Embed Size (px)
Citation preview
4/2/2013
1
Pediatric Orthopedic Trauma
Dan Hoernschemeyer, MDAssistant Professor, Pediatric Orthopaedics
Department of Orthopaedic Surgery; Univ of Missouri
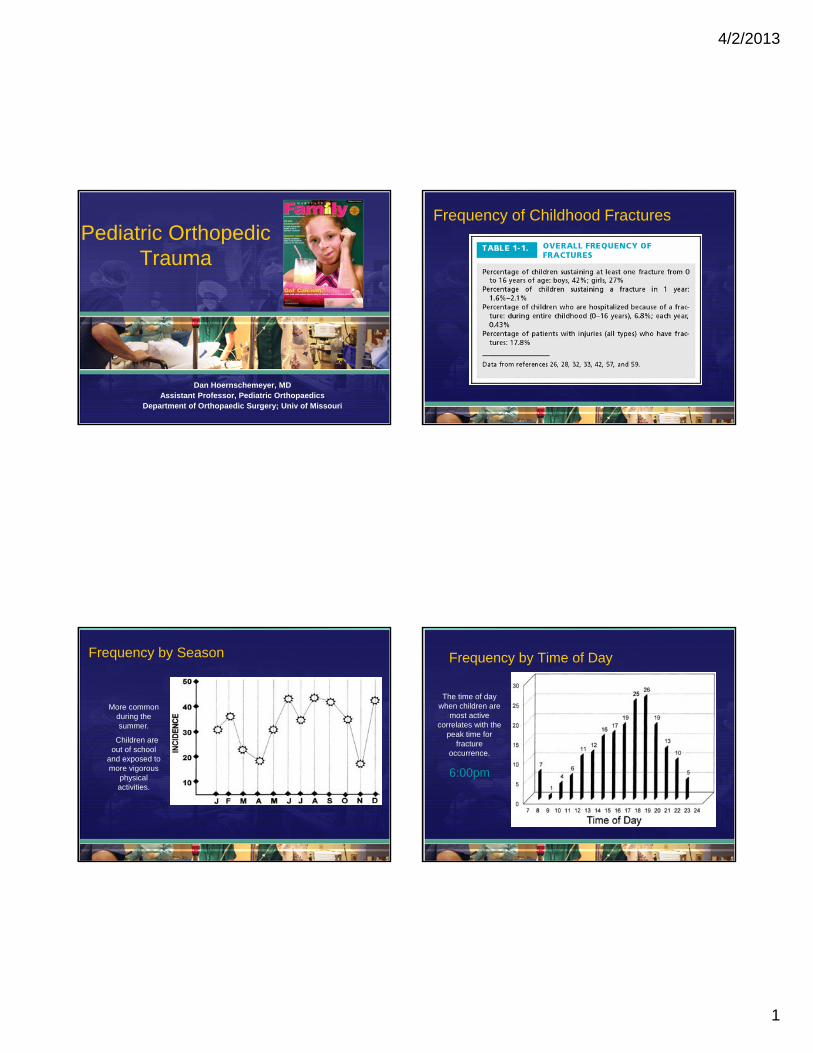
Frequency of Childhood Fractures
Frequency by Season
More common during the summer.
Children are out of school
and exposed to more vigorous
physical activities.
Frequency by Time of Day
The time of day when children are
most active correlates with the
peak time for fracture
occurrence.
6:00pm

4/2/2013
2
Specific Fracture Types Fractures Resulting from Accidental Trauma
• Playground– 90% were upper extremity fractures from a fall off
of monkey bars or climbing equipment– Change of playground surfaces
– concrete / dirt / rubber => bark (impact-absorbing)
• Skateboarding– Nature of skateboarding being high speed and
extreme maneuvers causes high-energy trauma fractures
• Roller Skates & In-line Skates– Most injuries involve elbow, forearm, wrist, and
fingers; < 20% use protective gear
Fractures Resulting from Accidental Trauma
• Trampoline– 1/3 of injuries result from falling off the trampoline
• Skiing– More than half of the injuries occur due to
collisions with stationary objects; i.e. trees, poles, stakes
• Snowboarding– Compared to skiers, snowboarders have 2-½
times as many fractures
4/2/2013
3
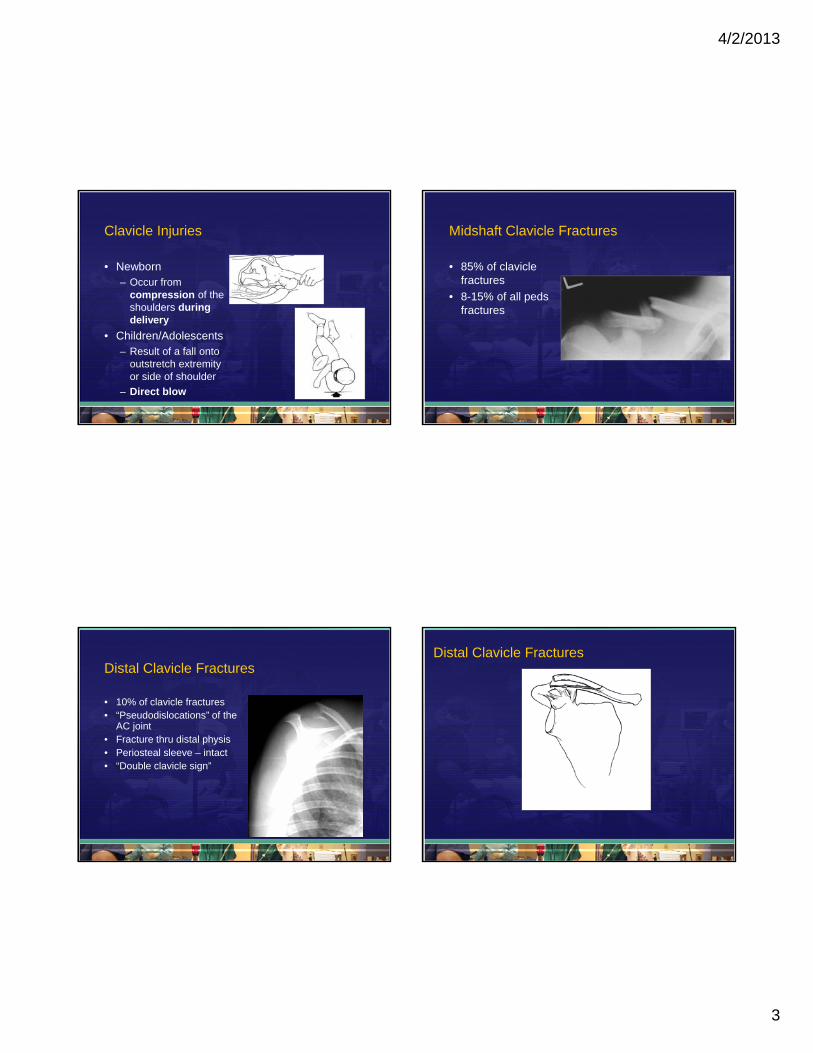
Clavicle Injuries
• Newborn– Occur from
compression of the shoulders during delivery
• Children/Adolescents– Result of a fall onto
outstretch extremity or side of shoulder
– Direct blow
Midshaft Clavicle Fractures
• 85% of clavicle fractures
• 8-15% of all peds fractures
Distal Clavicle Fractures
• 10% of clavicle fractures• “Pseudodislocations” of the
AC joint • Fracture thru distal physis• Periosteal sleeve – intact• “Double clavicle sign”
Distal Clavicle Fractures

