Embed Size (px)
Citation preview
![Page 1: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/1.jpg)
Short Stature and Tall StatureShort Stature and Tall Stature
Dr.HAKIMI,SpAKDr.HAKIMI,SpAKDr.HAKIMI,SpAKDr.HAKIMI,SpAK
Dr.MELDADr.MELDA DELIANA,SpAKDELIANA,SpAK
Dr.SISKADr.SISKA MAYASARI MAYASARI LUBIS,SpALUBIS,SpA
Dept. of child healthDept. of child health
Medical School, University of North SumatraMedical School, University of North Sumatra
![Page 2: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/2.jpg)
GrowthGrowth
•• Normal growthNormal growth
–– InfantInfant
–– ChildhoodChildhood–– ChildhoodChildhood
–– PubertyPuberty
•• Growth : change in size & maturationGrowth : change in size & maturation
•• Stature : sizeStature : size
![Page 3: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/3.jpg)
Cm/tahun
Growth Velocity Curve
InfantInfant ChildhoodChildhood PubertyPuberty
GHSex steroid
![Page 4: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/4.jpg)
Growth rate by ageGrowth rate by age
11--6 mo6 mo : 18 : 18 -- 22 cm/yr22 cm/yr
66--12 mo12 mo : 14 : 14 –– 18 cm/yr18 cm/yr66--12 mo12 mo : 14 : 14 –– 18 cm/yr18 cm/yr
1 yr1 yr : 11 cm/yr: 11 cm/yr
2 yr2 yr : 8 cm/yr: 8 cm/yr
3 yr3 yr : 7 cm/yr: 7 cm/yr
4 4 –– pubertypuberty : 5 : 5 –– 6 cm/yr 6 cm/yr
![Page 5: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/5.jpg)
Potensi Tinggi
CanalizationCatch-down
INFANT PERIOD
Growth Chart
cm
Catch-up
Potensi Tinggi Genetik
0 1 2 3 tahun
![Page 6: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/6.jpg)
Evaluation of growth Evaluation of growth
•• AnthropometryAnthropometry
–– Standing & sitting : proportionalStanding & sitting : proportional
–– Arm spanArm span–– Arm spanArm span
•• Bone age : Bone age :
–– GP, TW, RUTGP, TW, RUT
–– Normal, delayed, advancedNormal, delayed, advanced
–– prediction of final heightprediction of final height
![Page 7: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/7.jpg)
Growth chartGrowth chart
•• Growth curveGrowth curve
–– NCHS, Jumadias, HusainiNCHS, Jumadias, Husaini
•• Plotting growthPlotting growth•• Plotting growthPlotting growth
–– Normal, short, tallNormal, short, tall
•• Interpretation of plotInterpretation of plot
•• Potential genetic heightPotential genetic height
![Page 8: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/8.jpg)
Growth Chart
145
150
155
160
165
170
175
180
185
190
195
Height
97
50
3
80
85
90
95
100
105
110
115
120
125
130
135
140
2 4 6 8 10 12 14 16 18
Age (years)
Height
(cm)
![Page 9: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/9.jpg)
Growth Chart
145
150
155
160
165
170
175
180
185
190
195
Height
97
50
3
Tinggi Potensi Genetik
80
85
90
95
100
105
110
115
120
125
130
135
140
2 4 6 8 10 12 14 16 18
Age (years)
Height
(cm)
HACA
![Page 10: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/10.jpg)
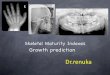
Bone ageBone age
•• Greulich & PyleGreulich & Pyle
–– Comparison of left wristComparison of left wrist
–– Prediction of FH after 6 yearsPrediction of FH after 6 years
–– Table Bayley & PinneauTable Bayley & Pinneau
•• Tanner Whitehouse IITanner Whitehouse II
–– Maturation of ossification centerMaturation of ossification center
–– More reliable : scoring systemMore reliable : scoring system
–– complicatedcomplicated
![Page 11: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/11.jpg)
Usia tulangUsia tulang
•• Tangan kiri caraTangan kiri cara
–– Atlas Greulich Atlas Greulich -- PylePyle
–– TannerTanner--Whitehouse Whitehouse
IIIIIIII
–– RWTRWT
•• PusatPusat--pusat osifikasipusat osifikasi
•• Prediksi tinggi akhirPrediksi tinggi akhir
![Page 12: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/12.jpg)
