-
7/30/2019 4. CXR (2010 C1)
1/103
2
Abnormal Cases
Bone
Cardiovascular
Airspace Disease including Silhouette Sign
Interstitial Disease and Pulmonary Edema Atelectasis
Pulmonary Nodule
Pleura and Diaphragm
Mediastinal Mass
-
7/30/2019 4. CXR (2010 C1)
2/103
3
Bone and Soft Tissues
-
7/30/2019 4. CXR (2010 C1)
3/103
Fractures
4
-
7/30/2019 4. CXR (2010 C1)
4/103
5
Presenting CXR
-
7/30/2019 4. CXR (2010 C1)
5/103
6
-
7/30/2019 4. CXR (2010 C1)
6/103
7
MRI
Computed Tomography
Pancoast Tumour
-
7/30/2019 4. CXR (2010 C1)
7/103
8
Cardiovascular
-
7/30/2019 4. CXR (2010 C1)
8/103
9154 slides
Increased Cardiac Size: Can be
Cardiac or PericardialPericardial EffusionDilated
Cardiomyopathy
What imaging would you use to differentiate between the two
?9
-
7/30/2019 4. CXR (2010 C1)
9/103
10154 slides
Left Ventricular Enlargement
Enlargement of Left Ventricle
Left
Ventricle
IVC
10
-
7/30/2019 4. CXR (2010 C1)
10/103
-
7/30/2019 4. CXR (2010 C1)
11/103
Pulmonary embolism
-
7/30/2019 4. CXR (2010 C1)
12/103
Pulmonary embolism
-
7/30/2019 4. CXR (2010 C1)
13/103
Airspace Disease and Silhouette
Sign
14
-
7/30/2019 4. CXR (2010 C1)
14/103
15
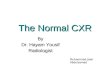
Normallung
Individual alveoli are
too small to resolve,
but together they
appear radiolucent.
-
7/30/2019 4. CXR (2010 C1)
15/103
16
Air-space Disease
Filling of alveoli by: water, blood,
pus, proteinaceous fluid, or cells
-opacities
-consolidation
-
7/30/2019 4. CXR (2010 C1)
16/103
Air-space pattern of lung disease 17
-
7/30/2019 4. CXR (2010 C1)
17/103
18
Airspace Disease
Filling in of acini (air space)
Air space (acinar) nodules
Coalesce to consolidation
Air bronchograms
Silhouette Sign
-
7/30/2019 4. CXR (2010 C1)
18/103
19
Air Space Disease: Etiology
Water-Pulmonary Edema
Pus-Infections, Non-infectious
inflammatory process
Blood-Pulmonary Hemmorhage Protein-Alveolar Proteinosis
Tumour-BAC, Lymphoma
-
7/30/2019 4. CXR (2010 C1)
19/103
22
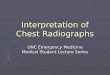
Air Bronchogram
Airways are not normally seen in a normalchest radiograph
because they are an air
structure within an aerated lung
When the aerated lung opacify, the bronchiibecome visualized
because of the
surrounding contrast effect.
-
7/30/2019 4. CXR (2010 C1)
20/103
23154 slides
airbronch
23
-
7/30/2019 4. CXR (2010 C1)
21/103
24
-
7/30/2019 4. CXR (2010 C1)
22/103
25CT Consolidation: Air Bronchograms
-
7/30/2019 4. CXR (2010 C1)
23/103
26
Silhouette Sign Definition: The effacement of a normal
structure
Example: Airspace disease may silhouette: right heart margin
with right middle lobe pneumonia
diaphragm with lower lobe pneumonia
-
7/30/2019 4. CXR (2010 C1)
24/103
27
Silhouette sign
sign describes the observation that an
intrathoracic lesion will obliterate borders
of shadows of similar radiodense structuresthat it contacts
example: right middle lobe pneumonia will
obliterate apex of the right heart border
-
7/30/2019 4. CXR (2010 C1)
25/103
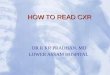
Silhouette sign
Normal
Pneumonia
(-) silhouette sign(visible heart silhouette)
Pneumonia
(+) silhouette sign
(no heart silhouette)28
-
7/30/2019 4. CXR (2010 C1)
26/103
Pulmonary edema+ silhouette sign
29
-
7/30/2019 4. CXR (2010 C1)
27/103
30
Pulmonary edema+ silhouette sign
Where is the Pneumonia?