4/2/2013
4
Distal Clavicle Fractures Clavicle Fracture Treatment
• Children and adolescents– Arm sling
– Figure-of-eight sling
Surgical Indications
• Displaced / shortened
• Open fractures
• Neurovascular injury
• Cosmetic reasons– “Trade a bump for a
scar”
Proximal HumerusGrowth Patterns
• Upper Extremity Growth occurs away from the elbow
• Humeral growth 80% proximal

4/2/2013
5
Extraordinary remodeling
potential of the proximal humerus
Treatment
• Accept any alignment if ≥ 2 yrs growth– Sling
– Sling and Swathe
– Hanging cast

4/2/2013
6
Humeral Shaft Fractures
• “If the bones are in the same room it will heal”
Elbow Fractures
• Supracondylar fractures (70%)
• Lateral condylar fractures (15%)
• Medial epicondylar fractures
• Radial head/neck fractures
• Transphyseal
• Olecranon
Pediatric Elbow Fractures• 5-10% of all fractures in children
• Distinguishing fractures from the six normal secondary ossification centers– Girls mature earlier than boys
Supracondylar Fractures
• 70% of all elbow fractures in children
• Average age: 6 y/o
• Anatomic predisposition:
– Ligamentous laxity
– Metaphyseal “remodeling”
– Thin cortex

4/2/2013
7
Dan Hoernschemeyer, MD
Classification
• Type I – nondisplaced or minimally displaced
• Type II – angulation with posterior cortex intact
• Type III – completely displaced
Dan Hoernschemeyer, MD
Vascular Injury
• Occurs 0.5-1%• Brachial artery
laceration/occlusion• m/c: posterolateral
displacement, open fx • Rely on clinical exam:
– Pale, non-viable vs. pink, viable
– Radial pulse?
• Suspect vascular compromise => direct surgical exploration
Neurologic Injury
• Occurs: 7%• AIN
– easily overlooked; currently felt to be m/c
• Radial nerve– felt to be m/c in past;
posteromedial displacement• Median nerve
– posterolateral displacement• Ulnar nerve
– common; olecranon pin traction; med. perc. pin
Type I Supracondylar Fractures
• Long arm cast– 4-6 weeks
• Sling is recommended
• Parents should be instructed on elevation of the extremity to reduce swelling – Fingers above the elbow
– Elbow above the heart

4/2/2013
8
Type II & III Supracondylar Fractures Type II & III Supracondylar Fractures
• Closed reduction– Percutaneous pinning
– Cast immobilization
Lateral Condyle Fractures
• Second most common elbow injury in children
Radiographic Findings
• AP radiograph may show little abnormality
• Oblique film – very important!

4/2/2013
9
Lateral Condyle Fracture
• Avoid unnecessary dissection, especially posteriorly => AVN
• Use 2 divergent or widely-spaced pins
Treatment Recommendations> 2mm or unreliable
• Reduced – percutaneous pin
• ORIF
Medial Epicondyle Fractures
• Average age: 9-12 y/o
• 4x boys > girls
• 3rd m/c fracture; fuse by 15 y/o
• Mechanism:– Acute avulsion by overpull of forearm flexor tendon
or ulnar collateral ligament
– Chronic tension stress injuries (Little League elbow)
Radiographic Findings
• Medial collateral ligament at base
• Entrapped epicondyle may be overlooked
Entrapped medial epicondyle fracture of 11 year old -AP/LAT at time of injury
CT Scan 5 weeks after injury shows entrapped med epicondyle

