Embed Size (px)
Citation preview
© 2015 Private & Confidential
Update in Outpatient Medicine
Robert A Gluckman, MD, MACPChief Medical Officer Providence Health Plans
© 2015 Private & Confidential2
Disclosures
• Stock Holdings– Abbott Labs– Abbvie– Bristol Myers Squibb– GE– Proctor and Gamble– Walgreens
© 2015 Private & Confidential3
Topics• Breast cancer screening• Treatment of low risk DCIS• BP targets revisited• Medication choice in resistant hypertension• Personalized treatment of chronic disease• Treatment of hyperlipidemia in intermediate risk patients• Vitamin D and statin myopathy• Restarting anticoagulants after GI Bleeding in a. fibrillation
© 2015 Private & Confidential4
ACS Breast Cancer Screening Guidelines• Recommendations limited to average risk women
Assess previous PMH, FH using risk tool
• Performed a systematic evidence review and graded the evidence
• Made strong vs. qualified recommendationsStrong recommendation- Most individuals would want the recommended course of actionQualified recommendation- Majority of individuals would want the recommended course of action but many would not- shared decision making
JAMA 2015;314:1599-1614
© 2015 Private & Confidential5
ACS BCS Guidelines Key points
• Begin screening at age 45 and continue as long as overall health is good and life expectancy ≥ 10 yrs.
Strong recommendation• Screen annually between ages 45-54
Qualified recommendation• Women ≥ 55 should transition to biennial screening
Qualified recommendation• Women should have the opportunity to start screening at age 40• Women should have the opportunity to undergo annual screening• Clinical breast exam not recommended
© 2015 Private & Confidential6
USPTF Breast Cancer Screening Guidelines• Recommends biennial screening for women age 50-74
(Grade B)
• Recommends the decision to start screening before age 50 is an individual one (Grade C)