Short statureShort stature
•• Height < 2SDHeight < 2SD
•• Sex, age and raceSex, age and race
•• Pattern of growth more important Pattern of growth more important
rather than absolute position on rather than absolute position on
growth curvegrowth curve
![Page 13: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/13.jpg)
Short statureShort stature
–– Variants of normalVariants of normal
–– Prenatal onsetPrenatal onset–– Prenatal onsetPrenatal onset
–– Post natal onsetPost natal onset
![Page 14: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/14.jpg)
Variants of normal (normal growth velocity)Variants of normal (normal growth velocity)
•• Familial short statureFamilial short stature
–– Parents height genetically shortParents height genetically short
–– normal bone agenormal bone age
–– short adultshort adult–– short adultshort adult
•• Constitutional delay of growth & pubertyConstitutional delay of growth & puberty
–– Delayed puberty in the familyDelayed puberty in the family
–– Normal growth velocity Normal growth velocity
–– normal adult heightnormal adult height
![Page 15: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/15.jpg)
Prenatal onsetPrenatal onset
•• Primary growth deficiencyPrimary growth deficiency
–– MalformationMalformation
–– syndromessyndromes–– syndromessyndromes
•• Secondary growth deficiencySecondary growth deficiency
–– Low maternal socioeconomicLow maternal socioeconomic
–– UndernutritionUndernutrition
–– Maternal disorder or diseaseMaternal disorder or disease
![Page 16: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/16.jpg)
Post natal onsetPost natal onset
•• NutritionalNutritional
•• Deprivation syndromeDeprivation syndrome
•• Cardiac defectCardiac defect•• Cardiac defectCardiac defect
•• Respiratory insufficiencyRespiratory insufficiency
•• Renal disfunctionRenal disfunction
•• HormonalHormonal
•• Chronic infection, chronic diseaseChronic infection, chronic disease
![Page 17: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/17.jpg)
EtiologyEtiology
•• Primary disturbances of growthPrimary disturbances of growth
–– Skeletal dysplasiasSkeletal dysplasias
–– Chromosomal abnormalitiesChromosomal abnormalities–– Chromosomal abnormalitiesChromosomal abnormalities
–– Metabolic causesMetabolic causes
–– IUGRIUGR
–– SyndromesSyndromes
–– GeneticGenetic
![Page 18: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/18.jpg)
Etiology Etiology
•• Secondary growth disturbancesSecondary growth disturbances
–– UndernutritionUndernutrition
–– Disorder of the bowel, kidney, heart, lungDisorder of the bowel, kidney, heart, lung–– Disorder of the bowel, kidney, heart, lungDisorder of the bowel, kidney, heart, lung
–– Psychosocial deprivationPsychosocial deprivation
–– Chronic infection, drugsChronic infection, drugs
–– Endocrine disorderEndocrine disorder
–– Idiopathic growth delayIdiopathic growth delay
![Page 19: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/19.jpg)
Diagnostic Approach to Short Diagnostic Approach to Short StatureStature
Short Stature
Abnormal
Normal
AbnormalConstitutional DelayNormal Variant
Proportional Dysproportional
ExtrauterineIntrauterine
![Page 20: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/20.jpg)
Endocrinological causesEndocrinological causes
•• Normal variant : CDGPNormal variant : CDGP
•• GH DeficiencyGH Deficiency•• GH DeficiencyGH Deficiency
•• HypothyroidHypothyroid
•• Precocious PubertyPrecocious Puberty
•• Cushing’s syndromeCushing’s syndrome
•• PseudohypoparathyroidismPseudohypoparathyroidism
![Page 21: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/21.jpg)
Treatment Treatment