4/2/2013
10
Medial Epicondyle Fractures
• Nondisplaced and minimally displaced fractures <5mm– Immobilization in splint, 1-2 weeks
– Followed by early active range of motion exercises
• Open reduction and internal fixation– Overhead athlete; fragment in the joint
Radial Head/Neck Fractures
• Ossification starts ~ 4 years old
• Classification (Wilkins)– I: valgus fractures
– II: fractures with elbow dislocation
– III: Monteggia variants
Complications
• Stiffness – *greatest with ORIF
• Synostosis
• AVN
• Physeal Closure/valgus
*Due either to injury or treatment

4/2/2013
11
Nursemaid’s Elbow

4/2/2013
12
Monteggia FractureBefore Treatment
Monteggia FractureAfter Treatment
Shaft of Radius and Ulna Fracture
• 5-10% of children’s fractures• More common distally than
proximally• Closed treatment is usually
successful, remodeling is significant, and malunion is uncommon

4/2/2013
13
Distal Radius/Ulna Fractures
• Significant remodeling potential
• Well molded cast is key– Short arm
• Nondisplaced fracture
– Long arm• Requiring reduction
• Pin physeal fractures only if “unstable”
• Growth disturbance very rare
Fractures of the Lower Extremities
• Hip• Pelvic• Femur• Knee
• Tibial Spine• Tibial Shaft
• Patellar• Ankle
Pediatric Hip Fractures
• <1% of all hip fractures
• 60% complication rate is much higher than the complication rate in adults– AVN
– Coxa vara
– Premature physeal closure
– Leg length discrepancy

4/2/2013
14
Blood Supply
• Changes over time– At birth femoral head is supplied by vessels from
the medial and lateral circumflex artery
– As the physis develops the metaphyseal blood supply diminishes and the lateral epiphysealvessels supply the femoral head.
• Care then to avoid the pisiformis fossa and the posterior superior femoral neck.
Pediatric Hip Fracture
• High energy injury
• If not given that history then look for pathologic fracture– Fibrous dysplasia
– UCB
Treatment
• Screw fixation
• 2-3 or hip screw and side plate– Cross physis if necessary for stabilization
– Only 1mm of growth at the proximal physis per year!
• i.e. a 3 year old girl with 10 years of growth remaining will have a 1 cm LLD
Pediatric Hip Fractures

4/2/2013
15
Pediatric Hip FracturePelvic Avulsion Fracture
• Adolescent
• Playing in sports
• Powerful contraction of attached muscle
• Treatment:– Rest
– Guarded wt. bearing w/ crutches
Peds Femur Fractures-by age
• < 6 years: Fall
• 6-9 years: struck by vehicle
• 14-17 years: MVA (occupant)
Hinton et al JBJS 1999; 81:500-507
Falls and Child Abuse
• “Major” fracture- mechanism is questioned– Actually is a valid mechanism!
• Fractures reported due to falls from bed or couchare abuse only in ~5%
Hennrikus et al CORR 2003; 407:148
• Inability to walk is a strong predictor of abuse(42% vs 3%)
Schwend et al JPO 2000; 20:475-481

4/2/2013
16
Early Spica
• No scars
• No implant
• Early discharge
• Good results - especially in young children --relies on size, overgrowth, remodeling
Early Spica-disadvantages
• Hard to get around
• Difficult to manage polytrauma
Who should we place in a spica cast??
• Lighter weight patient
• Patients with home care arrangements
• Patients that require less time in cast
• When a tutor is not needed
Who should we place in a spica cast??
• New set of issues:– Potty trained??
– Attending day care, pre-K, or kindergarten??
– Obese child
– Primary caregiver:• Single parent?
• Two working parents?

4/2/2013
17
5 y/o boy with pathologic femur fracture

4/2/2013
18
Stabilizing Pediatric Femur Fractures
Skin Traction
r
Fractures about the Knee
• Ligamentous injuriesare rare
• Stress views help sort out ligamentous versus physeal injury
• Distal femoral physealinjuries are more common than proximal tibial injuries

4/2/2013
19
SH I Distal Femur Fractures
Pin using 2 smooth k wires that X above the growth plate and are aimed anteriorly in the sagittal plane 10 degrees
Concerns
• Vascular injury– Equivalent to a knee dislocation
• Nerve injury– Popliteal or peroneal
• Physeal Closure– > 50%
Tibial Spine Fractures
• ACL pulls off the tibial spine (incompletely ossified) instead of the tendon rupturing
• Initially - plastic deformation in the ligament; which is hard to repair
• McKeever Classification
Tibial Spine Fractures

4/2/2013
20
Tibial Tubercle Fracture
• 3 Types:– Type 1: Fx through the
ossification centre of the tuberosity
• Treatment: Casting– Type 2: Fx
w/comminution of the ossification centre
• Treatment: Surgical Management
– Type 3: Fx extending into the knee w/some displacement
• Treatment: Surgical Management
Treatment of Tibial Tubercle Fracture
Patellar Sleeve Fracture
• Avulsion of cartilaginous inferior pole of the patella
• Diagnosis– High riding patella
– Loss of knee extension
– Gap to palpation at the inferior pole
Patellar Sleeve Fracture
• 8-12 y/o children
• Sleeve:– Articular cartilage,
periosteum, and retinaculum
• Surgical treatment:– > 3mm displacement
– Disrupted extensor mechanism

4/2/2013
21
Patellar Sleeve FractureProximal Tibial Metaphyseal Fractures
• Cozen fracture
• Will grow into a valgus deformity (1yr)
– Overgrowth medially
– Tethering of fibula• Expect spontaneous
correction
Tibial Shaft Fractures
• About 70% of tibial shaft fractures in children have an intact fibula
• Account for 4% to 5% of all pediatric fractures
• Occur most commonly in boys (3-4 and 15-16 y/o)
• Third most common long bone fracture in kids
Tibial Shaft Fractures
• Treatment:– Casting
– Pins and plaster
– External Fixator
– Flexible IM nails

