Embed Size (px)
Citation preview
1
48 yo Male With Right-Sided Testicular Pain x1 WeekCPC – ACOEP 11/3/2010
Christine A. Patte DOProgram Director, Swedish Covenant Hospital Emergency MedicineChicago, IL
2
DISCLOSURES
Nothing to disclose
3
48 yo Male With Right-Sided Testicular Pain x1 Week
4
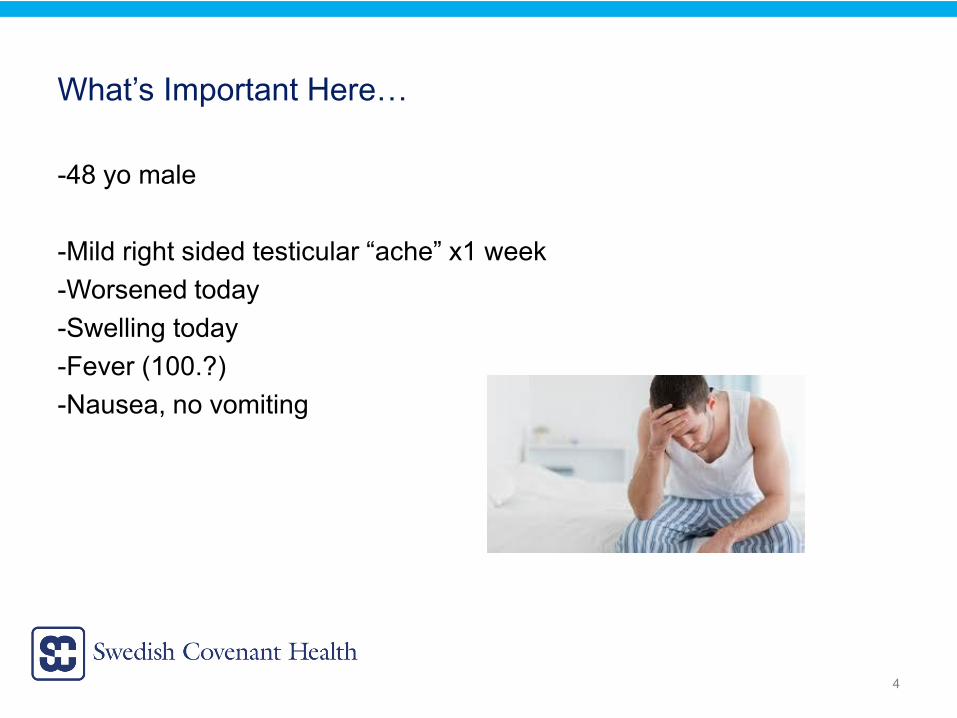
What’s Important Here…
-48 yo male
-Mild right sided testicular “ache” x1 week-Worsened today-Swelling today-Fever (100.?)-Nausea, no vomiting
5
What Else?
-Only prior history is seasonal allergies-Sexually active with 1 female partner (wife)
-Mild RLQ abdominal discomfort-Right-sided testicular pain and swelling-Right-sided lower back pain-Mild scrotal erythema
6
Differential Diagnosis of Testicular Pain?-Testicular torsion!-Epididymitis-Orchitis
-Epididymo-orchitis (most common complication of mumps in the adult male)-Trauma-Incarcerated inguinal hernia-Testicular cancer-Fournier’s Gangrene-Hydrocele? Spermatocele? Varicocele-Referred pain
-retrocecal appendicitis, abdominal aortic aneurysm, urolithiasis, lower lumbar or sacral nerve root impingement, retrocecal retroperitoneal tumor
-Torsion of the appendix testis-Torsion of appendix epididymis-Immunoglobulin A vasculitis (Henoch-Sch⍤nlein purpura)-Idiopathic Scrotal Edema
7
Emergent Treatment?Increased morbidity
Loss of testisInfertility
-Testicular torsion*-Acute epididymitis or epididymo-orchitis*-Fournier’s gangrene (necrotizing fasciitis of the perineum)
*Most common causes of acute scrotal pain in adults
8
What’s Important on the Physical Exam?
-Vitals?“Okay-ish”100.3 94 bpm 16 147/89 97% on RA
9
What’s Important on the Physical Exam?
-Vitals?“Okay-ish”100.3 94 bpm 16 147/89 97% on RA
-Appears somewhat uncomfortable-Abdomen is nontender
10
What’s Important on the Physical Exam?-Vitals?
