malcolm C, Hain R, Gibson F, Adams S, Anderson G, Forbat L. Challenging symptoms in children with rare life-limiting conditions: findings from a prospective diary and interview study with families. Acta Paediatr. 2012;101(9):985-992. doi:10.1111/j.1651-2227.2012.02680.x;
5. Medical Care of the Dying Textbook, 4th edition, Victoria Hospice Society. 2006. 6. Stallard P, Williams L, Lenton S, Velleman R. Pain in cognitively impaired, non-communicating children. Arch Dis
Child. 2001;85(6):460-462. 7. Siden, H. Treating Pain & Irritability of Unknown Origin (PIUO) in Children with Complex Conditions. Proposal
2015. 8. Hauer JM, Wical BS, Charnas L. Gabapentin Successfully Manages Chronic Unexplained Irritability in Children
With Severe Neurologic Impairment. Pediatrics. 2007;119(2):e519-e522. doi:10.1542/peds.2006-1609.
-###-

30
NONPHARMACOLOGICAL PAIN MANAGEMENT FOR CHILDREN
Kathy Davis, PhD, MSEd Associate Professor of Pediatrics
Director, Pediatric Palliative Care and Ethics University of Kansas Medical Center
Kansas City, KS [email protected]
Introduction Pain is defined by the International Association for the Study of Pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage (International Association for the Study of Pain, 1979). Pain in infants, children, and adolescents (referred to as children for remainder of this article) is often misunderstood, underestimated, and undertreated or untreated. Clinicians widely believed, up until the late 1980s, that the neonate was undeveloped and, thus, was incapable of feeling pain (Owens & Todt, 1984). Others continue to question a child’s pain experience, believing that children do not feel pain the way adults do. Clinicians continue to express concern about dosing of pain medications, especially opiates and, thus, have fear about overdosing the infant or child (Sidhu & Tickner, 2016). As a result of these and related deficits in knowledge, pain management in neonates and children is often minimized or ignored (Bawa et al., 2015). Pain assessment is complicated. There is not a physical means of assessing pain; rather, behavioral indicators including facial expression, verbalizations, or cry and body responses are often used to identify pain in children (Voepel-Lewis, 2011). Assessing and treating pain is critical due to the consequences of inadequate pain management which can be both short-term and long-term. Both physical and psychological sequalae may be long-term complications of poorly treated pain (Weisman et al., 1998; Kennedy et al., 2008; AAP Committee on Fetus & Newborn, 2006; Mitchell & Boss, 2002; Lonnqvist & Morton, 2005; Wong et al., 2012). Small babies are also at greater risk of developing long term effects that impact behavior and development when their pain is untreated or undertreated. Immediate effects of inadequate pain control in infants may include irritability, fear, sleep disturbance, and eating difficulties. Short term effects may involve delayed healing, impaired emotional bonding, and altered immune system while long term effects include memory of pain, developmental retardation, and altered response to future pain experiences (Mathew & Mathew, 2003). Although pain scales and behavioral observations may offer good information regarding a child’s pain, other children do not report pain because they do not want to disappoint caregivers or because they want to be brave (Gerik, 2005). While it is true that many children cry, whine, wiggle, or even act out as an expression of pain, other children become very quiet and very still when they experience pain, especially chronic pain. One of the most effective analyses of pain in a child is the parent’s report that the child “isn’t acting like themselves.” A change in the child’s typical behavior should be assessed as a possible indicator that the child is experiencing pain. When it is determined that pain is present, the next step is to determine the cause of the pain and develop a multimodal approach to pain management. There is no question that pharmacologic pain management is sometimes the best option for achieving good pain control. However, the pain experience is not unilateral but includes physiological, emotional, cultural, and cognitive components (Chiaretti et al., 2013). Thus, a combination of pharmacologic pain management and nonpharmacological pain strategies
31
may offer the best pain management strategy. Nonpharmacological interventions may also be the primary or only strategy that is required in some pain situations. To achieve the best results, the approach to acute pediatric pain management should be multidisciplinary, including psychologists, social workers, pediatric palliative care providers, child life specialists, parents/caregivers, nurses, and physicians, and multimodal, with nonpharmacological and pharmacologic components. A pain regimen that is stepwise and individually tailored to the individual is recommended for all pediatric patients (Ruest & Anderson, 2016). In 2001, a statement was published by the American Academy of Pediatrics and the American Pain Society regarding the treatment of infants’ and children’s pain. The statement noted that pediatricians are “responsible” for using a multimodal and multidisciplinary approach aimed at both treating and eliminating pain in children whenever possible (AAP Taskforce, 2001). Around the same time, the Joint Commission on Accreditation of Healthcare Organizations (TJC) referred to pain as the “fifth vital sign” and began mandating the assessment and documentation of patients’ pain (Phillips, 2000). In further support of this method of pain treatment in pediatrics, several clinical practice guidelines and research studies were published which recommended the use of validated pain assessment tools in concert with a multimodal and multidisciplinary approach to pain management (Chiaretti et al., 2013, Cramton & Gruchala, 2012; McGrath, 2011). Nonpharmacological Pain Management Nonpharmacological pain management is the management of pain and anxiety without the use of medications. Rather, this type of pain management uses ways to change thinking, perception, and focus to change ones pain experience. Common nonpharmacological pain strategies for children include:
Distraction/diversion (toys with lights or movement, video, computer games, iPad or tablet, choices, focus on dialogue or topic) Comforting touch (stroking, rubbing, massage, cuddling, holding, rocking) Tactile comfort (heat, cold, ice, transcutaneous electrical nerve stimulation (TENS), Buzzy Controlled breathing (bubbles, blowing, breathing exercises) Relaxation (progressive muscle relaxation, breathing exercises, music) Psychology - requiring training (guided imagery, biofeedback, music therapy, cognitive behavioral therapy (CBT), hypnosis Strategies for babies – (holding, rocking, 5 Ss, sucrose, breastfeeding, non-nutritive sucking)
The clinician’s role is to work with the child to develop an effective nonpharmacological pain management program for the child and to teach the child and parent(s) how to employ the strategies. Parents are the best coaches for their child for a variety of reasons. First, children naturally want their parent to be with them when they are experiencing pain. Thus, it is advantageous to provide the child with a coach in whom the child has trust and who is always available to them when painful stimuli present. Parents may feel helpless when their child is hurting if they feel unable to help them. Coaching parents about what to expect and providing developmentally appropriate ways for them to participate in their child’s care can be beneficial both to the child and parents (Krauss et al., 2016). In addition to the aforementioned strategies, children should always have adequate information about their body, their illness or diagnosis, and what is about to occur that may result in pain. Parents or other primary caregivers should always be available to the child. Children should have heavy doses of choices, control, laughter, and fun to ensure that their basic needs are being addressed.
32
Setting the stage, if there is time to do so, is an important first step. If the clinician is teaching nonpharmacological pain strategies, the setting should be age-appropriate and child-friendly in order to minimize anxiety and fear. An environment that is peaceful, calming, and inviting will encourage the child to come in with curiosity and inquiry but without fear or anxiety. Even if the setting is the emergency department or a treatment room where bright lights are necessary, the clinician should bring child-centered items and use language which will ensure the child perceives calmness and comfort. Toys, books, games, and other kid-friendly materials may help level the playing field for a fearful child. Child-friendly items can be stored in a large canvas bag, ready to be called into duty whenever needed. Supplies might include bubbles, a pinwheel, Silly Putty, a squeeze ball, toys with visual components such as lights or moving parts, rattles, whistles and New Year’s Eve blowers, puppets, handheld video games, a book with baby/toddler faces, or a book with the ABCs. Distraction techniques such as bubbles, toys, pinwheels, and technology devices can be employed by the child’s caregiver, child life specialists, or other staff without prior training (Cramton & Gruchala, 2012; Fein et al., 2012; Merritt, 2014; Wente, 2013). Attempting to teach more complex strategies when the child is anxious or when time is not sufficient may result in the child experiencing no benefit from the interventions or that, in the future, he or she may discount the idea of nonpharmacological pain interventions as being likely to fail. Of equal importance to the environment is the relationship between the clinician who will be guiding the child and parent in learning nonpharmacological techniques. Strategies are often taught by a psychologist, child life provider, educator, or a nurse. If the youngster is trying to determine if the clinician can be trusted, his ability to concentrate will be diminished. If the clinician is a stranger, scheduling at least one or two sessions to practice strategies prior to using them is recommended. During the first meeting, the child may choose the activity to “break the ice” and to get to know and trust the clinician. Possible activities include playing with a developmentally appropriate toy or activity, singing songs together, or doing a craft while getting to know, and trust, the clinician. Parents will also benefit from building a sense of trust in the clinician. Helping the child and parent/guardian develop the right approach to nonpharmacological pain management is a process which is essential to the success of nonpharmacological strategies. The child and parents must believe the strategies are going to be effective if they are going to be effective. This writing will recommend a method to ensure that each child in pain is receiving the pain management that he or she needs. That method is the Individualized Pain Management Plan (IPMP) which should be developed for each child who experiences pain. The IPMP should include both pharmacologic and nonpharmacological methods of pain management and be developed specifically for the unique, individual child with consideration of the child’s age, developmental stage, physiologic and psychologic components of pain, past pain experiences with pain, and, for children who can express it, personal preferences. The components of a child’s IPMP should be written out with copies distributed to the child, parent, physician, nurses, psychologist, child life specialist, and others who work regularly with the child. This article will help clinicians develop the IPMP for specific patients by including information unique to specific ages and stages along with strategies for pain management that have evidence for working with those groups of children.