4/2/2013
22
Toddler Fracture
• 18-24 months old
• Trip and fall
• Refusal to bear weight
• External rotation injury
• Distal third spiral fracture
Distal Tibia Physis Fractures
• Treated with closed reduction and long leg cast
• Displacement:– Acceptable => younger ; anteroposterior plane
– Adolescent with valgus/varus angulation• Cannulated screw or K-wire
• Periosteum / fibula => block reduction!
Principles of Distal Tibial Growth
• Distal tibia ossific nucleus– Appears => 2 – 3 y/o– Fuses:
• Girls => 15 y/o• Boys => 17 y/o
• Fuses central to medial and then lateral over 18 months!
• Distal fibula ossific nucleus– Appear => 2 y/o– Fused => 20 y/o
• Secondary ossification centers
Tillaux Fractures
• Older adolescent
• Physis:
– Medial => closed; Lateral => open
• Fracture runs though the physis, across the epiphysis, and into the joint
• Fracture fragment => anterior due to the anterior tibiofibular ligament
• Internal rotation => reduction

4/2/2013
23
Triplane Fractures
• Two-part or three-part fractures
• Fracture pattern: coronal, transverse, sagittal
• Closed reduction:– Internal rotation; very
difficult
Triplane Fracture
Triplane Fracture Triplane Fracture

4/2/2013
24
Thank You!!

1
Evaluation and Management of Idiopathic Scoliosis
_______________________________________________________________
Dan Hoernschemeyer, MD
Assistant Professor, Pediatric Orthopaedics
Department of Orthopaedic Surgery
University of Missouri - Columbia Dan Hoernschemeyer, MD
Scoliosis
• Lateral curvature of the spine (coronal)
• Three dimensional:– Sagital plane
– Vertebral rotation (axial plane)
• True Scoliosis: Cobb angle > 10°
Dan Hoernschemeyer, MD
Prevalence
• 2% - 3% for curves >10°
• 0.3% for curves >20°
• 0.1% for curves >40°
• Female to male ratio:– curves 11° - 20° (1.4:1)
– Curves > 20 (5:1)
• Males are much less likely to progress
Faternal Twins
Dan Hoernschemeyer, MD
57 degrees 30 degrees

2
Etiology
• Genetic component but most likely multifactorial
• Many other factors implicated but not proven:
- Melatonin deficiency
- Growth hormone
- Asymmetric spinal growth
- Increased platelet calmodulin
- Vestibulo-ocular system dysfunction
Adolescent idiopathic scoliosis. Monograph Series 28.
Dan Hoernschemeyer, MD
• Anterior spinal growth outpaces posterior spinal growth
Dan Hoernschemeyer, MD
Etiology
• Genetic Testing for Idiopathic Scoliosis:– Axial Biotech
• Scoliscore AIS Prognostic Test– DNA-based testing
» 53 genetic markers associated w/ severe curve progression (SNPs)
» SCORE: 1 - 200
» < 50 = low risk; > 180 = high risk
– Launched: 12/08
– Dr. James Ogilvie – chief investigator

3
Dan Hoernschemeyer, MD
Idiopathic Scoliosis
• Types include:– Infantile: 0 to 3 years of age
– Juvenile: 4 to 9 years of age
– Adolescent: 10 years of age to maturity
Infantile Idiopathic Scoliosis
• Boys (3:2)• Convex left curves (75%)• Uncommon – 1% in USA • Associated with:
– Plagiocephaly (72%)– DDH
• Postnatal positioning• Resolves in 90%
– RVAD < 20
• MRI for curves>20°
Infantile Idiopathic Scoliosis
Dan Hoernschemeyer, MD
Juvenile Idiopathic Scoliosis
• 4 - 9 year olds
• Neural axis anomalies (15-26%)– MRI for curves > 20°
• More aggressive than AIS
• Rare spontaneous resolution
• 100% need for surgery for curves
> 30° before puberty
Charles et al. Spine, Vol 31 (17). 2006Dobbs et al. JBJS, 84. 2002

4
Dan Hoernschemeyer, MD
School Screening
• Identify body asymmetry
• Forward bend test
• Value is often debated
• Referral rate:– 3.4 – 30%
Dan Hoernschemeyer, MD
Dan Hoernschemeyer, MD
Scoliometer
Dan Hoernschemeyer, MD
False Negatives
• 5 degrees => 100% sensitive; 47% specific
• 7 degrees => 83% sensitive; 86% specific

5
Natural History
• Curves > 30° before maturitytend to progress
• Curves ≥ 50° at maturity tendto progress ~ 1°/year into adulthood
• Curves ≥ 80°: VC < 65%
Weinstein et al. JBJS 1981; 63: 702Weinstein et al. JBJS 1983; 65: 447
Dan Hoernschemeyer, MD
Natural History
• Skeletally Immature– Age
• The younger you are the greater the risk of progression
– Curve Magnitude
• Larger curve => greater risk of progression
Dan Hoernschemeyer, MD
Natural History
• Skeletally Immature– Sex
• Females have a greater risk of progression
• Curves > 20° (5:1)
– Type of Curve• Thoracic >>> Lumbar
• Double curves >>> Single curves
Dan Hoernschemeyer, MD
Pulmonary Function
• Thoracic curves:
– Curves > 60° => 68% TLC (usually asymptomatic)
– Curves > 100° => 50% TLC (symptomatic)
• No correlation between:– Thoracolumbar / Lumbar curves and pulmonary
function

