Embed Size (px)
Citation preview

7/19/2014
1
48th Annual Meeting
Navigating the Oceans of Opportunity
Business Side of Pharmacy Leadership: Proving Pharmacy
Department Added Value
Heath Jennings, PharmD, MBA, FASHP, BCPS
Disclosure
I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with an organization whose philosophy could potentially bias my presentation
Objectives
Demonstrate how Pharmacy can achieve greater organizational value and return on investment
Describe how to use business analytics to show pharmacist value and impact on hospital costs
Explain the importance of pharmacy inventory management and how to improve secondary to drug utilization and formulary control
Present data to senior hospital administration to garner support for new pharmacy services, programs, and personnel
Who’s in the audience?
Current and future leaders?
Your leadership role: Is it formal or informal?
Director, manager, other?
Length of time in current role?
Desire to move up?
Why are you here today?
Considerations…
Economic challenges Crummy bond market & hospital investment portfolios
Reduced state budgets for Medicaid, rate cuts
Unemployed and uninsured seekers of healthcare
Healthcare reimbursement changes Slow the growth of health care expenditures
Need for greater efficiency and effectiveness
Alignment of incentives and continuum of care delivery
Payment system based on value versus volumes
Second Curve of Healthcare
Source: Adapted from Ian Morrison, 2011

7/19/2014
2
What is Value?
Interplay of cost-effectiveness and quality
“Bang for your buck”
Conflicting goals of health care stakeholders Patients – value the capacity of health care to help
them achieve wellness
Providers – view value in terms of the appropriateness of health care services rather than cost controls
Payers – emphasize comparative effectiveness and value evidence-based health care options that are cost effective
What is Pharmacy Value?
Patient Centered Care Improve drug therapy outcomes by optimizing
medication therapy and increasing patient safety
Inventory and Supply Chain Reduce medication-related expenses through group
purchasing, lean inventory management, and critical supply utilization
Billing and Revenue Cycle Proper coding and medication-related charge capture
to support appropriate patient billing and collections
Create new sources of revenue for health system
Pharmacy Value Perspectives
Safe – avoiding injuries to patients from the medication therapy that is intended to help them
Timely – reducing waits and sometimes harmful delays for those who receive and who deliver care
Effective – providing services based on scientific knowledge to all who could benefit, while refraining from providing services to those not likely to benefit
Efficient – avoiding wastes
Equitable – providing care that does not vary quality
Patient Centered – providing care that engages the customer and responsive to individualized needs
Our Mission:
To provide the highest level of quality care and
organizational value at the lowest possible cost
Healthcare Leader Mission:
Improve cash flow and operating margin Revenue cycle
Labor costs
Non labor costs
Reevaluate overall capital expenditure
Reevaluate investment policy
Reassess pension, retirement plans, health insurance and other employee benefits
Critically reevaluate all programs and services
Establishing Pharmacy Value
Understand the National Healthcare Agenda and Healthcare Reform actions
Understand how your facility prioritizes the National Agenda and response to Healthcare Reform
Develop and align your pharmacy services and programs accordingly
Develop skills in performance improvement, change management, and financial management

7/19/2014
3
Financial Management Skills Necessary to Prove Value Expense minimization skills
Revenue enhancement skills
Entrepreneurial and business development skills
Financial acumen Creating and communicating a ProFroma
Writing a business plan
Demonstration of quality Emphasizing Pharmacy’s value & quality impact
Developing and utilizing dashboards
Using external metrics, measures, and benchmarks
Why do pharmacists need financial management skills? Request and justify new resources and services
Participate in department budgeting process
Credibility with your Boss/director
Senior leadership
Finance’s agenda is YOUR agenda
Understand the “big picture” – how does pharmacy fit within the rest of the organization?
Pharmacy is uniquely situated to add value to the organization
Where do I start?
Basic Financial Terminology
Revenue – payer payments, rebate checks Expenses – supplies & labor
Income statement Net income (bottom line) = Revenue – Expenses Many organizations goal 4-6%
Balance sheet – summary of all account balances, including assets, liabilities and equity – as of a specific date (e.g. quarterly or year end)
Basic Financial Terminology
Cash flow – movement of cash into or out of the business based on internal business activities (operating cash flow)
EBIDTA – like cash flow, but excludes payments for interest, depreciation, taxes, and changes in working capital; used to analyze and compare profitability between companies
Days cash on hand – how long you can pay your bills if money stopped coming in!
Basic Financial Terminology
Cash to debt – marker of overall financial health of a company, estimate of how long it would take to repay debts if all cash flow devoted to repayment
Accounts receivable days – average number of days that it takes to collect revenue after billed
Accounts payable days – number of days that the institution takes (is allowed) to pay for supplies after purchased

