-
Melgar | Mendoza | Montenegro | Moshtaghi |
Pascual | Patricio |Santos, P. UERM 2015B Page 1 of 15
6.3 CHILDHOOD CANCER Dr. Castro February 27, 2014
Powerpoint
Recording
Nelsons Textbook of Pediatrics
Important/Emphasized points
Topics not discussed but were included in the chapters in
Nelsons
2014 trans
Actually, cancer in children is really rare. Hematologic
malignancies are more common in children. Leukemia and lymphoma are
the most common malignancies in children.
WORLDWIDE INCIDENCE OF
CHILDHOOD CANCER
Figure 1. Here, we can see the incidence of childhood cancer in
the
Philippines, it is around 11.5/100,000 population of
children.
LEADING CAUSES OF
MORBIDITY AND MORTALITY 1. Communicable diseases
2. Cardiovascular diseases
3. Cancer
STATISTICAL DATA ON CANCER
AGE-SPECIFIC CANCER INCIDENCE RATE
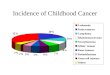
Figure 2. Note bimodal peak in the age specific cancer incidence
rate
During the first 4 years of life and during adolescence,
cancer in children differs very much from the adults:
o 1.) Type
Adults: Epithelial Cancer (Colon Cancer, Breast
Cancer, Cervical Cancer)
Children: Embryonal (Neuroblastoma, Primitive
Neuroectodermal)
o 2.) Age incidence
Adults: Increasing incidence with increasing age
Children: Bimodal distribution
INCIDENCE OF CHILDHOOD CANCER BY AGE
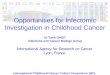
Figure 3. Again, note bimodal peak in the age-specific
cancer
incidence rate
Note nadir during childhood and rise again during the early
adolescence because of the lymphomas and sarcomas
First year of life: Neuroblastoma, Wilms Tumor,
Retinoblastoma
and the Primitive Neuroectodermal Tumor predominate
1-4 y/o: peak incidence; secondary to ALL
Adolescence: Osteosarcoma, Ewing Sarcoma, Soft tissue
Sarcoma or the Rhabdomyosarcoma, Hodgkin disease and the
germ cell tumors (testicular and ovarian cancer)
5-YEAR RELATIVE SURVIVAL RATE OF
ALL CANCERS IN CHILDREN
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 2 of 15
RELATIVE FREQUENCIES OF
CHILDHOOD CANCER
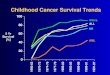
Figure 5. From Laudico, et. al in 1998
Leukemias are the most common (almost 50%), followed by
CNS tumors, retinoblastomas and lymphoma
Others consist of rhabdomyosarcoma, germ cell tumors and
bone
tumors
HEMATOLOGIC MALIGNANCIES Leukemias
o Acute lymphoblastic leukemia: 77%
o Acute myeloblastic leukemia: 11%
o Chronic myelogenous leukemia: 2-3%
o Juvenille myelomonocytic leukemia: 1-2%;
childhood-adult CML
Lymphomas
o Hodgkins lymphoma
o Non hodgkins lymphoma
Figure 6. Cells that are involved in leukemogenesis
Any problem in the maturational process causes maturational
arrest, thereby resulting to acute myelogenous leukemia
Ex: arrests of the development lead to proliferation of blasts
=
genesis of acute lymphoblastic leukemia
THE FOLLOWING WERE NOT DISCUSSED BUT WERE IN THE
2014A TRANS. ONCOGENESIS: GENES INVOLVED
So how does cancer develop? This is explained by oncogenesis.
Among all of
us, there is a potential for the development cancer.
Fortunately, our immune
system is competent to arrest the development of these oncogenic
materials.
Proto-oncogenes: normal genes, which secrete proteins for the
survival
of the cells; mutation = ONCOGENE
Oncogenes
Tumor suppressor genes p53 For immunocompetent individuals,
the tumor suppressor genes (specifically p53) is very strong. It
prevents
the expression of the oncogene and therefore the development of
cancer.
But in patients who would have problems with the suppressor
genes, as
well as the proto-oncogenes, cancer expression may be
expected.
.
Figure 7. Oncogene transformation
For example, this is a proto-oncogene which encodes for normal
cellular
proteins involved in growth signaling pathways. They can be
mutated
by chemicals, radiation or viruses and therefore, once mutated
they
become an oncogene with a potential for cancerinogenesis.
Table 1. Some of the oncogene activators of pediatric tumors
ONCOGENE ACTIVATOR OF PEDIATRIC TUMORS
MECHANISM CHROM GENES PROTEIN
FUNCTION
TUMOR
Chromosomal
translocation
t(9;22) BCR-
ABL
Chimeric
tyrosine
kinase
CML, ALL
t(1;19) E2A-
PBX1
Chimeric
transcription
factor
Pre-B ALL
t(14;18) CMYC Transcription
factor
Burkitts
lymphoma
t(15;17) APL-
RAR
Chimeric
transcription
factor
APL
Gene
amplification
Amplicon NMYC Transcription
factor
Neuroblastoma
EGFR growth factor
kinase,
tyrosine
kinase
Glioblastoma
Point mutation 1p NRAS GTPase AML
10q RET Tyrosine
kinase
MEN2
BCR-ABL (Break Cluster Region-Abelson) gene is generated by
the
translocation 9.22 is also called the Philadelphia
chromosome
o Hallmark of CML
o In some ALL, the translocation 9:22 is also seen; generates
the
BCR-ABL gene
Most commonly seen are BCR-ABL and the NMYC and APL-RAR
GUARDIAN OF THE GENOME
Figure 8. Mechanism by which genomic integrity is maintained
despite
chromosomal aberrations
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 3 of 15
The p53 protein repairs the damage from chemical carcinogens,
UV
radiation or anything
Can also cause cell cycle arrest to prevent multiplication of
abnormal
cells and therefore maintain the integrity of the cell
In some patients, p53 may be destroyed by radiation, and
viruses;
destruction may cause carcinogenesis.
