Embed Size (px)
Citation preview

20S Proceedings of the NASS 22nd Annual Meeting / The Spine Journal 7 (2007) 1S–163S
PURPOSE: No study to date has shown the superiority of single versus
dual rod instrumentation.
STUDY DESIGN/SETTING: Retrospective review of multi-center
database.
PATIENT SAMPLE: One hundred patients with Lenke Type 5 thoraco-
lumbar and lumbar scoliosis underwent anterior spinal fusion with instru-
mentation and structural interbody grafting. Sixty-one patients were
treated with dual rods, and 39 with a single rod.
OUTCOME MEASURES: Comparison of clinical and radiographic re-
sults at 2-year postoperative follow-up.
METHODS: There were no statistically significant differences in any pre-
op measurements between the 2 groups. Minimum follow-up was 2 years.
RESULTS: Mean preop/2-yr follow-up lumbar curve magnitude was 46o/
14o for the single rods and 48o/18o for the dual rods, with significant im-
provement in both groups (p!0.01). The mean lumbar curve correction for
the single rods at 1st postop, 1 yr, and 2 yr visits were 83%, 71%, and 71%,
respectively. Mean lumbar curve correction for the dual rods at 1st postop,
1 yr, and 2 yr visits were 72%, 65%, and 63%, respectively. Both groups
had significant improvement in the percent correction at 2-yr follow-up
(p!0.02). Mean preop/2-yr follow-up main thoracic curve magnitude
was 26o/16o for the single rods and 24o/16o for the dual rods. Mean pre-
op/2-yr follow-up T2-T12 kyphosis was 24o/25o for the single rods and
25o/26o for the dual rods. Mean preop/2-yr follow-up lumbar lordosis
was 61o/58o for the single rods and 59o/57o for the dual rods. There
was signicant improvement in the coronal C7 to CSVL measurements
made preop and at 2-yr follow-up in both groups (p!0.001). There was
no significant difference in either the PJK or DJK measurements made pre-
op and at 2-yr follow-up. Mean blood loss was lower (415 vs 620 cc) and
operative time shorter (263 vs 319 min) for the single rods (p!0.03). Four
patients with dual rods had a pseudarthrosis. One patient with dual rods
had a screw misplacement causing nerve root irritation requiring revision.
There were no infections.
CONCLUSIONS: At 2-yr follow-up, the radiographic results of single
versus dual rod instrumentation appear comparable, but with better main-
tenance of coronal percent correction, shorter operative times, and less
blood loss in the single rod group.
FDA DEVICE/DRUG STATUS: Anterior spinal instrumentation:
Approved for this indication.
doi: 10.1016/j.spinee.2007.07.046
Wednesday, October 24, 20075:25–6:25 PM
Special Interest Poster Presentation 3:Complications
40. Surgical Site Infection in Spinal Metastasis - Risk Factor and
Countermeasure
Satoru Demura, MD1, Norio Kawahara, MD1, Hideki Murakami, MD,
PhD1, Katsuro Tomita, MD1; 1Kanazawa University, Kanazawa, Japan
BACKGROUND CONTEXT: Surgery for spinal metastasis is associated
with an increased risk of surgical site infection (SSI), (incidence: 8 to
25%). Although previous studies have evaluated risk factors for SSI, such
studies lack statistical analysis, including multivariate analysis. A recent
study demonstrated the utility of prostaglandin E1 (PGE1) in decreasing
wound complications after laryngeal surgery in patients with prior irradi-
ation. The role of PGE1 in spine surgery has not been previously
evaluated.
PURPOSE: The purpose of this study is to identify and analyze indepen-
dent risk factors of SSI and to evaluate the potential of prostaglandin E1 to
decrease the risk of SSI in patients with spinal metastasis.
STUDY DESIGN/SETTING: A retrospective review (phase 1) and pro-
spective clinical study (phase 2).
PATIENT SAMPLE: Surgery for spinal metastasis was performed in 176
patients.
OUTCOME MEASURES: Infection rate and independent risk factors for
SSI were analyzed using multivariate logistic regression.