33
Nonpharmacological Pain Management for Infants Benjamin Franklin’s statement, “An ounce of prevention is worth a pound of cure” is very true in reference to managing pain. The pain experience is similar, and perhaps more intense, in infants, including newborn babies, than in older children and adults. Managing the pain of an infant is difficult because the baby cannot express what he or she is feeling and we can only guess, based on baby’s behavior. First, baby’s caregivers must be aware that the baby has the capacity to feel pain. With increased awareness of the baby’s capacity for pain, adult caregivers may be able to prevent some painful stimuli from affecting baby. In addition, assessing the cause and the severity of pain helps caregivers to plan next steps. Rather than listing strategies that may be offered or used in the baby’s IPMP, this section will discuss strategies that are known to be comforting to infants and which may be used to comfort a baby who is experiencing pain. Unlike older children, a baby’s needs do not require a formal IPMP. That is not to suggest that their pain is less, but that they are not yet able to make pain management choices. Parental holding and strategic positioning may also be a helpful place to start in reducing baby’s pain or discomfort. Reduced stress for infants may be achieved by placing baby in a position where he or she is comfortable and senses that he or she is secure. For example, baby may sit on Mama’s lap in a variety of positions: cradled; sitting on the mother’s lap facing away from mother; being held upright with head balanced on mother’s shoulder, etc. In each position, mother can embrace baby firmly but gently, providing a sense of security (Corff et al., 1995) and identifying which position seems to make baby most comfortable. Other strategies focus on oral routes of comfort such as non-nutritive sucking on a pacifier or sucking a pacifier that has a solution of 24-30% sucrose on the nipple (Lewindon et al., 1998; Harrison et al., 2010; Yilmaz et al., 2014). The use of sucrose combined with non-nutritive sucking, skin-to-skin contact, and breastfeeding during minor procedures has been associated with decreased objective measures of pain such as duration of crying and baby’s heart rate (Cramton, & Gruchala 2012). Some studies suggest that the most effective method of pain management for babies is breastfeeding (Reece-Stremtan & Gray, 2016; Shah et al., 2012; Shah et al., 2006). Non-nutritive sucking, sucrose combined with sucking a pacifier and breastfeeding appear to be effective only in children under 1 year of age (Harrison et al., 2015). A few other strategies have been tested for effect on pain with infants. The Five S’s for Soothing a Baby may calm a baby by re-creating the noises, movement, and snug environment of the womb (Karp, 2015). These strategies are said to help baby calm and achieve sleep. The strategies include swaddle, side or stomach position, “shush” the baby, swing, and suck. Although primarily suggested as methods to help baby go to sleep, the Five Ss are also used, together or alone, for babies experiencing pain. Two other techniques have variable results during testing. First, the Mimo pillow provides infants with comfort through mediation of a parent’s physiological features, such as heartbeat. Clinical tests are reported to show a shorter recovery time after diaper change and shorter drying times for infants (Chen et al., 2015). Second, mechanical vibration has been evaluated for relief of pain associated with heel sticks in neonates. Results were not conclusive since the technique was used along with sucrose and a pacifier, thus confounding the effect (Baba et al., 2010). For infants under the age of one year, much of what constitutes pain management comes from contact with the parent or other trusted caregiver. Developmental stage, maturity, and age may be factors in which pain management strategy works best for an infant. For example, very young infants may prefer skin-to-skin contact or “shush”ing, while the older infant may find the greatest comfort in being held tightly or rocked. Preferred techniques may also vary between caregivers. Baby may like Mom to provide skin-

34
to-skin contact, while the most effective pain management strategy with Dad exists when baby is lying on his or her side on Dad’s arm. Pain management for procedures such as a vaccination, blood draw, or other events known to induce sudden pain, should be offered not only during the procedure but also immediately following the procedure. Finding the most effective method requires trial and error between each baby and each caregiver who will be present during painful events or times. Nonpharmacological Pain Management for Children and Adolescents Pain management for children over the age of one year becomes highly differentiated as it must meet the preferences of the unique child as well as be appropriate for the child’s age, developmental stage, maturity, prior pain exposure and experience, and the type/intensity/frequency of pain the child is experiencing now. A good place to start is with a comprehensive assessment of the unique child. Nonpharmacological strategies should never be “one size fits all.” Individual differences in the child’s prior experiences with pain, plus his or her temperament and age are imperative to consider prior to developing the IPMP for the child (Landler & Tse, 2010). If one strategy is not effective, another strategy should be tried. In addition, nonpharmacological strategies, ideally, should not be attempted for the first time when the child is stressed out or frightened. Practice may never “make perfect” but it certainly does provide a child with competence and confidence in the case of nonpharmacological pain management strategies. Finally, another important tool is an understanding of developmental levels in relationship to pain management. An overview of age levels and what is known about a child’s concept of pain at each level will be offered, followed by specific pain management strategies known to work with that age. A word of caution: Age is not synonymous with developmental stage. The guidelines should be a launching point but should not bind the child to a certain strategy at a specific age. They are simply that: guides to offer a possible place to start with a child. Some children have very individual preferences which do not “fit” into a chart. Let the child guide the process rather than being bound by the suggestions. Toddlers Language and verbal skills are limited during the toddler period and are very inconsistent from child to child. The toddler will not be able to use words to tell us about his pain. Rather the toddler’s pain-related behaviors may inform us about his pain through the child’s facial expression, crying, body movements, holding or touching a certain body part, or extension of arms or legs. According to O’Rourke (2004) these behaviors provide more objective and reliable measures of pain than any “reports” that we may be able to try. Early research by Beyer and Wells (1989) provided insight into the communication of toddlers regarding pain experiences. A two-year-old can, usually, report the location of the pain and tell how it happened. However, such children do not yet possess the cognitive skills to describe the severity of the pain. By age three years, most children can describe the severity of the pain through the use of a three-level pain scale (no pain, a little pain, a lot of pain). Usually, children in this age group can engage in conversations and talk about whether or not they feel pain and “how bad it is.” In addition to the toddler’s emerging self-assessment of their pain, the reports of caregivers can be invaluable in assessing pain in this age group. Fear may impact the toddler’s pain experience as well as their expression of pain and reports of pain. However, caregivers may have difficulty assessing the toddler’s pain. Crying, screaming, or other behaviors associated with fear may be interpreted as pain by parents and health care providers. Toddlers may have developing capacity to report their pain or they may use only one word such as ”owie” or “boo-boo“ to describe their pain. Some children may become very quiet and inactive while in pain or their activity level may increase and be associated with whining and/or aggressive behavior. A parent’s report that “my child isn’t acting like he normally does” may tell us a lot or very little due to factors such as separation anxiety, memory of previous painful experiences, or
35
physical restraint (Rivera, 1991). Fear and anxiety can affect or intensify a child’s pain experience and how the child experiences and assimilates the painful situation (Cramton, & Gruchala, 2012). Therefore, it can be emotionally beneficial to address fear and anxiety by nonpharmacological methods such as distraction. Pain management can be used in the clinic, hospital, home, or any setting where the child experiences pain. Pain comes in a variety of shapes and sizes including that which is associated with the child’s diagnosis (sickle cell, arthritis, etc.) or from an injury or trauma (burns, dog bites, factures, skin grafts in plastic surgery, etc.). Pain management may prove challenging in children with recurrent pain such as abdominal pain or headaches. The medical provider may induce pain during procedures like injections, circumcisions, IV starts, etc. Nonpharmacological pain management strategies can be used in any location and for any type of pain. Once the child’s IPMP is developed, any necessary materials can be put into a small bag to travel with the child and parent and be ready for use. Some resources recommend positive reinforcement, or praising the child for being brave during a procedure, surgery, or while healing from an illness, or rewards like games, toys, etc., for the same purpose. This seems to be a dangerous message, however, as it suggests that the child has control over being “good” or behaving in the face of pain. If the child is unable to “be brave” or “good” and shows an expression of pain, the child is likely to feel that he or she has failed and now may feel even more out of control. Showing love, empathy, and support are likely to better help the child cope with a situation over which he or she has no control. Strategies for Toddlers A rule of thumb with toddlers is “keep it simple.” Always speak to the child’s primary health care provider before using any pain management strategy. The following strategies are known to be effective with toddlers: Parent/caregiver presence (whenever possible) Distraction – used during procedures (venipuncture, dressing change, etc.) and as needed Toys that move, have lights or sound Puppets Videos (determine which ones they prefer) Reading, playing a game Controlled breathing
Blowing bubbles, pinwheel Blowing away the pain Tactile – used before, during, after pain is induced and as needed Buzzy (https://buzzyhelps.com/) Cold Heat Touch or massage Cuddling Holding, Rocking Choices (“Would you like ice on your owie or do you want me to gently rub it?”)