WARNING SIGNS IN CHILDREN
Table 2. Acronym for general s/sx in children with CA-
CHILDREN
C Continued, unexplained
weight loss
Usually unexplained weight loss of 10-
15% in the last 6 mos despite good
appetite
H Headaches with vomiting
in the morning
Suggestive of CNS tumors
I Increased swelling or
persistent pain in bones or
joints
Leukemias and bone tumors
L Lump or mass in
abdomen, neck or
elsewhere
Lymphadenopathies and abdominal
masses
D Development of a whitish
spot in the pupil of the eye
Retinoblastoma
R Recurrent fevers not
caused by infections
Increasing WBC count with
lymphocytic predominance
E Excessive bruising or
bleeding
Leukemias and other tumors
infiltrating the bone marrow
N Noticeable paleness or
prolonged tiredness
Anemia, thrombocytopenia and
leukopenia
MULTIDISCIPLINARY CARE
Figure 9. Multi disciplinary care of children with cancer
Treatment of chidren would entail chemotherapy primarily and
then
surgical and radiotherapy plus molecular biology. Those on the
outside
ring are more of supportive care. Includes: analgesia, use of
cytokines,
transfusion, antibiotics, antiemetics and of course nutritional
support
PRIMARY MODALITIES OF THERAPY
Figure 10. Also illustrating multi disciplinary care of children
with cancer
COMMONLY USED ANTI-CANCER DRUGS
Figure 11. Some of the commonly used drugs with their
mechanism
We will not really be dealing on the specific drugs and there
are still a
lot being investigated in cooperative groups
THE LEUKEMIAS CLASSIFICATION
Incidence rates:
o Acute Lymphoblastic Leukemia: 77%
o Acute myelogenous Leukemia: 11%
o Chronic Myelogenous Leukemia: 2-3%
o Juvenile Myelomonocytic Leukemia: 1-2% Acute: characterized by
conal expansion of immature hematopoietic
precursors
Chronic: characterized by clonal expansion of mature marrow
elements
Congenital: diagnosed within the first 4 weeks of life
ACUTE LYMPHOBLASTIC LEUKEMIA (ALL) Peak incidence at 2-3 years
old
Boys > girls: 1.1:1 in ratio
Chromosomal abnormalities
o Down syndrome Trisomy 21 confers good prognosis
o Bloom syndrome
o Ataxia telangiectasia
o Fanconi anemia Identical twins: 70% risk for 2nd twin
SIGNS and SYMPTOMS
Feverbecause of neutropenia; there are not enough functional
neutrophils to conquer the infection
Bleedingbecause of thrombocytopenia
Bone painif the bone marrow is involved Particularly in the
lower extremities
Less often joint pain
Reticulo-endothelial organ system manifestations:
Lymphadenopathy
Hepatomegaly
Splenomegaly General Systemic Effect
Anorexia, fatigue, malaise, and irritability often are present,
as is an intermittent, low-grade fever.
Patients often have a history of an upper respiratory tract
infection in the preceding 1-2 mo.
Less commonly, symptoms may be of several months duration, may
be localized predominantly to the bones or
joints, and can include joint swelling. Bone pain is severe
and can wake the patient at night. As the disease progresses,
signs and symptoms of bone
marrow failure become more obvious with the occurrence of
pallor, fatigue, exercise intolerance, bruising, or epistaxis,
as
well as fever, which may be caused by infection or the
disease.
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 4 of 15
Organ infiltration can cause lymphadenopathy,
hepatosplenomegaly, testicular enlargement, or central
nervous system (CNS) involvement (cranial neuropathies
headache, seizures). Respiratory distress may be due to
severe anemia or mediastinal node comparison of the
airways.
LABORATORY STUDIES
CBC1st laboratory test to be done, including platelet
count.There may be varying anemias, thrombocytopenias,
increase WBCs or very low WBCs, and lymphocytic
predominance. Peripheral Blood Smear may show presence of
blasts.
Bone Marrow Aspiration
May also show blasts if the CBC is abnormal/does not show
any conferring findings. ALL is diagnosed by a bone marrow
evaluation that
demonstrates >25% of the bone marrow cells as a
homogeneous population of lymphoblasts. Staging of ALL is based
partly on a cerebrospinal fluid (CSF)
examination. If lymphoblasts are found and the CSF
leukocyte count is elevated, overt CNS or meningeal
leukemia is present. This finding reflects a worse stage and
indicates the need for additional CNS and systemic
therapies.
Chest X-ray
Blood Chemistriesin preparation for chemotherapy
Lumbar Tapto monitor CNS involvement
CLASSIFICATION of ALL
Morphologic Classification: French American British
(FAB) Very common, you look at the morphology of blast cells
o L1: blasts with very scanty cytoplasm
o L2: moderate amount of cytoplasm and nucleoli resembling
the blasts of the myeloid series
o L3: Burkitt leukemia; cytoplasmic vacuolization
The most important distinguishing morphologic
feature is the French American British L3 subtype
which is evidence of mature B-cell leukemia. The L3
type also known as Burkitt leukemia is one one of the
most rapidly growing cancers in humans and requires
a different therapeutic approach.
Aside from looking at the cells under the microscope, you
can
also type the cells present using flow
cytometry/immunophenotype so you have the T and the B cell
ALL.
WHO Classification: errors in the diagnosis are encountered
in the morphologic classification, so the WHO incorporated
chromosomal abnormalities, as well as immunotypic
abnormalities, in classifying leukemias, giving rise to:
B lymphoblastic leukemia/lymphoma
o Not Otherwise Specified (NOS)
o With recurrent genetic abnormalities
T lymphoblastic leukemia/lymphoma
RECURRENT GENETIC ABNORMALITIES
Used in determining the prognosis of leukemias
These are the genetic abnormalities found in children that
cause
leukemias:
t(9;22) [Philadelphia chromosome: presence indicates a poor
prognosis] (q34;q11.2); BCR-ABL-1
t(v;11q23); MLL rearranged
t(12;21) (p13;q22) TEL-AML1 (better prognosis; most common
in ALL) (ETV6-RUNX1)
With Hyperdiploidy
With Hypodiploidy
t(5;14) (q31;q34) IL3-IGH
t(1;19) (q23;p13.3) TCF3-PBX1
PROGNOSTIC FACTORS IN CHILDHOOD ALL (Table 3)
Factor Favorable
Prognosis
Intermediate
Prognosis
Unfavorable
Prognosis
Age (years) 1-9 10
50 or DNA index
> 1.16
Trisomies 4, 10,
17 t(12;21)/ETV6-
CBFA2
Diploid
t(1;19)/TCF3-
PRX1
t(9;22)/BCL-ABL-1
t(4;11)
CNS status CNS1 CNS2
Traumatic
spinal tap
with blasts
CNS3
Minimal
Residual
Disease (end of
induction)
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 5 of 15
Consolidation For maximal cell kill
Delayed intensification
MaintenanceDone monthly for three years. After, the
abnormal cells are totally eradicated giving cure to the
leukemia.
CNS prophylaxis/chemotherapy This is direct
intrathecal chemotherapy. Do a lumbar tap and inject
the drugs. Supportive care Through blood transfusion and
antibiotic
therapy.
Bone marrow transplant For patients who fail at the first
chemo
remission, do another cycle but if it fails again, they are
candidates for BMT already.
COMMONLY USED DRUGS IN ALL
Vincristine
Prednisone
Doxorubicin
L-asparaginase
6-mercaptopurine
Methotrexate
ACUTE MYELOGENOUS LEUKEMIA May also present like ALL so we must
differentiate the two.
Most common recurrent abnormality is the TEL-AML.
Pancytopenia WITH organomegaly: ALL
Pancytopenia WITHOUT organomegaly: most likely
AML
Age incidence is constant except for a peak in the neonatal
period and a slight increase during adolescence.