METHODS: 113 patients with spinal metastasis, treated between 1993
and 2002, were retrospectively reviewed (phase 1). Potential risk factors
for SSI included in the analysis were patient’s characteristics (age, diabe-
tes, preoperative nutrition, adjunctive treatment with chemotherapy, irradi-
ation, and corticosteroids) and surgery-related factors (repeated spinal
surgery, surgical procedures, blood loss amount and operation time). Risk
factors for SSI were analyzed using logistic regression. The second portion
of the study (Phase 2) was a prospective clinical trial investigating the util-
ity of PGE1 at reducing the rate of SSI in patients treated with preoperative
irradiation. Phase 2 occurred between 2003 and 2006, during which time
63 surgeries for with spinal metastasis were treated at our institute. The in-
fection rate and risk factors identified in phase 1 and 2 were compared.
RESULTS: The rate of SSI during Phase 1 was 7.1% (8/113 cases). Inde-
pendent risk factors identified by multivariate logistic regression were di-
abetes (odds ratio [OR] 17.1, p50.011), and preoperative irradiation at the
surgical site (OR 19.5, p50.016). The rate of SSI for patients who had ir-
radiation before surgery was 32% (7/22 cases), while the rate for patients
without irradiation was 1.1% (1/91 cases). This difference was statistically
significant (p!0.01, Fisher’s exact test). The rate of SSI in phase 2 was
3.2% (2/63 cases). For phase 2 patients that received preoperative surgical
site irradiation, the rate of SSI was 6.7% (1/15 cases).
CONCLUSIONS: This study identified diabetes and preoperative surgical
site irradiation to be independent risk factors for SSI in patients with spinal
metastasis. Irradiation has previously been shown to inhibit fibroblasts,
which are responsible for the remodeling of collagen in surgical wounds.
PGE1 was reported to decrease the rate of SSI in patients treated with ir-
radiation prior to laryngeal surgery. In the current study, PGE1 administra-
tion was found to significantly decrease the incidence of SSI in patients
with spinal metastases who underwent preoperative irradiation (6.7% vs.
32%). Although small patient numbers limits the current study, the positive
effect of PGE1 in patients with spinal metastasis is encouraging and merits
further evaluation.
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include
any applicable devices or drugs.
doi: 10.1016/j.spinee.2007.07.048
41. Neurological Deficit Following Percutaneous Vertebral
Stabilization
Alpesh Patel, MD1, Alexander Vaccaro, MD2, Greg Martyak2,
James Harrop, MD2, Todd Albert, MD2, Steven Ludwig, MD3, Jim
A. Youssef, MD4, Daniel Gelb, MD5, Hallett Mathews, MD6,
Jens Chapman, MD7, Timothy Kuklo, MD, JD8, Edward Chung3,
Alan Hilibrand, MD2, Greg Anderson, MD2; 1University of Utah, Salt Lake
City, UT, USA; 2Thomas Jefferson University, Philadelphia, PA, USA;3University of Maryland School of Medicine, Baltimore, MD, USA;4Durango Orthopedic Associates, PC, Durango, CO, USA; 5Baltimore,
MD, USA; 6MidAtlantic Spine Specialists, Richmond, VA, USA;7University of Washington, WA, USA; 8Walter Reed Army Medical Center,
Washington, DC, USA
BACKGROUND CONTEXT: Percutaneous vertebral stabilization proce-
dures, including vertebroplasty and kyphoplasty, have become a widely
utilized for the treatment of osteoporotic vertebral compression fractures,
primary and metastatic vertebral tumors, and traumatic burst fractures. De-
spite an increasing array of indications, there have been few reports of
adverse events. Neurologic complications associated with vertebroplasty
and kyphoplasty have been described previously as case reports and have
generally been considered as infrequent and minor in severity.
21SProceedings of the NASS 22nd Annual Meeting / The Spine Journal 7 (2007) 1S–163S
PURPOSE: The purpose of this study is to document a series of patients
with neurological deficit following percutaneous vertebral stabilization, to
identify patterns of neurologic injury, and to describe potential methods for
avoiding these injuries.
STUDY DESIGN/SETTING: A retrospective review.
