Embed Size (px)
Citation preview
CNS INFECTIONS
Ivo Bekavac, MD, PhD
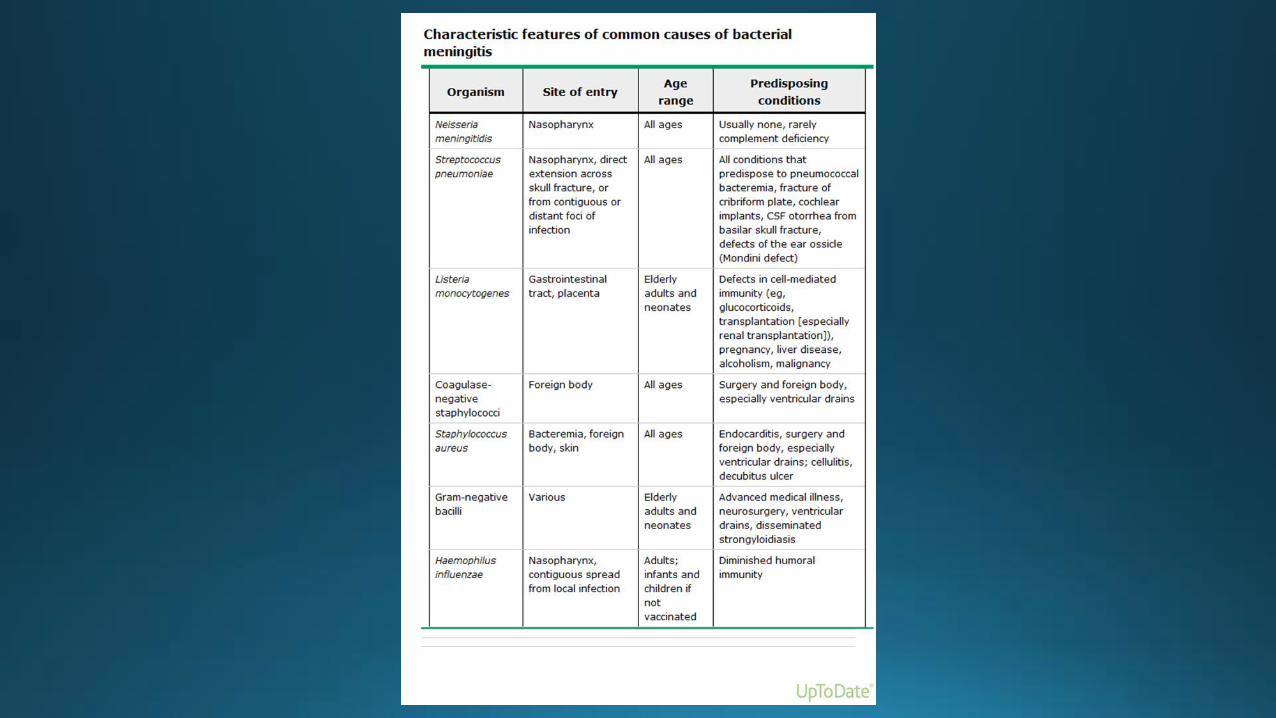
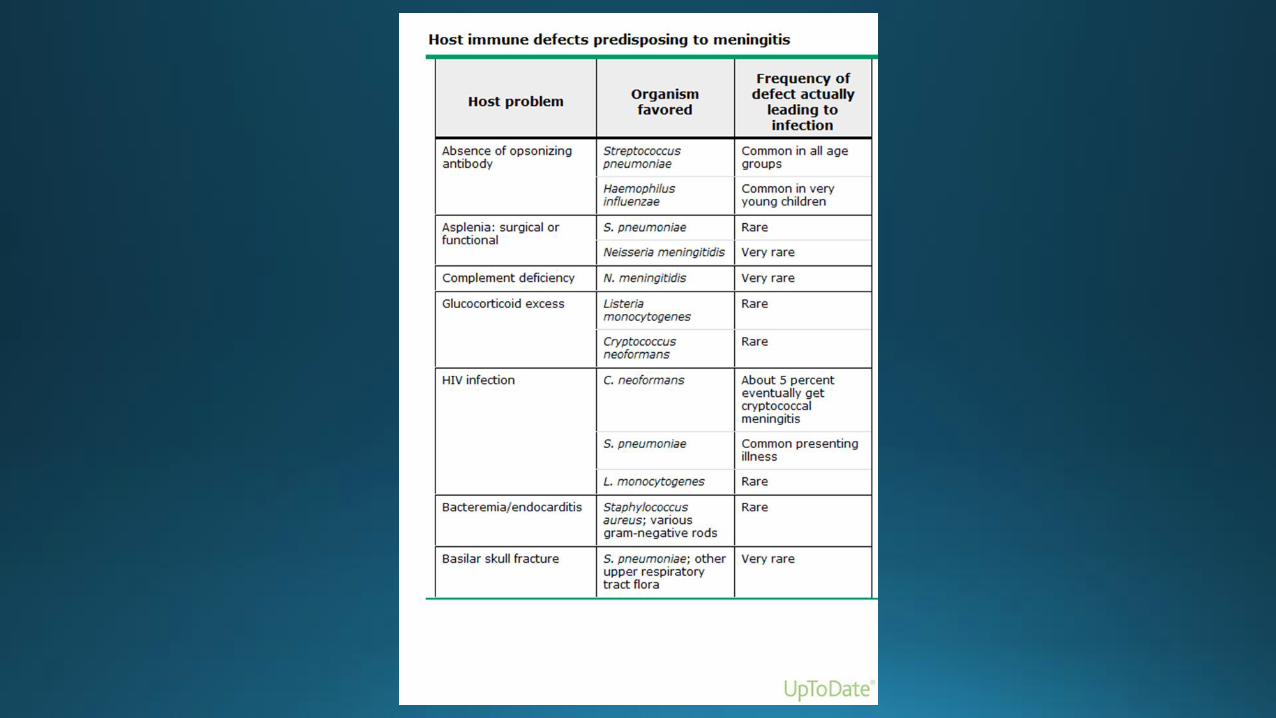
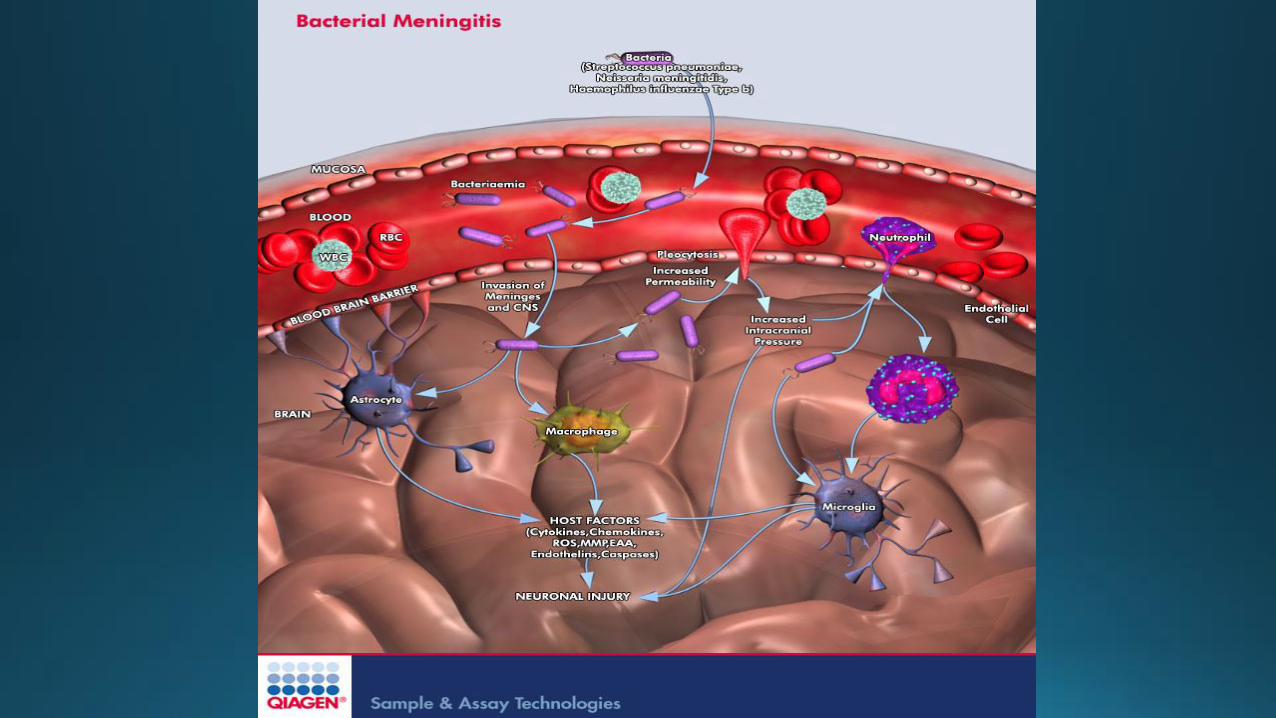
ACUTE BACTERIAL MENINGITIS BRAIN ABSCESS
Introduction
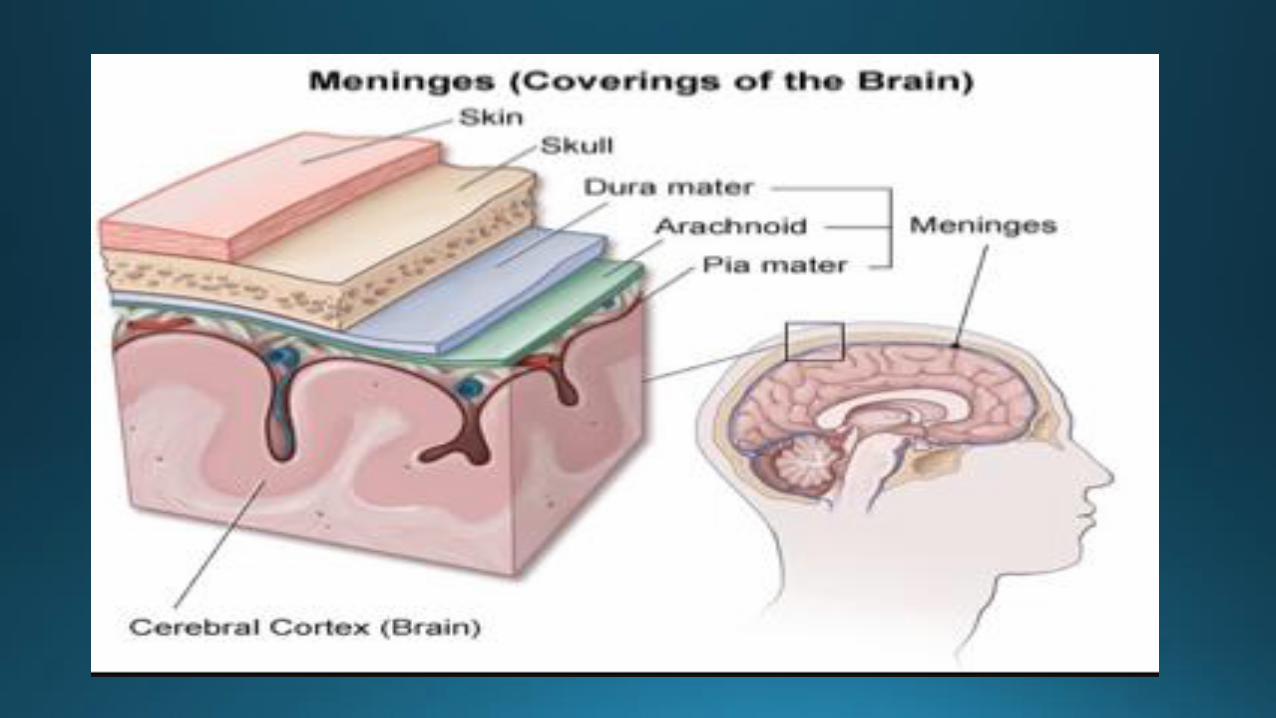
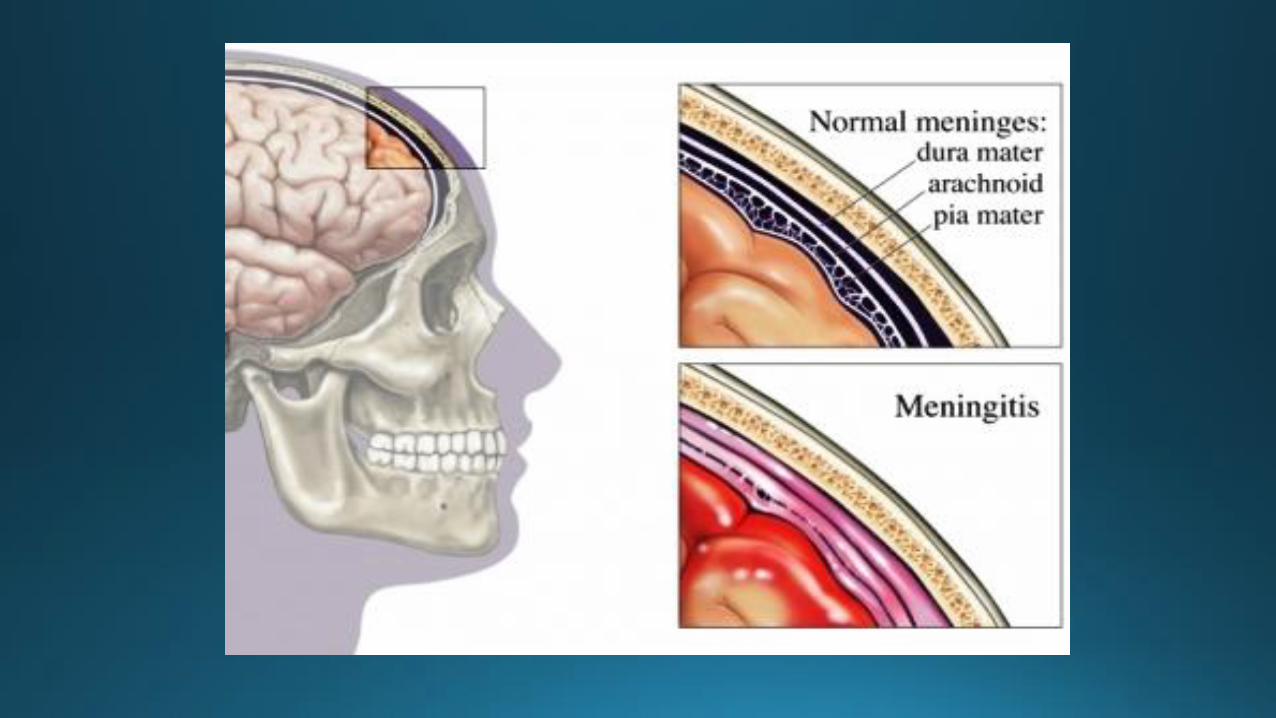
• Inflammatory disease of leptomeninges (arachnoid matter)
• Abnormal CSF studies (>WBC)
• 1.2 million/year worldwide
• Top 10 most common infectious causes of death
• 135000 deaths/year worldwide
• Neurologic sequelae are common

Epidemiology
• From original recognition in 1805 until the early 1900s, 100% fatal
• 1913- Simon Flexner intrathecal meningococcal antiserum
• 1930s- systemic antimicrobial therapy
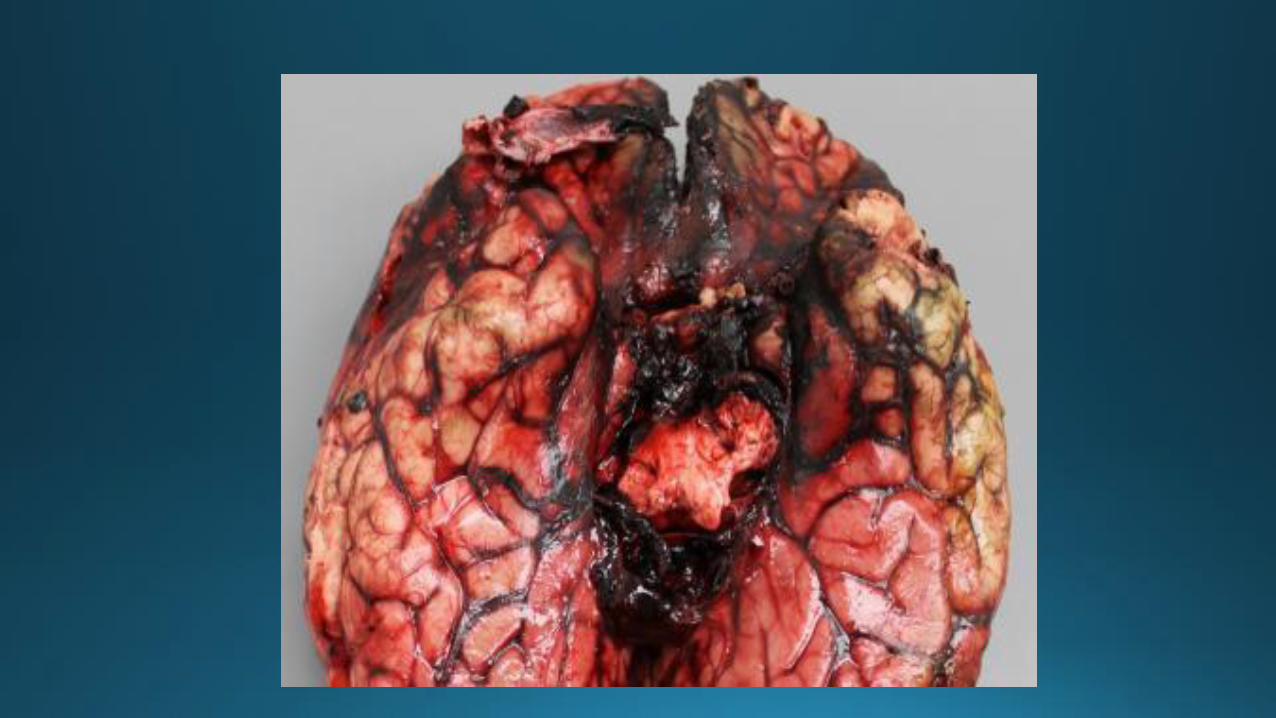
• Despite the effectiveness of current antibiotics, still significant morbidity and mortality
• Mortality 25%, morbidity 21-28%
Community-acquired
• Etiology
• Incidence
• Impact of pneumococcal conjugate vaccine
• Specific organisms
• Geography
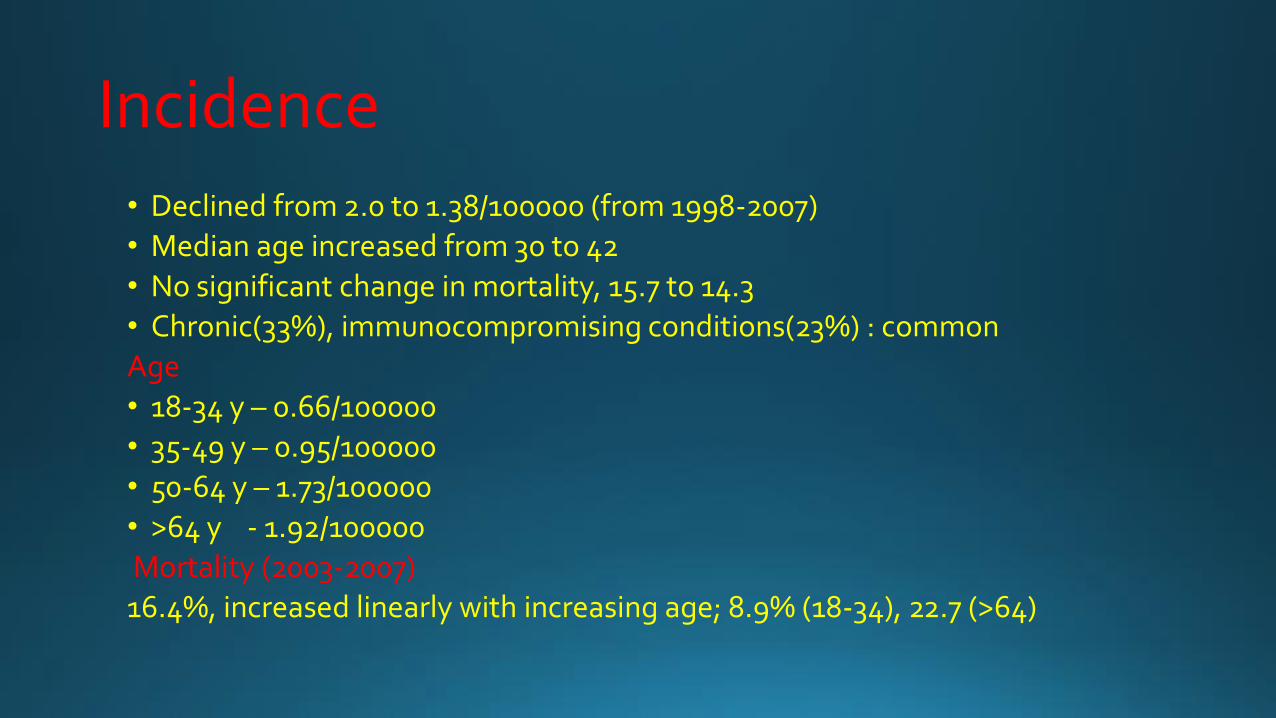
Incidence • Declined from 2.0 to 1.38/100000 (from 1998-2007)
• Median age increased from 30 to 42