Women placing more emphasis on benefit over harm may choose to begin biennial screening at age 40
• Evidence insufficient for screening age 75 and over, digital breast tomosynthesis (DBT) as primary screening or DBT, ultrasound or MRI as adjunctive screening for women with dense breasts and otherwise negative exam
Ann Intern Med published online Jan 12, 2016
© 2015 Private & Confidential7
Areas of ControversyAge to start screening
5 year risk for BC dx is similar from 45‐49 (0.9%) than 50‐54 (1.1%).
Incidence age 40‐44 0.6%
Similar distribution of BC deaths by age at diagnosis for women age 45‐49 (10%) and 50‐54 (12%)
Age to stop screeningIncrease in BC incidence increases to age 7926% BC deaths occur after age 74No benefit for screening women in poor health
(i.e. Charlson Co-Morbidity Index ≥ 2)
© 2015 Private & Confidential8
Areas of Controversy
Screening intervalPremenopausal women undergoing biennial mammography have a 28% increase in advanced stage disease compared with shorter screening intervals
Tumor characteristics similar in women > 50 undergoing annual vs. biennial screening
False positive recalls and biopsies decrease over 30% with biennial vs. annual screening
© 2015 Private & Confidential9 JAMA Surg. 2015; 150(8):739-745 © 2015 Private & Confidential10
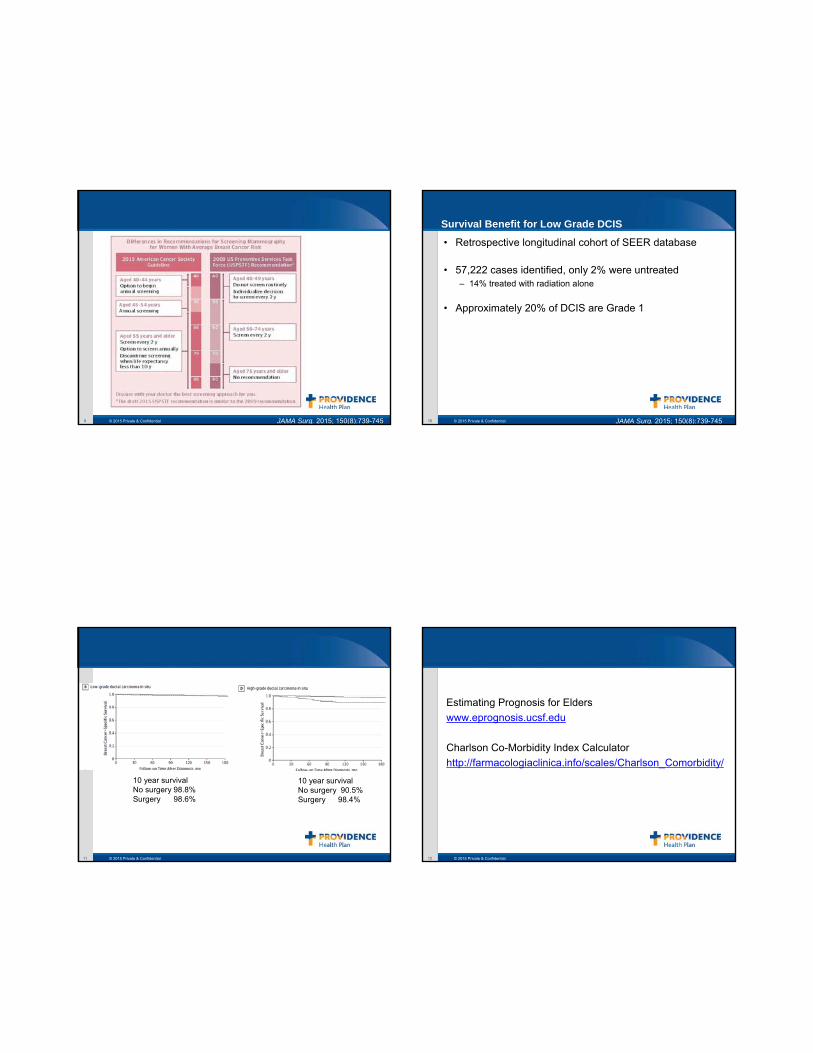
Survival Benefit for Low Grade DCIS
• Retrospective longitudinal cohort of SEER database
• 57,222 cases identified, only 2% were untreated – 14% treated with radiation alone
• Approximately 20% of DCIS are Grade 1
JAMA Surg. 2015; 150(8):739-745
© 2015 Private & Confidential11
10 year survival No surgery 98.8%Surgery 98.6%
10 year survivalNo surgery 90.5%Surgery 98.4%
© 2015 Private & Confidential12
Estimating Prognosis for Elderswww.eprognosis.ucsf.edu
Charlson Co-Morbidity Index Calculatorhttp://farmacologiaclinica.info/scales/Charlson_Comorbidity/
© 2015 Private & Confidential13
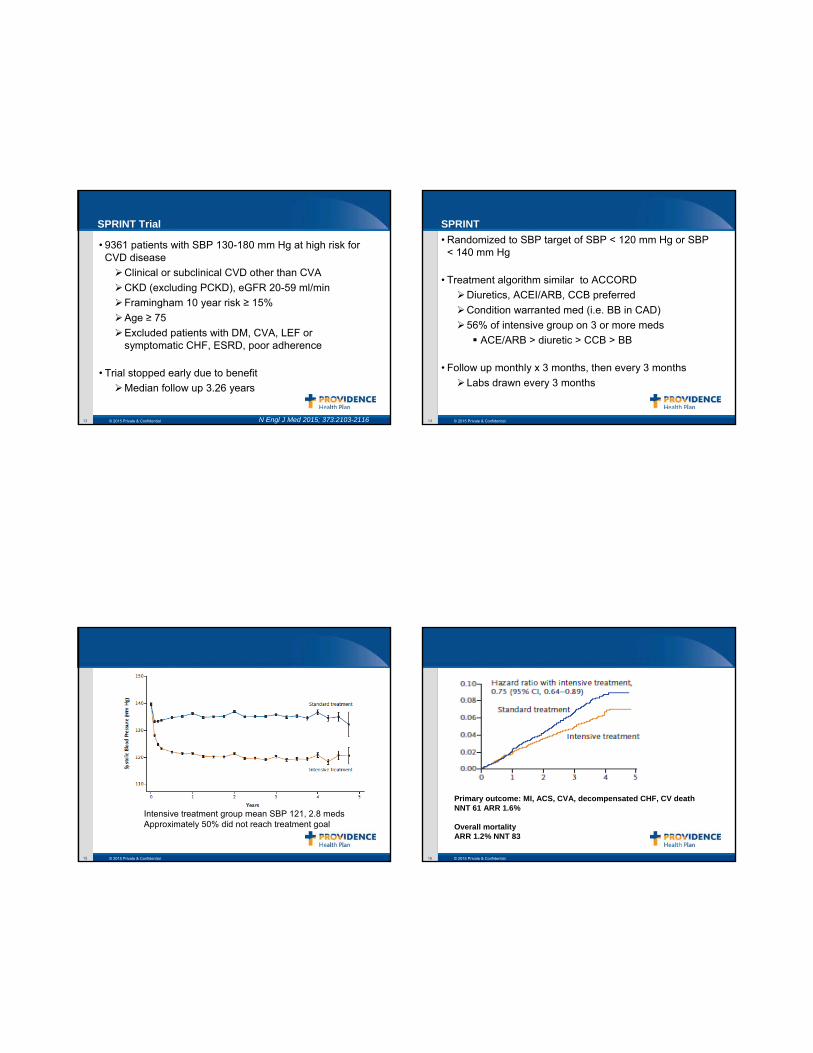
SPRINT Trial