PATIENT SAMPLE: Fourteen patients presenting with neurological
injury after percutaneous vertebral stabilization.
OUTCOME MEASURES: Neurological status, Complications.
METHODS: A retrospective review was performed on fourteen patients
with neurologic injury following percutaneous vertebral stabilization.
Radiographic data, physical examination, treatment strategy, and clinical
outcomes were recorded.
RESULTS: The average patient age was 74.9 years (range 46 to 88) with
three male and 11 female patients. Six patients underwent a vertebroplasty
procedure while eight were treated with kyphoplasty. Six patients devel-
oped neurologic deficits acutely (!24 hours of procedure). The remaining
eight patients developed neurologic symptoms at an average of 37.1 days
(range 3 to 112) post procedure. Neurologic deficits were recorded as
ASIA A in 4 patients, ASIA B in 2 patients, ASIA C in 1 patient, and
ASIA D in 7 patients. Twelve of fourteen patients (85.7%) required revi-
sion open surgical intervention for treatment of their neurologic injury.
Complications included death (3 patients), pulmonary embolism (1), cere-
brovascular accident (1), dural tear (1), and nerve root injury (1).
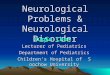
Figure 1. PMMA extravasation.
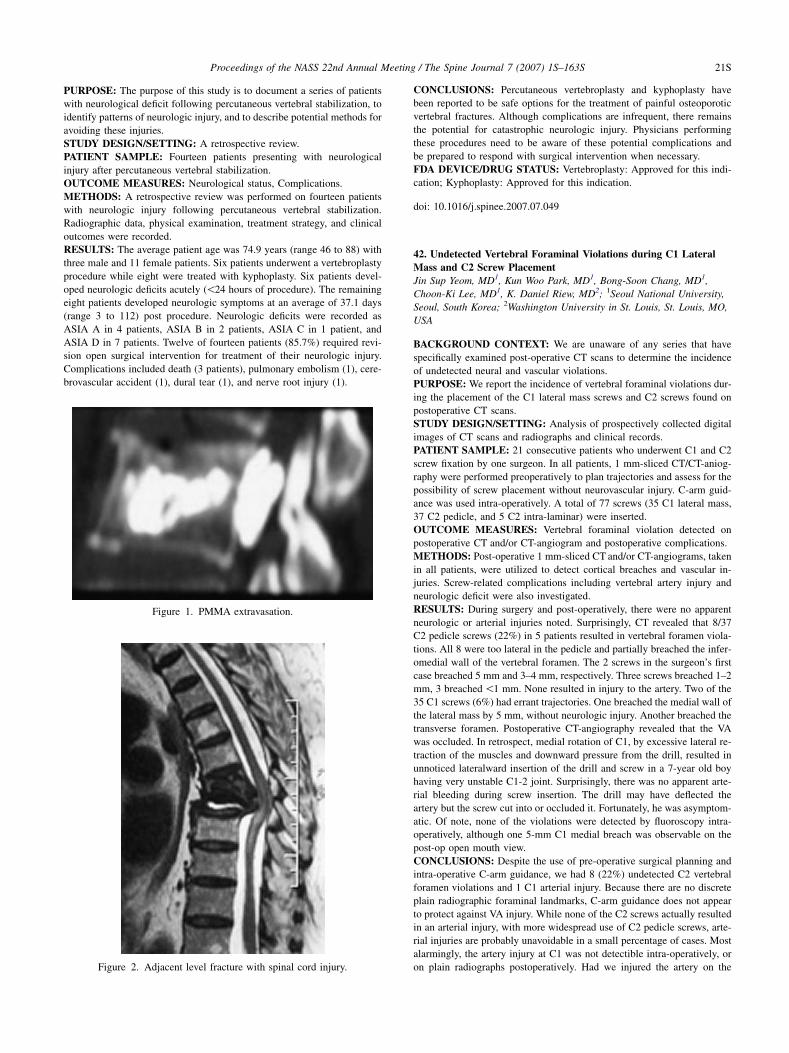
Figure 2. Adjacent level fracture with spinal cord injury.