• No significant change in mortality, 15.7 to 14.3
• Chronic(33%), immunocompromising conditions(23%) : common
Age
• 18-34 y – 0.66/100000
• 35-49 y – 0.95/100000
• 50-64 y – 1.73/100000
• >64 y - 1.92/100000
Mortality (2003-2007)
16.4%, increased linearly with increasing age; 8.9% (18-34), 22.7 (>64)
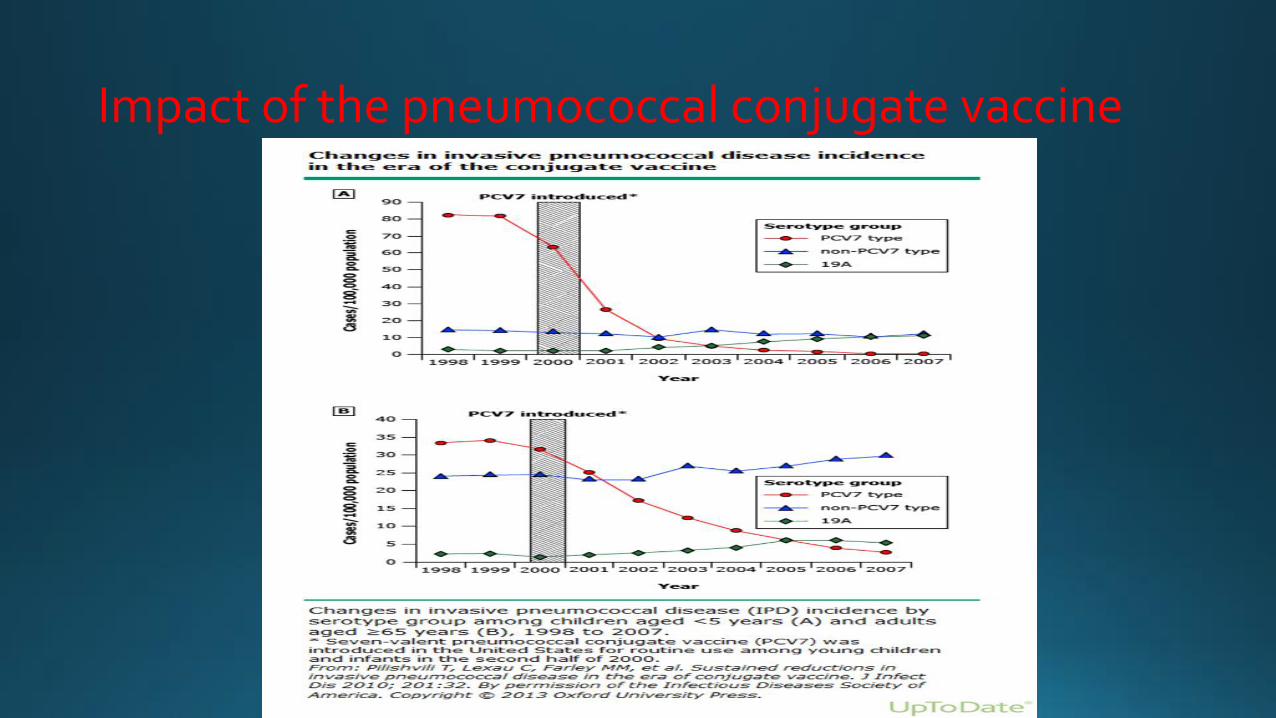
Impact of the pneumococcal conjugate vaccine
Clinical features
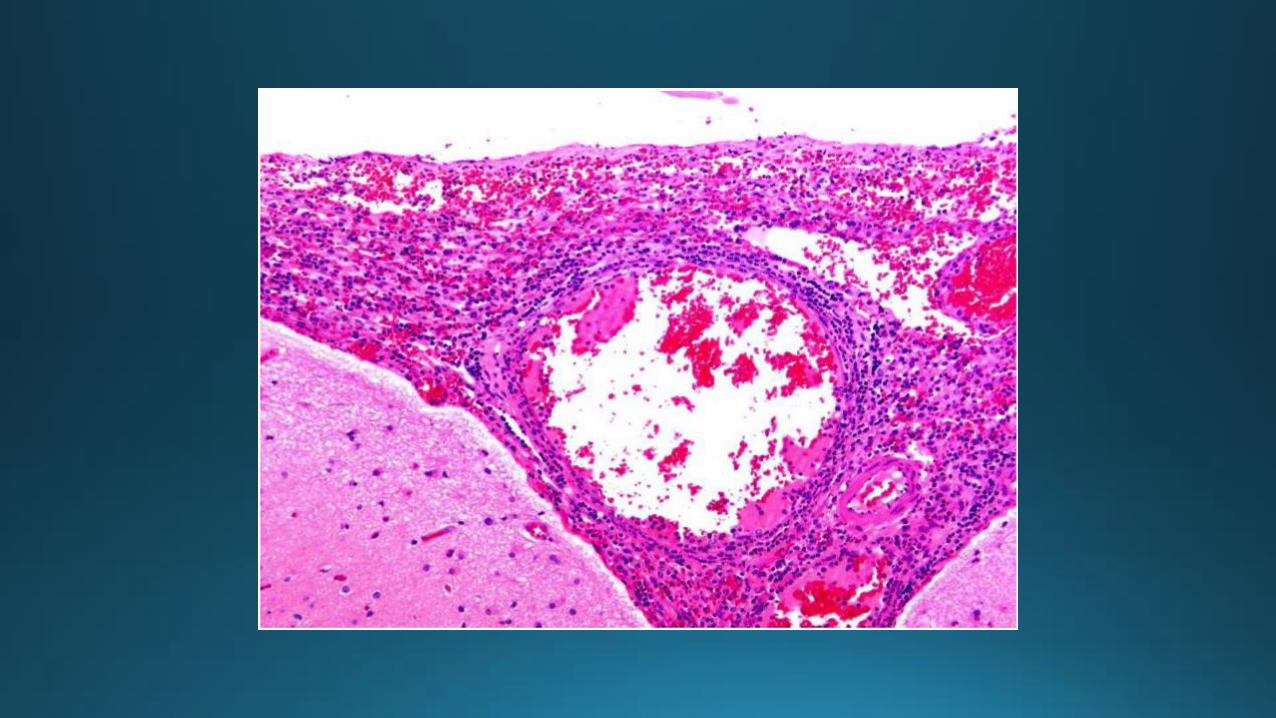
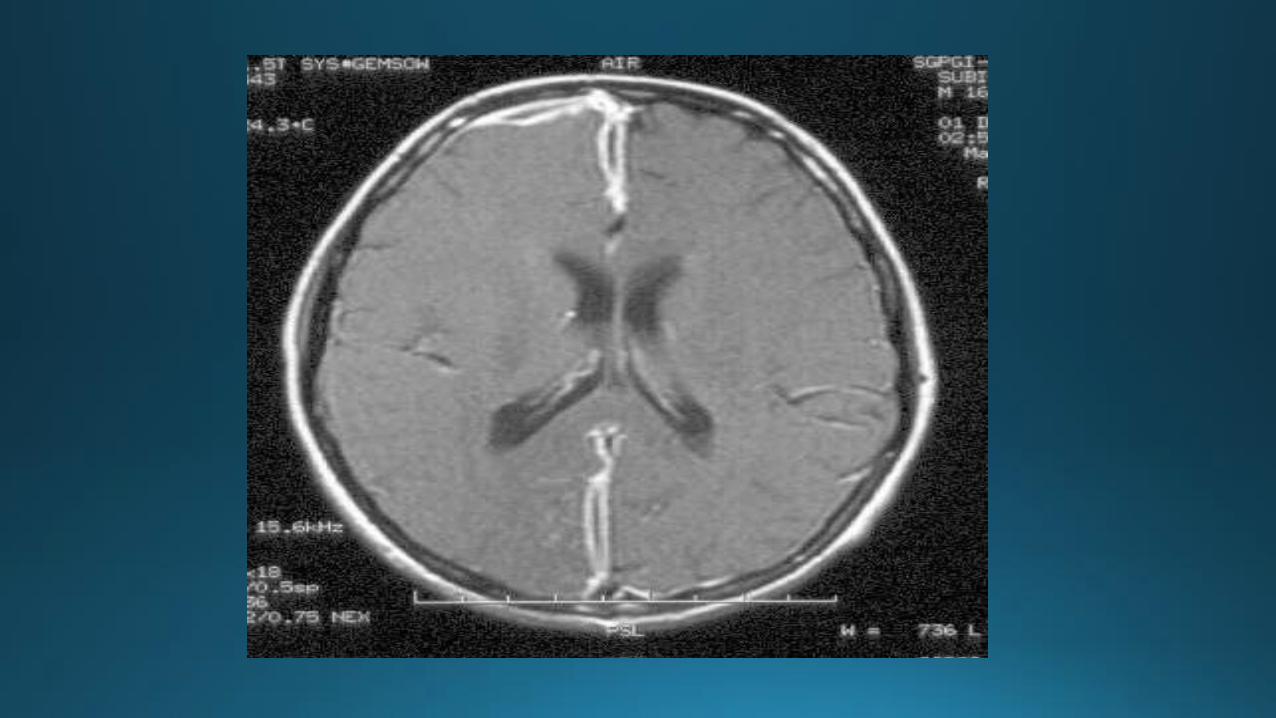
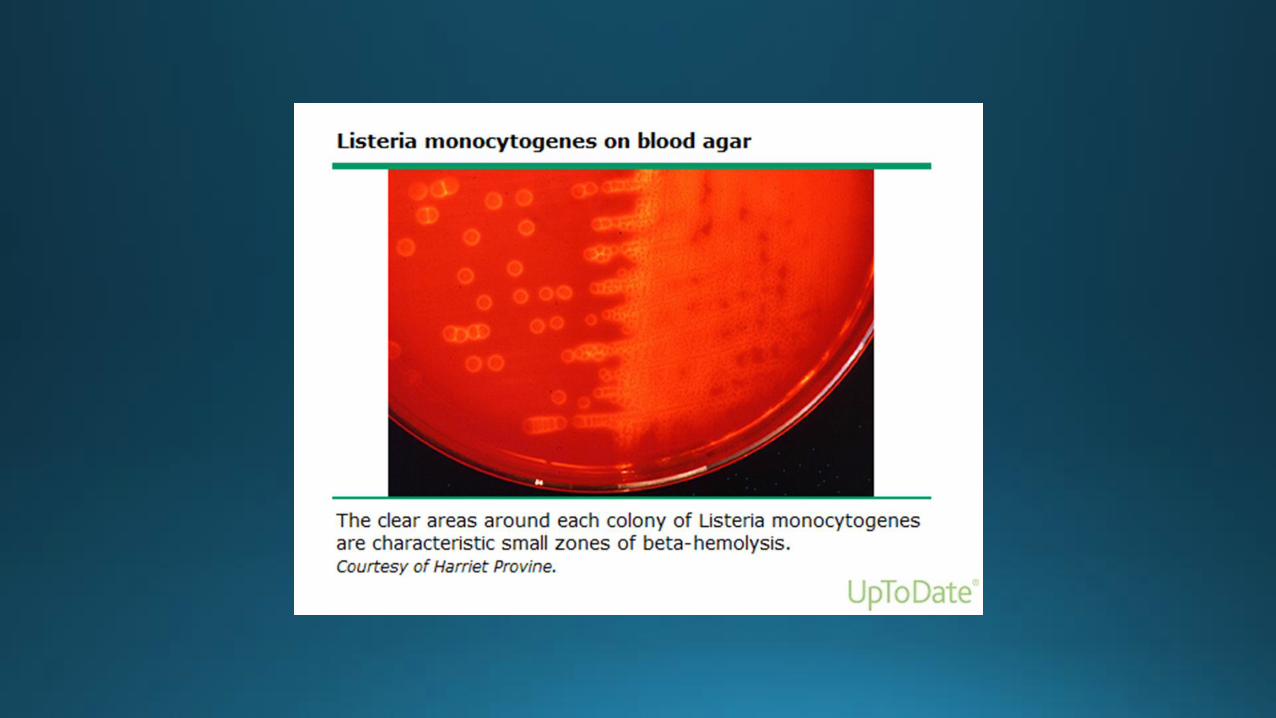
• Fever (95%) • Nuchal rigidity (88%) • Change in mental status (78%) • Headache (79-94%) Neurologic complication: • Seizure (Listeria) • Focal neurologic deficit (including CN palsy) • Papilledema • Cerebral infarction (25%) (36% with pneumococcal meningitis) • Hearing loss (late complication)

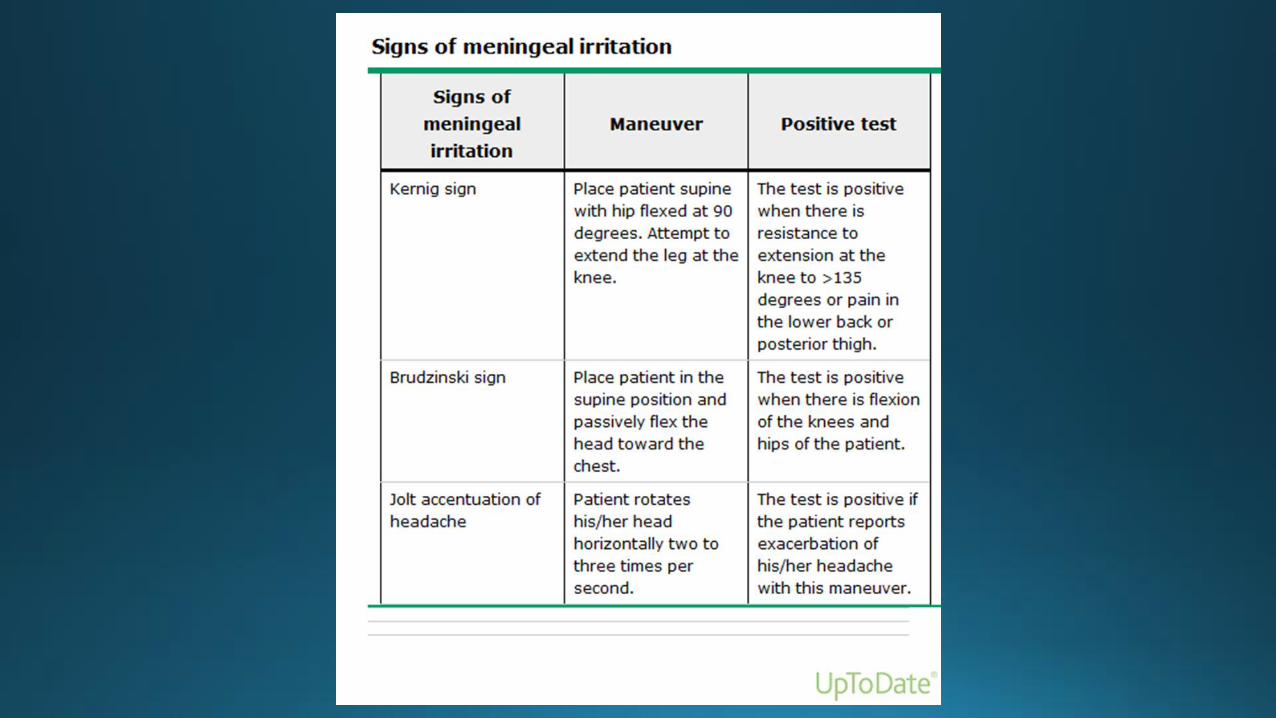
Examination for nuchal rigidity
• Inability to touch the chin to the chest; lateral motion of the neck is less reliable)
• Kernig sign – inability/reluctance to allow extension of the knee when the hip is flexed 90 degrees. (supine position/seated)
• Brudzinski sign – spontaneous flexion of the hips during attempted passive flexion of the neck.