• 9361 patients with SBP 130-180 mm Hg at high risk for CVD disease
Clinical or subclinical CVD other than CVACKD (excluding PCKD), eGFR 20-59 ml/minFramingham 10 year risk ≥ 15%Age ≥ 75Excluded patients with DM, CVA, LEF or symptomatic CHF, ESRD, poor adherence
• Trial stopped early due to benefitMedian follow up 3.26 years
N Engl J Med 2015; 373:2103-2116 © 2015 Private & Confidential14
SPRINT• Randomized to SBP target of SBP < 120 mm Hg or SBP
< 140 mm Hg
• Treatment algorithm similar to ACCORDDiuretics, ACEI/ARB, CCB preferredCondition warranted med (i.e. BB in CAD)56% of intensive group on 3 or more meds
ACE/ARB > diuretic > CCB > BB
• Follow up monthly x 3 months, then every 3 monthsLabs drawn every 3 months
© 2015 Private & Confidential15
Intensive treatment group mean SBP 121, 2.8 medsApproximately 50% did not reach treatment goal
© 2015 Private & Confidential16
Primary outcome: MI, ACS, CVA, decompensated CHF, CV deathNNT 61 ARR 1.6%
Overall mortalityARR 1.2% NNT 83
© 2015 Private & Confidential17 © 2015 Private & Confidential18
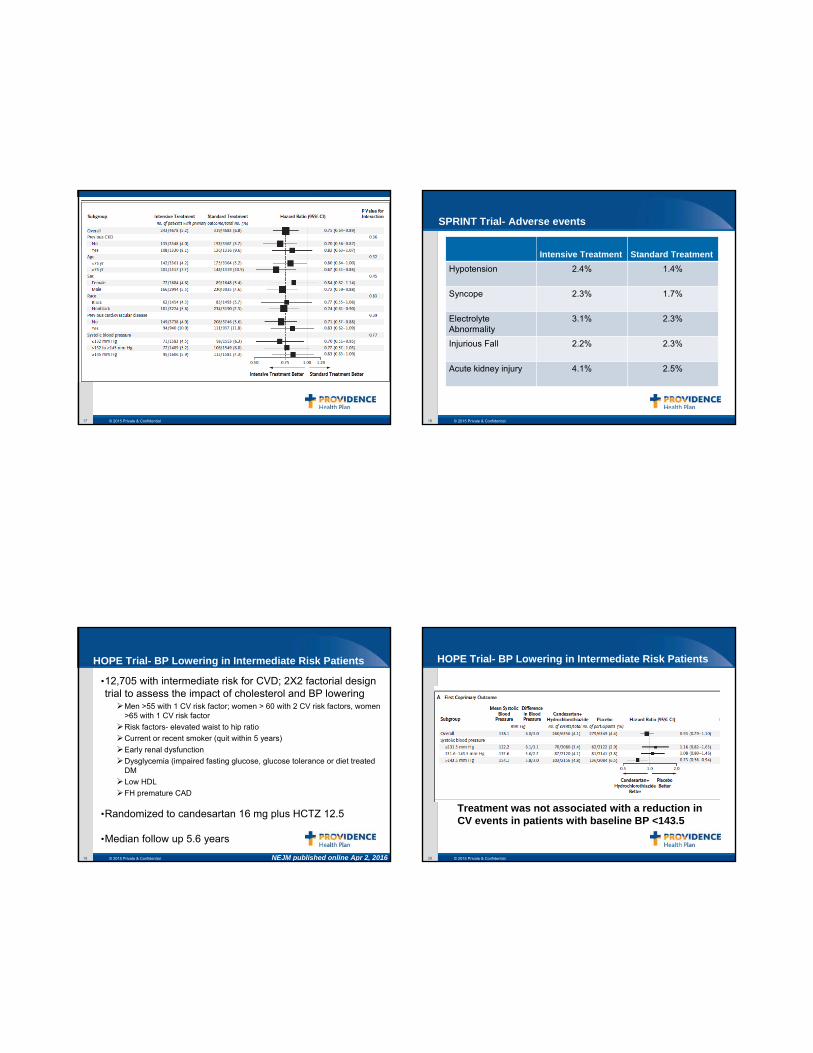
SPRINT Trial- Adverse events
Intensive Treatment Standard Treatment Hypotension 2.4% 1.4%
Syncope 2.3% 1.7%
Electrolyte Abnormality
3.1% 2.3%
Injurious Fall 2.2% 2.3%
Acute kidney injury 4.1% 2.5%
© 2015 Private & Confidential19
HOPE Trial- BP Lowering in Intermediate Risk Patients
•12,705 with intermediate risk for CVD; 2X2 factorial design trial to assess the impact of cholesterol and BP lowering
Men >55 with 1 CV risk factor; women > 60 with 2 CV risk factors, women >65 with 1 CV risk factorRisk factors- elevated waist to hip ratioCurrent or recent smoker (quit within 5 years)Early renal dysfunctionDysglycemia (impaired fasting glucose, glucose tolerance or diet treated DMLow HDLFH premature CAD
•Randomized to candesartan 16 mg plus HCTZ 12.5
•Median follow up 5.6 years
NEJM published online Apr 2, 2016 © 2015 Private & Confidential20
