Embed Size (px)
Citation preview

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 1/16
Normal
Labor and
Birth
The Five “Ps” of Labor
o Passageway: maternal
bony pelvis and tissues
o Passenger: the fetus
o Powers: primary and
secondary forces of labor
o Position: maternal
position
o Psyche: psychological
component of mother
The Passage
o Pelvis type
o Pelvis size
o Cervical effacement
o Cervical dilation

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 2/16
Cervical Effacement and Dilation
o Uterus divides into upper(contractile) and lower
(passive) segments.
o Effacement: taking up of
internal os and cervical canal
into uterine side walls
o Dilatation: Widening of
cervical os from opening < 1
cm to approximately 10 cm.
Formation of Lower Uterine Segment
Primigravida: Effacement usually occurs before dilation
Multipara: dilation & effacement usually occur together
The Passenger
o Fetal head
o Fetal attitude
o Fetal Lie
o Fetal presentation
o Fetal position
8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 3/16
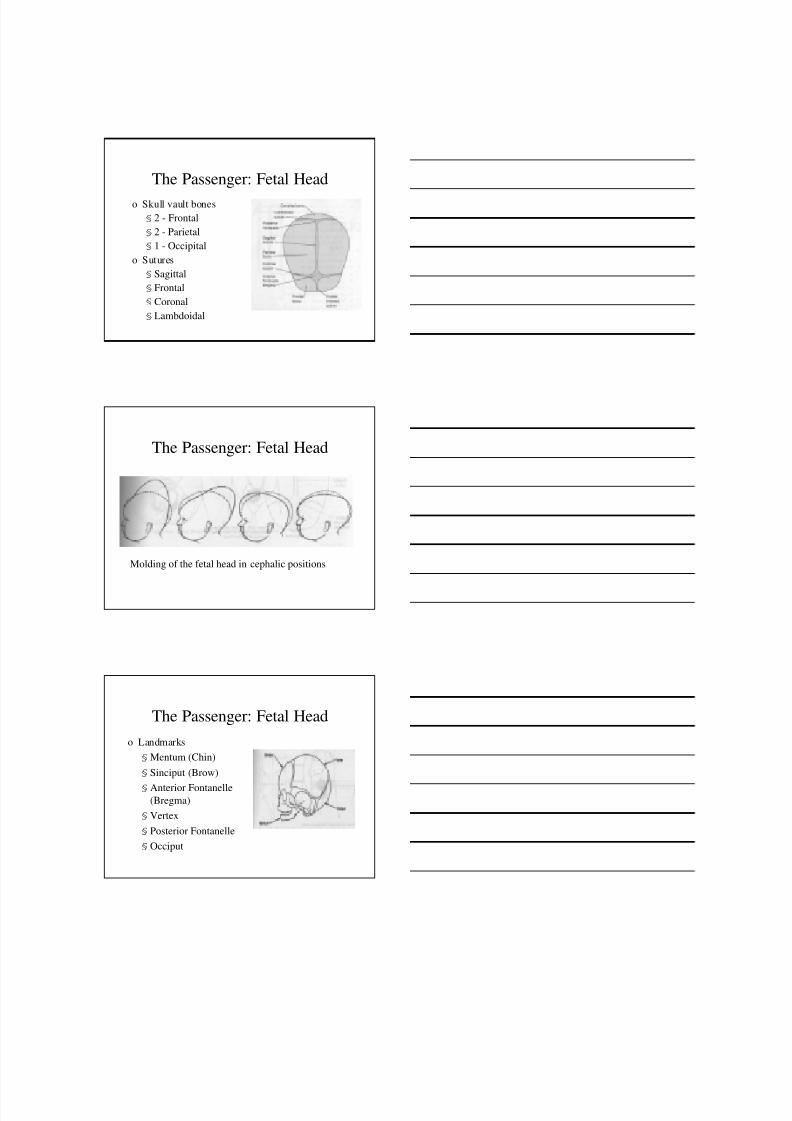
The Passenger: Fetal Head
o Skull vault bones
§ 2 - Frontal
§ 2 - Parietal
§ 1 - Occipital
o Sutures
§ Sagittal
§ Frontal
§ Coronal
§ Lambdoidal
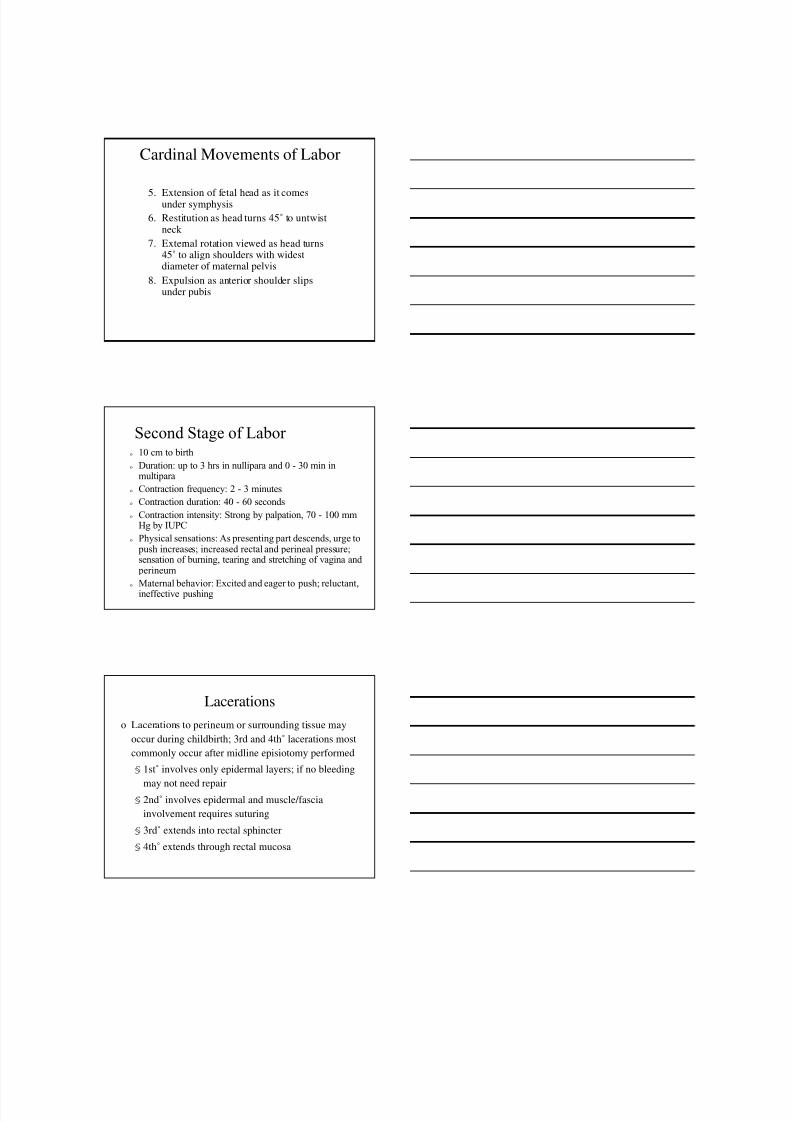
The Passenger: Fetal Head
Molding of the fetal head in cephalic positions
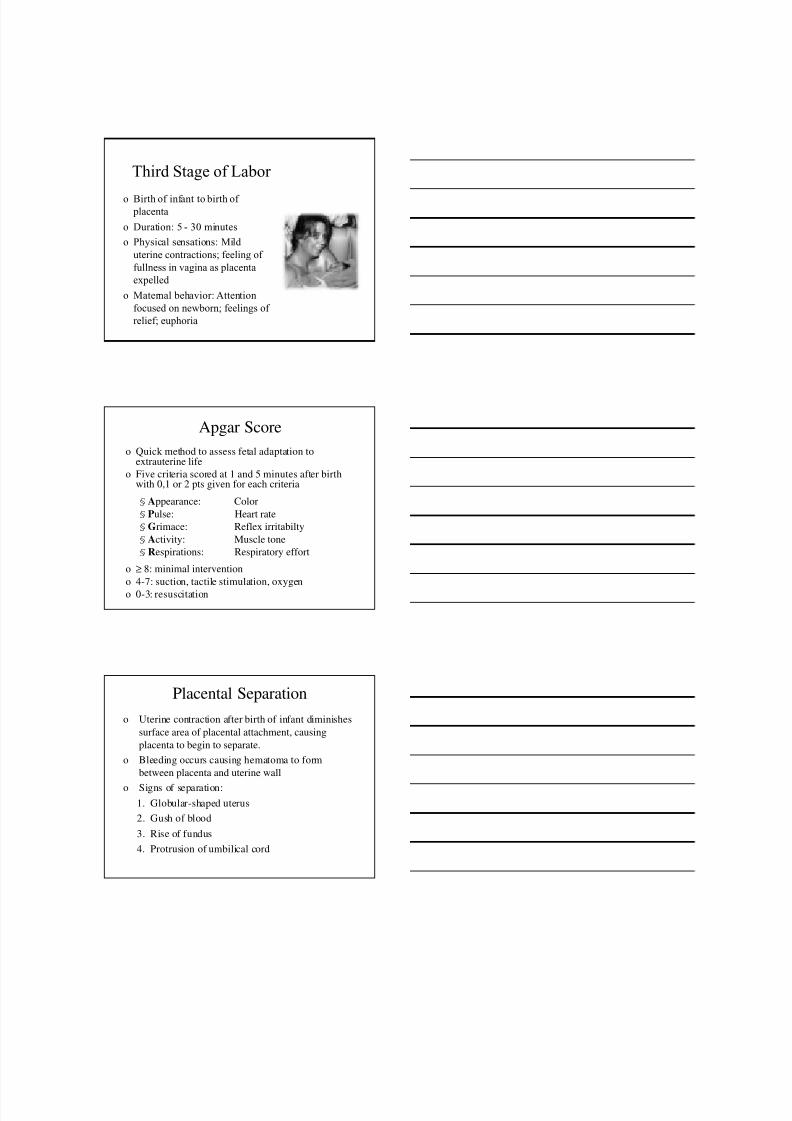
The Passenger: Fetal Head
o Landmarks
§ Mentum (Chin)
§ Sinciput (Brow)
§ Anterior Fontanelle(Bregma)
§ Vertex
§ Posterior Fontanelle
§ Occiput