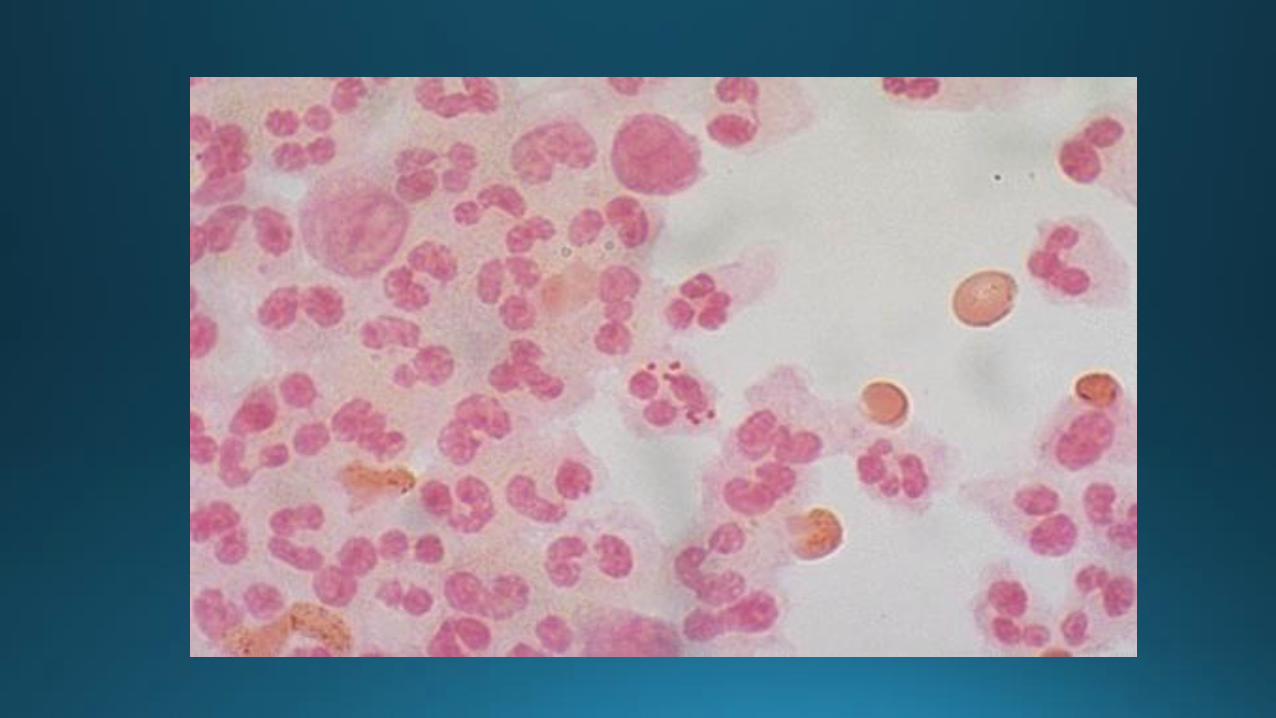
Laboratory features
Laboratory studies:
• Leukocytosis (left shift), leukopenia (severe infection)
• Thrombocytopenia
• Coagulation studies (disseminated intravascular coagulation)
• Hyponatremia (30%-usually mild)
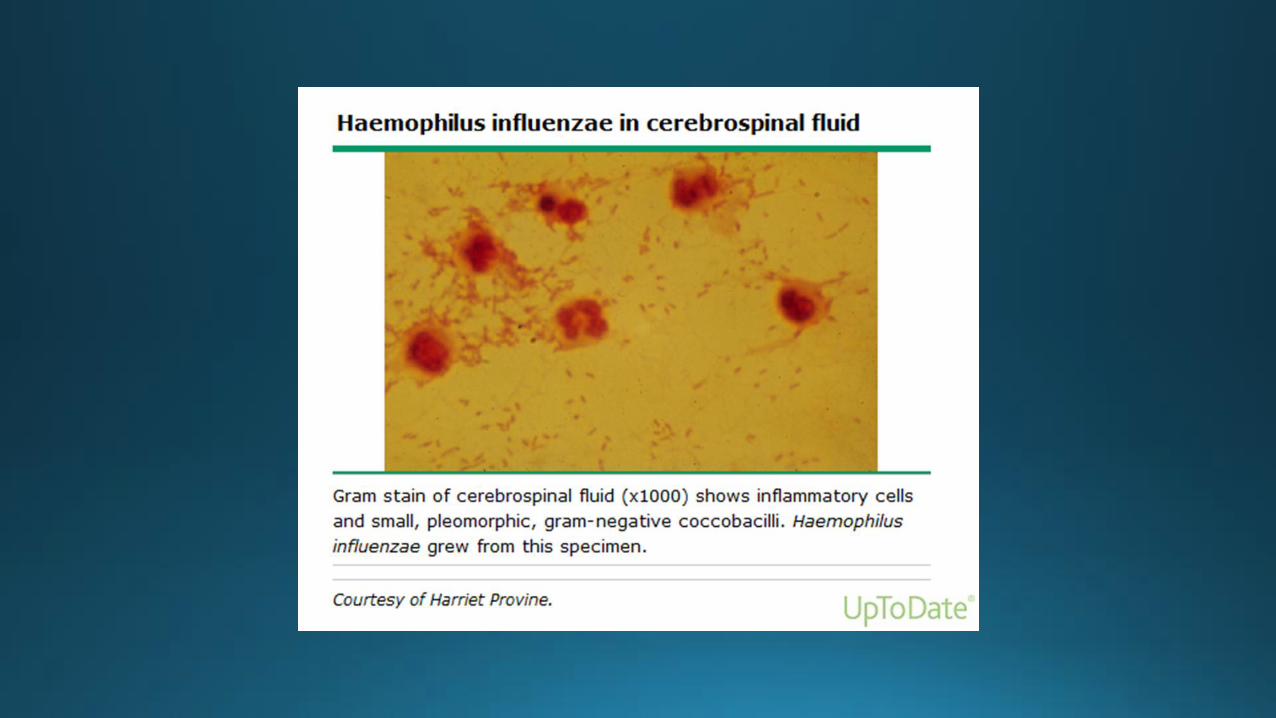
Blood cultures:
• Usually positive (50-90% with bacterial meningitis)
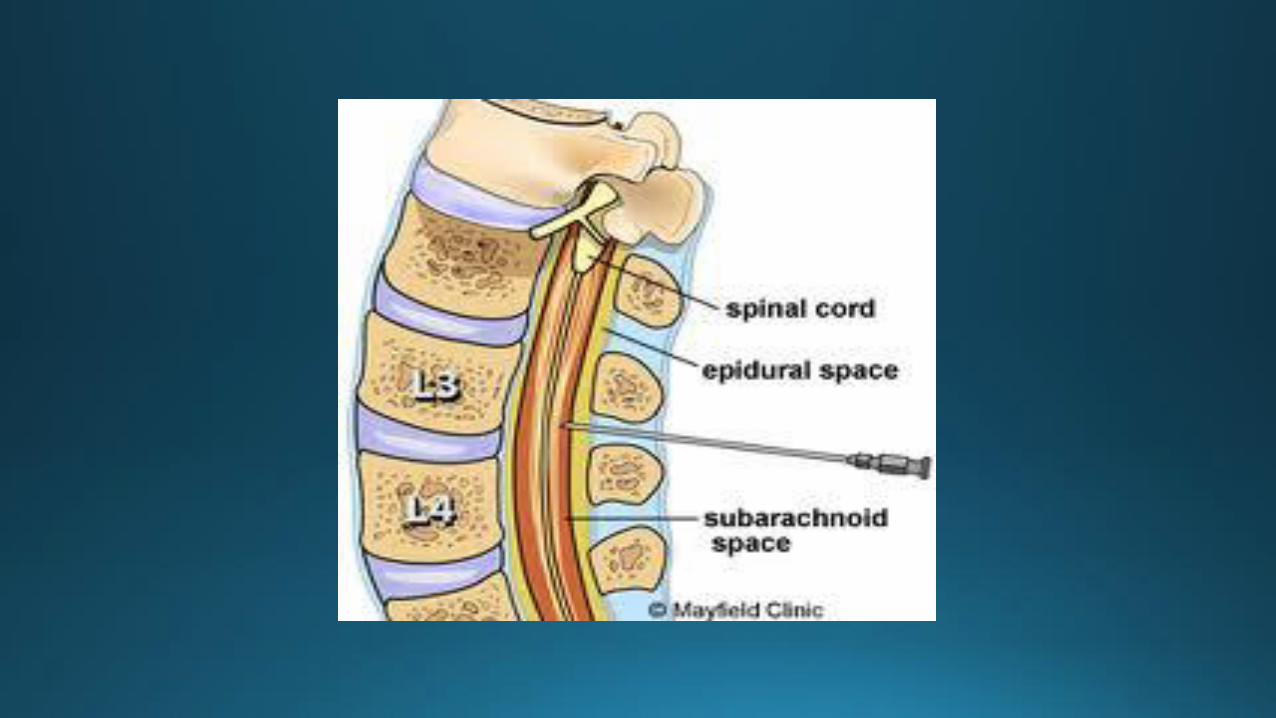
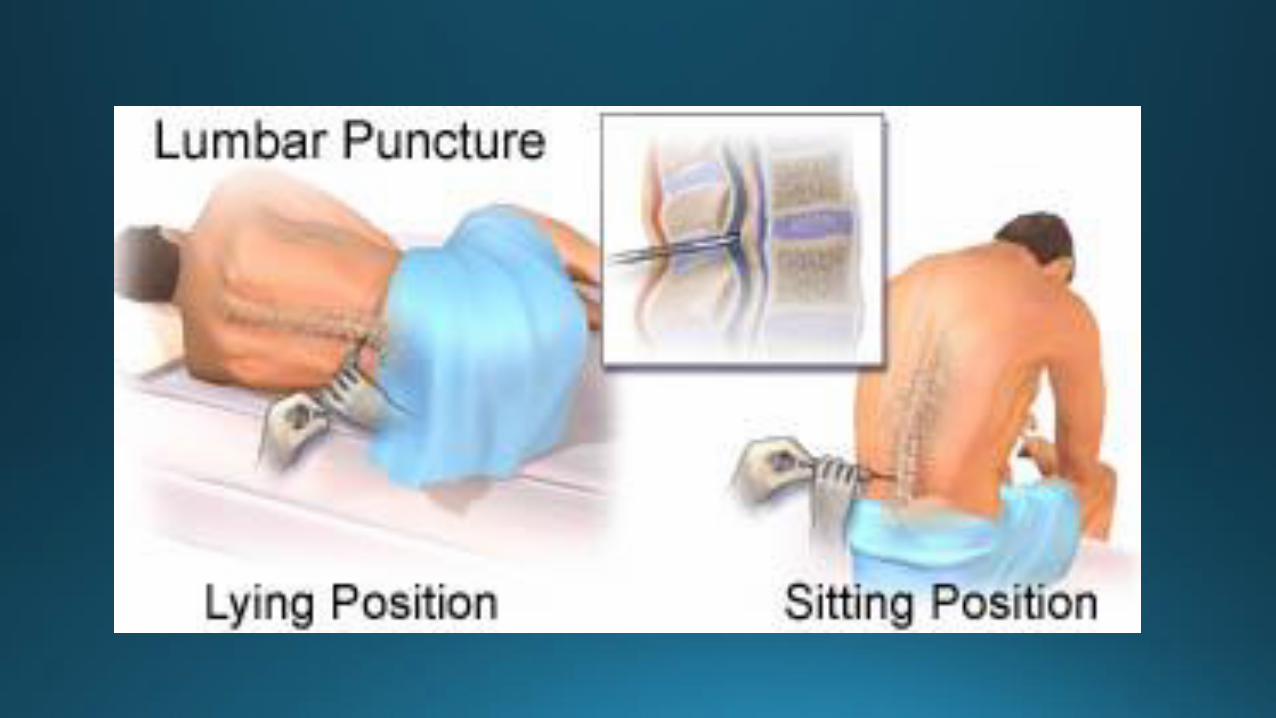
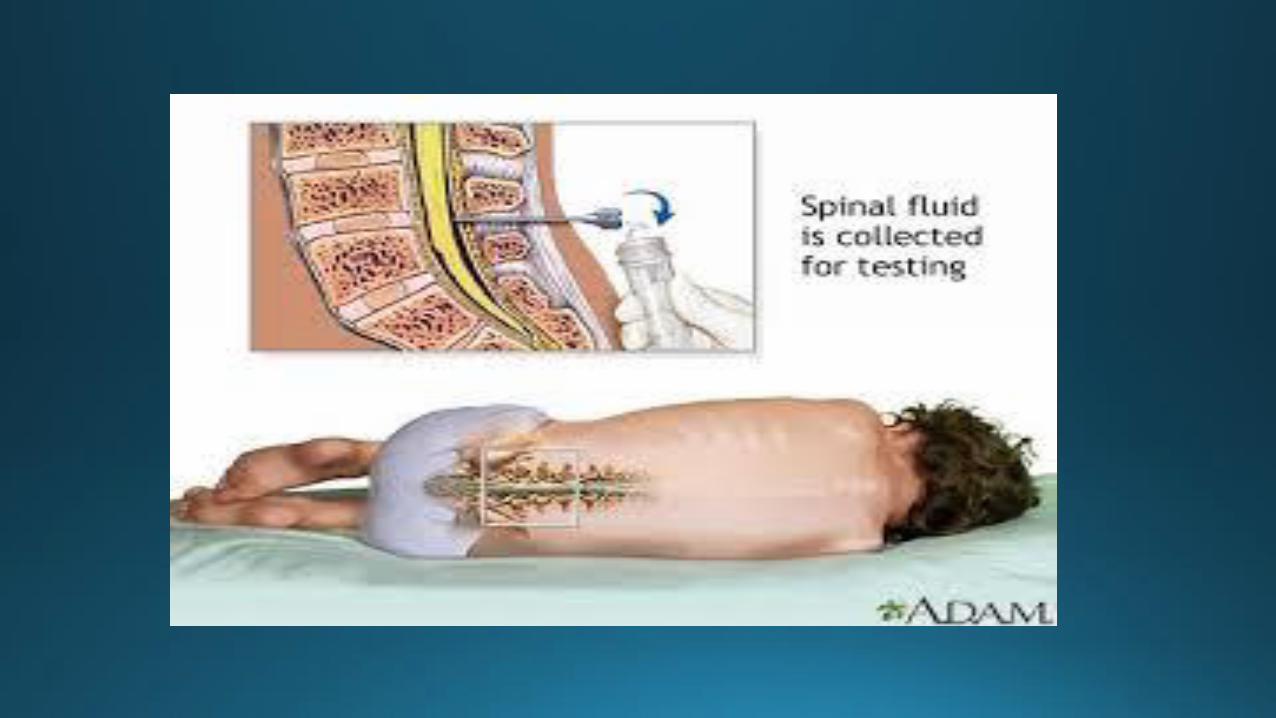
Lumbar puncture
• Crucial for establishing the diagnosis
Indications for CT scan before LP:
• Every patient with suspected meningitis should have CSF obtained unless LP is contraindicated (relative contraindications: evidence of >ICP (mass effect on CNS imaging, clinical signs of impending herniation), thrombocytopenia or another bleeding diathesis, spinal epidural abscess
CT scan should be performed (IDSA 2004)
• Immunocompromised state (HIV, immunosuppressive therapy, solid organ or hematopoetic stem cell transplantation
• History of CNS disease (mass lesion, stroke, focal infection)
• New onset of seizure (within one week of presentation)
• Papilledema
• Abnormal level of consciousness
• Focal neurologic deficit
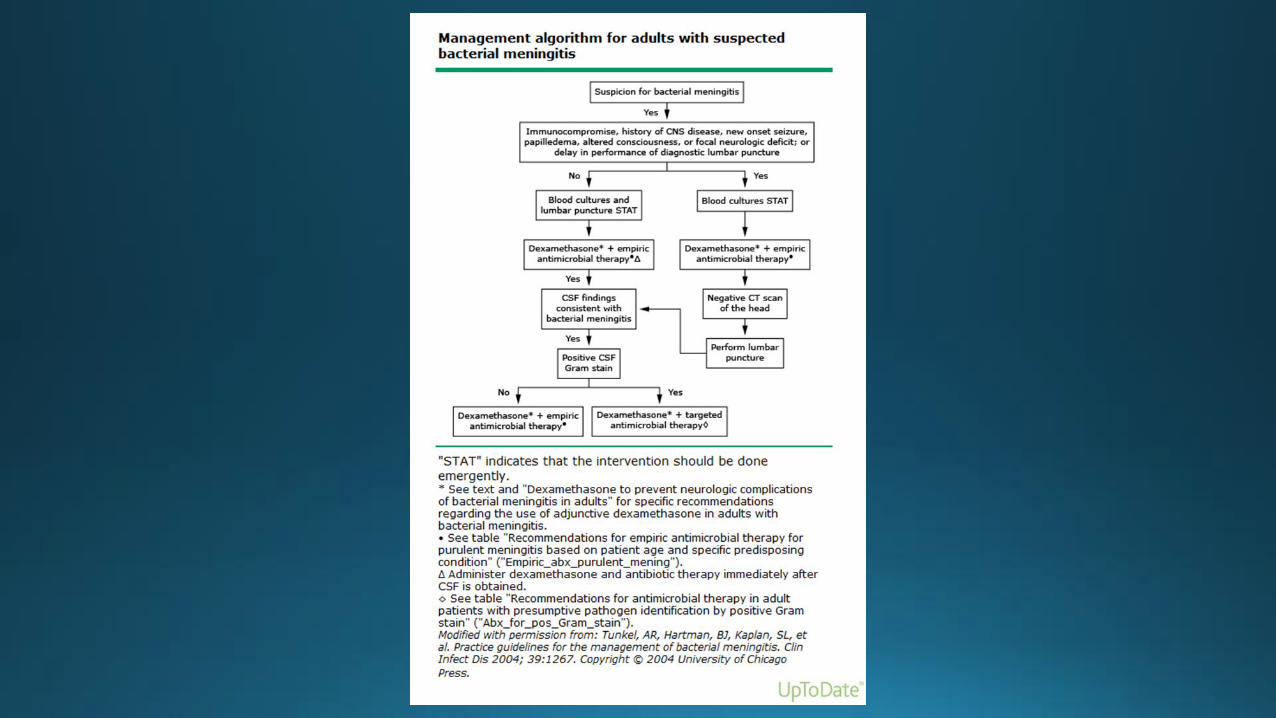
If LP is delayed
• Blood cultures should be obtained, empirical antibiotic treatment before CT/MRI, followed ASAP by the LP.
• In addition, dexamethasone (0.15 mg/kg i.v. q 6 hours)
Opening pressure
• Usually elevated (mean 350 mm H2O)




Rapid tests
• Latex agglutination (no longer routinely recommended)
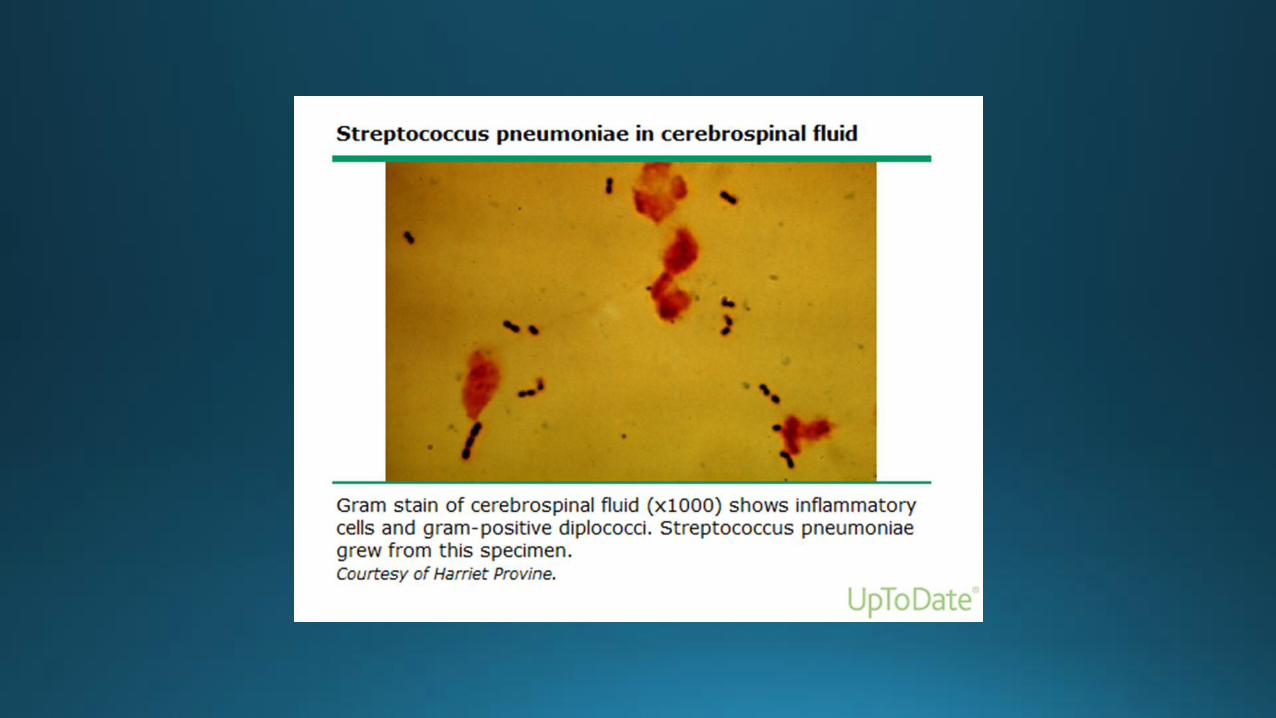
• Immonochromatographic test for S. Pneumoniae
• Polymerase chain reaction (PCR):
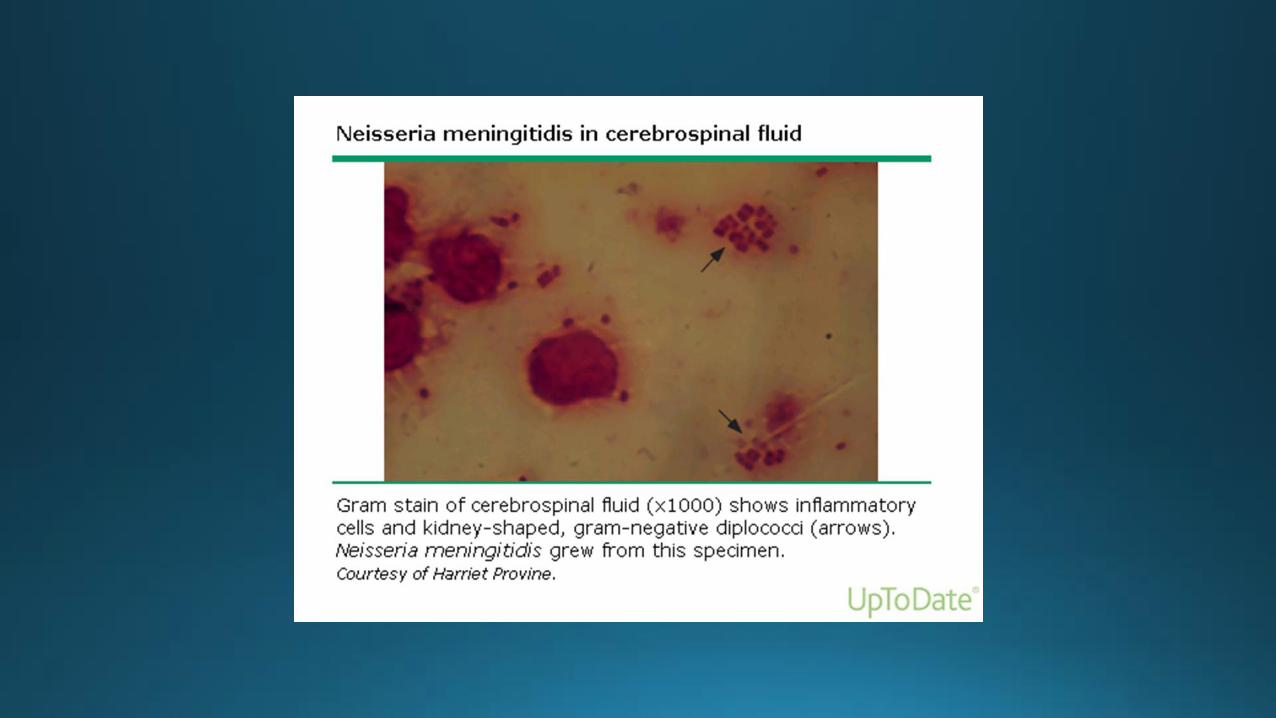
• N. meningitides
• S. pneumonia
• H. influenza type B

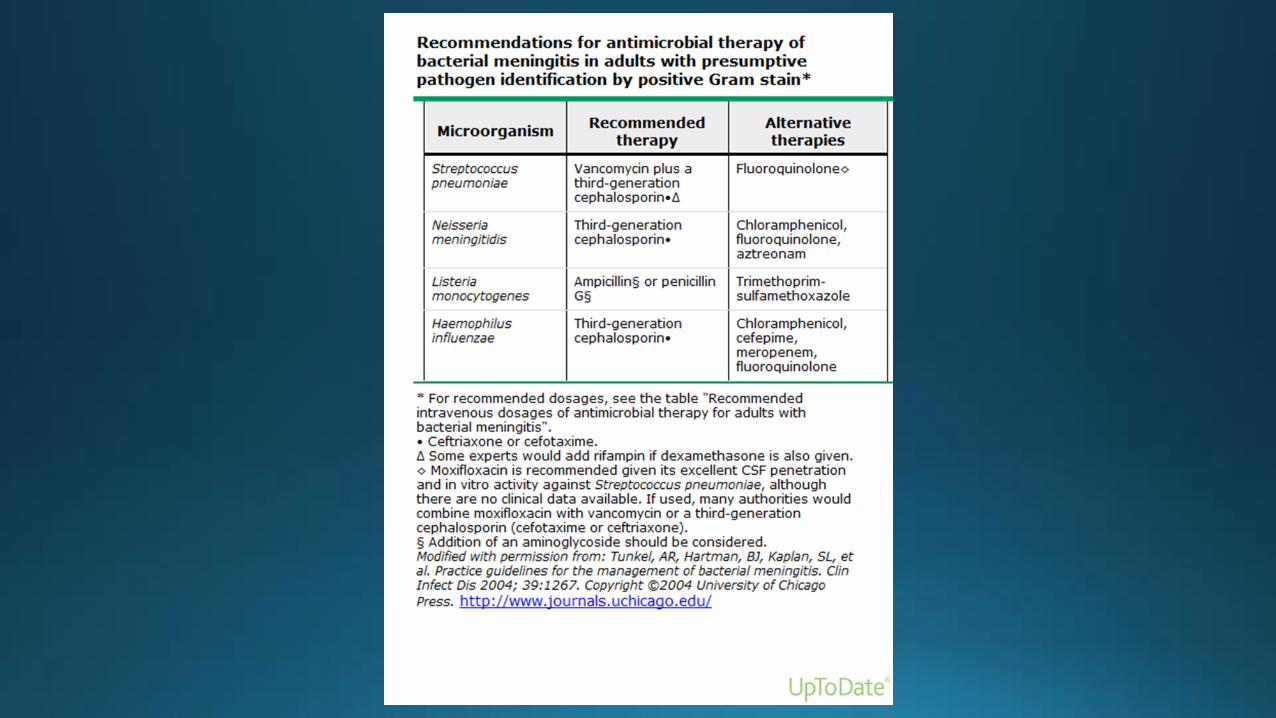
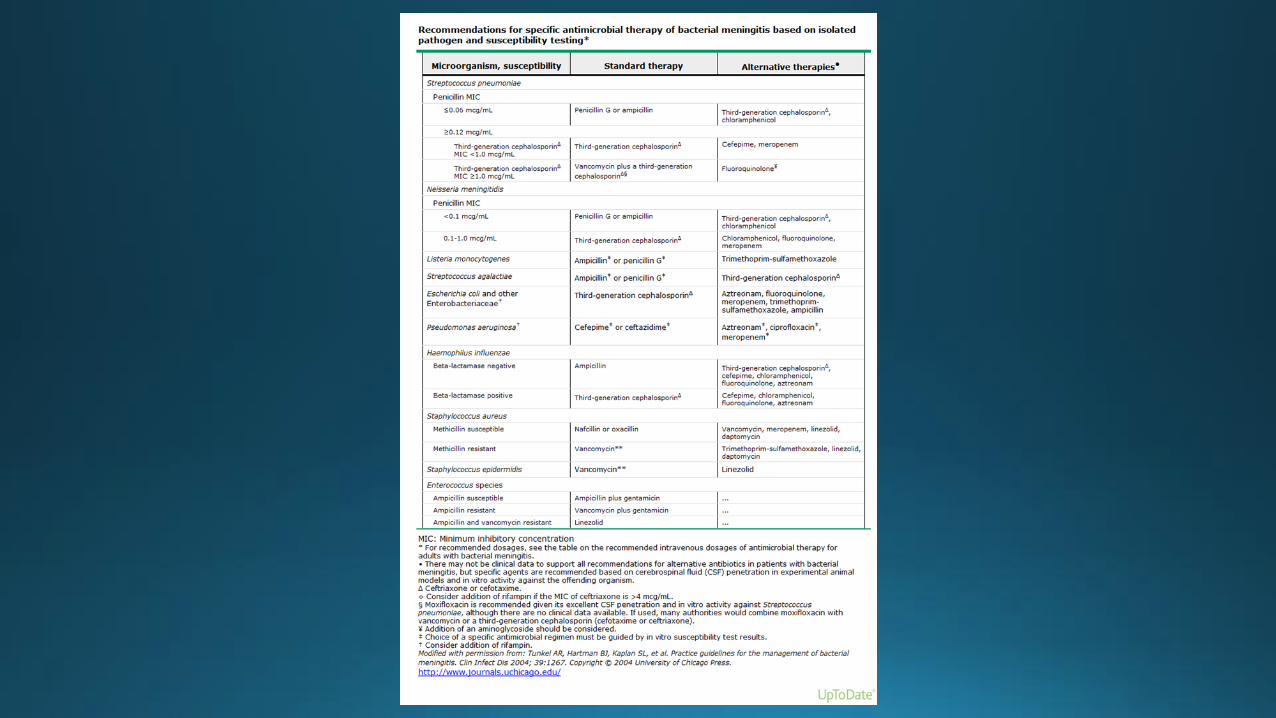
Initial therapy and prognosis of bacterial meningitis in adults
Avoidance of delay
• Antimicrobial therapy, along with adjunctive dexamethasone (when indicated) – should be initiated immediately after LP, or, if CT is to be performed before LP, immediately after blood cultures are obtained