CONCLUSIONS: Percutaneous vertebroplasty and kyphoplasty have
been reported to be safe options for the treatment of painful osteoporotic
vertebral fractures. Although complications are infrequent, there remains
the potential for catastrophic neurologic injury. Physicians performing
these procedures need to be aware of these potential complications and
be prepared to respond with surgical intervention when necessary.
FDA DEVICE/DRUG STATUS: Vertebroplasty: Approved for this indi-
cation; Kyphoplasty: Approved for this indication.
doi: 10.1016/j.spinee.2007.07.049
42. Undetected Vertebral Foraminal Violations during C1 Lateral
Mass and C2 Screw Placement
Jin Sup Yeom, MD1, Kun Woo Park, MD1, Bong-Soon Chang, MD1,
Choon-Ki Lee, MD1, K. Daniel Riew, MD2; 1Seoul National University,
Seoul, South Korea; 2Washington University in St. Louis, St. Louis, MO,
USA
BACKGROUND CONTEXT: We are unaware of any series that have
specifically examined post-operative CT scans to determine the incidence
of undetected neural and vascular violations.
PURPOSE: We report the incidence of vertebral foraminal violations dur-
ing the placement of the C1 lateral mass screws and C2 screws found on
postoperative CT scans.
STUDY DESIGN/SETTING: Analysis of prospectively collected digital
images of CT scans and radiographs and clinical records.
PATIENT SAMPLE: 21 consecutive patients who underwent C1 and C2
screw fixation by one surgeon. In all patients, 1 mm-sliced CT/CT-aniog-
raphy were performed preoperatively to plan trajectories and assess for the
possibility of screw placement without neurovascular injury. C-arm guid-
ance was used intra-operatively. A total of 77 screws (35 C1 lateral mass,
37 C2 pedicle, and 5 C2 intra-laminar) were inserted.
OUTCOME MEASURES: Vertebral foraminal violation detected on
postoperative CT and/or CT-angiogram and postoperative complications.
METHODS: Post-operative 1 mm-sliced CT and/or CT-angiograms, taken
in all patients, were utilized to detect cortical breaches and vascular in-
juries. Screw-related complications including vertebral artery injury and
neurologic deficit were also investigated.
RESULTS: During surgery and post-operatively, there were no apparent
neurologic or arterial injuries noted. Surprisingly, CT revealed that 8/37
C2 pedicle screws (22%) in 5 patients resulted in vertebral foramen viola-
tions. All 8 were too lateral in the pedicle and partially breached the infer-
omedial wall of the vertebral foramen. The 2 screws in the surgeon’s first
case breached 5 mm and 3–4 mm, respectively. Three screws breached 1–2
mm, 3 breached !1 mm. None resulted in injury to the artery. Two of the
35 C1 screws (6%) had errant trajectories. One breached the medial wall of
the lateral mass by 5 mm, without neurologic injury. Another breached the
transverse foramen. Postoperative CT-angiography revealed that the VA
was occluded. In retrospect, medial rotation of C1, by excessive lateral re-
traction of the muscles and downward pressure from the drill, resulted in
unnoticed lateralward insertion of the drill and screw in a 7-year old boy
having very unstable C1-2 joint. Surprisingly, there was no apparent arte-
rial bleeding during screw insertion. The drill may have deflected the
artery but the screw cut into or occluded it. Fortunately, he was asymptom-
atic. Of note, none of the violations were detected by fluoroscopy intra-
operatively, although one 5-mm C1 medial breach was observable on the
post-op open mouth view.
CONCLUSIONS: Despite the use of pre-operative surgical planning and
intra-operative C-arm guidance, we had 8 (22%) undetected C2 vertebral
foramen violations and 1 C1 arterial injury. Because there are no discrete
plain radiographic foraminal landmarks, C-arm guidance does not appear
to protect against VA injury. While none of the C2 screws actually resulted
in an arterial injury, with more widespread use of C2 pedicle screws, arte-
rial injuries are probably unavoidable in a small percentage of cases. Most
alarmingly, the artery injury at C1 was not detectible intra-operatively, or
on plain radiographs postoperatively. Had we injured the artery on the