Secondary AML: MDS and use of alkylating agents
Treatment-related AML. These are the patients who have
received chemotherapy for another tumor, and then after 6-
10 years, will develop AML.
o Cyclophosphamide
o Ifosfamide
o Etoposide
AML FAB CLASSIFICATION
The most common classification of the subtypes of AML is the
French American British (FAB) system. Although this system is
based on morphologic criteria alone, current practice also
requires
the use of flow cytometry to identify cell surface antigens and
use
of chromosomal and molecular genetic techniques for
additional
diagnostic precision and also to aid the choice of therapy.
Table 5. FAB System
M0 Acute UNDIFFERENTIATED leukemia
M1 AML WITHOUT maturation
M2 AML WITH maturation
M3 Acute PROMYELOCYTIC leukemia (APL)can be cured
by Vitamin A (retinoic acid). This is usually seen in
adolescent,
associated with increased bleeding tendencies. Other
classifications will require chemotherapy and bone marrow
transplantation.
M4 Acute MYELOMONOCYTIC leukemia
M5 Acute MONOCYTIC leukemic
present with very huge liver and spleen, and CNS
infiltration
M6 Erythroleukemia
diGuglielmo syndrome or
leukemia of the red cell precursor
M7 Megakaryocytic leukemia
leukemia of the platelet precursor
The World Health Organization (WHO) has proposed a new
classification system that incorporates morphology,
chromosome
abnormalities, and specific gene mutations. This system
provides
significant biologic and prognostic information.
AML WHO CLASSIFICATION
AML with recurrent genetic abnormalities
AML with myelodysplasia-related changes
Therapy-related myeloid neoplasms
AML, NOS
Pure erythroid leukemia
Erythroleukemia, erythroid/ myeloid
Myeloid sarcoma
Myeloid proliferation related to DS
Blastiplasmacytoiddendritic cell neoplasm
CLINICAL MANIFESTATIONS
Marrow failure
Anemia, thrombocytopenia and neutropenia; with bleeding,
infection and pallor
Subcutaneous nodules ("blueberry muffin" lesions)
Gingival hyperplasia (M4, M5)
DIC (M3) especially indicative of acute promyelocytic
leukemia
Chloromas or granulocytic sarcoma (M2) t(8;12)
translocation The characteristic feature of AML is >30% of
bone marrow cells
on BMA or biopsy constitute a fairly homogenous population
of
blast cells, with features similar to those that characterize
early
differentiation states of the myeloid-monocyte-megakaryocyte
series of blood cells.
The production of symptoms and signs of AML, as in ALL, is due
to replacement of bone marrow by malignant cells and due to
secondary bone marrow failure. Patients with AML can present
with any or all of the findings associated with marrow failure
in
ALL. In addition, patients with AML present with signs and
symptoms
that are uncommon in ALL, including subcutaneous nodules or
blueberry muffin lesions (especially in infants), infiltration
of
the gingiva (especially in M4 and M5 subtypes), signs and
laboratory findings of disseminated intravascular
coagulation
(especially indicative of acute promyelocytic leukemia), and
discrete masses, known as chloromas or granulocytic
sarcomas.
These masses can occur in the absence of apparent bone
marrow
involvement and typically are associated with the M2
subcategory
of AML with a t(8;21) translocation. Chloromas also may be seen
in the orbit and epidural space
TREATMENT
Chemotherapy
Matched-sibling bone marrow or stem cell transplant
For those who go into complete remission
Matched-unrelated donor (MUD) stem cell transplant Has
significant risk of graft vs host disease.
M3: all-trans retinoic acid Acute promyelocytic leukemia
has gene rearrangement involving retinoic acid receptor
Supportive care
Transfusion and antibiotics AML is harder to treat. ALL has
better prognosis.
Aggressive multiagent chemotherapy is successful in inducing
remission in about 85-90% of patients.
Targeting therapy to genetic markers may be beneficial.
Matched-sibling bone marrow or stem cell transplantation
after
remission has been shown to achieve long-term disease-free
survival in 60- 70% of patients.
Continued chemotherapy for patients who do not have a
matched
sibling donor is generally less effective than marrow
transplantation but nevertheless is curative in about 45-50%
of
patients.
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 6 of 15
DIFFERENCE BETWEEN ALL AND AML
MORPHOLOGY
Figure 12. The coalescing cytoplasmic granules in M3 are called
Auer
rods; Consider AML.
For ALL vs AML differentiation. Usually the lymphoblast is
mononuclear with a very scanty cytoplasm. Myeloblasts, on the
other
hand, have more cytoplasm with distinct nucleoli.
CYTOCHEMISTRY
Another method of differentiating ALL and AML done by
staining bone marrow samples.
ALL
o (+) periodic acid schiff (PAS)
AML
o (+) myeloperoxidase (MPO)
o (+) sudan black
o (+) specific and non-specific esterase The characteristic
feature of AML is that >20% of bone marrow
cells on bone marrow aspiration or biopsy touch preparations
constitute a fairly homogeneous population of blast cells,
with
features similar to those that characterize early
differentiation
states of the myeloid-monocyte-megakaryocyte series of blood
cells.
IMMUNOPHENOTYPE (FLOW CYTOMETRY)
For ALL and AML differentiation. This identifies the clusters
of
antigens present on cells.
ALL
o B cell: CD 19, CD 20, 21, 22, 23, 24
o Pre B: CD 10 (Common Acute Lymphocytic
Leukemia Antigen (CALLA))
o T cell: CD 3, CD 5, CD 7
o mixed lineage, biphenotypic
AML
o CD 13, CD 33
5-YEAR SURVIVAL RATE
Five years after the diagnosis, the patient is still alive and
free of
the symptoms of the disease.
ALL
o 85% survival rate
AML
o 50-60% survival rate
CHRONIC MYELOGENOUS LEUKEMIA 3% of all childhood leukemias
Cytogenetic hallmark the Ph chromosome t(9:22)
Figure 13. Philadelphia chromosome: translocation between
chromosome 9 and 22
PHILADELPHIA CHROMOSOME
t(9;22)
Bcr-abl gene attachment
Secretes p210 protein
o A tyrosine kinase protein
o Makes the cell resistant to apoptosis, which results to
increased WBC count
Figure 14. Philadelphia chromosome
Philadelphia Chromosome
The disease is characterized clinically by an initial chronic
phase
in which the malignant clone produces an elevated leukocyte
count with a predominance of mature forms but with increased
numbers of immature granulocytes.
The spleen is often greatly enlarged, resulting in pain in the
left
upper quadrant of the abdomen. In addition to leukocytosis,
blood counts can reveal mild anemia and thrombocytosis.
The presenting symptoms of CML are nonspecific and can
include fever, fatigue, weight loss, and anorexia.
Splenomegaly
also may be present. The diagnosis is suggested by a high
white
blood count with myeloid cells at all stages of differentiation
in
the peripheral blood and bone marrow and is confirmed by
cytogenetic and molecular studies that demonstrate the
presence
of the characteristic Philadelphia chromosome and the
BCR-ABL
gene rearrangement.