• Effects of delay: hypotension, altered mental status and seizure
• Causes of delay: atypical presentation, delay due to imaging
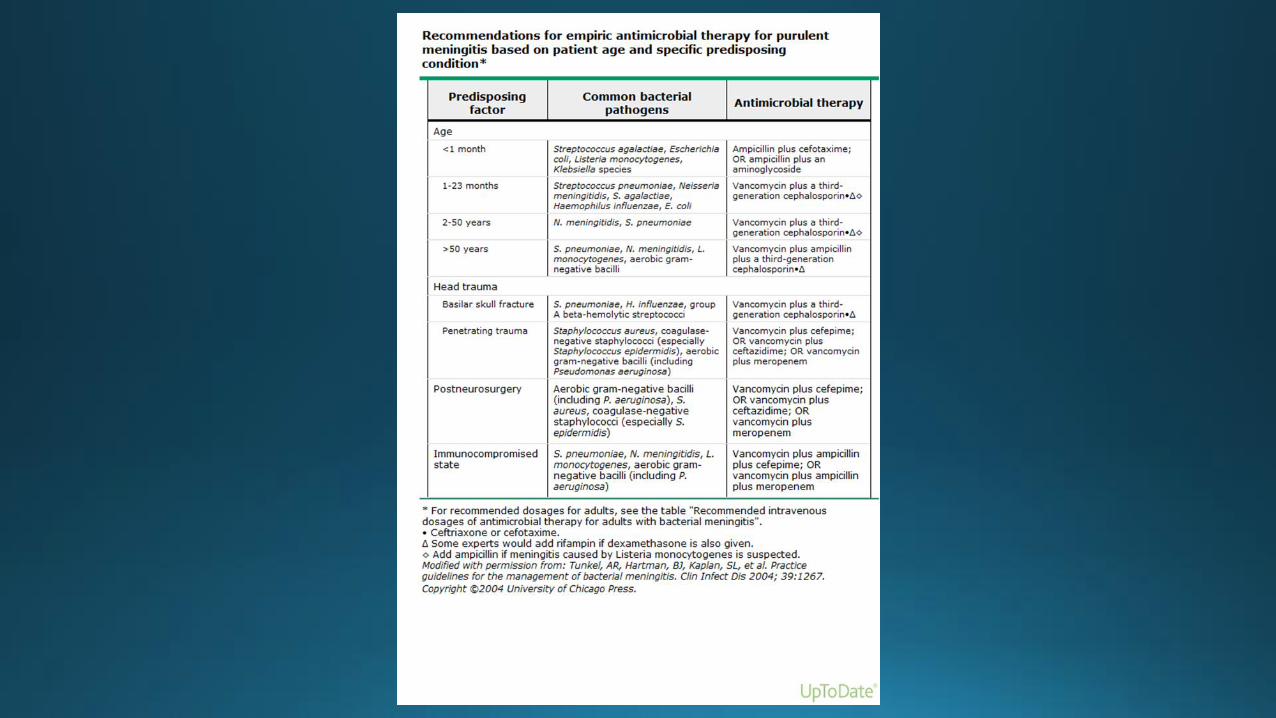
Antibiotic regimen
Requirements:
• Effectiveness against the infecting organism
• Drugs that enter CSF
• Structuring the regimen to optimize bactericidal efficacy
Adjunctive dexamethasone
• Indication: known or suspected pneumococcal meningitis
• Diminish the rate of hearing loss, other neurologic complications and mortality
• May reduce the entry of vancomycin into the CSF (rifampin)
Allergy to beta-lactams
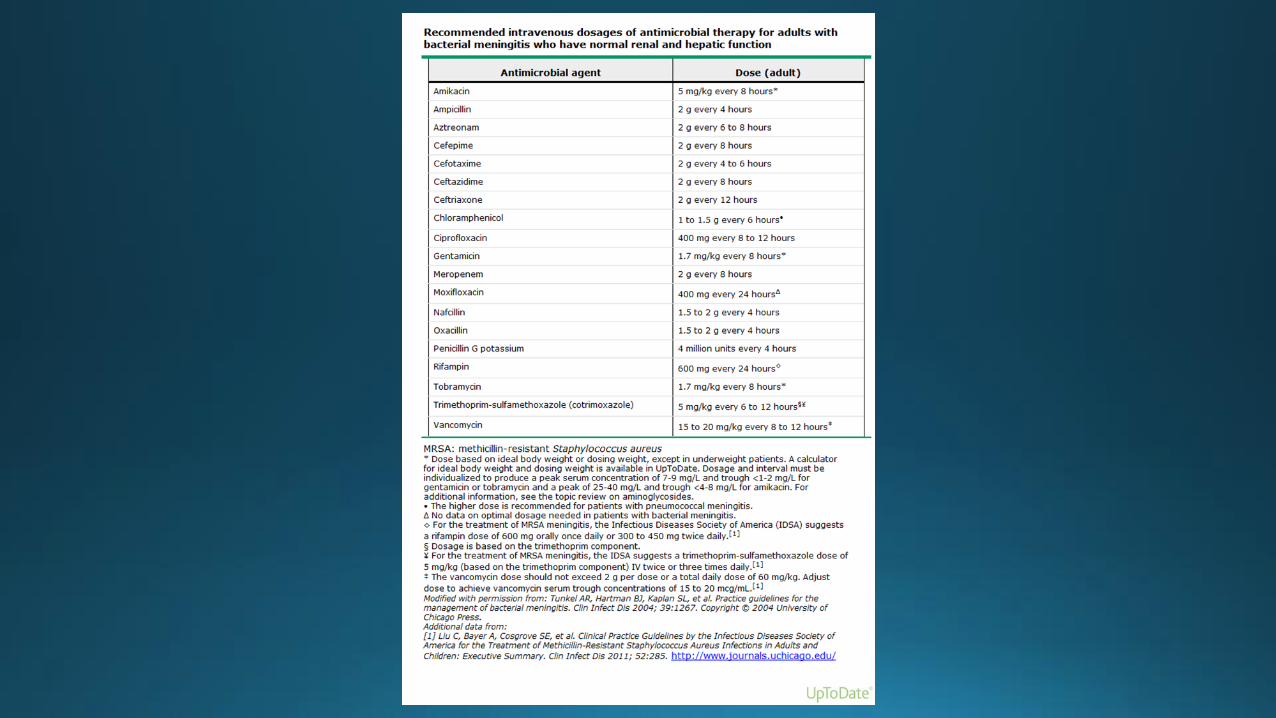
Vancomycin – 15-20 mg/kg IV q8-12 hours (max 2g/per dose, or a total daily dose 60 mg/kg; trough concentration 15-20 mcg/ml
+
Moxifloxacin – 400 mg IV qd
+
Trimethoprim-sulfamethoxazole – Listeria coverage- 5 mg/kg IV q 6-12 hrs
Supportive care
• Fluid management
• Reduction of intracranial pressure (insertion of ICP monitoring device)
• Lack of benefit of induced hypothermia
Repeat LP
• No evidence of improvement by 48 hours
• 2-3 days after the initiation of therapy (drug resistance)
• Persistent fever for more than eight days without another explanation
Prognosis Mortality: 16.4-22.7
Neurologic complications:
• Impaired mental status
• Increased ICP and cerebral edema
• Seizures
• Focal neurologic deficit (CV palsy, hemiparesis)
• Cerebrovascular abnormalities
• Sensorineural hearing loss
• Intellectual impairment
Prediction of risk (hypotension, altered mental status and seizure):
• Low risk (no clinical risk factors) – 9% adverse outcome
• Intermediate risk (one clinical risk factor) – 33%
• High risk (two or three risk factors) – 56%
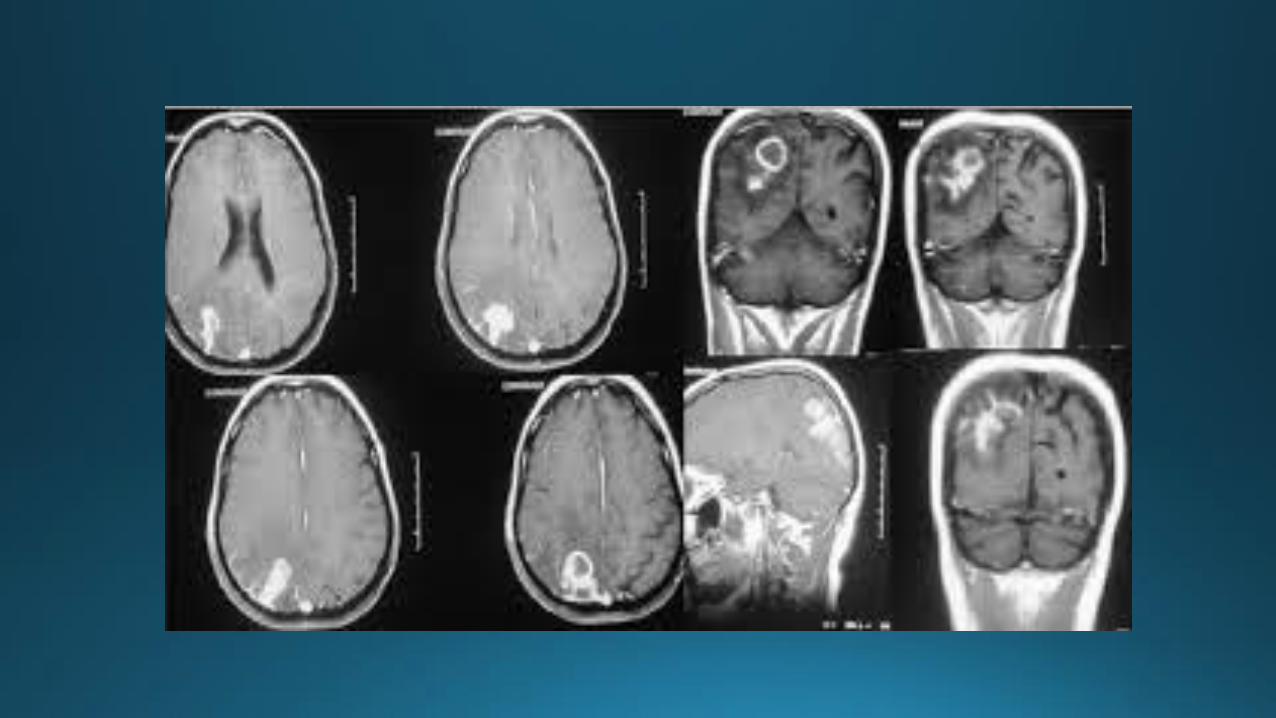
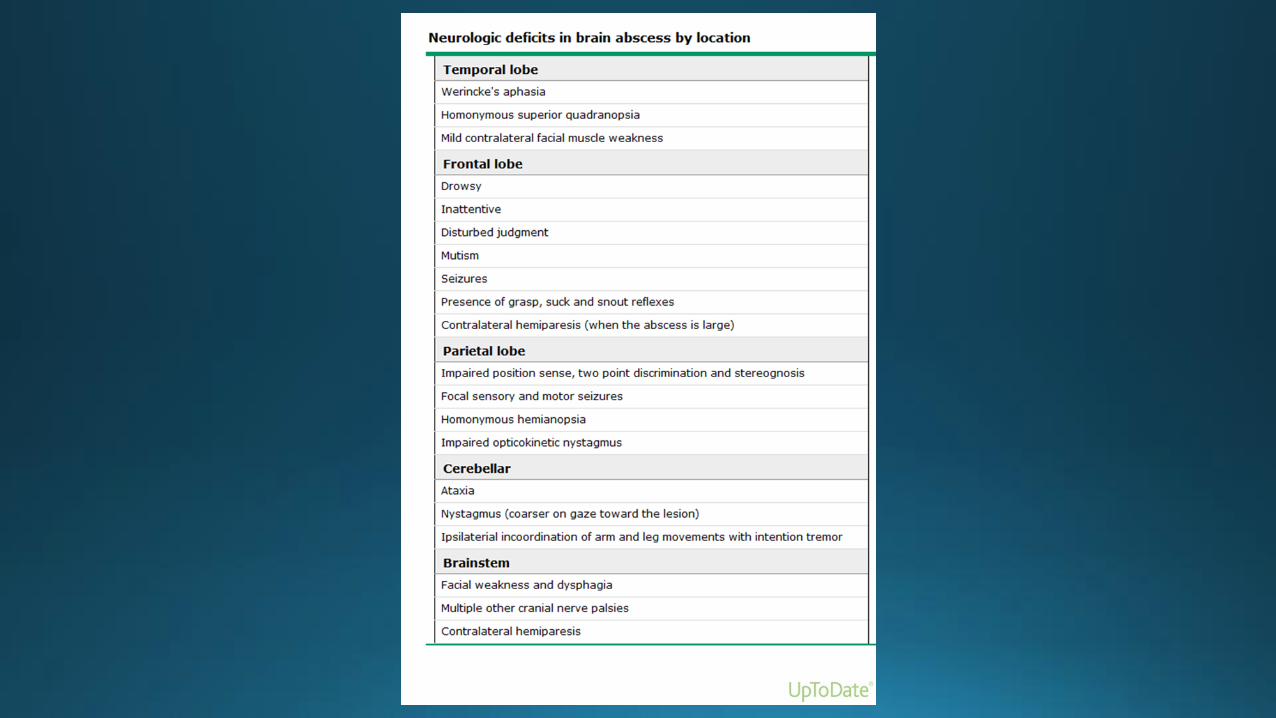
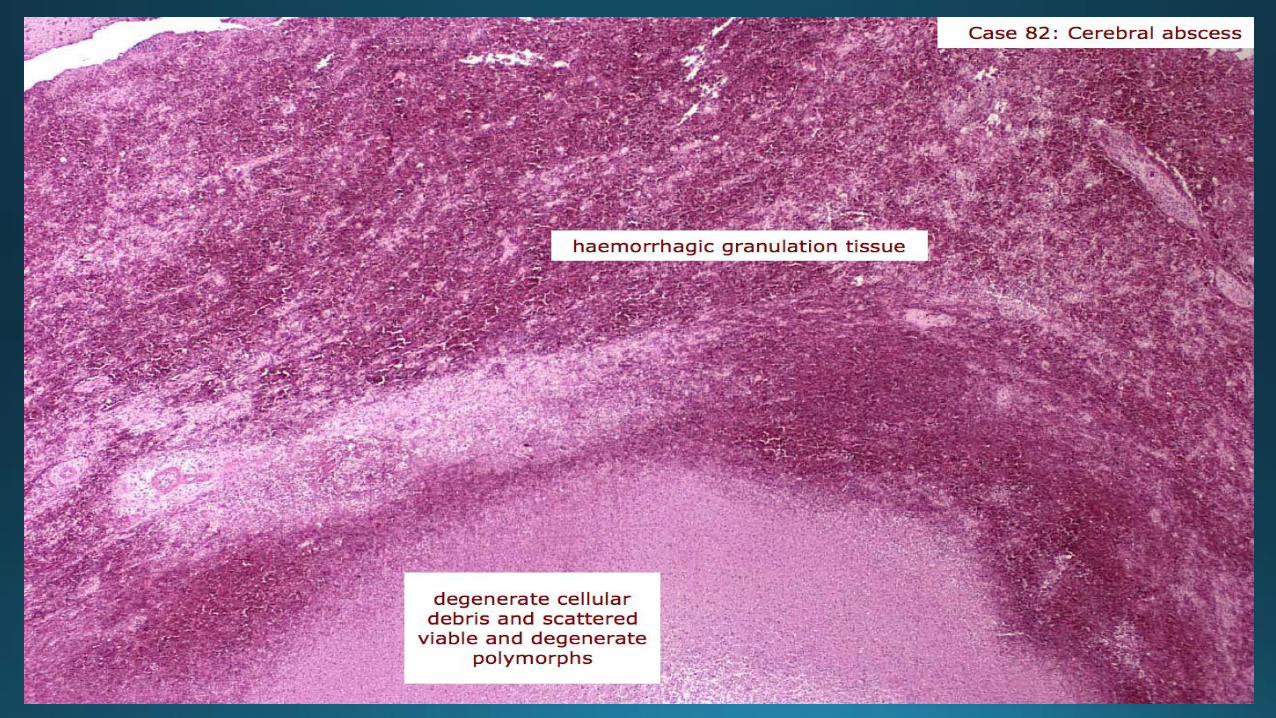
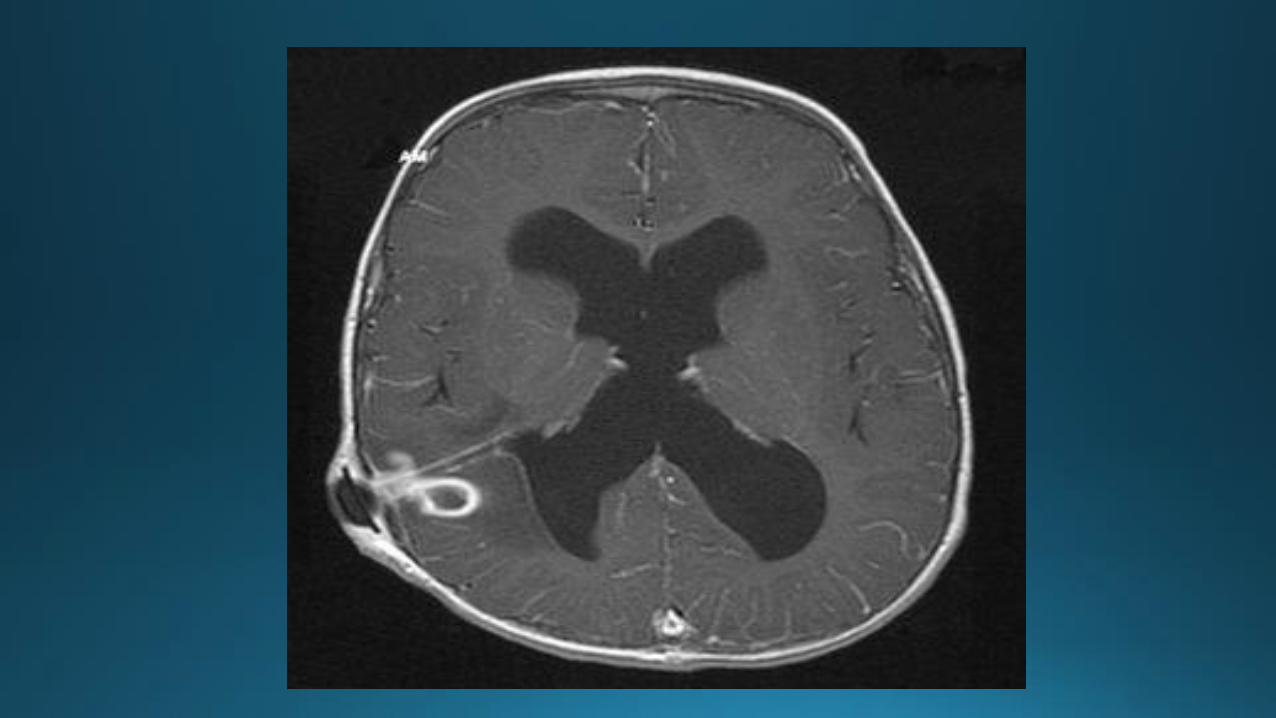
Brain abscess
• Focal collection within the brain parenchyma, which can arise as a complication of a variety of infections, trauma or surgery.