7/19/2014
4
How does this apply to us?
How is money made?
How we bill Charge master – bill for each line item
Each payer has its own rules – usually complicated
DRGs, bundles and outlier payments
How we get paid (simple version) Inpatient encounter (cost center) paid what is in the contractual agreement, not what it
actually costs to care for the patients
Outpatient encounter (revenue center) typically fee for service that is “discounted” based on
contractual agreements
What impacts payments?
Payers negotiate contracts with health care organizations based on quality, services and outcomes
Payer Types: Private – hopefully make money
Government – usually lose money
Self-pay - ???
What impacts payments?
Capitation Fixed sum of money paid per patient in advance to a healthcare entity
in exchange for contracted healthcare services regardless of quantity rendered or costs involved
Per Diem Rates Payment of a daily fee for specific services or outcomes, regardless of
the cost of provision or actual charges
May vary by level of care and usually flat all-inclusive rates
Diagnosis Related Groups (DRG) An inpatient or hospital classification system used to categorize illness by
diagnosis/treatment and to pay a hospitals for services
Used with PPS to reimburse inpatient hospitals, regardless of the cost to provide services
Considerations for Pharmacy
Pharmacy department is a major cost center Maybe also an important revenue center
Drugs billed ≠ inpatient revenue Calculations for drug charges can be complex Higher margin on cheaper products
Tracking inpatient revenue can be tricky
Typical emphasis is on expense management
$$Drug Expense Revenue
Expense Management
Must balance fiscal and patient care issues See issues from both perspectives
Know the literature on value of pharmacy services...and use it
Must spend the right amount of money on labor to manage a large supply budget Do it safely and effectively
80/20 rule

7/19/2014
5
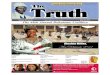
Pharmacy Operating Budget
Three key pharmacy expense classes:
80%
20%
Pharmacy Budget
Drugs & Supplies Labor
Labor = people (salary & benefits)
Drugs & Supplies = drugs, fluids, blood products (factors, albumin), other (labels, paper, etc.)
Other = travel, software, references
Manage your inventory (drugs and supplies)!!
Budget Impact Opportunities
Cost structure Labor expense management
Supply chain management
Operational wastes
Formulary & drug utilization
Revenue growth to improve margin New business growth
Revenue cycle practices Pricing, billing, documentation, collections
Inventory Management
Inventory Management…Supply Chain
Smart purchasing and contracting Strategic contract negotiation
Unit costs
Accounts payable timelines
Shortage versus non-shortage products
Days supply & days on hand
Inventory turns vs product waste Pharmacy areas
Automated dispensing machines
Inventory Management…Operational Wastes Transport – Moving people, products & information
Inventory – Storing parts, pieces, documentation ahead of requirements
Motion – Bending, turning, reaching, lifting
Waiting – For parts, information, instructions, equipment
Over production – Making more than is IMMEDIATELY required
Over processing – Tighter tolerances or higher grade materials than are necessary
Defects – Rework, scrap, incorrect documentation
Skills – Under utilizing capabilities, delegating tasks with inadequate training
Inventory Management…Operational Wastes High-cost drugs – verify before prep
Short stability list
Drip rounds
Dose-banding / rounding
Distribution model (batches, etc)
Tamper proof and reuse
ADC inventory versus cart fill
Inventory Management…Formulary Control Formulary strategies
Develop and enforce evidence based usage criteria
Restrictions (indication/specialty)
Non-Formulary / Do Not Stock
Pharma / Vendor access
Know your payer mix and revenue model Should the drug be used inpatient?
Restrict to OP / clinic use