36
Preschoolers
Pain assessment begins to become more reliable as children grow and develop. For example, most four-year-old children are able to use pain discrimination scales which use 4 or 5 categories of pain (Goodenough et al., 1997]. By around 5 years of age, children begin to realize the significance of the pain experience as they are able to rate the intensity of pain (St. Laurent-Gagnon et al., 1999). Preschoolers love to learn. Teaching them about their body and their pain is an essential part of nonpharmacological pain management. They also benefit from explanations about what is happening during procedures or why they are experiencing chronic pain. A benefit of nonpharmacological pain management strategies is that discussing the pain and creating an IPMP increases the child’s awareness of their pain as they learn to develop methods to gain ownership of their pain and, thus, increase control of the pain. The findings of Bringuler et al., (2009) suggest there are a moderate level of false negatives on the top 4 behavior rating scales, meaning there are children who are in pain and whose pain is not currently being recognized or acknowledged. The negative effects of untreated or undertreated pain in young children was previously discussed in this article. Functional MRI studies show the midbrain and higher cortical areas of the brain, known to modulate pain, are activated when distraction is introduced (Valet et al., 2014; Tracey et al., 2002). Since verbal reasoning or reassurance is not typically understood by children less than 5–7 years it follows that distraction techniques are likely to be more effective with preschoolers than other strategies of pain control. (Krauss et al., 2016). Strategies for preschoolers
Physical proximity of parent/caregiver (whenever possible)
Distraction All strategies recommended for toddlers Recalling lists (all of your teddy bears, favorite toy cars, kids in your class at
school/dance class/soccer team, etc. Manipulating squeeze ball Counting, reciting ABCs Video games Relaxation Breathing exercises (after practice) Muscle relaxation (turning your arm, body into “a bowl of gelatin”) Guided imagery Beginning strategies – picturing laying in their bed at home (after practice) School-age Children By the time a child reaches school age, he or she can report his or her pain more accurately and by 8 years he or she can describe the location reliably. At this age, psychological factors should also be considered as there may be a correlation with physical pain. School absence or recurrent headache or stomachache without physiologic cause may indicate that there are psychological issues resulting in physical symptoms (Gerik, 2005). School-age children can become engaged in a favorite activity or game and not show behavioral indications of pain and can show self-control when they are in pain. For some children, cultural or familial norms may suggest that pain should be minimized or the child may refuse to disclose pain in an attempt to deny pain (Rivera 1991). When engaged in distraction techniques, children
37
between the ages of 7 and 12 years showed a statistically significant reduction in pain compared to controls during venipuncture (Karakaya & Gozen, 2016). School-age children can also engage in other forms of pain management. Breathing exercises and progressive muscle relaxation are effective strategies at this stage of development. Practice helps make each of these strategies become effective options for pain management. School-age children often like to teach these strategies to parents, siblings, and others. One patient took the strategies back to school where the teacher used them when students became a little too active. Guided imagery is effective with some children at all ages of school-aged, depending on their developmental stage. Children with active imaginations may not only be able to visualize being in a favorite location, but also smell the smells, hear the sounds, and feel a warm breeze. By later in the school-age period, children may have success in using hypnosis to train the unconscious mind to promote pain relief (Gerik, 2005). Hypnosis is provided by individuals trained specifically in the practice. Strategies for School-age Children School-age children may benefit from any of the nonpharmacological pain management strategies. The task is to determine which strategies work best for specific child based on his or her unique issues and needs. Consider all previous mentioned strategies for toddlers and preschoolers in addition to:
Distraction All strategies recommended for toddlers and preschoolers
Recalling lists (name everyone in your class, row by row, etc.) Video games (become a key tool in distraction) iPad or Tablet Relaxation Breathing exercises can become a cornerstone of relaxation Progressive muscle relaxation Guided imagery Hypnosis Biofeedback Cognitive Behavior Therapy Adolescents Adolescents are approaching an ability to characterize and accurately describe their pain, intensity, and location because they know the words and concepts to discuss their pain. However, there is a strong psychologic component which may be important to teens (Gerik, 2005). It is common for adolescents to want to control their response to pain, especially in front of friends, and this need to maintain control may trump attempts to ensure adequate pain management. They want privacy and choice and may or may not want parents to be present (Srouji et al., 2010). In addition, adolescents crave privacy and do not want adults to know what they are thinking or feeling. As a result, it is important for clinicians to gain the trust of teens in order to understand and provide help in managing their pain. If a clinician fails to give the teen choice (i.e., regarding parents’ presence) or ask about a preference in morning rounds with others present, the adolescent may refuse to work with that individual (Gerik, 2005).
38
Adolescents do not just want – they expect – developmentally appropriate information about procedures, what they may anticipate, and how it will feel. It is not unusual to observe regression in the behavior of adolescents under stress (Hagan et al., 2001). It is difficult for teens to be told what will, and will not, work to alleviate their pain. Rather, they need to be able to refuse or request certain medications and strategies in order to make procedures or other pain-invoking events more tolerable (Srouji et al., 2010). Strategies for adolescents Adolescents may benefit from strategies from all previous categories – even from the toddler list – if they would admit it. Adolescents who have experienced regression may appreciate having parents nearby and having Mom rub their back or feet. Rituals, important to toddlers and preschoolers, may resume importance in normal adolescence when illness has removed all predictability and the familiarity of rituals is comforting. Trust cannot be overemphasized. Clinicians must gain the trust of adolescents in order to be able to help them with pain management. Distraction Music (headphones) Videos – YouTube, online Writing Journaling Blogging Pain journals Guided imagery – may be very successful when teens buy-in to this strategy Biofeedback Cognitive Behavioral Therapy (CBT) – allows ownership of pain control Hypnosis – See Guided imagery. Also successful with self-hypnosis.
Engaging with/teaching strategies to younger children – can only occur after mastering the strategies themselves.
Special Considerations Chronic pain is expressed in unique ways among children with chronic pain, which is different from the pain expressed by children with new onset pain (Fein et al., 2012; Krauss et al., 2016).The five-year survival rate for childhood cancer now exceeds 80% resulting in a large group of long-term survivors whose needs are just becoming known (Jemal et al., 2008). These survivors have experienced large numbers of invasive procedures such as bone marrow aspiration, lumbar punctures, and more. Furthermore, there was not yet evidence of the impact on untreated pain when many of these young people went through treatment. Thus, procedural pain, anxiety, and distress may have caused a significant burden on many cancer survivors treated in childhood. Former pediatric cancer patients and their parents have identified procedure-related pain as one of the most difficult and distressing parts of having cancer (Zernikow et al., 2005). Pai and Kazak (2006) identified that procedure-related distress exists for years after treatment has ended and Doellman (2003) found the same extended duration of anxiety and distress. More recently, 31% to 84% of children and adolescents with cancer reported using some form of complementary and alternative medical (CAM) therapies (Sencer & Kelly, 2007) and that they have found effectiveness in relieving procedure-related pain, anxiety, and distress (Evans et al., 2008). Another population with unique needs is that of children with developmental disabilities who may experience pain in a more intense or heightened manner. In addition, some children in this group do not

39
have communication skills that enable them to express pain or anxiety in a way that is readily understood (Fein et al., 2012; Krauss et al., 2016). Parents and caregivers provide the only link to identifying the youngster’s pain. Children who are on multiple medications (i.e., Benzodiazepines) may be at risk of sleep apnea. Special care must be taken for children who are on multiple medications (particularly benzodiazepines) or are at risk of respiratory insufficiency (e.g. sleep apnea). Those with hepatic or renal disease may have impaired metabolism or clearance of opioids and their metabolites. Patients with renal disease may be more sensitive to adverse effects from NSAIDs. Consultation with dosing guidelines or a pain specialist should be considered for such children. (Fein et al., 2012; Krauss et al., 2016). Conclusions Pain presents in a variety of settings and in various ways unique to each child. A child’s age, developmental stage, source of pain, previous pain experience, and maturity all may affect the pain experience. Assessing a child’s pain is difficult and requires consideration of all of the aforementioned variables. As a result, pain management is unique to each individual child who is experiencing pain. One size does not fit all and pain management strategies may need to be revised often for a child. The various pain management strategies may be used across developmental stages as desired by the child with pain. Infants, toddlers, preschoolers, school-age children, and adolescents may utilize unique ways to control their pain management strategies or may use some of the same pain management methods. The development of an Individualized Pain Management Program, or IPMP, will enable each child to incorporate strategies uniquely suited to them. Although children can learn to manage many of the strategies to control pain, a coach to help with some strategies is recommended. An ideal method is to have the clinician coach the pediatric patient and parent in learning pain management strategies. The goal is for the parent to become the child’s primary pain management coach. The parent will play a graduated role in helping the child from complete responsibility for implementing strategies for the infant, increasing to minimal input with adolescents. This partnership between parent and child mirrors the child’s growing independence while still allowing parents to have a meaningful role in caring for their child when he or she is experiencing pain. References American Academy of Pediatrics Committee on Fetus and Newborn, Section of Surgery and Section of
Anesthesiology and Pain Medicine (2006). Prevention and management of pain in the neonate: An update. Pediatrics; 118:2231–2241.