HOPE Trial- BP Lowering in Intermediate Risk Patients
Treatment was not associated with a reduction in CV events in patients with baseline BP <143.5
© 2015 Private & Confidential21
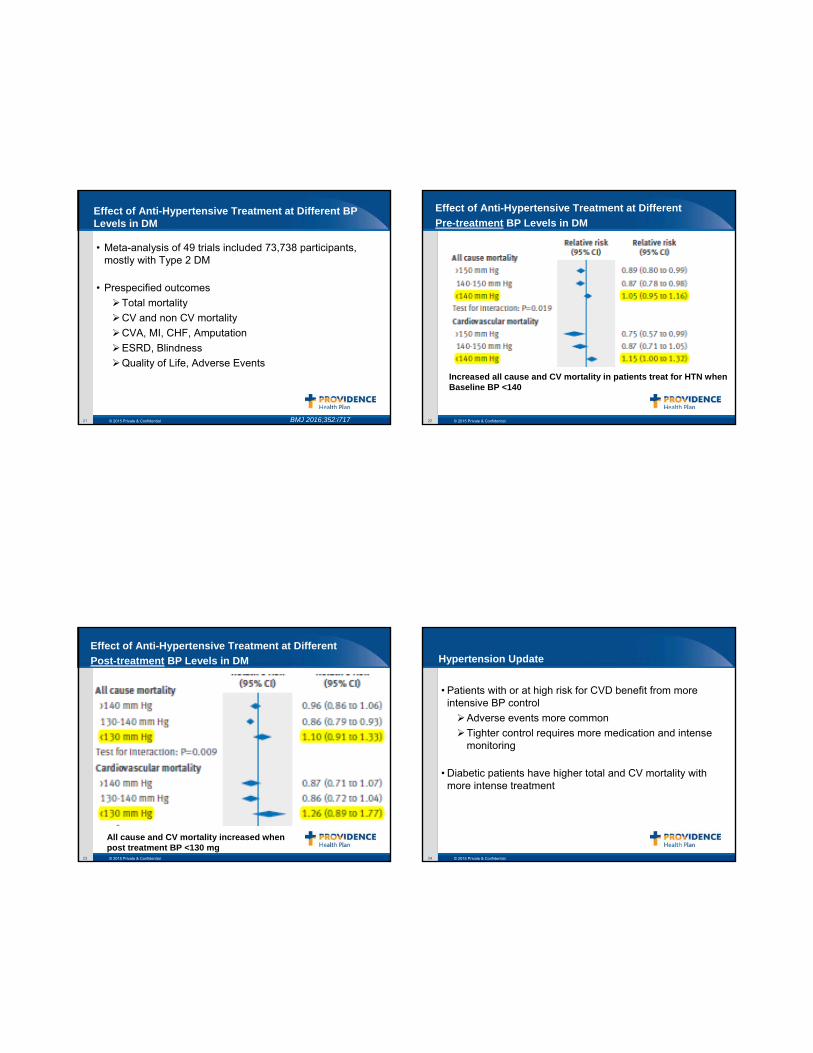
Effect of Anti-Hypertensive Treatment at Different BP Levels in DM
• Meta-analysis of 49 trials included 73,738 participants, mostly with Type 2 DM
• Prespecified outcomesTotal mortalityCV and non CV mortalityCVA, MI, CHF, AmputationESRD, BlindnessQuality of Life, Adverse Events
BMJ 2016;352:i717 © 2015 Private & Confidential22
Effect of Anti-Hypertensive Treatment at Different Pre-treatment BP Levels in DM
Effect of Anti-Hypertensive Treatment at Different Pre-treatment BP Levels in DM
Increased all cause and CV mortality in patients treat for HTN when Baseline BP <140
© 2015 Private & Confidential23
Effect of Anti-Hypertensive Treatment at Different Post-treatment BP Levels in DM
All cause and CV mortality increased when post treatment BP <130 mg
© 2015 Private & Confidential24
Hypertension Update
• Patients with or at high risk for CVD benefit from more intensive BP control
Adverse events more commonTighter control requires more medication and intense monitoring
• Diabetic patients have higher total and CV mortality with more intense treatment
© 2015 Private & Confidential25
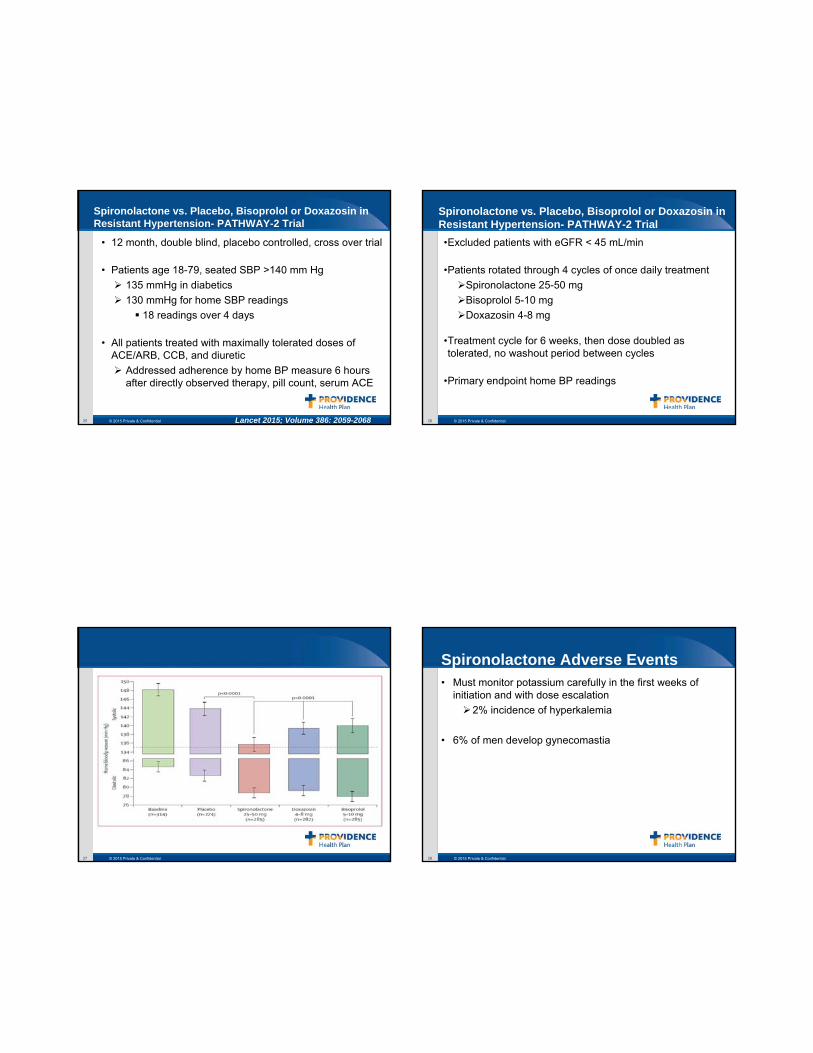
Spironolactone vs. Placebo, Bisoprolol or Doxazosin in Resistant Hypertension- PATHWAY-2 Trial
• 12 month, double blind, placebo controlled, cross over trial
• Patients age 18-79, seated SBP >140 mm Hg135 mmHg in diabetics130 mmHg for home SBP readings
18 readings over 4 days
• All patients treated with maximally tolerated doses of ACE/ARB, CCB, and diuretic
Addressed adherence by home BP measure 6 hours after directly observed therapy, pill count, serum ACE
Lancet 2015; Volume 386: 2059-2068 © 2015 Private & Confidential26