6
Dan Hoernschemeyer, MD
Back Pain and Scoliosis
• Present 23% at time of initial evaluation*– 9% will have an identifiable cause*
• Identifiable causes:– Spondylolysis – Scheuermann’s disease– Disk, syrinx, or tumor
• Extensive initial work up not indicated!!!*Ramirez et al. JBJS 1997; 79: 364
Dan Hoernschemeyer, MD
Clinical Evaluation
• Cutaneous lesions
• Gait
• Neuro exam, reflexes
• Limb length inequality
Dan Hoernschemeyer, MD
Clinical Evaluation
• Shoulder height
• Alignment– Plumb line
• Trunk Shift
• Rotation– Rib or scapula prominence
• Sagital deformity
Dan Hoernschemeyer, MD
Radiographs• Not indicated => minor
curve
• Standing 36” PA film from T1-S1
– Less XRT on breast tissue
• Lateral film– curve looks abnormal or
for preoperative purposes

7
Dan Hoernschemeyer, MD
Cobb Angle
Dan Hoernschemeyer, MD
Are we skeletally mature??
• Risser Sign
• Tanner Stage
• Peak height velocity
• Triradiate cartilage closure
• Menarchal age
• Tanner-Whitehouse stages
Skeletal Maturity??
• 14 y/o female– 30 deg curve
– Just started menses
– Risser 4

8
King-Moe Classification
Mainly a thoracic curve classification w/ no reference to sagittal balanceDan Hoernschemeyer, MD
No Treatment
• Curves <25°
– Immature patients (Risser 0-2): Follow up in 4 to 6 months
– Mature patients (Risser 4-5): Follow up not needed
• Curves 25° to 45° in (Risser 4-5) girls: Re-evaluate in 1 year
Dan Hoernschemeyer, MD
Brace Indications
• Curves 25°-45° (Risser 0-1):– Brace on initial evaluation
• Curves 25°-30° (Risser 2-3): – Brace if documented progression >5°
• Curves 30° -45° (Risser 2-3):– Brace on initial evaluation
– Brace treatment for curves >40° to 45° has a lower success rate
Dan Hoernschemeyer, MD
Boston Brace Milwaukee Brace

9
Dan Hoernschemeyer, MD
Boston Brace
• Introduced (1971)
• Low-profile brace
• Prefabricated
• Created from the full length x-rays
• Not effective:– Curves above T7
Boston Brace
Prevents progressionDoesn’t make better
Charleston Brace
Best for thoracolumbar and lumbar curves
(Night-time bending brace)
Katz et al. Spine 1997; 22: 1302
Brace Regimen• 23 hours per day is ideal
- Recent SRS meta-analysis revealed dose
dependent response (Rowe et al. J Bone & JointSurg; 78: 1997)
• 16 to 23 hours may have some benefit (Green N. JBJS 1986; 68: 738)
• Continue until maturity:– 2 years post-menarche– Risser 4 in females, Risser 5 in males– No significant gain in height
• Not that effective in males (Karol. Spine 2001; 26: 2001)

10
Treatment
• Surgical
- Skeletally immature w/ curves > 40-50°
- Skeletally mature w/ curves > 50°
* Exception may be well balanced
curves
- Use clinical judgment as well.
Fixation devices
Pedicle screws Hooks
13 y/o female
Dan Hoernschemeyer, MD
50 degrees
Post-op
Dan Hoernschemeyer, MD

11
54 degrees; 40 degrees
Selective thoracic fusion
• Originally recommended by King and Moe
for type II curves (JBJS 1983; 65: 1302)
• Decompensation of the lumbar curve common due to failure to identify double major curves (Spine 1990; 15: 927)
• Current criteria (Spine 1992; 17: S274)
1) Thoracic/Lumbar Cobb ratio > 1.2
2) Thoracic/Lumbar AVT ratio > 1.2
3) Thoracic/Lumbar AVR ratio > 1.0
Selective thoracic fusion
PSF T3-12
Anterior Spinal Fusion
• Anterior or Posterior?- Early enthusiasm for ASF * Saving fusion levels* ASF ideal for hypokyphosis
- Enthusiasm diminishing w/ use of pedicle screw
Potter et al. Spine 2005; 30: 1859