•• Depend on the etiologyDepend on the etiology
–– NutritionNutrition
–– Organic diseaseOrganic disease–– Organic diseaseOrganic disease
•• CHD, IDDMCHD, IDDM
–– HormonalHormonal
•• GH, Thyroid, Sex hormoneGH, Thyroid, Sex hormone
–– MechanicalMechanical
•• Bone lengthening : achondroplasiaBone lengthening : achondroplasia
![Page 22: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/22.jpg)
GH deficiencyGH deficiency
•• Short statureShort stature
•• ChubbyChubby
•• Abdominal adiposityAbdominal adiposity•• Abdominal adiposityAbdominal adiposity
•• MicropenisMicropenis
•• Single central incisorSingle central incisor
•• Frontal bossingFrontal bossing
•• ProportionalProportional
![Page 23: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/23.jpg)
GH DeficiencyGH Deficiency
•• Low growth velocity : < 25%Low growth velocity : < 25%
•• Retarded bone ageRetarded bone age
•• GH level < 10 ng/dlGH level < 10 ng/dl•• GH level < 10 ng/dlGH level < 10 ng/dl
–– Screening tests : sleep & excerciseScreening tests : sleep & excercise
–– Stimulation testStimulation test
•• 2 tests : ITT & Arginine,2 tests : ITT & Arginine,
•• Low IGFLow IGF--11
![Page 24: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/24.jpg)
Causes of GH DeficiencyCauses of GH Deficiency
•• CongenitalCongenital
–– IdiopathicIdiopathic
–– GeneticGenetic
–– Assosiated anatomic defect : SOD,midline defectAssosiated anatomic defect : SOD,midline defect–– Assosiated anatomic defect : SOD,midline defectAssosiated anatomic defect : SOD,midline defect
•• AcquiredAcquired
–– TraumaTrauma
–– NeoplasmaNeoplasma
–– Cranial irradiationCranial irradiation
–– etcetc
![Page 25: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/25.jpg)
TreatmentTreatment
•• Varies: GH 14 Varies: GH 14 -- 21 IU/m2/day21 IU/m2/day
•• 6 times/week6 times/week
•• Monitoring:Monitoring:•• Monitoring:Monitoring:
–– Height, velocityHeight, velocity
–– Side effectSide effect
•• Terminate :Terminate :
–– No response < 2 cmNo response < 2 cm
–– Epiphyseal plate closure Epiphyseal plate closure
![Page 26: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/26.jpg)
CDGPCDGP
•• Family historyFamily history
•• Growth velocity normalGrowth velocity normal
•• Bone age retardedBone age retarded•• Bone age retardedBone age retarded
•• Puberty : latePuberty : late
•• Adult height : normalAdult height : normal
•• Treatment : No NeedTreatment : No Need
![Page 27: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/27.jpg)
Congenital hypothyroidismCongenital hypothyroidism
•• Large posterior fontanelleLarge posterior fontanelle
•• Respiratory difficultyRespiratory difficulty
•• HypothermiaHypothermia
•• Feeding difficultyFeeding difficulty•• Feeding difficultyFeeding difficulty
•• LethargyLethargy
•• Delay in passing meconiumDelay in passing meconium
•• Abdominal distentionAbdominal distention
•• Vomitting Vomitting
•• Prolonged jaundicedProlonged jaundiced
•• Oedema Oedema
![Page 28: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/28.jpg)
Cushing’s SyndromeCushing’s Syndrome
•• Corticosteroid excessCorticosteroid excess
•• Growth retardation due toGrowth retardation due to–– Interferring protein anabolismInterferring protein anabolism
–– Impairing somatomedin productionImpairing somatomedin production–– Impairing somatomedin productionImpairing somatomedin production
•• HypertensionHypertension
•• Obesity predominant : trunk and neck, moon Obesity predominant : trunk and neck, moon faceface
•• Disturbances of glucose metabolismDisturbances of glucose metabolism
•• Purple striae, hirsutism, osteoporosis, Purple striae, hirsutism, osteoporosis, hypogonadismhypogonadism