Pathogenesis
Direct spread (20-60%) :
• Subacute and chronic otitis media, mastoiditis (inferior temporal lobe, cerebellum)
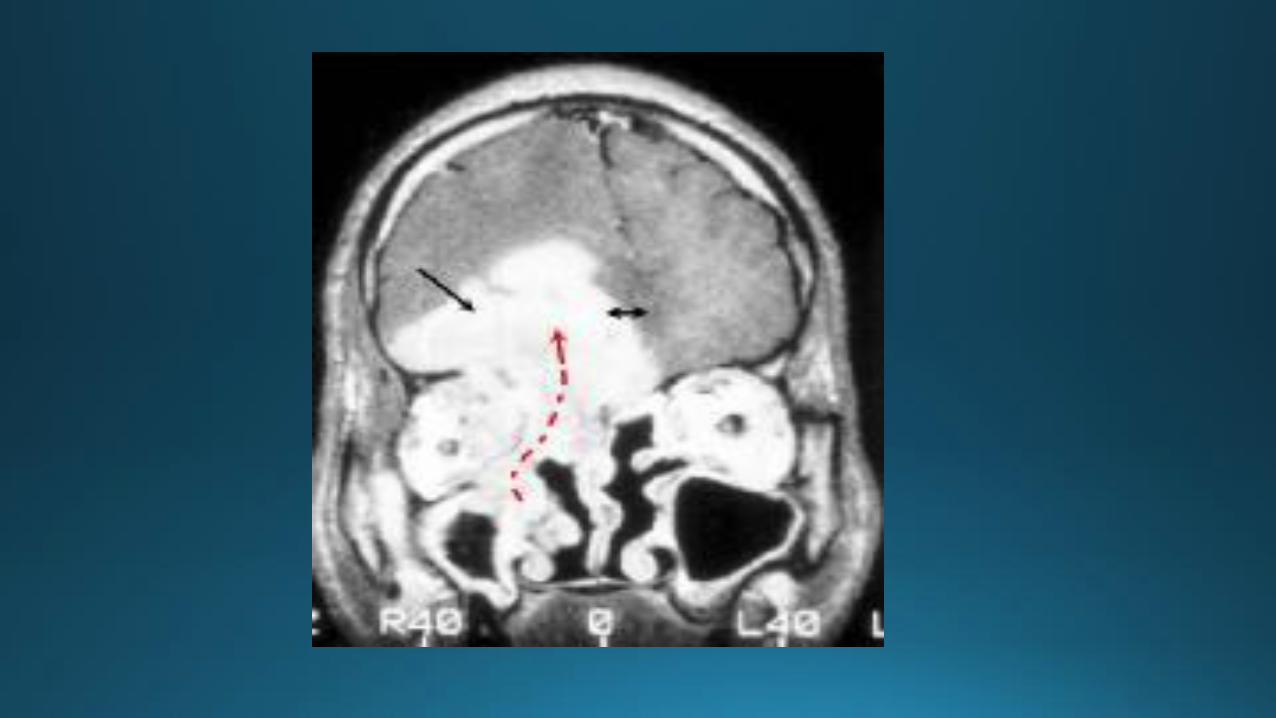
• Frontal or ethmoid sinuses (frontal lobes)
• Dental infection (frontal lobes)
• Bullet wounds
• Facial trauma
• Neurosurgical procedures
Pathogenesis
Hematogenous spread: • Multiple abscesses (MCA distribution, grey-white matter junction) • Chronic pulmonary infections • Skin infections • Pelvic infections • Intraabdominal infections • Bacterial endocarditis (2-4%) • Cyanotic congenital heart diseases • Intrapulmonary right-to-left shunting with pulmonary AVMs No primary site/underlying condition identified in 20-40%
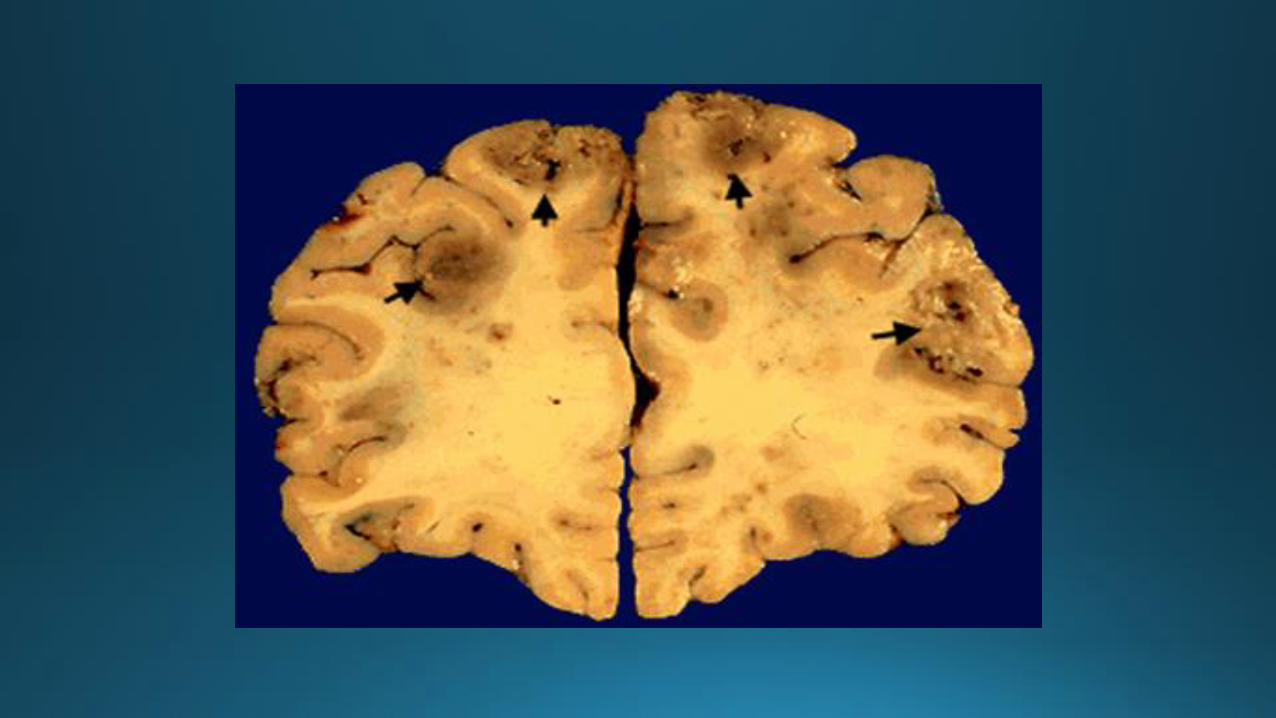
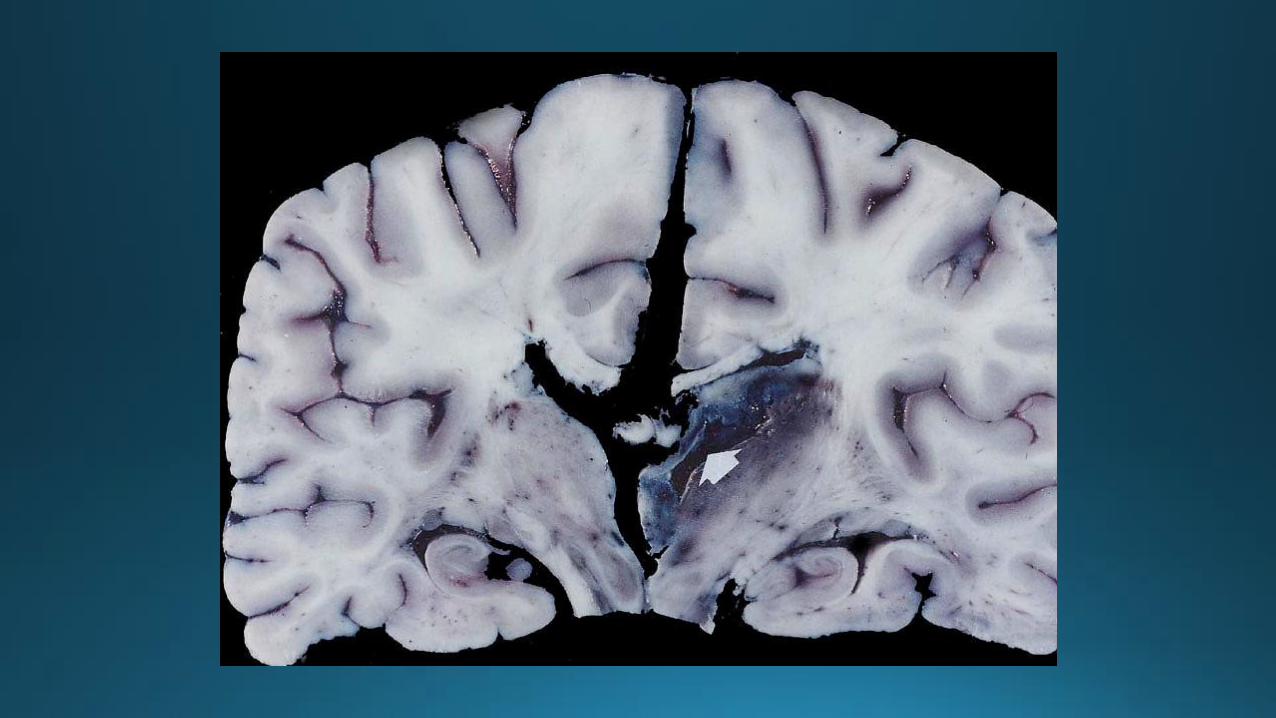
Pathology
• Early lesion (first two weeks) – poorly demarcated, edema, no tissue necrosis- cerebritis
• > two weeks – necrosis, liquefaction, fibrotic capsule
Clinical manifestation
• Initially nonspecific
• Diagnosis made at mean 13-14 days after the onset of symptoms
• Headache
• Neck stiffness (15%)
• Fever (45-50%)
• Seizures (25%)
• 3rd and 6th nerve palsies (>ICP)
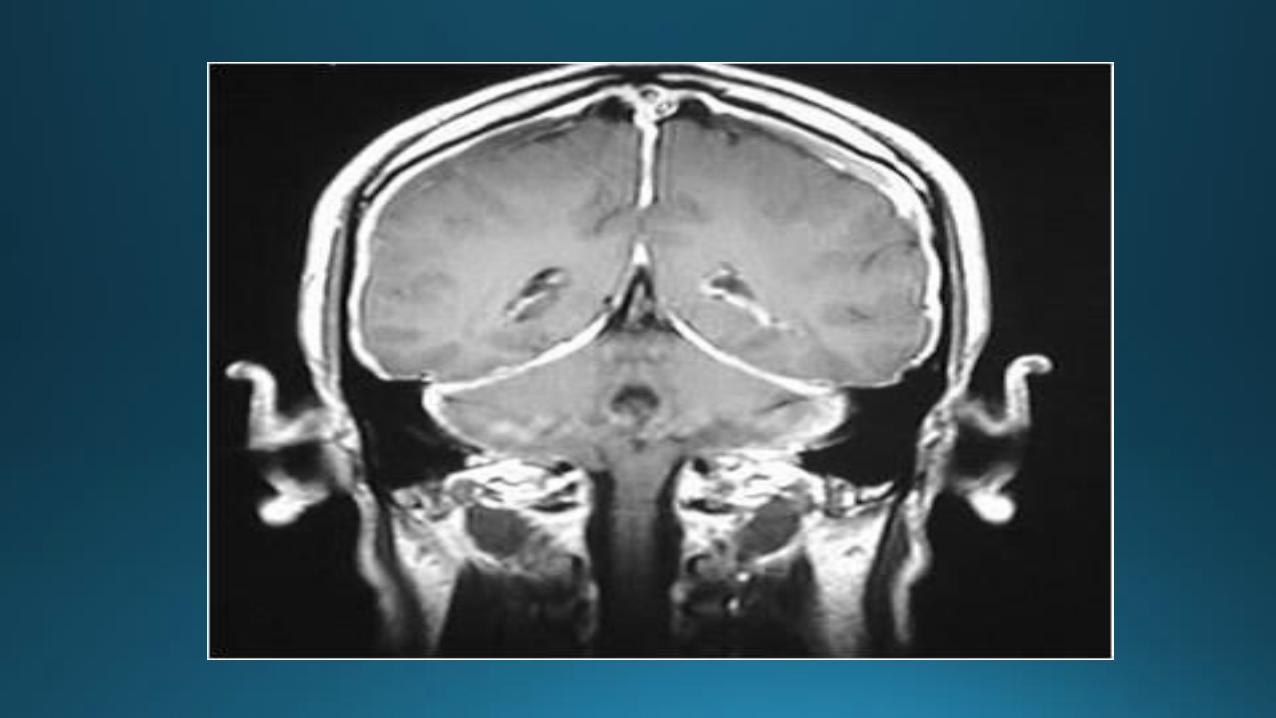
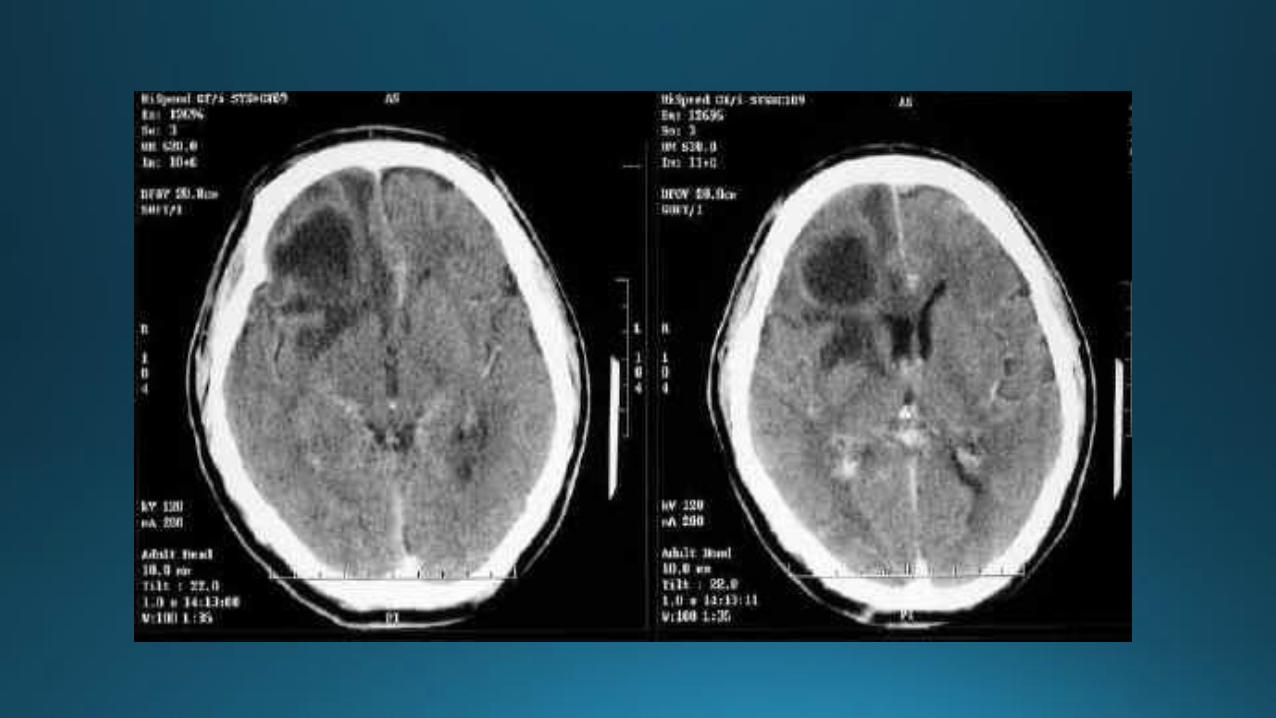
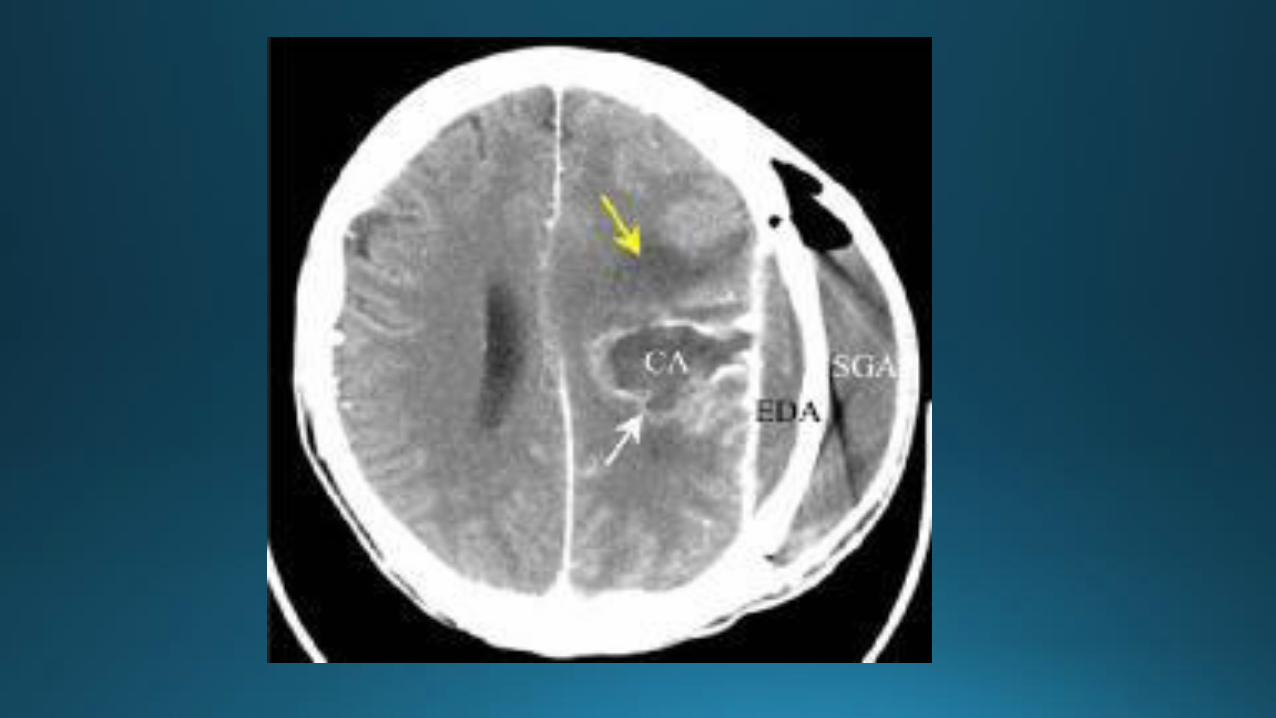
Diagnosis
• Neuroimaging (CT, MRI)
• LP (contraindicated in patients with focal symptoms and signs)
• Culture (stereotactic biopsy specimen)
• Serology (anti-toxoplasma immunoglobulin G in blood, anticysticercal Ab in CSF)
• Histopathology
• 16S ribosomal sequencing


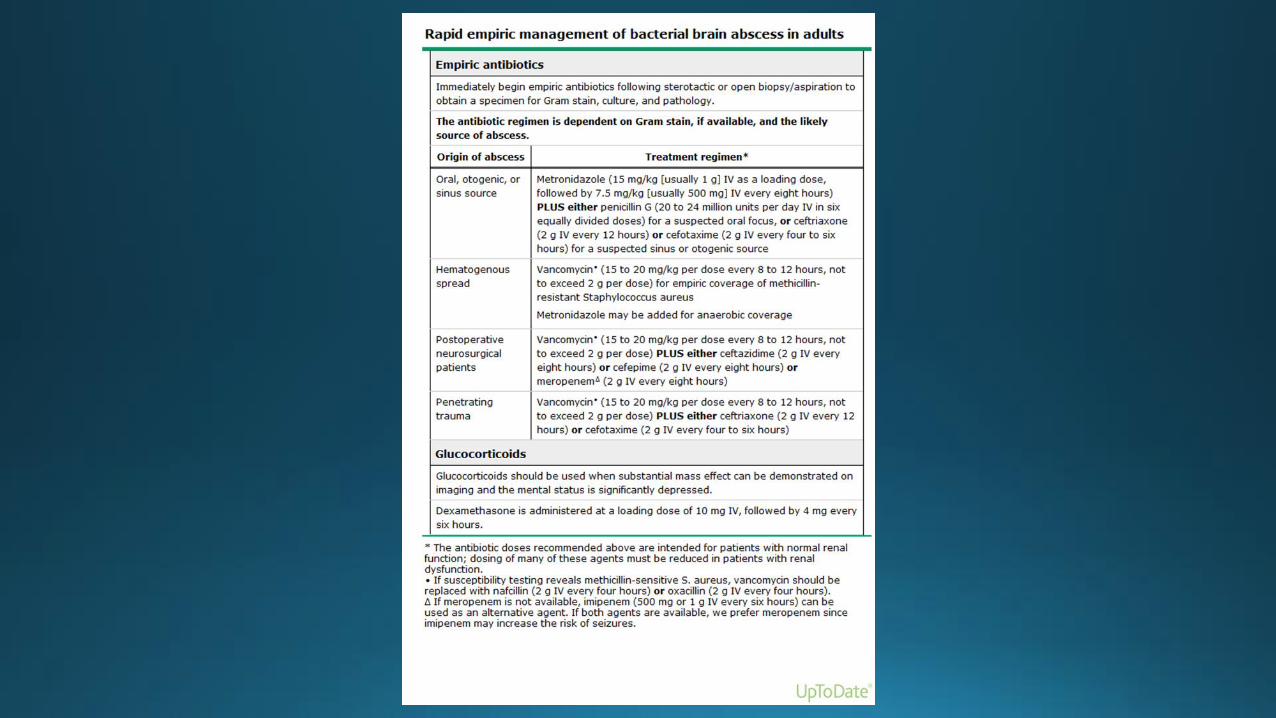
Therapy
Antibiotics:
• Empiric therapy
• Subsequent treatment
Surgery:
• Aspiration (preferred)
• Surgical excision (traumatic, fungal, multiloculated)
Glucocorticoids
• To treat mass effect (Dexamethasone load 10 mg IV, followed 4 mg q6 hours
• Disadvantages: reduction in contrast enhancement on CT, slowing of capsule formation, increased risk of ventricular rupture, decreasing the penetration of antibiotics into the abscess
Prognosis and outcome
• Mortality: 0-30%
Poor prognostic factors:
• Rapid progression of the infection before hospitalization
• Severe mental status changes on admission
• Stupor or coma (60-100% mortality)
• Rupture into the ventricle (80-100% mortality)
Neurologic sequelae:
• Seizures (30-60%)- >frontal lobe

ACUTE VIRAL ENCEPHALITIS
Meningitis versus Encephalitis
• Presence or absence of normal brain function
Meningitis
• Uncomfortable, lethargic, distracted by headache, but cerebral functions remain normal
Encephalitis
• Abnormalities in brain function, altered mental status, motor or sensory deficit, altered behavior, personality changes, speech or movement disorders, hemiparesis.
Seizures and postictal state can be seen with meningitis alone.
Viral versus postinfectious encephalitis
Viral:
• Viral invasion of the CNS, neuronal involvement, cultures
Postinfectious (acute disseminated encephalomyelitis-ADEM)
• Virus cannot be detected, neurons are spared. Perivascular inflammation and demyelination.
• Typically difficult to differentiate
• Measles, varicella, rubella CAN PRODUCE EITHER SYNDROME
Viral pathogens
• Most viruses can produce either meningitis or encephalitis