7/19/2014
6
Inventory Management…Drug Utilization Targeted drug programs
Work with physicians to set targets and guidelines
Know your payer mix per patient service line
Consider total institutional expenses Ventilator days
ICU days & total hospital LOS
Hospital readmissions or ED visits
Clinical benchmarking Internal tracking – over time and service comparisons
External benchmarking – UHC, Premier, etc.
“Soft $” vs.
“Hard $”
Cost reduction
Medication streamlining
Drug X for drug Z
Laboratory tests
Hospital or ICU LOS
Cost avoidance
Hospital or ICU readmit
Formulary restrictions
Inappropriate new drug use
Patient safety (↓ error, preventing cost of harmful med event)
Saved RN or MD time Nurse time at the bedside
Patient throughput and MD efficiency
↑ Operational efficiency
Sometimes cost avoidance
Hard = Actual $$ Soft = Theoretical $$
“Hard” and “Soft” Dollars
How do I get (keep) resources?
Gaining Resources…Defensive
Annual budget showdown
Go where the money is: Demonstrate the 80/20 rule
Cut salary budget, lose ability to control drug budget
Tie cost savings to drug budget and track savings to show Senior Leadership
Benchmarking Use your peers (apples and apples)
Span of control example with like organizations
Be Proactive with Finance Guys
Strong relationship with finance staff means a strong relationship with CFO
Collaborate early and often
CPAs are like RPhs…anal retentive Pay attention to details important to them
Follow their rules and processes
Understand, use, and appreciate their expertise
Communicate the Big Picture
Your senior leaders may have no idea of the full value of Pharmacy, even if you (or your Director) think he/she does
Remember, biggest operational expense is drugs, NOT labor
Demonstrate how Pharmacy labor controls costs and contributes to safety and quality
80%
20%
Pharmacy Budget
Drugs & Supplies Labor

