Embed Size (px)
DESCRIPTION
astra implants
Citation preview

Mandibular OverdenturesStabilized by Astra Tech Implants
with Either Ball Attachments orMagnets: 5-Year Results
David M. Davis, BUS, PhD, FDSRCS'Mark E. Packer, BDS, MPhii, FDSRCS''
Purpose; The purpose of this work was to report on the use of implant-stabilizedoverdetitures iti the mandible using the Astra Tech implant system with either ballattachments or magnets as the retentive mechanism. Materials and Methods: Mandibularoverdentures that used ball attachments on 2 implants were provided for 13 edentulouspatients; 12 edentulous patients were provided with mandibular overdentures withmagtiet retention, using 2 implants in 10 patients and 3 implants in 2 patients. Once theywere comfortable, the participants were placed on annual recall. Any other visits wereinitiated by the patients. Detaiied records were kept for all visits. At the annual recall thefollowing parameters were monitored: plaque levels, mucosal health, marginal bonelevels, and the patients' assessment of the treatment. The patients were followed for 5years. Results: There was no statistical difference between the 2 groups for mucosalhealth and postinsertion maintenance. The magnet group had more abutment sutfacescovered with plaque. Statistical analysis of the patients' subjective assessment of theirtreatment showed that the magnet group was less comfortable and chewing was lesseffective. Conclusion: The results indicate that both ball attachments and magnets usedon isolated Astra Tech implants in the mandible are viable treatment options. Bothattachment mechanisms provided patient satisfaction, although the ball attachments werebetter in this respect than the magnets. Int j Prosthodont 1999:12:222-229,
Implant-stabilized overdentures have been shown toprovide a successful long-term outcome, particularly
when used to restore the edentulous mandible.'"^^ Avariety of implant systems has been used, including theBrânemark system (Nobel Biocare),^'^'^'^"''^ the ITIsystem (Straumann),^''°''i the IMZ system (Steri-Oss),'''-''and the Astra Tech system (Astra Tech).^"^ The success
'Senior Lecturer and Honorary Consuitant. Department ofProsthetic Dentistry, The Dental institute. King's Coiiege Schoolof Medicine and Dentistry, London, England.''Lecturer. Department of Prosttietic Dentistry, The Dentai Institule,King's College School of Medicine and Dentiitry, London. Engiand.
Reprint requests: Dr David Dayis, The Dental institute. King'sCollege Sci^ool of Medic me and Dentistry, Caldecot Road, LondonSES 9RW, England, UK. Fax: + 17U346-37F5.
rates for these studies are very similar, as judged by sur-vival of the implants. In a review of 37 overdenturestudies, Batenburg et aP^ reported only 2 studies thatdid not have success rates of 90% or greater.
The most widely reported attachment mechanismis the linked bar, although ball attachments and mag-nets are also used. In a review by Batenburg et a l "34 of the studies used implants linked with a bar at-tachment and 21 used unlinked implants. Tbe mostcommonattachment used for unlinked implants is theball attachment,'^''''^"'^ with relatively few usingmagnets.•''•''̂ No difference has been reported amongthe different attachment mechanisms for success ratesin the mandible as measured by survival of the im-plants.''"*'^''^ Naert and coworkers^'^" used all 3 at-tachments. Tbey reported tbat the bar attachment
I of ProBtliodontics 222

Davis/Packer Astra Tech Implants with Ball or Magnet Attachments
was technically the most demanding compared tounlinked implants. However, from a maintenancepoint of view the bar was less demanding and pro-vided better patient satisfaction with the treatment.
The purpose of this study was to report on the useof implant-stabilized overdentures in the mandibleusing either magnets or ball attachments as the re-tentive mechanism. This article presents the 5-yeardata from this continuing prospective study.
Materials and Methods
Patients
A total of 25 edentulous patients participated in thisprospective study. All participants gave a history ofdifficulty in wearing a conventional completemandibular denture. The complaint had been presentfor a number of years and had not been resolved bytheprovisionof new dentures. Mandibular overden-tures that used ball attachments on 2 implants wereprovided for 13 patients (ball attachment group).Mandibular overdentures using magnet retentionwere provided for 12 patients (magnet group); 10patients had 2 implants stabilizing their overdenturesand 2 patients had 3 implants. The ball attachmentgroup comprised 8 women and 5 men with a meanage of57 years and a range of 41 to 72 years. The 12patients in the magnet group were all women with amean age of 57 years and a range of 45 to 76 years.There were 24 patients still in the study at the end ofthe 5 years, as one man from the ball attachmentgroup died toward the end of the second year.