SIGNS AND SYMPTOMS (CHRONIC PHASE)
Clinically stable for several years
5-10,000 WBC count is normal but patient present with 50,000
without any symptoms or infection
Upon diagnosis, the patient is usually in the chronic phase.
Patient is asymptomatic and will only be seen on routine CBC
or PE
Non-specific complaints: fever, night sweats, bone pain,
abdominal pain
Symptoms resulting from hyperviscosity, headaches,
strokes, retinal hemorrhages, papilledema, priapism
Hepatomegaly
Splenomegaly
Pallor
CML PHASES Table 6. Phases of CML and corresponding findings
Chronic Accelerated Blastic
Median
Duration
5-6 years 6-9 months 3-6
months
WBC >20,000 Thrombocytopenia
Blasts 0% >20% >30%
Basophils Increased >20%
Platelets Normal/increased Increased/decreased decreased
When patients develop into blastic phase, AML/ALL can
develop but usually AML so treatment is now directed towards
treating AML
CHRONIC
70% are diagnosed in this phase
Patients are usually asymptomatic
Stable for several years
Will present with non-specific complaints: fever, night
sweats,
bone pain, abdominal pain (due to splenomagaly)
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 7 of 15
ACCELERATED
After 10 years of being in the stable phase, if the patient did
not
receive a tyrosine kinase inhibitors (TKI) or did not respond
to
TKI, patients may move to the accelerated phase
Increasing blood and bone marrow leukemic blasts (20%)
and cytopenias
Rising basophil count
Refractoriness to therapy
Fever, night sweats, weight loss
Patients may still go back to chronic phase and eventually
become cured
10%, however, proceed to blastic phase
BLASTIC/BLASTIC CRISIS
Blasts >20% in blood or bone marrow
May become:
o Myeloid blast crisis: 80%
o Lymphoid blast crisis: 20%
Treated as an acute leukemia depending on type of cell
Poor prognosis
LABORATORY TESTS
CBC: leukocytosis and basophilia
Leukocyte Alkaline Phosphatase score: Low (usually 0)
To differentiate from infection
Infection has high WBC and high LAP score
BMA: granulocytic hyperplasia (numerous white cell
precursors)
Karyotype: Philadelphia chromosome t(9:22)
FISH: identification of bcr-abl gene
o Request for this if Philadelphia chromosome is
negative
Identification of p210
TREATMENT
Tyrosine kinase inhibitors (TKI)
o 1st generation: most common is Imatinib (Glivec)
100 mg tablet is usually Php1,500
Required dosage is 400-600 mg/day everyday =
Php 6,000/day
2nd generation: Dasatinib, Nilotinib
3rd generation: Bosutinib
Cytoreductive chemotherapy
o Symptomatic to decrease WBC count and prevent
hyperviscosity (in the form of hydroxyurea)
o Php 30/capsule
Interferons (IV)
Bone Marrow Transplant
Hematopoietic Stem Cell Transplant Imatinib mesylate (Gleevec),
an agent designed specifically to
inhibit the BCR-ABL tyrosine kinase, experience in children
suggests it can be used safely with results comparable to
those
seen in adults. While waiting for a response with imatinib,
disabling or
threatening signs and symptoms of CML can be controlled
during
the chronic phase with hydroxyurea, which gradually returns
the
leukocyte count to normal. Prolonged morphologic and cytogenetic
responses are expected,
but the opportunity for cure is enhanced by HLA-matched
family
donor allogeneic stem cell transplant, with up to 80% of
children
achieving a cure.
JUVENILE MYELOMONOCYTIC LEUKEMIA (JMML) Previously known as
Juvenile Chronic Myelocytic Leukemia
(JCML)
Also known as infantile monosomy syndrome
Usually presents in children < 2 years old
Rare JMML is a clonal proliferation of hematopoietic stem cells.
JMML is rare, constituting 1,000/uL
Bone marrow blasts < 20% Analysis of the peripheral blood
often shows an elevated
leukocyte count with increased monocytes, thrombocytopenia,
and anemia with the presence of erythroblasts. The bone marrow
shows a myelodysplastic pattern, with blasts
accounting for 10,000
Clonal abnormalities (Monosomy 7)
GM-CSF hypersensitivity of myeloid progenitors in vitro
LYMPHOMAS
HODGKIN LYMPHOMA Progressive enlargement of the lymph nodes
Unicentric in origin
Predictable pattern of spread by extension to contiguous
nodes
Usual LNs involved are cervical, axillary, epitrochlear,
inguinal,
and abdominal. Hodgkin lymphoma differs from Non-Hodgkin
wherein in Hodgkin lymphoma, the nodal spread is usually
towards contiguous/adjacent nodes, whereas in Non-
Hodgkin lymphoma, the nodal spread has no pattern.
ETIOLOGY AND EPIDEMIOLOGY
Cause is unknown
Bimodal age: 15-35 years old and >50 years old
Sex ratio in children: M:F = 3:1
Increased incidence among consanguineous family
members and among siblings with Hodgkin Lymphoma
Immunologic disorders: SLE, Rheumatoid arthritis, Ataxia
telangiectasia, Swiss-type agammaglobulinemia
High association with EBV
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 8 of 15
REED-STERNBERG CELL
Hallmark of classical Hodgkin lymphomahowever, not
all Hodgkin lymphomas will be positive for RS-cells
Owls eye appearance
Arise from germinal center B cells
Large cell in a reactive background of normal
lymphocytes, plasma cells, and eosinophils
Figure 14. Reed Sternberg cell
WHO/REAL CLASSIFICATION
Lymphocyte predominant, nodular (with or without
diffuse areas)
Classical Hodgkin Lymphoma
Lymphocyte-rich Classical HL
Nodular Sclerosis Classical HL
Mixed Cellularity Classical HL
Lymphocyte Depletion Classical HL
PRESENTING SIGNS AND SYMPTOMS IN CHILDREN (Table 7)
Presenting symptoms Percentage
Lymphadenopathy 90%
Mediastinal adenopathy
- Adolescents and young adults
- Children 39C, weight loss of
>10% of the total body weight over 3 months, and
drenching
night sweats. Less common and not considered of prognostic
significance are
symptoms of pruritus, lethargy, anorexia, or pain that
worsens
after ingestion of alcohol. Patients also exhibit immune system
abnormalities that often
persist during and after therapy.