“Okay-ish”100.3 94 bpm 16 147/89 97% on RA
-Appears somewhat uncomfortable-Abdomen is nontender
-Right testicle is significantly LARGER than left and diffusely TENDER to palpation-Mild erythema of scrotum without induration or fluctuance-Bogginess over the right inguinal ligament, also tender to palpation
-Cremasteric Reflex? Less consistent in older males -Hernia?
11
Differential Diagnosis of Testicular Pain?-Testicular torsion!-Epididymitis-Orchitis
-Epididymo-orchitis (most common complication of mumps in the adult male)-Trauma – but no history of this-Incarcerated inguinal hernia – not on physical exam provided
-Testicular cancer – but pain is acute-Fournier’s Gangrene – physical exam doesn’t seem to be
-Hydrocele? Spermatocele? Varicocele-Referred pain
-retrocecal appendicitis, abdominal aortic aneurysm, urolithiasis, lower lumbar or sacral never root impingement, retrocecal retroperitoneal tumor
-Torsion of the appendix testis – typically in children 7-14 yo-Torsion of appendix epididymis – typically in children 7-14 yo
-Immunoglobulin A vasculitis (Henoch-Sch⍤nlein purpura) – though scrotal pain CAN be the presenting symptom
-Idiopathic Scrotal Edema
12
RESULTS…should help us?!
-CBC with leukocytosis, neutrophiliaWBC 14.8 k/uL Neutrophils ABS 10.8 k/uL
-BMP wnl
-LA wnl
-UA wnl
Gonorrhea/Chlamydia Urine Probes – pending
13
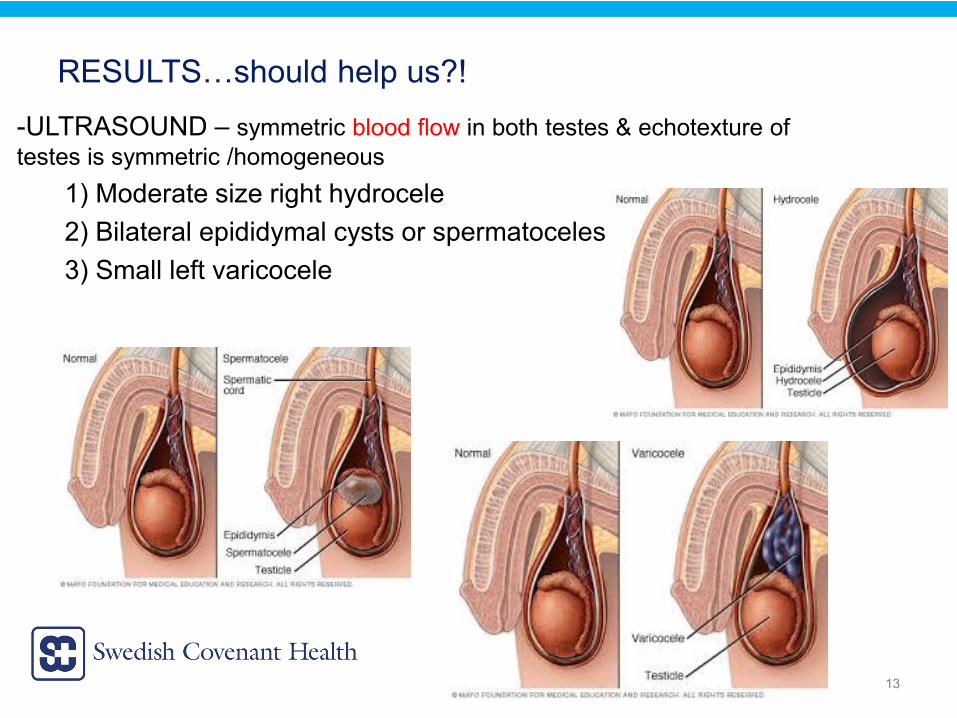
RESULTS…should help us?!-ULTRASOUND – symmetric blood flow in both testes & echotexture of testes is symmetric /homogeneous
1) Moderate size right hydrocele2) Bilateral epididymal cysts or spermatoceles3) Small left varicocele
14
Right Hydrocele & Epididymal Cyst or Spermatocele
Is this enough to account for patient’s symptoms?(Low grade) Fever/leukocytosisErythemaSignificant pain
15
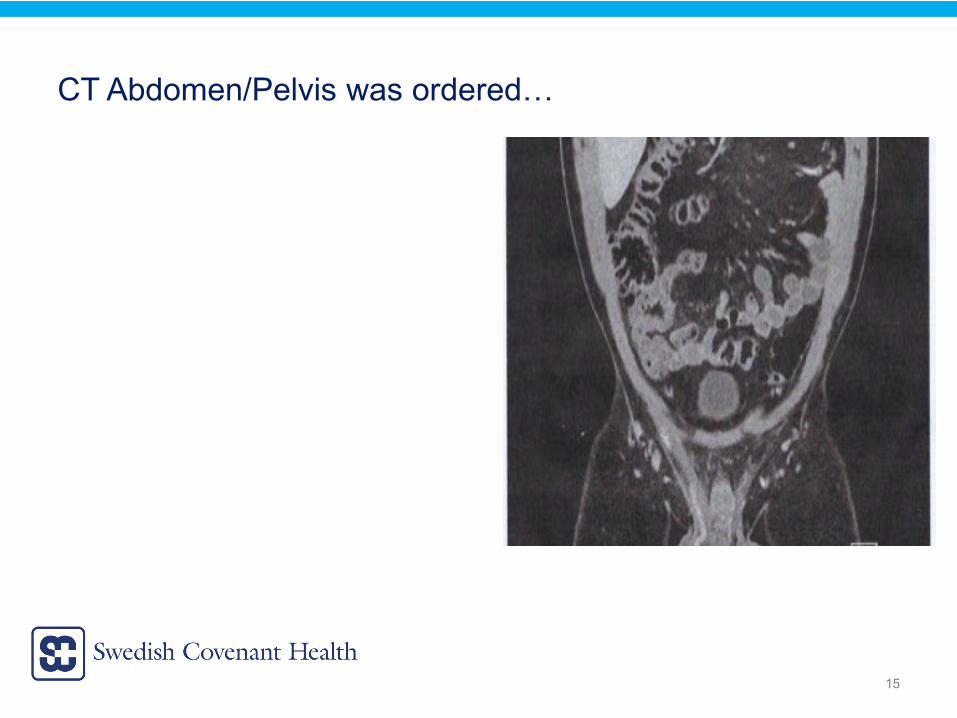
CT Abdomen/Pelvis was ordered…
16
17
18
Collecting All of the Data…
48 yo m w right testicular pain x1 week, worsened today. -Associated nausea, low grade fever-Leukocytosis, neutrophiliaSIRS CRITERIA
US: Moderate right hydrocele, bl epididymal cysts or spermatoceles (small left varicocele)