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 4/16
The passenger: The Fetal Head
Anteroposterior diameters
of the fetal skull
Transverse diameters
of the fetal skull
Passenger: Fetal Attitude
o Relation of fetal parts to
one another
o Normal attitude is flexion
of neck, arms and legs
o Hyperextension is
abnormal attitude
o Fetal attitude changes can
cause larger diameter of
fetal head to present to
pelvis
Passenger: Fetal Lie
o Relationship of longitudinal axis of fetus
to longitudinal axis of mother
§ Longitudinal lie: fetal spine is parallel tomother’s spine
l Transverse lie: fetal spine is at right angles tomother’s spine
l Vertex (head first) is most common, but
breech (buttocks or feet first), transverse
(laterally across uterus) and oblique
(diagonally across uterus) also possible

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 5/16
Passenger: Fetal Presentation
o Presentation refers to fetal part entering pelvis first
o Most common is cephalic but breech and shoulder
also occur.
o Cephalic presentations: vertex, military, brow or
face
o Breech presentations: complete, frank or footling
o Shoulder presentation: occurs rarely; presenting
part is shoulder, arm, back, abdomen or side
Passenger: Cephalic Presentations
o Vertex§ Most common
§ Head completely flexed
§ Smallest diameterpresents
§ Occiput is thepresenting part
o Brow§ Partially extended§ Largest diameter
presents§ Sinciput is presenting
part
o Face
§ Hyperextended
§ Small diameterpresents
§ Face is presenting part
o Military
§ Neither flexed orextended
§ Larger diameterpresents
§ Top of head is
presenting part
Passenger: Malpresentations
o Complete Breech
§ Fetus sitting with legscrossed in pelvis
§ Knees and hips areflexed
§ Buttocks and feet arepresenting part
o Frank Breech
§ Hips are flexed withknees extended
§ Buttocks are thepresenting part
o Footling Breech
§ Hips and legs areextended
§ Feet are the presentingpart
§ Can be a double orsingle footling
o Shoulder Presentation
§ AKA transverse lie
§ Presenting part isshoulder, arm, back,abdomen or side

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 6/16
Passenger: Fetal Position
o Fetal landmarks of presenting fetal part to are used todescribe position of fetus in relation to the front(anterior), back (posterior), or sides (right or left) of maternal pelvis.
Fetal Landmarks
l O = Occiput (vertex)
l M = Mentum (face)
l S = Sacrum (breech)
l A = Acromion process
(shoulder)
Maternal Pelvis
l R = Right side
l L = Left side
l A = Anterior
l P = Posterior
lT = Transverse
Categories of Presentations
ROA= Right Occipital
Anterior
LOA= Left Occipital
Anterior
LOT = Right Occipital
Transverse