American Academy of Pediatrics Taskforce. Committee on Psychosocial Aspects of Child and Family Health, Task Force on Pain in Infants, Children, and Adolescents. (2001). The assessment and management of acute pain in infants, children and adolescents. Pediatrics;108(3):793-797.
Baba LR, McGrath JM, Liu J. (2010). The efficacy of mechanical vibration analgesia for relief of heel stick pain in neonates: A novel approach. J Perinat Neonatal Nurs;24(3):274-83.
Bawa M, Mahajan JK, Aggerwal N, Sundaram J, Rao KL. (2015). Barriers to pediatric pain management in children undergoing surgery: A survey of health care providers. J Pain Palliat Care Pharmacother;29(4):353-8.
Beyer JE & Wells N. (1989). The assessment of pain in children. Pediatric Clinics of North America.36;4:837–854. Bringuler S, Pico M-C, Dadure C, Rocette A, Raux O, Boulhais M & Capdevila X. (2009). A prospective comparison
of post-surgical behavioral pain scales in preschoolers highlighting the risk of false evaluations. Pain.145;(1-2):60-68.
Chen W, Oetomo SB, Tetteroo D, Versteegh F, Mamagkaki T, Pereira MS, Janssen L, van Meurs A. (2015). Mimo pillow--an intelligent cushion designed with maternal heart beat vibrations for comforting newborn infants. EEE J Biomed Health Inform;19(3):979-85.
Chiaretti A, Pierri F, Valentini I, Russo I, Gargiullo L & Riccardi R. (2013). Current practice and recent advances in pediatric pain management. Eur Rev Med Pharmacol Sci. 17(Suppl 1):112–126.
Corff KE, Seideman R, Venkataraman PS, Lutes L, Yates B. (1995). Facilitated tucking: A nonpharmacologic comfort measure for pain in preterm neonates. J Obstet Gynecol Neonatal Nurs.;24(2):143-7.
40
Cramton RE, Gruchala NE. (2012). Managing procedural pain in pediatric patients. Curr Opin Pediatr; 24:530–538. Doellman D. (2003). Pharmacological versus nonpharmacological techniques in reducing venipuncture psychological
trauma in pediatric patients. Journal of Infusion Nursing; 26:103–109. Evans S, Tsao JC, Zeltzer LK. (2008). Complementary and alternative medicine for acute procedural pain in children.
Altern Ther Health Med;14(5):52-6. Fein A, Zempsky WT, Cravero JP. (2012). Relief of pain and anxiety in pediatric patients in emergency medical
systems. Pediatrics; 130:e1391–e1405. Gerik SM (2005). Pain management in children: developmental considerations and mind-body therapies. Southern
Medical Journal;98(3):295-302, Goodenough JB, Addicoat L, & Champion GD (1997). Pain in 4–6 year old children receiving muscular injections: A
comparison of the faces pain scale with other self-report and behavioural measures. The Clinical Journal of Pain. 13,60–73.
Hagan JF, Coleman WL, Foy JM, Goldson E, Navarro A, Tanner JL, Tolmas HC, Armstrong FD, DeMaso DR, Longstaffe S, Gilbertson P, Cohen GJ, Smith K; Committee on Psychosocial Aspects of Child and Family Health. Task Force on Pain in Infants, Children, and Adolescents. (2001). The assessment and management of acute pain in infants, children, and adolescents. Pediatrics;108(3):793-7.
Harrison D, Stevens B, Bueno M, Yamada J, Adams-Webber T, Beyene J, Ohlsson A. (2010). Efficacy of sweet solutions for analgesia in infants between 1 and 12 months of age: A systematic review. Arch Dis Child;95(6):406-13.
Harrison D, Yamada J, Adams-Webber T, Ohlsson A, Beyene J, Stevens B. (2015). Sweet tasting solutions for reduction of needle-related procedural pain in children aged one to 16 years. Cochrane Database Syst Rev.5;(5):CD008408.
International Association for the Study of Pain. Subcommittee on taxonomy. (1979). Pain terms: A list with definitions and notes on usage. Pain;6:249–52.
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ (2008). Cancer statistics, 2008. CA A Cancer Journal for Clinicians; 58:71–96
Karakaya A, Gozen D. (2016). The effect of distraction on pain level felt by school-age children during venipuncture procedure-randomized controlled trial. Pain Manag Nurs; 17:47–53.
Karp, H. (2015). The Happiest Baby on the Block. Bantam Books, NY, NY. Kennedy RM, Luhmann J, Zempsky WT. (2008). Clinical implications of unmanaged needle-insertion pain and
distress in children. Pediatrics; 122(Suppl 3):S130–S133. Krauss BS, Calligaris L, Green SM, Barbi E. (2016). Current concepts in management of pain in children in the
emergency department. Lancet; 387:83–92. Lewindon P, Harkness L and Lewindon N (1998). Randomised controlled trial of sucrose by mouth for the relief of
infant crying after immunization. Arch Dis Child;78(5):453-456. Lonnqvist PA, Morton NS. (2005). Postoperative analgesia in infants and children. Br J Anaesth; 95:59–68. Mathew PJ and Mathew JL (2003). Assessment and management of pain in infants. Postgrad Med J;79:438-44. McGrath PJ. (2011). Science is not enough: the modern history of pediatric pain. Pain;152:2457–2459. Merritt C. (2014). Fear and loathing in the ER: Managing procedural pain and anxiety in the Pediatric Emergency
Department. RI Med J; 97:31–34. Mitchell A, Boss BJ. (2002). Adverse effects of pain on the nervous systems of newborns and young children: a
review of the literature. J Neurosci Nurs; 34:228–236. O’Rourke D (2004). The measurement of pain in infants, children, and adolescents: From policy to practice. Physical
Therapy. 84; 6:560–570. Owens M., Todt E. (1984) Pain in infancy: Neonatal reaction to a heel lance, Pain, 20 (1), 77–86. Pai AL, Kazak AE. (2006). Pediatric medical traumatic stress in pediatric oncology: Family system interventions.
Current Opinion in Pediatrics; 18:558–562. Phillips DM (2000). JCAHO pain management standards are unveiled. Joint Commission on Accreditation of
Healthcare Organizations JAMA.;284(4):428-9. Reece-Stremtan S & Gray L. (2016). ABM Clinical Protocol #23: Nonpharmacological management of procedure-
related pain in the breastfeeding infant, revised 2016. Breastfeed Med. 2016 Sep 13. [Epub ahead of print] Rivera, WB. (1991). Practical points in the management of postoperative pediatric pain. J Post Anesth Nurs;6:40 –
42. Ruest S & Anderson A (2016). Management of acute pediatric pain in the emergency department. Curr Opin Pediatr.
28:298-304. Sencer SF, Kelly KM. (2007). Complementary and alternative therapies in pediatric oncology. Pediatric Clinics of
North America; 54(6):1043–1060. Shah PS, Aliwalas LI, Shah V. (2006). Breastfeeding or breast milk for procedural pain in neonates. Cochrane
Database Syst Rev. 19;(3):CD004950. Shah PS, Herbozo C, Aliwalas LL, Shah VS. (2012). Breastfeeding or breast milk for procedural pain in neonates.
Cochrane Database Syst Rev. 12;12:CD004950. Sidhu J & Tickner N (2016). An audit of the management of acute pain in children. Arch Dis Child;101(9):e2.
41
Srouji R, Ratnapalan S, Schneeweiss S (2010). Pain in children: Assessment and nonpharmacological management. Int J Pediatr, pii 474838.
St-Laurent-Gagnon T, Bernard-Bonnin AC, & Villeneuve E. (1999). Pain evaluation in preschool children and their parents, Acta Paediatrica. 88;4:422–427.
Tracey I, Ploghaus A, Gati J, Clare S, Smith S, Menon RS, Matthews PM. (2002). Imaging attentional modulation of pain in the periaqueductal gray in humans. J Neurosci; 22:2748–2752.
Valet M, Sprenger T, Boecker H, Willoch F, Rummeny E, Conrad B, Erhard P, Tolle TR (2004). Distraction modulates connectivity of the cingulo-frontal cortex and the midbrain during pain: An fMRI analysis. Pain; 109:399–408.