7/19/2014
7
0
500
1000
1500
2000
2500
3000
3500
Mar
-09
Ap
r-09
May
-09
Jun
-09
Jul-
09
Au
g-0
9
Se
p-0
9
Oct
-09
No
v-0
9
De
c-0
9
Jan
-10
Fe
b-1
0
Mar
-10
Ap
r-10
May
-10
Jun
-10
Jul-
10
Au
g-1
0
Se
p-1
0
Oct
-10
No
v-1
0
De
c-1
0
Jan
-11
Fe
b-1
1
Mar
-11
Ap
r-11
May
-11
Jun
-11
Jul-
11
Pat
ien
t E
nco
un
ters
(#)
Patient Safety Activities Patient Care Quality Activities Medication Therapy ManagementMedical Staff & Nursing Support Stewardship & Cost-Containment
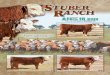
Clinical Pharmacy Interventions
Clinical Pharmacy Interventions
$-
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
$700,000
$800,000
$900,000
0
1000
2000
3000
4000
5000
6000
7000
Jul-
07
Se
p-0
7
No
v-0
7
Jan
-08
Mar
-08
May
-08
Jul-
08
Se
p-0
8
No
v-0
8
Jan
-09
Mar
-09
May
-09
Jul-
09
Se
p-0
9
No
v-0
9
Jan
-10
Mar
-10
May
-10
Jul-
10
Se
p-1
0
No
v-1
0
Jan
-11
Mar
-11
May
-11
Jul-
11
Ph
arm
aco
eco
no
mic
Imp
act
($)
Ph
arm
acis
t P
atie
nt
Car
e S
ervi
ces
(# E
nco
un
ters
)
Patient Care Services Impact ($)
Return on Investment (ROI)
Ratio dividing net benefit by total investment
Straightforward financial tool to define economic return of a project or piece of equipment
Measures “bang for your buck” Value of investment
= ( )Financial Gain – Annual Expense
Annual Expense
Clinical Pharmacy Interventions
77%
138%
196%
128%
144%
131%
121%
146% 15
6%
118%
118%
103% 11
4%
103%
123% 13
2%
146%
130%
117%
181%
216%
207%
187
%
227%
203%
196%
215% 22
0%
211% 22
2%
209%
$134
$185 $183
$175
$167
$144
$161
$150
$163
$145 $152
$140 $142
$126
$134
$126 $128
$119
$104
$122 $129 $130 $127
$134
$117 $120
$139 $137 $143
$152
$130
$-
$20
$40
$60
$80
$100
$120
$140
$160
$180
$200
0%
50%
100%
150%
200%
250%
Jul-
08
Au
g-0
8
Se
p-0
8
Oct
-08
No
v-0
8
De
c-0
8
Jan
-09
Fe
b-0
9
Mar
-09
Ap
r-09
May
-09
Jun
-09
Jul-
09
Au
g-0
9
Se
p-0
9
Oct
-09
No
v-0
9
De
c-0
9
Jan
-10
Fe
b-1
0
Mar
-10
Ap
r-10
May
-10
Jun
-10
Jul-
10
Au
g-1
0
Se
p-1
0
Oct
-10
No
v-1
0
De
c-1
0
Jan
-11
Ave
rag
e In
terv
enti
on
Val
ue
($)
Ret
urn
on
Inve
stm
ent
in P
har
mac
ist
Sal
ary
(%)
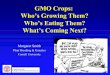
Return on Investment Average Impact per Intervention
Impact of Targeted Labor
90%
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Labor Expense per PIS Discharge Total Pharmacy Expense per PISDischarge
Perc
entil
e Pe
rfor
man
ce v
s Pe
er G
roup
External Benchmarking per Patient Care Service Line
Tradeoff between pharmacist labor and total pharmacy cost
of care (labor + drugs)
$140
$160
$180
$200
$220
$240
2002 2003 2004 2005 2006 2007 2008 2009
Phar
mac
y C
ost /
Inte
nsity
Adj
Dis
char
ge
Institution National
Expense Control vs. Inflation
6.8%
7.9%
5.5%
2.5%
5%
2.5%
2.5%
Hospital vs Inflationary Projections - $$/Patient Day