Implants
The Astra Tech System was used for all patients (Fig1 ). The threaded implants and abutments are made ofcommercially pure titanium. The abutment and abut-ment screw are constructed as a single unit. The abut-ment threads are within the implant to produce whatthe manufacturer calls a conical seal. For this study7 lengths of implants were available, ranging from 7.5to 19 mm with diameters of either 3.5 or 4 mm. Theabutments were available in 6 lengths, ranging from0 to 7.5 mm with a 45-degree taper at the top.
The ball attachment mechanism comprised a com-mercially pure titanium, ball-shaped attachment thatis threaded into the top of the abutment and a gold-alloy cap that is incorporated into the denture base.The magnet attachment mechanism consisted of astainless steel keeper coated with titanium and tita-nium nitride that is threaded into the abutment. Thesplit-pole magnet is incorporated into the denturebase and is made of neodymium-iron-boron.
Fig 1 Separated componeots of the Astra Tech implant sys-tem: ball attachment, left, and magnet keeper, right.
Surgical Technique
A total of 24 patients had 4 implants placed in themandible between the mental foramina using stan-dard implant protocol; one additional patient had 3implants placed. The participants were not allowedto wear their mandibular dentures for 2 weeks fol-lowing placement of the implants. After this period,the dentures were adjusted and relined with a provi-sional resilient material. The implants were left sub-merged for a minimum of 4 months.
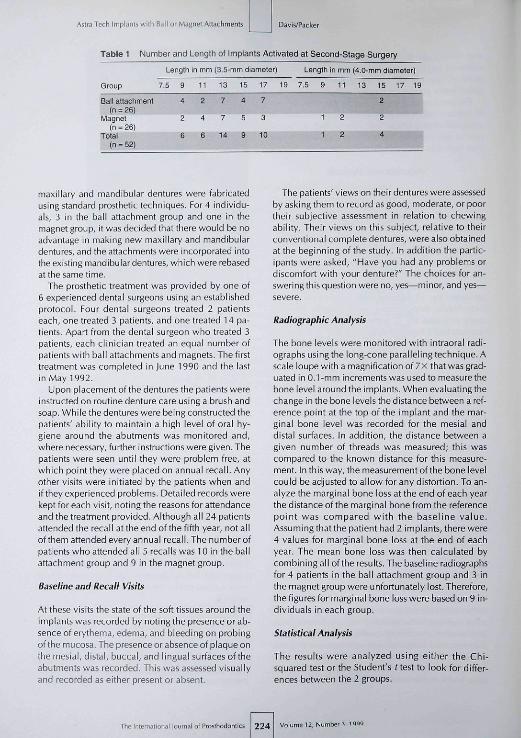
At second-stage surgery 52 of the 99 implants wereactivated (Table 1 ¡. Healing abutments were placedon the 2 implants that had been placed closest to thecanine region. When the time came to expose the im-plants it was found that in 2 individuals a more cen-trally placed implant had already perforated the mu-cosa. It was decided to use this implant in additionto the more favorably placed implants. All other im-plants were left as "sleepers." All surgical procedureswere carried out by the same oral and maxillofacialsurgeon.
Prosthetic Technique
Once the tissues had healed the healing abutmentswere replaced with definitive abutments and the pa-tients were allocated randomly to either the ball attach-ment group or the magnet group. In 21 individuals new
12, Number Î , 1999 2 2 3 The International Journal of Ffosthodontics
Astra Tech Implants wi lh Ball or Magnet Attactiments Oavis/Packer
Table 1 Number and Length of Implants Activated at Second-Stage Surgery
Length in mm (3.5-mm diameter) Length in mm (4.0-mm diameter)
Group 7.5
Ball attachment
Magnetm = 26]
Total(n = 52)
9
4
2
fi
11
4
6
13
7
7
14
15
4
5
9
17
3
10
19 7.5 9
1
1
11
2
2
13 15
2
2
4
17 19
maxiiiary and mandibuiar dentures were fabricatedusing standard prosthetic techniques. For 4 individu-áis, 3 in the baii attachment group and one in themagnet group, it was decided that there wouid be noadvantage in making new maxiiiary and mandibuiardentures, and the attachments were incorporated intothe existing mandibuiar dentures, which were rebasedat the same time.
