Embed Size (px)
Citation preview

Cardiac Cycle and Heart SoundsPart I
Mary Beth Fontana

Block Objectives
• Diagram the cardiac cycle, relating electrical and mechanical events to chamber and great artery pressures and ventricular volume; identify systole and diastole
• Describe the mechanism of production of normal and abnormal heart sounds: relate them to the electrical and pressure events of the cardiac cycle
Objectives
• Describe the use of the stethoscope– Auscultatory areas– Use of bell and diaphagm– Interpret the meaning of the auscultatory
findings

Resources• Lilly 5th edition Chapter 2 pp. 28-36,
Table 2.2 P. 42• Blaufuss.org. – heart sound tutorial quiz• There will be auscultation practice
sessions in week 7• The Blaufuss Sound Builder program used
in the practice sessions is available in the App store for a fee

Always Keep In Mind---
• The history and physical examination of the cardiovascular system make the vast majority of the diagnoses!!!!!!!

Auscultation Requires…….
• A quiet environment• A stethoscope with a bell for low pitched
sounds and diaphragm for high pitched sounds, well fitting ear pieces and short tubing
• A thinking auscultator who-– knows where to place the stethoscope to hear
specific sounds-based on anatomic relationships of the heart and great vessels to chest wall landmarks
•

Auscultatory Areas
Auscultatory Areas
Aortic Pulmonic
MitralTricuspidAortic 2nd ICS RSB
Pulmonic 2nd ICS LSB
Tricuspid LLSB
Mitral Apex 5th ICS MCL

A Thinking Auscultor
– Can describe the events in the cardiac cycle responsible for the production of the normal and abnormal heart sounds.
– can reproduce the diagram below relating electrical events, mechanical events and heart sounds. This cardiac cycle diagram will be the reference for the discussion of all of the heart sounds.
–

Cardiac Cycle
Chamber and Arterial Pressures
Electrical activation causes chamber contraction which raises pressure. Chamber relaxation and emptying cause pressure to fall
ECG

Generation of Heart Sounds• The opening and closing of the heart valves
are determined by pressure differences between the chambers and great vessels on either side of the valves
• Most of the heart sounds discussed in these 2 lectures are related to opening and closing of the cardiac valves
• The sounds occur when the valve leaflets, vessel or ventricular walls tense when they stop moving

Normal Heart Sounds
• First Heart Sound (S1) occurs when the mitral and tricuspid valves close
• Second Heart Sound occurs when the aortic and pulmonic valves close
• Opening of normal cardiac valves is silent

Descriptors of Heart Sounds
• Intensity or loudness• Frequency (high pitched or low pitched)• Splitting– clinically important for the
second heart sound

Intensity Depends Upon…..
• Mobility of the valve leaflets• The distance the leaflets move• The rate of pressure generation driving the
leaflet movement• Mass of the valve leaflets• Source to stethoscope distance

Cardiac Cycle
Chamber and Arterial Pressures
Left heart pressures and velocities are higher than in the right heart, so the contributions to S1 and S2 are louder, higher in frequency
ECG
LV 140/12
Ao 140/90
RV 30/8
PA 30/10
LA (12)
RA (8)

Mitral valve closes
Tricuspid valve closes
First Heart Sound S1
Ventricular depolarization causes ventricular contraction. S1 occurs when ventricular pressure exceeds atrial pressure. Mitral closes before tricuspid
S1LLSB and Apex with the diaphragm

Increased First Heart Sound
• Short PR interval• High cardiac output or tachycardia• Mobile valve leaflets with increased mass
– Scarred stenotic mitral valve– Redundant prolapsing mitral valve

Decreased First Heart Sound
• Long PR interval• Mitral regurgitation– murmur obscures S1,
lack of leaflet coaptation, slow closing velocity
• Decreased leaflet mobility from scarring, calcification– atrioventricular valve stenosis
• Noncompliant LV – high diastolic pressure “precloses” leaflets

Second Heart Sound S2
Aortic valve closes A2
Pulmonic valve closes P2
S1 S2
LV and RV pressures drop below aortic and PA pressures after ejection and relaxation. A2 is louder, best at 2RSB; normal P2 only heard at 2LSB

Increased A2, P2
• Arterial hypertension• Mobile leaflets with increased mass• Increased pulmonary blood flow (P2)
Decreased A2,P2
• Decrease mobility in severe valve stenosis• Calcification of aortic valve may restrict
mobility so severely that A2 is absent