-
7/30/2019 4. CXR (2010 C1)
28/103
31154 slides
Where is the Pneumonia?
31
-
7/30/2019 4. CXR (2010 C1)
29/103
32
-
7/30/2019 4. CXR (2010 C1)
30/103
33154 slides
Right Lower Lobe Pneumonia
Left
Right:
Partially seen 33
-
7/30/2019 4. CXR (2010 C1)
31/103
34154 slides
Left Lower Lobe Pneumonia
34
-
7/30/2019 4. CXR (2010 C1)
32/103
35154 slides
Where is the pneumonia?
35
-
7/30/2019 4. CXR (2010 C1)
33/103
36
-
7/30/2019 4. CXR (2010 C1)
34/103
37154 slides
Oblique(major)
fissure
Horizontal (minor fissure)
37
-
7/30/2019 4. CXR (2010 C1)
35/103
38154 slides
Right Middle Lobe Pneumonia
38
-
7/30/2019 4. CXR (2010 C1)
36/103
39
Interstitial Disease with Emphasis
on Pulmonary Edema
-
7/30/2019 4. CXR (2010 C1)
37/103
40
In a normal chest
radiograph, the visibleinterstitium is the
branching pulmonary
vessels
The branching
disappears peripherally
because they are beyond
resolution of the xray
-
7/30/2019 4. CXR (2010 C1)
38/103
41
Interstitial Disease
-
7/30/2019 4. CXR (2010 C1)
39/103
42
Hazy or ill defined interstitial lung disease
usually indicates acute disease
Sharp, well defined and distorted interstitiallung disease
usually indicates chronic
disease
Interstital dz appears as linear, nodular, orreticular
(net-like)
Interstitial Disease
Interstitial pattern of
-
7/30/2019 4. CXR (2010 C1)
40/103
43
Interstitial pattern of
lung disease
-
7/30/2019 4. CXR (2010 C1)
41/103
44154 slidesInterstitial Disease: Pulmonary Fibrosis 44
-
7/30/2019 4. CXR (2010 C1)
42/103
45
Interstitial Disease
Reticular=net-like
Nodular
Reticulonodular: Combination of the two
patterns
-
7/30/2019 4. CXR (2010 C1)
43/103
46154 slides
Reticular Pattern
46
Honeycombing in patient with single
-
7/30/2019 4. CXR (2010 C1)
44/103
47154 slides
Honeycombing in patient with single
lung transplant for pulmonary fibrosis
Normal Transplanted LungHoneycomb Native Lung 47
-
7/30/2019 4. CXR (2010 C1)
45/103
48154 slides
Miliary
Nodular Pattern: Miliary 48
-
7/30/2019 4. CXR (2010 C1)
46/103
55154 slides
cuffing
55
-
7/30/2019 4. CXR (2010 C1)
47/103
56Normal
-
7/30/2019 4. CXR (2010 C1)
48/103
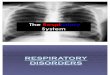
57
Kerley linesare a sign seen on CXRwith interstitial pulmonary
edema.