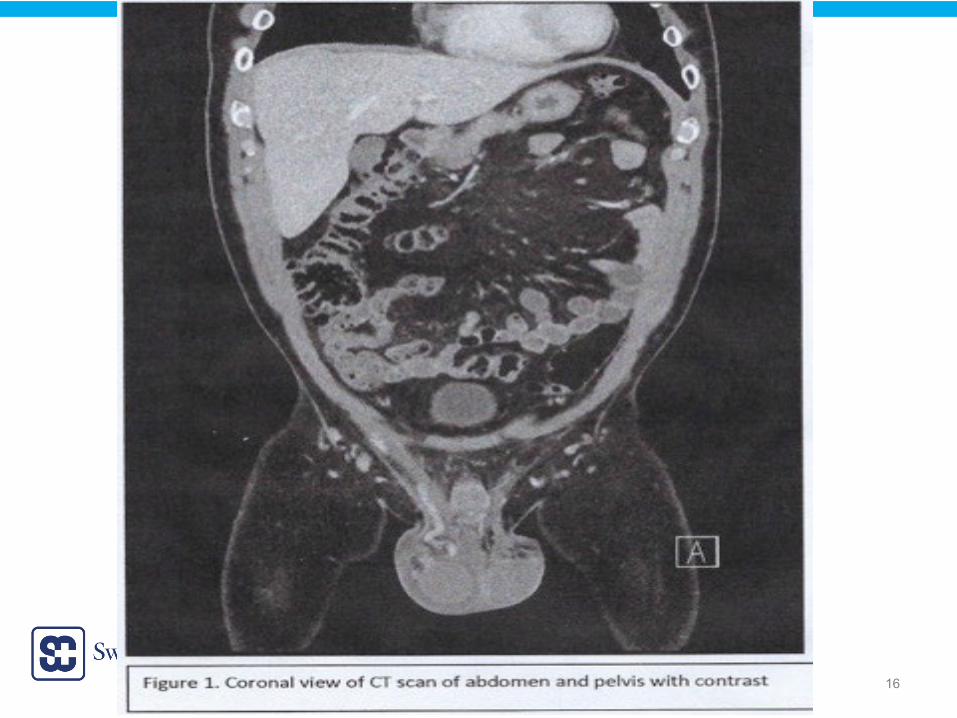
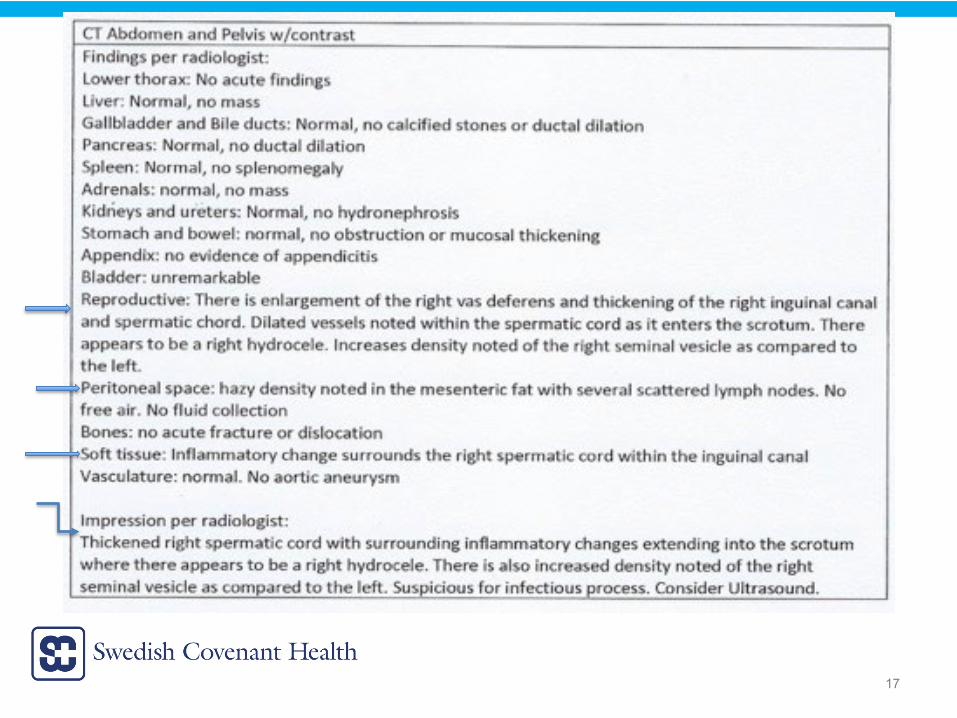
CT: Enlargement of R vas deferens, thickening of R inguinal canal and spermatic cord. Dilated vessels noted within spermatic cord as it enters the scrotum. Right hydrocele. Increased density of right seminal vesicle compared to left.Hazy density in the mesenteric fat w several scattered lymph nodes, no free air/fluid.
19
Collecting All of the Data…
Infectious or Inflammatory Process
20
Let’s Go Through Our Differential…
21
Differential Diagnosis of Testicular Pain?
-TESTICULAR TORSION–NO: SYMMETRIC BLOOD FLOW SEEN BILATERALLY
Intermittent Testicular Torsion?Pain/symptoms are constant
22
Differential Diagnosis of Testicular Pain?
-TRAUMAYes:
-testicular pain with tenderness on palpation-swelling
No:-history of trauma provided-hematocele, pyocele or testicular rupture-no signs of trauma on color doppler ultrasonography
23
Differential Diagnosis of Testicular Pain?
-TESTICULAR CANCERYes:
No:-no testicular masses seen
24
Differential Diagnosis of Testicular Pain?