7/19/2014
8
$102.66
$98.67$101.58
$118.27
$124.09$127.32
$144.89
$102.66
$114.77 $121.77
$134.19
$150.03
$159.03
$170.16
y = 7.3757x + 87.281R² = 0.8879
y = 11.403x + 90.475R² = 0.9942
$85
$95
$105
$115
$125
$135
$145
$155
$165
$175
1999 2000 2001 2002 2003 2004 2005
Hospital vs Inflationary Projections - $$/Patient Day
Hospital Projected Inf Linear (Hospital) Linear (Projected Inf)
Actual Expenses vs. Projected
Actual Drug Cost ($) per Patient Day
Drug Cost ($) per Patient Day based on US Inflation
External Benchmarking…$$
$125
$175
$225
$275
$325
FY05 FY06 FY07 FY08 FY09 FY10 FY11 YTD
Med
icat
ion
Co
st p
er P
har
mac
y In
ten
sity
Ad
just
ed
Dis
char
ge
Institution w/ PPMI UHC - 98%ile UHC - Median Institution w/o PPMI (projected)
$7.6
Total Impact to Insitution = $59
$12.7 million
$12.7 million
$11.4 million
$14.6 million
External Benchmarking…LOS
30.1
9.7
4.7 4.65.9
3.9
18.3
4.1
8.6 8.0 7.7
5.96.6
28.5
25.3
9.4
4.05.2 5.1
3.6
18.1
3.7
6.9 7.46.8
5.16.6
26.5
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
0
5
10
15
20
25
30
35
Len
gth
of
Sta
y In
dex
(O
bse
rved
/ E
xpec
ted
)
Len
gth
of
Sta
y (d
ays)
Patient Services (UHC Service Line)
FY2008 FY2011 FY08 Length of Stay Index FY11 Length of Stay Index
External Benchmarking…Mortality
1.65
1.26
1.08
0.52
0.78
0.71
1.31
0.73 0.
80
0.78
1.14
0.87
0.48
1.08
0.6
3
1.8
6
0.9
4
0.6
0
0.6
4 0.7
4
1.1
2
0.5
5
0.9
4
0.4
8
0.7
5
0.6
7
0.7
1
1.0
5
0.8
2
1.0
9
0.9
0
0.6
4
0.6
2 0.6
9 0.7
4
0.5
7
0.7
0
0.6
5
1.6
0
0.8
9
0.6
0
0.9
5
0.8
0
0.9
5
0.7
8
0.4
5
0.4
9
0.4
6
0.6
3
0.5
9
0.7
9
0.9
4
0.8
9
0.4
0
0.7
6 0.8
5
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
2.00
Mo
rtal
ity
Ind
ex (
Ob
serv
ed M
ort
alit
y / E
xpec
ted
Mo
rtal
ity)
Patient Services (UHC Service Line)
FY2008 FY2009 FY2010 FY2011
Clinical Outcomes Dashboard
Medical Oncology Cardiology
FY08 FY09 FY10 FY11 FY08 FY09 FY10 FY11
Cases (n) 1,753 1,782 1,757 1,454 2,057 1,728 1,766 1,306
Cases with ≥ 1 complication (per 100 Cases) 2 1 1 1 3 3 3 2
Mean observed mortality (%) 3.37% 2.92% 2.45% 2.20% 3.60% 3.36% 3.40% 3.02%
Mean expected mortality (%) 4.31% 4.54% 3.95% 4.50% 3.34% 3.59% 3.79% 3.89%
Mortality index (observed/expected) 0.78 0.64 0.62 0.49 1.08 0.94 0.90 0.78
Mean observed length of stay (days) 5.93 5.74 5.50 5.14 4.69 4.58 4.70 4.03
Mean expected length of stay (days) 6.48 6.54 6.49 6.36 5.22 5.19 5.19 5.44
Length of stay index (observed/expected) 0.92 0.88 0.85 0.81 0.90 0.88 0.90 0.74
Mean drug cost per case ($) $1,285 $1,034 $ 905 $1,240 $508 $525 $509 $448
Medicine General Ventilator Support
FY08 FY09 FY10 FY11 FY08 FY09 FY10 FY11
Cases (n) 5,816 5,462 4,883 4,206 286 285 279 234
Cases with ≥ 1 complication (per 100 Cases) 1 2 2 1 45 37 39 19
Mean observed mortality (%) 2.13% 2.51% 2.29% 1.35% 31.0% 29.1% 23.7% 24.1%
Mean expected mortality (%) 2.98% 3.38% 3.34% 2.96% 28.6% 27.8% 24.9% 28.5%
Mortality index (observed/expected) 0.71 0.74 0.69 0.46 1.08 1.05 0.95 0.85
Mean observed length of stay (days) 3.95 3.96 4.17 3.64 28.51 28.02 30.47 26.46
Mean expected length of stay (days) 4.53 4.51 4.48 4.41 31.58 29.24 31.85 28.80
Length of stay index (observed/expected) 0.87 0.88 0.93 0.83 0.90 0.96 0.96 0.92Mean drug cost per case ($) $422 $458 $545 $348 $4,272 $4,118 $3,875 $3,196
Gaining Resources…Proactive
Understand national trends Where is the rest of the world with antimicrobial
stewardship, ED pharmacy, medication histories, etc.?
Use examples of what other institutions are doing
Share literature with your CEO, VP, CFO ASHP push news, HealthLeaders.com, etc.
Be realistic and be a team player Understand financial, political, and cultural trends
Sometimes what you need is not the highest priority
Know when to push and when to bid your time