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 7/16
Categories of Presentations
ROP= Right Occipital
Posterior
LMA= Left Mentum
Anterior
LSP = Left Sacrum Posterior
o Relationship of presenting partto imaginary line drawnbetween ischial spines of maternal pelvis
o Ischial spines mark narrowestdiameter through which fetusmust pass
o The station at the level of ischial spines is 0
o If presenting part is higher thanspines, it is a negative number.
o If presenting part is lower than
spines, it is a positive number.
The Passenger: Fetal Station
Passenger: Engagement
› Engagement occurs when largest diameter
of presenting part reaches pelvic inlet and
can be felt on vaginal exam
› Floating: If presenting part directed
towards pelvis but can easily be moved out
of inlet› Ballotable: When presenting part dips into
inlet but can be displaced with upward
pressure from examiner s fingers
› Engaged: If presenting part fixed in pelvic
inlet and cannot be dislodged

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 8/16
The Power:Uterine
Contractions
Power: Forces of Labor
o Primary forces are involuntary contractions of
uterine muscle fibers, stimulated by
pacemaker in upper uterine segment
o Secondary forces consist of the voluntary use
of abdominal muscles during the second stage
of labor to facilitate the descent and delivery
of the fetus
Power: Primary Forces of Labor
o Effacement:
§ With each UC, muscles of upper uterine segmentshorten, exerting longitudinal traction on cervixcausing thinning and drawing up of internal os andcervical canal into uterine side walls
§ Measured from 0 to 100%o Dilation (aka dilatation)
§ As uterus elongates with UCs, fetal bodystraightens out and exerts pressure against loweruterine segment and cervix. Cervix opens as aresult, allowing for birth of fetus
§ Measured from 0 to 10 cm

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 9/16
Power: Primary Forces of Labor
Position of Laboring Woman
o Affects: circulation, fatigue,comfort
o Upright position (walking,sitting. kneeling, squatting)
§ Promotes descent of fetus
§ Improves blood flow
§ Relieves backache
§ Straightens axis of birthcanal
§ Increases pelvic outlet
Psyche
o Preparation for childbirth
o Sociocultural heritage
o Previous childbirth
experience
o Support from significantothers
o Emotional status
o Environmental influence

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 10/16
Premonitory Signs of Labor
o Lightening
o Bloody show
o Painful Braxton Hicks
o Cervical ripening
o Diarrhea
o Energy burst
False vs True Labor
False Labor
o Regular contractions
o Decrease in frequency andintensity
o Discomfort in lowerabdomen and groin
o Activitychange alters Ucs
o UCs stop when sleeping
o No appreciable cervicalchange
o Sedation decreases UCs
o Show usually not present
True Labor
o Regular contractions
o Progressive frequency andintensity
o Discomfort begins in back,radiating to abdomen
o Activity increases UCs;continue when sleeping
o Progressive effacement anddilation of cervix
o Sedation does not stop UCs
o Show usually present
Leopold’s First Maneuver

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 11/16
Leopold’s Second Maneuver
Leopold’s Third Maneuver
Leopold’s Fourth Maneuver

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 12/16
Stages of Labor and Birth
o First stage:begins with onset of true labor and ends
with complete dilation
o Second stage: begins with complete dilation and
ends with birth of infant
o Third stage: begins with expulsion of infant and
ends with expulsion of placenta
o Fourth stage: begins with expulsion of placenta,
lasting 1 to 4 hours
First Stage of Labor
Latent Phase
§ Cervical dilation: 0 - 3 cm
§ Duration: 8.6 hrs in nullipara - 5.3 hrs in multipara
§ Contraction frequency: 3 - 30 minutes; may beirregular
§ Contraction duration: 30 - 40 seconds
§ Contraction intensity: Mild by palpation, 25 - 40 mmHg by IUPC
§ Physical sensations: Menstrual-like cramps, lowbackache, light bloody show, diarrhea, possible SROM
§ Maternal behavior: Able to ambulate and talk through
contractions; pain controlled fairly well
First Stage of Labor
Active Phase
§ Cervical dilation: 4 - 7 cm
§ Duration: 4.6 hrs in nullipara - 2.4 hrs in multipara
§ Contraction frequency: 2 - 5 minutes
§ Contraction duration: 40 - 60 seconds
§ Contraction intensity: Moderate to strong by
palpation, 50 - 70 mm Hg by IUPC
§ Physical sensations: Increasing discomfort, trembling
of thighs/legs; pressure on bladder and rectum;
backache with occipitoposterior fetal position.
§ Maternal behavior: Working to keep control; quieter