Verghese ST, Hannallah RS. (2010). Acute pain management in children. J Pain Res; 3:105–123. Voepel-Lewis T (2011). The ongoing quandaries of behavioral pain assessment in children with neurocognitive
impairment. Dev Med & Child Neurol.53:101-107. Weisman SJ, Bernstein B, Schechter NL. (1998). Consequences of inadequate analgesia during painful procedures
in children. Arch Pediatr Adolesc Med; 152:147–149. Wente SJ. (2013). Nonpharmacologic pediatric pain management in emergency departments: A systematic review of
the literature. J Emerg Nurs;39:140–150. Wong C, Lau E, Palozzi L & Campbell, F (2012). Pain management in children: Part 1 — Pain assessment tools and
a brief review of nonpharmacological and pharmacological treatment options. Can Pharm J (Ott); 145(5): 222–225.
Yilmaz G, Caylan N, Oguz M, Karacan CD. (2014). Oral sucrose administration to reduce pain response during immunization in 16-19-month infants: A randomized, placebo-controlled trial. Eur J Pediatr.;173(11):1527-32.
Zernikow B, Meyerhoff U, Michel E, Wiesel T, Hasan C, Janssen G, Kuhn N, Kontny U, Fengler R, Görtitz I, Andler W. (2005). Pain in pediatric oncology--children's and parents' perspectives. Eur J Pain;9(4):395-406.
Appendix I Individualized Pain Management Programs (IPMP)
Jessie is a 10-year-old with Hodgkin’s lymphoma. She has had 2 recurrences and is on her third round of treatment. Her strategies of choice have changed a few times throughout the course of treatment. She now carries her IPMP with her, wherever she goes. Her school teacher helps with #5 and 6 on her IPMP, providing interventions at school when needed. Jessie can tell you what IPMP stands for and proudly tells new hospital staff or school personnel that she has and IPMP and what that means.
Jessie’s IPMP
Jessie’s Individualized Pain Management Program
Interventions Materials/Supplies
1. Bone marrow aspirates Conscious sedation N/A
2. Lumbar puncture Conscious sedation N/A 3. Venipuncture Distraction Buzzy, water toy, ABC book 4. Morning of BMT, LP Guided imagery Reclined position – go to
meadow at Grandma’s 5. Radiation – sore throat Tactile Cold compresses,
Mom/teacher rub back 6. Constipation Distraction Video game 7. General pain management Biofeedback Clinic appts 8. 9. 10. 11.

42
Appendix II Duane’s IPMP
Duane is a high school junior with a diagnosis of sickle cell anemia. Duane is well known to the staff of the hospital where he is treated and the hospice in his community as a result of his frequent hospitalizations and his relationship with hospice. Duane has been receiving services from hospice since early last year when his sickle cell pain became so severe he was in the hospital more often than out. An athlete at his school, Duane was suddenly faced with the inability to play sports that which he feels defines him. In addition to physical pain, the health care team believes that Duane has psychological layers of pain for which he requires intervention, as well.
lllllllllllll
-###-
Duane’s Individualized Pain Management s
Interventions Materials
Avascular necrosis – hip Tactile Heat, massage (Dad)
Avascular necrosis - hands Tactile Paraffin dip
Pain crisis – home mngmt Home meds Tylenol
“ Home meds Oxycontin
Pain crisis – hospital mngmt IV Fentanyl
“ Guided imagery Nurses
“ Self-hypnosis Palliative care director
On-going Writing Pain diary
On-going Cognitive behavioral therapy (CBT) Psychologist, self

43
BEING WITH: RECOGNIZING THE EXPERIENCE OF PARENTS
IN THE FACE OF THEIR CHILD’S PAIN
Rachel B. Levi, PhD Licensed Psychologist
Oakland, CA [email protected]
Being a Parent Becoming a parent is a life-altering experience. For many, the transition to and experience of parenting transforms a person’s identity, the structure of their daily life, and their priorities, and may come to shape how they experience the world and their relationships. Especially during the first year of life, parents rely on their support systems for practical, emotional, and social support, and rely upon their own internal resources to support them in caring for their infant who is fully dependent upon them for survival. While throughout typical development the level of care that children require will vary based upon the child’s constitution and lived experience, the normal trajectory is that children develop more independence and ability to manage their world. This internalized sense of security that allows a child to navigate the world around him/her is called attachment. Attachment is a core element of being a parent. Attachment theory was first presented by John Bowlby (1980) who noted that, similar to other mammals, an infant’s need to attach to caregivers/parents is innate. Attachment theory posits that children need a secure base or a secure attachment to the parents or caregivers in order to become independent and autonomous. Having a relationship with parents that is reliable, predictable, and secure provides children with a sense of safety and security that enables them to explore the world around them. The attachment between a parent and child begins before birth and is shaped throughout a child’s life. While attachment is dependent upon the temperaments of both parent and child, and how they come to respond and relate to each other, a parent’s ability to read, respond to, and appropriately attune to his or her child’s needs is critical in shaping the type of attachment that a child comes to form. A parent’s own attachment relationship with his or her parents impacts how he or she attaches to their child, how the person parents, and how he or she experiences being a parent (e.g., Siegel & Hartzell, 2003). Adults also derive a sense of security from some of the basic assumptions that we hold: assumptions about ourselves and about how the world works serve as a guide or internal compass and can often live in the background of our awareness (Janoff-Bulman 1992). The term “assumptive world” refers to the sense of reality that we hold which has been learned and then refined throughout one’s life (Beder, 2004; Parkes 1975). Many parents hold the hope(s) and assumption that their child will be well and healthy. Being a parent of a child who is ill
The diagnosis of a life-limiting condition and/or illness in a child immediately shifts the life of a parent into a “before” and “after”—after which “everything changes and we feel that nothing may ever feel the same again” (Shinoda Bolen, 1996, p. 23). The diagnosis of a child’s condition becomes a moment around which a parent’s existence becomes organized. Parents of seriously ill children live in the “After.”

44
This period of “after” is fluid and filled with beginnings, changes, growth, uncertainty, and loss. Although parents may present with hope and organize the narrative of their child’s illness and their experience with the illness around hope, anticipatory grief begins at the point of diagnosis. Parents grieve the “normal” life that they had with a “healthy” child. Life-limiting illness in a child is an assault to the natural order, to the way that life is “supposed” to unfold, and, to the assumptive world of most parents.
This assault is not something that is visible or can be seen. It can be conceptualized as the backdrop upon which everything that the parent experiences occurs. Another way to think about this profound shift is to think about décor on a wall in a child’s hospital room. Throughout the child’s admission, the parent may notice the design, and at times may even find himself or herself dwelling upon the design, while at other times the parent may not even notice the designs as attention is occupied. This décor may be so familiar and such a part of the landscape that hospital staff may not actively think about the décor or about the parents’ reaction to this décor, as there are so many other variables and needs to which to attend.
However, the wall décor is always there. It shapes the room, the design, and the structure of the space within which a family stays during a child’s admission, and within which the some of the experiences described later occur. It is not décor that the family has chosen, nor does the family have agency in determining the nature of the décor, and yet this décor is a part of the structure of the space that becomes their base during the admission.
The power of repeated psychological, existential, spiritual, and physical “assaults” to parents’ assumptive worlds is far more salient and influential than the wall décor in one’s (hospital) room. Yet, like the décor in the room, amidst a child’s serious illness a parent’s assumptive world and internal sense of security demand less attention and notice than the myriad of experiences and responsibilities endemic within the experience of parenting a child nearing the end of his or her life.
For months and sometimes years after a child’s diagnosis, parents typically endure a cascade of experiences which impact their own sense of safety and security in the world, as well as how they interact with their children, partner/spouse, and friends/family, and their personal and professional communities. These experiences may include: fluctuations in the child’s condition, medical crises, the need to make medical decisions often in the face of uncertainty and/or under conditions of threat to the child’s well-being, separation from family, trying to maintain a sense of ‘normalcy” for the child and family, and the aspects of their lives separate from the illness and medical world, and often, a child’s pain.
The Experience of Parents in the Face of their Child’s Pain
Pain is common in the lives of many children cared for by pediatric palliative care providers (e.g., Pritchard et al., 2008; Wolfe et al., 2000). Parenting a child with chronic pain is psychologically consuming and has widespread impacts upon the social, emotional, financial, interpersonal, and spiritual lives of parents, even when this pain occurs within the context of hope that the child may recover and be pain free (e.g., Jordan, Eccleston, & Osborn 2007; Palermo, 2000; Palermo & Eccleston, 2009).
Witnessing one’s child suffer violates the assumptive world of most parents, that children will be well and healthy. The “common” nature of pain amongst the children cared for by palliative care providers does not minimize its impact. In one study (Kreicbergs et al., 2005), 57% of parents whose children were treated for cancer had experienced unrelieved pain continued to be affected by this untreated pain 4-9 years following the child’s death. While caring for their ill child becomes a role around which parents organize their lives, a part of their identity, and can give them a sense of agency and meaning, parents describe the experience as isolating.