Spironolactone vs. Placebo, Bisoprolol or Doxazosin in Resistant Hypertension- PATHWAY-2 Trial•Excluded patients with eGFR < 45 mL/min
•Patients rotated through 4 cycles of once daily treatmentSpironolactone 25-50 mgBisoprolol 5-10 mgDoxazosin 4-8 mg
•Treatment cycle for 6 weeks, then dose doubled as tolerated, no washout period between cycles
•Primary endpoint home BP readings
© 2015 Private & Confidential27 © 2015 Private & Confidential28
Spironolactone Adverse Events• Must monitor potassium carefully in the first weeks of
initiation and with dose escalation2% incidence of hyperkalemia
• 6% of men develop gynecomastia
© 2015 Private & Confidential29
Deintensification of BP and Glucose Medication Treatment in Older Patients• Retrospective cohort study of 211,667 VA patients > 70
years old with DM and treated for hypertension
• Cohort stratified for BP and Glucose controlVery low
SBP < 120 mm Hg, HgBA1c < 6.0%Moderately low
SBP 120-129 or DBP < 65 mm Hg, HgBA1C 6.0-6.4%Not low
SBP > 130 or DBP >65 mm HG, HgBA1c ≥ 6.5%High
SBP > 140, DBP >90, HgBA1c ≥ 7.5%
JAMA IM Published online October 26, 2015 © 2015 Private & Confidential30
Deintensification of BP and Glucose Medication Treatment in Older Patients• 50% had very or moderately low BP
• 20% had very low or moderately low HgBA1c
• Most patients had life expectancy < 10 years
• Deintensification was uncommon and unrelated to life expectancy
• Most patients with low BP or HgBA1c did not have repeat measurements within 6 months
Implies that clinicians do not identify risk of overtreatment
© 2015 Private & Confidential31 © 2015 Private & Confidential32
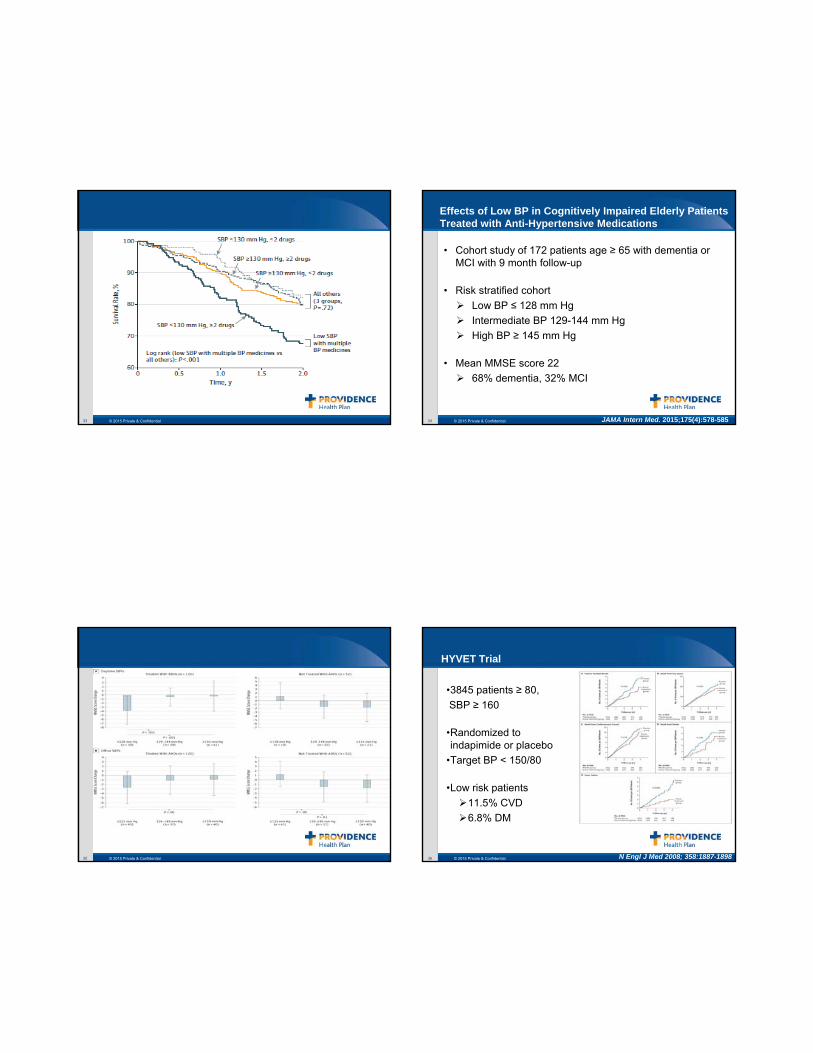
Treatment with Multiple BP Medications, Achieved BP and Mortality
• 1127 patients over age 80, residing in nursing homes
• Measured BP over 3 consecutive days
• Compared mortality in patients with SBP < 130 who received ≥ 2 anti-hypertensives with other participants.