7/19/2014
9
Gaining Resources…Proactive
Adding services (primarily labor cost) Emphasis value-added programs for institution
Build on current successes and existing infrastructure
Develop a good Business Plan Proposal to build a case for the new service or product
Demonstrate the return on investment (ROI)
Pro Forma – method of calculating financial results in order to emphasize either current or projected figures
Business Plans: Where do I start?
Review an example of a business plan that was approved in your organization
Ask colleagues elsewhere for template used to justify their new program ASHP Leadership Academy
Clarify expectations Who will be reading it?
How many pages is it expected to be?
Are their defined/expected sections standard for your organization?
Common Business Plans
Antimicrobial stewardship program
Anticoagulant management clinic
ICU sedation management program
ED pharmacist program
New disease state or service line partnerships Solid organ transplant
Orthopedics
Oncology
Cardiovascular surgery
Adverse Drug Events Prevention Program
High‐Risk Medication Management Program
Rapid Response Team
Code Response Team
Evidence‐Based Care for Acute Myocardial Infarction
Evidence‐Based Care for Congestive Heart Failure
Reduce Surgical Complications
Reduce MRSA
Prevent Central Line Infections
Prevent Surgical Site Infections
Prevent Ventilator Associated Pneumonia
Pharmacy Residency Program
Value-Added Opportunities
Talk Listen to your C-suite
Share your preliminary ideas and ask for their input Who doesn’t like being seen as an expert?
What do they believe is most pressing to the organization and who are the stakeholders?
What they think pharmacy can do to support that goal and to support the stakeholders?
Things You MUST Know
Your organization’s strategic plan Incorporate your new program to align easily
Also reference how your new service supports your institution’s Mission and Vision statements
Who are your key supporters and stakeholders? Who has your back? (be ready to name drop)
Physicians
Nursing Leadership
Quality Department
Patient Safety Officer

7/19/2014
10
Business Plan Components
Executive Summary
High overview (1 page)
This is like an “abstract”
Proposal: 2 sentences about the program
Organizational benefits
Cost
Write this last
Background
Published literature, best practices
Current practice at your facility (DATA!!)
Impact Regulatory Quality measures Safety standards
Business Plan Components
Description of Program
Proposed activities & new services
Define workflows
Patient populations or care areas supported
Interaction with other departments
Hours of service
Resource Requirements
Labor (FTEs) & salary Include benefits Think 5-year plan
Supplies Computer, technology Etc.
Patient safety Decrease errors
Patient satisfaction
Revenue generation Increase Rx volume
New reimbursement
Cost savings, avoidance Drug replacement
Decreased drug waste
Regulatory compliance Improved
Clinical outcomes Quality indicators Efficiency, effectiveness
of other providers Continuity of care
Decrease re-admission rates, ED visits
Business Plan Components
Benefits to the Organization
Benefit Calculations
ROI Calculation Pearls
Adhere to financial standards and partner with finance and decision support to know what they expect
Understand the difference between hard and soft savings
Always include ROI in business case for any new program or service
Become savvy with spreadsheets
Don’t leave it until the end – they take time!
Costs
Capital: Year 0 Technology, equipment,
remodeling
Operating: Years 1+ Drugs, labor,
maintenance, supplies
Financial Return
Revenue/margin Growth
Charge capture
Reimbursement capture
Savings Hard savings
Soft savings
Core Elements to be Presented