12
14 y/o female
Dan Hoernschemeyer, MD
57 degrees
Post-op
Dan Hoernschemeyer, MD
EOS Growing Rods
13
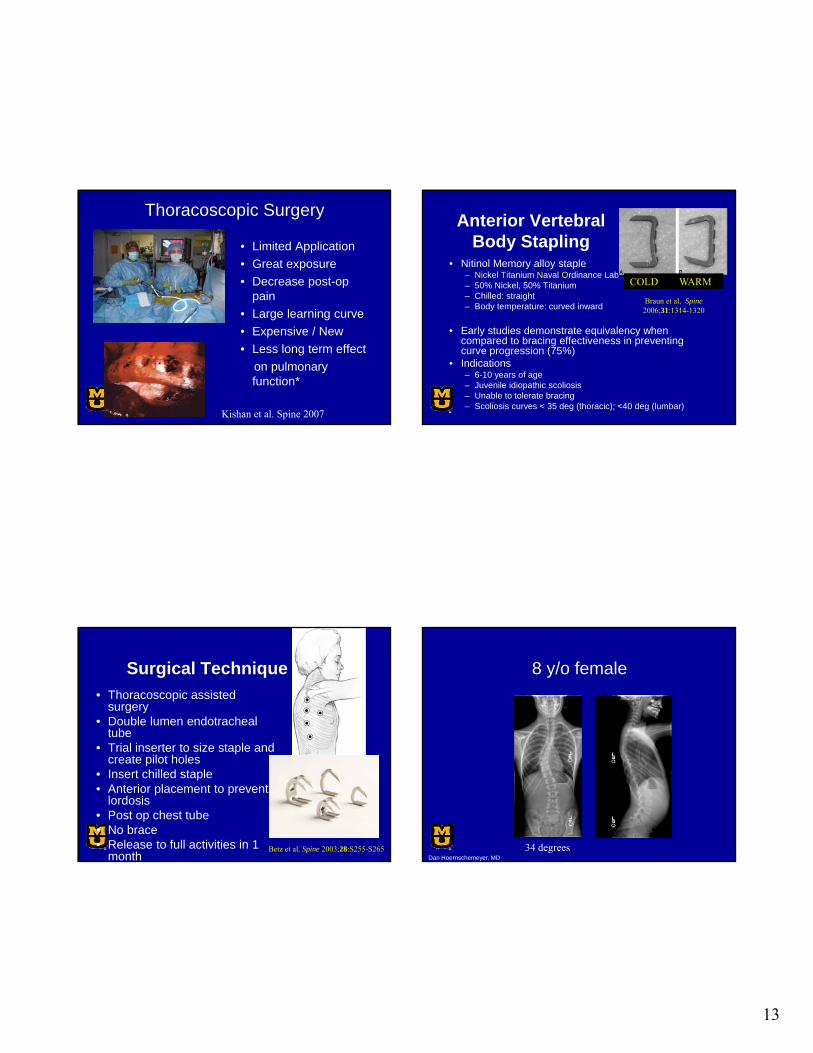
Thoracoscopic Surgery
• Limited Application
• Great exposure
• Decrease post-op pain
• Large learning curve
• Expensive / New
• Less long term effect
on pulmonary function*
Kishan et al. Spine 2007
Anterior Vertebral Body Stapling
• Nitinol Memory alloy staple– Nickel Titanium Naval Ordinance Lab– 50% Nickel, 50% Titanium– Chilled: straight– Body temperature: curved inward
• Early studies demonstrate equivalency when compared to bracing effectiveness in preventing curve progression (75%)
• Indications– 6-10 years of age– Juvenile idiopathic scoliosis– Unable to tolerate bracing– Scoliosis curves < 35 deg (thoracic); <40 deg (lumbar)
Braun et al, Spine 2006;31:1314-1320
COLD WARM
Surgical Technique
• Thoracoscopic assisted surgery
• Double lumen endotracheal tube
• Trial inserter to size staple and create pilot holes
• Insert chilled staple• Anterior placement to prevent
lordosis• Post op chest tube• No brace• Release to full activities in 1
monthBetz et al, Spine 2003;28:S255-S265
8 y/o female
Dan Hoernschemeyer, MD
34 degrees

14
Post-op
Dan Hoernschemeyer, MD Dan Hoernschemeyer, MD
• Thank You

4/2/2013
1
INTOEING AND OUTTOEING
Rotational Deformities of the Lower Extremities AKA
NORMAL DEVELOPMENT
The tibia in a newborn is internally rotated and should gradually externally rotate as the child matures. It is a gradual process and should gradually externally rotate to around 10 degrees of external rotation by 8 years of age with a mean of 15 degrees at maturity.
NORMAL DEVELOPMENT
At birth, femoral anteversion is around 30 degrees and gradually decreases to around 10 degrees by maturity.
Most newborns have an outtoeing exam. This is usually due to an external rotation contracture of the hip that should spontaneously resolve typically by the time they are standing or walking.
4/2/2013
2
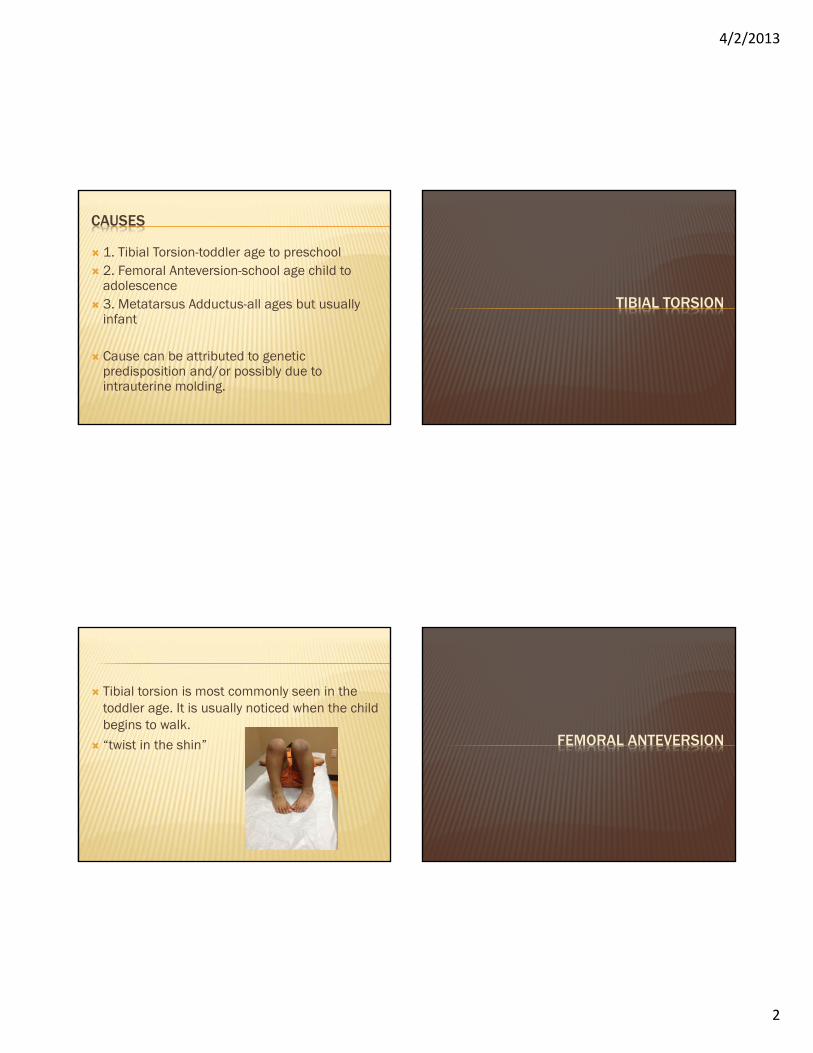
CAUSES
1. Tibial Torsion-toddler age to preschool 2. Femoral Anteversion-school age child to
adolescence 3. Metatarsus Adductus-all ages but usually
infant
Cause can be attributed to genetic predisposition and/or possibly due to intrauterine molding.
TIBIAL TORSION
Tibial torsion is most commonly seen in the toddler age. It is usually noticed when the child begins to walk.
“twist in the shin” FEMORAL ANTEVERSION