JAMA Intern Med. 2015; 175(6):989-995
© 2015 Private & Confidential33 © 2015 Private & Confidential34
Effects of Low BP in Cognitively Impaired Elderly Patients Treated with Anti-Hypertensive Medications
• Cohort study of 172 patients age ≥ 65 with dementia or MCI with 9 month follow-up
• Risk stratified cohortLow BP ≤ 128 mm HgIntermediate BP 129-144 mm HgHigh BP ≥ 145 mm Hg
• Mean MMSE score 2268% dementia, 32% MCI
JAMA Intern Med. 2015;175(4):578-585
© 2015 Private & Confidential35 © 2015 Private & Confidential36
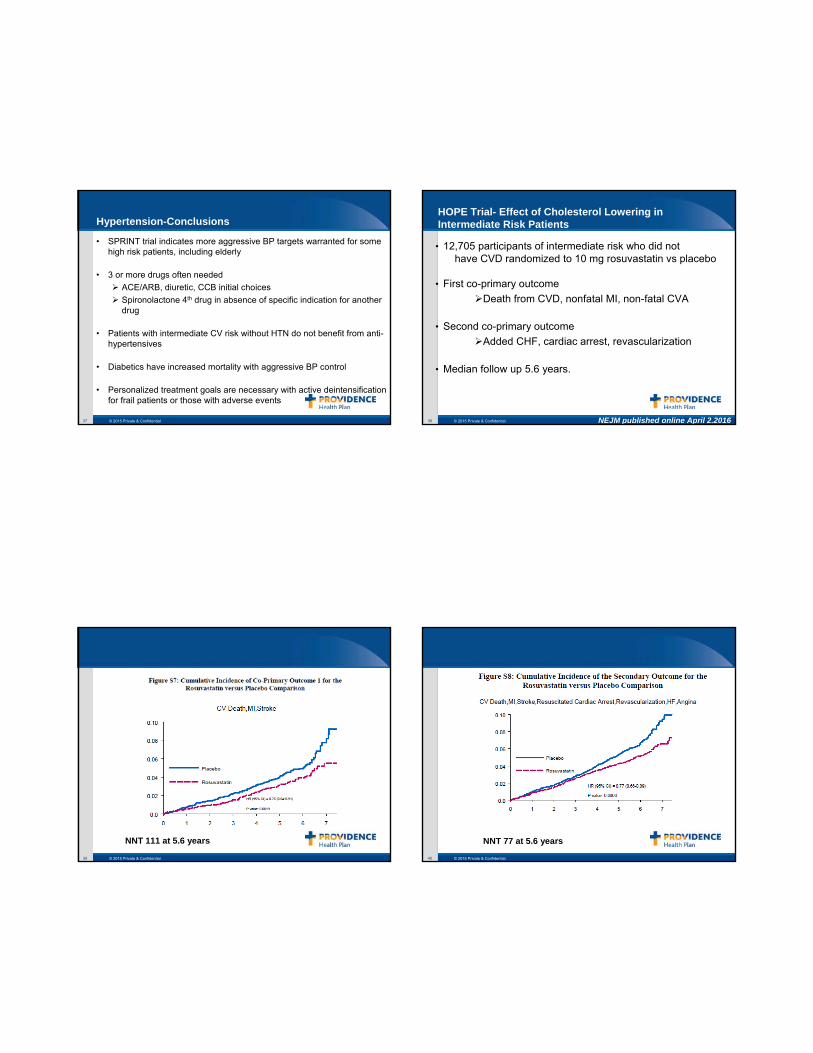
HYVET Trial
•3845 patients ≥ 80,SBP ≥ 160
•Randomized to indapimide or placebo
•Target BP < 150/80
•Low risk patients11.5% CVD6.8% DM
N Engl J Med 2008; 358:1887-1898
© 2015 Private & Confidential37
Hypertension-Conclusions
• SPRINT trial indicates more aggressive BP targets warranted for some high risk patients, including elderly
• 3 or more drugs often neededACE/ARB, diuretic, CCB initial choicesSpironolactone 4th drug in absence of specific indication for another drug
• Patients with intermediate CV risk without HTN do not benefit from anti-hypertensives
• Diabetics have increased mortality with aggressive BP control
• Personalized treatment goals are necessary with active deintensification for frail patients or those with adverse events
© 2015 Private & Confidential38
HOPE Trial- Effect of Cholesterol Lowering in Intermediate Risk Patients
• 12,705 participants of intermediate risk who did not have CVD randomized to 10 mg rosuvastatin vs placebo
• First co-primary outcomeDeath from CVD, nonfatal MI, non-fatal CVA
• Second co-primary outcomeAdded CHF, cardiac arrest, revascularization
• Median follow up 5.6 years.
NEJM published online April 2.2016
© 2015 Private & Confidential39
NNT 111 at 5.6 years
© 2015 Private & Confidential40
NNT 77 at 5.6 years
© 2015 Private & Confidential41
HOPE Trial- Effect of Cholesterol Lowering in Intermediate Risk Patients
• Patients at intermediate risk for CV disease have modest benefit from statin use
• Rosuvastatin will be available as a generic later this year
© 2015 Private & Confidential42
Statin Intolerance Due to Myalgias Can Be Resolved with Vitamin D Therapy• Some evidence that statin intolerance due to MSK symptoms
is associated with lower Vitamin D levels.