• Mumps, measles, varicella-zoster virus, rubella, influenza-postinfectious encephalitis
• Geographic location (St Louis, Japanese)
• Epidemiologic (bat exposure, dog bite-rabies)
• Clinical clues: profound weakness and rash-West Nile
• Uncommon: VZV, Epstein-Barr, HIV, human herpes virus-6
Historical clues
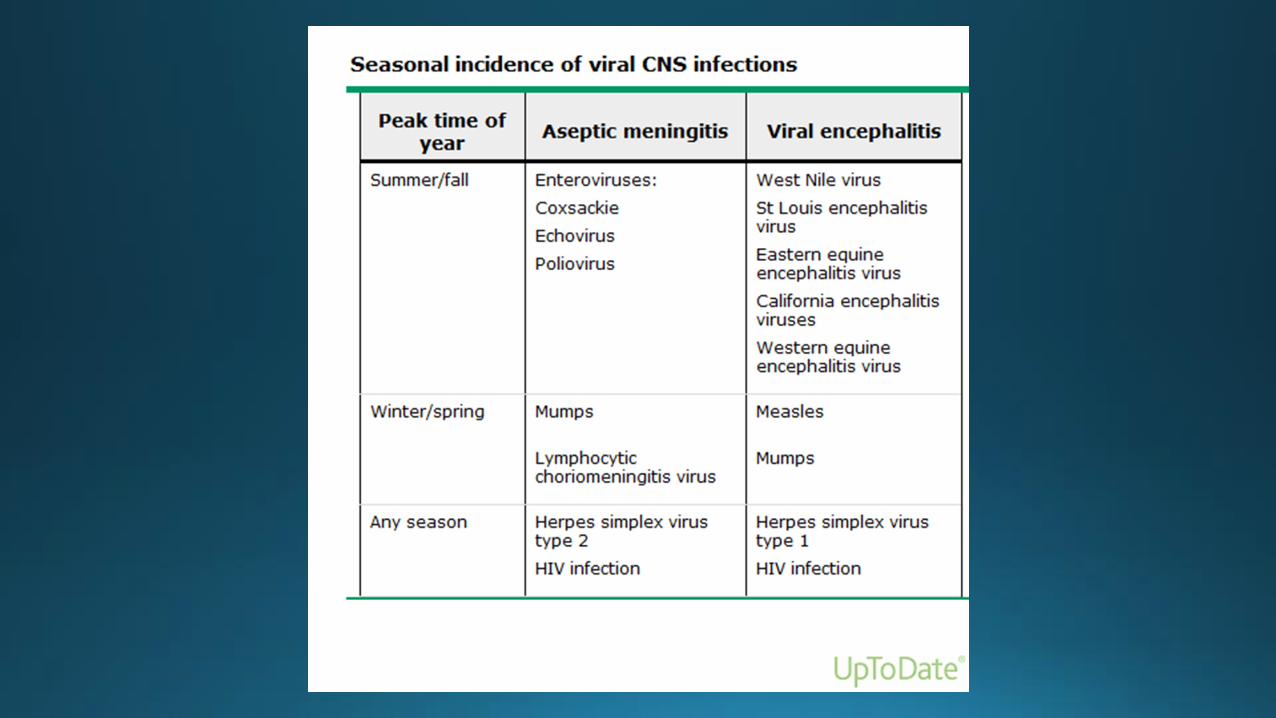
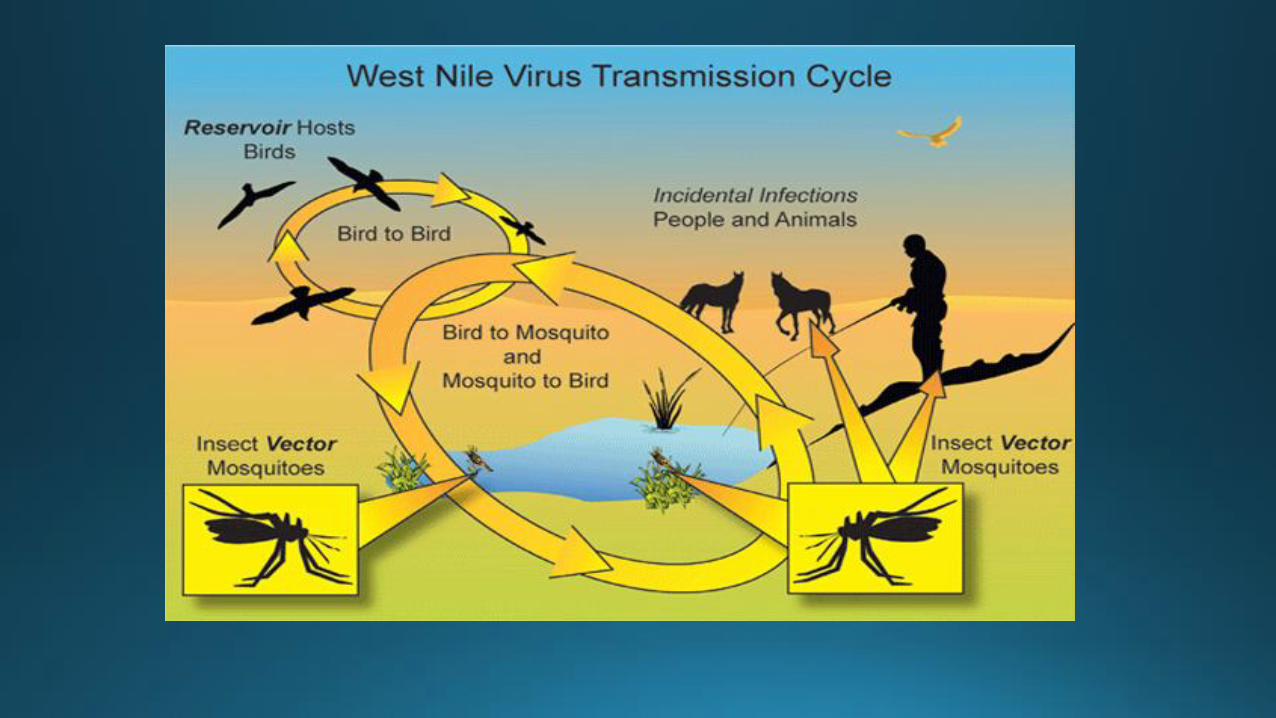
• Arboviruses (eastern equine, western equine, St. Louis, Venezuelan equine, West Nile) – when mosquitoes are active
• Herpes simplex virus – any time
• Viral encephalitides (walking in woods/high tick populations)- Colorado tick fever, non viral (Lyme disease, Rocky Mountain spotted fever)
• Prior to 1999 arboviruses were infrequent, WNV encephalitis
• Geography and animal exposure (Nipah-Malaysia, pigs and bats), Avian influenza (Vietnam), Lymphocytic choriomeningitis virus- rodent borne arenavirus
Clinical manifestation
• Altered mental status
• Meningeal irritation-usually absent with a pure encephalitis, present with meningoencephalitis
• Seizures-common
• Focal neurologic abnormalities
• Clinical presentation is generally nonspecific (fever, headache, nausea/vomiting, occasionally photophobia and neck stiffness)
Clues on physical examination
• Parotitis – mumps encephalitis (unvaccinated patient)
• Flaccid paralysis – West Nile (misdiagnosed wit GBS), maculopapular rash-50%
• Tremors of the eyelids, tongue, lips and extremities – St. Louis, WN
• Hydrophobia, aerophobia, pharyngeal spasms, hyperactivity – rabies
• Grouped vesicles in a dermatomal pattern – VZV; the absence of rash does not eliminate VZV
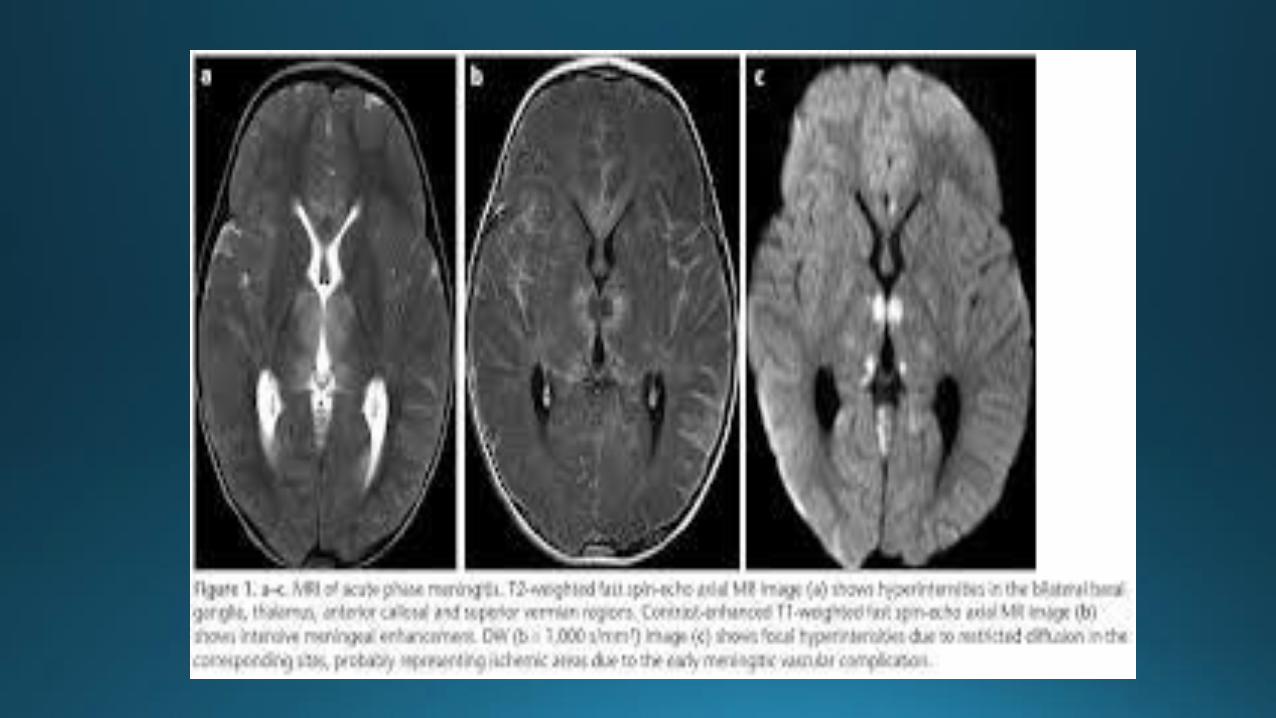
Imaging
May or may not demonstrate abnormal CT or MRI
• Temporal lobe – HSV encephalitis; VZV, EBV, HHV-6
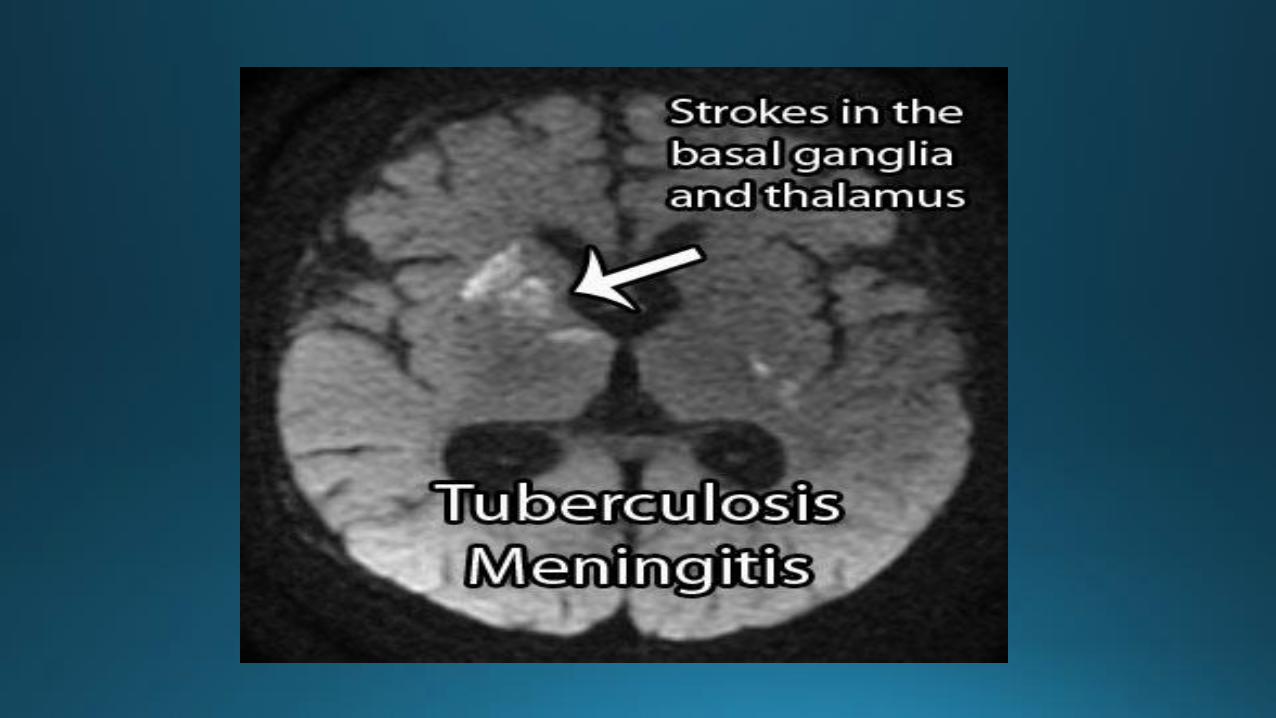
• Thalamus/basal ganglia – respiratory viral infection, CJD, arbovirus, tuberculosis
• Variety of abnormalities – basal ganglia, thalami, mesial TL, brainstem, cerebellum –WN infection
• Hydrocephalus – may suggest nonviral etiologies (bacterial, fungal, parasitic agents)
Electroencephalography – often abnormal in acute encephalitis; temporal lobe-HSV
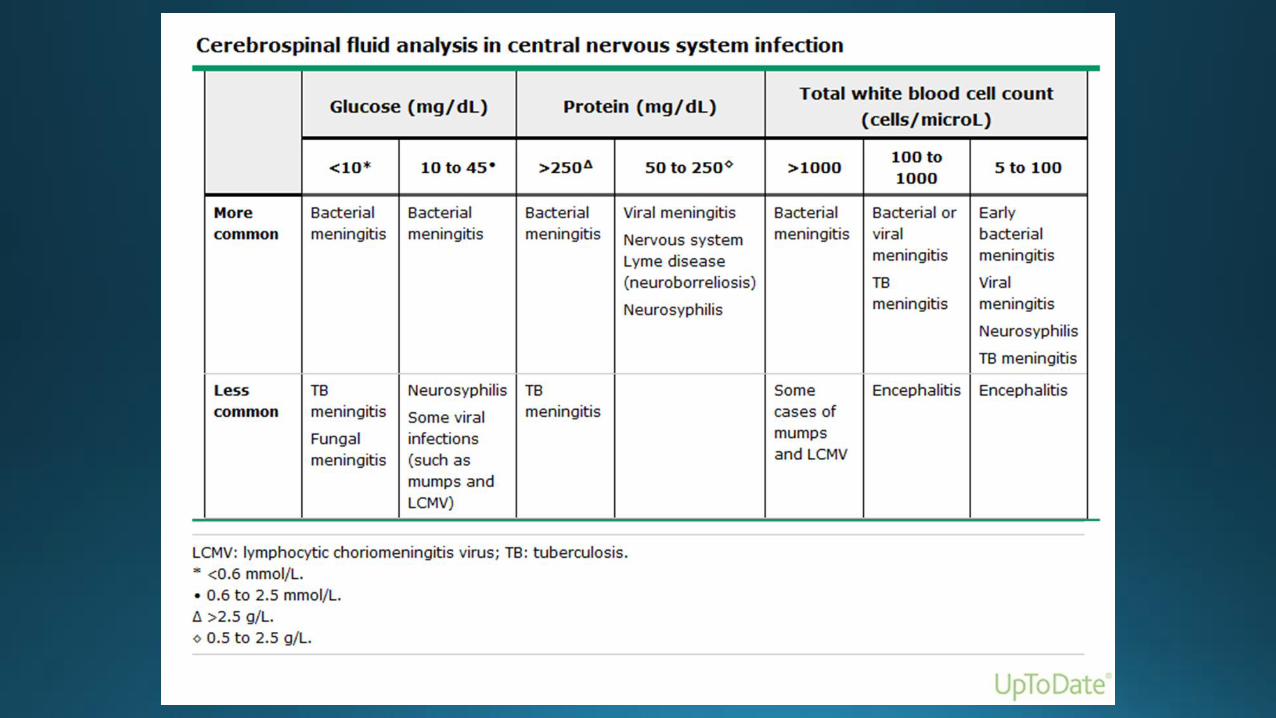
Cerebrospinal fluid findings
• Not diagnostic, confirms the presence of inflammation
• Leukocytosis, <250 cells (lymphocytic predominance; early > neutrophils)
• Elevated protein, <150 mg/dl
• Normal glucose
• Moderate decreased glucose (occasionally with HSV, mumps, enteroviruses)
• Red cell usually absent (except HSV-1 or other necrotizing encephalitis)
Diagnosis
• CSF analysis
• Viral culture (6% positive)
• Polymerase chain reaction (HSV-1, HSV-2, enteroviruses, VZV, CMV)
• Serology (WN IgM, St. Louis)
• Brain biopsy- as a last resort
• Definitive diagnosis (varies: 9-45%)

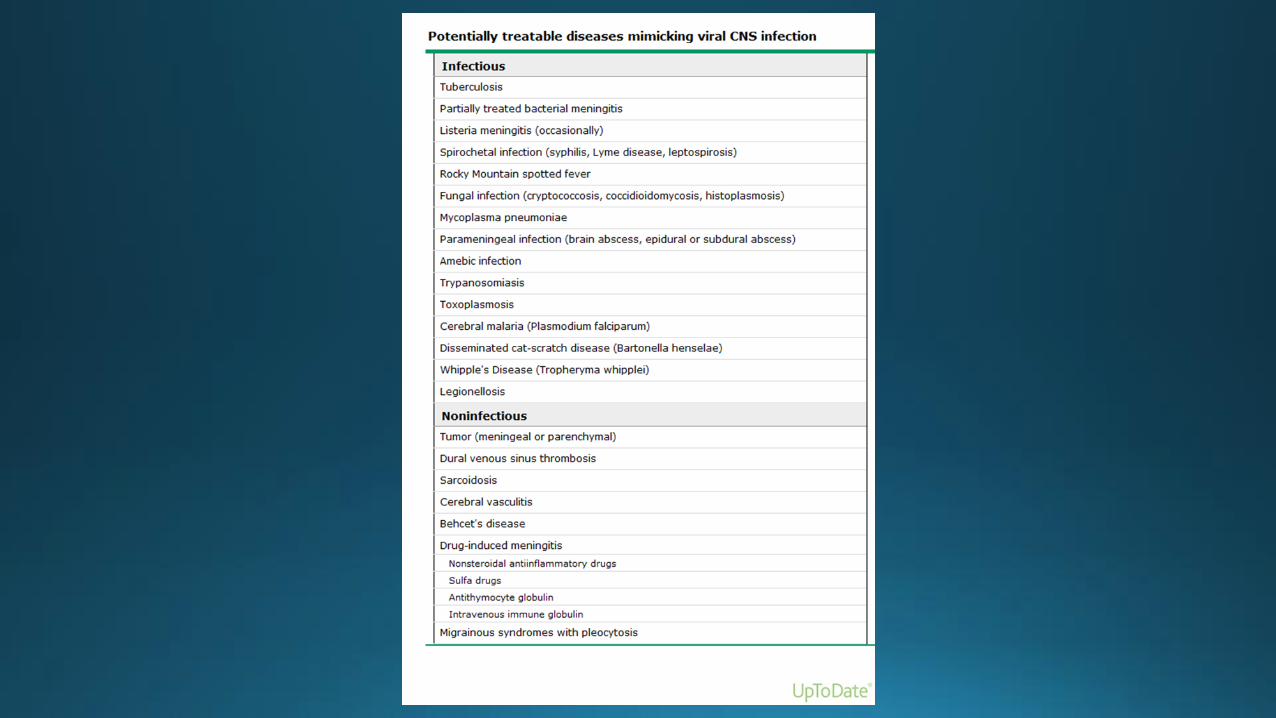
Differential diagnosis
• Intracranial tumors • Collagen vascular disorders • Vasculitis • Neoplastic disease • Adverse effects of medication • Brain abscess • Syphilis • Tuberculous meningitis • Fungal meningitis (coccidoides) • Toxoplasma, Cryptococcus (immunocompromised, AIDS)
Empiric therapy
HSV-1,HZV– acyclovir (10 mg/kg IV q8h)