45
When a child is in pain, parents assume the role of advocate as they have typically been present during each step of the child’s illness and treatment, and often are involved in decision making, while at the same time serving as attachment figures and security for the child in distress. Literature on childhood pain documents relationships between the ways in which parents respond to a child’s pain and the child’s emotional experience and functioning (e.g., Jessop, Riessman, & Stein, 1988). Parents serve as the container of their child’s emotions and make efforts to comfort and nurture their child in the face of pain.
It is known that the experience of caring for one’s child with a complex health condition is associated with a wide range of emotional experiences, including but not limited to the following: helplessness, hope, a deeper sense of meaning/appreciation for life, frustration, stress, anxiety, depression, marital tension, guilt, and a sense of living between at least two worlds (“normal” life and the culture of medicine/childhood illness) (Ferrell, Rhiner, Shapiro, & Dierkes, 1994; Sourkes, 1995; Vrijmoet-Wiersma et al, 2008), and these experiences have typically occurred over a period of years.
Parents of children who are living with illness continue to focus on and promote their child’s “normal” development. Parents also remain focused upon how they can “be good parents.” Although there has been little research into this topic, making informed and unselfish decisions in the child’s best interest, providing for the child’s needs, staying with the child independent of the circumstances, trying to prevent suffering and protect health, and teaching the child to respect others and make good choices were cited as some characteristics of “being a good parent” to a child with incurable cancer (Feudtner et al., 2015; Hinds et al., 2009)
In the face of a child’s pain, there is little room to pause and to reflect—pain management and relief is the goal. Yet here we are able to do so, to consider this dynamic that for many families is recurrent—a child who is seriously ill and/or approaching end of life, a parent ushering whatever resources he or she has available to relieve the child’s suffering, while at the same time soothing and comforting the distressed child and advocating with medical professionals, all within the context of a “shattered” assumptive world.
Being With Parents
What does it mean to “be with” parents while a child is in pain?
Providers may be physically present to assess the child’s pain and/or administer medication. Physical presence offers one layer of support to parents.
Entering these situations with some awareness of the backdrop against which the pain is occurring can yield another layer of support. Although pain often ushers in a crisis and asking parents questions about the following is not appropriate, consideration of some of the following questions as you are with a parent may create some psychological space to acknowledge and consider the backdrop of the parent’s experience.
What is the meaning of this pain to this parent? Does he or she have a narrative about this pain?
What is this child’s history with pain throughout the illness?
What is the context within which this pain is occurring (i.e., disease progression, change in a social situation, etc.)?
What supports this parent (i.e., family/friends, prayer, time with other children, music, etc.)? How do parents support each other? In what ways might the parents work as a team?
How does this parent see his or her role in managing this pain episode?

46
What are the parent’s fears?
What may help this parent feel like a “good parent” to this child during this episode?
Consideration of any of these questions during interactions of acute and/or chronic pain requires providers to hold and to attend to the acuity while also holding awareness of the bigger context within which parents live. Navigating these very different spaces is at the core of a parent’s existence during his or her child’s illness and end of life. Being with this reality can contribute to a parent feeling held and supported, and may strengthen the internal sense of security from which the parent functions.
Parents who are bereaved identify the following as helpful to them their process of living after the death of their child and grieving and mourning: strong relationships with the medical team, good communication, support (emotional, spiritual, logistical, and decision making), and a sense that providers are attempting to understand their experience (Contro, Larson, Scofield, Sourkes, & Cohen, 2002; Lichtenthal et al., 2015; Melin-Johansson, Axelsson, Jonsson Grundberg, & Hallqvist, 2014). Each of these qualities and ways of being contribute to a parent’s sense of emotional security.
During times in which the ground below us is shaking, we look for security. Comprehensive attention to pain management is the focus of this issue. Attention to the experience of parents is a critical aspect of such pain management. While we are not able to do this work in the face of managing a child’s pain episode, one can stay present and listen to the layers of communication. Doing so lends an increased sense of control and may free up more psychic space for a parent to use their energy to communicate with the child, share time, create memories, and to engage in meaning making, all of which are goals and priorities articulated by parents at the end of their child’s life. Making meaning: focusing upon the role of caring for their children (ill and healthy) and preserving their roles as a parent helps parents cope with the end of their child’s life and beyond (Kars, Grypdonck, & van Delden, 2011).
References
Beder, J. (2004). Loss of the assumptive world – How we deal with death and loss. Omega, 50(4), 255-265. Bowlby, J. (1980). Attachment and loss: Sadness and depression (Vol. 3). New York: Basic Books. Contro, N., Larson, J., Scofield, S., Sourkes, B., & Cohen, H. (2002). Family perspectives on the quality of pediatric
palliative care. Arch Pediatr Adolesc Med, 156(1), 14-19. Ferrell, B. R., Rhiner, M., Shapiro, B., & Dierkes, M. (1994). The experience of pediatric cancer pain, Part I: Impact of
pain on the family. J Pediatr Nurs, Dec; 9(6):368-79. Feudtner, C., Walter, J. K., Faerber, J. A., Hill, D. L., Carroll, K. W., Mollen, C. J., Miller, V. A., Morrison, W. E.,
Munson, D., Kang, T. I., & Hinds, P. S. (2015). Good-parent beliefs of parents of seriously ill children. JAMA Pediatrics, 169(1), 39–47.
Hinds, P. S., Oakes, L. L., Hicks, J., Powell, B., Srivastava, D. K., Spunt, S. L., Harper, J., Baker, J.N., West, N.K., & Furman, W. L. (2009). “Trying to Be a Good Parent” as defined by interviews with parents who made Phase I, terminal care, and resuscitation decisions for their children. Journal of Clinical Oncology, 27(35), 5979–5985.
Janoff-Bulman, R. (1992). Shattered assumptions: Towards a new psychology of trauma. New York: Free Press. Jessop, D. J., Riessman, C. K., & Stein, R.E. (1988). Chronic childhood illness and maternal mental health. J Dev
Behav Pediatr., 9:147–156. Jordan, A. L., Eccleston, C., & Osborn, M. (2007). Being a parent of the adolescent with complex chronic pain: An
interpretative phenomenological analysis. Eur J Pain.11, 49–56. Kars, M. M., Grypdonck, M. H. F., & van Delden, J. J. M. (2011). Being a parent of a child with cancer throughout the
end-of-life course. Oncology Nursing Forum, 38, 260–271. Kreicbergs, U., Valdimarsdottir, U., Onelov, E., Bjork, O., Steineck, G., & Henter, J. I. (2005). Care-related distress: A
nationwide study of parents who lost their child to cancer. Journal of Clinical Oncology, 23, 9162-9171. Lichtenthal, W. G., Sweeney, C. R., Roberts, K. E., Corner, G. W., Donovan, L. A., Prigerson, H. G., & Wiener, L.
(Dec 2015). Bereavement follow-up after the death of a child as a standard of care in pediatric oncology. Pediatr Blood Cancer, Dec 62 (Suppl 5), S834-69.
47
Melin-Johansson, C., Axelsson, I., Jonsson Grundberg, M. & Hallqvist, F. (2014). When a child dies: Parents' experiences of palliative care—An integrative literature review. Journal of Pediatric Nursing, 29, 660–669
Palermo, T. M. (2000). Impact of recurrent and chronic pain on child and family daily functioning: a critical review of the literature. J Dev Behav Pediatr, 21:58–69.
Palermo, T. M., & Eccleston, C. (2009). Parents of children and adolescents with chronic pain. Pain, 146(1-2), 15–17. Parkes, C. M. (1975). Determinants of outcome following bereavement. Omega, 6, 303-323. Pritchard, M., Burghen, E., Srivastava, D. K., Okuma, J., Anderson, L., Powell, B., Furman, W. L., & Hinds, P. S.
(2008). Cancer-related symptoms most concerning to parents during the last week and last day of their child’s life. Pediatrics, 121, e1301-e1309.
Shinoda Bolen, J. (1996). Close to the bone: Life threatening illness and the search for meaning. New York: Touchstone, Simon & Schuster.
Siegel, D.J., & Hartzell, M. (2003). Parenting from the inside out: How a deeper self-understanding can help you raise children who thrive. New York: Penguin Putnam.
Sourkes, B. (1995). Armfuls of time: The psychological experience of the child with a life-threatening illness. Pittsburgh, Pa: University of Pittsburgh Press.
Vrijmoet-Wiersma, C. M., van Klink, J. M., Kolk, A. M., Koopman, H. M., Ball, L. M., Maarten Egeler, R. (2008). Assessment of parental psychological stress in pediatric cancer: A review. J Pediatr Psychol, 33 (7): 694- 706
Wolfe, J., Grier, H. E., Klar, N., Levin, S. B., Ellenbogen, J. M., Salem- Schatz, S., et al. (2000). Symptoms and suffering at the end of life in children with cancer. The New England Journal of Medicine, 342, 326–333.