The prosthetic treatment was provided by one of6 experienced dentai surgeons using an estabiishedprotocol. Four dentai surgeons treated 2 patientseach, one treated 3 patients, and one treated 14 pa-tients. Apart from the dental surgeon who treated 3patients, each clinician treated an equai number ofpatients with bail attachments and magnets. The firsttreatment was compieted in June 1990 and the iastin May 1992,
Upon placement of the dentures the patients wereinstructed on routine denture care using a brush andsoap, Whiie the dentures were being constructed thepatients' abiiity to maintain a high level of oral hy-giene around the abutments was monitored and,where necessary, further instructions were given. Thepatients were seen until they were probiem free, atwhich point they were placed on annuai recali. Anyother visits were initiated by the patients when andif they experienced probiems. Detai led records werekept for each visit, noting the reasons for attendanceand the treatment provided, Aithough ali 24 patientsattended the recaii at the end of the fifth year, not aliofthem attended every annuai recaii. The number ofpatients who attended ail 5 recails was 10 in the bailattachment group and 9 in the magnet group.
Baseline and Recall Visits
At these visits the state of the soft tissues around theimpiants was recorded by noting the presence or ab-sence of erythema, edema, and bleeding on probingofthe mucosa. The presence or absence of piaque onthe mesiai, distai, buccai, and iinguai surfaces oftheabutments was recorded. This was assessed visuaiiyand recorded as either present or absent.
The patients' views on their dentures were assessedby asi<ing them to record as good, moderate, or poortheir subjective assessment in reiation to chewingabiiity. Their views on this subject, reiative to theirconventionai compiete dentures, were aiso obtainedat the beginning of the study, in addition the partic-ipants were asked, "Have you had any probiems ordiscomfott with your denture?" The choices for an-swering this question were no, yes—minor, and yes—•severe.
Radiographic Analysis
The bone ieveis were monitored with intraorai radi-ographs using the iong-cone parai iei ing technique, Ascale ioupewitha magnification of 7 X that was grad-uated in 0.1-mm increments was used to measure thebone Ievei around the implants. When evaiuating thechange in the bone ieveis the distance between a ref-erence point at the top of the implant and the mar-ginal bone ievel was recorded for the mesiai anddistai surfaces. In addition, the distance between agiven number of threads was measured; this wascompared to the known distance for this measure-ment, in this way, the measurement ofthe bone ieveicould be adjusted to ai iow for any distortion. To an-aiyze the marginal bone ioss at the end of each yearthe distance ofthe marginai bone from the referencepoint was compared with the baseiine vaiue.Assuming that the patient had 2 implants, there were4 vaiues for marginai bone ioss at the end of eachyear. The mean bone ioss was tben calcuiated bycombining aii ofthe resuits. The baseiine radiographsfor 4 patients in the baii attachment group and 3 inthe magnet group were unfortunately iost. Therefore,the figures for marginai bone ioss were based on 9 in-dividuáis in each group.
Statistical Analysis
The results were analyzed using either the Chi-squared test or the Student's t test to look for differ-ences between the 2 groups.
The Irternalioiial lournal of Proslliodontic 224 Volume 12, Numbe

Davi^acker Asrra Tech Implants with Ball or Magnet Attachments
Table 2 Mean Marginal Bone Loss at the End of Each Year (mm)*
Group
Ball attachmentMeanRange
MagnetMeanRange
1
-0.2 ± 0.4-1.7-0 8
-0.3 ± 0,6-2.0-1.0
2
-0.1 ±0.6-1.4-1.4
-0.4 ±0.6-1 6-1.1
3
0.1 ±0.3-1.4-1 6
-0.3 + 0.7-1,8-1.6
4
0.1 +0.4-3.0-1.5
-0.2 ±0.7-1.6-1.9
5
0.0 ±0.5-1.4-1.3
-0.3 + 0.8-1.7-1.7
"Student's (test applied to raw data. P = 0.0016.
Results
Implant Components
Integration was lost in one implant 6 tnontlns afterdenture insertion, while in a second patient an im-plant fractured toward the end of the first year. Bothot these patients were in the magnet group. One pa-tient in the ball attachment group fractured an im-plant toward the end of the fifth year. In all 3 instancesspare implants were activated, new abutments wereplaced, and the patients continued in the trial.