• Cohort of 146 patients with statin intolerance and Vitamin D levels < 32 ng/ml (mean 22ng/dl)
• Patients received Vitamin D 50,000-100,000 U/wk.
• 3 weeks after supplementation challenged with a statin (generally Rosuvastatin)
• Follow-up at 6,12 and 24 months-significant drop out• 88-95% of patients were myalgia free
International Journal of Cardiology Published online Oct 22, 2014
© 2015 Private & Confidential43
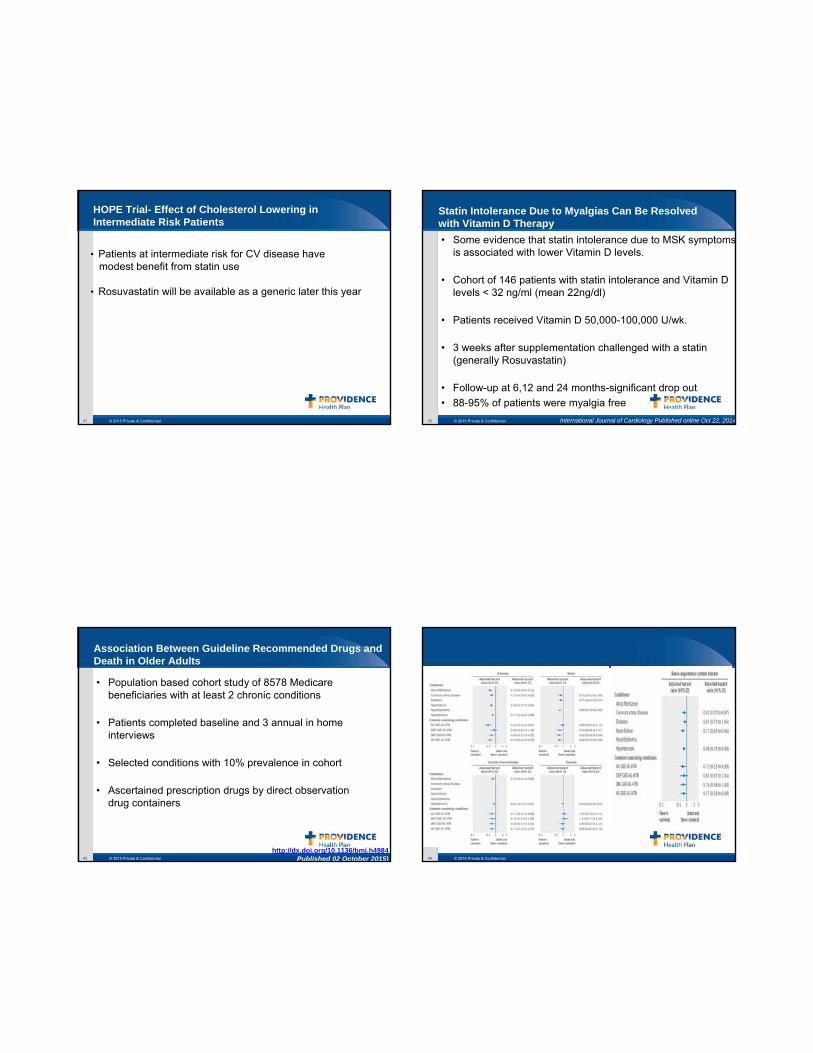
Association Between Guideline Recommended Drugs and Death in Older Adults
• Population based cohort study of 8578 Medicare beneficiaries with at least 2 chronic conditions
• Patients completed baseline and 3 annual in home interviews
• Selected conditions with 10% prevalence in cohort
• Ascertained prescription drugs by direct observation drug containers
http://dx.doi.org/10.1136/bmj.h4984Published 02 October 2015) © 2015 Private & Confidential44
© 2015 Private & Confidential45 © 2015 Private & Confidential46
Association Between Guideline Recommended Drugs and Death in Older Adults