4/2/2013
3
It is commonly seen in the older child. These children are frequently described as
comfortably sitting in the “W” position “twist in the hip” METATARSUS ADDUCTUS
Lateral border of the foot is curved instead of straight
“twist in the foot” or sometimes referred to as “1/3 clubfoot”- the forefoot turns in but not the hindfoot; no equinus
About 1% of infants may have this May be due to intrauterine crowding Can be seen in association with Developmental
Dysplasia of the hip (DDH)

4/2/2013
4
DIAGNOSIS
EXAMINATION
This will include a rotational profile exam and an exam of the child’s gait
Rotational Profile exam includes: Foot exam, Thigh-foot angle, Hip exam, and foot progression angle.
I also like to watch the child and how they ambulate and play in the exam room while I am obtaining their history.
METATARSUS ADDUCTUS
Foot exam- Examine the lateral border of the foot and check the heel bisector line.
A normal heel bisector line falls in between the second and third toe.
If it falls at the 3rd toe then they have mild metatarsus adductus.
If it falls at the 4th toe, it is moderate and 5th
toe means it is severe.

4/2/2013
5
The foot should also be checked for flexibility This will classify the foot as either actively
correctable, passively correctable, or rigid. Actively correctable feet straighten out when
the lateral border of the child’s foot is stroked by the examiner’s finger. This causes the muscles of the foot to contract correcting the foot shape to neutral position
The passively correctable foot straightens with gentle manipulation.
The rigid foot does not. Also in the metatarsus adductus foot the space
between the first and second toe may appear wide, especially when standing.
The ankle joint and heel alignment are normal
TIBIAL TORSION
Check the Thigh-foot angle The thigh-foot angle will help determine the degree of tibial torsion and if it is internally or externally rotated.
Let the foot fall in its natural position when assessing this.
While walking, these children’s knees tend to point out but the feet point in.
Occasional tripping may be reported with this condition.

4/2/2013
6
FEMORAL ANTEVERSION/RETROVERSION
Check internal and external rotation of the hips Make sure the pelvis is stabilized during this exam so that the exam is more accurate.
It may take two people perform this. I utilize the parents help as needed.
Internal rotation close to 90 degrees and external rotation less than 15 degrees is abnormal.
When these kids walk, their knees and feet may look like they point in (anteversion).
They may also kick their feet out to the side when running.
IN GENERAL
Check the foot progression angle while walking

4/2/2013
7
This is the angle between the long axis of the foot and a line of the forward direction of gait.
The foot progression angle is a summation of the rotational alignment of the leg.
The remainder of the exam then attempts to identify the level of the rotation.
I also try to do a thorough hip exam and examine the spine for any scoliosis or defects.
This is also a good time to look for any neurological issues/diseases. The neonatal and developmental history will assist in this.
GENERAL TREATMENT
TREATMENT
Educate, educate, educate….. Observation and explanation to the family that
it may take several years to improve/resolve. Bracing is cumbersome and has no value. If there is still functional or cosmetic concern
then surgery may be an option after the child is older, >10 years.

4/2/2013
8
Study published in the Journal of Pediatric Orthopaedics July-August 1996 that looked at 100 high school students and the relationship between sprinting ability and intoeing.
The findings suggested that a low-normal TFA and intoeing while sprinting may correlate with enhanced sprinting ability.
I use this article to help educate the parents and hopefully reduce some of their anxiety
TREATMENT FOR METATARSUS ADDUCTUS
The actively correctable foot does not require treatment and tends to correct spontaneously in the first 2 years of life. Reassurance and education for the family is important.
The passively correctable foot may or may not respond to stretching exercises. Observation vs. stretching vs. casting is controversial.
The rigid foot may be treated with serial casting. This tends to be more effective in the infant age. If indicated, it may also be treated surgically in the older child.
ADDITIONAL INFORMATION
ROTATIONAL MALALIGNMENT SYNDROME
This usually includes external tibial torsion and femoral anteversion (internal rotation).
It can cause patellofemoral tracking issues and pain.
It is also more likely to require operative intervention.