During the 5 years it was necessary to change theabutments in 4 patients. There were 2 patients whowere unhappy with their dentures in the region of theattachments as they felt bulky. It was therefore de-cided to replace the abutments with shorter ones. Inthe other 2 patients the ball attachments, whichscrewed into the top of the abutments, kept un-screwing. These abutments were replaced with "all-in-one" abutments of the same length (Fig 2). All-in-one abutments, which were introduced during thecourse of the study, are designed so that the abutmentand ball attachment are manufactured as one unit.
Mucosal Response
There was no statistical difference, over the 5 years,between the 2 groups when comparing the percent-age of abutments around which the mucosa showedsigns of erythema, edema, and bleeding on probing.The mean value for the ball attachment group was25% ± 15% and 17% ± 9% for the magnet group(Student's ftest, P= 0.211. There was, however, a sta-tistically significant difference between the 2 groupsfor the percentage of abutment surfaces that showedthe presence of plaque. The mean percentage valuefor the ball attachment group was 20% ± 7% and 33%± 10% for the magnet group {Student's ttest, P= 0,04).
Fig 2 "All-in-one" ball attachment.
Marginal Bone Levels
The bone loss around the implants was greatest dur-ing the first year, after which there was very littlechange (Table 2)- There was a statistical difference be-tween the 2 groups, with the magnet group exhibit-ing greater marginal bone loss than the ball attach-ment group (P= 0.016).
Postinsertion Maintenance
The ball attachment mechanism required 56 episodesof maintenance because of the ball attachmentsunscrewing, fracturing, or wearing and the clips
-r:\':\:-r^ ' 2 . Number J, 1999 225 The International lournal of Frosthodontics

Astra Tech Implants with Ball or Magnet Attachments Diivis/Packer
Table 3 Reasons for and Frequency of PostinsettionCare Related to Implants and Attachment Mechanisms
Table 4 Reasons for and Frequency of PostinsertionCare Related to Mandibular Overdentures
Ball attachment groupAbutment unscrewedAbutment changedBall attachment unsorewedBall attachment fracturedBall attachment wornClip adjustedClip replacedLoss of implantFracture of implantTotal
Magnet groupAbutment unscrewedAbutment changedKeeper unscrewedKeeper fracturedMagnet replacedLoss of implant
i Fracture of implantTotal
Total
23
2671
18401
62
5171
2111
37
No, of people
239516301
12
5131
1111
12
Ball attachment groupDenture adjustmentDenture rebasedDenture fracturedDenture remadeOther problemsTotal
Magnet groupDenture adjustmentDenture rebasedDenture fracturedDenture remadeOther problemsTotal
Total
215622
36
295663
49
No, ot people
95422
12
113463
12
Table 5 Patient Response to the Question "HaveYou Had Any Problems or Discomfort with YourProsthesis?"*
Pretreatment Posttreatmenl mean
Ball attachment groupNoneYes—mildYes—severe
Magnet groupNoneYes—mildYes—severe
82369
—5050
52 ±745 ±8
3 ± 4
31 ï1060 + 11
9 t 6
Ball attachment groupGoodfi^ ode ratePoor
fvlagnet groupGoodfi/loderatePoor
•Responses are expresses as a percentage of all responses for each yeChi-sqjared lest, P = 0.0Q5.
Table 6 Subjective Patient Assessment ofProstheses in Relation to Chewing Ability"
Pretreatrrent Posttreatment mean
83*1217 + 12
70 ±1321 i l l10±10
'Responses are expreised as a percentage of all responses for each year,Chi-squared test, P ^ 0,005,
requiring adjustment or replacement. The magnet at-tachment mechanism required 29 episodes of main-tenance because of keepers unscrewing or fracturingand the magnets needing replacement (Table i). Thisdifference was statistically significant ¡Chi-squaredtest, P= 0.052), The major maintenance requirementwith the ball attachments was the need to retightenthem, which requiredonevisit. The major requirementwith the magnets was that they needed to be replaced,which involvedat [east 2 visits. The total number of vis-its required to maintain the ball attachment mecha-nisms was EJO, while the magnet attachments required55 visits. On comparing the number of visits therewas no statistical difference between the 2 groups forthe amount of postinsertion maintenance.
The mandibular overdentures required attention on36 occasions in the ball attachment group and 49 oc-casions in the magnet group (Table 4). The category"other problems" consists of prosthetic chai lenges thatwere unrelated to the use of implants, for example the
need to reposition teeth to increase tongue space or theneed to reposition the anterior feeth to produce the cor-rect lip support.