Prognosis
HSV encephalitis-high mortality and morbidity
One year mortality -14%, epilepsy and neuropsychiatric sequelae-24% of surviving patients.
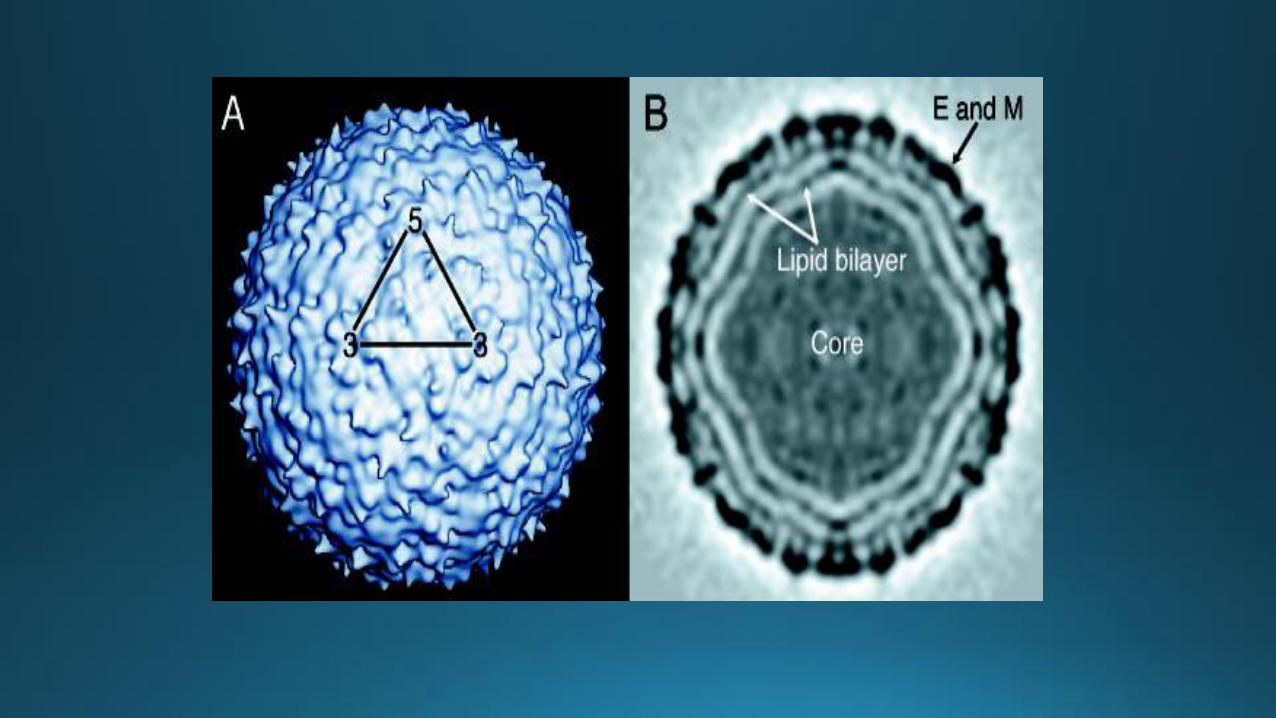
Clinical manifestations and diagnosis of West Nile virus infection • Member of Japanese encephalitis virus antigenic complex
• Wide range of clinical symptoms (asymptomatic to severe meningitis and encephalitis)

Clinical manifestation
• Most patients are asymptomatic
• Symptomatic: 20-40%
• Incubation- 2-14 days (longer in immunosuppressed)
• Immunity life long after infection
• Reinfection – very rare
West Nile fever
• Self-limited illness (indistinguishable from dengue fever or other viral grippes)
• Fever, headache, malaise, back pain, myalgia, anorexia X3-6 days
• Some patients very low grade or no fever
• Eye pain, pharyngitis, nausea, vomiting, diarrhea, abdominal pain
• Rash – 25-50%; associated with <risk of neuroinvasive disease and death. Maculopapular, chest, back and arms
• Acute symptoms- 3-10 days; long recovery (median 60 days)
• Fatigue- most persistent symptom


Neuroinvasive disease
WN virus infection:
• Encephalitis >older age (mild to severe encephalopathy, coma and death)
• Meningitis > children
• Flaccid paralysis (asymmetric, can occur wo meningitis or encephalitis)
• Extrapyramidal symptoms – common
• Cranial nerve palsies
• Seizures
• Cerebellar ataxia
• Optic neuritis
Other clinical features
• Chorioretinitis “target-like”, retinal hemorrhages, vitritis
• Rhabdomyolysis
• Fatal hemorrhagic fever and multi-organ failure and palpable purpura
• Hepatitis and pancreatitis
• Central diabetes insipidus
• Myocarditis
• Myositis and orchitis
Laboratory findings
• WBC-normal or elevated
• CSF-pleocytosis, >lymphocytes, elevated protein, normal glucose
• Neutrophilic predominance in meningitis (45%) and encephalitis(37%)
• 5% of meningitis – normal CSF studies
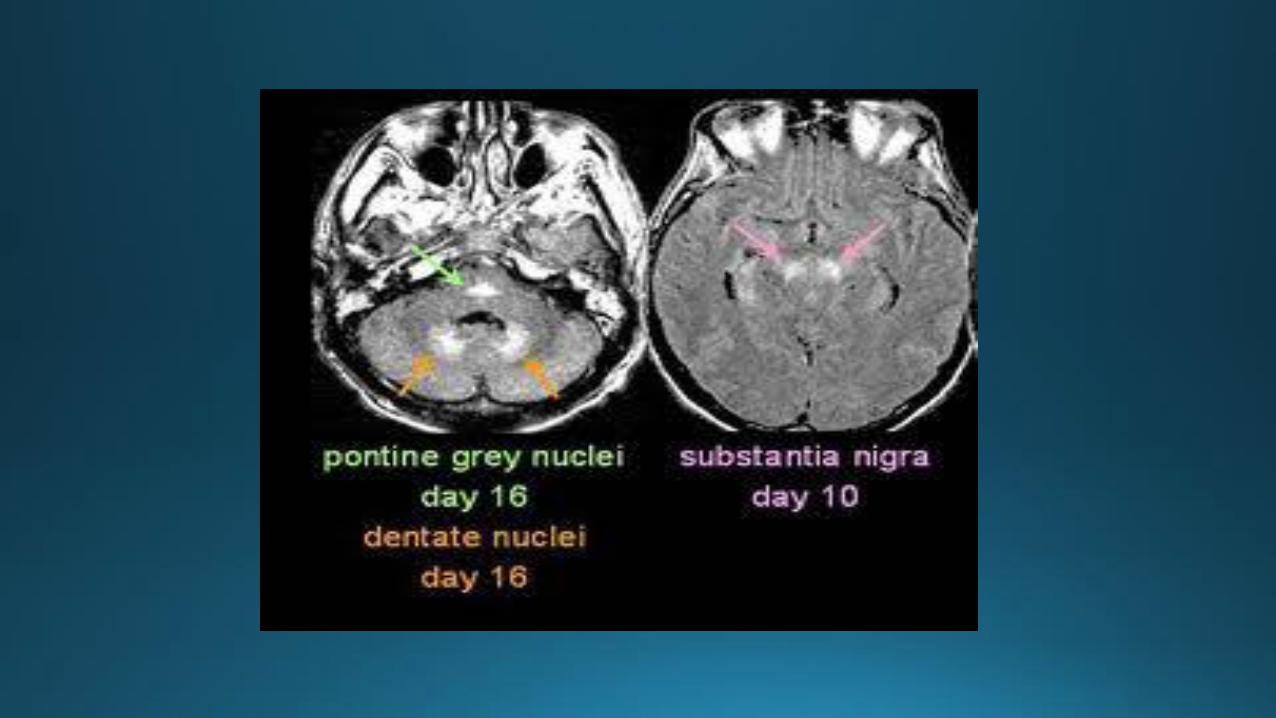
Imaging
• CT- no evidence of acute disease
• MRI – abnormal is not uncommon

Diagnosis
• Unexplained febrile illness, encephalitis/meningitis
• The median time from RNA detection to IgM seroconversion was 3.9 days; to IgG seroconversion 7.7 days
• The mean time before RNA levels became undetectable was 13.2 days
• The mean time to IgM negativity was 156 days
• Serologic testing- MAC-ELISA for IgM
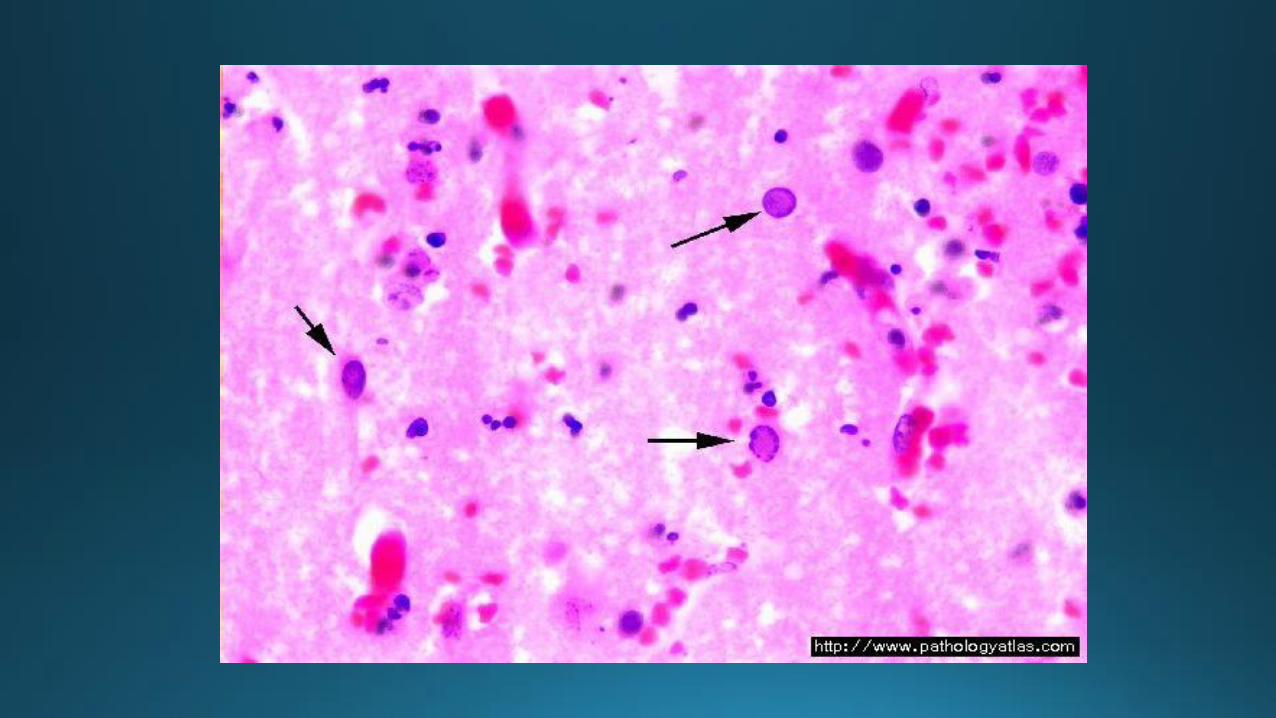
Herpes simplex type 1 encephalitis
• The most common cause of sporadic fatal encephalitis worldwide
• Rapid onset of fever, headache, seizures, focal neurologic signs and impaired consciousness
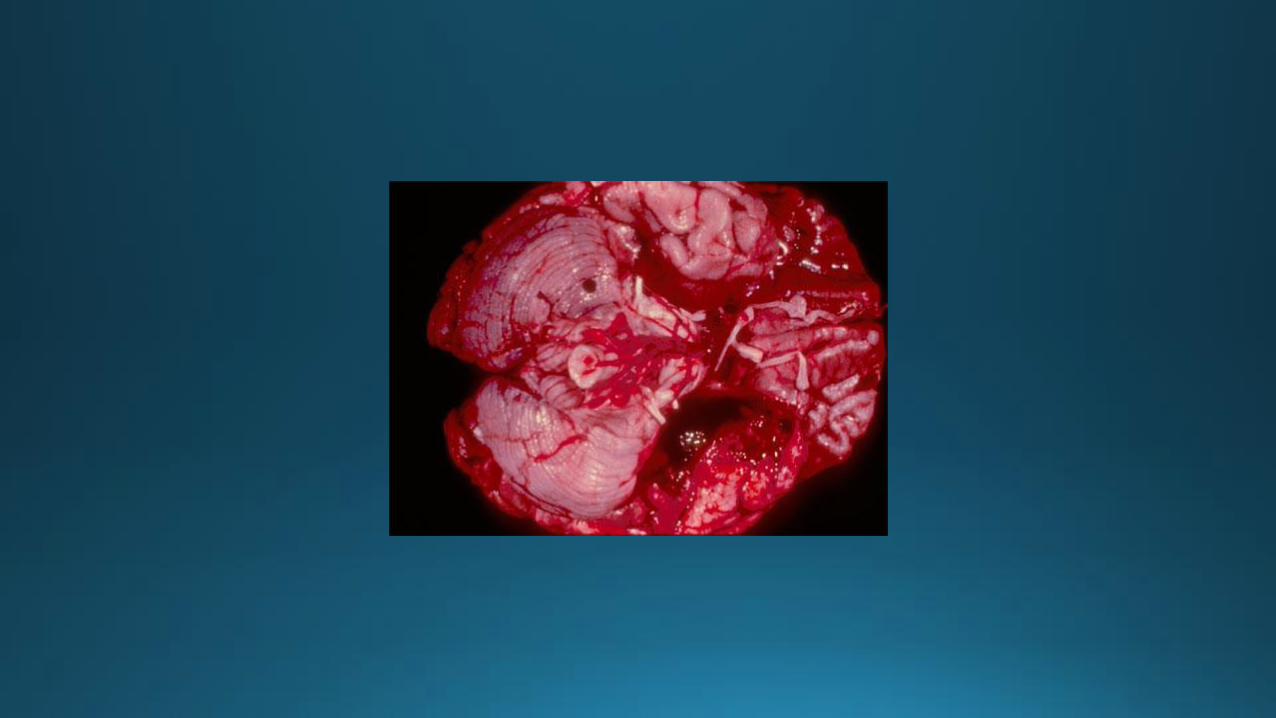
• Devastating disease with >morbidity and mortality
• 10-20% of all viral encephalitic cases in the USA (20,ooo)
• 1/3 children
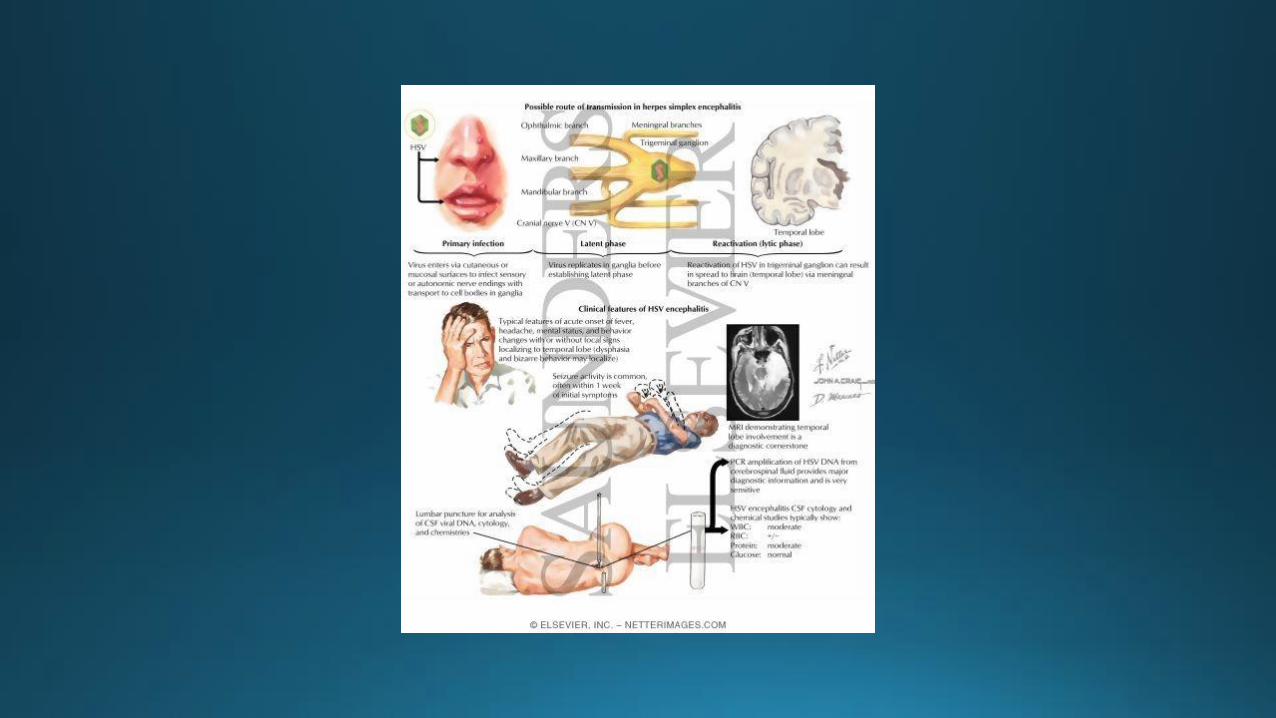
Routes of infection
• Immediate CNS infection: trigeminal nerve or olfactory tract following an episode of primary HSV-1 (<18 years old)
• After an episode of recurrent HSV-1 infection (viral reactivation)
• CNS infection wo primary or recurrent HSV-1 infection (latent HSV in situ within the CNS)
Host susceptibility: toll like receptors (TLRs)
Tissue injury – immune mediated.