4/2/2013
9
ANY CONCERNS-REFER TO PEDS ORTHO
THANKS!Kelly Scott,MSN,RN, FNP-BCNurse Practitioner in PediatricOrthopaedics, University of Missouri
REFERENCES
Orthopaedic Surgery Essentials. (2004). Pediatrics.Philadelphia: Lippincott Williams and Wilkins.
Staheli, L. T. (2006). Practice of Pediatric Orthopedics.Seattle: Lippincott Williams and Wilkins.
Texas Scottish Rite Hospital for Children. (2008). Tachdjian's Pediatric Orthopaedics 4th ed. Philadelphia: Saunders.
Fuchs,R & Staheli, L. Sprinting and Intoeing. Journal of Pediatric Orthopaedics: July/August 1996, pp.489-491.

4/2/2013
1
History• When, gradual or abrupt, where, how frequent?• Was there an injury associated with it?• Worsening with time? • Severity?• Interference with play/sports**• Who’s concerned: parent, grandparent,neighbor, therapist?
• Weight loss?
Physical‐ Palpation‐ ROM & Flexibility‐Gait* Antalgic (Fracture)* Trendelenburg (DDH, LCP, SCFE)* Proximal Muscle weakness (DMD)* Spastic Gait (CP)* Short limb gait (LLD)

4/2/2013
2
Transient Synovitis Septic Arthritis Developmental Dyplasia of the Hip (DDH) Legg‐Calve‐Perthes Disease Osteomylitis Slipped Capital Femoral Epiphysis (SCFE)
Inflammatory Synovitis Common cause of limping Seen most often in children 3‐8 y/o Often a history of precursor viral illness Hip most often affected They may have pain, stiffness, altered weight bearing
Labs usually normal (CBC, CRP, Sed rate) Treat with rest, observation, and NSAIDS (scheduled ibuprofen)
Improvement usually dramatic Signs and symptoms usually resolve over several days with the average duration being 10 days

4/2/2013
3
Urgent medical management due to the potential for significant joint destruction
Possible history of precursor mild trauma or concurrent infection/illness
Usually febrile systemic illness The child usually holds the affected extremity immobile
May have swelling of the joint, redness, warmth and tenderness to palpation
More ill appearing than transient synovitis Labs elevated (check CBC, Sed rate, CRP and blood cultures)
Treatment: Plain xrays, Admit to hospital, Ultrasound, joint aspiration to identify causative organism, antibiotics, low threshold for I &D if suspicious
Kocher criteria1) Temp > 38.52) Refusal to bear weight3) WBC > 12K4) ESR > 40
1 present – 3% (9%) 2 present – 40% (35%) 3 present – 93% (72%) 4 present – 99% (93%)Kocher et al. JBJS 1999; 81: 1622Kocher et al. JBJS 2004; 86: 1629
History:‐ Family history, breech, torticollis, foot deformities
Abnormal gait pattern:‐Trendelenburg gait – weakened abductor muscles
Other PE findings:‐ Shortened extremity, asymmetrical thigh folds, limited abduction,
Klisic test, hyperlordotic
Radiograph: order AP, Frog lateral pelvis, US in infant < 6mo‐Acetabular dysplasia, subluxation, dislocation

4/2/2013
4
Treatment ranges from Pavlik harness to surgery.
Refer to ortho
Hip disorder that causes collapse of the femoral head
May have a history of trauma Most prevalent in children 4‐12 y/o with boys > girls
Pain may be in hip, groin, or referred to thigh or knee
Often present with a limp that is exacerbated by physical activities and alleviated by rest
Hip range of motion is stiff

4/2/2013
5
X ray: AP and Frog lateral of the pelvis Treatment varies from rest to surgical treatement
Refer to Ortho
Classic history:
‐Minor trauma
‐Doing well for 1‐3 days
‐Increasing pain, swelling, not using extremity
Occurs in the metaphysis Most common sites:‐Distal humerus, distal radius, proximal femur, distal femur, proximal tibia
Acute‐produces local pain, swelling, warmth, erythema and tenderness, may have systemic symptoms
CRP and ESR usually elevated, check blood cultures too
Order x rays A bone scan may help localize the site of involvement if this is unclear
A MRI may be helpful to localize any abscess
Subacute‐An infection with duration longer than 2‐3 weeks
Often residual of acute osteo that has been contained but not eradicated
May have local swelling, warmth and tenderness
May present with a limp X‐ray changes: (7‐14 days) Periosteal reaction, periosteal elevation (abscess)

4/2/2013
6
Chronic osteomylitis‐untreated acute osteo
Treatment for Osteomylitis‐ Refer to ortho, aspiration or drainage of abscess, medical management if no abscess
Displacement between the proximal femoral epiphysis and metaphysis
Common adolescent hip disorder Can be acute or gradual Typically seen in boys 12‐15 y/o or girls 10‐13 y/o with boys > girls
Present with pain usually in the hip, groin, thigh or knee
Risk factors: Overweight, African American race, underlying endocrine disorders
Always think of the hip if they are presenting with knee pain
Decreased internal hip rotation May have an outtoeing gait on the affected side
Risk of contralateral involvement 20‐60%
X ray: Order AP and Frog lateral PelvisTreatment: Surgery and possible prophylacticfixation of the other side if necessary

4/2/2013
7
Juvenile Rheumatoid Arthritis Cerebral Palsy Muscular Dystrophy Fractures/ Injuries Leg Length Discrepancy Leukemia/Neoplasms Discitis /Back Pain Tarsal Coalition
Kelly Scott, RN, MSN, FNP‐BCNurse Practitioner Pediatric OrthopaedicsUniversity of Missouri





