DIAGNOSTIC INVESTIGATIONS & STAGING
Surgical
Excisional lymph node biopsy
Bilateral bone marrow biopsies/aspiration
Imaging studies (immediate)
CT Scan of neck, chest, abdomen, and pelvis (scan of
all the lymph node chains)
FDG-PET
Technetium 99 bone scintography
Laboratory studies
CBC
Blood chemistries for renal and hepatic functions (in
preparation for chemotherapy)
ESR (for prognostication)
Ferritin (for prognostication)
DIFFERENTIAL DIAGNOSES
TB (most common DDx due to mediastinal adenopathy)
Toxoplasmosis (also due to mediastinal adenopathy)
Non-Hodgkin Lymphoma
Metastatic cancer (due to generalized lymphadenopathy)
ANN ARBOR STAGING SYSTEM FOR
HODGKINS LYMPHOMA (Table 8)
I One LN involvement
II 2/more LNs but on the same side of the diaphragm
III 2/more LNs on both sides of the diaphragm
IV Involvement outside the LNs: bone marrow, liver,
extranodal sites
A Absence of B symptoms
B Presence of B symptoms
X Bulky disease
S Splenic involvement
E Extranodal
Stage I localized
Stage II and III (+) lymph node involvement
Stage IV metastatic disease
POOR PROGNOSTIC FACTORS
Advanced stages of disease (IIB, IIIB, IV)
Presence of B symptoms
Presence of bulky disease (large lymph nodes measuring
>10
cm or presence of mediastinal mass occupying >1/3 of the
chest
cavity)
Extranodal extension (spleen, ovaries, etc.)
Male sex
Elevated ESR
WBC 11.5 or higher
Hgb < 11 g/dL
TREATMENT
Combined chemotherapy
Low-dose involved field radiation (LD-IFRT) (in children
>6 years of age)
PROGNOSIS
Treated with curative intent
Overall survival rate:
> 90% with early stage
> 70% with advanced stage
10-20% with advanced stage may relapse
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 9 of 15
NON-HODGKIN LYMPHOMA Malignant clonal proliferation of
lymphocytes of T-, B-, or
indeterminate cell origin
Lymph nodes, Peyers patches, spleen
Bone marrow involvement in children
Rare: Bone and primary CNS
The bone marrow is more commonly involved compared to
Hodgkin lymphoma. If Hodgkin lymphoma presents with bone
marrow involvement, treatment already involves protocol for
leukemia.
INCIDENCE & EPIDEMIOLOGY
60% of all lymphomas in children and adolescents < 20
years old
Isolated cases of familial non-hodgkin lymphoma occur
M : F = 2.5 : 1 (slight male preponderance)
Peaks at 15-29 years of age
RISK FACTORS
Genetic: Immunologic defects (Agammaglobulinemia,
Ataxia telangiectasia, WAS, Severe combined
immunodeficiency)
Post-transplant immunosuppression
Drugs: Diphenylhydantoin
Radiation
Viral: EBV, HIV
CLASSIFICATION OF CHILDHOOD
NON-HODGKIN LYMPHOMA
Diffuse Large B cell Lymphoma (DLBCL)
Burkitt Lymphoma (B cell)
Lymphoblastic (usually T cell)
Anaplastic Large Cell Lymphoma (ALCL)
The clinical manifestations of childhood and adolescent NHL
depend primarily on pathologic subtype and primary and
secondary sites of involvement.
Approximately 70% of patients with NHL present with advanced
disease, at stage II or IV, including extranodal disease
with
gastrointestinal, bone marrow, and central nervous system
(CNS)
involvement.
BL commonly manifests as abdominal (sporadic type) or head
and neck (endemic type) disease with involvement of the bone
marrow or CNS.
LL commonly manifests as an intrathoracic or mediastinal
supradiaphragmatic mass and also has a predilection for
spreading to the bone marrow and CNS.
DLBCL commonly manifests as either an abdominal or
mediastinal (PMB subtype) primary and, rarely, dissemination
to
the bone marrow or CNS.
ALCL manifests either as a primary cutaneous manifestation
(10%) or as systemic disease (fever, weight loss) with
dissemination to liver, spleen, lung, mediastinum, or skin;
spread
to the bone marrow or CNS is rare.
MORPHOLOGIC & IMMUNOLOGIC FEATURES (Table 9)
MORPH DLBCL BURKITT LYMPHO-
BLASTIC
ALCL
CELL SIZE Large Intermediate Small
Intermediate Small Large
NUCLEAR
CHROMAT
IN
Clumped,
vesicular Coarse Fine, blastic
Clumped,
vesicular
NUCLEOLI Variable Variable Absent Variable
CYTOPLAS
M
Moderate
Abundant
Moderate
Scanty with
prominent
vacuoles
Scanty Moderate
Abundant
NODAL
PATTERN Diffuse
Diffuse,
starry-sky
pattern
Diffuse, starry-
sky pattern
Sinusoidal or
Diffuse
IMMUNOP
HENOTYPE
CD20+,
CD22+
CD20+,
CD22+
CD2 (80%),
CD19 (20%)
T cell, null
cell, CD30+,
ALK+
GENETIC FEATURES
Nice to know according to Dra.
Table 10. Genetic features of NHL
DLBCL Burkitt Lymphoblastic ALCL
t(8;14)(q24;q3
2), 12 gain, 21
gain, 15 loss,
3q27
rearrangeme
nts, 6q
deletion, 7q
gain, 11q
gain
t(8;14)(q24;q32),
t(8;22)(q24;q11),
t(2;8)(q11;q24),
1q duplication,
13q
abnormality, 6q
deletion, 7p
abnormality,
11q
abnormality
T cell receptor
arrangements TCL-1
t(7;14)(q35;q32),
t(14;14)(11;32), TCL-
2 t(11;13)(p13;p11),
TCL-3
t(10;14)(q24,q11),
TAL-1
t(1;14)(q32;q11)
t(2;5)(p23;
q25), ALK
translocati
on with
chromoso
me 1, 2, 3,
17
Figure 15. Starry sky pattern.
Some lymphoma cells die out and leave spaces, resulting to the
appearance of
stars within a sky.
DIAGNOSIS
CBC (to rule out metastatic disease to the bone marrow)
Serum electrolytes, uric acid, LDH, creatinine, calcium,
phosphorus
Liver function tests
CXR and chest CT if abnormal
Abdominal and pelvic ultrasound and/or CT
Gallium scan and/or bone scan
Bilateral BMA and biopsy (for staging)
CSF cytology (for staging)
FAB STAGING SYSTEM FOR
CHILDHOOD DBCL, BL, BLL
Group A
Completely Resected Stage I (Murphy)
Completely Resected Abdominal Stage II (Murphy)
Group B
All patients not eligible for Group A or Group C
Group C
Any CNS involvement and/or bone marrow involvement
(>25% blasts)
TREATMENT & PROGNOSIS
Proliferation of lymphoblasts are rapid with doubling
time as short as 24 hours
Some mediastinal masses may grow very large and cause
superior vena cava syndrome
Multi-agent systemic chemotherapy
Intrathecal chemotherapy (for those with CNS involvement)
Prognosis depends on appropriateness of protocol
PROGNOSTIC FACTORS
FAVORABLE:
Localized (Stages I and II)
Low LDH (
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 10 of 15
UNFAVORABLE:
High LDH (>500 or twice the upper normal level)
Combined bone marrow or central nervous system B-
NHL
Poor response to cyclophosphamide, vincristine,
prednisone (COP) reduction therapy in B-NHL
Primary mediastinal B cell lymphoma as primary B-
NHL
Visceral ALCL (Mediastinal, hepatic/splenic, or skin
involvement)
Minimal disease in bone marrow at diagnosis
SOLID TUMORS I. Neuroblastoma
II. Wilms Tumor
III. Retinoblastoma
IV. Tumors of the brain and spinal cord
V. Hepatoblastoma
VI. Rhabdomyosarcoma
VII. Ewing's sarcoma
VIII. Osteosarcoma
IX. Germ cell tumor
X. Histiocytosis
NEUROBLASTOMA Originates from the PRIMORDIAL NEURAL CREST
CELLS that give rise to the adrenal medulla (in the
abdomen) and sympathetic ganglia (beside the spinal cord).