7/19/2014
11
Example…Antibiotic Stewardship
Antibiotic "X" $100 per dose7 days of therapy
Total Cost "X" $700 per patient
Net Savings = $450 per patient(a.k.a. Financial Return)
Antibiotic "Y" $5 per dose7 days of therapy
$35 drug costs
PK Monitoring $15 per lab test3 tests
$45 lab costs
Pharmacist Time $60 per hourInitial Assessment 45 minutes
1 initial evaluation$45 labor costs
Pharmacist Time $60 per hourFollow Up 25 minutesAssessments 5 follow up eval.
$125 labor costs
Total Cost "Y" $250 per patient
Example…Antibiotic Stewardship
Per Patient Annual Volume TotalTotal Cost "X" $700 1000 patients $700,000 Total Cost "Y" $250 1000 patients $250,000 Net Savings $450,000
ROI = 2.65
Pharmacist $170 / patient $170,000 2.8 h / patient 1.4 FTE
Equivalent to one RPh for 8-hr shift x 7 days per week (~20 patients per week average)
Other Examples
Labor CostDrug
Savings Net Savings ROIEBDIT Impact
Blood Conservation 1,237,360 1,237,360 100.0%
Formulary and Cerner Changes 933,397 933,397 100.0%
Parenteral Nutrition 117,750 117,750 100.0%
ICU Sedation Management 792,000 1,273,025 481,025 0.61 37.8%
Antimicrobial Stewardship 1,026,652 2,048,787 1,022,135 1.00 49.9%
Thrombin Inhibitors 120,115 307,648 187,532 1.56 61.0%
Colony Stimulating Factors 163,212 422,409 259,197 1.59 61.4%
Pharmacy Compounding 196,500 723,155 526,655 2.68 72.8%
Drug Replacement Program 84,115 469,682 385,567 4.58 82.1%
Impact 2014 $2,382,594 $7,533,213 $5,150,620
23.5 FTE added to Budget
Additional Calculations
Total and cumulative net savings
Benefit/Cost Ratio
Net Present Value (NPV)
Internal Rate of Return (IRR)
Break-Even Point
Life expectancy
Work with your Finance Department on these calculations!!!
Patient safety (reduced error)
Patient satisfaction
Provider satisfaction
Operational efficiency
Continuity of care
Readmission rates
Patient outcomes
Regulatory compliance
Quality indicators including pay for performance
Improved throughput
MD efficiency
Education/research
Non Financial Benefits
Don’t Forget to Include…
Appendices (place in order of reference in Business Plan)
ROI data sheets with calculations and assumptions
Literature review
Flow charts
Gantt charts
Pilot data
Project plan
References Include both Best Practice documents & medical
literature
Regulatory Guidelines

7/19/2014
12
Keys to a Winning Proposal
Know Your Numbers Published literature & your organization
Make it personal Examples from your institution
Highlight benefits to: Patients
Providers
Other Departments
Etc.
Practice your “elevator speech”
Elevator Speech
Quick (30-60 seconds) overview of a service, project or proposal
Perfect for communicating new initiatives to others outside of pharmacy
Focuses on: Why it is important
What the impact will look like (WIIFM?)
What you are requesting the stakeholder to support
Helpful Hints
Have first draft ready in time to collect feedback 3-5 trusted peers (internal and external)
Develop FAQs and talking points for your boss
Build in assumptions for growth Critically reevaluate after years one and two
Always have a rolling 5-year plan
Look for synergies with future initiatives
Good publicity is not just a defense mechanism Initiation, maintenance, & expansion
Strength in your supporters
Align with Organizational Goals
A great business plan is a must, but timing is everything
Organizational Goals Change So yours have to, too
Be flexible, be supportive of the organization
Pressures on executives are high
Provide options Various means to solve a problem
Negative outcomes if a goal is not achieved
Phases to implementation
Doesn’t End with Job Well Done
Communicating your activities and accomplishments is critical
Presenting your success (humbly) is just as important
Your job is to remind / (re) educate Executives,
Nursing Leaders and Department Directors
Plan on repeating yourself often and as needed
An Opportunity Awaits You…

7/19/2014
13
48th Annual Meeting
Navigating the Oceans of Opportunity
Business Side of Pharmacy Leadership: Proving Pharmacy
Department Added Value
Heath Jennings, PharmD, MBA, FASHP, BCPS