The total number of episodes of maintenance re-lated to the implants, attachment mechanism, andmandibular prosthesis was 98 in the ball attachmentgroup and 86 in the magnet group. This maintenancerequired the ball attachment group to make a total of150 visits and the magnet group to make 158 visits.Thus, on average each patient in the ball attachmentgroup made 12.2 visits over the 5 years for postin-sertion care, while those in the magnet group made13.2 visits. There was no statistical difference be-tween the 2 groups when comparing the total amountof postinsertion care.
Patient Assessment
There was a statistically significant difference betweenthe 2 groups in response to the question "Have you
226 Volume 12, Numbe

Davis.'Packer
bad any problems or discomfort with your prosthe-sis?"; the ball attachment group appeared to be morecomfortable (Chi-squared test, P= 0.005) (Table 5).Similarly, chewing abilit>' also showed a statistical dif-ference, with the ball attachment group rating theirability higher iChi-squared test. P = 0.005] (Table 6).
Discussion
Only one implant was lost during the 5 years becauseoffailureofosseointegration. Thefaatbat2 implantsfractured is an indication of the bending stresses towhich implants are subjected. Clantz and Nilner'^concluded, from a biomechanical point of view, thatthe prognosis for overdenture treatment in patientswith osseointegrated implants is maximized when (/Jthe number of implants used to stabilize the over-denture is as great as possible, (2) the bar system hasbeen designed with the highest possible rigidity, and(3) tbe overdenture itself has some functional flexi-bility, judged by these criteria, the use of 2 isolated im-plants is the least favorable situation. Although thenumber of fractures is small, it does represent an im-plant fracture rate of 4%. It is therefore essential thatthe group of people in the present study is followedfor a longer period of time to see if there is an increasednumber of implant fractures. As both of the fracturedimplants had a diameter of 3.5 mm, it would seem tobe a sensible precaution to use the larger 4.0-mm di-ameter implant when using the Astra Tech implant sys-tem for overdentures, particularly wben using only 2implants.
The implant survival rate for the ball attachmentgroup was 96%, and that for the magnet group was92%. These survival rates are very similar to those ob-tained in other studies.^^'^^ Thus, it would seem thatthe Astra Tech System is one of a number of implantsystems that can be used successfully to stabilizeoverdentures in the mandible.
Tbe abutments in the magnet group consistentlyhad more surfaces covered in plaque than the ball at-tachment group. It was felt that the number of sun̂ acescovered in plaque would give an indication of the dif-ficulty in cleaning around the implants. The magnetkeepers are wider at the top than at the base (Fig 1 ).This leads to the creation of a space between the pros-thesis and the implant. This would encourage greaterplaque accumulation, which patients could find moredifficult to remove completely.
Naert et al'"' found a similar increase in plaquearound implant-stabilized overdentures when mag-nets were used, compared to ball attachments andbars. They attributed this difference to loss of moti-vation in the magnet group, who showed a tendencyto dissatisfaction with their magnets. As the amount
Astra Tech Implants with Ball or Magnet Attachments
of plaque increased, it was expected tbat there wouldbe a decrease in the health of the mucosa as indicatedby signs of erythema, edema, or bleeding on probing.However, no such correlation could be found.
Marginal bone loss around implants has been high-lighted as an important criterion for judging long-termimplant survival. The usual means of monitoringbone levels is with periapical radiographs. However,it can be difficult to obtain consistency between ra-diographs, particularly in individuals who have ahigh levei of the floor of the mouth relative to the crestof the ridge. This can result in radiographs that are dif-ficult to read. Both Johns et ai '" and Wright et aP^ re-ported that approximately V. of the radiographs in theirStudies were unreadable or missing. Jn a prospectivestudy such as the present one, the fact that 7 baseiineradiographs were missing is extremely disappointing.
Although the magnet group exhibited statisticallysignificantly more marginal bone loss than the ball at-tachment group, the figure for mean marginal boneioss of 0.33 mm after 5 years was less than the 0.2 mmper year recommended by Albrektsson et al.^^ Forboth groups, the marginal bone loss was greatestduring the first year, after which the bone level wasremarkably stable.