-INCARCERATED INGUINAL HERNIAYes:
-testicular pain with tenderness on palpation-Leukocytosis
No:-no hernia noted on physical exam or imaging (herniation of bowel or omentum into the scrotum will appear as a scrotal mass)-LA wnl
25
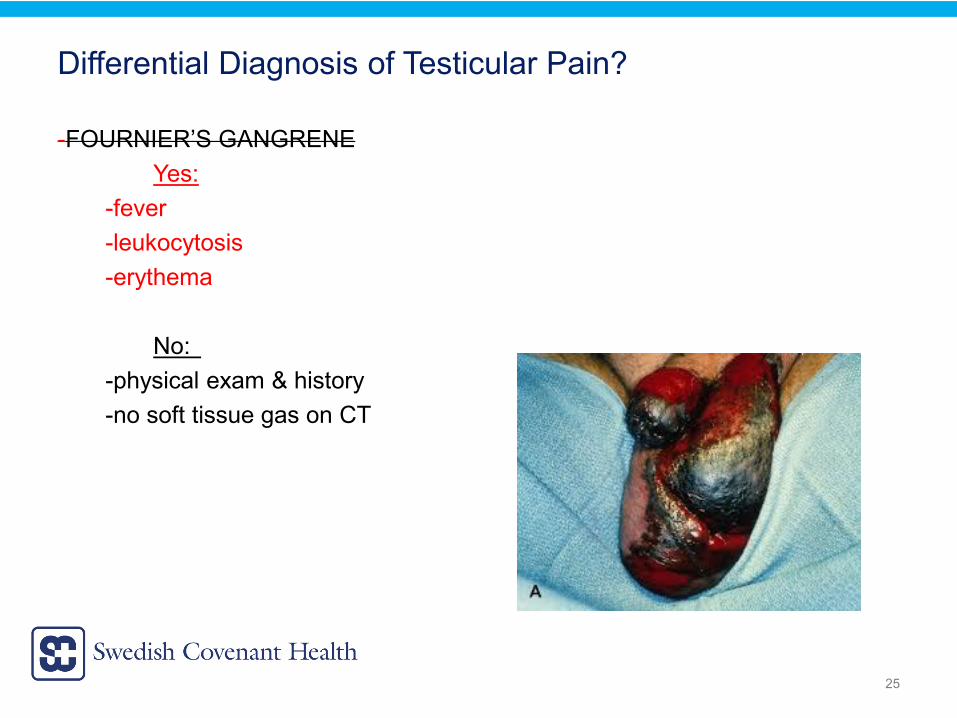
Differential Diagnosis of Testicular Pain?
-FOURNIER’S GANGRENEYes:
-fever-leukocytosis-erythema
No:-physical exam & history -no soft tissue gas on CT
26
Differential Diagnosis of Testicular Pain?
-REFERRED PAINYes:
No:-no abdominal pain – likely not appendicitis (and not seen on CT)-history - there’s localized testicular tenderness, swelling & erythema – likely not referred from something else like abdominal aortic aneurysm, nerve root impingement, retrocecal retroperitoneal tumor, urolithiasis (and not seen on CT)-no history of flank pain, no hematuria
27
Differential Diagnosis of Testicular Pain?
-HYDROCELE – likely reactive, but not the etiology of pt’s severe pain/symptoms
-SPERMATOCELE – likely not the etiology of pt’s severe pain/symptoms
-VARICOCELE – not seen on ultrasound on right side
28
Differential Diagnosis of Testicular Pain?
Idiopathic Scrotal EdemaNO – there are pathological findings on imaging
29
Differential Diagnosis of Testicular Pain?
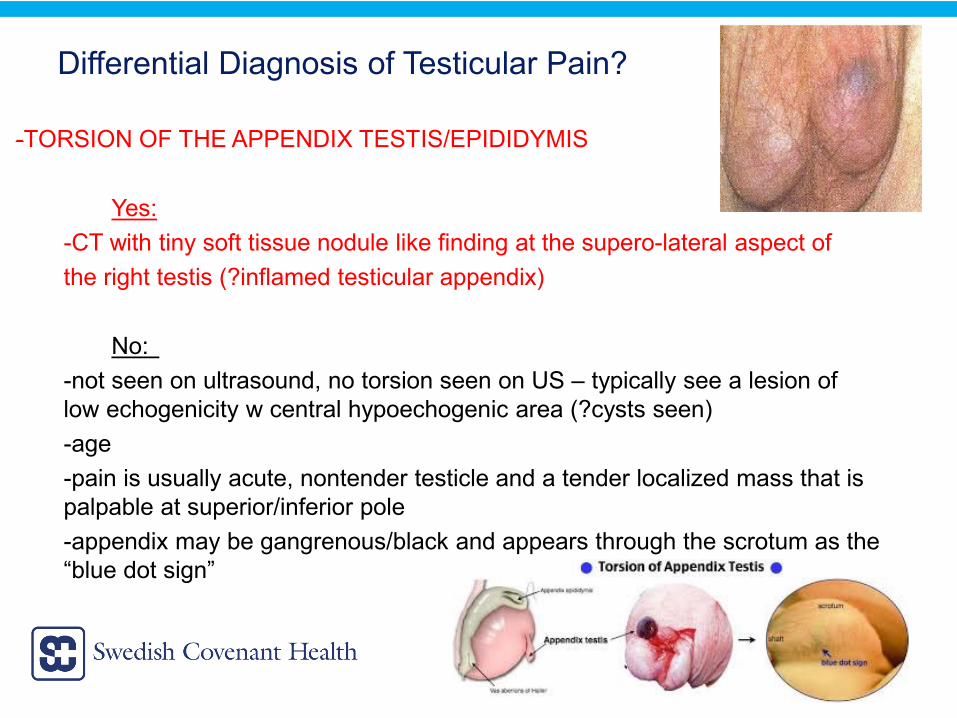
-TORSION OF THE APPENDIX TESTIS/EPIDIDYMIS
Yes:-CT with tiny soft tissue nodule like finding at the supero-lateral aspect of the right testis (?inflamed testicular appendix)