-###-

48
RECIPROCAL RELATIONSHIPS: GIVING AND RECEIVING CARE WITH CHILDREN IN SPIRITUAL PAIN
L. Dean Allen MDiv, PhD
Spiritual Care Coordinator, Covenant Care Hospice Professor of Ethics and Philosophy, Northwest Florida State College
Fort Walton Beach, FL [email protected]
The calls have come at different times, but always they have come with a sense of deep urgency because children were experiencing spiritual pain. While serving as a Spiritual Care Coordinator for a hospice provider, I have been called to visit with a family whose young child was dying. In addition to the five-year-old patient, the family included three siblings under the age of twelve. While serving as a church pastor, I was called to visit a family whose teenage son had just died tragically and unexpectedly. The teenager’s family included a younger sister and many friends stung by his death. Also, while serving as a pastor, I was called to a family’s home because their great-grandmother, who lived with them, was dying. Her great-grandchildren, ages eight and five, were present and filled with questions. In each situation, I went as quickly as possible and offered as much care as possible to help the children—and other family members—experiencing spiritual pain.
How does one care for children experiencing spiritual pain? The response offered by professional and personal caregivers is determined, to a large degree, by the ways in which they understand children’s spirituality. If spirituality is seen primarily as an individual quest, then overcoming spiritual pain is largely a solitary endeavor. Further, if children are viewed only as little people who must mature before they develop spiritual understanding, then adults will see them as capable only of receiving care from others who know better than the children themselves. This article presents an alternative view of children’s spirituality by challenging both an individualistic understanding of spirituality and a view of children as recipients, but not givers, of care.
Toward an Understanding of Spirituality
A prevailing understanding of spirituality gives primary attention and consideration to the individual. Each person, so the thinking goes, must follow her or his path to spiritual development, and each path is different and unique. When describing religion and spirituality in the United States, Bellah et al. (1985) refer to “Sheilaism,” the spiritual practices and religious views developed by one person, Sheila Larson, who said, “I believe in God. I’m not a religious fanatic. I can’t remember the last time I went to church. My faith has carried me a long way. It’s Sheilaism. Just my own little voice…. It’s just try to love yourself and be gentle with yourself” (p. 221). Citing Sheila as an example, Bellah et al. described a trend toward individualistic spirituality. If Sheila is in spiritual pain, then her response to it will be a solitary endeavor.
While much is commendable about a view of spirituality as an individual’s quest, it also diminishes the important role of a community in one’s spiritual formation. And, when one is experiencing spiritual pain alone, she or he can be removed from helpful and sustaining resources of others. While not excluding the deeply personal and intimate nature of spirituality, an understanding of spirituality that includes its communal nature opens possibilities for helping people, perhaps especially children, who are experiencing spiritual pain.
Sheridan (2004), Eaude (2014), and Palmer (2003) consider the importance of connections when they define spirituality. Sheridan (2004) defines spirituality as “the search for meaning, purpose, and connection with self, others, the universe and ultimate reality, however one understands it, which may or

49
may not be expressed through religious forms or institutions” (p. 10, emphasis added). Issues of meaning and purpose in relation to large questions of life are key to one’s spirituality, but these questions may be engaged in connection with others. Eaude (2014) says that “one paradox of children’s spiritual development is that it involves an individual journey, but that this involves developing relatedness—to other people, to the wider world, and, for some people, to a Transcendent Other” (p. 242, emphasis added). Palmer (2003) says spirituality is “the eternal human yearning to be connected with something larger than our own egos” (p. 377).
If spirituality is the yearning or search for connection, meaning, and purpose, then spiritual pain occurs when one’s search for such connection, meaning, and purpose is hindered, challenged, or prevented. Spiritual pain may be episodic and temporary, or it may be longer-term and persistent. Spiritual pain may be caused by many things, but the illness and death of a loved one certainly is one of its major causes.
When we understand spirituality as having a communal component, we are more open to the resources, care, and support of others to assist those experiencing spiritual pain. For example, when I was called to the home of the dying great-grandmother, I was greeted by the entire family, which included the young children. All of the family members were experiencing spiritual and emotional pain, but they were together. They shared their tears and fears, and they supported one another in the midst of their pain. The children were not rushed into a separate room or taken to a neighbor’s house. Instead, they were present with all the family members, which was helpful to them both in that moment and long-term.
Toward an Understanding of Children’s Spirituality
For many years, a developmental understanding of human faith and spirituality has been predominant (Fowler 1981; Peck 1987, 1993). Following publication of Fowler’s Stages of Faith in 1981, the prevailing view of spirituality has focused on evolution and maturation as a person moves through the stages of spiritual development (Moore et al. 2015, p. 261). Fowler (1981) suggested that humans move through seven stages of spiritual development, and Peck (1987, 1993) described four stages. Most attention is given to adult spiritual development. Subsequent scholars have challenged or augmented Fowler’s theory by focusing on spiritual lives of children. Kelemen (2004), for example, suggests that children intuitively view the world as designed and orchestrated by a Higher Power or Being. Barrett and Richert (2003) offer a “preparedness hypothesis” in which they suggest children are able to reflect on supernatural concepts. Johnson and Boyatzis (2006) argue that children have spiritual understandings that are supported by interactions with family and social settings. Based on these scholars, Moore et al. (2015) suggest “that children may have much more developed spiritual lives than was once thought” (p. 261). Thus, rather than developing in a basically linear pattern of increasing abstraction, children may possess spiritual sensitivity in varying degrees throughout their lives.
Why does a more nuanced view of children’s spirituality matter? If adults view children primarily as little people who must move through stages of faith development before they are mature, then they often will see children only as recipients of care. If you think that a child has not developed spiritual awareness, you likely will attempt to shield the child from difficulty and pain, which diminishes or excludes the possibility of children offering care to others.
A hospice patient’s family chose not to tell her young son that his mother was terminally ill. The family told the child only that his mother was not feeling well. The family could not believe the child had the maturity to handle the information about his mother, and they wanted to shield the child from pain. By viewing him in this way, however, they cut off the possibility of the child relating to his mother as fully as possible

50
during her dying days. Further, the family did not allow the child to care for his mother as he might have done with full knowledge of her condition.
If one understands children as capable of spiritual understanding and sensitivity throughout their lives, then children may be both recipients of care and givers of care to others. I argue that children are, indeed, capable of both giving and receiving care. Thus, children and caregivers may enter a reciprocal relationship in which both parties are able to relate to each other, care for each other, and help each other bear spiritual pain.
Reciprocal Relationships between Children and Caregivers
When adult caregivers view spirituality as communal as well as personal, it can guide their actions as they relate to children in spiritual pain. By viewing spirituality as having an indispensable communal element, adult caregivers will focus on the importance of relationships. Researchers (Andrews & Marotta, 2005) have shown that grieving children give great attention to relationships. Children have primary attachments with surviving parents, siblings, grandparents, and other loved ones. When these adults recognize the communal nature of a child’s spiritual pain, they can give attention to the child’s words and actions about the deceased person. For example, many children want to talk about a dead loved one and have dreams about their loved ones. Caregivers should encourage children to talk about their deceased loved one because this is a key element of maintaining a relationship with the deceased. Many children also maintain relationships through continuing observance of rituals such as birthdays and Mother’s Day or Father’s Day, visiting a cemetery, drawing pictures or making gifts for the deceased person. These actions should be encouraged as avenues for expressing and attending to spiritual pain. Beyond family members and adult friends, children also can develop relationships with professional caregivers while in the midst of spiritual pain. Many professional caregivers such as social workers, clergy, psychologists, and physicians can develop relationships with children as they are in spiritual pain. Recognizing the communal aspect of spirituality, Eaude (2014) argues that adult caregivers can foster “hospitable space” that is open, inclusive, and reciprocal to nurture children’s spirituality (p. 236).
Children in spiritual pain often attach meaning to “linking objects” such as photographs or videos of the deceased, articles of clothing from the deceased, items of importance to the deceased, or gifts given by the deceased (Andrews & Marotta 2005). The objects help children maintain relationship with the deceased person, and adults who recognize the communal nature of spirituality and spiritual pain can affirm children in these activities. The surviving sibling of the deceased teenager wanted to talk about her brother, to share pictures of him, to keep his basketball jersey, and to listen to music he liked. These linking objects helped her maintain relationship with her brother following his death.
When adult caregivers see children as capable of possessing spiritual sensitivity throughout their lives, they can develop a reciprocal relationship in which children both receive care and give care when in the midst of spiritual pain. Noddings (2003) suggests that children need opportunities both to be cared for and also to care for others. Bugge et al. (2014) describe helpful ways in which children cared for surviving parents in a post-death family environment. Children in spiritual pain should be cared for by attentive, competent, and caring adults. Children should be allowed to express their spiritual pain to the degree they wish and in ways that are helpful for them. Children should be allowed to reflect on their situation by speaking, playing, drawing, acting, and dancing. Adults should give them attention and maintain relationship with them. Care, however, is not unidirectional. Children should be invited—comfortably and without coercion—to offer care to others while they are in the midst of spiritual pain.