Bone Ioss around implants has usually been meas-ured in tenths of a millimeter. However, Sewerin^"has shown that a 1-degree change in the angulationof the x-ray beam results in a change in the measuredbone level of 0.1 mm. Benn-' has estimated that anymeasured change in marginal bone height of lessthan 1 mm is likely to be an artifact. Thus, in view ofthe small sample size in this study and the vvide rangeof the readings (Table 2), it is quite possible that thedifferences in bone loss between the 2 groups are notreal. Further studies with a larger pool of participantswould be necessary to confirm any differences. Naertand coworkers'"* -- could find no differences in mar-ginal bone levels among 3 groups of overdenture pa-tients, with each group having a different attachmentmechanism.
One of the purposes of a clinical trial is to exam-ine the efficacy of a particular treatment modality andto make modifications in light of the experiencegained. The drawback with this is that the piece ofequipment that is being tested becomes obsolete.This is demonstrated by the design of the ball at-tachment, which was changed during the course ofthis trial. The screw part of the ball attachment wasthe weakest link in this attachment mechanism. Toovercome this problem, Astra Tech introduced an at-tachment in which the ball and the abutment aremade as one unit (Fig 2). This all-in-one attachmenthas replaced the separate ball attachment, which isnow no longer available. The all-in-one attachment
Z,.:,.,,.^ :2,Ni imberî, 1999 2 2 7 Ttie Internat ion, al of Pro5thodonlics

Astra Tech Implant! with EIÍIII or Magnet Attachments Davis/Packer
was used on 2 patients during the course of thisstudy. These 2 individuals accounted for 16 of the 33occasions when the ball attachment required atten-tion. Once the all-in-one ball attachments were used,there were no further episodes of the attachmentsloosening. Thus, it seems likely that the use of thisnew abutment would have improved the security ofthe ball attachment and therefore reduced the amountof postinsertion care. However, further studies arenecessary to confirm this view.
The data for clip adjustment is underreported inthat at least 3 individuals made their own adjust-ments to maintain retention. It could be argued thatone of the advantages of the clips is that they allowwearers to make their own adjustments, unlike fail-ure of the magnets, which requires the individual toreturn to the dental office for treatment.
The magnets do corrode and cease to function. Inthe present study 3 patients required magnet re-placement on one occasion, 6 on 2 occasions, and2 patients on 3 occasions. Only one patient did nothave the magnets replaced during the 5 years of thestudy. In this individual, the magnets ceased to func-tion during the third year of the study, but becauseof illness the patient was unable to return to havethem replaced. They were eventually replaced, butoutside the 5-year period covered by this paper. Themean life of the magnets was 103 weeks, with arange of 40 to 183 weeks.
None of the overdentures was strengthened origi-nally. Glantz and Nilner'^ have highlighted the factthat, from a biomechanical point of view, the prog-nosis for overdenture treatment ¡s maximized whenthe overdenture has some functional flexibility. Theinclusion of a cobalt-chromium alloy strengthenerconflicts with this requirement. In 2 individuals theoverdentures fractured twice within a short period oftime, and the overdentures were therefore remadewith the inclusion of a cobalt-chromium alloystrengthener. However, it seems advisable not to dothis as a matter of routine in view of the potential forincreasing the loading onto the 2 implants.
The number of visits made for postinsertion care ex-cludes the annual recall visits, unless they involvedan episode of maintenance. It could be argued thatannual recall visits are an essential part of implantmaintenance and so should be included in the totalnumber of visits irrespective of whether they resultedin the provision of extra care. However, as the pur-pose of the study was to examine the amount ofmaintenance required to maintain the overdenturesand implants, it was decided to exclude those annualrecall visits when no maintenance was required.
The use of the ball attachments and the magnets bothseemed to provide patient satisfaction and improved
ability to chew effectively when compared to patientdenture assessment prior to the placement ol implants.There is the suggestion that the magnet ¡itoup was lesscomfortable and chewing was less etieciive whencompared to the ball attachment group. However,there was no direct comparison of the 2 types of at-tachments on the same patients. The participants weretherefore not able to compare the effectiveness of the2 attachment mechanisms. Burns et aP' have carriedout such a study with 17 subjects using O ring andmagnet attachments. The subjects were satisfied withboth overdentures but showed a strong preference forthe O ring. It is likely that the preference for ball at-tachments over the magnets is related to the better re-tention provided by the ball attachments,^ '̂̂ ^
Conclusion
The evidence indicates that both ball attachments andmagnets used on isolated Astra Tech implants in themandible are viable treatment options. There was nodifference between the 2 groups in either soft tissuehealth around the implants or the amount of postin-sertion maintenance. The magnet group had signifi-cantly more abutment surfaces with plaque on them.Both groups exhibited marginal bone loss that wasless than 0,2 mm per year. Both attachment mecha-nisms provided patient satisfaction, aithough there isthe suggestion that the ball attachments were betterin this respect than the magnets.