Normal Splitting of S2
• A2 and P2 normally superimposed in expiration
• Inspiration delays P2 due to…..– Negative intrathoracic pressure increases
right heart filling. The RV takes longer to eject the increased volume
– Negative intrathoracic pressure increases pulmonary capacitance, delaying the back flow to close the pulmonic valve

Abnormal Splitting of S2
• Widened splitting – electrical or mechanical delay of the RV delays P2. Split S2 in expiration widens with inspiration
• Fixed splitting – atrial septal defect continuously increases right heart filling, delaying P2, unaffected by respiration
• Paradoxical splitting – electrical or mechanical delay in LV delays A2 so it follows P2. P2 moves out to meet A2 with inspiration

Cardiac Cycle and Heart Sounds Part II
Mary Beth Fontana

Extra Systolic Heart Sounds

Ejection Clicks
Aortic valve opens
Pulmonic valve opens
Audible opening of mobile congenitally stenotic aortic or pulmonic valves, also dilated aorta or PA
S1EC
Follows S1 by duration of isovolumic contraction
High pitched, best at LSB
S2

Nonejection Clicks
S1 A2SC Prolapsing mitral or tricuspid valve leaflets reach limit of motion and tense later in systole

Extra Diastolic Heart Sounds

Opening Snaps
Mitral valve opens
Tricuspid valve opens
Audible opening of mobile stenotic mitral or tricuspid valves; high pitched at LLSB or apex
Ventricular pressure drops below atrial pressure
S1
S2
OS

Third Heart Sound S3
LV early diastolic filling S3
RV early diastolic filling S3
S1
S2
S3
Early diastole after S2. Low pitched-with the bell, left lateral decubitus
Dilated ventricle with poor function and/or increased early diastolic filling
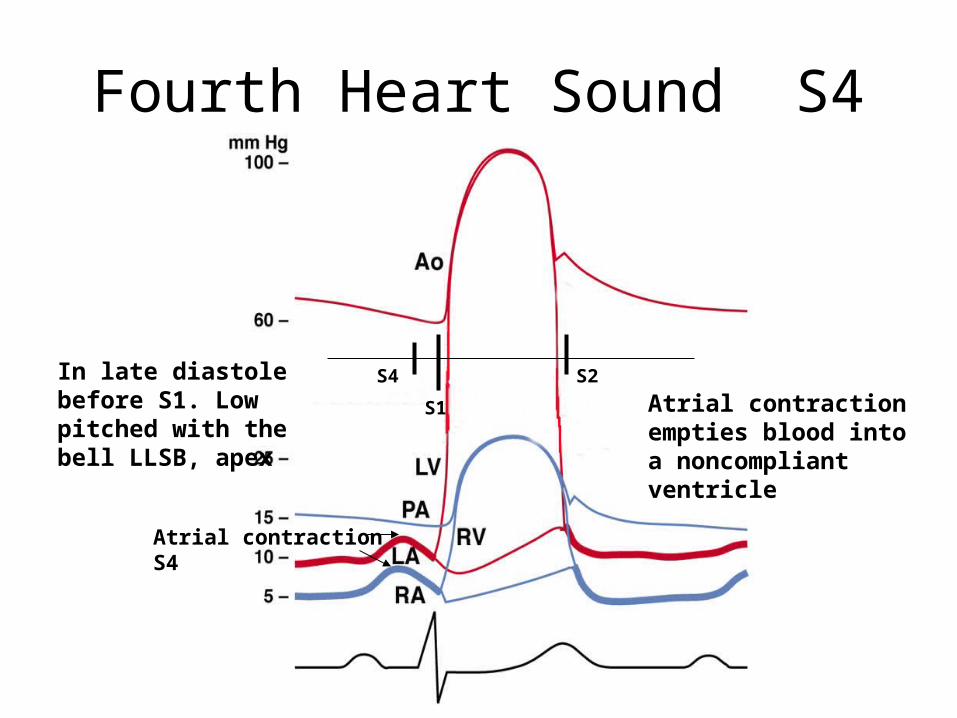
Fourth Heart Sound S4
Atrial contraction S4
S4S1
S2Atrial contraction empties blood into a noncompliant ventricle
In late diastole before S1. Low pitched with the bell LLSB, apex

Summary of Heart Sounds
S4 S1
EC
SC A2
P2
OS
S3






