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 13/16
First Stage of Labor Transition
§
Cervical dilation: 8 - 10 cm§ Duration: 3.6 hrs in nullipara - variable in multipara
§ Contraction frequency: 1.5 - 2 minutes
§ Contraction duration: 60 - 90 seconds
§ Contraction intensity: Strong by palpation, 70 - 90 mm
Hg by IUPC
§ Physical sensations: Increased bloody show; urge to
push; increased rectal pressure, ROM may occur.
§ Maternal behavior: Ambulation difficult; may be
irritable, agitated; self-absorbed; needs more support;
may feel discouraged and unable to cope
Cardinal Movements of Labor
o Descent
o Flexion
o Internal Rotation
o Extension
o Restitution
o External Rotation
o Expulsion
Cardinal Movements of Labor
o Adaptations made by fetus to maneuverthrough pelvis during labor and birth.
o In occiput (most common presentation),movements occur in following order:
1. Engagement of presenting part occurs
2. Descent of fetus into pelvis3. Flexion of fetal head (often occurs with
descent)
4. Internal rotation of fetal head toaccommodate widest diameter of maternalpelvis
8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 14/16
Cardinal Movements of Labor
5. Extension of fetal head as it comesunder symphysis
6. Restitution as head turns 45˚ to untwistneck
7. External rotation viewed as head turns45˚ to align shoulders with widestdiameter of maternal pelvis
8. Expulsion as anterior shoulder slipsunder pubis
Second Stage of Labor o 10 cm to birth
o Duration: up to 3 hrs in nullipara and 0 - 30 min inmultipara
o Contraction frequency: 2 - 3 minutes
o Contraction duration: 40 - 60 seconds
o Contraction intensity: Strong by palpation, 70 - 100 mmHg by IUPC
o Physical sensations: As presenting part descends, urge to push increases; increased rectal and perineal pressure;sensation of burning, tearing and stretching of vagina and perineum
o Maternal behavior: Excited and eager to push; reluctant,ineffective pushing
Lacerations
o Lacerations to perineum or surrounding tissue may
occur during childbirth; 3rd and 4th˚ lacerations most
commonly occur after midline episiotomy performed
§ 1st˚ involves only epidermal layers; if no bleeding
may not need repair§ 2nd˚ involves epidermal and muscle/fascia
involvement requires suturing
§ 3rd˚ extends into rectal sphincter
§ 4th˚ extends through rectal mucosa
8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 15/16
Third Stage of Labor
o Birth of infant to birth of placenta
o Duration: 5 - 30 minutes
o Physical sensations: Mild
uterine contractions; feeling of
fullness in vagina as placenta
expelled
o Maternal behavior: Attention
focused on newborn; feelings of
relief; euphoria
Apgar Score
o Quick method to assess fetal adaptation toextrauterine life
o Five criteria scored at 1 and 5 minutes after birthwith 0,1 or 2 pts given for each criteria
§Appearance: Color
§ Pulse: Heart rate
§Grimace: Reflex irritabilty
§Activity: Muscle tone
§Respirations: Respiratory effort
o ≥ 8: minimal intervention
o 4-7: suction, tactile stimulation, oxygen
o 0-3: resuscitation
Placental Separation
o Uterine contraction after birth of infant diminishes
surface area of placental attachment, causing
placenta to begin to separate.
o Bleeding occurs causing hematoma to form
between placenta and uterine wall
o Signs of separation:
1. Globular-shaped uterus
2. Gush of blood
3. Rise of fundus
4. Protrusion of umbilical cord

8/13/2019 4. Labor and Birth
http://slidepdf.com/reader/full/4-labor-and-birth 16/16
Placental Separation
Placental Delivery
o When signs of separation appear:
§Ask woman to bear down
§ If undelivered, firm, gentle traction applied to cordwith pressure on fundus
§ Shiny Schultz: Separation occurs from inner toouter margins of placenta allowing fetal side todeliver first
§Dirty Duncan: Separation occurs from outermargins first, causing placenta to roll up withmaternal surface first.
§ Considered retained when 30 minutes have elapsed
without delivery of placenta
Fourth Stage of Labor
o One to four hours following birth
o Tremendous hemodynamic changes occur
o Blood not lost at birth (250 - 500 ml) isredistributed into venous beds
o B P drops, pulse increaseso Uterus is contracted and is midline
o Fundus is usually midway between umbilicus andsymphysis pubis
o Shaking chill is common
o Hypotonic bladder may lead to urinary retention





