Acknowledgment
The authors would like to thank Astra Tech for their support ofthis work.
References
1. Engquist B, BergendalT, KaiiusT, Linden U. A retrospective mul-ticenter evaluation of osseoinlegrated implants supporting over-dentLres. ln t | Orai Maxillofac Implants 1988;3:129-134.
2. Mrricske-Stern R, Clinical evaluation ot overdenture restorationssupported by osseointegrated titanium implants: A retrospectivestudy, int J Oral Masillofac Implants 1ÍÍ9O;5:375-3B3.
3. Naert I, Quirynen M, Theuniers G, van Steenberghe D, Prostheticaspects of osseointegrated tixtures supporting overdentures. A4-year report. | Prostliet Dent 1991 ;65:671-68O.
4. Chan MFW-Y, Johnston C, Howeli RA, Cawood Jl. Prostheticmanagement of the atrophie mandible using endosseous im-plants and oveidentures: A six year review. Br Dent J 1995;179:329-337.
5. Sprekermann M, ¡ansen VK, Richter EJ, A10-year follow up studyof IMZandTPS implants in the edentulous mandible using bar-retained overdentures. Int J Oral Maxillofac Implants 1995;10:231-243.
6. |em(T, Char], Harnett J, Heath RM, Hutton JE, |ohns RB, et al.A 5-year prospective multicenter follow-up report on overden-tures supported by osseointegrated implants. Intj Oral Maxillofaclmpiantsl996;11:29I-298.
The Internat ¡an a I |ourral of Prosiliodontics 228
Davis/Packer Asirá Tech Implants with Ball or Magnet Attachments
7- Yusuf H, Raira N, Observations on 25 patienK treated wilh ballretained overdenlures. Eyr | Prosthodont Restorative tJent 1996;4:T8l-!83,
8. Walmsley AD, Frame]W. Implant supported overdentures—TheBirmingham experience, ) Dent SuppI 1997;25:43-i7,
9. Cotfredsen K, Implant supported overdentures—TheCopenhagen experience, J Dent SjppI 1997;25:39^2,
10, Mencske-Stem R, Zarb CA, Overdentures: An altemative implantmethodology for edentulous patients. Int J Prosthodont1593;6:203-208,
11. Mericske-Stem R, Steiniin Schaftner T, Marti P, Geering AH. Peri-implant mucosal aspects of ITI implants supporting overdenlures,A five-year longitudinal study. Clin Oral Implants Res 1994-5:9-18,
n. Bergendal T, Engquist B. Implant-supported ovenJentures: A lon-gitudinal study, Int I Oral Maxillofac Implants 1998;13-.353-262,
13. Batenburg RHK, Meijer H|A. Raghoebar CM, Vissink A. TreatTneniconcepts for mandibular overdentures supported by endosseousimplants: A literature review. Inl J Oral Maxillofac Implants 1998-13J39-545.
14. Naert I, Cizani S, VuylstekeM, van Steenberghe D. A 5-vear ran-domized clinical trial on the intluence of splinted and unsplintedoral implants in mandibular overdcnture therapy. Part 1 : Peri-implant outcome. Clin Oral Implants Res 1998:9:170-177.
15. Clantz P-O, Nilner K. Biomechanical aspects of overdenturetreatment, i Dent SuppI l997;35:21-24.
16. CuneMS,dePunerC, Hoogstratenl.Ananonwideevaluativestudyon implant-retained overdentures, J Dent Supp11997;25:13-19.
17. Johns RB, lemt T, Heath MR, Hutton JE, McKenna S, McNamaraDC, el al. A mullicenter study ol" overdentures supported byBrânemark implants. Inl | Oral Maxillofac Implants J992-7-513-522,
1 a. Wright PS, Watson RM, Heath MR. The effects of prefabricatedbar design on ihe success of overdentures stabilized by im-plants. Inll Oral Maxillofac Implants l995;10:79-87.