They are thin linear pulmonary opacities
caused by fluid or cellular infiltration
into the interstitium of the lungs
-
7/30/2019 4. CXR (2010 C1)
49/103
58
-
7/30/2019 4. CXR (2010 C1)
50/103
59154 slidesKerly B Lines 59
-
7/30/2019 4. CXR (2010 C1)
51/103
60154 slides
Edema kerly A
Pulmonary Edema
Minor fissure
60
Ed k l A
-
7/30/2019 4. CXR (2010 C1)
52/103
61154 slides
Edema kerly A
Septal Lines 61
-
7/30/2019 4. CXR (2010 C1)
53/103
-
7/30/2019 4. CXR (2010 C1)
54/103
63Kerley A
-
7/30/2019 4. CXR (2010 C1)
55/103
Other Lung Diseases
64
-
7/30/2019 4. CXR (2010 C1)
56/103
65
Emphysema (imaging findings)
bilaterally flat, depressed hemidiaphragm lung overinflation
increased pulmonary radiolucency
increased retrosternal space (>4.5cm)
accentuated kyphosis
increased intercostal spaces
prominent hilar vasculature, decreased
peripheral
bullae
-
7/30/2019 4. CXR (2010 C1)
57/103
66
emphysema
normal
Emphysema
-
7/30/2019 4. CXR (2010 C1)
58/103
67
Emphysema
-
7/30/2019 4. CXR (2010 C1)
59/103
68
-
7/30/2019 4. CXR (2010 C1)
60/103
69
Normal vs.
emphysematous
lung tissue
-
7/30/2019 4. CXR (2010 C1)
61/103
71
Bullous emphysema
-
7/30/2019 4. CXR (2010 C1)
62/103
72
Bullous emphysema
Bullous Emphysema
-
7/30/2019 4. CXR (2010 C1)
63/103
73154 slides
EnlargedRetrosternal
Air Space
Flattened Diaphragms
Bullous Emphysema
73
-
7/30/2019 4. CXR (2010 C1)
64/103
74
Atelectasis
-
7/30/2019 4. CXR (2010 C1)
65/103
75154 slides 75
Left lower lobe collapse
-
7/30/2019 4. CXR (2010 C1)
66/103
76154 slides
Left lower lobe collapse
Further investigations?
76
-
7/30/2019 4. CXR (2010 C1)
67/103
77154 slides 77
-
7/30/2019 4. CXR (2010 C1)
68/103
78154 slides 78
Diagnosis: LLL Collapse
-
7/30/2019 4. CXR (2010 C1)
69/103
79154 slides
Diagnosis: LLL Collapse
Collapse secondary to central obstructing
tumour
79
-
7/30/2019 4. CXR (2010 C1)
70/103
80
Pulmonary Nodule
-
7/30/2019 4. CXR (2010 C1)
71/103
81154 slides
Solitary Pulmonary Nodule: What Would You Do Next?
1) Compare with Any Available Previous
2) Computed Tomography
81
-
7/30/2019 4. CXR (2010 C1)
72/103
82154 slides
Solitary Pulmonary Nodule can be:
Benign: Densely calcified noduleMalignant: Adenocarcinoma
82
-
7/30/2019 4. CXR (2010 C1)
73/103
83154 slidesMultiple Nodules: Diagnosis? Metastases 83
-
7/30/2019 4. CXR (2010 C1)
74/103
Pleura
84
Pl d Di h
-
7/30/2019 4. CXR (2010 C1)
75/103
85
Pleura and Diaphragm
Pleural EffusionLateral decubitus>Lateral>PA in
sensitivity
Pneumothorax
Upright
Deep sulcus sign in supine
Small Pleural Effusion
-
7/30/2019 4. CXR (2010 C1)
76/103
86154 slides 86
Small Pleural Effusion
-
7/30/2019 4. CXR (2010 C1)
77/103
87154 slides
Normal:Sharp Angles
Blunted posterior costophrenic sulcus 87
Large Pleural Effusion
-
7/30/2019 4. CXR (2010 C1)
78/103
88154 slides
Large Pleural Effusion
88
Lateral Decubitus
-
7/30/2019 4. CXR (2010 C1)
79/103
89154 slides
Lateral Decubitus
89
Pleural Effusion in Supine Patient
-
7/30/2019 4. CXR (2010 C1)
80/103
91154 slides
Pleural Effusion in Supine Patient
Pleural effusion
layers posteriorly
in a supineposition
Cause diffuse
increased density
91
-
7/30/2019 4. CXR (2010 C1)
81/103
93
-
7/30/2019 4. CXR (2010 C1)
82/103
95154 slides
Inspiration Expiration
95
-
7/30/2019 4. CXR (2010 C1)
83/103
96154 slides
Collapsed Right Lung
Tension Pneumothorax: Requires chest tube
Tracheal Deviation
What would you do with this patient?