No:-not seen on ultrasound, no torsion seen on US – typically see a lesion of low echogenicity w central hypoechogenic area (?cysts seen)-age-pain is usually acute, nontender testicle and a tender localized mass that is palpable at superior/inferior pole-appendix may be gangrenous/black and appears through the scrotum as the “blue dot sign”
30
Differential Diagnosis of Testicular Pain?
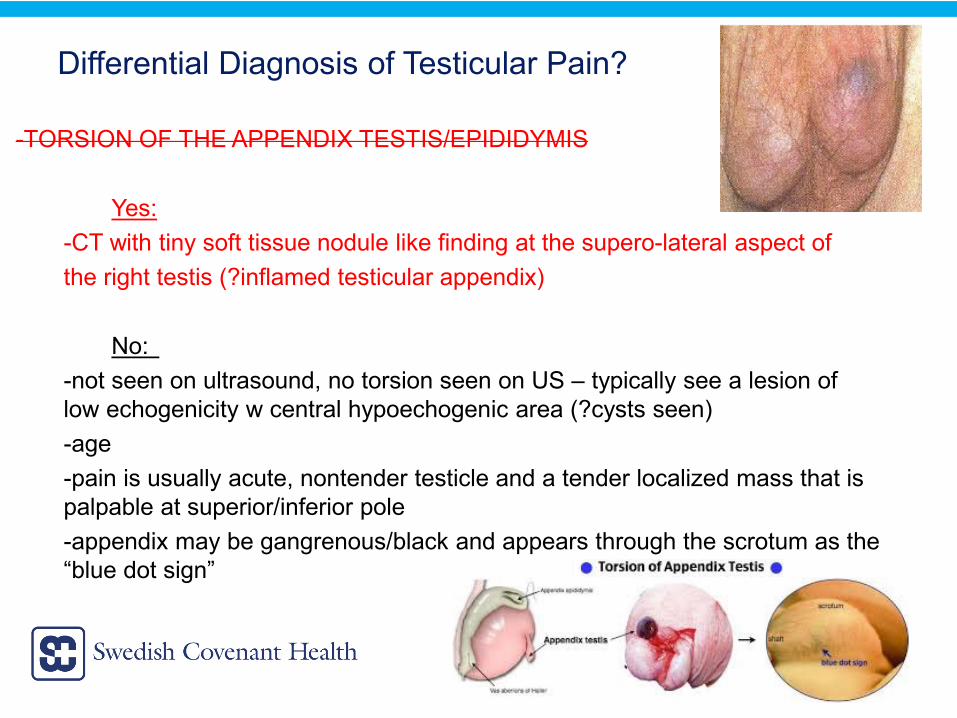
-TORSION OF THE APPENDIX TESTIS/EPIDIDYMIS
Yes:-CT with tiny soft tissue nodule like finding at the supero-lateral aspect of the right testis (?inflamed testicular appendix)
No:-not seen on ultrasound, no torsion seen on US – typically see a lesion of low echogenicity w central hypoechogenic area (?cysts seen)-age-pain is usually acute, nontender testicle and a tender localized mass that is palpable at superior/inferior pole-appendix may be gangrenous/black and appears through the scrotum as the “blue dot sign”
31
Differential Diagnosis of Testicular Pain?-EPIDIDYMITIS(-ORCHITIS)
Yes:-testicular pain with tenderness on palpation-swelling-scrotal wall erythema-reactive hydrocele -Can cause serious illness in rare cases with fever-Leukocytosis
*WILL LEAVE ON DIFFERENTIALNo:
-discharge-findings on US -?Prehn sign -sexual history (heavy physical exertion & direct trauma can also predispose pts)-pyuria – though UA may be normal in 15-59%
-viral sxs (mumps, rubella, parvovirus etc.)