51
In the case of the five-year-old hospice patient with three siblings in the home, the siblings were in the midst of anticipatory grief before their brother’s death. Their parents encouraged the siblings to relate to their sick brother, which they did. They talked with him, watched videos with him, and joined him as he played with toy trains. As his condition deteriorated, and he could not leave his bed, the siblings were encouraged to visit him in his room, to sit with him in bed, to draw pictures for him, and to pray with him. And the parents encouraged the patients to offer care to his siblings when able by talking with them, laughing with them, and receiving their gifts and gestures with gratitude. When I visited the family’s home, the siblings offered me glasses of water and sandwiches. Receiving their offerings was a key part of encouraging and facilitating their own caring for others. The parents, and the team of caregivers, developed a beautiful web of reciprocal relationships in which children in spiritual pain both received care and offered care to others.
Professional caregivers face many challenges when relating to children in spiritual pain. As a Spiritual Care Coordinator with a hospice provider, I have productivity expectations from my company and time constraints from serving in a large geographical area. It can be tempting to visit with children quickly; to assess their physical, psychosocial, and spiritual needs rapidly; and to offer care before moving on to other patients and families in need. This temptation is real, and the challenge it presents is difficult to overcome. As a professional caregiver, however, I know that it is helpful to remind myself that (1) children of various ages have spiritual awareness and sensitivity and (2) children can both receive and give care.
References
Andrews, CR, & Marotta, SA. 2005. Spirituality and Coping among Grieving Children: A Preliminary Study. Counseling and Values 50: 38-50.
Barrett, JL, & Richert, RA. 2003. Anthropomorphism or Preparedness? Exploring Children’s God Concepts. Review of Religious Research 44: 300-312.
Bellah, RN, Madsen, R, Sullivan, WM, Swidler, A, Tipton, S. 1985. Habits of the Heart: Individualism and Commitment in American Life. Berkeley: University of California Press.
Bugge, KE, Darbyshire, P, Rokholt, EG, Haugstvedt, KTS, Helseth, S. 2014. Young Children’s Grief: Parents’ Understanding and Coping. Death Studies 38: 36-43.
Eaude, T. 2014. Creating Hospitable Space to Nurture Children’s Spirituality – Possibilities and Dilemmas Associated with Power. International Journal of Children’s Spirituality 19(3-4): 236-248.
Fowler, J. 1981. Stages of Faith: The Psychology of Human Development and the Quest for Meaning. New York: Harper Collins.
Johnson, CN, & Boyatzis, CJ. 2006. Cognitive-Cultural Foundations of Spiritual Development. The Handbook of Spiritual Development in Childhood and Adolescent (pp. 21-34). Eds. Roehlkepartain, E, et al. Thousand Oaks, CA: SAGE.
Kelemen, D. 2004. Are Children Intuitive Theists? Reasoning about Purpose and Design in Nature. Psychological Science 15: 295-301.
Moore, K, Talwar, V, Moxley-Haegert, L. 2015. Definitional Ceremonies: Narrative Practices for Psychologists to Inform Interdisciplinary Teams’ Understanding of Children’s Spirituality in Pediatric Settings. Journal of Health Psychology 20(3): 259-272.
Noddings, N. 2003. Caring – A Feminine Approach to Ethics and Moral Education. Berkeley: University of California Press.
Palmer, PJ. 2003. Teaching with Heart and Soul: Reflections on Spirituality in Teacher Education. Journal of Teacher Education 54(5): 376-383.
Peck, MS. 1987. The Different Drum: Community Making and Peace. New York: Simon & Schuster. Peck, MS. 1993. Further along the Road Less Traveled: The Unending Journey toward Spiritual Growth. New York:
Simon & Schuster. Sheridan, MJ. 2004. Predicting the Use of Spiritually-derived Interventions in Social Work Practice: A Survey of
Practitioners. Journal of Religion and Spirituality in Social Work 32(4): 5-25. -###-
52
ITEMS OF INTEREST
In each issue of our ChiPPS e-journal, we offer additional items of interest.
1. NHPCO Palliative Care Online Resources: NHPCO has a variety of pediatric hospice and palliative care resources available at www.nhpco.org/pediatrics. Also, more palliative care resources are available at www.nhpco.org/palliativecare, including:
Community –Based Palliative Care Legal and Regulatory Resources Webinars and Courses Plus more for NHPCO members
Palliative Care Programs and Professionals Join NHPCO today as a palliative care (non-hospice) member:
Individual Palliative Care Membership Palliative Care Group Application - Save by registering your entire team
2. Pediatric Hospice and Palliative Care Resources: CaringInfo, a program of the National Hospice and Palliative Care Organization, provides
free resources to help people make decisions about end-of-life care and services before a crisis. www.caringinfo.org
When Your Child is in Pain Talking With Your Child About His or Her Illness Talking to Your Child's Doctor: When Your Child Has a Serious Illness When a Child Dies: A Guide for Family and Friends Helping Children Cope with the Loss of a Loved One
Center to Advance Palliative Care: Did you know there are new tools to support your
program? CAPC is pleased to announce the launch of three new resources for pediatric programs:
Pediatric Palliative Care Survey in the CAPC National Registry: Submit your program data now to generate individualized performance reports on program structure and operations, as well as comparisons to other pediatric palliative care programs. CAPC membership is not required.
The Pediatric Palliative Care Field Guide: A catalog of field-wide program development tools, support sources for field research, and an updated value statement to help programs make the case for pediatric palliative care resources.
The CAPC Pediatric Palliative Care Toolkit: A collection of new, practical tools and technical assistance for pediatric palliative care programs developed by leaders and experts across the country. Available to members now in CAPC Central.
3. Pediatric Hospice and Palliative Care Training:
Hospice and Palliative Care Association Of New York State: Competency Programs for
Hospices, Tuesday, December 6, 2016. A successful competency program lowers risks and increases outcomes by ensuring employees, subcontractors, students, and volunteers are qualified to provide patient services. Everyone must have the necessary knowledge, education, skills, and experience to perform their jobs and meet accrediting and Medicare standards. Register HERE.
53
Hospice and Palliative Care Association Of New York State: Marketing in a World that is Consolidating: Why Data is Your Best Tool! This webinar will review the metrics upon which ACOs will be scored and determine the data providers may have to present to an ACO (or other provider) to receive referrals. Learn how a hospice can make the case for palliative care services for chronic, but not terminal, patients and how this may cause a savings. Join us for a review of the regulatory issues when partnering with an ACO and what that might entail for home health, private duty, or hospice providers, including the potential fraud/abuse issues and potential defenses. Register HERE.
Hospice and Palliative Care Association Of New York State: HPCANYS 2-Day
Interdisciplinary Pediatric Palliative Care Training Unique to New York. The interdisciplinary team approach for both the child and family is what sets an excellent pediatric palliative care program apart. This training will focus on how disciplines overlap and support each other to provide optimum care for children at end of life. HPCANYS’ Pediatric Palliative Care training recognizes that all team members are an important part of the Plan of Care and each team member has something valuable to contribute. Register HERE.
Boston’s Children’s Hospital Pediatric Pain and Opioid Education. This program provides training in acute and chronic pain management for pediatric patients, with an emphasis on safe and effective opioid use. Topics covered include neurobiology of pain; addiction, abuse and safe opioid prescription practices; licensing, the law and opioid prescribing; treatment of chronic pain; and safe storage and disposal of medications. Register HERE.
November is National Hospice & Palliative Care Month. Don't miss this chance to save! Order any live or recorded webinar and receive 10% off. Enter the code CELEBRATE at checkout. View available webinars HERE.
NHPCO’s 32nd Management and Leadership Conference Preconference Dates: April 29 -30, 2017 Main Conference: May 1-3, 2017 Washington Hilton, Washington DC. Look for information HERE.
4. Journal / News Articles AAP Conference Preview: Tips for breaking bad news to patients, parents. Read more
here.
Student, faculty member study pediatric palliative care in Uganda. Little is known about end-of-life (EOL) care for adolescents and young adults (AYA) with cancer.1,2 How often do AYA Medicaid patients use hospice versus intensive measures? Read more here.
5. Subjects and Contributors for Future Issues of This E-Journal. For upcoming 2017 E-Journal issues, we plan to address issues related to: Symptom Management. If you know of good topics and/or contributors (including yourself) for these and/or other future issues of this e-journal, please do not be shy! Step right up and contact Christy Torkildson at [email protected]; or Chuck Corr at [email protected]. We will work with you!
6. Reader's Corner. Our Reader's Corner columns provide brief summaries and bibliographical information about journal articles and other publications that are important and likely to be of widespread interest to individuals who are involved or interested in pediatric hospice and palliative care, but that may not be known to readers. We welcome suggestions for publications to include in our Reader’s Corner and/or summaries and comments on such articles. Please send suggestions to Christy Torkildson at [email protected].
-###-