96
-
7/30/2019 4. CXR (2010 C1)
84/103
Supine chest radiograph of a neonate illustrates the deep sulcus
sign with abnormal
deepening and lucency of the left lateral costophrenic angle
().97
-
7/30/2019 4. CXR (2010 C1)
85/103
Supine Patient
-
7/30/2019 4. CXR (2010 C1)
86/103
99154 slidesDeep Sulcus 99
-
7/30/2019 4. CXR (2010 C1)
87/103
100
Non Dependent Portion of Lung at Base in Supine Patient
Deep Sulcus:
What can you do to confirm?
-
7/30/2019 4. CXR (2010 C1)
88/103
101154 slidesLeft lateral decubitus 101
-
7/30/2019 4. CXR (2010 C1)
89/103
102
Mediastinum: Overview
Classification of Mediastinum
Examples of mediastinal masses
Classification of Mediastinum
-
7/30/2019 4. CXR (2010 C1)
90/103
103
Classification of Mediastinum
Anatomic
Superior: above sternal angle
Anterior
Middle: heart and pericardium
Posterior
There are radiographic classification e.g.
Felsons
Classification of Mediastinum
-
7/30/2019 4. CXR (2010 C1)
91/103
104
ANATOMIC CLASSIFICATION
The mediastinum is divided into 4 parts
Superior mediastinumApex of thorax to a planepassing through the
manubrio-sternal junction and fourthdorsal vertebral body
Anterior mediastinumIs anterior to heart & great
vessels
Middle mediastinumContains heart & greatvessels, lymph
nodes
Posteriormediastinum
Contains descending thoracicaorta,
azygous/hemiazygousveins,esophagus, thoracic duct,nerves &
lymph nodes
-
7/30/2019 4. CXR (2010 C1)
92/103
105
Anterior Mediastinal Mass
The 4 Ts
Thyroid
Thymus (Thymoma)Teratoma
Terrible Lymphoma (Tumour)
Thyroid Goiter
-
7/30/2019 4. CXR (2010 C1)
93/103
106154 slides
Thyroid Goiter
Most common
superior
mediastinal mass
extending tothoracic inlet
Note Tracheal Deviation106
Benign thymoma
-
7/30/2019 4. CXR (2010 C1)
94/103
107154 slides
Benign thymoma
Normal 107
Lateral CXR shows: mass is anterior
-
7/30/2019 4. CXR (2010 C1)
95/103
108154 slides
Lateral CXR shows: mass is anterior
NORMAL 108
Computed Tomography
-
7/30/2019 4. CXR (2010 C1)
96/103
109154 slides
p g p y
Thymoma
Do you know any
associated
clinical syndrome?
109
i h i
-
7/30/2019 4. CXR (2010 C1)
97/103
110154 slides
Hiatus hernia
110
-
7/30/2019 4. CXR (2010 C1)
98/103
111
Lymphadenopathy
-
7/30/2019 4. CXR (2010 C1)
99/103
112
Lymphadenopathy
LungCancer
-
7/30/2019 4. CXR (2010 C1)
100/103
113
Small cell CA
-
7/30/2019 4. CXR (2010 C1)
101/103
114154 slides Normal
Hilar and Mediastinal Lymphadenopathy
Diagnosis?114
Hilar Lymphadenopathy on lateral
-
7/30/2019 4. CXR (2010 C1)
102/103
115154 slides
Normal115
Sarcoidosis
-
7/30/2019 4. CXR (2010 C1)
103/103