• Guideline based therapy is effective in the elderly, especially for CVD drugs
• In this cohort, Clopidogrel, Metformin and SSRI’s did not impact mortality
© 2015 Private & Confidential47
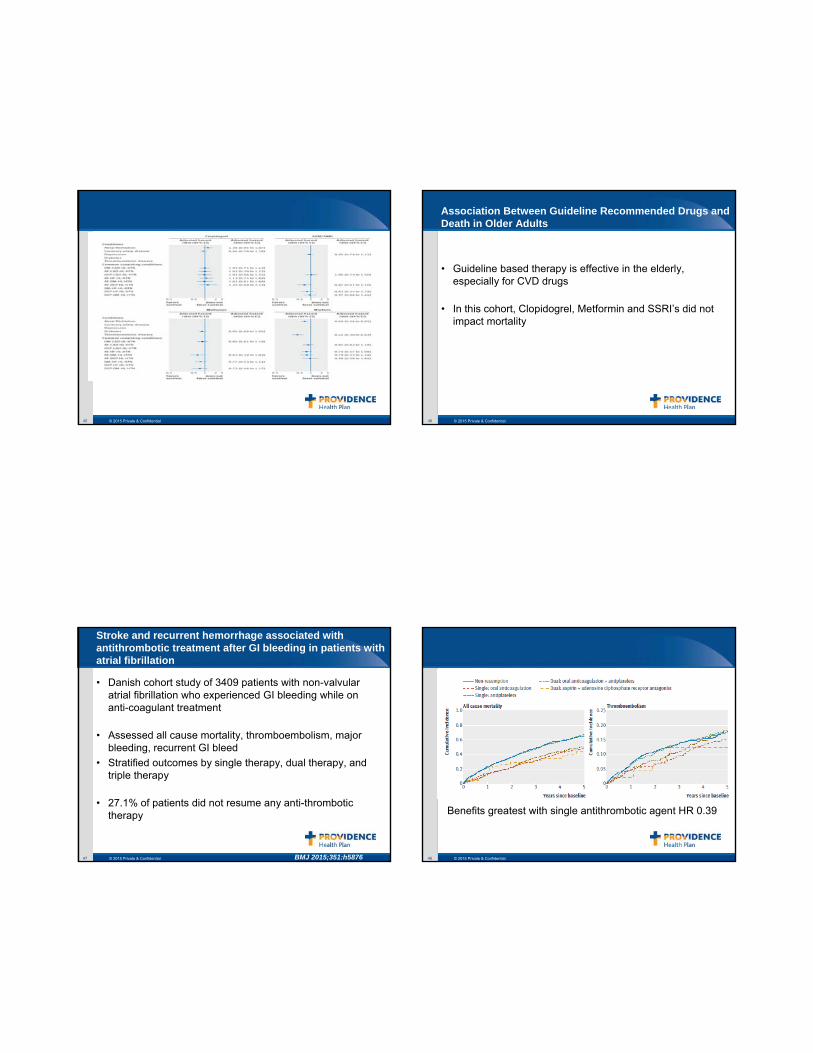
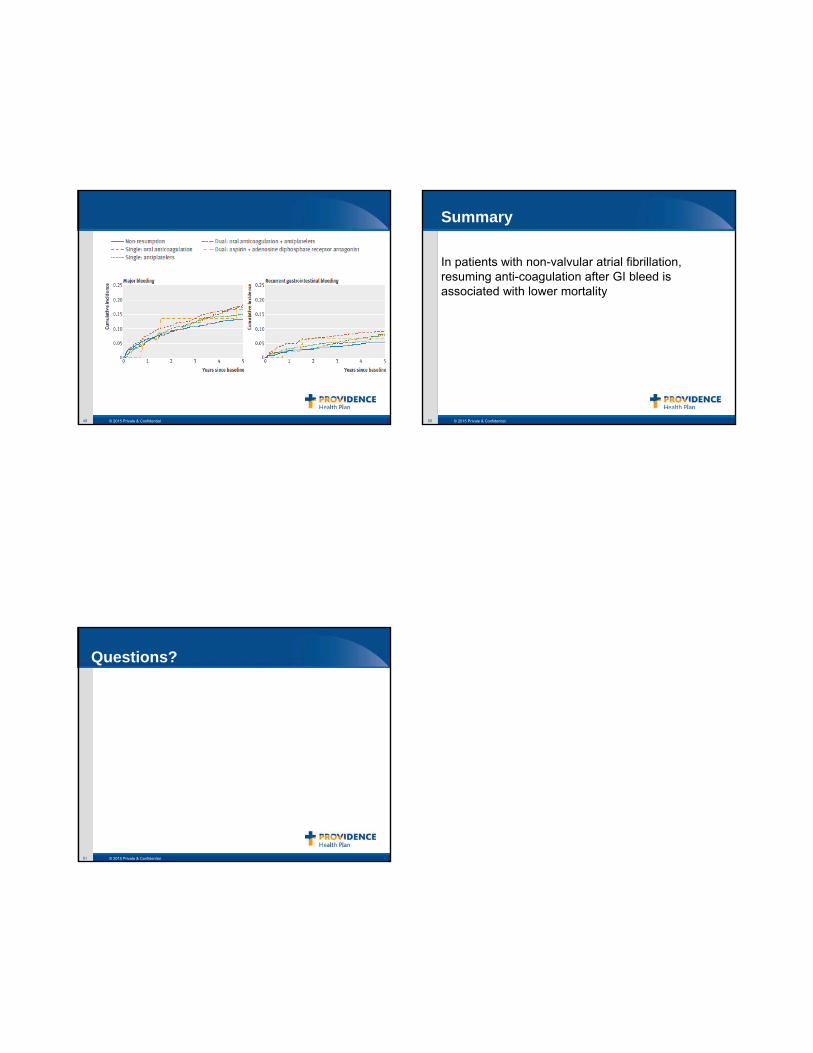
Stroke and recurrent hemorrhage associated with antithrombotic treatment after GI bleeding in patients with atrial fibrillation
• Danish cohort study of 3409 patients with non-valvular atrial fibrillation who experienced GI bleeding while on anti-coagulant treatment
• Assessed all cause mortality, thromboembolism, major bleeding, recurrent GI bleed
• Stratified outcomes by single therapy, dual therapy, and triple therapy
• 27.1% of patients did not resume any anti-thrombotic therapy
BMJ 2015;351:h5876 © 2015 Private & Confidential48
Benefits greatest with single antithrombotic agent HR 0.39
© 2015 Private & Confidential49 © 2015 Private & Confidential50
Summary
In patients with non-valvular atrial fibrillation, resuming anti-coagulation after GI bleed is associated with lower mortality
© 2015 Private & Confidential51
Questions?