32
Differential Diagnosis of Testicular Pain?
-EPIDIDYMITIS(-ORCHITIS)-But, the CT findings show more than this -Could this have spread to vas deferens/spermatic cord?
*At this point – I’d cover the patient with antibiotics for the most common microbial agents causing epididymitis in sexually active males (chlamydia, N. gonorrhea, E. coli, also viruses)
-ceftriaxone 250 mg IM x1+
doxycycline 100 mg po BID x 10 d (or azithromycin 1 g po x1)*Our patient is >35 yo and low risk for STIs: levofloxacin 500 mg po QD x 10d (or trimethoprim-sulfamethoxazole 1 DS tab BID x 10 d)-Consider HIV testing
33
Differential Diagnosis of Testicular Pain?
-IMMUNOGLOBULIN A VASCULITIS (HENOCH SCHÖNLEIN PURPURA)Yes:
-scrotal pain may be acute or insidious-scrotal pain may be the presenting symptom-Ultrasound markers of IgAV (HSP) = hydrocele, swelling in epididymis and scrotal skin, normal blood flow to testes
No:-no other symptoms of systemic vasculitis
-nonthrombocytopenic purpura, arthralgia, renal disease, abdominal pain, GI bleeding
-Usually in children (though can rarely occur in adults)
34
So, not the right patient for HSP, but….vasculitis? Thrombosis?
35
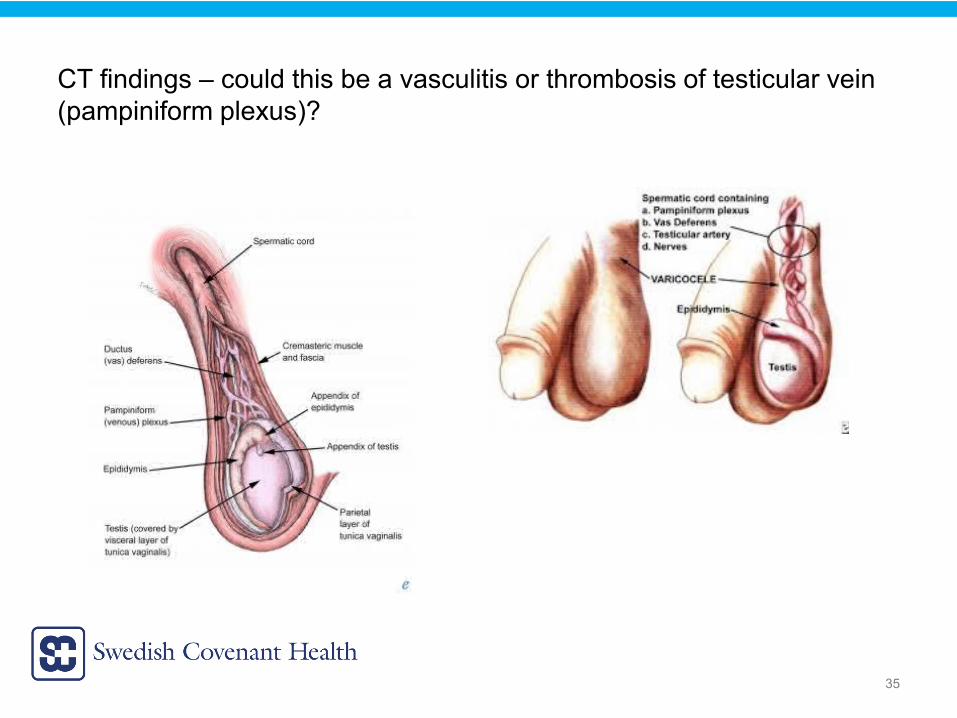
CT findings – could this be a vasculitis or thrombosis of testicular vein (pampiniform plexus)?