You have risk of tumor from the pineal gland down to the
adrenal medulla.
MOST COMMON OF THE EXTRACRANIAL SOLID
TUMORS IN CHILDREN (8-10% OF ALL
CHILDHOOD CANCER)
MOST COMMON CANCER DIAGNOSED IN
INFANCY
2 years old: median age at diagnosis
90% of cases are diagnosed before the age of 5
Boys > girls
GENETIC: SOMATIC DELETION of CHROMOSOME
BAND 1P36, which is a frequent site in neuroblastoma
cells.
CLINICAL PRESENTATION
Adrenal mass - USUAL PRESENTATION or any MASS
ALONG THE SYMPATHETIC NEURAL CHAIN
65% - Abdomen
Unilateral palpable neck mass (lymphadenopathy)
Raccoon eyes: orbital hemorrhage
Bone pain, limping, back pain
Opsomyoclonus ataxia syndromerepetitive uncontrolled
movement of the eye (dancing eyes and dancing feet: primary
tumor is in the chest or abdomen w/o any in the brain)
ABDOMINAL MASS CROSSES THE MIDLINE
Internet: In children, most cases are associated with
neuroblastoma and most of the others are suspected to be
associated with a low-grade neuroblastoma that spontaneously
regressed before detection. In adults, most cases are
associated
with breast carcinoma or small-cell lung carcinoma. It is one
of
the few paraneoplastic (meaning 'indirectly caused by
cancer')
syndromes that occur in both children and adults, although
the
mechanism of immune dysfunction underlying the adult
syndrome is probably quite different.
May resemble other small round cell tumors, such as
rhabdomyosarcoma, Ewing sarcoma, and non-Hodgkin
lymphoma.
On plain radiograph or CT, the mass contains hemorrhage and
calcification (in Wilms, no calcification).
RECOMMENDED CRITERIA FOR DIAGNOSIS
ESTABLISHED IF:
o Unequivocal pathologic diagnosis (biopsy) is made
from tumor tissue by light microscopy (with or
without, immunohistology, EM) and/or increased
urine or serum cathecholamines or metabolites
OR
o Bone marrow aspirate or Trephine biopsy contains
unequivocal tumor cells (syncythia or
immunologically positive clumps of cells) and
increased urine or serum catecholamines
Cathecholamine metabolites:
o Homovanillic acid (HVA)
o Vanillylmandelic acid (VMA)
Figure 16. Homer Wright Rosettes - neuroblastoma cells
INTERNATIONAL NEUROBLASTOMA
STAGING SYSTEM (Table 11)
STAGE 1 Tumor confined to the organ of origin
STAGE 2
A
B
Tumor extend beyond the organ of origin but
does not cross midline
Without ipsilateral LN involvement
With ipsilateral LN involvement
STAGE 3 Tumors extend beyond the midline with or
without LN bilateral involvement
STAGE 4 Disseminated to distant sites
STAGE 4S
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 11 of 15
What is important here? The Shimada Histology and the N-Myc.
N-Myc is an oncogene for neuroblastoma. Poorer prognosis if
you
have more N-Myc.
THERAPY
LOW RISK:
o Surgery to remove the entire mass for Stage 1 and
Stage 2
o Observation for Stage 4s
INTERMEDIATE:
o Surgery
o Chemotherapy
o Radiation For incomplete response to chemotherapy
Children with stage III and infants younger than 1 y/o with
stage
IV and favorable characteristics= excellent prognosis
Diagnostics should be done for classification of Shimada and
MYCN amplification so that those with unfavorable
characteristics can have more aggressive treatment and those
with favorable characteristics can have less toxic therapy.
HIGH RISK:
o Chemotherapy Induction then high dose
o Bone Marrow Transplant Autologous bone marrow transplantation
or stem cell
WILMS TUMOR A complex mixed embryonal neoplasm composed of
three
elements: blastema, epithelia, stroma
MOST COMMON PRIMARY MALIGNANT RENAL
TUMOR OF CHILDHOOD, a.ka. nephroblastoma
Most are SOLITARY lesions
Multifocal:
o 7% involve in both kidneys
o 12% within a single kidney
>85% can cured by current therapies
Table 13. CONGENITAL ANOMALIES
ASSOCIATED WITH WILMS TUMOR (WT)
Cryptorchidism 43.6
Sporadic hemihypertophy 25.1
Hypospadias 20.0
Bechwith Weidermann: hemihypertrophy,
macroglossia, visceromegaly
10.7
Wilms tumor, aniridia, GU malformation, MR
(a.k.a. WAGR syndrome)
7.5/1000
Denys-Drash Syndrome: male
pseudohermaphrodism, early onset renal failure
4.0
RISK FACTORS
Environmental vs. genetic
WT appears to result from the loss of function of certain
suppressor genes as opposed to the activation of
oncogenes
GENETIC: autosomal dominant
o WT 1 (band 11p13): WILMS TUMOR SUPPRESSOR
GENE -obliterated or absent
o WT 2 (band 11p15): WILMS TUMOR GENE - present
that promotes the development of WT
o FWT 3 (17q) and FWT2 (19q): FAMILIAL LOCUS Usually
sporadic
Familial cases: decreased age at diagnosis and increased
frequency of bilateral disease, absent congenital anomalies
SIGNS AND SYMPTOMS
Table 14. INITIAL SIGNS AND SYMPTOMS OF WILMS TUMOR
SIGNS AND SYMTOMS FREQ. %
Palpable mass in the abdomen 60
Hypertension 25
Hematuria 15
Obstipation 4
Weight loss 4
UTI 3
Diarrhea (watery) 3
Previous Trauma 3 Others: nausea and vomiting, abdominal pain,
inguinal
hernia, cardiac insufficiencies, acute surgical abdomen,
pleural effusion, polycythemia, hydrocephalus
8
MASS THAT DOES NOT CROSS THE MIDLINE
STAGING FOR RENAL TUMORS (Table 15)
STAGE I Completely resected tumor limited to kidney with
intact capsule
STAGE II Completely resected tumor
Penetration of renal capsule
STAGE III Residual tumor present after surgery
STAGE IV Presence of Hematogenous Metastasis (lung, liver,
bone, brain)
STAGE V BOTH KIDNEYS
TREATMENT
Figure 17. TREATMENT -depends on the stage and histology.