19. Albrefctsson T. ZarbC, Worthington P, Eriksson AR, The long-termefficacy of currently used dental implants: A review and proposedcriteria of success. Inl | Oral Maxillofac Implants 1986:1:11-25.
20. Sewerin IP. Errors in radiographie assessment of marginal boneheight around osseoirtegrated implants, Scand J Den Res 1990-98:428-433,
21. Benn DK. A review of the reliability of radiographie measure-ments in estimating alveolar bone changes. | Clin Periodontol1990;! 7:14-21.
22. Naert I, Quirynen M, Hooghe M, van Steenberghe D. A com-parative prospective study of splinted and unsplinted Biäneniarkimplants in mandibular overdenlure therapy: A preliminary re-port. J Prosthet Dent ¡994:7] :4a6-492,
23. Burns DR, Unger JW, Elswick RK, Ciglio |A, Prospective clini-cal evaluation of mandibular implant ovefdentures: Part II—Patient satisfaction and preference. I Prosthet Deni I995;73-364-369,
24. Burns DR, UngerjW, Elswick RK, 8eck DA. Prospective clinicalevaluation of mandibular implant overdentures: Part I—Retention,stability and tissue response. J Prosthet Dem 1995;73:354-363.
Literature Abslract-
Effect of occlusal appliances and clenching on the internally deranged TMJspace.
Stabilization appliances (SA) and mandibular antenor repositioning appliances (MARA) havebeen used for treatment ot temporomanaibular disorders (TMD). These appliances have beenassumed to reduce interarticLJlar surface compression in the temporomandibuiar jûrnt fTMJ)during closing and clenching. This study aimed to test that assumption. Inciusion cnteria torthe 7 patients who sought treatment at a TMD clinic were anterior disc displacement (ADD)without reduction verified by MRI, history of unilateral TMJ pain and locking during opening,and/or difficulty in jaw opening for less than 6 months. All teeth except third moiars were re-quired for participating in the study and the exciusion criterion was clear evidence of osseouschanges in the TMJ. The SA used in this study was a maxiliary compiete appiiance with a flatocclusal table, which increased the vertical dimension of occlusion by 3 mm in the anterior re-gion. The MARA was designed to hold the mandible in a straight, forward position 2 mm fromintercuspal position. Bilateral tomograms were faken of these 7 patients with ADD during com-fortable closure and maximal clenching in maximum intercuspation; tomograms were aisotaken with the 2 different types of splints in situ. The tomogram with the slice ievei nearest tothe central part of the condyle was selected. Six images tor each joint were taken, one base-line and tive expérimentai conditions with tfie SA and MARA, Outlines of the condyle and tem-poral fossa were automatically determined by an edge-detection protocol, and the minirrurrjoint space dimensions were automatically measured for each expenmental condition as theoutcome variable. The results showed no significant ditferences in minimum joint space dimen-sions between the splints (SA or MARA] or between any of the splints and maximum intercus-pation. It was concluded that these appliances do not induce an increase in joint space duringclosing and clenching In joints with ADD without reduction.
Kubokl T, Takenami V, Orsîni MG, Maekawa K, Yamashlta A, A2uma Y, Clark GT. J Orotac Pain1999:13:38-48 Relerences: t5. Heprints; Dr Takuo KuOoki, Department of Fixed Prosthodontios,Okayama University Dental School, 2-5-1 Shikata-clio, Okayama 7Q0-8525. Japan, e-maii:kubokiSder t.okayam a-u. ac. jp—A W
"2,Numt)er3,l999 229 The Intemational ioun











![Oh Pretty Woman4sc].pdfã ### ### ### ### ### ### ### ### 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 2 4 2 4 2 4 2 4 2 4 2 4 2 4 2 4 2 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4](https://img.pdfslide.net/doc/110x75/60cfb349cd0cbb00d32b6774/oh-pretty-woman-4scpdf-4-4-4-4-4-4-4-4-4-4.jpg)
![Welcome [s3.eu-central-1.amazonaws.com]...bb bb bb bb bb # # # # # b b bb bb bb bb bb bb bb bb 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 44 4](https://img.pdfslide.net/doc/110x75/5e9f761d9d1aa23b1a09f03e/welcome-s3eu-central-1-bb-bb-bb-bb-bb-b-b-bb-bb-bb-bb-bb-bb-bb.jpg)

