Clinical features
• Acute neurologic findings (<1 week in duration)
• Altered mentation and level of consciousness
• CN deficits
• Hemiparesis
• Aphasia, dysarthria
• Focal seizures
• Fever
Various behavioral syndromes associated with HSV-1 encephalitis: Hypomania, Kluver-Bucy syndrome, varying states of amnesia
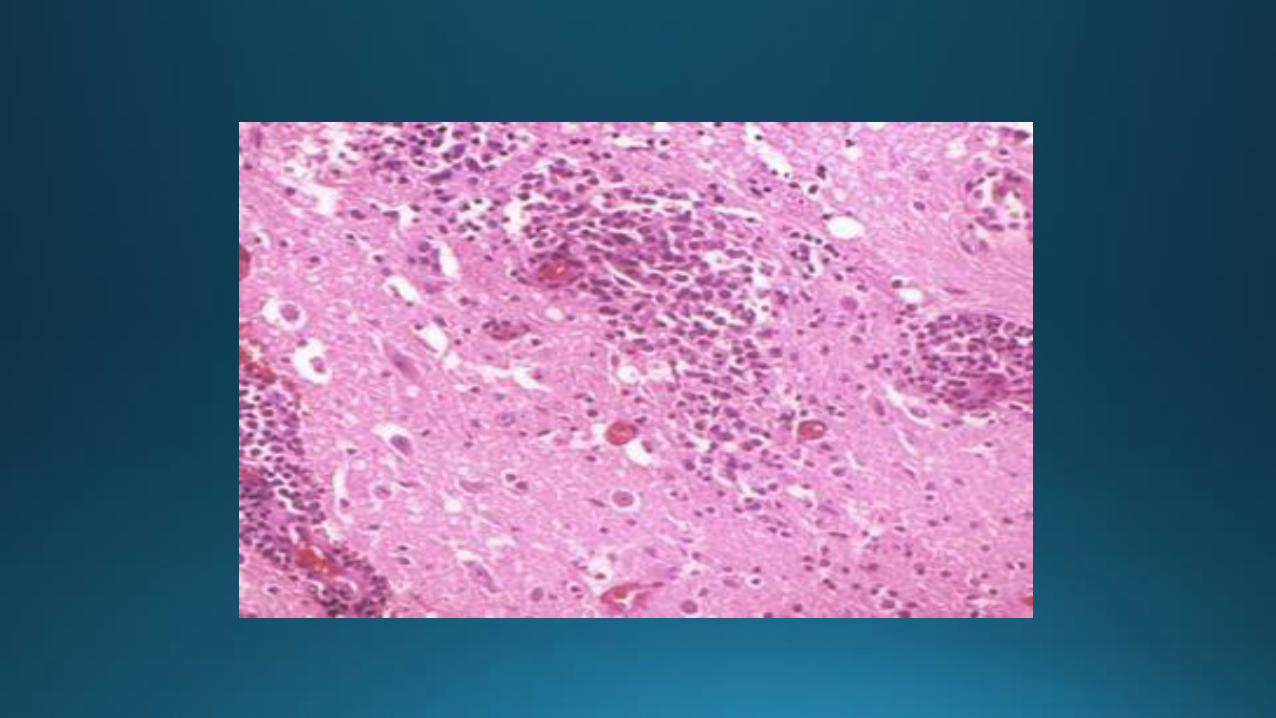
Laboratory abnormalities
• CSF: lymphocytic pleocytosis, >RBC (84%), >protein
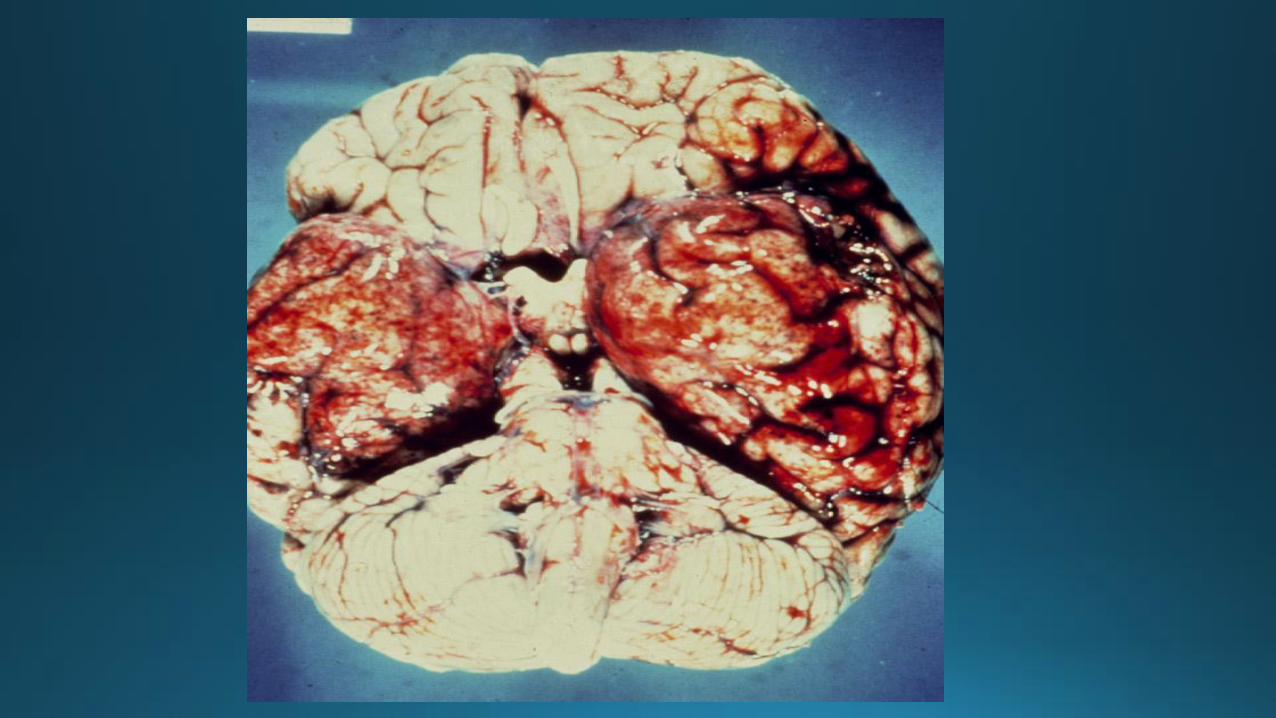
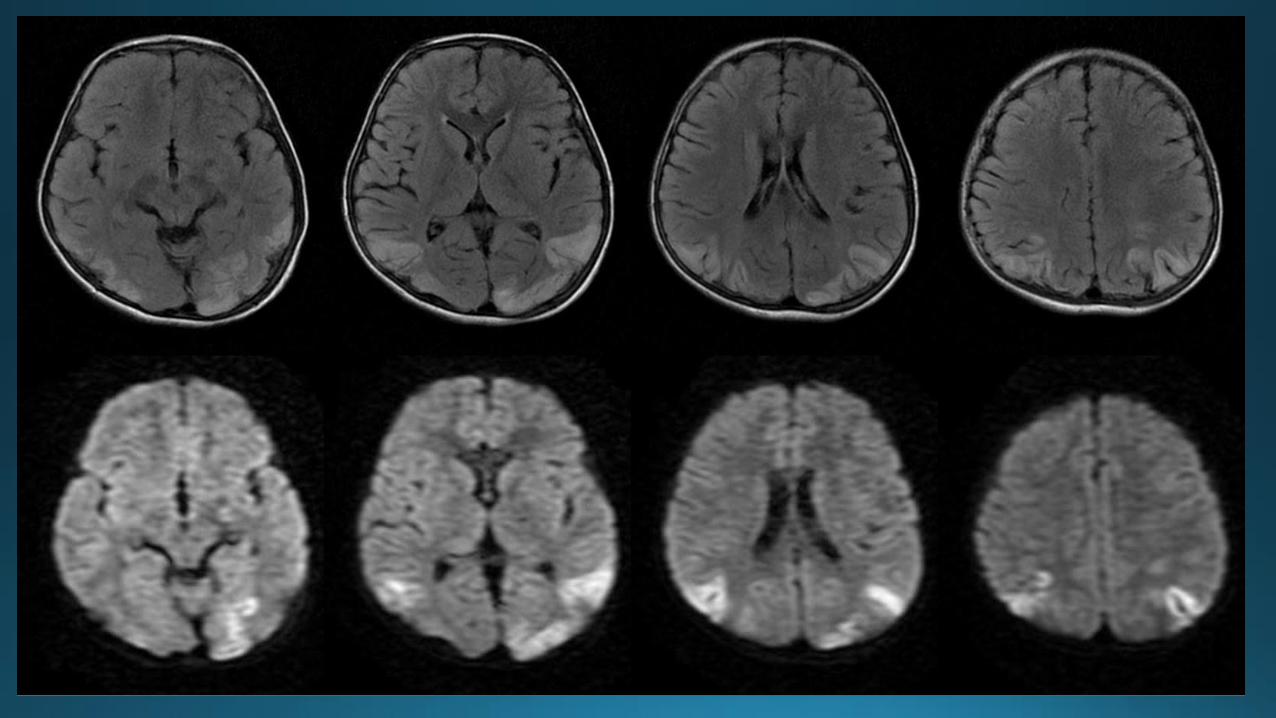
Imaging studies
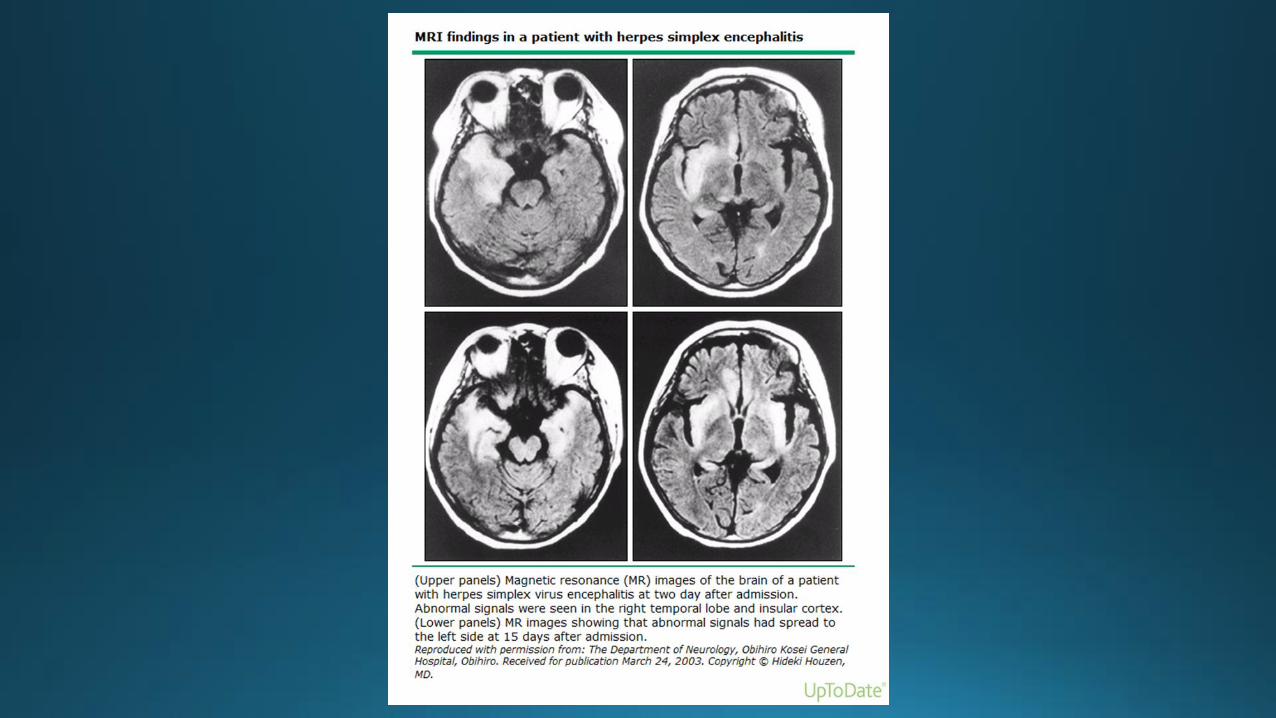
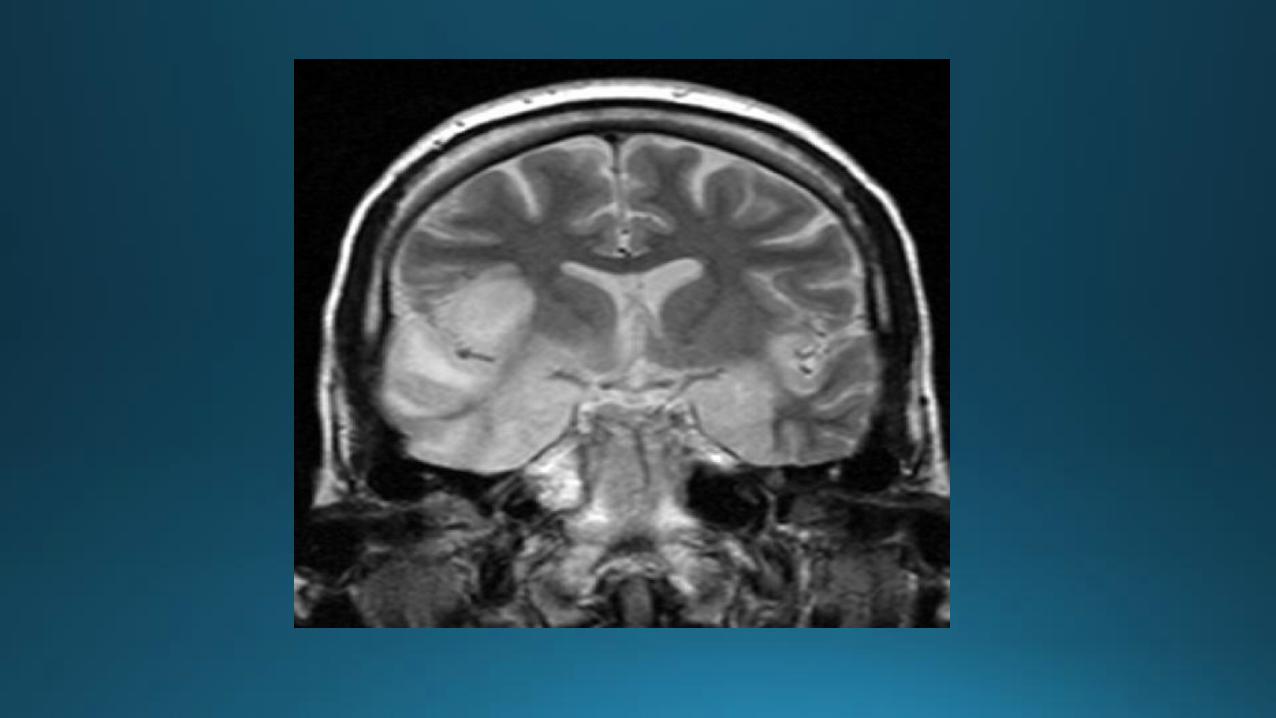
• Temporal lobe – predominately unilateral, mass effect
• Extratemporal – up to 55%
• CT – only 50% sensitivity
EEG- focal findings in >80%

Differential diagnosis
• Other viral etiologies (WN, ST. Louis, Western/Eastern equine encephalitis), other herpesviruses (CMV, EBV, VZV)
• Brain abscess or subdural empyema • Post-infectious conditions (Reye syndrome) • ADEM • Subacute sclerosing panencephalitis • Neurosyphilis • Primary or secondary brain tumors • Paraneoplastic and autoimmune encephalitis • Other noninfectious causes: SDH, SLE, adrenal leukodystrophy,
vasculitis, Behcet, toxic encephalopathy
Diagnosis
• PCR – high sensitivity (98%), and specificity (94-100%)
• Brain biopsy
• CSF antigen and antibody determination – not helpful in the early diagnosis (viral antibody titers are firs positive after 10-14 days of illness)
• Viral culture
Treatment
Acyclovir- only effective in halting viral replication, it should be given early
Early treatment:
• Before loss of consciousness
• Within 24 hours of the onset of symptoms
• GCS 9-15
10 mg/kg IV q8h for 14-21 days (with dose adjustment for renal insufficiency)
DISCONTINUATION OF THERAPY BASED ON PCR RESULTS
• Patients with a low prior probability of HSV encephalitis (normal MRI, <5 WBC in CSF, normal mental status, negative CSF HSV PCR: < 1%. Stop after 72 hours.
• High probability, negative PCR reduces the disease likelihood to 5%
Prognosis
• 70% mortality in untreated
• Most of the survivors have serious neurologic deficits
• 20-30% mortality with appropriate diagnosis and treatment