All must undergo BIOPSY and SURGERY, and MULTI-AGENT
CHEMOTHERAPY. No RT for STAGE 1.
Bilateral WT: unilateral nephrectomy and contralateral
partial
nephrectomy or bilateral partial nephrectomy
IN COMPARISON (Table 16)
NEUROBLASTOMA VS WILMS TUMOR
Neuroblastoma Wilms tumor
Arise in the celiac axis: (adrenal
gland paravertebral sympathetic
ganglia)
EXTENDS ACROSS the midline
contains often CALFICATIONS
and hemorrhage
Intrarenal
DOES NOT CROSS midline
NO CALCIFICATION
Other renal tumors in Nelsons: congenital mesoblastic
nephroma, nephroblastomatosis, multicystic nephroblastoma,
renal cell carcinoma.
RETINOBLASTOMA MOST COMMON EXTRACRANIAL SOLID TUMOR
IN CHILDREN
Most commonly diagnosed in INFANTS
2/3 cases before 2 years and 95% before 5 years
Clinical forms:
o BILATERAL (40%): characterized by germline
mutations in RB1 gene
o INHERITED from Affected survivor (25%)
o NEW GERMLINE MUTATION (75%)
o UNILATERAL (60%)
Classification:
o Laterality: Unilateral, or Bilateral
o Focality: Unifocal or Multifocal
o Genetics: Hereditary or non-hereditary
o Family History: Familial or Sporadic
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 12 of 15
Genetics:
o AUTOSOMAL DOMINANT (85-90%)
o Majority of Children acquire new mutation (15-25%)
Risks of RB
o Risk of RB in offspring of RB survivors:
Bilateral disease - 45%
Unilateral disease- 2%
o Risk of RB in siblings
Bilateral - 45%
Unilateral - 30%
CLINICAL PRESENTATION
AGE at presentation correlated with LATERALITY
Bilateral:
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 13 of 15
Headache + nausea/vomiting +
papilledema:midline/infratentorial
Torticollis: cerebellar tonsil herniation
UMN (clonus, hyperreflexia): brainstem
Focal disorders such as motor weaknesses, sensory changes,
speech disorders, reflex abnormalities: supratentorial
Infants with hand preference: supratentorial
Parinaud syndrome (upward gaze paresis, pupillary dilatation
reactive to accommodation but not to light, nystagmus to
convergence, eyelid retraction): pineal region
DIAGNOSTIC EVALUATION
CT scan (Cranial)
MRI: for posterior fossa tumors; gold standard
MRA
Magnetic Resonance Spectroscopy
PET
CSF Analysis
Bone Marrow Aspiration
Bone scan
TREATMENT
Surgery
Radiotherapy
Chemotherapy
There are discussions on certain tumors in Nelsons, such as on
astrocytoma, oligodendroglioma, mixed gliomas, ependymal,
choroid plexus, embryonal, pineal parenchymal, neuronal,
craniopharyngioma, meningeal, brainstem and germ cell. Read
on
them further if you prefer but Doctora told us that she will
be
asking questions mainly from her lecture.
HEPATOBLASTOMA Occurs primarily in young children, 80% diagnosed
before
3 years of age
Increased risk: VLBW infants, familial adenomatous polyposis,
Beckwith-Wiedemann syndrome
Presents as an upper abdominal mass or as generalized
abdominal enlargement
90% with elevated alpha feto protein
TREATMENT
Only those in whom complete resection of mass can be
achieved have a reasonable chance for cure
Possible in 40-50% of children
Chemotherapy plays an ancillary role in eradicating
subclinical metastasis in completely resected disease
CHEMO + RT in unresectable diseases
Liver transplant
5-YEAR SURVIVAL RATE
Stage I/II: 90%
Stage III: 60%
Stage IV: 20%
RHABDOMYOSARCOMA 3RD most common extra-cranial tumor
(neuroblastoma (#1)
and Wilms tumor(#2) ) Most common pediatric soft tissue
sarcoma
Two age peaks: 2-6 years and 15-19 years
Arise from the same embryonic mesenchyme as striated
skeletal muscles
Anatomic sites:
o Head and Neck 40%
o GUT 29%
o Extremities 14%
o Trunk 12%
o Others 5% Associated with neurofibromatosis and maternal
breast cancer in
the Li Fraumeni syndrome
HISTOLOGIC SUBTYPES (Table 19)
Pathologic Subtypes Usual Site of Origin Usual Age (years)
Distribution
Embryonal (ERMS):
60% of cases,
intermediate
prognosis
Head & Neck, Orbit,
GUT
3-12
Solid Botryoid
(grape-like
projection)
Bladder, Vagina,
Nasopharynx, Bile
Ducts
0-8
Spindle Cell Paratesticular 2-12
Alveolar (ARMS):
poorest prognosis
Extremities, Trunk,
Perineum
6-21
RMS, NOS Extremities, Trunk 6-21
On light microscopy, it belongs to small round blue cell
tumors
including Non-Hodgkin lymphoma, neuroblastoma and Ewing
sarcoma
CLINICAL MANIFESTATIONS
Mass that may or may not be painful
Metastatic sites (20% at diagnosis): lung, bone marrow,
lymph nodes, bones
DIAGNOSTIC EVALUATION
History and PE: measurement and lymph node
involvement
Blood Chemistry
Primary Tumor Imaging
Metastatic Work-up High index of suspicion because its
presentation is similar with
other conditions that involves masses/tumors
IMAGING WORK-UP
CT Scan or MRI of Primary: to evaluate the extent of loco-
regional disease
Chest CT: to evaluate presence of metastasis
Bone Scan: to evaluate for distant metastasis
STAGING
Pre-treatment clinical stage
Post-treatment clinical stage
PROGNOSIS
Curable in majority of children receiving optimal therapy
(>70% survival after diagnosis)
Extent of disease is the most important prognostic factor
Alveolar histology has the worst prognosis
TREATMENT
Local Control: radiotherapy
Systemic Control: chemotherapy
Complete resection = best prognosis; however, not all are
completely resectable
Based on the primary tumor location and disease stage
(clinical
group)
o Group I: complete local excision then chemotherapy
o Group II (microscopic residual tumor): surgery local
radiation and systemic multiagent chemotherapy
o Group III (gross residual tumor): systemic multiagent
chemotherapy irradiation surgery (if possible)
o Group IV (metastatic): systemic chemotherapy and
irradiation
Other nonrhabdomyosarcoma soft tissue sarcomas are
relatively
rare in children. Most common, in order of descending
prevalence, are synovial sarcoma, fibrosarcoma, malignant
fibrous histiocytoma and neurogenic tumors.