36
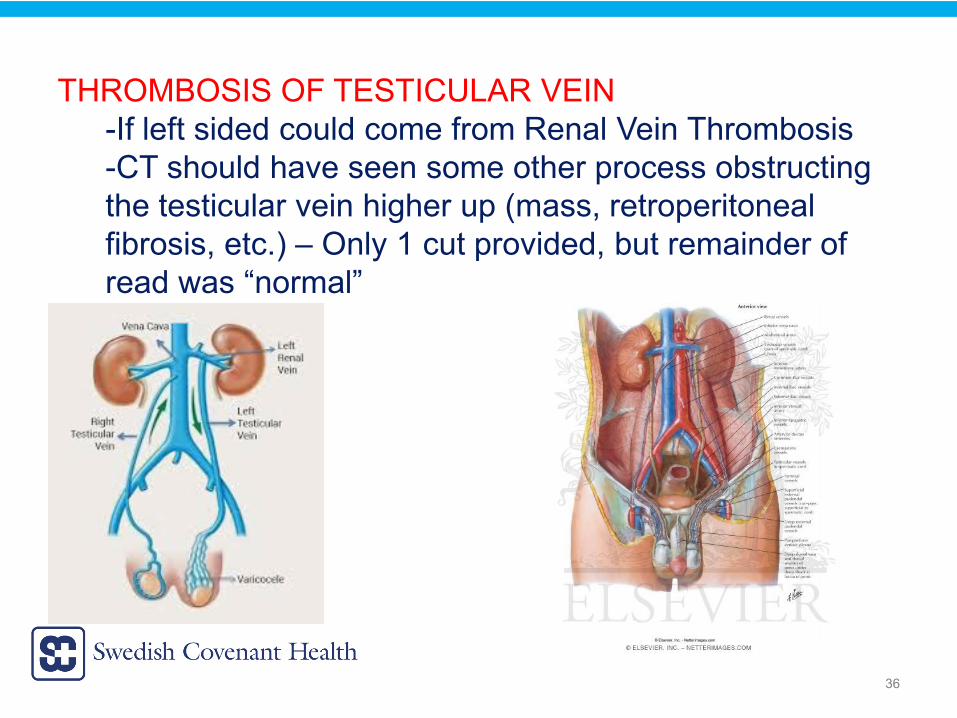
THROMBOSIS OF TESTICULAR VEIN-If left sided could come from Renal Vein Thrombosis-CT should have seen some other process obstructing the testicular vein higher up (mass, retroperitoneal fibrosis, etc.) – Only 1 cut provided, but remainder of read was “normal”
37
TESTICULAR VEIN THROMBOSIS (PAMPINIFORM PLEXUS)
?SPONTANEOUSVS
OBSTRUCTIVE PROCESS (possibly not seen on the CT image we received)
38
TESTICULAR VEIN THROMBOSIS (PAMPINIFORM PLEXUS)
Almost all of the reported cases of spontaneous thrombosis of the pampiniform plexus have involved the LEFT side (our patient’s symptoms are on the RIGHT). The reason is due to anatomical factors – compression of the left renal vein by the superior mesenteric artery (nutcracker phenomenon) and absent or incompetent valves in the left spermatic vein. The testicular vein on the left branches off of the left renal artery.
Risks for thrombosis: Virchow’s triad: blood stasis, coagulation factors and mural factors
39
DIAGNOSIS
Testicular Vein (Pampiniform Plexus) Thrombosis
40
REFERENCES1. Chi A.C. Acute right varicocele: a clue to congenital vascular anomaly. Urology, 85 (2015), pp. e39-e40.2. Kamel K, et al. Bilateral spontaneous thrombosis of the pampiniform plexus; A rare etiology of acute scrotal pain: A case report and review of literature. African Journal of Urology 24.1 (2018), pp. 14-18.3. McGavin D. Thrombosis of the pampiniform plexus. Lancet (1935), pp. 368-369.4. McGee SR. Referred scrotal pain: case reports and review. J Gen Intern Med 1993; 8:694.5. Molokwu CN et al. Outcomes of scrotal exploration for acute scrotal pain suspicious of testicular torsion: a consecutive case series of 173 patients. BJU Int 2011; 107:990.6. Siegel A et al. Epididymitits in infants and boys: underlying urogenital anomalies and efficacy of imaging modalities. J Urol 1987; 138:1100.7. Torjian TH et al. Epididymitis and orchitis: an overview. Am Fam Physician 2009; 79:583.8. Updated recommended treatment regimens for gonococcal infections and associated conditions – United States, April 2007. www.cdc.gov/std/treatment/2006/GonUpdateApril2007.pdf
41
THANK YOU!
42





