•• Muscular weaknessMuscular weakness
![Page 29: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/29.jpg)
PseudohypoparathyroidismPseudohypoparathyroidism
•• Short statureShort stature
•• Mental retardationMental retardation
•• Albright’s osteodystrophyAlbright’s osteodystrophy•• Albright’s osteodystrophyAlbright’s osteodystrophy
•• Round faciesRound facies
•• Ectopic calcification Ectopic calcification
![Page 30: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/30.jpg)
Pola pertumbuhan Pola pertumbuhan
linierlinier
![Page 31: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/31.jpg)
Pola pertumbuhanPola pertumbuhan
![Page 32: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/32.jpg)
ConclusionConclusion
•• Short stature Short stature
–– Etiology : varies; endocrinology Etiology : varies; endocrinology
–– Treatable, depend on the etiologyTreatable, depend on the etiology–– Treatable, depend on the etiologyTreatable, depend on the etiology
–– Psychosocial problemPsychosocial problem
•• Growth monitoring : importantGrowth monitoring : important
•• Anthropometric measurementAnthropometric measurement
–– Clue to diagnosisClue to diagnosis
![Page 33: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/33.jpg)
EtiologyEtiology
•• Primary disturbances of growthPrimary disturbances of growth
–– Skeletal dysplasiasSkeletal dysplasias
–– Chromosomal abnormalitiesChromosomal abnormalities–– Chromosomal abnormalitiesChromosomal abnormalities
–– Metabolic causesMetabolic causes
–– IUGRIUGR
–– SyndromesSyndromes
–– GeneticGenetic
![Page 34: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/34.jpg)
Tall StatureTall Stature
•• Height > 2 SDHeight > 2 SD
•• Age, sex and raceAge, sex and race
![Page 35: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/35.jpg)
Etiology Etiology
•• GeneticGenetic–– Familial tall statureFamilial tall stature
–– Familial rapid maturationFamilial rapid maturation
•• HormonalHormonal•• HormonalHormonal–– GH excessGH excess
–– HyperthyroidHyperthyroid
–– Androgen/estrogen excessAndrogen/estrogen excess
•• SyndromesSyndromes–– Weaver, Sotos, Marfan, KleinefelterWeaver, Sotos, Marfan, Kleinefelter
•• Metabolic disordersMetabolic disorders
![Page 36: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/36.jpg)
Diagnostic approachesDiagnostic approaches
•• Height, velocityHeight, velocity
•• DysmorphismDysmorphism
•• Family historyFamily history•• Family historyFamily history
![Page 37: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/37.jpg)
TreatmentTreatment
•• To treat or not to treatTo treat or not to treat
–– Family or patient requestFamily or patient request
–– Contra indicationContra indication
•• Psychosocial problemPsychosocial problem
•• Female > maleFemale > male
•• Ethynil estradiol 100 ug/dayEthynil estradiol 100 ug/day
•• Testosterone 200 Testosterone 200 -- 250 mg every 2 250 mg every 2 –– 3 3 weekweek
![Page 38: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/38.jpg)
ConclusionConclusion
•• Short stature & tall stature Short stature & tall stature
–– Treatable, depend on the etiologyTreatable, depend on the etiology
–– Psychosocial problemPsychosocial problem–– Psychosocial problemPsychosocial problem
•• Growth monitoring : importantGrowth monitoring : important
•• Anthropometric measurementAnthropometric measurement
–– Clue to diagnosisClue to diagnosis
![Page 39: 3.SHORT STATURE TALL STATURE.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-endokrinologi/mk_end_slide_short... · •• Bone age : Bone age : –– GP, TW, RUTGP, TW, RUT ––](https://reader042.pdfslide.net/reader042/viewer/2022041201/5d46972b88c99391138c63c7/html5/page/39.jpg)