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 14 of 15
EWING SARCOMA 80% are younger than 20 years at diagnosis
Round blue cell tumor Undifferentiated sarcoma of the bone
Table 20. Round Blue Cell Tumors
MARKER EWING
SARCOMA
NEURO
BLASTOMA
RHABDOMYO
SARCOMA
LYMPH
OMA
Neuron Specific
Enolase
+/- +* +/- -
S-100 +/- +* +/- -
NFTP +/- + +/- -
Desmin +/- - +* -
Actin +/- - +* -
Vimentin +/- - +* +
Cytokeratin +/- - +/- -
LCA - - - +*
HNK-1 +/- + + -
32-
Microglobulin
+ - +/- +
CD99 +* - + +/-
CLINICAL FEATURES
Local Pain-96%
Local Swelling- 61%
Fever- 21%
Pathologic Fractures- 16%
DIAGNOSTIC EVALUATION
History and PE
X-Ray of affected bone (with ONION SKINNING)
Blood Chemistry
Metastatic Evaluation:
Lung
Bone
Bone Marrow
Figure 18. Onion Skinning seen in Ewing Sarcoma
TREATMENT
Surgery
Radiation
Chemotherapy
PROGNOSIS
5 year disease-free survival: 60-70%
Metastatic Disease: 20-30%
OSTEOSARCOMA Bone growth: development is correlated with linear
bone
growth
Genetic factors: Rb gene and p53
Environmental Factors: previously irradiated bones
Pathologic Hallmark: production of osteoid Children younger than
15 years old, taller than their peers
(adolescent growth spurt: association with rapid bone growth
and
malignant transformation)
Associated with hereditary retinoblastoma, Li-Fraumeni
syndrome, Rothmund-Thomson syndrome, Paget disease, Ewing
sarcoma, enchondromatosis, multiply hereditary exostoses,
fibrous dysplasia
CLASSIFICATION
Classic (usually seen)
Osteoblastic
Chondroblastic
Fibroblastic
Telanglectatic
Small Cell
Periosteal
Parosteal
SYMPTOMS
Local pain- 90%
Local swelling- 50%
Decreased range of motion- 45%
Pathologic fracture-8%
Joint effusion
SKELETAL DISTRIBUTION
Lower long bones -74.5%
Upper long bones-11.2%
Pelvic region-3.6%
Face or skull-3.2%
Mandible-1.9%
Chest region-1.8%
Vertebral column-1.2%
Lower short bones-1.1%
Upper short bones -0.3%
DIAGNOSTIC EVALUATION
Involve blood chemistries, imaging techniques, and work-up
for
metastasis
Radiographic Findings:
Soft Tissue extension-75%
Radiating calcification/sunburst- 60%
Osteosclerotic lesions- 45%
Lytic lesions-30%
Mixed lesions -25%
Figure 19. Radiographs with typical osteosarcoma sunburst
PROGNOSIS
DFS, non-metastatic, treated with adjuvant chemotherapy:
60-80%
Metastatic Disease: 2 year survival 10-30%
30-40% of patients will have metastasis at diagnosis
TREATMENT
Surgery
Surgical biopsy
Amputation (if extensive)
Limb-salvaging surgery
Chemotherapy
Neoadjuvant (pre-op)
Adjuvant (post-op)
-
6.3 | Childhood Cancer
Candice de Belen. Nika Gil. Alexandra de Rossi.
Lucien Torres-Gomez. F-PJ. Clariz Pempengco. Piocholo Pascual.
UERM 2015B Page 15 of 15
GERM CELL TUMOR From primordial germ cells of the human
embryo
Occurs at gonadal and extragonadal sites
Bimodal age distribution:
o Peak < 3 years old: Extragonadal and testicular
tumors
o Peak adolescence: Gonadal tumors
Table 21. Germ Cell Tumors
SITES FREQUENCY
Sacrococcygeal 42%
Ovary 24%
Testis 9%
Mediastinum 7%
Pineal region 6%
Retroperitoneum 4%
Other sites 8%
For infants, the most common site is sacrococcygeal. For
adolescents, ovary and the testis. They may occur at gonadal
and
extragonadal sites.
HISTOLOGIC VARIANTS
o Germinoma
Dysgerminoma (Ovary)
Seminoma (Testis)
o Immature teratoma
o Embryonal carcinoma
o Yolk sac tumor (endodermal sinus tumor)
o Choriocarcinoma
CLINICAL PRESENTATION
Depends on Primary Site:
Ovarian: abdominal pain (may mimic acute abdomen);
abdominal mass
Testicular: irregular, non-tender masses
Extragonadal: depends on tumor location
Constipation and urinary retention for sacrococcygeal
tumors
Respiratory distress for mediastinal tumors
Pineal Gland: neurologic signs and symptoms
LABORATORY WORK-UP (Table 22)
TUMOR MARKER Germ Cell Tumor HALF-LIFE
AFP Yolk sac tumor
Embryonal carcinoma
5-7 days
B-HCG Choriocarcinoma
Embryonal Carcinoma
Germinomas
24-36 hours
LDH Dysgerminomas
PLAP
AFP and B-HCG are usually elevated in germ cell tumors. AFP
is also elevated in hepatoblastoma. LDH and placental
alkaline
phosphatase can also be elevated. But the primary tumor
markers of germ cell tumors are AFP and B-HCG.
TREATMENT
Surgery
Radiotherapy
Chemotherapy
LANGERHANS CELL HISTIOCYTOSIS Most cases occur between 1-15
years of age
Presumptive Diagnosis: Langerhans Cells
Definitive Diagnosis: CD1A( Birbeck Granules), Langerin Also
known as histiocytosis X and involves the Class I histiocytes
Figure 20. Birbeck granules (tennis racket-like) on
electro-microscope.
ORGANS INVOLVED
Bone: pelvis, femur, ribs, skull (punched out lesions of
skull
is most common), orbit
Skin (lesions)
Lymph Nodes
Bone Marrow
Lungs
Hypothalamic-Pituitary Axis
Spleen
Liver
CLINICAL FEATURES
Eosinophilic granuloma (isolated skin lesion)
Hand-Schuller-Christian disease (skull)
ABT-Letterer Siwe disease (skull)
CANCER TREATMENT
Surgery
Chemotherapy
Radiotherapy
Immunotherapy (vaccines and monoclonal antibodies)
PREVENTION OF CHILDHOOD CANCER
IMMUNIZATION
o Hepatitis B vaccine: hepatocellular carcinoma
o HPV vaccine: cervical cancer
Adopt a HEALTY LIFESTYLE to reduce risk of cancer in
adults
o Tobacco
o Alcohol
o High-Fat Diet
o Obesity
o Exercise
Looking back, it's easy to see when a mistake has been made.
To
regret a choice that seemed like a decent idea at the time.
But if we use our best judgment and listen to our hearts, we're
more
likely to see that we chose wisely, and avoid the deepest most
painful
regret of them all
the regret that comes from something amazing pass you by.
Greys Anatomy s10 e13